Osteochondral Fractures of the Knee: Comprehensive Principles and Surgical Management
Key Takeaway
Osteochondral knee fractures frequently occur in adolescents and young adults following acute patellar dislocation or high-energy twisting injuries. Presenting with acute hemarthrosis and mechanical symptoms, these injuries demand a high index of suspicion. While undisplaced pediatric fractures may be managed conservatively, displaced fragments require prompt surgical intervention. Treatment involves either excision of non-viable fragments or anatomical reduction and internal fixation, often combined with medial patellofemoral ligament (MPFL) repair to restore joint congruity and stability.
Introduction to Osteochondral Knee Fractures
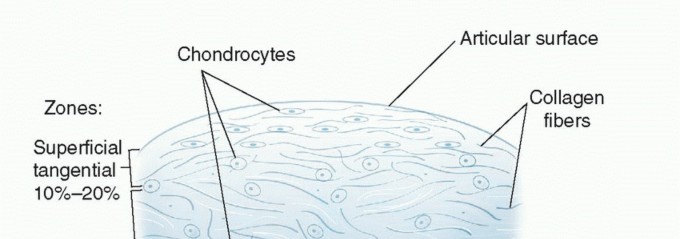
Osteochondral fractures of the knee represent a significant clinical challenge, frequently affecting adolescents and young adults. These injuries involve the separation of a segment of articular cartilage along with its underlying subchondral bone. Historically, the prevalence of these injuries was highlighted in an extensive Army Air Force survey of approximately 186 patients presenting with loose bodies in the knee. In 21 of these cases, the loose bodies were definitively traced to osteochondral fractures originating from either the femoral condyles or the patella.
Rosenberg’s seminal observations further delineated the epidemiology, noting that osteochondral fractures of the lateral femoral condyle are disproportionately common in adolescent boys. He postulated that these fractures are frequently the sequelae of transient patellar dislocations. The shearing force generated during the dislocation and subsequent relocation of the patella avulses a fragment of the condyle, a mechanism virtually identical to that which produces osteochondral fractures of the patella itself.
Prompt diagnosis and meticulous surgical management are paramount. Failure to recognize and appropriately treat these injuries can lead to chronic pain, recurrent effusions, mechanical locking, and early-onset post-traumatic osteoarthritis.
Biomechanics and Mechanism of Injury
Understanding the kinematics of the patellofemoral joint is essential for diagnosing and treating osteochondral fractures. The mechanisms of injury can be broadly categorized into indirect shearing forces (associated with instability) and direct traumatic impaction.
The Dislocation-Relocation Shearing Mechanism
According to Milgram’s classic description, the most common mechanism of injury to the patella and lateral femoral condyle involves a violent, transient lateral subluxation or dislocation of the patella. The sequence of events is as follows:
1. Lateral Translation: The patella is forcefully subluxated over the lateral femoral condyle, often during a twisting motion with the knee in slight flexion and valgus.
2. Articular Scoring: The immense force of the subluxation scores the articular surfaces of both the patella and the femur.
3. Mechanical Catching: The medial border of the patella becomes mechanically caught against the prominent, unyielding edge of the lateral femoral condyle.
4. Violent Relocation: As the powerful quadriceps muscle contracts and snaps the patella back into the trochlear groove, the sharp edge of the femoral condyle acts as a chisel. It shears an osteochondral fragment directly from the inferior and medial edge of the patella, or conversely, the patella shears a fragment from the lateral femoral condyle.
Rotational and Direct Trauma
A secondary mechanism involves forced internal rotation of the femur against a fixed tibia on a weight-bearing, flexed knee. This rotational torque can result in an acute dislocation of the patella and a concomitant fracture of the lateral femoral condyle. Additionally, direct, high-energy blows to the flexed knee (such as dashboard injuries in motor vehicle collisions) can cause focal osteochondral impaction fractures, though these are less common than shearing injuries.
Clinical Pearl: Osteochondral fractures of the patella are estimated to occur in up to 5% of all acute patellar dislocations in adolescents. Always scrutinize the medial patellar facet and the lateral femoral condyle on post-dislocation imaging.
Clinical Evaluation
Patient History and Presentation
Patients typically present following an acute twisting injury or a recognized patellar dislocation, frequently accompanied by a loud, painful "pop" or "snap."
* Acute Hemarthrosis: Rapid onset of swelling within 2 to 12 hours is a hallmark sign, indicating bleeding from the subchondral bone.
* Mechanical Symptoms: Patients may report a sensation of a loose body, catching, or frank locking of the knee joint if the osteochondral fragment becomes incarcerated between the articulating surfaces.
* Medial Tenderness: Exquisite tenderness over the medial retinaculum and the medial patellofemoral ligament (MPFL) is highly indicative of a recent lateral patellar dislocation.
Physical Examination
A comprehensive examination must be performed, though it may be limited by acute pain and effusion.
