Question 76
A 30-year-old woman sustains a transverse amputation of the distal phalanx of the index finger, leaving exposed bone. What is the most appropriate management of the soft-tissue defect?
Explanation
V-Y advancement flaps are ideal for fingertip amputations that are transverse or dorsal oblique in nature. Healing by secondary intention is contraindicated with exposed bone. Shortening of exposed bone to allow primary skin closure is a possible alternative, as long as significant shortening of the index finger is avoided. A Moberg flap is useful only for distal amputations of the thumb. The first dorsal metacarpal artery-island pedicled flap uses tissue from the dorsum of the proximal index finger, and is typically used to resurface defects of the thumb. Fassler PR: Fingertip injuries: Evaluation and treatment. J Am Acad Orthop Surg 1996;4:84-92.
Question 77
What is the best approach to reduce and stabilize a displaced volar lunate facet fracture of the wrist?
Explanation
A volar lunate fragment of a distal radial fracture is considered a critical component to overall joint stability and function. Obtaining a reduction is difficult through a standard volar approach to the radius between the flexor carpi radialis and radial artery. Visualization and reduction of the ulnar volar facet is not possible from this approach. An extended carpal tunnel incision provides access to the entire articular surface, except for the distal radial styloid component. Hanel DP, Jones MD, Trumble TE: Wrist fractures. Orthop Clin North Am 2002;33:35-57.
Question 78
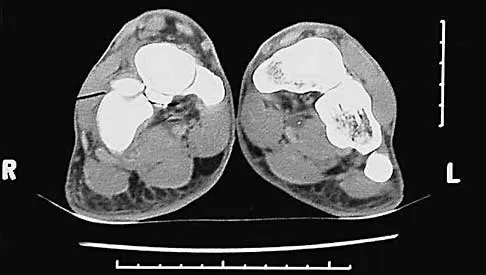
A 17-year-old man sustained a 5-mm laceration on the lateral aspect of the hindfoot while working on a farm. Examination in the emergency department revealed no fractures. Twenty-four hours later, he returns to the emergency department with increasing foot pain. Thin brown drainage is seen emanating from the wound. He has a temperature of 102.0 degrees F (38.9 degrees C), a pulse rate of 120, and a blood pressure of 80/40 mm Hg. Examination of the foot reveals diffuse swelling, ecchymosis, tenderness, and crepitus with palpation. Current radiographs are shown in Figures 40a and 40b. Management should now consist of


Explanation
40b The mechanism and environment in which the injury occurred, the clinical picture, and the radiographic findings of gas in the tissues suggest an anaerobic Gram-positive bacterial infection. This can be a life- and limb-threatening infection. Treatment should consist of wide debridement of all devitalized tissue, and intravenous antibiotics should be started. Wounds should be left open to allow bacterial effluent and increase oxygen tension in the wound. Hyperbaric oxygen may be used as an adjuvant but is no substitute for debridement. Pellegrini VD, Reid JS, Evarts CM: Complications, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 1, pp 458-463.
Question 79
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of

