Osteochondral Lesions of the Talus: Surgical Management

Key Takeaway
Osteochondral lesions of the talus (OLT) represent a complex spectrum of transchondral fractures primarily driven by trauma. Effective management requires precise staging via MRI and CT. While stable lesions may respond to immobilization, displaced or cystic lesions necessitate surgical intervention. Operative strategies range from arthroscopic debridement and microfracture to retrograde drilling and advanced cartilage restoration, tailored to the lesion's morphology and location.
Introduction and Historical Context
The nomenclature surrounding osteochondral lesions of the talus (OLT) has historically been fraught with ambiguity, reflecting an evolving understanding of their etiology and natural history. Terms such as osteochondritis dissecans, osteochondral fracture, transchondral fracture, and talar dome fracture have been used interchangeably.
The historical timeline of OLT recognition provides critical context for modern management:
* 1888 (König): Coined the term osteochondritis dissecans to describe loose bodies in the knee, theorizing spontaneous bone necrosis as the primary driver.
* 1922 (Kappis): Recognized the morphological similarities between knee lesions and those in the ankle joint.
* 1932 (Rendu): Documented an intra-articular fracture of the talus mirroring osteochondritis dissecans.
* 1959 (Berndt and Harty): Conducted an exhaustive review and cadaveric study, definitively concluding that "osteochondritis dissecans" of the talus is, in reality, a trauma-induced transchondral (osteochondral) fracture. They established the foundational four-stage classification system still referenced today.
Clinical Pearl: Despite the historical use of "osteochondritis dissecans," the modern orthopedic consensus recognizes acute trauma or chronic microtrauma as the primary etiology in the vast majority of talar dome lesions.
Epidemiology and Etiology
Osteochondral lesions of the talus account for approximately 4% of all osteochondral lesions in the body; however, this figure likely underestimates the true incidence. Advanced imaging studies suggest that OLTs may occur in up to 50% of acute ankle sprains and fractures, particularly within athletic populations.
A significant clinical challenge is the initial misdiagnosis. Nearly 50% of OLTs are missed on initial emergency department radiographs, frequently dismissed as simple "ankle sprains."
While a history of trauma is documented in over 85% of patients, Flick and Gould demonstrated a distinct anatomical variance in traumatic etiology:
* Lateral Lesions: 98% associated with a definitive history of trauma.
* Medial Lesions: 70% associated with a history of trauma.
Other proposed, though less common, etiologies include local osteonecrosis, systemic vasculopathies, endocrine/metabolic factors, joint malalignment, and genetic predisposition.
Pathoanatomy and Biomechanics
The anatomical location of the lesion dictates its morphological characteristics and the underlying mechanism of injury.
Medial Talar Dome Lesions
Medial lesions are statistically more common than their lateral counterparts.
* Mechanism of Injury: Inversion, plantar flexion, and lateral rotation of the tibia on the talus.
* Location: Typically posterior.
* Morphology: Deep and cup-shaped.
* Displacement: Usually non-displaced, remaining stable within the subchondral crater.
Lateral Talar Dome Lesions
- Mechanism of Injury: Inversion combined with strong dorsiflexion.
- Location: Typically anterior.
- Morphology: Shallow and wafer-shaped.
- Displacement: Highly prone to displacement and mechanical symptom generation.

Clinical Presentation and Diagnostic Imaging
Patients typically present with deep, aching ankle pain exacerbated by weight-bearing. Pathognomonic signs of an underlying OLT following an inversion injury include persistent effusion, delayed synovitis, and mechanical symptoms such as locking, catching, or "giving way" 4 to 5 weeks post-injury.
Radiographic Evaluation
Standard anteroposterior (AP) and lateral radiographs often fail to isolate the lesion due to tibial overlap. Oblique and plantar flexion views are mandatory to profile the talar dome.

