Midshaft Clavicle Fractures: An Evidence-Based Guide to Diagnosis, Management, and Outcomes
Key Takeaway
Operative management for midshaft clavicle fractures is indicated for open fractures, neurovascular compromise, or severe skin compromise. Relative indications include significant displacement (>100%), shortening (>1.5-2cm), severe comminution, and nonunion, especially in high-demand patients, aiming to restore anatomical alignment and optimize functional outcomes.
Introduction and Epidemiology
Midshaft clavicle fractures are a common musculoskeletal injury, accounting for approximately 2.6 percent to 5 percent of all adult fractures and up to 44 percent of all shoulder girdle fractures. They typically result from a direct blow to the shoulder or a fall onto an outstretched arm. Historically, these fractures were predominantly managed non-operatively, with high union rates and satisfactory functional outcomes reported for many fracture patterns. However, advancements in surgical techniques and fixation hardware, coupled with a deeper understanding of fracture biomechanics and the functional implications of malunion, have led to an evolving paradigm in treatment.
The shift towards operative management for specific fracture patterns is driven by evidence suggesting improved functional outcomes, lower rates of symptomatic malunion, and reduced time to union in select patient populations. This comprehensive review aims to delineate the current understanding of midshaft clavicle fractures, providing an evidence-based framework for treatment selection, surgical technique, and post-operative management, targeting orthopedic surgeons, residents, and medical students.
Demographics and Mechanism of Injury
The epidemiology of midshaft clavicle fractures demonstrates a bimodal distribution. The first peak occurs in young, active males, typically in their second or third decade of life, usually secondary to high-energy trauma such as motor vehicle collisions, cycling accidents, or contact sports. The mechanism often involves a direct lateral compressive force applied to the shoulder girdle. The second peak occurs in elderly individuals, predominantly females, and is associated with low-energy falls, reflecting underlying osteopenia or osteoporosis.
Classification Systems
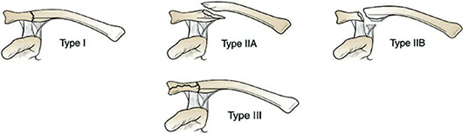
Standardization of fracture description is paramount for guiding treatment and comparing outcomes in the literature. The Allman classification broadly categorizes clavicle fractures by anatomic location, with Type I representing midshaft fractures (accounting for approximately 80 percent of all clavicle fractures). The Robinson classification provides a more granular assessment of midshaft fractures (Type 2), further subdividing them based on displacement and comminution. Type 2A represents undisplaced fractures, while Type 2B represents displaced fractures. Type 2B is further divided into 2B1 (simple or single butterfly fragment) and 2B2 (comminuted or segmental). This classification has demonstrated high inter-observer reliability and prognostic value regarding the risk of nonunion with non-operative management.
Surgical Anatomy and Biomechanics
The clavicle is a unique S-shaped long bone, serving as the sole bony connection between the axial skeleton and the upper extremity. Its critical functions include maintaining the length of the shoulder girdle, protecting the underlying neurovascular structures, and providing attachment points for several muscles vital for shoulder motion and stability.
Key Anatomical Features
The structural anatomy of the clavicle dictates both its fracture patterns and the surgical approaches utilized for fixation. The medial two-thirds are convex anteriorly and tubular in cross-section, while the lateral one-third is concave anteriorly and flattened superior-inferiorly. The midshaft is the narrowest and weakest portion, lacking ligamentous support, making it most susceptible to fracture under axial loading.
Muscular attachments exert significant deforming forces on fracture fragments. Superiorly, the trapezius inserts on the lateral third, while the sternocleidomastoid originates from the medial third. Inferiorly, the subclavius lies in the subclavian groove, the pectoralis major originates from the medial half, and the deltoid originates from the lateral half. Ligamentous attachments include the sternoclavicular ligaments medially and the acromioclavicular and coracoclavicular ligaments laterally. The coracoclavicular ligaments (trapezoid and conoid) are crucial for suspending the scapula from the clavicle.
Neurovascular Proximity
A thorough understanding of the regional neurovascular anatomy is critical to avoid iatrogenic injury during surgical intervention. Immediately posterior and inferior to the middle third of the clavicle lie the subclavian artery, subclavian vein, and the brachial plexus. The subclavian vein is the most anterior of these structures and can be situated mere millimeters from the posterior cortex of the clavicle, particularly in the medial midshaft.