Explanation
41b Open reduction and internal fixation of distal humeral fractures in elderly patients often fails. These fractures characteristically have a very small distal segment and poor bone quality, resulting in failure of fixation and nonunion. Nonunion is often painful and functionally debilitating. Total elbow arthroplasty provides good results when used for distal humeral fractures in elderly patients with osteopenic bone and fracture patterns thought to be irreconstructable. Long arm casting may result in union, but the resulting stiffness is unacceptable for an active patient. Elbow arthrodesis has few indications. A sling and range-of-motion exercises will often result in a painful and debilitating nonunion at the fracture site. Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Question 80
A 35-year-old man sustains a closed Monteggia fracture. Examination reveals that sensation, vascular status, and finger flexion are normal. When he extends his wrist, it deviates radially, and he is unable to extend his fingers or thumb. After reduction of the fracture, what is the next step in treatment for the extensor deficits of the thumb and fingers?
Explanation
The posterior interosseous nerve is located adjacent to the radial neck, placing it at risk for a traction injury with a dislocation of the proximal radius. The typical neurapraxia that results can be expected to resolve with observation within the first 6 to 12 weeks. If recovery is not clinically evident by 3 months, neurophysiologic studies are indicated. Jessing P: Monteggia lesions and their complicating nerve damage. Acta Orthop Scand 1975;46:601-609.
Question 81
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0 degrees F (35 degrees C). What is the recommended treatment of the femoral fracture at this time?
Explanation
This is a "borderline trauma" patient where serious consideration for damage control orthopaedic surgery is required. His prolonged hypotension, abdominal injury, and chest injury put him at higher risk for serious postinjury complications. Further surgery, such as definitive fracture fixation, adds metabolic load and injury to his system. It is prudent to consider femoral fracture stabilization with an external fixator until he is physiologically recovered as evidenced by a normal base excess and/or lactate acid levels, as well as all other parameters of resuscitation. A borderline patient has been described as polytrauma with an ISS > 20 and thoracic trauma (AIS > 2); polytrauma and abdominal/pelvic trauma (Moore > 3) and hemodynamic shock (initial BP < 90 mm Hg); ISS > 40; bilateral lung contusions on radiographs; initial mean pulmonary arterial pressure > 24 mm Hg; pulmonary artery pressure increase during intramedullary nailing > 6 mm Hg. Factors that worsen the situation following surgery include multiple long bones and truncal injury (AIS > 2), estimated surgery time of more than 6 hours, arterial injury and hemodynamic instability, and exaggerated inflammatory response (eg, Il-6 > 800 pg/mL). It is incumbent on the orthopaedic surgeon who is a member of the trauma team to make sure that he or she is aware of these factors and guides the team to the best patient care. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Question 82
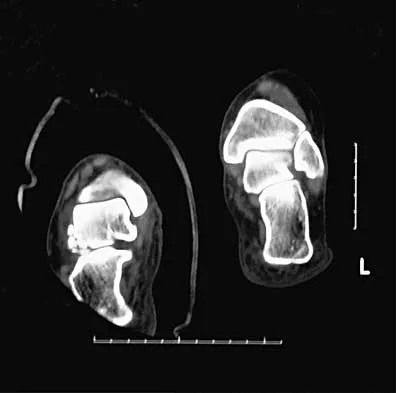
A 10-year-old girl has a right elbow deformity that is the result of trauma 5 years ago. She has no pain despite the arm deformity. The radiographs in Figures 42a and 42b show complete healing. This radiographic appearance demonstrates what complication?


Explanation
42b Cubitus varus is a common complication of displaced supracondylar humeral fractures that are treated with closed reduction and cast immobilization. Treatment with closed reduction and percutaneous pinning decreases the incidence of this complication. Cubitus varus also can occur in minimally displaced fractures when unrecognized collapse of the medial column of the distal humerus is not corrected with manipulation. This can be detected on physical examination of the carrying angle or on radiographs measuring Baumann's angle, both in comparison to the opposite side. Cubitus varus may result in unacceptable cosmesis and may predispose the patient to fractures of the lateral condyle. The lateral radiograph demonstrates the crescent sign from overlap of the distal humerus with the olecranon seen in patients with cubitus varus. Patients with growth arrest to the medial trochlear physis would have atrophy of the trochlea on radiographs. Flynn JM, Sarwark JF, Waters PM, et al: The surgical management of pediatric fractures of the upper extremity. Instr Course Lect 2003;52:635-45. Papandrea R, Waters PM: Posttraumatic reconstruction of the elbow in the pediatric patient. Clin Orthop 2000;370:115-126.
Question 83
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?


Explanation
43b The patient has a volar displaced two-part intra-articular distal radial fracture-dislocation of the wrist. Although a closed reduction is usually easily obtained, it is very difficult to maintain the reduction without internal fixation. The approach is determined by the direction of the dislocation, in this case volar. Stabilization with a buttress plate neutralizes the axial loading forces on the fractured fragment. A dorsal placed angular stable plate will not provide this buttress effect and will make the reduction difficult.
Question 84
A 26-year-old man was thrown from a car and sustained the injury seen in Figures 44a and 44b. Nonsurgical management of this injury is recommended. Which of the following factors increases the risk of nonunion?


