Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Introduction and Epidemiology
Coronal shear fractures of the distal humerus, specifically those isolating the capitellum and the capitellar-trochlear region, represent a rare, morphologically complex subset of intra-articular injuries. Comprising approximately 1% of all elbow fractures and up to 6% of distal humerus fractures, these injuries present profound diagnostic and therapeutic challenges to the orthopedic surgeon. The intrinsic complexity of these fractures arises from their entirely intra-articular nature, the paucity of attached soft tissues, the limited subchondral bone available for stable internal fixation, and the highly tenuous vascular supply to the anterior articular fragments.
Historically, the management of these fractures was fraught with high complication rates. Fragment excision was frequently employed for displaced fractures, a practice that predictably resulted in devastating lateral column instability, progressive valgus deformity, post-traumatic osteoarthritis, and profound functional impairment. The modern orthopedic paradigm has unequivocally shifted toward anatomic reduction and stable internal fixation (ORIF). Contemporary principles mandate the exact restoration of articular congruity, re-establishment of lateral column stability, and the facilitation of immediate, early postoperative mobilization. This paradigm shift has been heavily supported by advanced cross-sectional imaging modalities and the evolution of specialized internal fixation techniques, most notably the advent of variable-pitch headless compression screws (HCS) and anatomically pre-contoured periarticular plates.
Pathogenesis and Mechanism of Injury
Capitellum and capitellar-trochlear shear fractures exhibit a bimodal epidemiologic distribution. They typically result from a low-energy fall on an outstretched hand (FOOSH) in the osteoporotic elderly population, whereas high-energy trauma (e.g., motor vehicle collisions, falls from height) is the primary etiology in younger cohorts. The pathomechanical sequence involves the transmission of an axial load through the radius to the lateral column of the distal humerus while the elbow is in a partially flexed posture (typically 30 to 45 degrees).
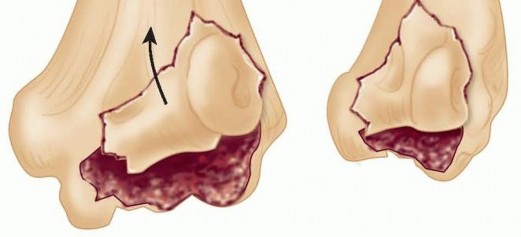
In this semi-flexed position, the radial head acts as a mechanical battering ram. The axial force is translated into a coronal plane shear vector upon impact with the capitellum. This high-velocity shear force propagates through the articular cartilage and subchondral bone of the distal humerus. The resulting fracture fragments, which vary considerably in morphologic complexity and volume, typically displace superiorly and anteriorly into the radial fossa. This characteristic displacement predictably results in a rigid mechanical block to elbow flexion.
Furthermore, the surgeon must maintain a high index of suspicion for associated injuries, which are frequently present and can severely complicate management if missed. These include fractures of the radial head, proximal ulna, and carpal bones, as well as critical ligamentous disruptions. Lateral ulnar collateral ligament (LUCL) avulsions are particularly common, while medial collateral ligament (MCL) tears or triceps ruptures occur less frequently but require active exclusion.
Classification Systems
Accurate classification is paramount for preoperative planning, anticipating the required surgical approach, and determining the optimal biomechanical fixation strategy. The Bryan and Morrey classification, subsequently modified by McKee, historically categorized these fractures based on the anatomic extent and osseous volume of the articular fragment.
- Type I (Hahn-Steinthal): Involves a large, hemispherical osseous fragment of the capitellum with a substantial subchondral bone base.
- Type II (Kocher-Lorenz): Involves an articular cartilage sleeve with minimal to no attached subchondral bone, making internal fixation exceptionally difficult.
- Type III (Broberg-Morrey): Represents a highly comminuted capitellar fracture.
- Type IV (McKee Modification): Describes a coronal shear fracture that extends medially across the trochlear groove to include the lateral ridge of the trochlea, representing a more extensive destabilization of the articular spool.
