Question 51
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of


Explanation
Displaced clavicular fractures lateral to the coracoid process (Neer type II and III) are best managed nonsurgically with sling immobilization and physical therapy, starting with pendulum exercises and progressing to active-assisted exercises when comfortable. Supervised therapy should be performed for 3 months or until full painless motion is achieved. In one study by Robinson and Cairns, this form of treatment provided patients with a 86% chance of avoiding a secondary reconstructive procedure. Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Question 52
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
With soft-tissue loss, local or free flap coverage may be necessary to treat exposed tendon and bone. However, a vacuum-assisted closure device is a good temporizing dressing. It prevents external contamination, reduces edema around the wound, increases oxygen tension in the wound, and promotes the formation of granulation tissue. The use of this negative pressure device has been described in both acute traumatic and in chronic wound scenarios. If sufficient granulation tissue forms, closure may be by split graft, avoiding a more complex coverage procedure. Immediate skin grafting over the exposed anterior tibial tendon and tibia would have a low likelihood of success. Dressing changes with sulfasalazine may be beneficial in a burn wound to assist with removal of skin slough; however, in a granulating wound, the material may be toxic to early epithelialization. Xenograft is a foreign body and should not be applied to an acute contaminated open wound. Historically, a cross-leg flap was a treatment alternative for lower extremity soft-tissue loss; however, its current applications are extremely limited. Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Question 53
The humeral nonunion shown in Figure 27 is most likely to unite when using what method of treatment?

Explanation
The radiograph shows an atrophic nonunion of the humeral shaft. The management of humeral nonunions has been studied with compression plates and bone graft, as well as intramedullary nailing and bone graft. Compression plating with bone graft results in the highest rate of union. Compression plating by itself is not adequate, given the bone loss and lack of callous in this nonunion. Pulsed electromagnetic fields is a viable option for hypertrophic nonunions where there is inherent stability. Intramedullary nailing does not provide as much compression and stability as that achieved with compression plating. Pugh DM, McKee MD: Advances in the management of humeral nonunion. J Am Acad Orthop Surg 2003;11:48-59.
Question 54
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
Most patients lose elbow range of motion after open reduction and internal fixation of a distal humeral fracture. Ulnar nerve dysfunction, nonunion, and infection all occur less commonly. Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
Question 55
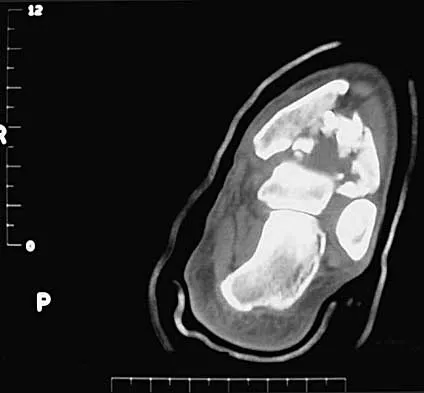
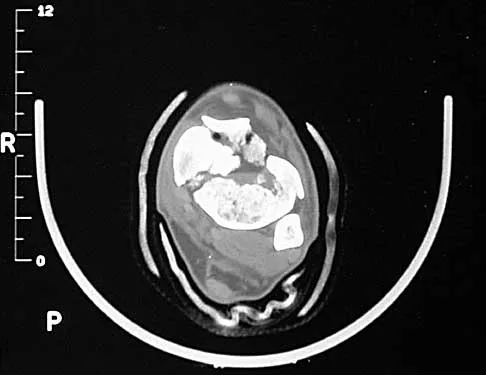
The radiographs and CT scan seen in Figures 28a through 28d reveal what type of acetabular fracture pattern?