Explanation
44b The patient has a displaced comminuted clavicle middle one third fracture from a high-energy mechanism. Recent literature on high-energy clavicular fractures suggests a higher rate of nonunion than previously reported. A nonunion rate of 30% has been reported by Hill and associates when the fracture fragments are displaced more than 1.5 cm. In addition, several patients had neurologic symptoms related to the injury. Robinson and associates reported an increased risk of nonunion in women, elderly patients, comminuted fractures, and injuries with a lack of cortical contact. Hill JM, McGuire MH, Crosby LA: Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-539. Wick M, Muller EJ, Kollig E: Midshaft fractures of the clavicle with a shortening of more than 2 cm predispose to nonunion. Arch Orthop Trauma Surg 2001;121:207-211.
Question 85
A 13-year-old girl was riding on an all-terrain vehicle when the driver struck a tree. She sustained the injury shown in Figures 45a through 45d. This injury is best described as what type of acetabular fracture pattern?


Explanation
45b 45c 45d The fracture is a both-column fracture in the Judet/Letournel classification and a C3 in the AO classification. There is extension into the sacroiliac joint along the pelvic brim and comminution along the posterior column above the sciatic notch. Both the anterior and posterior columns are separately broken and displaced. However, the defining feature of a both-column pattern, as seen in this patient, is that all articular fragments are on fracture fragments and no joint surface is left intact to the axial skeleton above. The use of three-dimensional images makes it easier to view the location of the fracture fragments and the amount and direction of displacement. Helfet DL, Beck M, Gautier E, et al: Surgical techniques for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 533-603. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Question 86
A woman injures the metacarpophalangeal (MCP) joint of her thumb while skiing. Examination reveals tenderness along the ulnar aspect of the MCP joint. Radially directed stress of the joint in full extension produces 5 degrees of angulation. When the MCP joint is flexed 30 degrees, a radially directed stress produces 45 degrees of angulation. Radiographs are otherwise normal. Management should consist of
Explanation
Injuries to the ulnar collateral ligament of the MCP joint of the thumb commonly occur in recreational skiers. Historically, this injury has been referred to as "gamekeeper's thumb." The ligament consists of the proper collateral ligament and the more volar accessory collateral ligament. In extension, the accessory ligament is taut, and in flexion, the proper ligament is taut. For a complete tear of the ligament complex to occur, there must be laxity in full extension. Incomplete tears respond well to thumb spica splinting or casting for 2 to 3 weeks and gradual resumption of range of motion. Prolonged immobilization of incomplete injuries leads to higher rates of MCP joint stiffness. Stener B: Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1971;44:869.
Question 87
A 37-year-old laborer falls 12 feet and sustains a comminuted tibial plafond fracture. Three years after treatment using standard techniques, what will be the most likely outcome?
Explanation
Two recent studies by Pollak and associates and Marsh and associates have focused on function after high-energy tibial plafond fractures. Findings are unfavorable even when anatomic reduction is performed in the best centers and patients are provided excellent rehabilitation. Function improves up to 2 years after injury, but even basic walking skills remain adversely affected. Virtually all patients have long-term adverse general health effects compared to their gender and age-matched peers. Posttraumatic degenerative arthritis is present in most ankles. Patients should be told early about the long-term prognosis, and early vocational/psychological counseling should be given. Despite these adverse outcomes, only a minority of patients require fusion or arthroplasty. Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 88
A 45-year-old woman sustains an injury to her lower leg. Examination reveals that there is a deformity with no neurologic or vascular problems. The skin is intact. Radiographs are shown in Figures 46a and 46b. Which of the following factors would make closed management the least appropriate choice for this injury?


