Question 26
Figures 14a and 14b show the initial radiographs of an 18-year-old man who fell while snowboarding. Figures 14c and 14d show the radiographs obtained following closed reduction. Examination reveals that the elbow is stable with range of motion. Management should now consist of




Explanation
14b 14c 14d The initial radiographs reveal a simple elbow dislocation without associated fractures. After successful closed reduction, the range of stability should be assessed. If the elbow is stable, nonsurgical management should consist of a short period of immobilization followed by range-of-motion exercises. Immobilization for more than 3 weeks results in significant elbow stiffness. Surgical repair is indicated for dislocations that are irreducible, have associated fractures, or where stability cannot be maintained with closed treatment. Cohen MS, Hastings H II: Acute elbow dislocations: Evaluation and management. J Am Acad Orthop Surg 1998;6:15-23.
Question 27
A 12-year-old boy sustains open comminuted midshaft tibial and fibular fractures while playing indoor soccer. The wound is grossly clean and measures 7 cm with some periosteal stripping. Antibiotics and tetanus toxoid are administered immediately in the emergency department. Following irrigation and debridement of the wound in the operating room, treatment should include

Explanation
Open fractures in children have similar rates of short-term complications such as compartment syndrome, vascular injury, and nerve injury when compared to adult fractures. Primary wound closure should be used for Gustillo and Anderson type 1 or uncomplicated type 2 fractures after surgical debridement. Skeletal stabilization may consist of external fixation, flexible nails, or casting with or without supplementary pin fixation. For an open comminuted midshaft fracture, external fixation is the treatment of choice. Reamed intramedullary nailing is contraindicated in children with an open physis. Plate fixation has a high complication rate in severe open fractures. Jones BG, Duncan RD: Open tibial fractures in children under 13 years of age-10 years experience. Injury 2003;34:776-780. Bartlett CS III, Weiner LS, Yang EC: Treatment of type II and type III open tibia fractures in children. J Orthop Trauma 1997;11:357-362. Robertson P, Karol LA, Rab GT: Open fractures of the tibia and femur in children. J Pediatr Orthop 1996;16:621-626.
Question 28
Which of the following is an advantage of unreamed nailing of the tibia compared to reamed nailing?


Explanation
The debate between reamed versus unreamed intramedullary nailing of the tibia continues. Although unreamed nailing was proposed for open fractures to minimize infection, its simplicity made it appealing for closed fractures. However, most studies to date show that the only advantage of unreamed nailing is less surgical time. All studies show higher nonunion rates with increased hardware failure and increased time to union for unreamed nailing. Even in open fractures graded up to Gustilo Grade IIIA, the reamed tibial nail performs better. Larsen LB, Madsen JE, Hoiness PR, et al: Should insertion of intramedullary nails for tibial fractures be with or without reaming? A prospective, randomized study with 3.8 years' follow-up. J Orthop Trauma 2004;18:144-149.
Question 29
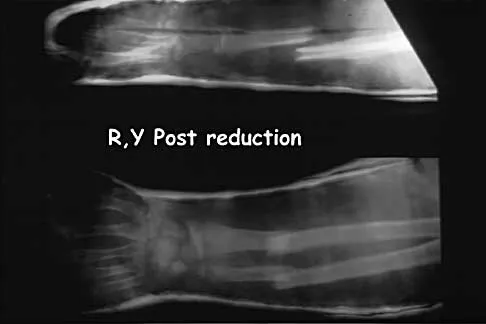
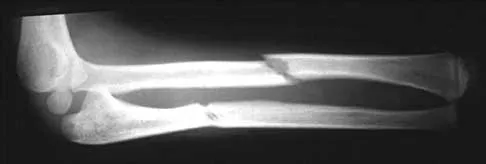
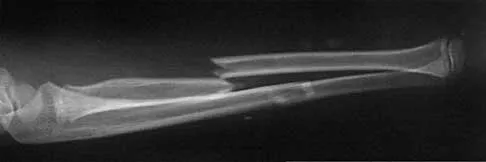
A 12-year-old boy sustained a both bone forearm fracture 10 weeks ago and underwent closed reduction and casting. Examination now reveals that the injury is healed, but he is unable to extend his little and ring fingers of the injured hand with his wrist extended. Full extension is possible with the wrist flexed. A radiograph and clinical photograph are shown in Figures 15a and 15b. The remainder of his hand and wrist examination and neurologic evaluation in the hand are normal. What is the most likely diagnosis?