Superficially, the supraclavicular nerves arise from the cervical plexus (C3-C4) and descend over the clavicle to provide sensation to the anterior chest wall and shoulder. These nerves are highly variable in their branching patterns (medial, intermediate, and lateral branches) and are vulnerable during surgical incision and dissection. Injury to these nerves results in anterior chest wall numbness, which is a frequent source of post-operative patient dissatisfaction.
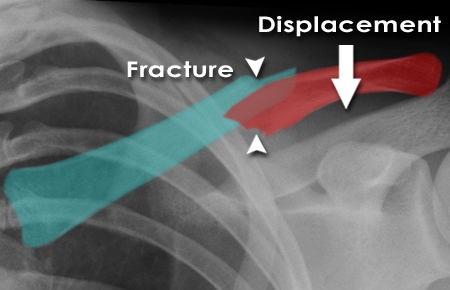
Biomechanics of Fracture and Displacement
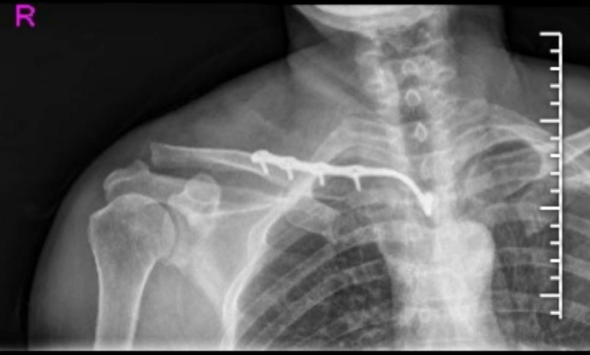
Midshaft clavicle fractures typically result in characteristic displacement patterns driven by the aforementioned muscular attachments. The medial fragment is invariably pulled superiorly and posteriorly by the sternocleidomastoid muscle. Conversely, the lateral fragment is pulled inferiorly and medially by the weight of the arm and the action of the deltoid and pectoralis major muscles.
This combination of forces frequently leads to significant shortening, particularly in the presence of comminution. Shortening greater than 1.5 to 2.0 centimeters alters the resting length and tension of the shoulder girdle musculature, altering glenohumeral and scapulothoracic kinematics. Biomechanical studies have demonstrated that significant clavicular shortening decreases the efficiency of the pectoralis major and latissimus dorsi, and can lead to scapular dyskinesia. The intramedullary canal of the clavicle is relatively narrow and variable, making traditional intramedullary nailing technically demanding and less rotationally stable for comminuted patterns compared to plate osteosynthesis.
Indications and Contraindications
The decision-making process for midshaft clavicle fractures requires a careful assessment of fracture characteristics, patient factors, and functional demands. While many fractures still heal with non-operative management, specific indications for surgical intervention have become more clearly defined based on prospective randomized trials demonstrating decreased nonunion rates and improved early functional outcomes with internal fixation for specific fracture patterns.
Operative Versus Non Operative Decision Matrix
The following table summarizes the widely accepted absolute and relative indications for the operative management of midshaft clavicle fractures, contrasted with indications for non-operative care.
| Category | Operative Management | Non Operative Management |
|---|---|---|
| Absolute Indications | Open fractures | Undisplaced fractures |
| Associated neurovascular injury | Minimally displaced fractures (< 100% translation) | |
| Skin tenting with impending compromise | Fractures with < 1.5 cm shortening | |
| "Floating shoulder" (ipsilateral scapular neck fracture) | Active infection over the surgical site (Contraindication) | |
| Relative Indications | Displacement > 100% (no cortical contact) | Medically unfit for anesthesia |
| Shortening > 1.5 to 2.0 cm | Severe cognitive impairment precluding rehab compliance | |
| Severe comminution or Z-deformity | Low functional demand patients | |
| Polytrauma requiring early weight-bearing through upper extremities | ||
| High-demand athletes or manual laborers | ||
| Symptomatic nonunion or malunion |
Non-operative management typically consists of a period of immobilization in a simple sling or figure-of-eight brace. Current literature suggests no functional difference or difference in union rates between a sling and a figure-of-eight brace, though slings are generally associated with higher patient comfort and fewer skin complications. Non-operative treatment of significantly displaced fractures carries a nonunion rate of approximately 15 percent, compared to 1 to 2 percent with operative fixation. Furthermore, non-operative management of displaced fractures has a higher incidence of symptomatic malunion, which can present with weakness, rapid fatigability, and cosmetic deformity.
