Spring Ligament Reconstruction: Regain Foot Stability
Key Takeaway
For anyone wondering about Spring Ligament Reconstruction: Regain Foot Stability, Spring ligament failure is the lengthening or disruption of the spring ligament complex, causing talonavicular joint subluxation and often a progressive flatfoot deformity. This condition typically involves ligament degeneration, tears, or attenuation, frequently due to repetitive stress. Severe cases, particularly with flatfoot and significant tears, may necessitate **spring ligament reconstruction** to restore foot alignment and function.
Introduction and Epidemiology
Spring ligament failure represents a critical pathological event in the cascade of adult acquired flatfoot deformity, recently reclassified as Progressive Collapsing Foot Deformity. The spring ligament complex, anatomically known as the plantar calcaneonavicular ligament, is the primary static stabilizer of the talonavicular joint. Failure of this complex consists of lengthening, attenuation, or complete disruption, resulting in predictable subluxation at the talonavicular joint.
Epidemiologically, spring ligament insufficiency is most frequently encountered in middle-aged to elderly females, often in conjunction with posterior tibial tendon dysfunction. However, isolated spring ligament tears can occur in athletic populations secondary to acute trauma or repetitive microtrauma. The pathogenesis is primarily driven by the repetitive stresses of a preexisting pes planovalgus architecture, which places increased eccentric strain on the medial soft tissue stabilizers of the foot. Failure most often occurs in the setting of a degenerated, fibrotic ligament, though acute traumatic avulsions are documented.
Once spring ligament failure occurs, it frequently results in progressive, multiplanar deformity of the foot at the talonavicular joint and hindfoot. Because the foot progresses out from under the talar head dorsally and laterally, the talar head migrates medially and plantarly in relation to the rest of the foot. Recognizing the precise location and severity of the spring ligament injury is paramount, as failure to address this specific anatomical defect during flatfoot reconstruction leads to high rates of recurrent deformity and persistent medial-sided pain.
Surgical Anatomy and Biomechanics
Structural Anatomy of the Spring Ligament Complex
The spring ligament is not a single discrete band but rather a complex of ligaments composed primarily of a superomedial portion and an inferior portion. It forms the structural floor and medial wall of the acetabulum pedis, articulating directly with the articular cartilage of the talar head.

Anatomy of the spring ligament complex from a dorsal view with the talar head removed. The superomedial portion is medial to the posterior tibial tendon.
The superomedial portion is the most robust and clinically significant component. It is located medial to the posterior tibial tendon and often blends intimately with the superficial deltoid ligament (specifically the tibiospring ligament). It originates from the superomedial aspect of the sustentaculum tali and the anterior facet of the calcaneus, coursing distally to insert on the medial navicular adjacent to its articular surface.

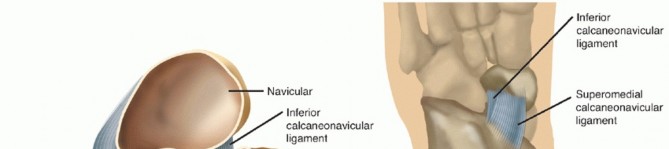
Anatomy of the spring ligament complex seen from the plantar view. The inferior portion originates from the notch between the anterior and medial calcaneal facets.
The inferior portion (plantar calcaneonavicular ligament) originates from the notch between the anterior and medial calcaneal facets. It inserts on the inferior surface of the midnavicular, just lateral to the insertion of the superomedial portion of the spring ligament. A third, less constant band—the medioplantar oblique ligament—is occasionally described in anatomical literature but holds less distinct clinical relevance during surgical reconstruction.
Kinematics and Pathomechanics
Biomechanically, the spring ligament complex acts as a sling for the talar head. It resists plantarflexion and medial deviation of the talus during the stance phase of gait.

Illustration demonstrating the medial and plantar migration of the talar head following spring ligament attenuation.
Because of its specific anatomical location, failure of the superomedial portion results primarily in medial migration of the talar head, leading to forefoot abduction and uncovering of the talonavicular joint. Conversely, failure of the inferior portion results primarily in plantar migration of the talar head, contributing to the collapse of the medial longitudinal arch and increased talar pitch.