Explanation
15b In this patient, examination reveals an inability to extend the fingers with the wrist extended, but full extension is possible with wrist flexion. These findings demonstrate isolated tenodesis of the flexor digitorum to the ring and little fingers. These findings are not consistent with compartment syndrome or nerve injury. Scarring or entrapment of tendons in forearm fractures can occur. Watson PA, Blair W: Entrapment of the index flexor digitorum profundus tendon after fracture of both forearm bones in a child. Iowa Orthop J 1999;19:127-128. Shaw BA, Murphy KM: Flexor tendon entrapment in ulnar shaft fractures. Clin Orthop 1996;330:181-184. Kolkman KA, van Niekerk JL, Rieu PN, et al: A complicated forearm greenstick fracture: Case report. J Trauma 1992;32:116-117.
Question 30
An otherwise healthy 35-year-old woman reports dorsal wrist pain and has trouble extending her thumb after sustaining a minimally displaced fracture of the distal radius 3 months ago. What is the next most appropriate step in management?

Explanation
Extensor pollicis longus tendon rupture can occur after a fracture of the distal radius, even a minimally displaced one. Poor vascularity of the tendon within the third dorsal compartment is the suspected etiology, not the displaced fracture fragments. Tendon transfer will suitably restore active extension of the thumb interphalangeal joint. Christophe K: Rupture of the extensor pollicis longus tendon following Colles fracture. J Bone Joint Surg Am 1953;35:1003-1005.
Question 31
Figure 16a shows the radiograph of a 34-year-old woman who sustained a basicervical fracture of the femoral neck. The fracture was treated with a compression screw and side plate. Seven months postoperatively, she continues to have significant hip pain and cannot bear full weight on her hip. A recent radiograph is shown in Figure 16b. Management should now consist of


Explanation
16b The patient sustained a high-angle femoral neck fracture. The follow-up clinical findings and radiograph show that she now has a nonunion with failed internal fixation. The joint appears preserved. In a healthy, young patient, arthroplasty of the femoral head, although possible, is not ideal. Excellent healing and function can be obtained in 70% to 80% of patients with femoral neck nonunion with a valgus intertrochanteric osteotomy. Marti RK, Schuller HM, Raaymakers EL: Intertrochanteric osteotomy for non-union of the femoral neck. J Bone Joint Surg Br 1989;71:782-787.
Question 32
An 18-year-old man was in a motor vehicle accident and sustained a closed head injury, right displaced scapular body and glenoid fractures, a right proximal humeral fracture, fractures of ribs one through three, facial fractures, and bilateral pubic rami fractures with minimal displacement. He has a systolic blood pressure of 80/40 mm Hg despite fluid resuscitation. A radiograph is shown in Figure 17. Spiral CT does not identify any thoracic or abdominal injuries. What is the next most appropriate step in management?


Explanation
The patient has sustained high-energy upper extremity and chest injuries. He continues to remain hemodynamically unstable with no obvious thoracic or abdominal injury responsible for bleeding. The pelvic fracture is unlikely to be causing significant bleeding. A scapulothoracic dissociation and possible disruption of one of the great vessels of the upper extremity should be considered. Evaluation of peripheral pulses or blood pressure indices bilaterally in the upper extremities is a simple way to evaluate the need for further work-up. If there is any discrepancy or further concern, angiography of the involved extremity is necessary. Althausen PL, Lee MA, Finkemeier CG: Scapulothoracic dissociation: Diagnosis and treatment. Clin Orthop 2003;416:237-244.
Question 33
What is the major difference in outcome following open reduction and internal fixation (ORIF) of the tibial plafond at 2 to 5 days versus 10 to 20 days?