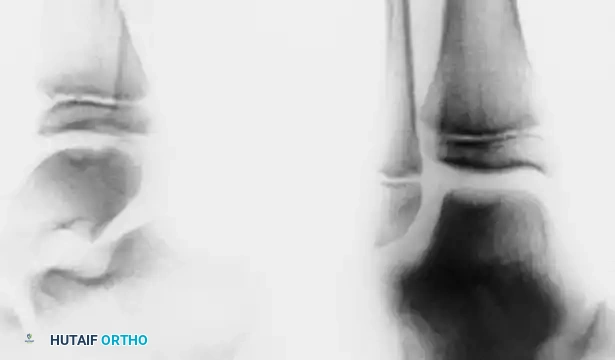
Radiographs of a stage III lateral lesion. (A) Preoperative radiograph showing a detached but undisplaced fragment. (B) Postoperative resolution following excision.

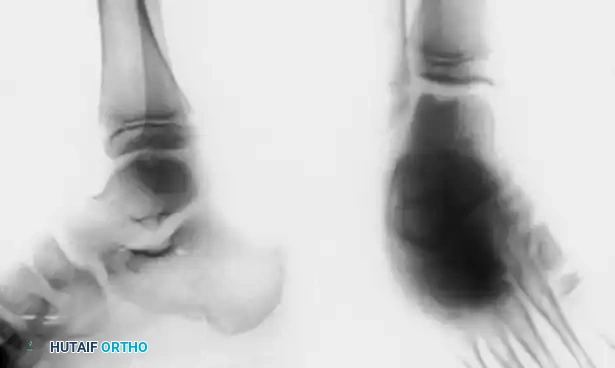
Early evidence of OLT in a child with open physes (A), demonstrating consolidation after 6 months of conservative management (B).
Advanced Imaging (CT and MRI)
If radiographs are negative but clinical suspicion remains high (or if a technetium bone scan is positive), advanced imaging is required.
Computed Tomography (CT):
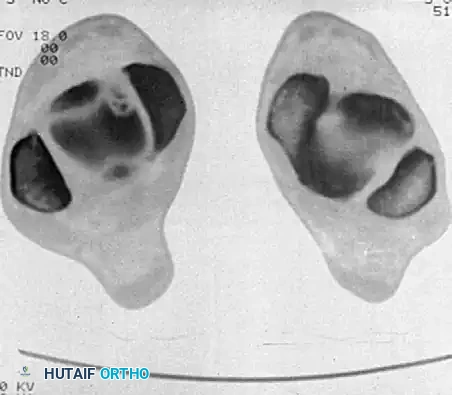
CT scans utilizing 2-mm cuts in both axial and coronal planes are the gold standard for defining the osseous architecture, exact size, location, and the presence of subchondral cysts. CT is indispensable for preoperative planning, specifically to determine if a medial malleolar osteotomy is required for access.
Magnetic Resonance Imaging (MRI):
MRI is the modality of choice for evaluating the integrity of the articular cartilage and identifying early (Stage I) lesions characterized solely by bone marrow edema. It is highly sensitive for detecting synovial fluid interposition between the fragment and the talar bed, indicating instability.



Comprehensive Classification Systems
Accurate staging is paramount for guiding treatment. The classification of OLTs has evolved across multiple imaging modalities.
Plain Radiograph & CT Classifications
Berndt & Harty (1959) - Plain Radiographs:
* Stage I: Small area of compression of subchondral bone.
* Stage II: Partially detached osteochondral fragment.
* Stage III: Completely detached osteochondral fragment remaining in the crater (undisplaced).
* Stage IV: Displaced osteochondral fragment.
Loomer et al. (1993) - CT Modification:
* Added Stage V: Radiolucent subchondral cystic lesion.
Ferkel & Sgaglione (1994) - CT Staging:
* Stage I: Cystic lesion within the dome, intact roof.
* Stage IIA: Cystic lesion communicating with the talar dome surface.
* Stage IIB: Open articular surface lesion with overlying non-displaced fragment.
* Stage III: Undisplaced lesion with lucency.
* Stage IV: Displaced fragment.
MRI Classifications
Hepple et al. (1999):
* Stage 1: Articular cartilage damage only.
* Stage 2a: Cartilage injury with underlying fracture and surrounding bony edema.
* Stage 2b: Stage 2a without surrounding bony edema.
* Stage 3: Detached but undisplaced fragment.
* Stage 4: Detached and displaced fragment.
* Stage 5: Subchondral cyst formation.
Arthroscopic Classifications
Arthroscopy remains the definitive diagnostic tool as it allows direct tactile probing of the cartilage.
Cheng et al. (1995):
* Grade A: Smooth, intact but soft or ballottable.