Explanation
46b All the factors listed, with the exception of an ipsilateral femoral fracture, are representative of a low-energy stable tibial shaft fracture that will do well with closed reduction and immobilization in a long leg cast, followed by weight bearing as tolerated and then a functional brace or patellar tendon bearing cast until union is achieved. Shortening will not increase from that seen on these initial radiographs. The spiral fracture provides a broad surface for healing, and the fibular fracture at another level indicates a stable soft-tissue envelope which, with the immobilization device, will stabilize the fracture reduction. An ipsilateral femoral fracture is a strong indication to surgically stabilize both fractures. Trafton PG: Tibial shaft fractures, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 2153-2169.
Question 89
Which of the following medications may have a negative effect on bone healing following fracture?
Explanation
Nonsteroidal anti-inflammatory drugs that are COX-1 primary inhibitors have been shown in animal studies to delay or inhibit fracture healing. COX-2 inhibitors also delay healing but to a lesser extent than COX-1 inhibitors. The other medications listed do not alter fracture callus formation. Gerstenfeld LC, Thiede M, Seibert K, et al: Differential inhibition of fracture healing by non-selective and cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs. J Orthop Res 2003;21:670-675.
Question 90
A 16-year-old boy has abdominal and back pain after being involved in a high-velocity head-on motor vehicle accident. He was restrained in the rear of the automobile by a lap belt only. A radiograph and CT scan are shown in Figure 47. The patient has no other injuries. Optimal management should include
Explanation
Pediatric bony Chance fractures occur following severe flexion injuries as seen after motor vehicle accidents with lap belt restraints. There is a high rate of associated intra-abdominal injuries. In the absence of associated injuries, these fractures are best treated with immobilization. Bed rest is not necessary. Surgical fixation usually is not needed. Surgical stabilization and two-level fusion may be indicated in select individuals with progressive kyphosis of more than 25 degrees or other conditions that preclude cast or brace immobilization. Greenwald TA, Mann DC: Pediatric seatbelt injuries: Diagnosis and treatment of lumbar flexion-distraction injuries. Paraplegia 1994;32:743-751. Glassman SD, Johnson JR, Holt RT: Seatbelt injuries in children. J Trauma 1992;33:882-886.
Question 91
What inflammatory mediator has been most closely associated with the magnitude of the systemic inflammatory response to trauma and with the development of multiple organ dysfunction syndrome (MODS)?
Explanation
Multiple cytokines (inflammatory mediators) are released following trauma, and their levels can be measured in serum. Persistent elevated levels of IL-6 (> 800 pg/mL) indicate an exaggerated systemic inflammatory response to trauma and have been associated with the development of MODS. Recent work has shown that extensive surgical procedures should be avoided when IL-6 levels remain elevated to prevent the precipitation of MODS. In the future, it is likely that this mediator and possibly others will be used to determine timing and techniques of future treatment. Patrick DA, Moore FA, Moore EE, et al: Jack A. Barney Resident Research Award winner: The inflammatory profile of interleukin-6, interleukin-8, and soluble intercellular adhesion molecule-1 in postinjury multiple organ failure. Am J Surg 1996;172:425-429. Pape HC, van Griesven M, Rice J, et al: Major secondary surgery in blunt trauma patients and perioperative cytokine liberation: Determination of the clinical relevance of biochemical markers. J Trauma 2001;50:989-1000.
Question 92
An 8-year-old girl sustained a displaced fracture at the base of the femoral neck in a motor vehicle accident. Management should consist of
Explanation
Pediatric intracapsular hip fractures are challenging because of the high rates of complications, including osteonecrosis and varus malunion. These patients should be treated as emergencies. Principles of treatment include anatomic reduction with internal fixation. Screw fixation short of the physis is preferred and may need to be supplemented with spica cast immobilization. Fixation may be achieved with smooth pins across the physis when little metaphyseal bone is available. Fixation across the physis with threaded screws is acceptable only when the patient is close to skeletal maturity. Pediatric hip screws are appropriate if immediately available. Emergent open reduction, capsulotomy, or joint aspiration may decrease the rate of osteonecrosis. Cheng JC, Tang N: Decompression and stable internal fixation of femoral neck fractures in children can affect the outcome. J Pediatr Orthop 1999;19:338-343. Azouz EM, Karamitsos C, Reed MH, et al: Types and complications of femoral neck fractures in children. Pediatr Radiol 1993;23:415-420. Song KS, Kim YS, Sohn SW, et al: Arthrotomy and open reduction of the displaced fracture of the femoral neck in children. J Pediatr Orthop B 2001;10:205-210.
Question 93
The plate seen in Figure 48a was applied to the fracture seen in Figure 48b, and is functioning in what capacity?