While the Bryan and Morrey system is descriptively useful, the Dubberley classification has gained significant prominence due to its direct implications for surgical fixation and approach. This system categorizes the injury based on the radiographic pattern of the articular fragments and, crucially, the presence or absence of posterior lateral column comminution.
- Type 1: Fracture of the capitellum (with or without trochlear ridge involvement).
- Type 2: Capitellum and trochlea fractured as a single, contiguous fragment.
- Type 3: Capitellum and trochlea fractured as separate, unlinked fragments (highly unstable).
Crucially, the Dubberley system utilizes modifiers to dictate the biomechanical requirements for fixation:
* Modifier A: Absence of posterior condylar comminution.
* Modifier B: Presence of posterior condylar comminution.
Fractures designated as Type B lack a stable posterior osseous buttress. Fixation utilizing only anterior-to-posterior (AP) headless compression screws in Type B fractures will inevitably fail due to cyclic shear loading during early range of motion. These injuries absolutely mandate supplemental posterior lateral column plating to neutralize shear forces and prevent superior migration of the articular construct.
Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of distal humeral osteology, ligamentous isometry, and regional vascularity is essential for executing a safe surgical exposure, achieving anatomic reduction, and constructing durable internal fixation.
Osteology of the Distal Humerus
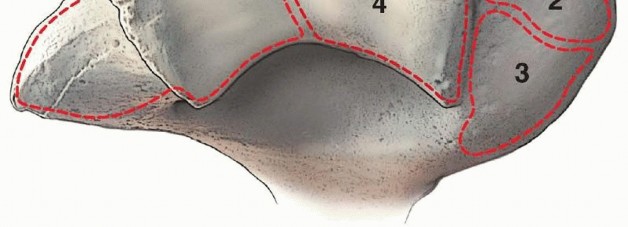
The distal humerus is structurally conceptualized as a triangular frame composed of a medial and lateral column supporting the central articular spool (the trochlea) and the lateral articular hemisphere (the capitellum). The capitellum is oriented distally and anteriorly, projecting at an angle of approximately 30 degrees relative to the longitudinal axis of the humeral shaft.
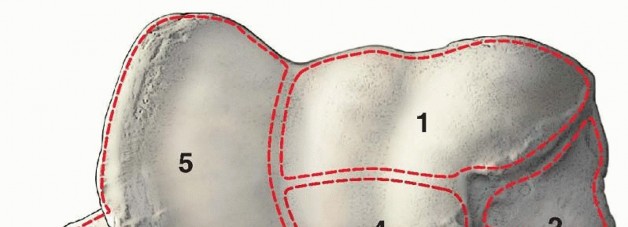
The anterior surface of the capitellum is covered by thick hyaline cartilage designed to articulate with the concave radial head. The radial head rotates on this anterior surface during elbow flexion and translates to articulate with the inferior surface during full elbow extension. Notably, the posterior aspect of the lateral condyle is entirely devoid of articular cartilage. This non-articular posterior cortex serves as the critical structural buttress for the lateral column and provides the anatomic origin for the lateral collateral ligament complex.
Ligamentous Anatomy and Stability
The lateral collateral ligament (LCL) complex, specifically the lateral ulnar collateral ligament (LUCL), is the primary static restraint to posterolateral rotatory instability (PLRI) of the elbow joint. The LUCL originates from the lateral epicondyle at a precise isometric point located posterosuperior to the axis of rotation, and it inserts distally onto the supinator crest of the proximal ulna.

During surgical exposure for coronal shear fractures, preserving the LUCL origin is of paramount importance. If the fracture line extends proximally into the lateral epicondyle, or if the surgical approach necessitates the detachment of the ligamentous origin to achieve adequate articular visualization, the LUCL must be meticulously repaired. This is typically accomplished using suture anchors or transosseous tunnels at the conclusion of the procedure to prevent catastrophic iatrogenic PLRI.
Vascular Supply to the Capitellum
The delicate vascular anatomy of the distal humerus dictates the significant risk of avascular necrosis (AVN) following shear fractures. The arterial supply to the capitellum is predominantly derived from posterior perforating vessels.
