Is Surgical Correction of Juvenile Bunion Right for Your Child?
Key Takeaway
This topic focuses on Is Surgical Correction of Juvenile Bunion Right for Your Child?, Correction of juvenile bunion targets a complex adolescent foot deformity. It involves addressing metatarsus primus varus (medial first metatarsal deviation), hallux valgus (lateral great toe deviation), and an enlarged medial eminence. The intervention aims to restore proper alignment and function, considering the multifactorial nature of the condition.
Introduction and Epidemiology
Juvenile hallux valgus (JHV) represents a complex, multifactorial forefoot deformity characterized by a lateral deviation of the hallux at the first metatarsophalangeal (MTP) joint, medial deviation of the first metatarsal (metatarsus primus varus), and often an enlarged medial eminence of the first metatarsal head. Unlike its adult counterpart, JHV presents in skeletally immature or adolescent patients, typically before physeal closure, and often lacks the degenerative osteoarthritic changes common in adults. The etiology is considered multifactorial, involving both intrinsic genetic predispositions and extrinsic environmental factors.
The epidemiology of JHV indicates a higher prevalence in females and a significant familial component, with an autosomal dominant inheritance pattern frequently observed. While some studies report prevalence rates ranging from 1% to 8% in adolescent populations, the true incidence requiring surgical intervention is lower. The natural history of JHV is often one of progression during growth spurts, leading to increased pain, difficulty with shoe wear, and functional limitations. Conservative management strategies are typically exhausted prior to considering surgical intervention, with the primary goal being pain relief, functional improvement, and prevention of further deformity progression during skeletal maturation. Understanding the nuances of JHV, particularly the presence of open physes and the absence of degenerative arthritis, is paramount for selecting appropriate and durable surgical corrections.
Surgical Anatomy and Biomechanics
The anatomical and biomechanical characteristics of juvenile hallux valgus distinguish it significantly from adult bunion deformities, primarily due to the ongoing skeletal development and lack of degenerative changes. The deformity is triplanar, involving transverse, sagittal, and coronal planes.
Medial Deviation of the First Metatarsal
Metatarsus primus varus, defined by an increased intermetatarsal (IM) angle, is a hallmark of JHV. This angle, measured between the longitudinal axes of the first and second metatarsals, is typically considered abnormal when exceeding 9 degrees. This medial deviation of the first metatarsal shaft positions the first metatarsal head more medially, contributing to the lateral deviation of the hallux.

Medial Cuneiform First Metatarsal Joint Obliquity
An often-overlooked contributor to metatarsus primus varus is the obliquity of the medial cuneiform-first metatarsal joint. An abnormally oblique joint orientation predisposes the first ray to adduct, thereby increasing the IM angle and contributing to the overall deformity. This anatomical variant implies that corrections solely at the metatarsal shaft or head may not fully address the proximal architectural defect.
First Metatarsophalangeal Joint Valgus Angulation
The valgus angulation of the great toe at the first MTP joint is a direct consequence of the metatarsus primus varus and associated soft tissue imbalance. This is quantified by the hallux valgus angle (HVA), typically considered abnormal when exceeding 15 degrees. Unlike adult bunions, the first MTP joint in JHV generally lacks significant osteoarthrosis, maintaining a relatively congruent joint space initially, although chronic subluxation can lead to adaptive changes.
Soft Tissue Imbalance and Sesamoid Subluxation
Pathological soft tissue changes are critical in the progression and stability of JHV.
* Adductor Hallucis Muscle: This muscle, originating from the base of the 2nd-4th metatarsals and inserting into the lateral aspect of the proximal phalanx, plays a significant role. Its contracture or persistent pull contributes to lateral deviation of the hallux and pronation of the toe.
* Abductor Hallucis Muscle: In JHV, the abductor hallucis muscle may become displaced plantarly and laterally from its normal medial course, losing its mechanical advantage to abduct and pronate the hallux. This allows unopposed pull of the adductor hallucis and potentially the flexor hallucis brevis lateral head.
* Collateral Ligaments and Joint Capsule: The lateral collateral ligament and lateral joint capsule become contracted, further pulling the hallux into valgus. Conversely, the medial collateral ligament and medial capsule become attenuated and lax.
* Extensor Hallucis Longus (EHL) and Flexor Hallucis Longus (FHL) Tendons: These tendons may also subluxate laterally, contributing to the deforming forces and pronation of the hallux.
Lateral translation and rotation of the sesamoid complex under the first metatarsal head are common findings in JHV. This subluxation reflects the lateral displacement of the flexor hallucis brevis tendons and alters the biomechanics of the MTP joint, further destabilizing the joint. The degree of sesamoid subluxation is a significant indicator of deformity severity and often dictates the extent of lateral soft tissue release required.

