Fix Long Metatarsals: Metatarsal Shortening Osteotomy Relief

Key Takeaway
Here are the crucial details you must know about Fix Long Metatarsals: Metatarsal Shortening Osteotomy Relief. A metatarsal shortening osteotomy, exemplified by the Weil osteotomy, is a surgical treatment for metatarsophalangeal (MTP) joint subluxation or dislocation. This procedure is often indicated when excessive metatarsal length contributes to abnormal forefoot pressure distribution or plantar plate pathology. Its goal is to restore normal joint alignment and function, mitigating issues like chronic dislocation.
Introduction and Epidemiology
Subluxation or dislocation of the metatarsophalangeal joints results in a disruption of the fibers of the plantar plate, which is the central structure implicated in metatarsophalangeal joint dislocation. The plantar plate provides a critical cushion to the joint and absorbs substantial weight-bearing forces during the terminal stance phase of the gait cycle. The key point in deciding how to treat this pathology is to determine whether the underlying structural abnormality leads to abnormal pressure distribution across the forefoot.

Pathology of the lesser metatarsophalangeal joints, often presenting as metatarsalgia with associated toe deformities, is a prevalent complaint in orthopedic foot and ankle clinics. The condition predominantly affects females, often presenting in the fifth to seventh decades of life. The etiology is multifactorial, involving a combination of intrinsic biomechanical faults and extrinsic factors such as constrictive footwear. When conservative measures fail to alleviate the abnormal pressure distribution and resultant pain, surgical intervention becomes necessary. The evolution of surgical management has shifted significantly toward joint-preserving, intraarticular shortening osteotomies, primarily to restore the anatomic cascade of the metatarsal parabola and decompress the soft tissues of the metatarsophalangeal joint.

Surgical Anatomy and Biomechanics
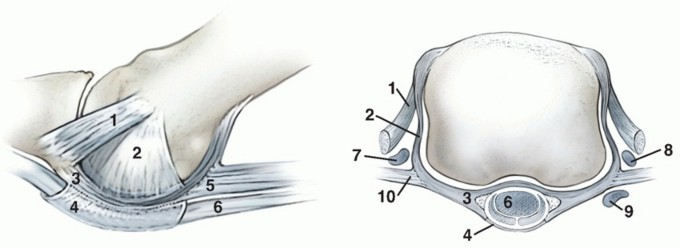
The proximal phalanx and the fibrocartilaginous plantar plate form a highly specialized anatomic and functional unit at the metatarsophalangeal joint. The plantar plate is a thick, rectangular, fibrocartilaginous structure that is the major factor of dorsoplantar stability. It attaches firmly to the base of the proximal phalanx distally and becomes continuous with the plantar fascia proximally. However, except for the attachments of the two collateral ligaments, the plantar plate is without substantial fibrous attachment to the metatarsal head itself. This anatomical arrangement allows the metatarsal head to glide smoothly over the plate during dorsiflexion of the toes.

The dynamic stability of the lesser metatarsophalangeal joints relies on a delicate balance of tendinous forces. The extensor digitorum longus tendon extends to the proximal phalanx and continues to the proximal interphalangeal joint. The primary antagonists of this extensor mechanism are the flexor tendons (flexor digitorum longus and brevis) and the static restraint of the plantar plate. Furthermore, the function of the interossei and lumbrical muscles is to hold the proximal phalanx in a neutral position, acting plantar to the axis of rotation of the metatarsal head to provide intrinsic plantarflexion force.

When an osteotomy is performed, altering the length or elevation of the metatarsal head directly impacts this intrinsic musculature. If the metatarsal head is inadvertently elevated or shortened excessively without addressing the soft tissue tension, the axis of rotation shifts dorsal to the intrinsic tendons, converting them from flexors to extensors, which contributes to postoperative deformities.

Pathogenesis of Joint Instability
High functional stresses of weight bearing and repetitive hyperextension of the metatarsophalangeal joint can lead to attenuation or frank rupture of the plantar plate, followed by progressive subluxation or dislocation of the toe. The plantar plate significantly contributes to stabilizing the sagittal plane of the lesser metatarsophalangeal joints.

