Question 26
The use of nasotracheal intubation for airway management is contraindicated in the acute multiply injured patient when the patient has

Explanation
The use of nasotracheal intubation is less desirable in patients with respiratory arrest because placement of the tube is most reliable when the patient is breathing. Nasotracheal intubation is advantageous in patients with suspected cervical spine trauma because it does not require hyperextension of the neck. A nasotracheal tube may be more comfortable than an orally placed tube because it is fixed at several points and moves less freely within the larynx, subglottic area, and trachea. The presence of a hemothorax or pneumothorax does not affect the choice of airway control but does require placement of a chest tube. Colice GL: Prolonged intubation versus tracheostomy in the adult. J Intern Care Med 1987;2:85.
Question 27
A 65-year man has right hip pain after a fall. Radiographs reveal a reverse oblique intertrochanteric femoral fracture. Treatment consists of reduction and internal fixation. Which of the following implants is most commonly associated with nonunion and hardware failure?


Explanation
Reverse oblique intertrochanteric femoral fractures account for 5% of all intertrochanteric or subtrochanteric fractures. They are uncommon but not rare and will be encountered in practice. The sliding hip screw is associated with the most problems because of its design. When reverse oblique fractures are fixed with a sliding hip screw, the action of the construct causes medial displacement of the distal fragment rather than compression of the proximal and distal fragments. All of the other implants prevent medial displacement of the distal segment. It should not be assumed that simply using one of the other implants is reason for success. There is a significant failure rate for each of these implants with reverse oblique fractures. The implant must be ideally placed and the fracture must be reduced. Haidukewych GJ, Israel TA, Berry DB: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650. Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
Question 28
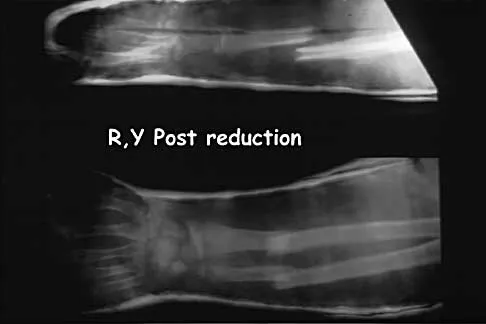
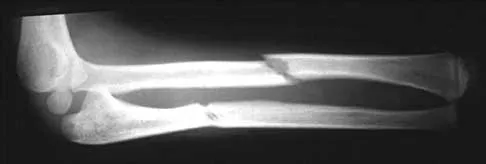
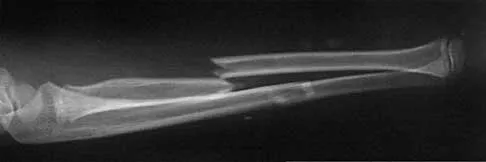
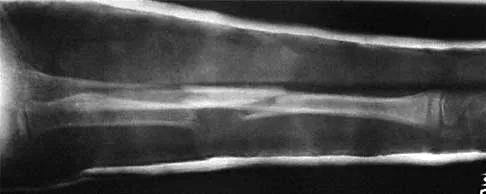
Figure 13a shows the radiograph of a 9-year-old girl who sustained complete transverse fractures of the radial and ulnar shafts while in-line skating. A manipulative closed reduction is performed, and the result is seen in Figure 13b. What is the next most appropriate step in management?




Explanation
13b Bayonet apposition of the radius and ulnar shafts is quite acceptable, as long as the angulation is less than 10 degrees. The rotation must be acceptable as well. This patient went on to full healing, with full supination and pronation of the forearm and no cosmetic deformity. Price CT, Scott DS, Kurzner ME, Flynn JC: Malunited forearm fractures in children. J Pediatr Orthop 1990;10:705-712.
Question 29
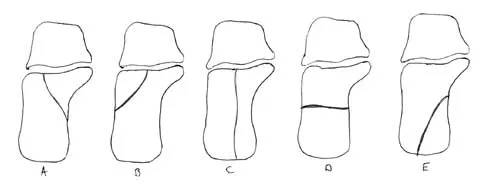
In Figure 14, the primary fracture line in a calcaneal fracture is best depicted by which of the following schematics?