Explanation
48b A Weber type B ankle fracture occurs with a supination external rotation mechanism of injury. The fibula generally fails with a spiral fracture pattern. The lag screws provide compression, and the plate acts to neutralize rotational and angular bending forces. A buttress plate resists vertical shear forces. A tension band is used over areas that may fail in tension, such as an olecranon fracture. Compression is provided by the lag screws, and distraction is again resisted by the lag screws.
Question 94
Which of the following findings is considered the strongest indication for surgical treatment of a mallet fracture of the distal phalanx?
Explanation
The majority of mallet fractures can be treated nonsurgically with a distal interphalangeal joint extension splint. Excellent results can be obtained in most patients with splinting alone. The fragment size, amount of displacement, and degree of articular incongruity usually do not affect final outcome, as long as the joint is reduced. Surgical fixation takes on several forms but is fraught with complications including skin/wound problems, loss of fixation, nonunion, and stiffness of the distal interphalangeal joint. Volar subluxation of the distal phalanx remains the primary indication for surgical treatment. Green DP, Butler TE Jr: Fractures and dislocations in the hand, in Rockwood CA, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 621-623.
Question 95
A 20-year-old woman sustained the closed injury shown in Figures 49a and 49b in a motor vehicle accident. Examination reveals that this is an isolated injury; however, she has a complete radial nerve palsy. Management should consist of


Explanation
49b Lacerated radial nerves are associated with open humeral fractures. All open humeral fractures with radial nerve palsy should be managed with radial nerve exploration and skeletal stabilization. Closed humeral fractures with associated radial nerve palsy usually have an intact nerve with neurapraxia. Most of these patients recover without surgical treatment. If the patient has multiple injuries, skeletal stabilization may be indicated to improve mobilization. For an isolated closed humeral fracture with a radial nerve palsy, the treatment of choice is splinting for 1 to 2 weeks, followed by a humeral fracture brace. Ring D, Chin K, Jupiter JB: Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004;29:144-147.
Question 96
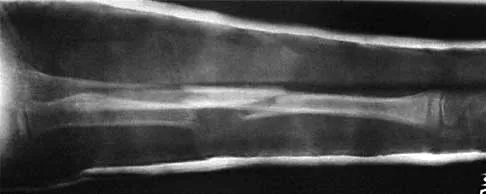
The fracture shown in Figure 50 is most reliably treated with what form of fixation?

Explanation
The radiograph shows a comminuted proximal ulnar fracture. The most reliable fixation is a posterior plate, acting as a tension band plate. The fracture involves the proximal shaft of the ulna; therefore, a 3.5-mm compression plate or one of similar size should be used to provide adequate stability. Kirschner wires and tension band wires do not provide axial stability of the comminution of the ulna. Compression screws alone will most likely fail and will not provide axial rotational stability to the construct. A medial plate will not resist the distraction forces across this fracture. McKee MD, Seiler JG, Jupiter JB: The application of the limited contact dynamic compression plate in the upper extremity: An analysis of 114 consecutive cases. Injury 1995;26:661-666.
Question 97
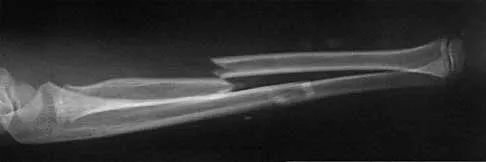
A man sustained the injury shown in Figures 51a and 51b. He underwent closed reduction of the radial head dislocation and open reduction and internal fixation of the ulnar fracture. What is the most common cause of persistent radial head subluxation?