Physis and Skeletal Immaturity
A crucial differentiating factor in JHV is the presence of open physes in the first metatarsal and proximal phalanx. The first metatarsal physis is located proximally, which limits the safe application of proximal metatarsal osteotomies that could compromise longitudinal growth. Similarly, the proximal phalanx physis must be considered during Akin-type osteotomies. This necessitates careful surgical planning to avoid physeal arrest or angular deformities.
Other Associated Findings
- Generalized Ligamentous Laxity: Many adolescents with JHV present with generalized ligamentous laxity, which can contribute to the development and progression of the deformity.
- Flexible Pes Planus: A flexible flatfoot deformity often coexists with JHV. The associated hyperpronation of the foot can exacerbate the metatarsus primus varus and the valgus deformity of the hallux.
- Gastrocnemius Contracture: A tight heel cord can lead to compensatory pronation of the foot, thereby indirectly contributing to the deforming forces on the first ray.
- Pronation of the Great Toe: The hallux itself often exhibits internal rotation or pronation, further complicating the deformity. This is often associated with the lateral subluxation of the sesamoids and altered muscle pull.
In summary, the surgical anatomy of JHV involves a complex interplay of osseous malalignment, soft tissue imbalance, and physeal considerations, all contributing to a progressive, multiplanar deformity.
Indications and Contraindications
The decision for surgical correction of juvenile hallux valgus is complex, weighing the risks and benefits of intervention against the potential for continued progression and functional impairment. Surgical indications are primarily driven by symptoms and objective measures of deformity progression, particularly after failed conservative management.
Indications for Operative Management
- Pain: Persistent pain at the medial eminence or the first MTP joint during activity or shoe wear that is unresponsive to appropriate conservative measures.
- Progressive Deformity: Documented radiographic progression of the hallux valgus angle (HVA) or intermetatarsal (IM) angle over time, particularly during growth spurts.
- Functional Limitation: Difficulty participating in sports or daily activities due to foot pain or abnormal mechanics.
- Shoe Wear Difficulty: Inability to find comfortable footwear due to the prominent medial eminence or severe hallux valgus.
- Failure of Conservative Management: A minimum of 6-12 months of appropriate non-operative treatment, including wide toe-box shoes, orthotics, activity modification, and NSAIDs, without significant improvement in symptoms or deformity.
- Deformity Severity: While specific thresholds vary, an HVA greater than 25-30 degrees, an IM angle greater than 12-15 degrees, or significant sesamoid subluxation often point towards surgical intervention, especially in symptomatic patients.
- Skeletal Maturity: While JHV implies immaturity, most surgeons prefer to operate closer to skeletal maturity, typically in the mid-to-late adolescent years, to minimize recurrence and avoid physeal complications, particularly for more aggressive procedures. However, severe, rapidly progressing deformities in younger adolescents may necessitate earlier intervention.
Contraindications for Operative Management
- Asymptomatic Deformity: Cosmetic concerns alone are generally not an indication for surgical correction in JHV due to potential complications and recurrence rates.
- Mild Deformity: Mild hallux valgus without pain or functional impairment.
- Unrealistic Patient or Parent Expectations: A thorough discussion of surgical outcomes, potential complications, and recurrence rates is crucial.
- Active Infection: Local or systemic infection is an absolute contraindication.
- Severe Neurovascular Compromise: Significant peripheral neuropathy or vascular insufficiency.
- Insufficient Skeletal Maturity: For procedures that involve significant manipulation or osteotomy near the proximal first metatarsal physis, surgery may be deferred until closer to physeal closure to minimize risk of physeal arrest or growth disturbance.
- Poor Patient Compliance: Inability or unwillingness to adhere to rigorous postoperative rehabilitation protocols.
- Certain Systemic Conditions: Uncontrolled diabetes, severe peripheral vascular disease, or specific genetic syndromes that may impair wound healing or bone consolidation.
