Question 51
A 42-year-old woman with a long-standing history of rheumatoid arthritis undergoes total shoulder arthroplasty for persistent pain that has failed to respond to nonsurgical management. Intraoperative radiographs reveal an oblique, minimally displaced fracture of the greater tuberosity. Based on these findings, what is the best course of action?

Explanation
The risk of intraoperative fracture in osteoporotic bone in patients with rheumatoid arthritis is significant. Fractures most often occur during humeral head dislocation and positioning for canal reaming. If the fracture occurs at the greater tuberosity, cerclage suture fixation of the tuberosity fracture with autogenous cancellous bone graft from the resected humeral head is the treatment of choice. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 215-225.
Question 52
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
Explanation
Osteochondritis of the capitellum is characterized by pain, swelling, and limited motion. Catching, clicking, and giving way also can occur. It commonly affects athletes who participate in competitive sports with high stresses, such as pitching or gymnastics. Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
Question 53
The incidence of ipsilateral phrenic nerve blockade after an interscalene block approaches
Explanation
The most common side effect of an interscalene block is ipsilateral phrenic nerve blockade. The phrenic nerve arises chiefly from the fourth cervical ramus (with contributions from the third and fifth) and is the sole motor supply to the diaphragm. Phrenic nerve palsy usually is well tolerated in healthy patients but should be avoided in patients with limited pulmonary function (severe restrictive or obstructive lung disease, myasthenia gravis, or contralateral hemidiaphragmatic dysfunction). The incidence of ipsilateral phrenic nerve blockade afer interscalene block approaches 100%. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14;546-556.
Question 54
What is the most consistent finding regarding glenohumeral kinematics in patients with symptomatic tears of the rotator cuff?
Explanation
Normal glenohumeral kinematics are represented by ball-and-socket modeling when the rotator cuff is intact. This is true for motion that involves more than 30 degrees of abduction. In patients with shoulder pain and symptomatic rotator cuff tears, superior translation occurs with abduction beyond 30 degrees. This is quite evident in massive tears but is seen consistently to a lesser degree with smaller tears. Yamaguchi K, Sher JS, Anderson WK, et al: Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
Question 55
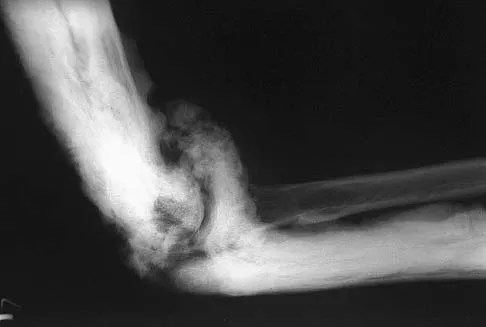
A 28-year-old man sustained numerous injuries in an accident including a dislocation of the elbow and a severe closed head injury that resulted in unconsciousness. The elbow was reduced in the emergency department. After 1 month of rehabilitation, the patient reports pain and stiffness. A radiograph is shown in Figure 23. Management should now consist of

Explanation
In a young individual with a chronic dislocation of the elbow and heterotopic bone formation, the treatment of choice is open reduction, heterotopic bone excision, anterior and posterior capsular releases, and a dynamic hinged fixator to begin protected early postoperative range of motion. It is important to understand that the fixator protects the reconstruction and allows early range of motion, but it does not maintain the reduction and should not be expected to do so. Pin fixation across the elbow delays early motion and is not recommended. Total elbow arthroplasty is not indicated, and ulnohumeral arthroplasty is for a primary arthritic condition. Garland DE, Hanscom DA, Keenan MA, et al: Resection of heterotopic ossification in the adult with head trauma. J Bone Joint Surg Am 1985;67:1261-1269.
Question 56
A 52-year-old man has had right shoulder pain in the deltoid region that increases at night for the past 2 months. He denies any history of trauma. Examination reveals mild tenderness over the greater tuberosity, and the Neer and Hawkins impingement signs are positive. AP and outlet lateral radiographs are shown in Figures 24a and 24b. Initial management should consist of