Explanation
51b The radiographs reveal a Monteggia injury, with a proximal ulnar shaft fracture and a radial head dislocation. Treatment involves open reduction and internal fixation of the ulnar fracture. With correct reduction of the ulna, the radial head is reducible and remains stable, despite an obvious soft-tissue injury around the elbow. Problems with persistent radial head subluxation are almost always attributed to malreduction of the ulnar fracture. Rare causes of persistent radial head subluxation are interposition of soft tissues in the joint and lateral ligamentous injuries. Jupiter JB, Kellam JF: Diaphyseal fractures of the forearm, in Browner B, Jupiter J, Levine A, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1992, pp 1421-1454.
Question 98
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Explanation
A widened medial clear space indicates instability caused by an associated tear of the deltoid ligament; therefore, nonsurgical management is not warranted. Weber type B distal fibular fractures without a deltoid tear have a medial clear space of < 4 mm, even under stress, and may be successfully treated nonsurgically. The presence of medial hindfoot ecchymosis and medial ankle tenderness is not fully indicative of medial soft-tissue instability; however, these findings may indicate a deltoid injury and should raise suspicion of an unstable fracture injury pattern. Stress testing is necessary to demonstrate the presence or absence of instability. A small amount of comminution is also cause for increased suspicion of an unstable pattern; however, it is not a direct contraindication when considering nonsurgical management. Two millimeters of fibular displacement without lateral shift of the talus is an acceptable position when considering nonsurgical management of Weber type B distal fibular fractures. Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
Question 99
Locked plating techniques have been shown to have biomechanical advantages over standard plating in which of the following scenarios?
Explanation
Locked plating is becoming more common. Some biomechanical data comparing locked plating to standard plating have been reported for osteoporotic distal femoral fractures and humeral shaft fractures. Significant differences were seen mainly for osteoporotic fractures without cortical contact. Not all osteoporotic fractures and all comminuted fractures have been shown to demonstrate significant mechanical improvement with locked plating compared to standard plating. Spiral fractures often can be repaired with a lag screw, obtaining adequate cortical contact. Osteoporotic fractures with a torsion mode of failure failed earlier with locked plating systems than with standard plating systems. Zlowodzki M, Williamson S, Cole PA, et al: Biomechanical evaluation of the less invasive stabilization system, angled blade plate, and retrograde intramedullary nail for the internal fixation of distal femur fractures. J Orthop Trauma 2004;18:494-502.
Question 100
A 25-year-old man sustained a head injury after being ejected from his car. Examination reveals a Glasgow Coma Scale score of 7 and a swollen right knee. Clinical examination shows that the knee is very unstable, suggesting tears of the medial collateral and anterior and posterior cruciate ligaments, as well as the posterior lateral corner. What is the most appropriate first step to rule out a vascular injury?
Explanation
A knee dislocation carries the potential for an arterial injury and has always brought up the question of need for arteriography to rule out this limb-threatening injury. However, arteriography has an inherent complication rate that may compromise the general care of the patient. In over 240 published cases with documented knee dislocations that were evaluated for vascular injury by physical examination (without imaging studies), not a single missed injury was reported, for a 100% negative predictive value (0% false-negative rate). This degree of accuracy at excluding major vascular injury is unsurpassed by the results obtained with arteriography but with no risk involved and a marked savings in time, equipment, and costs. Therefore, the most appropriate first step to rule out vascular injury is examination of the pedal pulses. If there is any doubt about an arterial injury, another option is the ankle-brachial index (ABI). If the ABI is greater than 0.9, the chance of arterial injury is again nonexistent. However, a positive physical examination or an ABI of less than 0.9 is not 100% predictive of an arterial injury; therefore, arteriography is recommended. Miranda FE, Dennis JW, Veldenz HC, et al: Confirmation of the safety and accuracy of physical examination in the evaluation of knee dislocation for injury of the popliteal artery: A prospective study. J Trauma 2002;52:247-252.
Finish Exam?
You cannot change answers after submitting.