Explanation
Long-term outcomes following tibial plafond fractures treated with ORIF are satisfactory in most patients despite a high incidence of posttraumatic osteoarthritis. If ORIF is delayed until 10 to 20 days following injury, the major difference in outcomes is fewer complications associated with wound healing. Ankle strength, pain, range of motion, and the development of arthritis are equal regardless of the time until fixation. Sirkin M, Sanders R, DePasquale T, et al: A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 1999;13:78-84.
Question 34
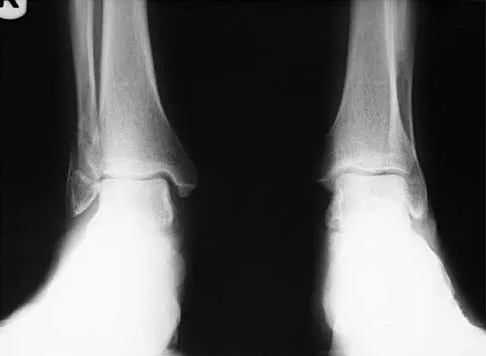
Figure 18a shows the initial lateral radiograph of a 6-year-old girl who sustained a fracture in a motor vehicle accident and was treated in a cast 1 year ago. She now has the valgus deformity seen in Figure 18b. Treatment should consist of





Explanation
18b Proximal tibial metaphyseal fractures may result in late genu valgum as a result of asymmetric growth of the proximal tibia. These patients are best treated with observation because the deformity is likely to remodel. Osteotomy is not indicated and potentially will lead to recurrence. Stapling of the medial tibial physis is appropriate in patients who have a severe and progressive deformity. Cozen L: Knock-knee deformity in children: Congenital and acquired. Clin Orthop 1990;258:191-203. Jackson DW, Cozen L: Genu valgum as a complication of proximal tibial metaphyseal fractures in children. J Bone Joint Surg Am 1971;53:1571-1578. Brammar TJ, Rooker GD: Remodeling of valgus deformity secondary to proximal metaphyseal fracture of the tibia. Injury 1998;29:558-560. Ogden JA, Ogden DA, Pugh L, et al: Tibia valga after proximal metaphyseal fractures in childhood: A normal biologic response. J Pediatr Orthop 1995;15:489-494.
Question 35
Figure 19 shows the radiograph of a 45-year-old woman who has a painful nonunion. Treatment should consist of


Explanation
The radiograph reveals a reverse obliquely subtrochanteric/intertrochanteric fracture. Open reduction and internal fixation should be accomplished with a 95-degree fixed angle device. An intramedullary nail with screw fixation into the head is another possible technique. Either method should correct the varus deformity. Exchange of a high-angled screw and plate device to a longer side plate and bone grafting does not afford any improvement in the mechanical stability. Hardware removal and retrograde intramedullary nailing is not indicated for this level of a proximal femoral injury. Placement of an implantable bone stimulator may change local biologic factors but would not enhance mechanical stability. The patient's femoral head is intact without signs of collapse; therefore, hardware removal, proximal femoral resection, and total hip arthroplasty are not warranted. Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Question 36
A 7-year-old boy has a swollen and deformed right arm after falling off his bicycle. Radiographs reveal a completely displaced posterolateral supracondylar humeral fracture. Examination reveals a warm, pink hand and forearm but absent pulses. What is the next most appropriate step in management?


Explanation
The incidence of vascular injury in supracondylar humeral fractures is directly related to the degree and direction of displacement. Significant posterior lateral displacement tends to result in brachial artery and median nerve injuries, and posterior medial displacement may lead to radial nerve injury. The brachial artery is always injured at the level of the fracture; therefore, angiography or MRA will not assist in locating the injury. The treatment of choice is surgical reduction and stabilization of the fracture, followed by reassessment of the vascular status. If the hand is pink and warm or pulses can be detected with doppler, it is reasonable to follow the extremity closely after surgery. If the arm becomes pulseless and white, immediate anterior exploration of the arm is indicated. The artery is often entrapped in the fracture and once extricated, will provide adequate blood flow. If the artery is injured, a primary repair or vein graft is needed. Shaw BA: The role of angiography in assessing vascular injuries associated with supracondylar humerus fractures remains controversial. J Pediatr Orthop 1998;18:273. Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 37
What is the treatment of choice for the injury shown in Figures 20a through 20c?




