HY 2026
00:00
Start Quiz
Question 801
High Yield
Figure 42 shows the sagittal T2-weighted MRI scan of a patient's right knee. These findings are most commonly seen with a complete tear of the

Explanation
The MRI scan reveals disruption of the lateral capsule and ligaments with fluid in the soft tissues laterally. Additionally, there is a large bone bruise on the medial femoral condyle. This combination indicates injury to the posterolateral complex. These injuries often have coexisting anterior and/or posterior cruciate ligament injuries. Failure to recognize the posterolateral corner injury can lead to failure of anterior or posterior cruciate ligament reconstructions. LaPrade RF, Gilbert TJ, Bollom TS, et al: The magnetic resonance imaging appearance of individual structures of the posterolateral knee: A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 2000;28:191-199.
Question 802
High Yield
Which of the following pharmacologic agents is most likely to adversely affect the success rate of bony union after lumbar arthrodesis?
Explanation
Glassman and associates reported a significantly higher pseudarthrosis rate when ketorolac was used postoperatively compared to a similar group of patients who were not given ketorolac. Animal studies from the same institution support these clinical findings. To reduce narcotic dosage, nonsteroidal anti-inflammatory drugs (NSAIDs) have been promoted as an adjunct for postoperative analgesia in patients undergoing spinal fusion. However, a high failure rate of arthrodesis has been associated with postoperative use of NSAIDs. The analgesics oxycodone hydrochloride, hydrocodone/acetaminophen, and tramadol, as well as the tricyclic antidepressant imipramine, have not been shown to inhibit fusion. Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Question 803
High Yield
A 45-year-old man sustains a low-velocity gunshot wound to the base of the right thumb. The open wound is allowed to heal by secondary intention, resulting in a contracture of the first web space. Clinical photographs are shown in Figures 49a through 49c. Treatment should now consist of



Explanation
The contracture is too large for a Z-plasty, which allows a 75% increase in length. Excision of the scar with placement of a skin graft is prone to contracture. A posterior interosseous fasciocutaneous flap will provide enough well-vascularized tissue and is well suited to reach the first dorsal web space. Buchler U, Frey HP: Retrograde posterior interosseous flap. J Hand Surg Am 1991;16:283-292.
Question 804
High Yield
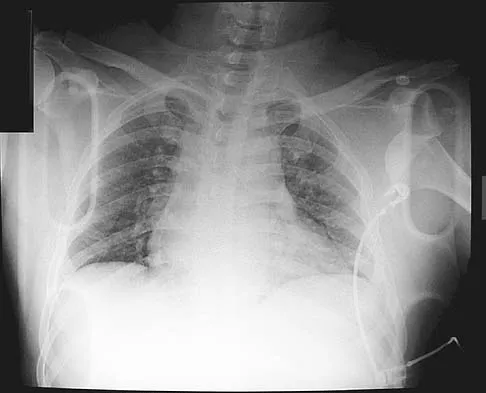
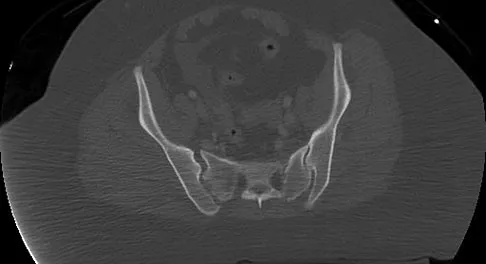
Figure 11 shows the radiograph of a 26-year-old man with type I diabetes mellitus who was struck by a motor vehicle. What is the most common complication associated with this pelvic fracture?