Explanation
The schematic labeled A best depicts the primary fracture line in a calcaneal fracture. The primary fracture line in an axial-loading fracture of the calcaneus occurs from superior-lateral to inferior-medial. This fracture line separates the calcaneus into sustentacular and tuberosity fragments and typically enters the subtalar joint through the posterior facet. Although additional fracture lines typically occur, the primary fracture line is almost always present. If surgical reduction is planned, reducing the primary fracture is always a key step. Macey LR, Benirschke SK, Sangeorzan BJ, Hansen ST: Acute calcaneal fractures: Treatment option and results. J Am Acad Orthop Surg 1994;2:36-43.
Question 30
A 45-year-old man who sustains a medial subtalar dislocation while playing basketball undergoes immediate closed reduction. No fractures or osteochondral defects are noted on postreduction radiographs. The next most appropriate step in management should consist of


Explanation
Most subtalar dislocations can be easily reduced by closed methods. If no fractures or defects are seen on the postreduction radiographs, then the success rate with cast immobilization is good. Medial dislocations have a better prognosis than lateral dislocations. Late instability is rare; therefore, the duration of immobilization should not be excessive. Most subtalar dislocations result in some stiffening of the hindfoot, and painful degenerative arthrosis is the most common serious complication.
Question 31
A 21-year-old woman sustained a minimally displaced traumatic spondylolisthesis of C2 (Hangman's fracture) after striking the windshield with her forehead during a motor vehicle accident. Management should consist of
Explanation
According to the classification of Levine and Edwards, a type I Hangman's fracture is minimally displaced without angulation and represents a stable injury. Good clinical success has been achieved with nonsurgical management consisting of use of a rigid collar until the patient reports pain relief, followed by quick mobilization.
Question 32
A 25-year-old patient who sustained multiple bilateral rib fractures, a pulmonary contusion, a left nondisplaced transtectal acetabular fracture, and a closed humerus fracture in a motor vehicle accident 2 weeks ago is transferred from another hospital. The humerus fracture has been surgically treated. There are no signs of infection, and the trauma surgeon wants to mobilize the patient as soon as possible. Radiographs are shown in Figures 15a and 15b. Management of the humerus fracture should consist of



Explanation
15b The radiographs show a distal third humerus fracture that is angulated, rotated, and not rigidly fixed. Rigid fixation is needed because mobilization is highly desirable to improve pulmonary function. The acetabular fracture is through the weight-bearing dome but is nondisplaced. Nonsurgical management of the acetabular fracture requires at least 6 weeks of touchdown weight bearing to minimize the forces across the hip joint. Open reduction and plate fixation would achieve anatomic reduction and immediate mobilization. A single posterolateral 4.5-mm plate or two 3.5-mm plates at 90 degrees are possible alternatives. Immediate weight bearing on a plated humerus fracture with the use of crutches or a walker has been shown to be safe and would allow touchdown weight bearing, protecting the hip. None of the other options would achieve this goal for this distal fracture.
Question 33
Figure 16 shows the radiograph of a 23-year-old man who has severe right shoulder pain after his motorcyle hit a bridge guardrail. He is neurologically intact. Nonsurgical management will most likely result in



Explanation
Internal fixation of the clavicle, glenoid, or both has been recommended for fractures of the clavicle and glenoid neck (floating shoulders). Recently, the inherent instability of these dual fractures has been questioned in a biomechanical model without further disruption of the coracoclavicular or acromioclavicular ligamentous structures. Nonsurgical management of the majority of combined scapular/glenoid fractures in patients with less than 10 mm of displacement has resulted in excellent shoulder function and will most likely achieve an excellent result in this patient. Egol KA, Connor PM, Karunakar MA, Sims SH, Bosse MJ, Kellam JF: The floating shoulder: Clinical and functional results. J Bone Joint Surg Am 2001;83:1188-1194. Williams GR Jr, Naranja J, Klimkiewicz J, et al: The floating shoulder: A biomechanical basis for classification and management. J Bone Joint Surg Am 2001;83:1182-1187.
Question 34
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?