Explanation
28b 28c 28d The AP, obturator oblique, and iliac oblique views of the pelvis reveal a fracture that disrupts the iliopectineal and ilioischial lines, indicating a fracture that involves both anterior and posterior columns. However, it does not have the other features of anterior or posterior column fracture patterns. A displaced posterior wall fracture is also present, best seen on the obturator oblique view. The anterior to posterior directed fracture line on the CT scan indicates a transverse fracture; therefore, the patient has a transverse with posterior wall fracture pattern. A T-type fracture would be similar but would have a break into the obturator ring. Tile M: Describing the injury: Classification of acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 427-475.
Question 56
A 26-year-old man sustained an isolated injury to his left hip joint in a motor vehicle accident. Closed reduction was performed, and the postreduction radiograph is shown in Figure 29. Management should now consist of
Explanation
The patient has a posterior fracture-dislocation of the hip and following reduction, an incarcerated fragment of bone resulted in an incongruent reduction. Whereas expedient removal of the fragment is required to limit articular cartilage damage, this situation is not an emergency and the procedure may be performed when the appropriate surgical team is available and the patient is stabilized. Skeletal traction through either the femur or tibia may relieve some pressure on the joint and prevent articular damage. Nonsurgical care for incarcerated fragments is contraindicated. Tile M, Olson SA: Decision making: Non operative and operative indications for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 496-532.
Question 57
A 35-year-old man is brought to the emergency department following a motorcycle accident. He is breathing spontaneously and has a systolic blood pressure of 80 mm Hg, a pulse rate of 120/min, and a temperature of 98.6 degrees F (37 degrees C). Examination suggests an unstable pelvic fracture; AP radiographs confirm an open book injury with vertical displacement on the left side. Ultrasound evaluation of the abdomen is negative. Despite administration of 4 L of normal saline solution, he still has a systolic pressure of 90 mm Hg and a pulse rate of 110. Urine output has been about 20 mL since arrival 35 minutes ago. What is the next best course of action?
Explanation
The patient is at risk for a pelvic vascular injury and major hemorrhage. This type of complication of pelvic trauma is highest in motorcyclists. Once it is recognized that the pelvic ring has opened, it is important to close that ring to tamponade any venous bleeding with a pelvic binder and to add a skeletal traction pin to the limb on the involved side. This will correct any translational displacement. The noninvasive pelvic binders or sheets are easy to apply and are very effective. They do not compromise future care and allow the surgeons access to the abdomen. External fixation or pelvic resuscitation clamps require a certain amount of skill to apply and are not always available. If the pelvic stabilization does not improve the hemodynamic parameters in 10 to 15 minutes, angiography is necessary.
Question 58
A healthy 25-year-old man sustains a grade IIIB open tibial fracture. Following appropriate debridement, irrigation, and stabilization with an external fixator, the soft-tissue injury is shown in Figure 30. What is the most appropriate definitive soft-tissue coverage procedure?
Explanation
This is a very large near circumferential defect with posterior as well as anterior skin and muscle injury. Bone is exposed. The posterior muscles cannot be rotated since they are part of the zone of injury. The bone and other poorly vascularized areas of this wound would not accept a skin graft. The best chance for limb salvage will be to obtain soft-tissue coverage with a free tissue transfer using the latissimus dorsi. Mathes SJ, Nahai F: Vascular anatomy of muscle: Classification and applications, in Mathes SJ, Nahai F (eds): Clinical Application for Muscle and Musculocutaneous Flaps. St Louis, MO, CV Mosby, 1982, p 20.
Question 59
A 25-year-old woman undergoes surgical treatment of a displaced proximal humeral fracture via a deltopectoral approach. At the first postoperative visit, she reports a tingling numbness along the anterolateral aspect of the forearm. What structure is most likely injured?
Explanation
Sensation along the anterolateral aspect of the forearm is supplied by the lateral antebrachial cutaneous nerve, the terminal branch of the musculocutaneous nerve. The musculocutaneous nerve can be injured by proximal humeral fractures or dislocations, and is also at risk during surgical exposure if excessive retraction is placed on the conjoint tendon. The musculocutaneous nerve enters the conjoint tendon 1 cm to 5 cm distal to the coracoid process. McIlveen SJ, Duralde XA, D'Alessandro DF, et al: Isolated nerve injuries about the shoulder. Clin Orthop 1994;306:54-63.
Question 60
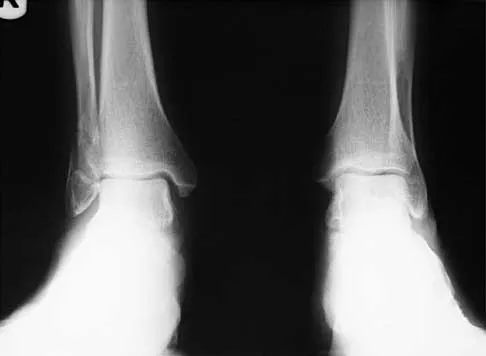
A 7-year-old girl has pain and swelling of the right elbow after falling off her bicycle. Radiographs are shown in Figure 31. What is the most appropriate initial step in management?