Explanation
The most common complication following acetabular or pelvic ring injury is deep venous thrombosis (DVT). Without prophylaxis, rates of DVT are as high as 70% to 80%. With prophylaxis, the rates are around 10%. Infection rates in surgical repair of acetabular fractures are relatively low but a history of diabetes mellitus and a significant Morel-Lavalle lesion certainly increase the risk. However, even with these two complicating factors, the rates of infection are still lower than 10%. Sciatic nerve palsy rates from the injury alone approach 20% and iatrogenic injury is usually less than 2%. Degenerative changes to the hip following this injury approach 20% to 25%, even with an anatomic reduction. Geerts WH, Code KI, Jay RM, et al: A prospective study of venous thromboembolism after major trauma. N Engl J Med 1994;331:1601-1606.
Question 805
High Yield
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?



Explanation
In the presence of a supination external rotation-type fracture of the distal fibula (Weber type B), stability of the ankle is best assessed by performing an external rotation stress AP view of the ankle. This test is used to assess the integrity of the deltoid ligament. The presence of a deltoid ligament rupture results in instability and generally is best managed surgically. The gravity stress test can also be used. Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398. McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Question 806
High Yield
Which of the following properties apply to the human meniscus when compared with articular cartilage?

Explanation
The meniscal cartilage, like articular cartilage, possesses viscoelastic properties. The extracellular matrix is a biphasic structure composed of a solid phase (collagen, proteoglycan) that acts as a fiber-reinforced porous-permeable composite, and a fluid phase that may be forced through the solid matrix by a hydraulic pressure gradient. Although these properties are shared with articular cartilage, the meniscus is more elastic and less permeable than articular cartilage. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 3-23.
Question 807
High Yield
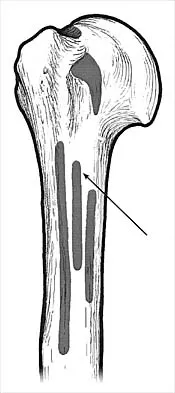
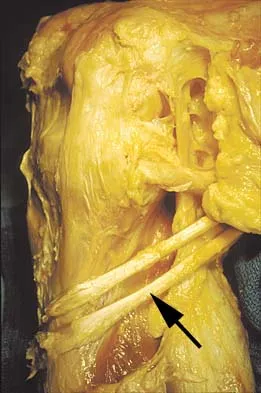
What muscle attaches to the site shown by the arrow in Figure 2?
Explanation
The latissimus dorsi inserts on the humerus metaphysis between the pectoralis major (posterior) and teres major (anterior). Teres minor inserts on the base of the greater tuberosity. Pectoralis minor does not insert on the humerus. Williams PL, Warwick R, Dyson M, Bannister LH: Neurology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 1131-1132.
Question 808
High Yield
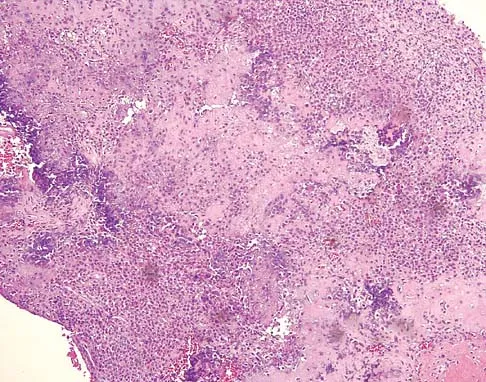
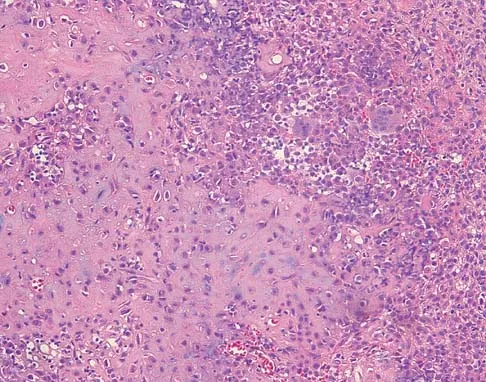
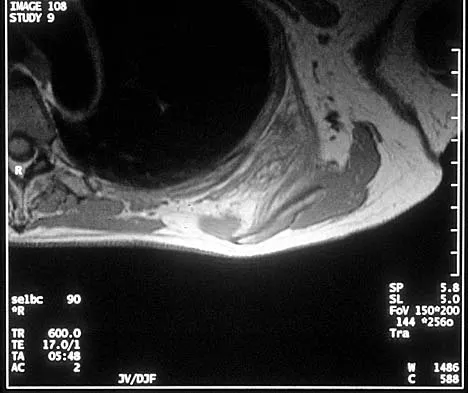
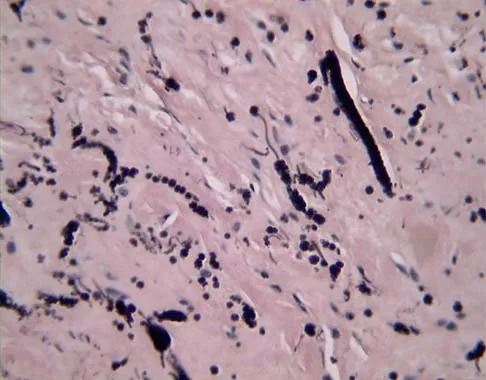
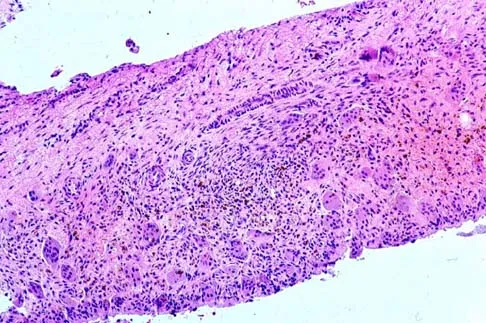
A 16-year-old girl has had pain in the left groin for the past 4 months. She notes that the pain is worse at night; however, she denies any history of trauma and has no constitutional symptoms. There is no history of steroid or alcohol use. Examination reveals pain in the left groin with rotation of the hip. There is no associated soft-tissue mass. A radiograph and MRI scan are shown in Figures 32a and 32b, and biopsy specimens are shown in Figures 32c and 32d. What is the most likely diagnosis?