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is essential for successful surgical execution and the minimization of complications. This begins with a comprehensive clinical and radiographic evaluation.
Radiographic Evaluation and Templating
Standard radiographic evaluation includes an anteroposterior (AP) view of the clavicle and a 15 to 20 degree cephalic tilt view. The cephalic tilt view projects the clavicle free from the underlying ribs and provides a more accurate assessment of superior-inferior displacement and shortening. In cases of severe comminution, marked displacement, or suspected intra-articular extension into the sternoclavicular or acromioclavicular joints, a computed tomography (CT) scan with 3D reconstructions is highly recommended. CT imaging provides precise characterization of butterfly fragments and aids in determining the appropriate length and contour of the fixation construct.
Pre-operative templating should be performed using digital software to estimate plate length, screw sizes, and the necessity for lag screws. The surgeon must evaluate the bone quality and the location of the fracture relative to the medial and lateral ends of the clavicle to ensure adequate cortical purchase can be obtained on both sides of the fracture. Generally, a minimum of three bicortical screws (six cortices) on each side of the fracture is required for stable plate osteosynthesis.
Anesthesia and Positioning
Surgery is typically performed under general anesthesia. The addition of a regional anesthetic, such as an interscalene brachial plexus block or a superficial cervical plexus block, provides excellent peri-operative analgesia and reduces the requirement for systemic opioids.
The patient is positioned in a modified beach chair position with the head of the bed elevated 30 to 45 degrees. A bump is placed between the scapulae to allow the shoulder girdle to fall posteriorly, which frequently aids in restoring the length of the clavicle and reducing the fracture. The head must be securely stabilized, and the eyes protected. The entire upper extremity, shoulder girdle, and ipsilateral anterior chest wall to the sternum are prepped and draped free. This wide sterile field allows for manipulation of the arm to assist with fracture reduction and permits extension of the incision if necessary. The C-arm fluoroscopy unit should be positioned on the contralateral side or at the head of the bed, ensuring orthogonal views of the clavicle can be obtained without compromising the sterile field.
Detailed Surgical Approach and Technique
Open reduction and internal fixation (ORIF) with plate osteosynthesis remains the gold standard for the operative management of displaced midshaft clavicle fractures. Intramedullary fixation is an alternative for specific simple fracture patterns but is less commonly utilized due to hardware migration risks and lack of rotational control in comminuted fractures.
Incision and Superficial Dissection
The surgical approach utilizes an incision parallel to the longitudinal axis of the clavicle. Historically, an incision directly over the superior border of the clavicle was utilized. However, to minimize the risk of symptomatic hardware prominence and to improve cosmesis, an anteroinferior incision or an incision placed within Langer’s lines (supraclavicular bra-strap line) is often preferred.
The skin and subcutaneous tissues are incised down to the platysma. The platysma is carefully divided in line with the incision. At this stage, meticulous attention must be paid to identifying and protecting the branches of the supraclavicular nerve. These branches run perpendicular to the clavicle in the subcutaneous tissue. Whenever feasible, the nerves should be mobilized and retracted using vessel loops. Transection of these nerves leads to a predictable area of anesthesia over the anterior chest, and while often well-tolerated, painful neuroma formation can occur.
Deep Dissection and Fracture Exposure
Following the identification and protection of the superficial nerves, the clavipectoral fascia is incised. The periosteum is incised longitudinally along the anterior or superior border of the clavicle, depending on the planned plate position. Periosteal stripping must be kept to an absolute minimum, exposing only enough bone to achieve reduction and apply the plate. Excessive periosteal stripping devascularizes the bone fragments, significantly increasing the risk of nonunion. In highly comminuted fractures, butterfly fragments should be left attached to their soft tissue pedicles to preserve their blood supply.
Reduction Techniques
Fracture reduction is often the most challenging aspect of the procedure due to the deforming muscle forces. The medial fragment is typically elevated, and the lateral fragment is depressed and shortened. Reduction can be facilitated by manipulating the ipsilateral arm; abducting and extending the arm often helps restore length.