These critical end-arteries arise from the lateral arcade, a rich anastomotic network formed by the radial collateral branch of the profunda brachii artery and the recurrent radial artery. Because the anterior articular fragment in a coronal shear fracture is entirely intra-articular and devoid of soft tissue attachments, the injury intrinsically disrupts this posterior blood supply. Consequently, the anterior fragment is rendered essentially avascular at the time of injury. It relies entirely on rigid anatomic reduction and stable fixation to facilitate revascularization through the process of creeping substitution. Extensive soft tissue stripping of the posterior lateral column during surgical exposure further compromises this delicate vascular network and must be strictly minimized.
Indications and Contraindications
The management of capitellar and capitellar-trochlear shear fractures is almost exclusively surgical. Non-operative management is strictly reserved for a highly select, functionally low-demand patient population, or those with absolute medical contraindications to anesthesia. Conservative treatment of displaced fractures inevitably results in a rigid mechanical block to flexion, severe capsular contracture, and rapidly progressive post-traumatic arthrosis.
Operative Decision Making
Open reduction and internal fixation (ORIF) remains the gold standard for all displaced coronal shear fractures. The primary surgical objective is the absolute restoration of the articular surface to allow for immediate, unrestricted postoperative range of motion.
In cases of severe, un-reconstructable comminution (e.g., severe Dubberley Type 3B fractures in profoundly osteoporotic bone), total elbow arthroplasty (TEA) may be considered as a primary intervention. This is generally reserved for elderly, low-demand patients where stable fixation is deemed impossible. Fragment excision, once a common historical practice, is now largely condemned due to the resultant lateral column shortening, altered joint kinematics, and multi-planar instability.
| Clinical Scenario | Recommended Management Strategy | Rationale and Biomechanical Considerations |
|---|---|---|
| Non-displaced Type 1 Fracture | Non-Operative (Immobilization 1-2 weeks, then early ROM) | Extremely rare clinical entity. Requires rigorous radiographic follow-up to ensure no secondary displacement occurs. |
| Displaced Type 1-4 Fractures | Open Reduction and Internal Fixation (ORIF) | Restores articular congruity, removes the mechanical block in the radial fossa, and allows immediate early mobilization. |
| Dubberley Type B (Posterior Comminution) | ORIF with supplemental posterior lateral column plating | Headless compression screws alone will fail due to the lack of a posterior cortical buttress. The plate neutralizes cyclic shear forces. |
| Severe Comminution in Elderly/Low Demand | Total Elbow Arthroplasty (TEA) | Provides immediate stability and functional motion when rigid fixation of osteoporotic, highly fragmented bone is impossible. |
| Isolated Kocher-Lorenz (Cartilage only) | Excision vs. Bioabsorbable pin fixation | The fragment often lacks sufficient subchondral bone for screw purchase. Small fragments may be excised if the lateral column remains perfectly stable. |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is required to anticipate the necessary surgical approach, the potential requirement for structural bone grafting, and the specific implant inventory needed to address complex fracture morphologies.
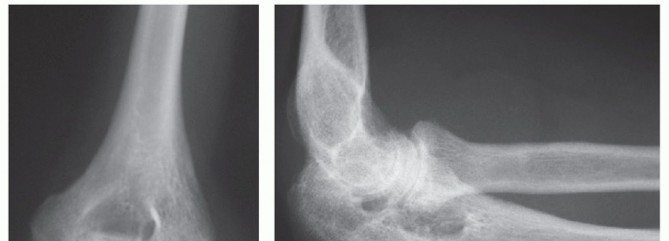
Imaging Modalities
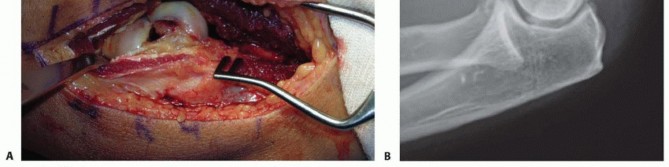
Standard anteroposterior (AP) and lateral radiographs of the elbow are the initial diagnostic steps. The lateral radiograph is particularly crucial, often revealing the characteristic "double arc sign." This pathognomonic sign represents the subchondral bone of the capitellum and the lateral trochlear ridge displaced superiorly and anteriorly, indicating a complex shear fracture extending into the trochlea (McKee Type IV / Dubberley Type 2 or 3).