Explanation
Based on the epiphyseal location and sharp, well-defined borders, the radiograph suggests chondroblastoma. Histologically, multinucleated giant cells are scattered among mononuclear cells. The nuclei are homogenous and contain a characteristic longitudinal groove. Although not seen here, "chicken-wire calcification" with a bland giant cell-rich matrix is also typical for chondroblastoma. Clear cell chondrosarcoma occurs in epiphyseal locations but has a more aggressive histologic pattern and occurs in an older age group. Giant cell tumors occur in the epiphysis but have a more uniform giant cell population histologically. Aneurysmal bone cyst often results in bone remodeling and has a different pathologic appearance. Osteonecrosis has a typical histologic pattern of empty lacunae and necrotic bone. Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755. Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Question 809
High Yield
Figures 33a and 33b show the radiographs of a 10-year-old girl who reports a 4-month history of medial foot pain after she was kicked while playing soccer. The pain is worse with activity and partially relieved by rest. Examination reveals tenderness directly over a prominent navicular tuberosity. Management should consist of


Explanation
An accessory tarsal navicular is located at the medial tuberosity of the navicular bone. Nearly all children and adolescents who have a symptomatic accessory tarsal navicular bone become asymptomatic when they reach skeletal maturity. Initial management should include activity restrictions, shoe modification to avoid pressure over the prominent navicular, and non-narcotic analgesics. Although anecdotal, the use of arch supports may be helpful. When pain is refractory to these methods, a short period of cast immobilization may be useful. Surgery should be reserved for patients who have disabling symptoms despite a prolonged period of nonsurgical management. When surgery is indicated, simple excision of the accessory navicular is recommended. Sella EJ, Lawson JP, Ogden JA: The accessory navicular synchondrosis. Clin Orthop 1986;209:280-285.
Question 810
High Yield
Which of the following nutraceuticals has been associated with perioperative bleeding?