A hallux valgus deformity is often associated with a subluxated second metatarsophalangeal joint. The laterally deviating hallux physically pushes the second toe laterally, which alters the vector of the intrinsic and extrinsic tendons, leading to instability and eventual subluxation. Furthermore, joint instability may result from an excessive length of the second or third metatarsal relative to the first metatarsal. A long lesser metatarsal alters the normal weight-bearing cascade, subjecting the specific metatarsophalangeal joint to disproportionate sheer and axial loads. The second metatarsophalangeal joint is then biomechanically more subject to the pressure of tight stockings or shoes.

Once the plantar plate is elongated and ruptured, the dorsal capsule and the extensor tendon become contracted due to unopposed tension, leading to a chronically dislocated metatarsophalangeal joint. The proximal phalanx eventually rests on the dorsal aspect of the metatarsal neck, driving the metatarsal head plantarly into the weight-bearing surface of the foot, resulting in intractable plantar keratosis.

Indications and Contraindications
The primary indication for a metatarsal shortening osteotomy is recalcitrant metatarsalgia associated with a disproportionately long metatarsal, with or without metatarsophalangeal joint subluxation or dislocation. Patients typically present with a history of painful forefeet over a long period of months or years. The pain usually occurs dorsally over the toe and on the plantar side of the metatarsal head.

Surgical intervention is considered only after exhaustive non-operative management, including custom orthotics with metatarsal offloading pads, shoe modifications, and non-steroidal anti-inflammatory drugs, have failed to provide relief.
| Parameter | Operative Indications | Non Operative Indications |
|---|---|---|
| Pain Duration | Chronic, refractory to >6 months conservative care | Acute or subacute, responsive to offloading |
| Deformity | Fixed subluxation or dorsal dislocation of MTP joint | Flexible deformity, reducible with taping |
| Metatarsal Length | Positive Maestro criteria (abnormally long lesser ray) | Normal metatarsal cascade |
| Plantar Pathology | Intractable plantar keratosis beneath metatarsal head | Diffuse callus without focal bony prominence |
| Associated Deformity | Concomitant severe hallux valgus requiring correction | Isolated mild metatarsalgia without structural fault |

Contraindications to the procedure include active local or systemic infection, severe peripheral vascular disease compromising the healing potential of the distal extremity, and profound peripheral neuropathy (such as advanced Charcot neuroarthropathy) where the patient cannot protect the osteotomy postoperatively. Relative contraindications include spastic neurologic disorders that may overpower the bony fixation and soft tissue repairs.

Pre Operative Planning and Patient Positioning
Each patient must be analyzed individually, with attention to a detailed history and a careful clinical examination. Ruling out differential diagnosis, such as Morton's neuroma, Freiberg's infraction, or inflammatory arthropathies, is mandatory.
Clinical Examination
Determining circulatory status is necessary to assess not only the feasibility of an individual procedure but also whether multiple procedures can be performed simultaneously if necessary. Palpation of dorsalis pedis and posterior tibial pulses, along with capillary refill assessment, is mandatory. Clinical examination of cutaneous sensory response using Semmes-Weinstein monofilaments may indicate a systemic disease such as diabetes.

The drawer test is utilized to evaluate the stability of all the metatarsophalangeal joints and the reducibility of lesser toe deformities in plantarflexion. The examiner stabilizes the metatarsal neck with one hand and grasps the base of the proximal phalanx with the other, applying a dorsal-to-plantar translational force. Increased translation compared to the contralateral foot, or a palpable "clunk," indicates plantar plate insufficiency. The surgeon must also assess: How stable overall is the first ray? First ray hypermobility often transfers weight to the lesser rays.

Passive range of motion must be documented. Normal range of motion is 60 to 80 degrees of full extension to 40 degrees of full flexion. Loss of flexion may be a result of the contracted extensor tendons or because the proximal phalanx already lies dorsal to the second metatarsal head. Inspection of the plantar aspect of the foot will reveal plantar keratosis. This callus is a circumscribed keratotic area under the metatarsal head that usually corresponds to the exact location of the depressed metatarsal head.

Radiographic Evaluation
Standard weight-bearing anteroposterior, lateral, and oblique radiographs of the foot are required. The AP view is utilized to assess the metatarsal cascade (Maestro criteria) to determine the exact amount of shortening required. The lateral view helps identify dorsal subluxation or dislocation of the proximal phalanx. Advanced imaging, such as MRI or ultrasound, can be utilized to definitively diagnose a plantar plate tear, though the diagnosis is heavily reliant on clinical examination.