* Effusion Assessment: A tense hemarthrosis is usually palpable. Aspiration of the joint may reveal lipohaemarthrosis (fat globules suspended in blood), which is pathognomonic for an intra-articular fracture.
* Patellar Apprehension Test: Gentle lateral translation of the patella at 20-30 degrees of knee flexion will elicit severe apprehension and guarding, confirming underlying patellofemoral instability.
* Range of Motion: Extension may be blocked if a large loose body is trapped in the intercondylar notch or the patellofemoral articulation.
Diagnostic Imaging
A high index of suspicion must be maintained, particularly in adolescents and young adults seeking treatment for an acute hemarthrosis. The diagnosis of an osteochondral fracture can be subtle and is easily missed on standard trauma radiographs.
Radiographic Evaluation
High-quality, multi-planar radiographs are mandatory. The standard series should include:
* Anteroposterior (AP) and Lateral Views: May show large fragments or a lipohaemarthrosis (fat-fluid level on a cross-table lateral).
* Skyline / Merchant View: Critical for evaluating the patellofemoral joint space, patellar tilt, and avulsion fractures of the medial patellar facet.
* Tunnel / Notch View: Helpful for visualizing fragments originating from the posterior aspect of the femoral condyles.
* Oblique Views: Can profile the condylar margins to reveal subtle donor site defects.
Advanced Imaging (MRI and CT)
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating acute knee hemarthrosis. MRI exquisitely details the cartilaginous component of the loose body, identifies the exact donor site (often showing classic "kissing" bone bruises on the lateral femoral condyle and medial patella), and evaluates the integrity of the MPFL.
- Computed Tomography (CT): While less sensitive for pure cartilage injuries, a CT scan is invaluable for preoperative planning in cases of large, displaced bony fragments, allowing the surgeon to assess the exact size, morphology, and comminution of the fracture.
Principles of Management
The primary goals of treatment are to restore articular congruity, remove mechanical irritants, and stabilize the patellofemoral joint to prevent recurrent injury.
Conservative Management
Undisplaced osteochondral fractures, particularly in skeletally immature children, can often be treated successfully with conservative methods.
* Protocol: Immobilization in a cylinder cast or rigid knee immobilizer in extension for 3 to 4 weeks, followed by a structured physical therapy program focusing on quadriceps strengthening and gradual restoration of range of motion.
* Monitoring: Serial radiographs are required to ensure the fragment does not displace.
Operative Management
Displaced osteochondral fractures mandate prompt operative intervention to prevent further damage to the articular cartilage and the development of secondary osteoarthritis.
Surgical Warning: Delaying surgery in the presence of a displaced osteochondral fragment can lead to rounding of the fragment edges, swelling of the cartilage, and degradation of the subchondral bone, rendering anatomical reduction and fixation impossible.
Excision vs. Fixation
The decision to excise or fix the fragment depends primarily on its size, location, and the quality of the subchondral bone.
* Excision: Frequently, fragments are too small, highly comminuted, or purely cartilaginous, making technical fixation back into their bed impossible. These fragments should be excised, and the donor bed debrided to stable, vertical margins. Microfracture may be considered for small, full-thickness defects in weight-bearing zones.
* Internal Fixation: Larger fragments (typically >1.5 cm in diameter) with sufficient subchondral bone should be anatomically reduced and stabilized in their native beds.
Surgical Techniques
Arthroscopic Evaluation and Fragment Management
- Diagnostic Arthroscopy: The procedure begins with a thorough diagnostic arthroscopy to locate the loose body, assess the donor site, and evaluate for concurrent injuries (e.g., meniscal tears, ligamentous rupture).
- Fragment Retrieval: The fragment is carefully grasped and extracted through an enlarged portal. It is inspected on the back table to assess its viability and suitability for fixation.
- Bed Preparation: If fixation is planned, the donor crater is debrided of fibrous tissue and hematoma using a curette or motorized shaver to expose bleeding subchondral bone, ensuring a congruent fit.
Open Reduction and Internal Fixation (ORIF) of Osteochondral Fragments
For fragments amenable to fixation, a mini-arthrotomy is often required to achieve perfect anatomical reduction.
1. Approach: A medial or lateral parapatellar mini-arthrotomy is performed directly over the donor site.
2. Reduction: The fragment is keyed back into its bed. Provisional fixation is achieved with smooth Kirschner wires.
3. Fixation: Definitive fixation is typically achieved using headless titanium compression screws, bioabsorbable pins, or chondral darts. The implants must be countersunk below the level of the articular cartilage to prevent scoring of the opposing joint surface.
4. Concurrent Soft Tissue Repair: Surgical treatment of adolescents with osteochondral fractures resulting from acute patellar dislocation must include medial soft tissue repair (MPFL repair or reconstruction) to improve patellar alignment and prevent recurrent dislocation.
Complex Patellar Fractures and Tension Band Wiring
In cases where the osteochondral fracture involves a substantial portion of the patella, or presents as a transverse fracture with distal pole comminution, robust internal fixation is required to counteract the massive tensile forces of the extensor mechanism.