* Grade B: Rough surface.
* Grade C: Fibrillation/fissuring.
* Grade D: Flap present or bone exposed.
* Grade E: Loose, undisplaced fragment.
* Grade F: Displaced fragment.
Indications for Treatment
Treatment algorithms are dictated by patient age, activity level, lesion size, location, and stability.
Conservative Management
Non-operative treatment is indicated for:
* Incomplete medial and lateral lesions (Stage II).
* Completely detached but undisplaced medial lesions (Stage III).
* Almost all lesions occurring in skeletally immature patients (children with open physes).
Protocol: Immobilization in a short-leg cast or a patellar tendon-bearing (PTB) brace for 4 to 6 weeks, followed by progressive physical therapy. If symptoms persist or imaging shows progression after 4 to 6 months, surgical intervention is warranted.
Surgical Warning: Literature indicates that non-operative management of chronic, cystic talar lesions yields successful outcomes in only 45% to 54% of cases. Prolonged conservative treatment in displaced or highly symptomatic lesions may lead to progressive degenerative joint disease.
Operative Management
Surgical intervention is indicated for:
* All displaced lesions (Stage IV).
* Completely detached lateral lesions (Stage III) due to their high non-union rate and propensity for displacement.
* Lesions failing 4-6 months of conservative therapy.
Operative strategies fall into three broad categories:
1. Debridement and Marrow Stimulation: Excision, curettage, and microfracture/drilling.
2. Direct Repair: Internal fixation (retrograde K-wires, bioabsorbable pins) or retrograde drilling with bone grafting.
3. Cartilage Restoration: Osteochondral autograft transfer (OATS), allografts, or autologous chondrocyte implantation (ACI).
Surgical Techniques
Preoperative Planning and Approach Selection
CT imaging with 2-mm coronal and axial cuts is critical to localize the lesion into the anterior, middle, or posterior third of the talar dome.
* Lateral Lesions: Because the lateral malleolus is positioned posterior to the central axis of the tibia, lateral lesions (even in the middle or posterior third) can usually be accessed via an anterior arthroscopic or mini-open approach without osteotomy.
* Medial Lesions: Posterior-medial lesions frequently require a medial malleolar osteotomy for perpendicular access to the defect.
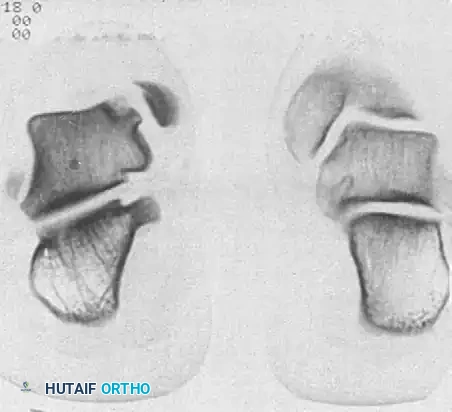
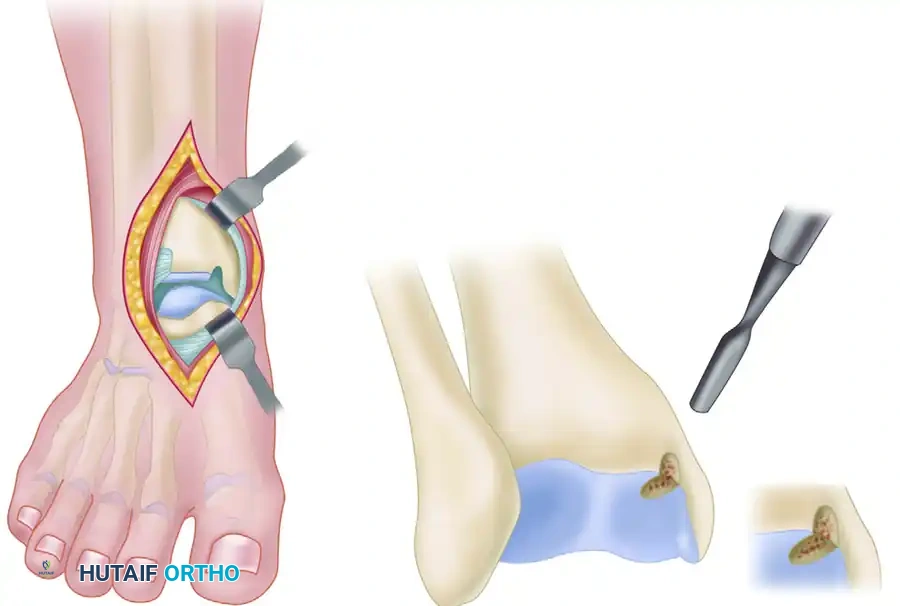
Diagram illustrating access to the talar dome, highlighting the necessity of medial malleolar osteotomy for deep posterior-medial lesions.