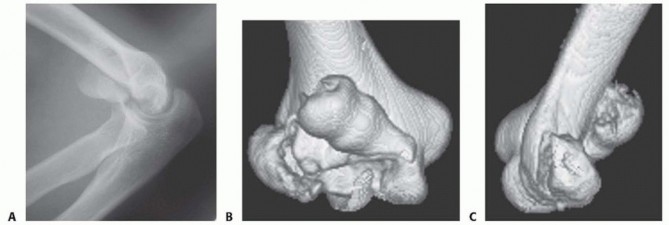
However, plain radiography consistently underestimates the complexity of articular comminution and the true extent of posterior lateral column involvement. Therefore, a computed tomography (CT) scan with two-dimensional multiplanar reformats and three-dimensional (3D) reconstructions is mandatory for all suspected coronal shear fractures. The CT scan precisely delineates the fracture pattern, identifies independent and unlinked articular fragments (Dubberley Type 3), and critically assesses the structural integrity of the posterior condyle (Dubberley Type B), which ultimately dictates the need for posterior buttress plating.
Patient Setup and Tourniquet Placement
The procedure is typically performed under general anesthesia, often supplemented with a regional supraclavicular or axillary nerve block for optimal postoperative pain control and to facilitate early rehabilitation.

Patient positioning depends heavily on surgeon preference and the anticipated surgical approach derived from CT imaging. The supine position, with the arm draped across the chest on a radiolucent hand table, is excellent for isolated lateral or anterolateral approaches. Alternatively, the lateral decubitus position with the arm resting over a padded post allows for simultaneous lateral and posterior access. This is highly advantageous if a posterior approach utilizing an olecranon osteotomy is required for complex, multi-fragmentary trochlear shear fractures. A sterile pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, inflated to standard upper extremity pressures after meticulous exsanguination.
Detailed Surgical Approach and Technique
The surgical execution requires precise, atraumatic handling of the articular fragments, profound respect for the soft tissue envelope, and the application of biomechanically sound fixation constructs.
Choice of Surgical Approach
The choice of surgical approach is dictated entirely by the fracture morphology identified on the preoperative 3D CT scan.
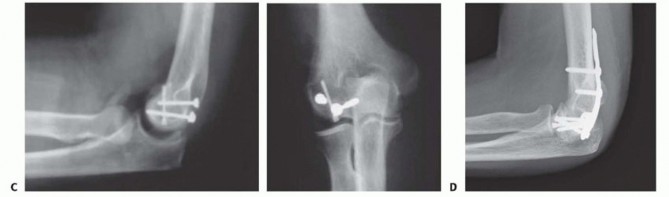
1. Extended Lateral Approach (Kocher Interval): This is the workhorse approach for most Dubberley Type 1 and 2 fractures. The incision is centered over the lateral epicondyle. The deep interval is developed between the extensor carpi ulnaris (ECU) and the anconeus. This provides excellent visualization of the posterior capitellum and the lateral column. To visualize the anterior articular surface, the anterior capsule must be elevated, and the common extensor origin may need to be partially reflected.
2. Kaplan Approach: Utilizing the more anterior interval between the extensor carpi radialis brevis (ECRB) and the extensor digitorum communis (EDC), this approach provides superior direct anterior visualization of the capitellum. However, it carries a higher risk of iatrogenic injury to the posterior interosseous nerve (PIN), which crosses the operative field distally within the supinator muscle.
3. Posterior Approach with Olecranon Osteotomy: Reserved for complex Dubberley Type 3 fractures with extensive medial trochlear extension. An apex-distal chevron osteotomy of the olecranon provides unparalleled visualization of the entire distal humeral articular surface, facilitating the reduction of complex multi-fragmentary patterns.