Explanation
24b The patient has the findings of classic subacromial impingement. Initial management should consist of stretching exercises directed at the posterior capsule and a program of rotator cuff and deltoid strengthening exercises performed below the horizontal in a "safe" plane. The judicious use of subacromial cortisone injections (one or two) may be helpful. Anterior acromioplasty is reserved for patients who have failed to respond to nonsurgical management. Morrison DS, Frogameni AD, Woodworth P: Non-operative treatment of subacromial impingement syndrome. J Bone Joint Surg Am 1997;79:732-737. Neer CS: Impingement lesions. Clin Orthop 1983;173:70-77.
Question 57
A 70-year-old woman is brought to the emergency department with a two-part greater tuberosity fracture with an anterior subcoracoid dislocation. One day after successful closed reduction, examination reveals marked swelling of the involved arm, forearm, and hand, as well as large amounts of "weeping" serous fluid but no obvious lacerations. The fingers are warm and pink, and the pulses are normal distally with good refill. Edema is present. There is no pain with passive and active motion of the elbow, wrist, and fingers. What is the next most appropriate step in management?
Explanation
Although not as common as arterial injury, venous thrombosis secondary to trauma of the subclavian or axillary vein can be problematic; therefore, venous duplex ultrasound scanning is the diagnostic study of choice. Arteriography may not show venous thrombosis in the venous run-off phase. The clinical history does not fit the usual presentation of a compartment syndrome or complex regional pain syndrome.
Question 58
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
Explanation
According to Morgan and associates, a type II SLAP lesion can create or is associated with a superior instability pattern. They suggest that this can exist without a co-existing anteroinferior instability pattern. They reported that repair of the SLAP lesion alone resulted in satisfactory outcomes in 90% of patients and a return to throwing in more than 90% of pitchers. The arthroscopic findings in this patient do not support a diagnosis of anteroinferior laxity or instability; therefore, thermal capsular shift or capsular placation is not necessary. Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565. Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Question 59
With increasing abduction in the scapular plane, maintaining neutral rotation, contact area, and contact pressure per unit area between the humeral head and glenoid follows what pattern if the total load across the joint is held constant?
Explanation
The glenohumeral joint becomes more congruent at higher levels of abduction. As a consequence, contact area increases. As the load is spread more evenly across the joint, contact pressure per unit area decreases as long as the total load across the joint is held constant. Warner JJP, Bowen MK, Deng XH, et al: Articular contact patterns of the normal glenohumeral joint. J Shoulder Elbow Surg 1998;7:381-388.
Question 60
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of



Explanation
26b 26c Open reduction and subscapularis and lesser tuberosity transfer into the defect is the treatment of choice in young individuals who have defects that involve between 20% to 45% of the head. Disimpaction and bone grafting is an option in injuries that are less than 3 weeks old. Closed reduction 2 to 3 months after injury usually is unsuccessful and increases the risk of fracture or neurovascular injury. Total shoulder arthroplasty is reserved for defects of greater than 50% or with associated glenoid surface damage. Hemiarthroplasty should be avoided in young individuals unless 50% or more of the head is involved. Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Question 61
Which of the following ligaments are the primary static restraints to inferior translation of the arm when the shoulder is in 0 degrees of abduction and neutral rotation?
Explanation
Biomechanical ligament sectioning studies have implicated both the superior glenohumeral and coracohumeral ligaments as restraints to inferior translation when the shoulder is in 0 degrees of abduction and neutral rotation. Although there is controversy over the significance of each ligament, both are involved to some degree. The middle glenohumeral ligament is more important in the midranges of abduction, and the inferior ligament is more important at 90 degrees of abduction. The coracoacromial and coracoclavicular ligaments play no role in glenohumeral restraint. Warner JJ, Deng XH, Warren RF, et al: Static capsuloligamentous restraints to superior-inferior translation of the glenohumeral joint. Am J Sports Med 1992;20:675-685.
Question 62
A 44-year-old man who sustained an elbow dislocation 3 months ago now reports pain and restricted elbow motion. Radiographs are shown in Figures 27a and 27b. Management should consist of


Explanation
27b The treatment of choice for an ankylosed chronically dislocated elbow is surgical reduction. Open reduction with application of an external fixator provides excellent results for this complex problem. Radial head arthroplasty is indicated for a radial head fracture that cannot be reconstructed. Attempts at closed reduction will be unsuccessful and should not be attempted in a stiff elbow. In chronic dislocations, direct reinsertion of injured ligaments is not feasible because of soft-tissue contracture. Jupiter J, Ring D: Treatment of unreduced elbow dislocation with hinged external fixation. J Bone Joint Surg Am 2002;84:1630-1635.
Question 63
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?