Arthroscopic Debridement and Microfracture
For lesions smaller than 1.5 cm², arthroscopic excision of the fragment, curettage of the necrotic base, and marrow stimulation (microfracture) is the gold standard.
- Positioning: Supine with a non-invasive ankle distractor.
- Portals: Standard anteromedial and anterolateral portals.
- Preparation: The loose fragment is excised. The sclerotic base of the crater is aggressively curetted until healthy, bleeding punctate bone is encountered.
- Microfracture: An arthroscopic awl is used to create holes 3-4 mm apart and 4-5 mm deep into the subchondral bone to release marrow elements (mesenchymal stem cells) that will form a fibrocartilage repair tissue (Type I cartilage).
Retrograde Percutaneous Drilling and Bone Grafting
For early lesions (intact cartilage but subchondral cystic changes/necrosis), retrograde drilling preserves the articular surface while stimulating healing. This is highly effective in young patients and those with open physes.
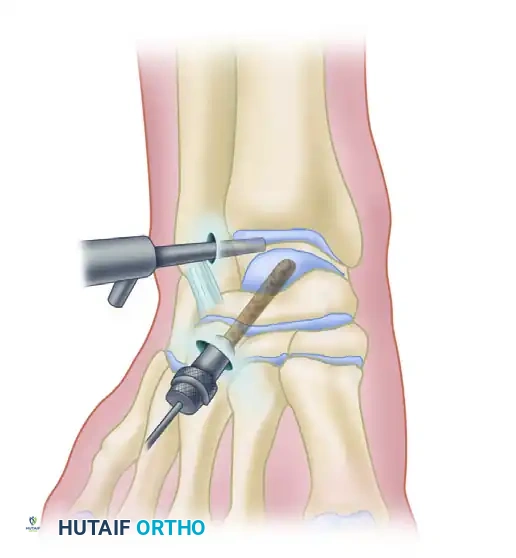
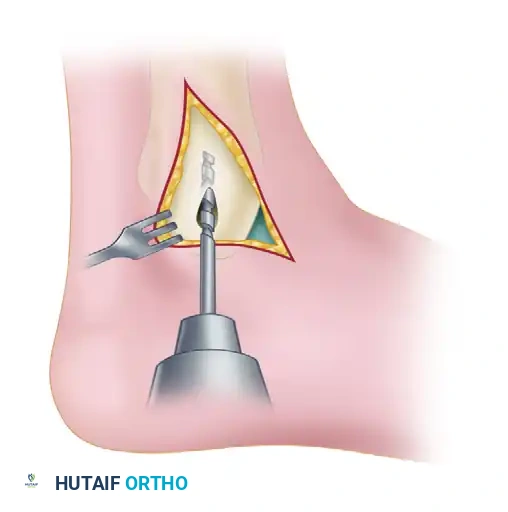
Arthroscopic retrograde drilling and bone grafting as described by Stone and Gould. (A) A guide pin is placed through the sinus tarsi using a modified ligament guide. (B) Graft material is compressed into the channel.
Surgical Steps:
1. Targeting: Under arthroscopic visualization, the intact articular cartilage is confirmed. A modified anterior cruciate ligament (ACL) drill guide is placed through the anterolateral portal, targeting the center of the lesion.
2. Drilling: A guide pin is advanced percutaneously from the sinus tarsi (for medial lesions) or the medial talar neck (for lateral lesions) into the subchondral cyst, stopping just short of the articular cartilage.