Dissection and Internervous Planes
Regardless of the approach utilized, meticulous hemostasis and the identification of key anatomic landmarks are essential. When utilizing the lateral approach, the surgeon must identify and protect the LUCL. If the LUCL is intact but obstructs anatomic reduction, it may be carefully elevated with a thin osseous wafer from the lateral epicondyle to facilitate robust later repair. The fracture hematoma is thoroughly evacuated from the radial fossa, and the joint is copiously irrigated to remove all osteochondral debris that could lead to third-body wear or mechanical locking.
Fracture Reduction Techniques
Reduction of coronal shear fractures can be exceptionally technically demanding due to the lack of soft tissue attachments available to manipulate the fragments. The anterior articular fragment is often rotated and firmly impacted into the metaphyseal bone of the distal humerus.

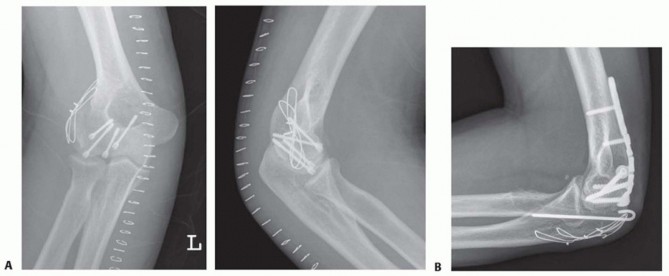
Fine dental picks, Freer elevators, and small pointed reduction forceps are utilized to gently disimpact and provisionally reduce the fragment without damaging the articular cartilage. Smooth Kirschner wires (K-wires) can be inserted into the non-articular portions of the fragment to act as "joysticks" for multi-planar manipulation. Once anatomic reduction is achieved, provisional fixation is secured with multiple parallel K-wires directed from anterior to posterior. The reduction must be confirmed visually by assessing the congruity of the articular surface and fluoroscopically via true lateral imaging to ensure no step-off or gap remains.
Internal Fixation Strategies
The mainstay of definitive fixation for the articular fragments is the use of variable pitch headless compression screws (HCS). These specialized screws provide dynamic interfragmentary compression while allowing the screw head to be buried completely beneath the articular cartilage, thereby preventing catastrophic impingement against the radial head.
Screw Trajectory:
Screws can be placed in an anterior-to-posterior (AP) or posterior-to-anterior (PA) trajectory.
* AP Trajectory: Biomechanical studies indicate that AP directed screws offer superior pull-out strength and interfragmentary compression. However, this trajectory requires violating the intact anterior articular cartilage. When utilizing this technique, the screws must be countersunk at least 1-2 millimeters below the chondral surface to prevent iatrogenic radial head wear.
* PA Trajectory: Placing screws from posterior to anterior avoids damage to the anterior articular cartilage and preserves the pristine gliding surface for the radial head. However, this technique is technically demanding, requires precise fluoroscopic guidance to ensure the threads fully capture the anterior fragment without breaching the joint space, and generally provides slightly less biomechanical compression than AP screws.

For complex Dubberley Type 3 fractures, the trochlear fragment must be anatomically reduced and fixed to the capitellar fragment first, effectively converting it into a Type 2 pattern, before securing the entire reconstructed articular complex to the distal humerus.
Management of Posterior Comminution (Dubberley Type B):
The presence of posterior lateral column comminution fundamentally alters the biomechanics of the fixation construct. HCS fixation relies entirely on the intact posterior cortex acting as a stable buttress. In Type B fractures, this critical buttress is compromised. If only AP or PA screws are utilized, the articular fragment will displace superiorly under the shear forces generated during early postoperative mobilization. Therefore, Type B fractures absolutely mandate the application of a posterior anti-glide or buttress plate. A 2.0 mm or 2.4 mm mini-fragment locking or non-locking plate is anatomically contoured to the posterior aspect of the lateral column to neutralize shear forces and provide rigid stability.