Explanation
Lateral condylar fractures are challenging to treat because of late displacement and development of a nonunion that may lead to valgus instability, pain, or tardy ulnar nerve palsy. Fractures such as this one with more than 2 mm of displacement on any radiographic view are prone to nonunion and should be stabilized. Fractures with less than 2 mm of displacement usually are stable and may be treated nonsurgically. In these patients, careful follow-up is recommended within several days of casting to check for fracture displacement. Arthrography or MRI may be helpful in these minimally displaced fractures. Fractures with an intact articular cartilage surface, such as noted on these studies, are unlikely to displace further. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425. Attarian DE: Lateral condyle fractures: Missed diagnoses in pediatric elbow injuries. Mil Med 1990;155:433-434. Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 61
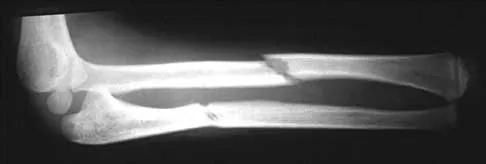
A 32-year-old man sustained a fracture of his upper arm in a motor vehicle accident. Radiographs are shown in Figure 32. Because of other associated injuries, surgical stabilization is chosen. What technique will result in the least complications and the best outcome?

Explanation
Most humeral fractures will heal with nonsurgical functional brace management. When the initial pain has subsided in a coaptation splint, the patient is converted to a functional brace and allowed to use the arm for activities. The fracture should heal within 6 weeks to 12 weeks with acceptable results. Surgery is indicated if there is vascular injury, open injury, floating elbow, chest injury, bilateral humeral fractures, or if a reduction cannot be obtained or maintained. The surgical treatment of choice is either antegrade reamed locked intramedullary nailing or plate osteosynthesis. Plate osteosynthesis appears to offer better results with respect to union, function, and risk of complications. Schemitsch EH, Bhandari M: Fractures of the humeral shaft, in Browner BD: Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1481-1511.
Question 62
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
This injury pattern is one of a direct trauma to the mid aspect of the foot. Without additional forces involved, capsular ligamentous injury is not anticipated; therefore, the injury should be a stable pattern. Treatment should consist of protected weight bearing as tolerated in a walking boot or walking cast. Surgical intervention with open reduction and internal fixation, percutaneous pinning, or open reduction and internal fixation with primary tarsometatarsal joint fusion is not indicated with this pattern of injury. The use of external bone stimulation in this acute fracture setting is not indicated. With injuries to the midfoot area where the exact mechanism of injury is uncertain, there should be a high index of suspicion for an associated injury to the tarsometatarsal joint, and standing radiographs or stress radiographs should be obtained. Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Question 63
During a posterior approach to the glenoid with retraction as shown in Figure 33, care should be taken during superior retraction to avoid injury to which of the following structures?
Explanation
During a posterior approach to the shoulder for either a scapular fracture, glenoid fracture, or posterior shoulder pathology, the interval between the teres minor and infraspinatus is split. Excessive superior retraction on the infraspinatus, or excessive dissection superomedially under the infraspinatus muscle and tendon can cause injury to the suprascapular nerve and/or artery. During dissection in this interval, the axillary artery and axillary nerve are well protected. A branch of the circumflex scapular artery ascends between the teres minor and infraspinatus muscle, but it is at risk during dissection on the scapula in the mid portion of the interval and not during superior retraction. The profunda brachii artery is not present in this interval. Jerosch JJ, Greig M, Peuker ET, et al: The posterior subdeltoid approach: A modified access to the posterior glenohumeral joint. J Shoulder Elbow Surg 2001;10:265-268. Judet R: Surgical treatment of scapular fractures. Acta Orthop Belg 1964;30:673-678.
Question 64
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction. Rockwood and Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Question 65
Figures 34a through 34c show the radiographs of a 51-year-old woman who injured her elbow in a fall from standing height. Examination reveals that elbow range of motion is limited by pain only. Management should consist of