The following table summarizes the key considerations for operative versus non-operative management:
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Pain | Persistent, activity-limiting pain unresponsive to conservative care. | Mild, intermittent pain controlled with shoe modification and NSAIDs. |
| Deformity | Progressive HVA >25-30°, IM angle >12-15°, significant sesamoid subluxation. | Asymptomatic or mildly symptomatic, non-progressive deformity. |
| Function | Impaired ambulation, sports participation, or daily activities. | No significant functional limitation. |
| Shoe Wear | Inability to comfortably wear most shoes despite wide toe-box options. | Accommodated by appropriately sized and shaped footwear. |
| Progression | Documented radiographic progression during observation. | Stable deformity without documented progression. |
| Skeletal Status | Nearing skeletal maturity or severe, rapidly progressing deformity in younger patient. | Young, growing patient with mild deformity, allowing for continued observation. |
| Comorbidities | No significant medical comorbidities impacting surgery or healing. | Uncontrolled systemic diseases or conditions precluding surgery. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical for optimizing outcomes in juvenile hallux valgus correction. This process involves a comprehensive clinical assessment, detailed radiographic analysis, and careful consideration of the specific surgical technique tailored to the patient's deformity and skeletal maturity.
Clinical Assessment
A detailed history should include the onset of symptoms, pain characteristics, progression of deformity, previous conservative treatments, and the presence of any associated systemic conditions (e.g., generalized ligamentous laxity, neuromuscular disorders). Physical examination focuses on:
* Foot Type: Assessment for flexible pes planus, rearfoot pronation, and gastrocnemius contracture (Silfverskiöld test).
* First MTP Joint: Range of motion (dorsiflexion, plantarflexion, circumduction), stability, and presence of any crepitus or synovitis.
* Hallux Deformity: Clinical measurement of HVA and interphalangeal angle, assessment of hallux pronation.
* First Ray Mobility: Evaluation of sagittal plane mobility of the first ray (hypermobility or stiffness).
* Neurological and Vascular Status: Standard assessment of sensation and pedal pulses.
* Skin Condition: Inspection for calluses, irritation, or interdigital lesions.
Radiographic Assessment
Weight-bearing radiographs are indispensable for precise deformity analysis and surgical planning.
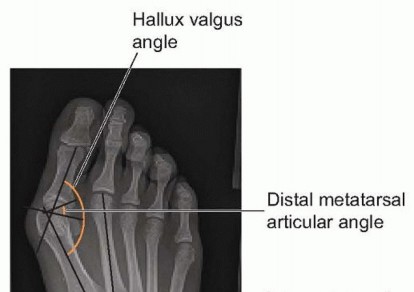
* Anteroposterior (AP) View:
* Hallux Valgus Angle (HVA): Angle between the longitudinal axes of the first metatarsal and the proximal phalanx. Normal <15°.
* Intermetatarsal Angle (IMA): Angle between the longitudinal axes of the first and second metatarsals. Normal <9°.
* Distal Metatarsal Articular Angle (DMAA): Angle between the articular surface of the first metatarsal head and the longitudinal axis of the first metatarsal shaft. Normal <10°. An increased DMAA (pes valgus) indicates an incongruent MTP joint and suggests the need for biplanar osteotomies (e.g., Reverdin-Laird, bicorrectional osteotomy).
* Metatarsophalangeal Joint Congruity: Assessment for lateral subluxation or incongruity.
* Medial Cuneiform-First Metatarsal Angle: Evaluation of any obliquity at the TMT joint.
* Physeal Status: Assessment of the proximal first metatarsal and proximal phalangeal physes.
* Lateral View:
* First Metatarsal Declination Angle: Assessment for plantarflexion or dorsiflexion of the first metatarsal.
* Sesamoid Position: Evaluates plantar subluxation or integrity of the sesamoid complex.
* Sesamoid Axial View:
* Sesamoid Position: Critical for assessing lateral subluxation of the fibular sesamoid relative to the first metatarsal head. This directly correlates with the severity of lateral soft tissue contracture.
* Hallux Pronation: Can sometimes be inferred from this view if the sesamoids appear rotated.
* Oblique View: Can be helpful for assessing the lesser metatarsals and overall foot architecture.
Image acquisition of weight-bearing radiographs is critical for accurate measurements.

Surgical Goals and Procedure Selection
Based on the clinical and radiographic findings, specific surgical goals are established:
1. Correction of metatarsus primus varus (IM angle).
2. Correction of hallux valgus (HVA) and hallux pronation.
3. Rebalancing of soft tissues around the MTP joint.
4. Preservation of the physeal plates in skeletally immature patients.
5. Resection of the medial eminence (if symptomatic).
6. Address associated deformities (e.g., gastrocnemius contracture).
The choice of surgical procedure depends on multiple factors:
* Patient Age and Skeletal Maturity: Open physes dictate physeal-sparing osteotomies.
* Severity of Metatarsus Primus Varus (IM angle): Distal osteotomies are generally suitable for mild-moderate IM angles (<15°), while shaft or proximal osteotomies are considered for larger angles.
* Severity of Hallux Valgus (HVA): Often corrected in conjunction with IM angle.