Explanation
20b 20c The radiographs show multiple carpometacarpal dislocations. Reduction is often obtainable but difficult to maintain. Internal fixation is required to maintain the reduction, preferably with Kirschner wires. Closed reduction and percutaneous pinning is preferred by some surgeons. Others recommend open reduction to remove irreconstructable osteochondral fragments from the individual joints and to ensure correct reduction of the carpometacarpal joints. Kirschner wires are removed at 6 to 8 weeks. Prokuski LJ, Eglseder WA Jr: Concurrent dorsal dislocations and fracture-dislocations of the index, long, ring, and small (second to fifth) carpometacarpal joints. J Orthop Trauma 2001;15:549-554.
Question 38
A 32-year-old man has intense right hand and wrist pain, a deformed wrist, and numbness in his fingers after falling off his motorcycle. This is an isolated injury. Examination reveals a swollen wrist, normal capillary refill to all fingers, and limited flexion of all fingers. Radiographs are shown in Figures 21a and 21b. Neurologic examination of the hand will most likely reveal



Explanation
21b The patient has a perilunate dislocation. A volar dislocation of the lunate is often associated with median nerve dysfunction. This injury to the wrist is often overlooked because of its benign clinical appearance and the presence of other injuries, as it is caused by high-energy mechanisms. Ruby LK, Cassidy C: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1297-1300.
Question 39
A 55-year-old woman fell and sustained an elbow dislocation with a coronoid fracture and a radial head fracture. The elbow is reduced and splinted. What is the most common early complication?


Explanation
The patient has a dislocation of the elbow with displaced coronoid process and radial head fractures. The elbow is extremely unstable after this injury, and recurrent dislocation in a splint is the most common early complication. Skeletal stabilization of the fractures is required to restore stability of the joint. Characteristics of the fractures will determine the techniques required to restore stability. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 40
A 25-year-old man sustained the closed injury shown in Figures 22a and 22b. Examination reveals that this is an isolated injury, and he is hemodynamically stable. Treatment should consist of




Explanation
22b The treatment of choice for closed diaphyseal femoral fractures in adults is reamed intramedullary nailing with static interlocking. Reaming allows placement of a larger, stronger implant and offers better healing rates than unreamed nailing. Static interlocking ensures that there is no loss of reduction because of underappreciated fracture lines or comminution. Brumback RJ, Virkus WW: Intramedullary nailing of the femur: Reamed versus nonreamed. J Am Acad Orthop Surg 2000;8:83-90.
Question 41
Figure 23 shows the radiograph of an elderly man who fell on his right arm. What is the most important determinate of a good outcome following this injury?



Explanation
Minimally displaced fractures of the proximal humerus have a good outcome if physical therapy is initiated within 2 weeks of the injury. Results are not affected by age, open reduction and internal fixation, or involvement of the greater tuberosity. Immobilization for longer than 3 weeks will often result in stiffness. Koval KJ, Gallagher MA, Marsicano JG, et al: Functional outcome after minimally displaced fractures of the proximal part of the humerus. J Bone Joint Surg Am 1997;79:203-207.
Question 42
A 40 year-old-man was involved in a motor vehicle accident and sustained the pelvic injury seen in Figures 24a and 24b. Definitive management of the injury should consist of reduction by


Explanation
24b The radiograph reveals disruption of the symphysis pubis and a displaced left sacral fracture. A posterior injury with displacement of greater than 1 cm is unstable, and a sacral fracture is particularly unstable. Surgical stabilization is required for these unstable anterior and posterior injuries. External fixation provides little stability to an unstable posterior pelvic injury. Reduction and internal fixation of the symphysis pubis and sacral fracture will provide the most stable pelvis with the least resultant deformity and allow patient mobilization. Tile M: Management of pelvic ring injuries, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 168-202.
Question 43
A 35-year-old patient sustained a bimalleolar ankle fracture. What is the most reliable method of predicting a tear of the interosseous membrane?