Explanation
28b The radiographs show nonunion of both the greater and lesser tuberosities. Tuberosity pull-off and nonunion remain among the most common causes of failed humeral head arthroplasty for fracture. Strict attention to securing the tuberosities to each other and to the shaft, and autogenous bone grafting from the excised humeral head will decrease the incidence of pull-off and improve healing rates. Active-assisted range-of-motion and strengthening exercises should be delayed until tuberosity healing is noted radiographically, usually at 6 to 8 weeks postoperatively. Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475. Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation. Phys Ther 1975;55:850-858.
Question 64
Initial postoperative management after repair of an acute rotator cuff tear includes
Explanation
In the immediate postoperative period following repair of an acute rotator cuff tear, passive forward elevation and external rotation should be performed within the safe zone determined at surgery. Early active range of motion (prior to tendon healing), internal rotation behind the back, and resistive exercises increase the risk of rupture of the repair. Iannotti JP: Full-thickness rotator cuff tear: Factors affecting surgical outcome. J Am Acad Orthop Surg 1994;2:87-95.
Question 65
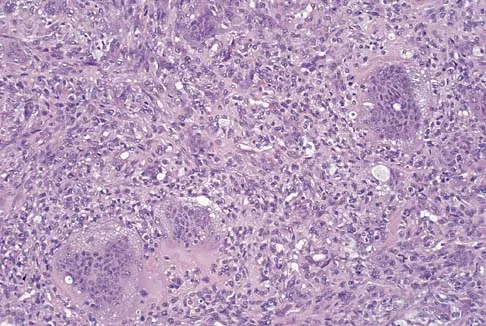
A 34-year-old woman reports constant midlateral arm pain after sustaining minimal trauma to the shoulder. Radiographs and a biopsy specimen are shown in Figures 29a and 29b. What is the most likely diagnosis?

Explanation
29b Eighty percent of giant cell tumors occur in patients older than age 20 years, with the peak incidence in the third decade of life. Most of these tumors are eccentrically located and epiphyseal in location. They are lytic in nature as in this patient. Although named for the hallmarked multinucleated giant cells seen in the lesion, the basic cell type is the spindle-shaped stromal cell. Chondroblastoma is highly cellular and contains large multinucleated giant cells with intercellular chondroid material, some of which is calcified. Chondromyxoid fibroma has chondroid tissue separated by strands of more cellular tissue with occasional multinucleated giant cells. Desmoplastic fibroma is characterized by poorly cellular fibrous tissue, and lymphoma is highly cellular with characteristic round cells. Campanacci M, Baldini N, Boriani S, et al: Giant cell tumor of bone. J Bone Joint Surg Am 1987;69:106-114.
Question 66
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
In the thrower's elbow, ulnar neuritis is felt to result from both chronic compression and traction on the nerve that occurs during the throwing motion. Occasionally, subluxation of the nerve also can lead to symptoms. If nonsurgical management fails to provide relief, transposition of the nerve to an anterior subcutaneous location is the surgical procedure of choice. The nerve is held in its new position by one or two fascial slings created from the fascia of the common flexor origin. Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Question 67
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
The superior ulnar collateral, inferior ulnar collateral, and posterior ulnar recurrent arteries provide consistent vascular supply to the ulnar nerve. This supply is segmental in nature. No identifiable direct anastomosis is seen between the superior ulnar collateral and the posterior ulnar recurrent arteries. The inferior ulnar collateral artery provides the only direct vascularization to the nerve and is located in the region just proximal to the cubital tunnel. The segmental nature of the blood supply to the ulnar nerve underscores the importance of its preservation during transposition.
Question 68
A 56-year-old man underwent right total shoulder arthroplasty 2 months ago. Recently while reaching with his shoulder in a flexed and adducted position, he noted shoulder pain and afterwards he could not externally rotate his arm. An axillary radiograph is shown in Figure 30. What is the most likely cause of this problem?

Explanation
Anteversion of the humeral component may result in anterior instability of the component. Posterior instability after total shoulder arthroplasty is usually the result of some combination of the following factors: untreated anterior soft-tissue contractures, excessive posterior capsular laxity, and excessive retroversion of the humeral and/or glenoid components. Cofield RH, Edgerton BC: Total shoulder arthroplasty: Complications and revision surgery. Instr Course Lect 1990;39:449-462.
Question 69
A 70-year-old man seen in the emergency department has had left shoulder pain and a fever of 101.5 degrees F (38.6 degrees C) for the past 3 days. He denies any history of trauma. Examination reveals tenderness anterosuperiorly and at the posterior glenohumeral joint line. He has very limited range of motion (passive and active). Laboratory studies show a WBC count of 12,000/mm3 and an erythrocyte sedimentation rate of 48 mm/h. Initial management should consist of
Explanation
It appears that the patient has septic arthritis of the glenohumeral joint; therefore, initial management should consist of aspiration of the glenohumeral joint and subacromial space separately, followed by Gram stain and culture of the fluid. Based on the findings, broad-spectrum IV antibiotics should be started. If the diagnosis of septic arthritis is confirmed, then arthroscopic or open surgical drainage usually is indicated. Sawyer JR, Esterhai JL Jr: Shoulder infections, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997.
Question 70
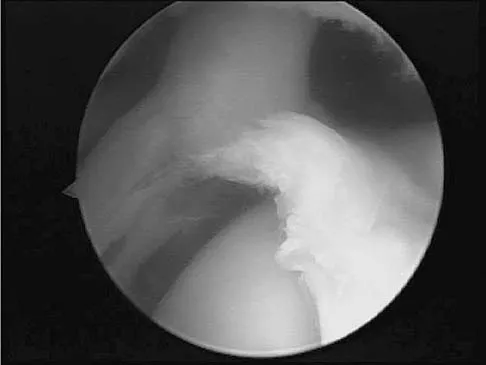
A 40-year-old man who is an avid weight lifter has had chronic pain in the proximal anterior shoulder for the past year. He denies any history of trauma. Examination reveals tenderness at the intertubercular groove, a positive speed test, and a positive Neer impingement sign. Nonsurgical management has failed to provide relief, and he is now considering surgery. Arthroscopic findings in the glenohumeral joint are shown in Figure 31. Based on these findings, treatment should consist of