Patient positioning is supine on the operating table. A bump may be placed under the ipsilateral hip to correct natural external rotation of the lower extremity, ensuring the foot rests in a neutral position facing the ceiling. A calf or thigh tourniquet is applied to provide a bloodless surgical field.

Detailed Surgical Approach and Technique
The Weil osteotomy is the gold standard for metatarsal shortening. It is an intraarticular, extra-capsular (in terms of the primary cut initiation) osteotomy that allows for controlled shortening of the metatarsal without altering its plantar elevation, provided the cut is made parallel to the weight-bearing surface.
Incision and Soft Tissue Dissection
A dorsal longitudinal incision is made centered over the affected metatarsophalangeal joint. If adjacent rays are being addressed (e.g., second and third metatarsals), a single incision in the intermetatarsal space can be utilized to access both joints, minimizing soft tissue stripping and preserving the dorsal skin bridges. Dissection is carried down through the subcutaneous tissue, taking care to identify and retract the dorsal cutaneous nerve branches.

The extensor apparatus is identified. A longitudinal incision is made either through the extensor digitorum longus tendon (tendon-splitting approach) or immediately adjacent to it, retracting the tendon laterally or medially. A Z-lengthening of the extensor digitorum longus may be performed at this stage if severe contracture is present, which is common in chronic dislocations.

Joint Exposure and Capsulotomy
A dorsal capsulotomy is performed to expose the metatarsal head and the base of the proximal phalanx. The collateral ligaments are released from their metatarsal origins to allow for adequate plantarflexion of the proximal phalanx, which provides comprehensive exposure of the entire metatarsal head. A McGlamry elevator may be passed plantarly to release any adhesions between the metatarsal head and the underlying plantar plate and sesamoid apparatus.

Osteotomy Execution
The orientation of the saw blade is the most critical step of the procedure. The osteotomy is initiated at the dorsal cartilage reflection of the metatarsal head. The oscillating saw blade must be directed proximally and plantarly. The angle of the cut should be approximately 10 to 15 degrees relative to the longitudinal axis of the metatarsal shaft, but more importantly, it must be exactly parallel to the plantar aspect of the foot (the weight-bearing surface).

If the cut is made too steep (greater than 15 degrees), proximal translation of the capital fragment will result in significant plantar depression of the metatarsal head, which can lead to transfer metatarsalgia. Conversely, if the cut is made too shallow, the saw blade will exit too far proximally in the diaphyseal bone, compromising the structural integrity of the metatarsal shaft and increasing the risk of fracture or nonunion.

Metatarsal Head Translation and Fixation
Once the osteotomy is complete, the metatarsal head (the plantar fragment) is translated proximally along the osteotomy plane to achieve the preoperatively templated shortening. Typically, 2 to 5 millimeters of shortening is sufficient to decompress the joint and restore the metatarsal cascade. The fragment can also be translated slightly medially or laterally to correct mild transverse plane deformities.

The osteotomy is provisionally fixed with a smooth Kirschner wire directed dorsal-distal to plantar-proximal. Fluoroscopy is utilized to confirm the alignment, the amount of shortening, and the restoration of the metatarsal parabola.

Permanent fixation is achieved using a single, specialized osteotomy screw (typically 2.0 mm or 2.5 mm in diameter). The screw is inserted over the guidewire (if cannulated) or via a standard drill and tap technique. The screw must be countersunk into the dorsal cortical bone to prevent hardware prominence and subsequent irritation of the extensor tendons. After the screw is securely placed, the overhanging dorsal bone of the proximal fragment is resected flush with the metatarsal head using a rongeur or oscillating saw.

Concomitant procedures, such as direct plantar plate repair via transosseous tunnels in the proximal phalanx, or a proximal interphalangeal joint arthrodesis for a rigid hammer toe deformity, are performed at this stage. The capsule is closed, and the skin is reapproximated.
Complications and Management
While the Weil osteotomy provides superior outcomes compared to historical alternatives, it is not without complications. The most frequently cited complication is the "floating toe" deformity.