Explanation
The Weber and Lauge-Hansen fracture classifications suggest that the interosseous membrane (IOM) is torn with certain fracture patterns. In a recent study that evaluated ankle fractures with MRI, Nielson and associates identified 30 patients with IOM tears. Ten of the tears did not correspond with the level of the fibular fracture. The authors concluded that stability of the syndesmosis should not be based on the level of the fibular fracture alone but should also include an intraoperative stress test. Transsyndesmotic fixation should be considered for those fractures where the intraoperative stress test demonstrates instability. A widened medial clear space may occur with a deltoid injury and distal fibular fracture in the absence of a significant tear of the interosseous membrane.
Question 44
When performing a flexor tendon repair of a digit other than the thumb, what structures of the flexor tendon sheath should be preserved?


Explanation
The A2 and A4 pulleys are considered the most important parts of the pulley system. If these two structures are preserved, 80% of finger flexion can be maintained. If the pulley system is not left intact or is not reconstructed, "bow-stringing" of the flexor tendons occurs with loss of full flexion. The A2 pulley is over the proximal phalanx and the A4 pulley is over the middle phalanx. Doyle JR: Anatomy of the finger flexor tendon sheath and pulley system. J Hand Surg Am 1988;13:473-484.
Question 45
A distal radius fracture in an elderly man is strongly predictive for what subsequent injury?




Explanation
Fractures of the distal radius increase the relative risk of a subsequent hip fracture significantly more in men than in women. A previous spinal fracture has an equally important impact on the risk of a subsequent hip fracture in both genders.
Question 46
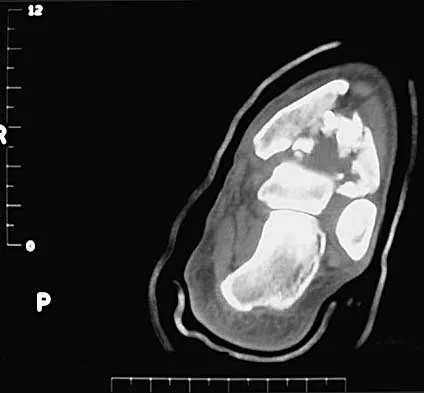
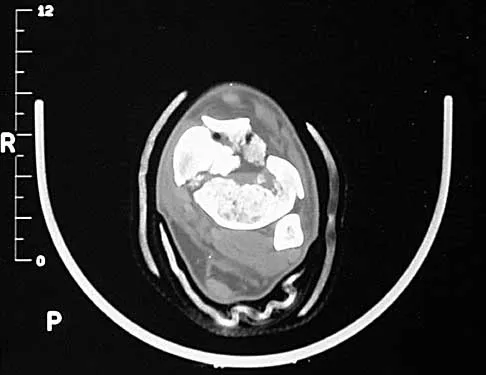
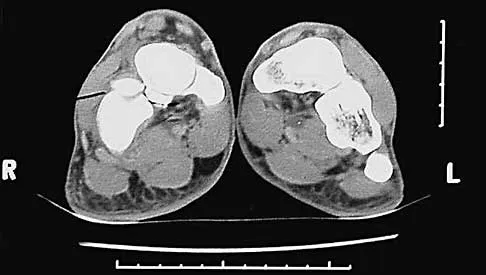
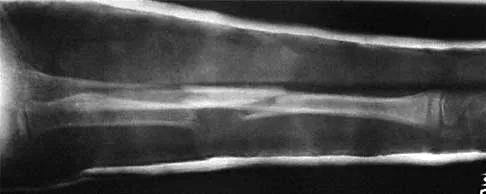
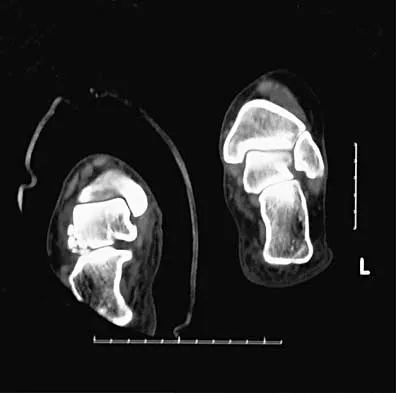
A 13-year-old girl injures her ankle playing soccer. Radiographs reveal a displaced Tillaux fracture. CT scans are shown in Figure 25. What is the most important consideration for appropriate management?