Sagittal and axial representations of talar head migration. Most commonly, the migration is both medial and plantar due to combined failure of the complex.
Tears most commonly occur in the superomedial portion of the spring ligament complex, adjacent to the posterior tibial tendon, but can occur in the inferior portion as well. The ligament complex may exhibit focal tears, large full-thickness defects, or diffuse attenuation with substantial myxoid degeneration.
Indications and Contraindications
Clinical Evaluation and Imaging
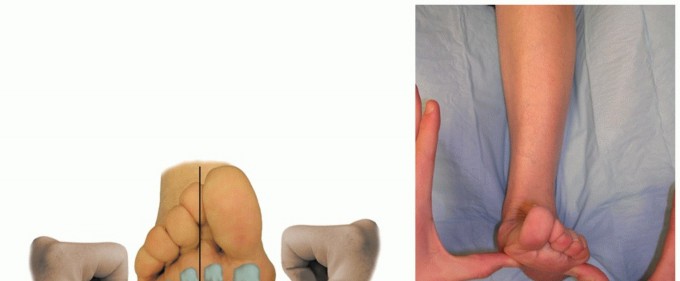
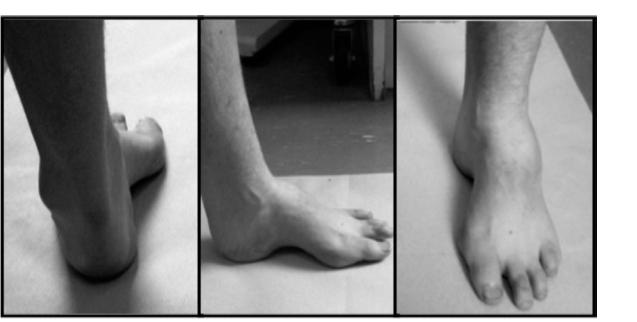
It is necessary to look at the overall alignment of the foot to determine how to treat failure in the spring ligament. Clinical examination typically reveals a flatfoot posture with increased heel valgus, forefoot abduction, and midfoot sag. The "too many toes" sign is invariably present. Palpation will elicit tenderness directly over the superomedial spring ligament, which is located between the medial malleolus and the navicular tuberosity, often deep to or slightly plantar to the posterior tibial tendon.
Weight-bearing radiographs are mandatory. Key radiographic parameters indicating spring ligament failure include an increased talonavicular coverage angle (uncovering of the talar head), an increased Meary's angle (talus-first metatarsal angle), and decreased calcaneal pitch. Magnetic Resonance Imaging (MRI) is highly sensitive for detecting spring ligament pathology. If a flatfoot is present with increased heel valgus or abduction through the midfoot and there is a full tear of more than 30 percent of the ligament or severe attenuation, the risk of progression of deformity is exceptionally high, warranting surgical intervention.
Operative vs Non Operative Management
| Indication Type | Clinical and Radiographic Findings | Recommended Management |
|---|---|---|
| Non-Operative | Flexible deformity, mild symptoms, intact spring ligament on MRI, high surgical risk | Custom articulated AFO, physical therapy, NSAIDs, activity modification |
| Operative | Symptomatic flexible PCFD, MRI confirmed >30% tear or severe attenuation of spring ligament | Joint-sparing reconstruction (Spring ligament repair/reconstruction + osteotomies + tendon transfers) |
| Operative | Rigid deformity, severe arthritic changes at the talonavicular or subtalar joints | Arthrodesis (Subtalar, Talonavicular, or Triple Arthrodesis) |
| Contraindications | Active infection, severe peripheral vascular disease, Charcot neuroarthropathy | Debridement, optimization, Charcot-specific offloading |
Pre Operative Planning and Patient Positioning
Surgical Strategy and Adjunctive Procedures
Spring ligament reconstruction is rarely performed in isolation. The underlying biomechanical forces that caused the ligament to fail must be addressed to protect the repair. Preoperative planning must include a comprehensive assessment of the necessary adjunctive procedures. These typically include a medializing calcaneal osteotomy to correct hindfoot valgus, a lateral column lengthening (Evans osteotomy) to correct forefoot abduction, and a posterior tibial tendon debridement with flexor digitorum longus transfer. If residual forefoot varus exists after hindfoot correction, a medial cuneiform dorsal opening wedge osteotomy (Cotton osteotomy) or first tarsometatarsal arthrodesis is planned.

Preoperative planning includes assessment of all necessary bony corrections to protect the medial soft tissue reconstruction.
Patient Positioning and Equipment
The patient is positioned supine on the operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, allowing neutral positioning of the foot. This facilitates access to both the medial aspect of the foot for the spring ligament reconstruction and the lateral aspect for the lateral column lengthening and calcaneal osteotomy.
A well-padded thigh tourniquet is applied. Standard orthopedic instrumentation is required, including fluoroscopy, osteotomes, oscillating saws, and appropriate fixation constructs (plates, screws, staples) for the osteotomies. For the spring ligament itself, the surgeon should have a variety of suture anchors available, typically ranging from 2.5 mm to 3.5 mm, loaded with high-strength non-absorbable suture or suture tape. If an allograft reconstruction is planned due to severe tissue deficiency, a prepared semitendinosus or peroneus longus allograft and appropriate interference screws should be available.
Detailed Surgical Approach and Technique
Incision and Superficial Dissection
A medial utility incision is utilized. The incision begins approximately 2 cm proximal to the tip of the medial malleolus, courses distally along the path of the posterior tibial tendon, and extends to the level of the medial cuneiform. Care must be taken to protect the saphenous vein and nerve, which are typically retracted anteriorly and dorsally.