Direct reduction techniques utilize pointed reduction forceps. A Weber clamp can be placed across the main fragments to restore length and alignment. If a large butterfly fragment is present, it can be anatomically reduced and provisionally stabilized with Kirschner wires or definitively fixed with independent lag screws prior to the application of the neutralization plate. In cases of severe, irreducible shortening, a laminar spreader can be carefully placed between the major fragments to dial in length, taking extreme care not to plunge posteriorly into the neurovascular bundle.
Plate Selection and Application
The choice between superior and anteroinferior plating depends on fracture morphology, surgeon preference, and biomechanical considerations.

Superior Plating:
Applying the plate to the superior surface of the clavicle places it on the tension side of the bone, which is biomechanically advantageous. Pre-contoured locking plates are widely available and match the complex S-shape of the clavicle, reducing the need for intra-operative bending. However, the superior aspect of the clavicle has minimal soft tissue coverage, leading to a higher incidence of symptomatic hardware prominence, particularly in thin individuals, which may necessitate hardware removal. During superior plating, the drill bit is directed inferiorly; the surgeon must use a drill stop or meticulous technique to avoid plunging into the subclavian vessels or pleura.
Anteroinferior Plating:
Placing the plate on the anteroinferior surface offers several advantages. The screws are directed posterosuperiorly, aiming away from the critical neurovascular structures and pleura, providing a significant safety margin. Furthermore, the screws can be longer, as they traverse the wider anteroposterior dimension of the clavicle, potentially increasing pull-out strength. The plate is also better covered by the anterior soft tissues, reducing hardware prominence. However, contouring a standard reconstruction plate to the anteroinferior surface can be challenging, though pre-contoured anteroinferior plates are now available.
Once the plate is appropriately positioned and the fracture is reduced, the plate is secured. A non-locking screw is typically placed first to pull the bone to the plate, followed by locking screws for fixed-angle stability, particularly in osteoporotic bone or comminuted patterns. A minimum of three bicortical screws per major fragment is required.
Closure
Following thorough irrigation and hemostasis, the clavipectoral fascia and platysma are meticulously closed in a separate layer to ensure adequate coverage of the hardware. The subcutaneous tissue and skin are closed using standard techniques. A sterile dressing is applied, and the arm is placed in a sling.
Complications and Management
While operative management of clavicle fractures yields high union rates and excellent functional outcomes, it is not without risks. The surgeon must be prepared to manage both early and late complications.

Summary of Operative Complications
The following table outlines the most common complications associated with the surgical fixation of midshaft clavicle fractures, their approximate incidence in the literature, and established salvage strategies.
| Complication | Approximate Incidence | Salvage Strategy and Management |
|---|---|---|
| Symptomatic Hardware | 10% - 30% | Hardware removal after clinical and radiographic union (typically > 12-18 months). More common with superior plating. |
| Neuroma / Chest Wall Numbness | 10% - 20% | Supraclavicular nerve injury. Often self-limiting. Refractory neuromas may require excision and burying of the nerve stump into muscle. |
| Nonunion | 1% - 5% | Revision ORIF with autologous bone grafting (iliac crest) and robust fixation (locking plate +/- orthogonal plating). Assess for indolent infection. |
| Infection (Deep) | 1% - 4% | Irrigation and debridement. Retention of hardware if stable and fracture unhealed, with targeted IV antibiotics. Hardware removal if healed or unstable. |
| Adhesive Capsulitis | 2% - 5% | Aggressive physical therapy. Intra-articular corticosteroid injections. Rarely requires arthroscopic capsular release. |
| Hardware Failure | 1% - 3% | Revision ORIF. Often secondary to nonunion, poor bone quality, or inadequate initial fixation (e.g., insufficient cortices). |
| Neurovascular Injury | < 1% | Immediate intra-operative consultation with vascular or thoracic surgery. Prevented by meticulous drilling technique and directional awareness. |
| Pneumothorax | < 1% | Chest tube thoracostomy if symptomatic or large. Prevented by avoiding inferiorly directed plunging with the drill. |
Management of Nonunion and Malunion
Nonunion is defined as the lack of radiographic progression of healing at six months post-injury, accompanied by clinical symptoms (pain, mobility at the fracture site). Atrophic nonunions require biological augmentation, typically via iliac crest bone grafting, combined with rigid internal fixation. Hypertrophic nonunions primarily require mechanical stabilization to heal, often achieved by removing the fibrous tissue, decorticating the bone ends, and applying a robust locking plate construct.