* Presence of DMAA (Pes Valgus): Requires specific biplanar osteotomies.
* First Ray Hypermobility: May necessitate TMT fusion in select, severe cases, though rarely in juvenile patients.
* Gastrocnemius Contracture: May require an adjunctive heel cord lengthening procedure.
Anesthesia and Patient Positioning
- Anesthesia: General anesthesia is typically employed, often supplemented with a regional ankle block for postoperative pain control.
- Tourniquet: A thigh or ankle tourniquet is used to maintain a bloodless field, crucial for precise osteotomy and soft tissue dissection.
- Patient Positioning: Supine position on the operating table. The foot is prepped and draped to the mid-calf, allowing for full range of motion assessment during the procedure. A bump under the ipsilateral hip may be used to internally rotate the limb slightly for better access to the medial aspect of the foot.
Detailed Surgical Approach and Technique
Surgical correction of juvenile hallux valgus typically involves a combination of soft tissue releases, bony osteotomies, and capsular plication, all performed with careful attention to preserving physeal integrity. The specific technique is customized based on the magnitude of the deformity, the patient's skeletal maturity, and the presence of associated conditions. A common approach involves a distal metatarsal osteotomy combined with a lateral soft tissue release and medial capsular reefing.
General Principles
- Lateral Soft Tissue Release: Addressing the contracted lateral structures is often the initial step to facilitate reduction of the hallux.
- Bony Correction: Osteotomies are performed to correct metatarsus primus varus, hallux valgus, and often the DMAA.
- Medial Capsular Plication: Tightening the medial capsule helps stabilize the correction and prevent recurrence.
- Physeal Protection: Paramount in juvenile cases; osteotomies must be planned to avoid or minimize injury to the proximal metatarsal and proximal phalangeal physes.
- Rigid Fixation: Adequate internal fixation is crucial for stability and early rehabilitation.
Surgical Steps for a Distal Metatarsal Osteotomy (e.g., Modified Chevron) with Lateral Release and Medial Plication
This description outlines a frequently used technique for moderate juvenile hallux valgus.
1. Incision and Dissection
- A curvilinear incision is made along the medial aspect of the first MTP joint, beginning proximally to the metatarsal head and extending distally to the mid-proximal phalanx. The incision should allow adequate exposure of the metatarsal head, joint capsule, and medial eminence.
- Dissection is carried down through the subcutaneous tissue. Care is taken to identify and protect the dorsal medial cutaneous nerve of the hallux.
- The medial capsule is incised longitudinally along the border of the abductor hallucis tendon. The medial eminence is exposed.
2. Medial Eminence Resection
- Using a sagittal saw, the prominent medial eminence of the first metatarsal head is resected. The cut should be parallel to the weight-bearing surface of the foot and aim to remove only the exostosis, leaving the articular cartilage intact. Excessive resection can lead to devascularization or instability.
3. Lateral Soft Tissue Release
- This step is crucial for achieving full correction and reducing the tension on the lateral structures.
- Adductor Hallucis Tendon Release: A small incision (typically 1-2 cm) is made on the dorsolateral aspect of the first MTP joint, either directly over the adductor tendon insertion or through the first web space. The adductor hallucis tendon, which inserts into the lateral base of the proximal phalanx and the fibular sesamoid, is identified and tenotomized.
- Lateral Capsulotomy: Through the lateral incision, or often through the main medial incision with the joint distracted, the lateral collateral ligament and lateral joint capsule are incised. This can involve a complete release or a targeted partial release depending on contracture severity. Care must be taken to avoid injury to the extensor hallucis longus tendon dorsally and the neurovascular bundle laterally.
- Fibular Sesamoid Release: If the fibular sesamoid is significantly subluxated and tightly bound, it may need to be released from its adhesions to the lateral aspect of the first metatarsal head.
4. Distal Metatarsal Osteotomy (Modified Chevron)
- The goal is to laterally translate the metatarsal head, thereby correcting the metatarsus primus varus and reducing the HVA.
- Pilot Holes: Two small drill holes are made on the dorsomedial and plantar-medial aspects of the first metatarsal neck, just proximal to the articular surface. These serve as starting points for the osteotomy.
- V-Osteotomy: A V-shaped osteotomy is performed using a sagittal saw. The apex of the V is distal, pointing towards the metatarsal head. The dorsal arm of the osteotomy is made approximately 5-7 mm proximal to the articular cartilage, extending laterally and slightly proximally. The plantar arm extends from the plantar aspect of the metatarsal head, meeting the dorsal arm laterally. This precise cut ensures preservation of the physis, which is located more proximally.
