Question 1
A 36-year-old woman sustained a tarsometatarsal joint fracture-dislocation in a motor vehicle accident. The patient is treated with open reduction and internal fixation. What is the most common complication?

Explanation
The most common complication associated with tarsometatarsal joint injury is posttraumatic arthritis. In one series, symptomatic arthritis developed in 25% of the patients and half of those went on to fusion. In another series, 26% had painful arthritis. Initial treatment should consist of shoe modification, inserts, and anti-inflammatory drugs. Fusion is reserved for failure of nonsurgical management. Hardware failure may occur, but it is clinically unimportant. Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618. Arntz CT, Veith RG, Hansen ST Jr: Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am 1988;70:173-181.
Question 2
What is the most appropriate indication for replantation in an otherwise healthy 35-year-old man?


Explanation
Vascular anastamoses are exceedingly difficult with amputations distal to the nail fold as the digital vessels bifurcate or trifurcate at this level, and little functional benefit is gained compared to other means of soft-tissue coverage. Single digit amputations, other than the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time of less than 6 hours. Urbaniak JR: Replantation, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1085.
Question 3
Figure 1 shows the radiograph of an 11-year-old boy who stubbed his great toe while playing soccer barefoot. He is able to walk home despite a small amount of bleeding at the nail fold. Management should consist of


Explanation
Great toe fractures through the physis should be considered open fractures if there is bleeding at the nail fold. Treatment should include irrigation and debridement and appropriate antibiotics. Immobilization with a cast is usually sufficient for treatment of the fracture. Noonan KJ, Saltzman CL, Dietz FR: Open physeal fractures of the distal phalanx of the great toe: A case report. J Bone Joint Surg Am 1994;76:122-125.
Question 4
Figure 2a shows the radiograph of a 48-year-old man who was involved in a motorcycle accident. A CT scan is shown in Figure 2b. The patient underwent pelvic angiography for persistent hypotension despite resuscitation. What vessel is most likely to be injured?



Explanation
2b The pelvic injury is a severe anterior-posterior compression III or Tile C injury. The vessel most likely injured is the superior gluteal artery, but several arterial bleeding sources are likely. Vertical shear injuries can also injure this vessel, but it is much less common. When arterial injury follows a lateral compression injury, it is usually related to injury of a more anterior vessel like the obturator artery or a branch of the external iliac artery. O'Neill PA, Riina J, Sclafani S, et al: Angiographic findings in pelvic fractures. Clin Orthop 1996;329:60-67.
Question 5
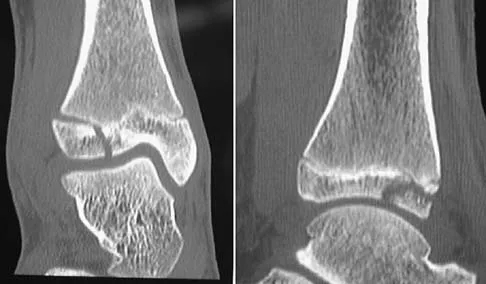
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of


Explanation
Although this is a fracture of the medial and lateral malleoli, the degree of displacement and comminution of the medial dome indicate that this injury is similar to a pilon fracture. Initial management should consistent of stabilization to allow for soft-tissue healing. The use of temporizing spanning external fixation should be the initial step, followed by limited or more extensive open reduction and internal fixation when the soft-tissue status will allow. Initial placement in either a short or long leg cast does not provide the needed stability and does not allow for care and monitoring of soft tissues. In addition, maintaining reduction of the talus may be very difficult. Immediate open reduction and internal fixation through an injured soft-tissue envelope adds the risk of difficulties with incision healing and a higher risk of deep infection. In the acute setting, a primary ankle fusion through this soft-tissue envelope is not indicated. Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509. Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Question 6
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?



Explanation
Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60. Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292. Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
Question 7
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?




Explanation
Excision of the fracture fragment typically leads to rapid return to function. Fixation techniques are difficult to perform because of the size of the bone; hardware prominence is common. Nerve deficits are not typically noted in this injury. The motor branch of the ulnar nerve in Guyon's canal must be protected during the surgical approach. Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Question 8
In an acute closed boutonniere injury, what is the most appropriate splinting technique for the proximal interphalangeal joint?