Explanation
The patient has a simple fracture pattern that can be reduced anatomically and stabilized with absolute stability by interfragmental compression and protection plating. This will guarantee a 95% to 98% union rate with no radial nerve palsy. Intramedullary nailing does not equal these results in a simple fracture pattern in the humerus. Bridge plating is indicated for multifragmented fracture patterns when anatomic reduction and absolute stability cannot be achieved. External fixation is reserved for severe open fractures. Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166. Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
Question 35
A 28-year-old painter has had increasing pain in his hand and forearm after sustaining a paint injection wound to the tip of his left index finger 24 hours ago. Management should consist of


Explanation
The clinical presentation soon after injury may be surprisingly innocuous, but all high-pressure injection injuries of various materials are best treated by emergent surgical debridement of all foreign material from the flexor tendon sheath as well as the subcutaneous tissues. Subsequent hospital admission, IV antibiotics, and possible repeat debridements usually are necessary. The use of antibiotics alone is inadequate treatment of this severe injury. Pinto MR, Turkula-Pinto LE, Cooney WP, Wood MB, Dobyns JH: High-pressure injection injuries of the hand: Review of 25 patients managed by open wound technique. J Hand Surg Am 1993;18:125-130. Urbaniak JR, Evans JP, Bright DS: Microvascular management of ring avulsion injuries. J Hand Surg Am 1981;6:25-30. Tsai TM, Manstein C, DuBou R, Wolff T, Kutz JE, Kleinert HE: Primary microsurgical repair of ring avulsion amputation injuries. J Hand Surg Am 1984;9:68-72. Kay S, Werntz J, Wolff T: Ring avulsion injuries: Classification and prognosis. J Hand Surg Am 1989;14:204-213.
Question 36
A 21-year-old basketball player inverts his foot during practice. Examination reveals obvious deformity of the hindfoot with a prominence of the talar head dorsolaterally and medial displacement of the forefoot. A radiograph is shown in Figure 17. What is the most likely obstacle to closed reduction?


Explanation
The patient has a medial subtalar dislocation. These injuries should be reduced as soon as possible to minimize risk to the skin. Most often, this can be done easily, and further radiographic evaluation then can be performed as necessary. On rare occasions, closed reduction is not possible because of fractures of the articular surface of the talus, navicular, interposed extensor digitorum brevis, or transverse fibers of the cruciate crural ligament. The posterior tibial tendon is the most common obstruction to closed reduction in lateral subtalar dislocations, which are less common than medial dislocations. The majority of both injuries can be managed by closed reduction and immobilization. Mulroy RD: The tibialis posterior tendon as an obstacle to reduction of a lateral anterior subtalar dislocation. J Bone Joint Surg Am 1953;37:859-863. Heckman JD: Fractures and dislocations of the foot, in Rockwood CA, Green DP, Bucholz RW (eds): Fractures in Adults. Philadelphia, PA, JB Lippincott, 1991, pp 2093-2100.
Question 37
A 27-year-old woman sustained a bilateral C5-6 facet subluxation in a motor vehicle accident. Neurologic evaluation reveals normal motor, sensory, and reflex functions. She is awake, alert, and cooperative. Initial management should consist of


Explanation
As long as the patient is alert and cooperative, an attempt can be made to reduce the dislocation. This should not be attempted in a patient who is obtunded, comatose, or uncooperative. If any neurologic changes are noted during the reduction maneuver, the attempt should be stopped, appropriate radiographic studies obtained, and open reduction and stabilization planned in the operating room.
Question 38
A 22-year-old patient sustained a jamming injury to the right little finger. The lateral radiograph shown in Figure 18 reveals comminution of the base of the middle phalanx, with palmar and dorsal metaphyseal cortical involvement. The articular surface also is disrupted. Management should consist of


Explanation
This fracture, known as a pilon fracture, represents comminution of the base of the middle phalanx with both palmar and dorsal cortical disruption. The treatment method that allows the best function and fewest complications is indirect reduction achieved through specific dynamic splinting or the use of specifically designed proximal interphalangeal joint external fixators. Early mobilization can be achieved by either of these techniques. Volar plate arthroplasty is indicated for a simple fracture-dislocation of the proximal interphalangeal joint with comminution of the volar fracture fragment and dorsal dislocation of the remaining articular surface. Open reduction and internal fixation or percutaneous pinning adds surgical risks and scarring and typically will not provide added stability. Cast immobilization will not achieve the goal of early range of motion. Stern PJ, Roman RJ, Kiefhaber TR, McDonough JJ: Pilon fractures of the proximal interphalangeal joint. J Hand Surg Am 1991;16:844-850.
Question 39
Figure 19 shows the radiograph of a 12-year-old boy who sustained an injury to his hand when another child fell on him. Management should consist of