A floating toe occurs when the toe fails to purchase the ground during weight-bearing. Biomechanically, this is caused by the proximal translation of the metatarsal head, which slackens the plantar intrinsic musculature (interossei and lumbricals). If the axis of rotation of the metatarsal head shifts dorsal to these tendons, they lose their plantarflexion moment and act as extensors. Furthermore, the resection of the dorsal overhanging bone effectively shortens the dorsal lever arm, contributing to the imbalance.
| Complication | Estimated Incidence | Pathophysiology and Salvage Strategy |
|---|---|---|
| Floating Toe | 15% - 30% | Pathophysiology: Intrinsic muscle slackening, shift of rotation axis. Salvage: Flexor-to-extensor tendon transfer (Girdlestone-Taylor), aggressive postoperative plantarflexion taping. |
| Transfer Metatarsalgia | 5% - 10% | Pathophysiology: Inadequate shortening of the index metatarsal or over-shortening causing load shift to adjacent rays. Salvage: Custom orthotics, secondary shortening osteotomy of the newly overloaded ray. |
| Nonunion / Delayed Union | < 2% | Pathophysiology: Thermal necrosis from saw blade, inadequate fixation, poor vascularity. Salvage: Revision with bone grafting and robust plate/screw fixation. |
| Hardware Prominence | 5% - 8% | Pathophysiology: Failure to adequately countersink the dorsal screw head. Salvage: Simple hardware removal after radiographic union is achieved (typically >3 months). |
| Avascular Necrosis | < 1% | Pathophysiology: Excessive soft tissue stripping of the metatarsal head capsule. Salvage: Offloading; if joint collapses, excisional arthroplasty or joint replacement. |

To mitigate the risk of floating toe, surgeons must ensure the osteotomy cut is exactly parallel to the plantar foot, avoid excessive shortening (>5mm), and consider performing a concomitant flexor-to-extensor tendon transfer or plantar plate repair to restore the plantarflexion moment.
Post Operative Rehabilitation Protocols
Postoperative care is critical to maintaining the surgical correction and preventing stiffness. The foot is placed in a bulky compressive dressing immediately postoperatively. The toe is aggressively taped in a plantarflexed position to stretch the dorsal capsule and counteract the tendency for a floating toe.

Patients are typically permitted heel weight-bearing or flat-foot weight-bearing in a rigid, postoperative shoe or fracture boot immediately after surgery.
Phase 1 (0 to 2 weeks): Focus on edema control, wound healing, and strict adherence to the rigid shoe. The dressings are removed at 10 to 14 days for suture removal.
Phase 2 (2 to 6 weeks): The toe is continuously taped in plantarflexion. Active and passive range of motion exercises of the metatarsophalangeal joint are initiated to prevent arthrofibrosis. Patients are instructed to manually plantarflex the toe multiple times a day. Weight-bearing continues in the rigid shoe.
Phase 3 (6 weeks and beyond): Radiographs are obtained to confirm bony union of the osteotomy. Once union is evident, patients are transitioned to supportive athletic shoes with a wide toe box. High-impact activities and pivoting sports are generally restricted until 10 to 12 weeks postoperatively, depending on the patient's functional recovery and resolution of edema.
Summary of Key Literature and Guidelines
The surgical management of lesser metatarsophalangeal joint pathology was revolutionized when Weil presented in 1992 in Europe a joint-preserving, intraarticular shortening osteotomy, and Barouk first published it in 1996. Prior to this, surgeons relied heavily on extra-articular osteotomies or joint destructive procedures.
Researchers from Europe and the United States have shown in extensive anatomic, clinical, and radiologic studies the advantages of the Weil osteotomy compared to alternative procedures. Historically, a dorsal soft tissue release with pin fixation, silicone implants, metatarsal neck osteotomies without fixation (such as the Helal osteotomy), and metatarsophalangeal joint excisional arthroplasties have been reported in the literature as surgical alternatives.
However, a high rate of complications such as nonunions, malalignments, and transfer lesions are associated with these alternative surgical procedures. The Helal osteotomy, for example, relies on uncontrolled dorsal displacement of the metatarsal head, frequently resulting in unpredictable healing and severe transfer metatarsalgia. Excisional arthroplasty destroys the joint mechanics entirely, leading to a dysfunctional, flail toe.
The Weil osteotomy provides a geometrically stable cut that allows for precise, mathematically calculable shortening while providing a broad surface area for rigid internal fixation. Current academic consensus and orthopedic guidelines strongly support the use of the Weil osteotomy, often combined with direct plantar plate repair, as the procedure of choice for addressing metatarsophalangeal joint instability, subluxation, and associated metatarsalgia driven by long lesser metatarsals.
Clinical & Radiographic Imaging
You Might Also Like