Explanation
Rupture of the central slip of the extensor mechanism and a varying degree of lateral band volar migration are the pathologic entities in an acute boutonniere injury. Splinting the proximal interphalangeal joint in full extension allows reapproximation of the central slip to the base of the middle phalanx. Distal interphalangeal joint flexion is permitted to allow movement of the lateral bands distally and dorsally, preventing contracture. Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Question 9
A 20-year-old man sustained a closed tibial fracture and is treated with a reamed intramedullary nail. What is the most common complication associated with this treatment?


Explanation
The most common complication is anterior knee pain (57%). The knee pain is activity related (92%) and exacerbated by kneeling (83%). Although knee pain is the most common complication, most patients rate it as mild to moderate and only 10% are unable to return to previous employment. Some authors report less knee pain with a peritendinous approach when compared to a tendon-splitting approach. In one study, nail removal resolved pain in 27%, improved it in 70%, and made it worse in 3%. The incidence of the other complications was: infection 0% to 3%, nonunion 0% to 6%, and malunion 2% to 13%. Compartment syndrome is rare after nailing. Court-Brown CM: Reamed intramedullary tibial nailing: An overview and analysis of 1106 cases. J Orthop Trauma 2004;18:96-101. McQueen MM, Gaston P, Court-Brown CM: Acute compartment syndrome: Who is at risk? J Bone Joint Surg Br 2000;82:200-203.
Question 10
An 8-year-old boy sustained an isolated distal radial fracture that was reduced and immobilized with 10 degrees of residual dorsal tilt. What is the next step in management?



Explanation
Distal radial fractures in children are common, and a large amount of displacement is acceptable. In general, 20 degrees of dorsal displacement and complete bayonet apposition in girls to age 12 years and in boys to age 14 years can be expected to remodel with an excellent outcome. The potential for increased fracture displacement and subsequent malunion may exist in up to one third of patients with displaced fractures with less than anatomic reduction. Therefore, early follow-up is recommended and remanipulation is indicated should loss in reduction occur. Consideration for percutaneous pinning of isolated distal radial fracture is reasonable in patients with little growth remaining. In these patients, higher rates of redisplacement exist with little chance for remodeling. Gibbons CL, Woods DA, Pailthorpe C, et al: The management of isolated distal radius fractures in children. J Pediatr Orthop 1994;14:207-210. McLauchlan GJ, Cowan B, Annan IH, et al: Management of completely displaced metaphyseal fractures of the distal radius in children. J Bone Joint Surg Br 2002;84:413-417. Proctor MT, Moore DJ, Patterson JH: Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br 1993;75:453-454.
Question 11
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?


Explanation
According to a study by the Scoliosis Research Society, the use of anterior decompression is most predictable for improving neurologic status. This is particularly true of bowel and bladder functional loss. Laminectomy is contraindicated because it further destabilizes the spine. Posterior instrumentation and indirect reduction through distraction and ligamentotaxis only incompletely decompress the compromised canal and are successful only if performed within 48 hours of injury. While some improvement may occur with closed management, the amount of recovery is less than that achieved with surgical decompression. A posterior approach and instrumentation may be added to the anterior decompression based on the characteristics of associated injuries to the posterior element. Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Question 12
What is the most likely complication following treatment of the humeral shaft fracture shown in Figure 6?





Explanation
The humerus was treated with an intramedullary nail. Findings from two prospective randomized studies of intramedullary nailing or compression plating of acute humeral fractures have shown approximately a 30% incidence of shoulder pain with antegrade humeral nailing. This is the most common complication in both of these series. Nonunions are present in approximately 5% to 10% of humeral fractures treated with an intramedullary nail. Infection has an incidence of approximately 1%. Elbow injury is unlikely unless the nail is excessively long. Rarely, injury to the radial nerve is possible if it is trapped in the intramedullary canal. Chapman JR, Henley MB, Agel J, et al: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166.
Question 13
A 4-year-old girl sustains an isolated spiral femoral fracture after falling from her tricycle. Management should consist of



Explanation
Immediate spica casting is ideal for younger children with uncomplicated femoral fractures that are the result of relatively low-energy injury. Surgical stabilization of pediatric femoral fractures is most commonly performed in children who are older than age 6 years or in children with other factors associated with their femoral fracture, such as concomitant head injury, open fracture, floating knee, severe comminution, or vascular injury. Flynn JM, Skaggs DL, Sponseller PD, et al: The surgical management of pediatric fractures of the lower extremity. Instr Course Lect 2003;52:647-659. Sponseller PD: Surgical management of pediatric femoral fractures. Instr Course Lect 2002;51:361-365. Wright JG: The treatment of femoral shaft fractures in children: A systematic overview and critical appraisal of the literature. Can J Surg 2000;43:180-189.
Question 14
A 16-year-old girl sustained the injury shown in Figure 7a. CT scans are shown in Figures 7b through 7d. The results of treatment of this injury have been shown to most correlate with which of the following factors?