Explanation
Tillaux and triplane fractures occur in adolescents as the result of an external rotation injury of the ankle. As seen on the CT scan, the growth plate starts to close during adolescence; therefore, growth arrest resulting in limb-length discrepancy or angulation is less of a concern in this age group than achieving joint congruity. The joint should be surgically reduced if displacement is greater than 2 mm to minimize the chances of late arthrosis. Kay RM, Matthys GA: Pediatric ankle fractures: Evaluation and treatment. J Am Acad Orthop Surg 2001;9:268-278. Kling TF Jr: Operative treatment of ankle fractures in children. Orthop Clin North Am 1990;21:381-392.
Question 47
What measure of physiologic status best evaluates whether an injured patient is fully resuscitated and best predicts that perioperative complications will be minimized following definitive stabilization of long bone fractures?

Explanation
Serum lactate levels can be used to evaluate the effectiveness of the resuscitation of patients who have multiple injuries. Even after resuscitation, patients may have occult hypoperfusion as defined by a serum lactate level of greater than 2.5 mmol/L. The studies referenced indicate that these patients are at increased risk of perioperative complications such as organ failure or adult respiratory distress syndrome if definitive surgical fixation of the orthopaedic injuries is pursued prior to correction of the occult hypoperfusion. The other markers may be an indication of current physiology but have not been correlated with perioperative risks. Blow O, Magliore L, Claridge JA, et al: The golden hour and silver day: Detection and correction of occult hypoperfusion within 24 hours improves outcomes from major trauma. J Trauma 1999;47:964-977. Crowl A, Young JS, Kahler DM, et al: Occult hypoperfusion is associated with increased morbidity in patients undergoing early femur fracture fixation. J Trauma 2000;48:260-267.
Question 48
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of



Explanation
The radiograph shows a volarly dislocated lunate. Initial emergent treatment of perilunate dislocations should consist of closed reduction and splinting, especially if the patient exhibits median nerve compression. Open reduction and pinning or ligament repair are necessary but are not emergent. A dorsal approach is sometimes required for ligament repair or bony visualization; however, this can be done in a more semi-elective manner. Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
Question 49
A 10-year-old girl has a midshaft both bone forearm fracture. After attempted closed reduction, alignment consists of bayonet apposition, 10 degrees of malrotation, and 8 degrees of volar angulation. Management should now consist of


Explanation
Acceptable alignment in both bone forearm fractures is related to age and location. In children younger than age 9 years, angulations of 15 degrees and malrotation of 45 degrees are acceptable. In children older than age 9 years, acceptable alignment is 10 degrees of angulation and 30 degrees of malrotation. Bayonet apposition is acceptable provided that the angular and rotational reductions are held within these guidelines. A long arm cast provides better control of deforming forces than a short arm cast. Do TT, Strub WM, Foad SL, et al: Reduction versus remodeling in pediatric distal forearm fractures: A preliminary cost analysis. J Pediatr Orthop B 2003;12:109-115. Flynn JM: Pediatric forearm fractures: Decision making, surgical techniques, and complications. Instr Course Lect 2002;51:355-360. Ring D, Waters PM, Hotchkiss RN, et al: Pediatric floating elbow. J Pediatr Orthop 2001;21:456-459.
Question 50
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by

Explanation
In the treatment of ankle fractures, the superficial peroneal nerve is most commonly injured by the use of a direct lateral approach to the ankle. The superficial peroneal nerve and its branches exit the fascial hiatus approximately 9 cm to 10 cm proximal to the tip of the distal fibula with a range of 4 cm to 13 cm, and their course is typically anterior to the midlateral plane of the fibula. However, small branches may course across the surgical plane directly laterally. A posterior-lateral approach diminishes the risk of injury to the superficial peroneal nerve and its branches; however, by moving farther posterior, the sural nerve and its branches may be at increased risk. Cast immobilization may injure the cutaneous nerves about the ankle; however, the risks are greater with surgical intervention. A medial or anterior-medial approach to the ankle will not injure the superficial peroneal nerve at the ankle level. Redfern DJ, Sauve PS, Sakellariou A: Investigation of incidence of superficial peroneal nerve injury following ankle fracture. Foot Ankle Int 2003;24:771-774.
Finish Exam?
You cannot change answers after submitting.