Symptomatic malunion, typically seen after non-operative management of severely shortened fractures, presents with shoulder weakness, rapid fatigability, and altered scapular kinematics. Corrective osteotomy is indicated for these patients. The procedure involves taking down the malunion, restoring the anatomic length of the clavicle (often requiring an intercalary structural bone graft), and applying rigid plate fixation.
Post Operative Rehabilitation Protocols
A structured, phased rehabilitation protocol is critical for optimizing functional recovery while protecting the surgical fixation. The protocol must be tailored to the individual patient, the security of the fixation, and the presence of any associated injuries.
Phase One Early Protection
From post-operative day one to approximately two weeks, the primary goals are pain control, wound healing, and protection of the osteosynthesis. The patient is immobilized in a sling. Immediate active range of motion of the elbow, wrist, and hand is encouraged to prevent stiffness and reduce edema. Pendulum exercises for the shoulder can be initiated within the first few days, provided the patient is comfortable. Active shoulder elevation is strictly avoided to prevent excessive muscular forces across the fracture site.
Phase Two Active Motion
Between two and six weeks post-operatively, as early soft callus formation begins, the sling is gradually weaned. The patient transitions to active-assisted and then active range of motion exercises for the shoulder. Supine forward elevation using a wand or the contralateral arm is initiated, progressing to upright active elevation. Internal and external rotation exercises are also incorporated. Strengthening exercises and lifting are still prohibited during this phase.
Phase Three Strengthening and Return to Function
At six to eight weeks, clinical and radiographic evaluation should demonstrate progressive fracture consolidation. Once healing is confirmed, resistance exercises and formal strengthening of the rotator cuff and periscapular stabilizers are initiated. Isotonic exercises using resistance bands or light weights are introduced. Scapular dyskinesia, if present, is specifically addressed through targeted physical therapy.
Return to high-demand activities, heavy manual labor, or contact sports is generally permitted between three and four months post-operatively, contingent upon full, painless range of motion, normal strength compared to the contralateral side, and definitive radiographic evidence of bony union.
Summary of Key Literature and Guidelines
The paradigm shift towards the operative management of displaced midshaft clavicle fractures is heavily rooted in high-quality prospective randomized controlled trials.
The landmark study by the Canadian Orthopaedic Trauma Society (COTS), published in the Journal of Bone and Joint Surgery in 2007, fundamentally altered the treatment landscape. This multicenter randomized clinical trial compared non-operative treatment (sling) to operative treatment (plate fixation) in 132 patients with completely displaced midshaft clavicle fractures. The study demonstrated significantly improved functional outcomes (DASH and Constant scores) at all time points up to one year in the operative group. Furthermore, the nonunion rate was 15 percent in the non-operative group compared to only 2 percent in the operative group. Symptomatic malunion occurred in 9 percent of the non-operative cohort and 0 percent of the operative cohort.
Subsequent meta-analyses and systematic reviews have corroborated these findings. Altamimi et al. demonstrated that operative fixation of displaced midshaft fractures reduces the relative risk of nonunion by 86 percent compared to non-operative treatment. Robinson et al. conducted extensive epidemiological and prognostic studies, identifying risk factors for nonunion in non-operatively managed fractures, including advancing age, female gender, complete displacement, and significant comminution.
Despite the strong evidence favoring surgery for displaced fractures, the orthopedic surgeon must maintain a balanced perspective. Recent literature has highlighted the high rate of secondary operations for hardware removal following plate fixation (up to 30 percent in some series). Therefore, the decision to operate must involve a shared decision-making process, carefully weighing the benefits of early functional return and decreased nonunion risk against the inherent risks of surgery, infection, and the potential need for future hardware removal. Current guidelines recommend operative fixation for completely displaced fractures with > 1.5 cm of shortening, severe comminution, or in high-demand patients, while maintaining non-operative management as the standard of care for minimally displaced or undisplaced fractures.
You Might Also Like