Explanation
7b 7c 7d The patient has a very low T-type acetabular fracture; however, the head is not congruent under the dome so surgical reduction is necessary. The anterior and posterior columns are displaced and will move independent from each other. The extended iliofemoral is the only approach allowing for visualization and reduction of each column. A combined anterior and posterior approach may also be used. The timing of surgery should be within the first 3 weeks of injury to optimize chances of obtaining an accurate reduction because this is an important factor in determining outcome. Letournel E, Judet R (eds): Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer-Verlag, 1991.
Question 15
An 18-month-old child sustains a crush amputation of the tip of the index finger. Bone is exposed, but the nail is intact. Management should consist of


Explanation
Children have a much greater capacity to heal soft-tissue injuries than adults. Most crush or avulsion fingertip amputations in children, particularly those younger than age 2 years, can be treated with serial dressing changes, even with bone exposed. Das SK, Brown HG: Management of lost finger tips in children. Hand 1978;10:16-27.
Question 16
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a


Explanation
The wound described indicates loss of soft tissue directly to the level of the tendon, precluding use of skin grafts if excursion of the tendon is desired. A cross-finger flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb. Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
Question 17
An active 49-year-old woman who sustained a diaphyseal fracture of the clavicle 8 months ago now reports persistent shoulder pain with daily activities. An AP radiograph is shown in Figure 8. Management should consist of

Explanation
The radiograph reveals an atrophic nonunion of the diaphysis of the clavicle. Electrical or ultrasound stimulation may be an option in diaphyseal nonunions that have shown some healing response with callus formation, but these techniques are not successful in an atrophic nonunion. The preferred technique for achieving union is open reduction and internal fixation with bone graft. Percutaneous fixation has no role in treatment of nonunions of the clavicle. Boyer MI, Axelrod TS: Atrophic nonunion of the clavicle: Treatment by compression plating, lag-screw fixation and bone graft. J Bone Joint Surg Br 1997;79:301-303.
Question 18
Examination of a 25-year-old man who was injured in a motor vehicle accident reveals a fracture-dislocation of C5-6 with a Frankel B spinal cord injury. He also has a closed right femoral shaft fracture and a grade II open ipsilateral midshaft tibial fracture. Assessment of his vital signs reveals a pulse rate of 45/min, a blood pressure of 80/45 mm Hg, and respirations of 25/min. A general surgeon has assessed the abdomen, and a peritoneal lavage is negative. His clinical presentation is most consistent with what type of shock?


Explanation
Assessment of the acutely injured patient follows the Advanced Trauma Life Support protocol. Cervical cord injury is often associated with a disruption in sympathetic outflow. Absent sympathetic input to the lower extremities leads to vasodilatation, decreased venous return to the heart, and subsequent hypotension. With hypotension, the physiologic response of tachycardia is not possible because of the unopposed vagal tone. This results in bradycardia. Patient positioning, fluid support, pressor agents, and atropine are used to treat neurogenic shock.
Question 19
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include



Explanation
9b With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient's physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 20
A patient sustained the injuries shown in the radiographs and clinical photograph seen in Figures 10a through 10c. The neurovascular examination is normal. The first step in emergent management of the extremity injuries should consist of






Explanation
10b 10c The figures show an open tibial fracture, a femoral shaft fracture, and femoral head dislocation. The most urgent treatment is reduction of the femoral head, as timing to reduction has been correlated with preventing osteonecrosis. After reduction of the femoral head, the next priority is wound management, followed by stabilization of the femoral and tibial fractures with either splinting, traction, or external fixation. Sahin V, Karakas ES, Aksu S, et al: Traumatic dislocation and fracture-dislocation of the hip: A long-term follow-up study. J Trauma 2003;54:520-529.
Question 21
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include