Exposure of the medial structures. The posterior tibial tendon sheath is incised to reveal the underlying pathology.
The flexor retinaculum is incised, and the posterior tibial tendon sheath is opened. The posterior tibial tendon is inspected. In cases of advanced disease, it is often attenuated, longitudinally split, or completely ruptured. The tendon is debrided or excised as necessary, and the flexor digitorum longus tendon is identified and harvested for subsequent transfer.
Deep Dissection and Spring Ligament Exposure
With the posterior tibial tendon retracted or excised, the underlying spring ligament complex is exposed. The capsule of the talonavicular joint is identified. The superomedial band of the spring ligament is carefully inspected.

Direct visualization of the attenuated spring ligament complex after retraction of the posterior tibial tendon.
The surgeon must assess the quality of the ligamentous tissue. A distinct longitudinal tear may be present, or the tissue may be diffusely thinned and redundant. A probe is used to assess the integrity of the attachment sites on the sustentaculum tali and the navicular.

Probing the spring ligament defect. Large defects or severe attenuation dictate the choice between direct repair and graft reconstruction.
Direct Repair and Imbrication Technique
If the ligament is attenuated but possesses sufficient tissue quality, a direct repair with imbrication is performed. The redundant tissue is often managed with a "pants-over-vest" imbrication technique to restore tension.

Preparation of the bony footprint on the medial navicular for suture anchor placement.
The medial aspect of the navicular is decorticated using a rongeur or a high-speed burr to create a bleeding bony bed that will promote soft tissue healing. Depending on the exact location of the failure, the sustentaculum tali may also require decortication.

Placement of a solid suture anchor into the medial navicular to secure the spring ligament repair.
Suture anchors (typically 2.5 mm to 3.5 mm) are placed into the prepared navicular footprint. The sutures are passed through the proximal stump of the superomedial spring ligament.

Sutures are passed through the ligamentous tissue utilizing a locking configuration to prevent pull-through.
It is critical that the repair is tied with the foot held in the corrected position—specifically, with the talonavicular joint reduced, the forefoot adducted, and the heel in neutral or slight varus. This ensures the ligament heals at the appropriate length to maintain the arch.
Allograft Reconstruction Technique
In cases where the spring ligament is completely deficient, severely degenerated, or retracted, a direct repair will inevitably fail. In these instances, an allograft reconstruction is indicated to bridge the gap and provide robust stabilization.

Preparation of the allograft tissue. The graft is sized and tensioned on the back table prior to insertion.
A semitendinosus or split peroneus longus allograft is commonly utilized. Tunnels are drilled in the sustentaculum tali and the medial navicular. The graft is passed through these tunnels to recreate the superomedial and inferior bands of the spring ligament complex.

The allograft is passed through the osseous tunnels and secured with interference screws or suspensory fixation.
The graft is tensioned with the foot in maximum correction and fixed using biocomposite interference screws. Care must be taken not to over-constrain the talonavicular joint, which can lead to a rigid supination deformity and lateral column overload.