Explanation
34b 34c The radiographs show a small minimally displaced radial head fracture that is amenable to nonsurgical management. Early range-of-motion exercises will best restore function and minimize stiffness. A long arm cast for any length of time will result in severe elbow stiffness. Morrey BF: Radial head fracture, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 341-364.
Question 66
Figure 35 shows the radiograph of a 12-year-old boy who fell off a snowmobile and landed on his left shoulder. He has a closed injury. Management should consist of

Explanation
Proximal humeral fractures in children are classified as metaphyseal or Salter-Harris type I or II fractures, and most of these fractures are treated with closed methods. Eighty percent of the growth of the humerus comes from the proximal physis; therefore, tremendous remodeling potential is present. Indications for open reduction include open fractures or severely displaced fractures in adolescents with minimal growth remaining. Acceptable limits of reduction in adolescent proximal humeral fractures include bayonet apposition and angulation of less than 35 degrees. Common blocks to reduction in adolescents include the biceps tendon and periosteum. For this fracture, use of a shoulder sling without reduction will lead to healing and an excellent result as the proximal humerus remodels. Kohler R, Trillaud JM: Fracture and fracture separation of the proximal humerus in children: Report of 136 cases. J Pediatr Orthop 1983;3:326-332. Beaty JH: Fractures of the proximal humerus and shaft in children. Instr Course Lect 1992;41:369-372. Dobbs MB, Luhmann SL, Gordon JE, et al: Severely displaced proximal humeral epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Beringer DC, Weiner DS, Noble JS, et al: Severely displaced proximal humeral epiphyseal fractures: A follow-up study. J Pediatr Orthop 1998;18:31-37.
Question 67
What is the most common complication requiring reoperation after dorsal plating for a distal radius fracture?
Explanation
The most common complication of dorsal plating is extensor tenosynovitis, which often causes pain and is a frequent reason for hardware removal. Other less frequent complications include loss of reduction and extensor tendon ruptures, with flexor tendon ruptures occuring to an even lesser degree. Rozental TD, Beredjiklian PK, Bozentka DJ: Functional outcome and complications following two types of dorsal plating for unstable fractures of the distal part of the radius. J Bone Joint Surg Am 2003;85:1956-1960.
Question 68
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include


Explanation
36b The patient has an oligotrophic nonunion of the distal femoral fracture. Although the proximal fracture appears incompletely united, it was stable at exchange nailing. The treatment of choice is exchange reamed nailing to at least 2 mm above the nail in place. Bone grafting is debatable. Recent studies have shown a 70% to 75% success rate with exchange nailing only, so in nonhypertrophic nonunions, bone grafting can be considered. Nonsurgical management consisting of observation or external stimulation runs the risk of implant failure. Plate fixation is acceptable but is considered a second choice because of the need to consider stabilization of the proximal fracture until union is achieved. Also, plate fixation definitely requires bone grafting. Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141. Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Question 69
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of