Explanation
The patient has a displaced radial neck fracture. Displaced radial neck fractures with angulation of more than 30 to 45 degrees require reduction. Methods of attempted closed reduction include wrapping the arm with an Esmarch's bandage and applying direct pressure over the maximum deformity of the radial head. More aggressive methods include a Kirschner wire used as a joystick or intramedullary reduction as described by the Metaizeau technique. Open reduction should be avoided because of complications such as stiffness or osteonecrosis. Indications for open reduction are irreducible displacement of more than 45 degrees with severe restriction of forearm rotation. Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop 2000;20:7-14. Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39. Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Question 22
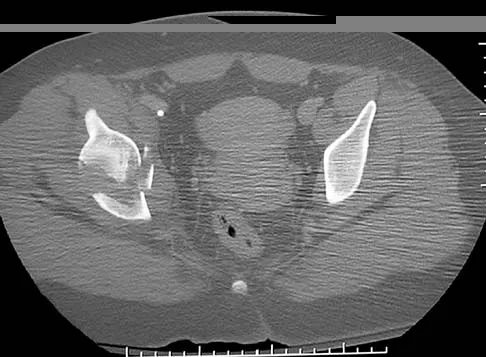
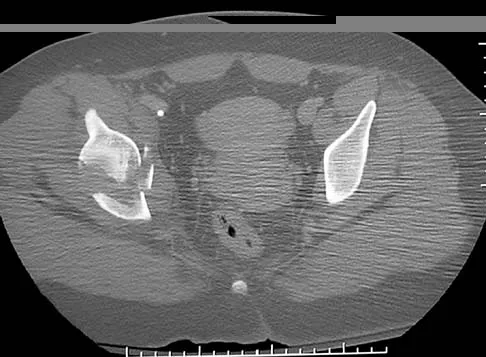
Figures 12a and 12b show the radiographs of a 56-year-old man with diabetes mellitus who has had left foot swelling with no pain for the past several weeks. He denies any history of trauma. Examination reveals warmth, moderate swelling, no tenderness, and mild pes planus with standing. Pulses are palpable, and his sensory examination is grossly intact to light touch. Standing radiographs are shown in Figures 12c and 12d. What is the most likely diagnosis?






Explanation
12b 12c 12d The radiographs show tarsometatarsal joint subluxation without fragmentation. The clinical history and delay in presentation with the radiographic findings suggest a neuropathic or Charcot arthropathy involving the midfoot area. Intact sensory examination to light touch is not diagnostic for an intact peripheral neurologic system; monofilament testing is a more accurate office baseline examination for the presence of sensory peripheral neuropathy. With an acute traumatic Lisfranc fracture-dislocation, a history of a traumatic event is necessary, and radiographic abnormalities are expected, although nonstanding radiographs still may be misleading. Acquired pes planus due to posterior tibial tendon rupture may have negative nonstanding radiographs. Standing radiographs may reveal pes planus. However, intermetatarsal disruption is not expected as seen in a Lisfranc abnormality. Localized osteomyelitis of the foot without a penetrating injury or cutaneous ulceration is extremely unlikely and does not fit with the clinical picture described. An isolated metatarsal stress fracture would show osseous irregularity without the instability pattern pictured. Brodsky JW: The diabetic foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 895-969.
Question 23
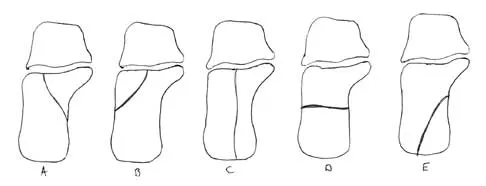
A 25-year-old student sustains the injury shown in Figures 13a through 13c after falling off a curb. Initial management should consist of




Explanation
13b 13c The radiographs reveal a fracture entering the 4-5 intermetatarsal articulation, consistent with a zone 2 injury. This classically is also referred to as a Jones fracture. The history and radiographic findings indicate this is an acute fracture, which guides management. A zone 1 fracture enters the fifth tarsometatarsal joint, and a zone 3 fracture is a proximal diaphyseal fracture distal to the 4-5 articulation. Initial management is usually nonsurgical and consists of non-weight-bearing in a short leg cast. This method has been shown to result in a better healing rate compared to weight bearing as tolerated. Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
Question 24
What structure is most often injured in a volar proximal interphalangeal joint dislocation?


Explanation
Closed ruptures of the central slip of the extensor tendon may occur with volar proximal interphalangeal joint dislocation, forced flexion of the proximal interphalangeal joint, or blunt trauma to the dorsum of the proximal interphalangeal joint. The other structures are not typically injured in proximal interphalangeal joint dislocations. Treatment typically requires static splinting of the proximal interphalangeal joint. In the more common dorsal proximal interphalangeal joint dislocation, the volar plate is injured, and early range of motion may be started after reduction. Doyle JR: Extensor tendons: Acute injuries, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1925.
Question 25
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?
Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Finish Exam?
You cannot change answers after submitting.