- Head Translation: The distal fragment (metatarsal head) is then translated laterally on the proximal shaft fragment. The amount of translation is guided by the desired correction of the IM angle, typically 50-75% of the metatarsal shaft width. Over-translation should be avoided to prevent hallux varus.
- Fixation: Once the desired position is achieved, the osteotomy is stabilized. In juvenile patients, this often involves one or two small K-wires (e.g., 0.045-inch or 0.062-inch) placed across the osteotomy site. Alternatively, a single cortical screw (e.g., 2.0 mm or 2.4 mm) can be used, ensuring it does not impinge on the articular surface or physis. Screw fixation offers greater rigidity and allows for earlier weight-bearing.

5. Medial Capsular Plication (Reefing)
- After bony correction, the medial joint capsule, which was initially incised, is meticulously reefed (tightened) and imbricated. This involves overlapping and suturing the capsule to further stabilize the first MTP joint, preventing recurrence of the hallux valgus and correcting any residual pronation. Absorbable sutures (e.g., 2-0 or 3-0) are commonly used.
6. Adjunctive Procedures (If Necessary)
- Akin Osteotomy: If there is residual valgus deformity at the interphalangeal joint, a medial closing wedge osteotomy of the proximal phalanx may be performed. The cut is made distal to the physis. Fixation is typically with a K-wire or small staple.
- Gastrocnemius Recession/Lengthening: If a significant gastrocnemius contracture is identified preoperatively, a percutaneous or open gastrocnemius recession (e.g., Strayer, Baumann) may be performed to address the associated foot pronation.
7. Wound Closure
- The wounds are irrigated, and hemostasis is ensured.
- Subcutaneous layers are closed with absorbable sutures.
- The skin is closed with absorbable sutures (e.g., 4-0) or non-absorbable sutures/staples.
- A sterile dressing is applied, followed by a soft compressive bandage and a plaster splint or surgical shoe, positioning the hallux in a slight varus overcorrection to allow for swelling and minor loss of correction.

Other Osteotomy Options in Juvenile Hallux Valgus
- Reverdin-Laird Osteotomy: Similar to Chevron but with an additional plantar cut or wedge resection to correct an increased DMAA (pes valgus).
- Scarf Osteotomy: A Z-shaped osteotomy of the first metatarsal shaft, allowing for translation, shortening, lengthening, and rotation of the metatarsal head. It provides excellent stability and versatile correction but requires a longer metatarsal incision and careful technique to avoid nonunion or avascular necrosis. Typically reserved for older adolescents closer to skeletal maturity due to the extensive periosteal stripping.
- Proximal Metatarsal Osteotomies (e.g., Crescentic, Opening/Closing Wedge): These osteotomies are generally avoided in skeletally immature patients due to the risk of physeal injury, as the physis is located proximally. They are typically reserved for severe metatarsus primus varus in patients with closed physes or in very specific cases where other options are insufficient and physeal sparing techniques are employed.
- Lapidus Procedure (First Tarsometatarsal Arthrodesis): Rarely indicated in juvenile hallux valgus, this procedure is reserved for severe metatarsus primus varus, particularly with first ray hypermobility or TMT joint obliquity, typically in older adolescents approaching skeletal maturity or with physeal closure. It effectively reduces the IM angle at its source but fuses a joint.
The selection of the specific osteotomy or combination of procedures is paramount and requires a thorough understanding of the deformity's characteristics, the patient's growth status, and the biomechanical goals of the surgery.
Complications and Management
Despite meticulous surgical technique, complications can occur following surgical correction of juvenile hallux valgus. A comprehensive understanding of potential adverse events, their incidence, and appropriate management strategies is essential for orthopedic surgeons.
Common Complications
-
Recurrence of Deformity:
- Description: Reappearance of hallux valgus or metatarsus primus varus. This is the most common complication in juvenile bunion surgery, with reported rates varying widely from 10% to 50%, often attributed to continued growth, incomplete correction, or inadequate addressing of underlying etiologies (e.g., ligamentous laxity, foot pronation).
- Management: Mild, asymptomatic recurrence may be observed. Symptomatic or progressive recurrence often necessitates revision surgery, potentially with a more aggressive osteotomy or a different approach. Adjunctive procedures (e.g., gastrocnemius recession) may be considered if not performed initially.
-
Undercorrection or Overcorrection:
- Description: Under-correction results in residual hallux valgus; overcorrection leads to hallux varus. Both can be immediate or become apparent post-healing.
- Management: Mild undercorrection may be acceptable if asymptomatic. Significant undercorrection or hallux varus often requires revision surgery. For hallux varus, soft tissue procedures (e.g., medial capsule release, lateral capsule imbrication, adductor transfer) may suffice for mild cases. Severe hallux varus may require reverse osteotomies or fusion.