Explanation
The patient has a Salter-Harris type III fracture of the proximal phalanx of the thumb. It is usually caused by an abduction injury where the ulnar collateral ligament avulses a fragment away from the proximal epiphysis and is the most common childhood gamekeeper's injury. If there is greater than 1 mm of separation or a significant articular step-off, an open reduction, performed through an extensor aponeurosis-splitting approach, is required to reestablish joint congruity and stability. Percutaneous or closed methods of reduction are usually ineffective. The dorsal approach avoids the volar neurovascular structures. Since the ulnar collateral ligament is still attached, this area does not need to be visualized. The major goal is to reestablish joint congruity and bony stability. This can be easily performed via the dorsal approach. Carey TP: Fracture and dislocations of the phalanges, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 435-436.
Question 40
Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of





Explanation
20b 20c The radiographs reveal a severely comminuted distal humerus fracture. A long arm cast, functional bracing, and closed reduction and percutaneous pin fixation all have a poor outcome and could result in a nonunion that will be very difficult to treat. Open reduction and internal fixation is indicated in most supracondylar humerus fractures, but total elbow arthroplasty is a good alternative in elderly patients who have multiple medical problems and when the fracture pattern may preclude stable enough internal fixation to allow postoperative motion. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Question 41
An 18-year-old man has acute respiratory distress after sustaining injuries in a motorcycle accident. He has a blood pressure of 80/60 mm Hg and a pulse rate of 110/min. Examination reveals chest tympany to percussion, distended neck veins, and deviation of the trachea away from his right hemithorax where the breath sounds are diminished. Heart sounds are regular and normal on auscultation. Initial management should consist of


Explanation
Tension pneumothorax occurs when air trapped in the pleural space between the lung and chest wall achieves sufficient pressure to compress the lungs and shift the mediastinum. Urgent needle decompression of the pleural space air followed by definitive chest tube placement is the treatment of choice.
Question 42
A 27-year-old man has neck pain after being involved in a motor vehicle accident. A lateral cervical radiograph is shown in Figure 21. What would be the most common neurologic finding?



Explanation
The radiographic findings are consistent with a type II Hangman's fracture or traumatic spondylolisthesis of C2. This occurs with more than 3 mm of displacement according to the classification of Levine and Edwards. Even though the radiograph reveals significant displacement, the overall space available for the neural elements is increased, therefore minimizing the risk of neural compromise. Neurologic injury is most frequently encountered in type III injuries that are associated with bilateral facet dislocations of C2 on C3 but is infrequent in type I (less than 3 mm displacement) and type II traumatic spondylolisthesis. When neurologic deficits are associated with type II injuries, it is usually the result of an associated head injury. Cruciate paralysis occurs as a result of the crossover of the motor and sensory tracts at different levels of the cord at the C1-C2 junction. This results in normal sensation but complete loss of motor function. Levine AM: Traumatic spondylolisthesis of the axis (Hangman's fracture), in Levine AM, Eismont FJ, Garfin S, Zigler JE (eds): Spine Trauma. Philadelphia, PA, WB Saunders, 1998, pp 287-288.
Question 43
After stabilizing a bimalleolar ankle fracture with a plate and lag screws for the fibula and two interfragmental compression screws for the medial malleolus, a syndesmosis screw is indicated in which of the following situations?


Explanation
It is imperative to recognize the need for a position screw (syndesmosis screw) to hold the syndesmosis in proper alignment when surgically stabilizing an ankle fracture. Although many different fracture patterns are suspicious for a disrupted syndesmosis, the only sure way to assess the syndesmosis is to stress it with abduction and external rotation of the talus and attempt to displace the fibula from the incisura fibularis. Under fluoroscopy, the talus will move laterally and displace the fibula, show a valgus talar tilt, or show an increase in the medial clear space. If any or all of these signs occur, a syndesmosis screw is inserted after making sure that the fibula is reduced into the incisura fibularis. This screw may traverse three or four cortices but must not act as a lag screw. It usually is inserted with the ankle in maximal dorsiflexion, although this is probably not necessary because it is almost impossible to overcompress the syndesmosis. The diameter of the screw does not make any difference. It may or may not be removed but not before 3 months. Tornetta P III, Spoo JE, Reynolds FA, Lee C: Overtightening of the ankle syndesmosis: Is it really possible? J Bone Joint Surg Am 2001;83:489-492. Stover MD, Kellam JF: Articular fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 105-119. Hahn DM, Colton CL: Malleolar fractures, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 559-581.
Question 44
A 32-year-old man sustains multiple injuries in a motorcycle accident including ipsilateral open right femur and comminuted tibia fractures. He has acute abdominal distention and tenderness to palpation. The pelvis is stable to examination. He has a blood pressure of 70/40 mm Hg despite appropriate fluid resuscitation and a pulse rate of 120/min; the pulse is thready. Which of the following procedures is considered the highest priority in the management of this patient?