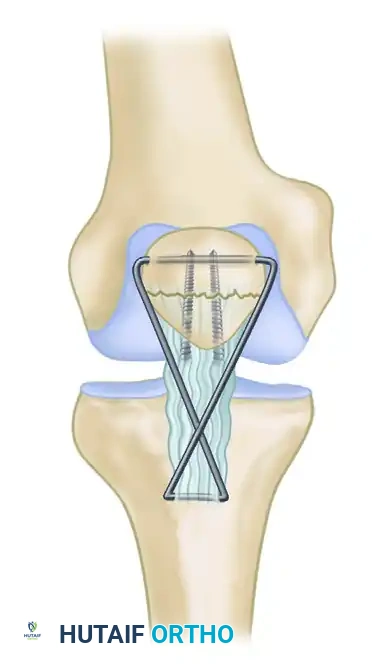
As illustrated in the surgical diagram above, complex patellar fractures can be managed with a modified tension band technique to offload the repair:
1. Anatomical Reduction: The articular surface of the patella is anatomically reduced and provisionally held with reduction forceps.
2. Primary Fixation: Two parallel cannulated screws are placed longitudinally across the fracture site to provide interfragmentary compression.
3. Tension Band Construct: To protect the repair, especially when the distal pole is compromised, a tension band wire or heavy non-absorbable cable is utilized.
4. Tibial Tubercle Anchoring: Two cables are inserted through transverse holes drilled in the tibial tubercle and the proximal pole of the patella.
5. Figure-of-Eight Configuration: The cables are crossed anteriorly to the patellar ligament to form a figure-of-eight and are crimped or twisted to each other. This construct effectively neutralizes the tensile forces of the quadriceps, converting them into compressive forces at the articular surface during knee flexion, thereby allowing for early mobilization.
Postoperative Protocol and Rehabilitation
The postoperative rehabilitation protocol must be carefully tailored to the specific surgical intervention performed (excision vs. fixation) and the security of the soft tissue repair.
Phase 1: Protection and Healing (Weeks 0-4)
- Weight-Bearing: If an osteochondral fragment was fixed in a weight-bearing zone, the patient is typically restricted to toe-touch weight-bearing (TTWB) or non-weight-bearing (NWB) for 4 to 6 weeks. If the fragment was excised or located on the patella, weight-bearing in extension may be permitted earlier.
- Bracing: A hinged knee brace locked in extension is used during ambulation.
- Range of Motion (ROM): Continuous Passive Motion (CPM) or active-assisted ROM is initiated early (0-90 degrees) to promote cartilage nutrition and prevent arthrofibrosis, provided it does not stress the MPFL repair or the fracture fixation.
Phase 2: Progressive Loading (Weeks 4-8)
- Weight-Bearing: Gradual progression to full weight-bearing as tolerated.
- ROM: Progression to full, unrestricted range of motion.
- Strengthening: Initiation of closed-kinetic-chain exercises (e.g., mini-squats, leg presses) to rebuild quadriceps and VMO strength, avoiding deep flexion angles that place excessive shear stress on the patellofemoral joint.
Phase 3: Advanced Strengthening and Return to Play (Weeks 8-16+)
- Proprioception: Advanced balance and proprioceptive training.
- Sport-Specific Drills: Introduction of plyometrics, cutting, and pivoting maneuvers once the patient has achieved 85-90% limb symmetry index (LSI) on functional testing.
- Clearance: Return to competitive sports is typically permitted between 4 to 6 months postoperatively, contingent upon complete radiographic healing of the osteochondral fragment, absence of effusion, and full restoration of dynamic knee stability.
Complications
Despite meticulous surgical technique, complications can arise:
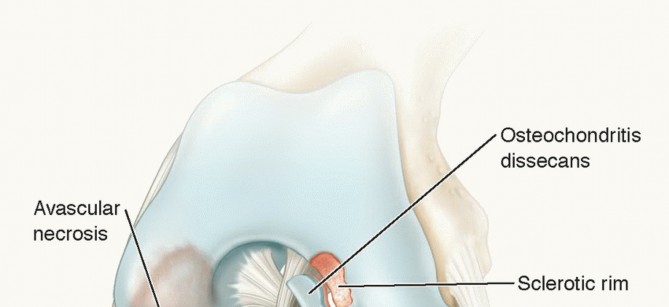
* Nonunion / Avascular Necrosis: The fixed osteochondral fragment may fail to integrate, leading to fragmentation and recurrent loose bodies.
* Arthrofibrosis: Stiffness and loss of flexion are common if early ROM is not instituted.
* Recurrent Instability: Failure to adequately address the underlying MPFL pathology can result in recurrent patellar dislocations and subsequent chondral damage.
* Post-Traumatic Osteoarthritis: Even with anatomical reduction, the initial chondral injury initiates an inflammatory cascade that may predispose the joint to early degenerative changes. Long-term follow-up is essential.
You Might Also Like