Explanation
Monteggia fractures in children must be recognized. Early appropriate treatment is much easier than delayed reconstruction for a missed radial head dislocation. In younger children, attempts should be made to reduce the ulna fracture and radial head dislocation with traction and manual manipulation. Anterior Monteggia fractures are the most common, and in this variety the radius is much better stabilized in elbow flexion. Posterior Monteggia fractures are less common and may be managed in elbow extension. Closed reduction is much more successful in younger children; ulnar fixation with a rod or plate may be needed in older patients with unstable fractures. Annular ligament repair is rarely needed in the acute fracture. Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554. Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
Question 70
What is the most important factor in determining recovery after surgical repair of a complete laceration of a nerve at the wrist?
Explanation
All other factors being equal, a patient's age is the most important factor in determining outcome after peripheral nerve injury. Repair of a nerve laceration within the first 2 weeks is generally considered appropriate. Fascicular repair may be of benefit in larger proximal nerves to reapproximate appropriate nerve bundles; distally perineural or epineural repair is sufficient. Use of a fibrin tissue sealant for nerve repair does not result in improved outcomes over suture repair. Nerve conduits have shown promise in digital nerves but do not have proven benefit in larger caliber nerves. Sunderland S: Nerve Injuries and Their Repair: A Critical Appraisal. New York, NY, Churchill Livingstone, 1991. Wilgis ES, Brushart TM: Nerve repair and grafting, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1325. Narakas A: The use of fibrin glue in repair of peripheral nerves. Orthop Clin North Am 1988;19:187-199.
Question 71
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 72
A 25-year-old laborer sustains a transverse fracture of the proximal 25% of the scaphoid. CT reconstructions reveal a 1-mm fracture gap. What is the most appropriate treatment?
Explanation
A higher risk of nonunion and the need for prolonged immobilization is seen after nonsurgical management of proximal pole fractures of the scaphoid. Because of the relatively poor blood supply of the proximal pole, surgical treatment with a compression screw is advocated for fractures of the proximal third of the scaphoid. Clay NR, Dias JJ, Costigan PS, et al: Need the thumb be immobilized in scaphoid fractures? A randomised prospective trial. J Bone Joint Surg Br 1991;73:828-832.
Question 73
A 34-year-old man sustained a tibial fracture in a motorcycle accident. What perioperative variable is associated with the greatest relative risk for reoperation to achieve bone union?
Explanation
In a recent analysis of 200 patients with tibial fractures, Bhandari and associates attempted to identify variables that were predictive of reoperation. The variables in the study were type of injury (fracture pattern), degree of open injury, mechanism of injury, cortical bone contact, postoperative complications, polytrauma, anti-inflammatory drug use, nail insertion technique (reamed versus nonreamed), smoking history, alcohol use, diabetes mellitus, peripheral vascular disease, age, disability status pre-injury, gender, surgeon, time to surgery, steroid use, phenytoin use, antibiotic use, anticoagulant use, and type of fixation used. Three variables were statistically significant predictors of reoperation to achieve bone union in the first postinjury year: transverse fracture pattern, open fracture, and cortical contact of 50% or less. Using these three variables, four reoperation risk groups were identified based on the number of these three variables present: 0, 1, 2, or 3. The risk for reoperation was 0%, 18%, 47%, and 94%, respectively. The authors concluded that these statistics can provide prognostic information to patients and help identify those high-risk patients where early intervention to achieve union is indicated. In addition, the data highlights the significance of achieving cortical contact at the time of initial fixation.
Question 74
Figure 38a shows the radiograph of a 12-year-old boy who underwent a reamed intramedullary nailing for a closed femoral shaft fracture. One year after rod removal, he reports groin pain. A current radiograph is shown in Figure 38b. The findings are most likely the result of


Explanation
38b Osteonecrosis of the femoral head is a known complication from the use of rigid intramedullary nails for femoral fractures in adolescents. When the nails are placed through the piriformis fossa, the lateral ascending vessels of the femoral neck may be injured, resulting in osteonecrosis of the femoral head in 1% to 2% of patients. Rigid reamed nails placed into the piriformis fossa are contraindicated in children with open growth plates because the physis is a barrier to blood supply and the ligamentum teres does not provide sufficient vascularity. Alternative fixation methods for femoral fractures in adolescents include external fixation and open reduction and internal fixation. Nailing through the tip of the trochanter may decrease the incidence of this serious complication. Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516. Stans AA, Morrissy RT, Renwick SE: Femoral shaft fracture treatment in patients age 6 to 16 years. J Pediatr Orthop 1999;19:222-228. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
Question 75
A 36-year-old woman has neck pain in the upper cervical region and occipital discomfort after being involved in a motor vehicle accident. Examination reveals no forehead or scalp lacerations. The neurologic examination is normal. A CT scan shows no evidence of bony injury. Figures 39a and 39b show a lateral radiograph and an MRI scan. Management should consist of


Explanation
39b The lateral radiograph shows 8 mm of atlantoaxial translation. In the absence of a bony injury, this represents rupture of the transverse atlantal ligament. The MRI scan reveals soft-tissue swelling posterior to the odontoid and a high intensity zone in the atlanto-dens interval consistent with acute injury. These injuries require arthrodesis because nonsurgical measures will not provide stability. Techniques for C1-2 fusion include Gallie, Brooks, or triple wiring. Transarticular screw fixation across the C1-2 articulation provides the most rigid means of fixation and the highest arthrodesis rates but is technically demanding. Anterior C2-3 arthrodesis will not address the level of instability. The normal atlanto-dens interval is 3 mm in an adult and 4 mm in a child. Kurz LT: Transverse atlantal ligament insufficiency, in Clark CR (ed): The Cervical Spine. Philadelphia, PA, Lippincott-Raven, 1998, pp 401-407.
Finish Exam?
You cannot change answers after submitting.