Explanation
The arthroscopic image shows a tear through more than 50% of the biceps tendon; therefore, treatment should consist of tenodesis or tenotomy of the tendon. However, because this patient is relatively young and active, the treatment of choice is tenodesis of the biceps tendon. Sethi N, Wright R, Yamaguchi K: Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-654. Eakin CL, Faber KJ, Hawkins RJ, et al: Biceps tendon disorders in athletes. J Am Acad Orthop Surg 1999;7:300-310.
Question 71
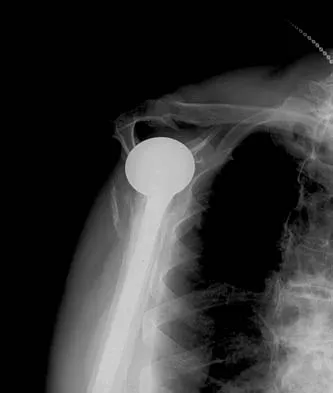
A 59-year-old man reports moderate shoulder pain and very restricted range of motion after undergoing humeral arthroplasty for osteoarthritis 1 year ago. An AP radiograph is shown in Figure 32. Management should now consist of

Explanation
The radiograph reveals that an insufficient amount of the proximal humerus was excised in the index procedure, resulting in malalignment of the humeral component, overstuffing of the glenohumeral joint, and glenoid arthritis. It is unlikely that physical therapy or soft-tissue releases alone will be adequate. Revision of the humeral component, recutting of the proximal humerus to allow a more anatomic alignment of the humeral component, appropriate soft-tissue releases, and glenoid arthroplasty will offer the best chance of improvement in this difficult situation. Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties. Clin Orthop 1982;170:189-195.
Question 72
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
The beach chair position may cause sudden hypotension and bradycardia as a result of the Bezold-Jarisch reflex. This reflex occurs when venous pooling and increased sympathetic tone induce a low-volume, hypercontractile ventricle, resulting in activation of the parasympathetic nervous system and sympathetic withdrawal. The reported incidence of this phenomenon associated with the sitting position is between 13% to 24%. Left untreated, the result may be cardiac arrest. Pneumothorax or central nervous system toxicity after interscalene block is rare and has an incidence of less than 0.2%. Laryngeal nerve block associated with interscalene nerve block can occur but usually results in hoarseness secondary to ipsilateral vocal cord palsy. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Question 73
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
In a cadaver ligament sectioning study, the posterior capsular ligament was considered the most important structure for anterior-posterior stability of the sternoclavicular joint. The anterior capsular ligament also helps prevent anterior displacement but not to the same degree as the posterior ligament. The interclavicular ligament provides little support for anteroposterior translation. Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 74
A 35-year-old man has atraumatic painless limited elbow motion. Radiographs are shown in Figures 33a and 33b. What is the most likely diagnosis?

Explanation
33b Based on the radiographic findings, the patient has melorheostosis, a rare, benign connective tissue disorder that is characterized by a cortical thickening of bone. It produces a "dripping candle wax" appearance with dense hyperostosis that flows along the cortex. Ectopic bone formation is a consideration but is associated with injuries or burns. Bone infarcts produce intraosseous sclerosis typically affecting the distal femur with the "smoke up chimney" appearance. Infection is always a consideration but typically does not have the linear osteitis seen in melorheostosis. Juxacortical chondroma is a benign cartilage growth that arises from the capsule and may involve the underlying cortical bone but rarely the medullary canal. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 75
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
Nearly all approaches to shoulder arthroplasty require detachment of the subscapularis tendon from the humerus and subsequent repair. Healing of this tenotomy is one of the limiting factors in postoperative recovery. Failure of the tenotomy repair must be recognized and treated early with repeat repair or pectoralis muscle transfer for optimal results. Failure of the subscapularis is diagnosed clinically as excessive external rotation and weakness, especially in the lift-off or belly press position. Muscle testing can be difficult in the postoperative period and may not be possible to assess in those positions. Although MRI might be useful to confirm the diagnosis, studies may be limited by artifact. CT or electromyography would not be diagnostic. Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Finish Exam?
You cannot change answers after submitting.