Final appearance of the reconstructed spring ligament complex, demonstrating restored tension and talonavicular reduction.
Execution of Adjunctive Osteotomies
Following the medial soft tissue reconstruction, the necessary bony procedures are performed.
1. Medializing Calcaneal Osteotomy: An oblique incision is made over the lateral calcaneus. An osteotomy is performed posterior to the posterior facet. The posterior tuberosity is translated medially by 8 to 10 mm and secured with one or two large fragment cannulated screws. This shifts the mechanical axis medially, reducing the valgus thrust on the reconstructed spring ligament.
2. Lateral Column Lengthening: If severe forefoot abduction is present, an Evans osteotomy is performed 1.5 cm proximal to the calcaneocuboid joint. A tricortical bone graft or metallic wedge is inserted to lengthen the lateral column, which indirectly reduces the talonavicular joint and offloads the medial soft tissues.
3. Cotton Osteotomy: If a residual supinatus (forefoot varus) exists after the hindfoot is corrected, a dorsal opening wedge osteotomy of the medial cuneiform is performed to plantarflex the first ray and restore the tripod mechanics of the foot.
Complications and Management
Surgical management of spring ligament insufficiency is technically demanding and carries a risk of specific complications. Meticulous surgical technique and appropriate patient selection are critical to minimizing these risks.
| Complication | Incidence | Etiology and Pathophysiology | Prevention and Salvage Strategies |
|---|---|---|---|
| Recurrent Deformity | 5-15% | Failure to adequately address bony malalignment, under-tensioning of the repair, or poor tissue quality. | Ensure adequate calcaneal medialization and lateral column lengthening. Salvage requires revision with allograft augmentation or definitive arthrodesis. |
| Over-tightening and Supination Deformity | 2-8% | Excessive tensioning of the spring ligament reconstruction or over-correction of the lateral column lengthening. | Tension the repair with the foot in neutral, not excessive varus. Salvage may require surgical release or lateral column shortening. |
| Nerve Injury | 3-10% | Iatrogenic injury to the saphenous nerve medially or the sural nerve laterally during osteotomies. | Careful superficial dissection and meticulous retraction. Management involves desensitization, gabapentinoids, or surgical neurectomy for painful neuromas. |
| Nonunion of Osteotomies | 2-5% | Poor bone stock, thermal necrosis during sawing, smoking, or premature weight-bearing. | Use sharp saw blades, copious irrigation, and rigid internal fixation. Salvage requires revision internal fixation with bone grafting. |
| Hardware Prominence | 10-20% | Prominent screw heads at the calcaneal osteotomy site or medial navicular anchors. | Countersink screws where possible. Management is symptomatic hardware removal after definitive osseous union is achieved. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is designed to protect the delicate soft tissue reconstruction while allowing for osseous union of the adjunctive osteotomies.
Phase 1 Strict Immobilization
For the first 2 weeks postoperatively, the patient is placed in a bulky, non-weight-bearing short leg splint. The foot is immobilized in neutral dorsiflexion and slight inversion to eliminate tension on the medial repair. Strict elevation is mandated to minimize edema and promote wound healing.
Phase 2 Transition to Cast or Boot
At the 2-week mark, sutures are removed. If the wounds are well-healed, the patient is transitioned to a short leg fiberglass cast or a rigid controlled ankle motion (CAM) boot. The patient remains strictly non-weight-bearing for an additional 4 weeks. Radiographs are obtained at the 6-week mark to assess the healing of the calcaneal, Evans, and Cotton osteotomies.
Phase 3 Progressive Weight Bearing
Assuming radiographic evidence of early bone healing at 6 weeks, the patient may begin progressive weight-bearing in the CAM boot. This typically starts with 25% body weight and advances over the subsequent 4 to 6 weeks. Formal physical therapy is initiated, focusing on active and active-assisted range of motion of the ankle and subtalar joints. Passive stretching into eversion is strictly prohibited, as this places undue stress on the healing spring ligament reconstruction.
Phase 4 Return to Function
At 10 to 12 weeks postoperatively, the patient is transitioned from the CAM boot to a supportive athletic shoe equipped with a custom-molded orthotic or an articulated ankle-foot orthosis, depending on the severity of the initial deformity and patient compliance. Physical therapy shifts focus to proprioception, closed kinetic chain strengthening, and gait retraining. Maximal medical improvement is typically not reached until 9 to 12 months postoperatively.
Summary of Key Literature and Guidelines
The understanding of spring ligament pathology has evolved significantly, largely driven by advanced imaging and biomechanical studies. Deland et al. provided foundational anatomical studies demonstrating the distinct bands of the spring ligament and their respective roles in maintaining the acetabulum pedis. Their work highlighted that the superomedial band is the primary restraint to talar head subluxation.
More recently, consensus guidelines from major orthopedic foot and ankle societies have transitioned the nomenclature from Adult Acquired Flatfoot Deformity (AAFD) to Progressive Collapsing Foot Deformity (PCFD). This change reflects the multi-ligamentous nature of the disease, acknowledging that the spring ligament, deltoid ligament, and interosseous talocalcaneal ligaments all contribute to the collapse.
Clinical outcome studies by Myerson and Toolan have demonstrated that isolated soft tissue repairs (e.g., posterior tibial tendon transfer and direct spring ligament repair) yield unacceptably high failure rates in the presence of fixed bony malalignment. Current academic guidelines mandate that spring ligament reconstruction must be protected by appropriate load-shifting osteotomies. Furthermore, biomechanical studies have validated the use of allograft tissues for spring ligament reconstruction in cases of severe attenuation, showing that graft constructs can restore near-native kinematics to the talonavicular joint when combined with a medializing calcaneal osteotomy.
You Might Also Like