Complications and Management
Despite meticulous surgical technique and modern implants, complications following ORIF of capitellar shear fractures are not uncommon, given the severity of the initial trauma, the intra-articular nature of the injury, and the delicate vascular anatomy.
Intraoperative and Postoperative Complications
Avascular necrosis (AVN) of the capitellum is a feared complication, though modern headless screw fixation and preservation of the posterior soft tissue envelope have reduced its incidence compared to historical techniques. If AVN leads to structural collapse and severe arthrosis, salvage options include radial head excision, radiocapitellar interposition arthroplasty, or total elbow arthroplasty in older patients.
Post-traumatic stiffness is the most frequently encountered complication. The elbow capsule is highly prone to aggressive fibroblastic proliferation and contracture following trauma and surgical intervention. Heterotopic ossification (HO) may also contribute to restricted motion. Hardware prominence or intra-articular screw penetration can cause mechanical impingement, rapid cartilage wear, and pain, necessitating hardware removal once definitive fracture union is confirmed radiographically.
| Complication | Estimated Incidence | Etiology / Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Post-Traumatic Stiffness | 20% - 40% | Capsular contracture, prolonged immobilization, heterotopic ossification (HO). | Aggressive physical therapy, dynamic splinting. Open or arthroscopic capsular release if refractory after 6 months. |
| Avascular Necrosis (AVN) | 5% - 15% | Disruption of posterior blood supply (lateral arcade), extensive soft tissue stripping. | Observation if asymptomatic. If symptomatic structural collapse occurs: TEA (elderly) or radiocapitellar arthroplasty/interposition. |
| Hardware Prominence / Impingement | 10% - 20% | Inadequate countersinking of anterior HCS, backing out of implants over time. | Arthroscopic or open hardware removal after absolute radiographic evidence of complete fracture union. |
| Nonunion / Fixation Failure | < 5% | Failure to recognize and plate posterior comminution (Dubberley Type B), technical error. | Revision ORIF with structural bone grafting and robust posterior plating. TEA in low-demand, elderly patients. |
| Posterolateral Rotatory Instability | 2% - 5% | Unrecognized LUCL avulsion, failure to adequately repair the LUCL during the lateral approach. | LUCL reconstruction utilizing autograft (e.g., palmaris longus) or allograft. |
Post Operative Rehabilitation Protocols
The ultimate functional outcome relies as much on a meticulously executed postoperative rehabilitation protocol as it does on the surgical intervention itself. The primary objective is to prevent debilitating elbow stiffness while simultaneously protecting the healing fracture construct and any repaired ligamentous structures.
Early Mobilization Strategies
If rigid anatomic fixation is achieved and the collateral ligaments are stable (or securely repaired), early active range of motion (ROM) should be initiated within 3 to 5 days postoperatively.
Phase I (0-2 Weeks): The elbow is initially placed in a well-padded posterior splint at 90 degrees of flexion to allow for soft tissue rest, hematoma organization, and reduction of edema. Edema control is paramount. At the first postoperative visit, the splint is removed, and gravity-assisted active and active-assisted ROM exercises are commenced. If the LUCL was repaired, the arm is placed in a hinged elbow brace with an extension block (typically set at 30 degrees) to protect the repair. Forearm pronation is maintained during extension exercises to unload the lateral ligamentous complex and prevent varus stress.
Phase II (2-6 Weeks): The primary goal during this phase is to achieve full functional ROM (typically defined as 30 to 130 degrees of flexion). Passive stretching by a therapist is strictly avoided during this phase, as it can exacerbate capsular inflammation, cause microtrauma, and strongly stimulate heterotopic ossification. Strengthening exercises are delayed until definitive radiographic evidence of early fracture consolidation is observed.
Long Term Functional Outcomes
Phase III (6-12 Weeks and Beyond): Once clinical and radiographic union is confirmed (typically around 6-8 weeks postoperatively), progressive resistance exercises and functional strengthening are initiated. The hinged brace, if utilized,
You Might Also Like