-
Avascular Necrosis (AVN) of the Metatarsal Head:
- Description: Ischemic insult to the first metatarsal head, particularly a risk with distal osteotomies (e.g., Chevron) if periosteal stripping is excessive or vascular supply is compromised. Incidence is low, typically <5%, but can lead to devastating long-term consequences.
- Management: Prevention is key through careful surgical technique. If suspected, protected weight-bearing and close observation. Established AVN may lead to collapse and secondary arthritis, potentially requiring joint-sparing procedures (e.g., débridement, bone grafting) or, in severe cases, MTP fusion in adulthood.
-
Physeal Arrest or Growth Disturbance:
- Description: Damage to the proximal first metatarsal physis or proximal phalangeal physis during osteotomy can lead to growth arrest, limb length discrepancy, or angular deformity (e.g., metatarsus adductus if first metatarsal physis is damaged). This is a unique risk in juvenile patients.
- Management: Prevention through meticulous physeal-sparing techniques. If arrest occurs, monitoring for progression. Corrective osteotomies may be considered later to address length or angular deformities.
-
Nonunion or Malunion of Osteotomy:
- Description: Failure of the osteotomy fragments to heal (nonunion) or healing in an unacceptable position (malunion). Rates are generally low with stable fixation.
- Management: Nonunion may require revision surgery with bone grafting and more rigid fixation. Malunion, if symptomatic, requires corrective osteotomy.
-
Infection:
- Description: Superficial or deep surgical site infection. Incidence is generally low (<2%).
- Management: Superficial infections may respond to oral antibiotics. Deep infections require surgical débridement, intravenous antibiotics, and potentially hardware removal.
-
Hardware Irritation or Failure:
- Description: K-wires or screws can become prominent, cause pain, or break.
- Management: Symptomatic hardware typically requires removal after bony union is achieved.
-
Stiffness of the First MTP Joint:
- Description: Limited range of motion, often due to excessive capsular plication, prolonged immobilization, or inflammatory response.
- Management: Aggressive physical therapy. Manipulation under anesthesia or even arthrolysis may be considered in persistent, severe cases.
-
Transfer Metatarsalgia:
- Description: Pain under the lesser metatarsal heads, typically the second or third, due to altered weight-bearing mechanics after first ray surgery (e.g., excessive shortening or elevation of the first metatarsal).
- Management: Non-operative measures (metatarsal pads, orthotics). Surgical options may include lesser metatarsal osteotomies in refractory cases.
-
Nerve Injury:
- Description: Injury to the dorsal medial cutaneous nerve (sensory branch of the superficial peroneal nerve) resulting in numbness or painful neuroma.
- Management: Prevention through careful dissection. Neuropathic pain may be managed with medications; intractable neuromas may require excision.
The following table summarizes common complications and their management:
| Complication | Incidence (Approximate) | Salvage/Management Strategy |
|---|---|---|
| Recurrence of Deformity | 10-50% | Observation (asymptomatic), revision surgery (more aggressive osteotomy, different approach), adjunctive procedures (e.g., gastrocnemius recession). |
| Undercorrection | Variable | Observation (asymptomatic), revision surgery. |
| Overcorrection (Hallux Varus) | 1-5% | Soft tissue release/imbrication, revision osteotomy, MTP fusion (rarely). |
| Avascular Necrosis (AVN) | <5% | Protected weight-bearing, observation. In severe cases: joint-sparing procedures, MTP fusion. |
| Physeal Arrest/Growth Disturbance | <5% | Monitoring for deformity progression. Corrective osteotomy for significant length/angular deformities. |
| Nonunion/Malunion | <2% | Revision surgery with bone grafting, more rigid fixation (nonunion). Corrective osteotomy (symptomatic malunion). |
| Infection | <2% | Oral antibiotics (superficial). Surgical débridement, IV antibiotics, hardware removal (deep). |
| Hardware Irritation/Failure | 5-10% | Symptomatic hardware removal after bony union. |
| Stiffness of First MTP Joint | Variable | Aggressive physical therapy, manipulation under anesthesia, arthrolysis. |
| Transfer Metatarsalgia | 5-15% | Orthotics, metatarsal pads. Lesser metatarsal osteotomies (refractory cases). |
| Nerve Injury (Dorsal Medial) | 5-10% | Observation, pain management. Excision for intractable neuroma. |
Post Operative Rehabilitation Protocols
A structured and progressive postoperative rehabilitation protocol is crucial for achieving optimal functional outcomes and minimizing complications after juvenile hallux valgus correction. The protocol must consider the healing time of osteotomies, soft tissue repairs, and the need to protect the physeal plates.