3. Fluoroscopic Confirmation: Intraoperative C-arm fluoroscopy confirms the trajectory and depth.
4. Decompression and Grafting: The tract is over-drilled. The cystic contents are curetted. To prevent articular collapse, the void is backfilled. Options include cancellous autograft, surgical-grade calcium sulfate, or bone marrow aspirate concentrate (BMAC) harvested from the iliac crest.
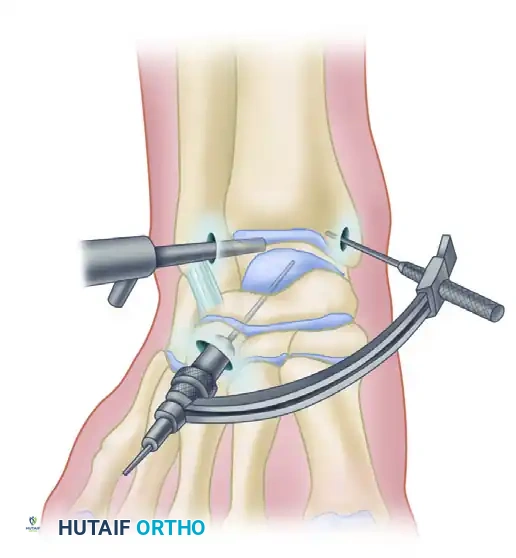
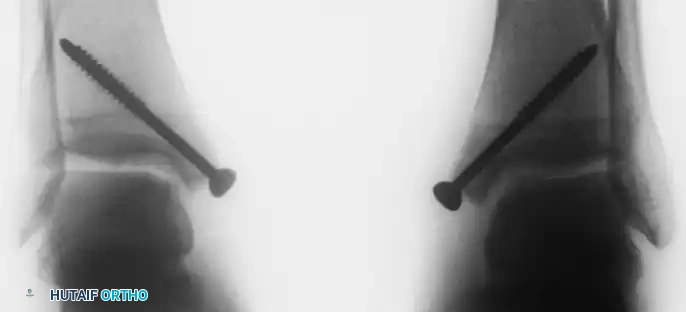
Retrograde drilling of an osteochondral lesion. After confirming intact cartilage, the subchondral lesion is drilled in a retrograde fashion and grafted.
Intraoperative fluoroscopy confirming the trajectory of the retrograde drill.
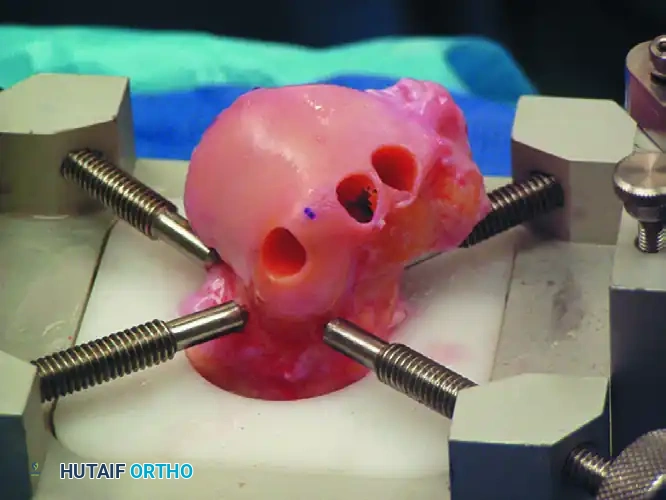
Open Medial Malleolar Osteotomy
When large, posterior-medial lesions require structural grafting (OATS) or direct fixation, an open approach via medial malleolar osteotomy is required.
- Incision: A longitudinal incision is made over the medial malleolus.
- Pre-drilling: Before the osteotomy, two parallel holes are drilled from the tip of the medial malleolus proximally into the tibial metaphysis. These are tapped for 4.0-mm cancellous screws to ensure perfect anatomic reduction during closure.
- Osteotomy: A chevron-type (V-shaped) osteotomy is performed using an oscillating saw, directed toward the axilla of the medial clear space. The osteotomy is completed with an osteotome to preserve bone dust and create a rough surface for healing.
- Exposure: The medial malleolus is reflected inferiorly on its intact deltoid ligament hinge, exposing the medial talar dome.
- Lesion Management: The lesion is addressed (e.g., OATS procedure).
- Closure: The malleolus is reduced and secured with the previously selected screws.





You Might Also Like