Explanation
The patient is in hemorrhagic shock, and timely hemostasis in the operating room should be the highest priority. Further imaging and insertion of central lines carry the risk of further delays in arresting the source of the patient's bleeding. Albumin (colloid) solutions have questionable indications, are expensive, and have been associated with increased mortality. Crystalloid solutions such as normal saline or lactated Ringer's solution are the initial resuscitative fluid of choice until blood becomes available. Pneumatic antishock garments have been associated with higher mortality rates, particularly in patients with cardiac and thoracic vascular injuries. Krettek C, Simon RG, Tscherne H: Management priorities in patients with polytrauma. Langenbecks Arch Surg 1998;383:220-227.
Question 45
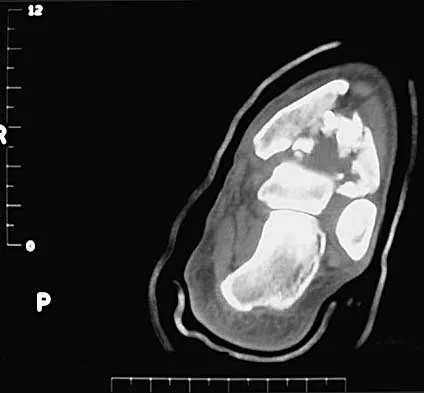
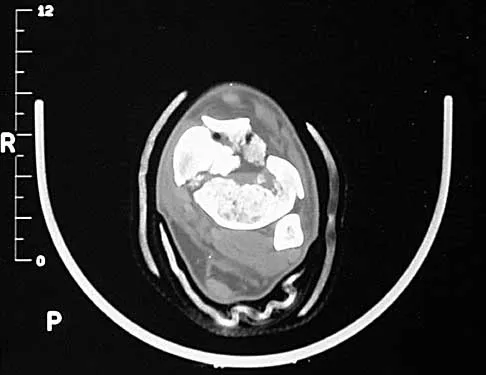
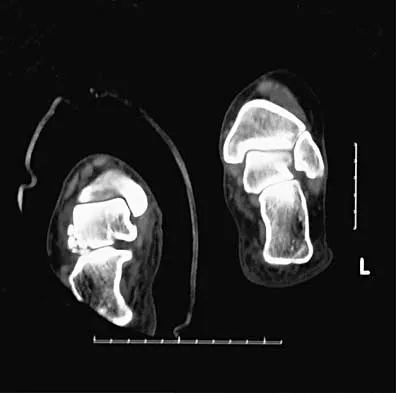
A 35-year-old man sustained an injury to his lower extremity after falling 10 feet from a ladder; initial management was nonsurgical. He now reports chronic hindfoot and anterior ankle pain. Radiographs are shown in Figures 22a and 22b. Surgical reconstruction of this painful process should consist of



Explanation
22b The radiographs reveal a hindfoot deformity that developed following a severe, comminuted, intra-articular fracture of the calcaneus. There is deformity of the calcaneal body and collapse of the talus into the calcaneus, leading to dorsiflexion of the talus and anterior ankle joint impingement. Distraction bone block subtalar joint arthrodesis will assist with correction of the calcaneal height and will allow for an improved talar declination angle. With this procedure, care must be taken to avoid placing the hindfoot into further varus. A similar reconstruction option not listed would be a calcaneal osteotomy and arthrodesis as described by Romash. Talectomy and tibiocalcaneal arthrodesis are not warranted because the primary structure of the talus and ankle joint is well preserved. In situ subtalar joint arthrodesis will not correct the deformity, and symptoms about the ankle and hindfoot would most likely persist. Lateral wall calcaneal exostectomy may decrease pain from subfibular impingement but will not deal directly with subtalar joint arthrosis and deformity. Carr JB, Hansen ST , Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86. Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 46
An 8-year-old boy falls and injures his thumb. A radiograph is shown in Figure 23. Initial management should consist of