Immediate Postoperative Period (Days 0-14)
- Immobilization: The foot is typically immobilized in a well-padded compressive dressing and a posterior plaster splint or rigid postoperative shoe. The hallux is often positioned in a slightly overcorrected varus position.
- Weight-Bearing: Non-weight-bearing (NWB) is generally recommended for the initial 2 weeks to protect the osteotomy site and allow for initial soft tissue healing. Crutches or a knee scooter are used.
- Elevation and Ice: Strict elevation of the operative limb above heart level is encouraged to minimize swelling. Regular application of ice packs (20 minutes every 2-3 hours) helps manage pain and edema.
- Pain Management: Opioid and non-opioid analgesics are prescribed as needed. Regional blocks can provide excellent initial pain control.
- Wound Care: The dressing is typically changed by the surgeon at the first postoperative visit (around 7-14 days). Incisions are inspected for signs of infection or wound dehiscence. Sutures or staples are removed at this time if non-absorbable.
Early Mobilization and Protected Weight-Bearing (Weeks 2-6)
- Immobilization: Transition from a splint to a rigid sole surgical shoe or a removable walking boot (CAM walker) at the 2-week mark.
- Weight-Bearing: Gradual progression to protected weight-bearing. Partial weight-bearing (PWB) in the surgical shoe or boot is initiated, progressively increasing as tolerated. Full weight-bearing (FWB) in the boot may be allowed by 4-6 weeks if radiographs show early signs of osteotomy healing.
- Range of Motion (ROM): Gentle active and passive range of motion exercises for the first MTP joint are initiated at 2-3 weeks, focusing on dorsiflexion and plantarflexion. The goal is to regain functional motion without stressing the osteotomy. Hallux abduction/adduction exercises are incorporated cautiously.
- Physical Therapy: Referral to a physical therapist may be beneficial to guide ROM exercises, manage edema, and instruct on safe ambulation with crutches/boot.
Progressive Strengthening and Functional Restoration (Weeks 6-12)
- Immobilization: The surgical shoe or boot is typically discontinued around 6-8 weeks, depending on radiographic evidence of bony union and clinical comfort. Transition to supportive, wide toe-box athletic shoes.
- Weight-Bearing: Full weight-bearing in regular shoes is permitted once bony union is confirmed.
- Strengthening: Progressive strengthening exercises for the intrinsic foot muscles, ankle dorsiflexors/plantarflexors, and evertors/invertors are emphasized. Proprioceptive exercises (e.g., single-leg stance, balance board) are introduced.
- Stretching: Continued stretching, especially for any residual gastrocnemius or soleus tightness, is important.
- Gait Training: Focus on normal gait mechanics and correcting any compensatory patterns.
- Scar Management: Gentle scar massage can begin once the incision is fully healed.
Return to Activity and Sports (Weeks 12+)
- Low-Impact Activities: Patients can gradually return to low-impact activities (e.g., walking, cycling, swimming) starting around 10-12 weeks, provided there is no pain and full MTP joint motion has been restored.
- High-Impact Activities and Sports: Return to higher-impact sports (e.g., running, jumping, court sports) is typically permitted at 4-6 months postoperatively, contingent upon full recovery of strength, range of motion, and absence of pain. This should be a gradual process, often guided by sport-specific drills.
- Orthotics: Custom or off-the-shelf orthotics may be recommended long-term, especially in patients with associated pes planus or hypermobility, to help maintain foot alignment and prevent recurrence.
- Follow-up: Regular clinical and radiographic follow-up continues until skeletal maturity to monitor for recurrence or other long-term complications. Hardware removal may be considered for symptomatic K-wires (typically at 6-8 weeks) or screws (typically after 6-12 months).
The rehabilitation protocol is individualized based on the specific surgical procedure performed, the extent of correction, the patient's age, and their progress. Close communication between the surgeon, physical therapist, patient, and parents is essential for successful rehabilitation.
Summary of Key Literature and Guidelines
The surgical management of juvenile hallux valgus (JHV) remains a topic of ongoing discussion and evolving consensus within orthopedic literature. Key areas of focus include the differentiation from adult hallux valgus, the impact of skeletal immaturity, and the long-term efficacy and recurrence rates associated with various surgical techniques.
Differentiation and Pathogenesis
Early literature, such as studies by Scranton et al. (1979) and Miller (1958), highlighted the distinct characteristics of JHV, particularly the absence of degenerative changes and the higher incidence of generalized ligamentous laxity and flexible pes planus compared to adults. Current understanding, as summarized by Coughlin and Saltzman (2009), emphasizes the multifactorial nature of JHV, involving genetic predisposition, anatomical variations (e.g., metatarsus primus varus, oblique cuneiform-metatarsal joint), and biomechanical factors (e.g., hyperpronation, gastrocnemius contracture). This understanding underscores the importance of addressing all components of the deformity.
Surgical Techniques and Outcomes
Numerous surgical procedures have been described for JHV, broadly categorized by the location of the osteotomy: distal, shaft, or proximal metatarsal osteotomies, often combined with soft tissue procedures and sometimes an Akin osteotomy.
- Distal Metatarsal Osteotomies (e.g., Chevron, Reverdin-Laird): These are frequently employed due to their physeal-sparing nature. Studies, such as those by Sammarco and Idusuyi (2002) on the modified Chevron, demonstrate good clinical and radiographic outcomes in a majority of patients. However, they may be less effective for severe metatarsus primus varus. Recurrence rates for these procedures in JHV range from 10% to 30%, which is generally higher than in adults. The Reverdin-Laird osteotomy, which addresses an increased DMAA, has shown promise in improving MTP joint congruity and reducing recurrence for specific deformities.
- Shaft Osteotomies (e.g., Scarf): The Scarf osteotomy offers greater versatility in correcting severe IM angles, shortening/lengthening, and rotation. While initially more complex, several series, including those by Weil and Wagner (1998) and Barouk (1995), have reported excellent results in adults and older adolescents. Its use in skeletally immature patients requires meticulous technique to avoid physeal injury and potential complications like avascular necrosis due to extensive periosteal stripping.
- Proximal Metatarsal Osteotomies: These are generally reserved for older adolescents with near-complete physeal closure or for very severe metatarsus primus varus, as they directly address the deformity closer to its apex. Examples include proximal crescentic or closing wedge osteotomies. Due to the proximity of the first metatarsal physis, these carry a higher risk of growth disturbance in younger adolescents.
- First Tarsometatarsal Arthrodesis (Lapidus Procedure): While a gold standard for severe metatarsus primus varus and hypermobility in adults, the Lapidus procedure is rarely indicated in JHV, primarily due to the concern for growth plate fusion and the availability of less invasive physeal-sparing options. It may be considered in severe, recurrent cases in patients approaching skeletal maturity with demonstrated TMT joint instability or obliquity.
Recurrence and Long-Term Outcomes
Recurrence remains a significant challenge in JHV surgery, often attributed to the continued growth potential and underlying etiologic factors. Factors contributing to recurrence include inadequate initial correction, failure to address ligamentous laxity or underlying foot pronation, and continued abnormal biomechanical forces. Long-term studies suggest that recurrence rates can increase with longer follow-up periods. Addressing associated factors like gastrocnemius contracture or pes planus with adjunctive procedures (e.g., gastrocnemius recession, orthotics) may help reduce recurrence. The overall consensus is that surgical intervention in JHV should aim for maximal correction of all deformity components while carefully preserving growth potential.
Guidelines and Recommendations
Current guidelines emphasize a conservative approach as the first line of management. Surgical intervention is typically reserved for symptomatic, progressive deformities that have failed non-operative treatment.
* Age and Skeletal Maturity: While no absolute age exists, most surgeons prefer to operate closer to skeletal maturity (late adolescence) to minimize recurrence and physeal complications, particularly for more extensive osteotomies.
* Radiographic Assessment: Comprehensive weight-bearing radiographs including AP, lateral, and sesamoid axial views are mandatory for precise deformity analysis (HVA, IM angle, DMAA, sesamoid position).
* Procedure Selection: The choice of procedure should be individualized based on the severity and location of the deformity, the presence of DMAA, the status of the physes, and the surgeon's experience. Distal physeal-sparing osteotomies combined with soft tissue release are often the initial choice for mild-moderate deformities.
* Postoperative Care: Rigorous rehabilitation protocols are critical, emphasizing controlled weight-bearing, early range of motion, and strengthening to achieve optimal functional outcomes.
In conclusion, surgical correction of juvenile hallux valgus requires a nuanced approach, acknowledging the unique aspects of the growing foot. While various techniques have proven effective, surgeons must prioritize physeal preservation, achieve comprehensive multiplanar correction, and meticulously manage postoperative rehabilitation to minimize recurrence and optimize long-term patient satisfaction and function. Continued research is needed to further refine indications, techniques, and long-term outcomes in this challenging patient population.
Clinical & Radiographic Imaging

You Might Also Like