Explanation
The radiograph shows a complete simple dislocation of the metacarpophalangeal joint. The clue to this injury is the perpendicular alignment of the proximal phalanx to the metacarpal on the lateral radiograph. This must be differentiated from the complete complex dislocation pattern that is irreducible because of the interposed volar plate. In lateral radiographs of these injuries, the long axes of the proximal phalanx and the metacarpal are parallel. Simple dislocations are amenable to closed reduction and casting. Some authors have recommended ulnar collateral ligament repair if instability is detected on examination after reduction. O'Brien ET: Part IV: Dislocations of hand and carpus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 429-431.
Question 47
A 28-year-old anesthesia resident has aching pain in his dominant right forearm after injuring it while playing basketball 1 week ago. He reports that he is unable to perform regional anesthesia that requires manipulation of a needle. Examination reveals that he is unable to flex the interphalangeal joint of the thumb, and flexion of the distal interphalangeal joint of the index finger is weak. Management should consist of

Explanation
The patient has anterior interosseous nerve palsy. Initial management should consist of splinting followed by observation; surgical decompression may be required if there is no improvement in the functional deficit in 6 months. Anterior interosseous nerve palsy is classically described as an inability to flex the interphalangeal joint of the thumb because of flexor pollicis longus paralysis and a weakness or inability to flex the distal interphalangeal joint of the index finger because of weakness and/or paralysis of the flexor digitorum profundus to the index finger. There has been some controversy in the literature as to whether this represents a true peripheral compression neuropathy or neuritis. Recent recommendations have been to extend the period of observation from 3 to 6 months before surgical decompression, as most cases will resolve within 6 months. Miller-Breslow A, Terrono A, Millender LH: Nonoperative treatment of anterior interosseous nerve paralysis. J Hand Surg Am 1990;15:493-496.
Question 48
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of



Explanation
In this age group, bayonet apposition can produce very good results. Healing occurs rapidly, and remodeling usually is complete in less than 1 year. All of the other methods have significant risks of complications and are unnecessary for this fracture. Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 144-148.
Question 49
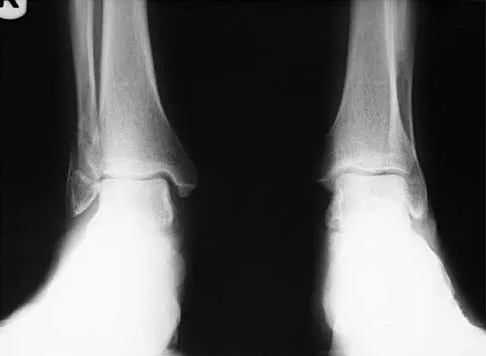
The cortical injury to the posterolateral distal fibula shown in Figure 25 indicates involvement of which of the following structures?

Explanation
The patient has a rim avulsion fracture that is the result of a forceful twisting injury as the superior peroneal retinaculum is avulsed from its fibular attachment along with a small rim of bone. Injuries to the anterior talofibular ligament or calcaneal fibular ligament would show cortical avulsions more anteriorly or distally at the fibular tip. Deltoid ligament injuries would reveal medial radiographic changes. In a true injury to the syndesmosis, if osseous structures do show avulsion, it would be more directly posterior or anterior on the distal fibula or would occur on the tibial surface. Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Question 50
A 52-year-old woman underwent open reduction and internal fixation for radial and ulnar shaft fractures 2 months ago. In a second fall she refractured her forearm and required revision surgery with bone grafting. One month after the second operation she notes erythema, swelling, and drainage from the volar radial incision. In addition to antibiotic treatment, management should consist of
Explanation
Deep infections after plating of closed fractures of the forearm are unusual. However, the risk increases with repeat surgeries. Debridement of all infected, nonviable tissue is the initial step in management. The fixation may be retained if it is stable, but if the plate and screws are loose, they should be removed and revision performed after removal of nonviable bone. Either external fixation or repeat plating may be performed. Late infections after fracture union may be treated with plate and screw removal, debridement, and IV antibiotics. Kellam JF, Fischer TJ, Tornetta P III, Bosse MJ, Harris MB (eds): Orthopaedic Knowledge Update: Trauma 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 53-63. Moed BR, Kellam JF, Foster RJ, Tile M, Hansen ST Jr: Immediate internal fixation of open fractures of the diaphysis of the forearm. J Bone Joint Surg Am 1986;68:1008-1017.
Finish Exam?
You cannot change answers after submitting.