Explanation
Ginkgo biloba is a popular nutraceutical for patients who have early dementia, intermittent claudication secondary to peripheral vascular disease, vertigo, and tinnitus. It is reported to improve mental alertness and cognitive deficiency. It has antiplatelet properties as a result of one of its components, ginkgolide B, which displaces platelet-activating factor from its receptor binding sight. Rowin and Lewis reported on spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Vale also reported on subarachnoid hemorrhage associated with ginkgo biloba. Bebbington and associates reported on persistent postoperative bleeding after total hip arthroplasty secondary to ginkgo biloba usage. Furthermore, the use of ginkgo biloba with aspirin or other antiplatelet agents or anticoagulants represents a relative contraindication. Physicians should be aware not only of prescribed medications but also alternative nutraceuticals that are used by the patient. Rowin J, Lewis SL: Spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Neurology 1996;46:1775-1776. Vale S: Subarachnoid hemorrhage associated with ginkgo biloba. Lancet 1998;352:36.
Question 811
High Yield
Compared to postoperative radiation therapy, preoperative radiation therapy has a higher rate of what complication?

Explanation
Radiation therapy is commonly used as an adjuvant in the treatment of soft-tissue sarcomas, but a controversy exists whether it should be preoperative or postoperative. Radiation therapy can be given prior to or following resection of the tumor. Postoperative radiation is usually given in a higher dose to a larger treatment field. This commonly results in a higher incidence of fibrosis and lymphedema. There is no statistical difference in local recurrence rate between the two radiation treatment plans. Neuropathy is more commonly a complication of chemotherapy. Preoperative radiation therapy has been shown to have a higher wound complication rate than postoperative radiation. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Question 812
High Yield
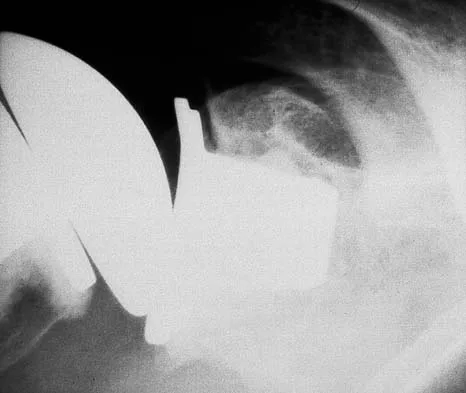
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure 5. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion?

Explanation
Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humeral fractures in patients older than age 70 years. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight of more than 5 pounds must be followed to avoid loosening. Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Question 813
High Yield
An acetabular reinforcement cage is most often indicated for which of the following conditions?
Explanation
An acetabular reinforcement cage is required infrequently except when there is pelvic discontinuity in which there is no posterior column support of the acetabular cup. A larger cup inserted with cement and morselized bone graft is an effective technique for contained cavitary and anterior wall defects. Zone 1 osteolysis and a medial wall defect are essentially the same as a contained cavitary defect and can be reconstructed using cementless cups. Berry DJ, Lewallen DG, Hanssen A, Cabanela ME: Pelvic discontinuity in revision total hip arthroplasty. J Bone Joint Surg Am 1999;81:1692-1702.
Question 814
High Yield
Figure 1 shows the radiograph of an 11-year-old boy who stubbed his great toe while playing soccer barefoot. He is able to walk home despite a small amount of bleeding at the nail fold. Management should consist of

Explanation
Great toe fractures through the physis should be considered open fractures if there is bleeding at the nail fold. Treatment should include irrigation and debridement and appropriate antibiotics. Immobilization with a cast is usually sufficient for treatment of the fracture. Noonan KJ, Saltzman CL, Dietz FR: Open physeal fractures of the distal phalanx of the great toe: A case report. J Bone Joint Surg Am 1994;76:122-125.
Question 815
High Yield
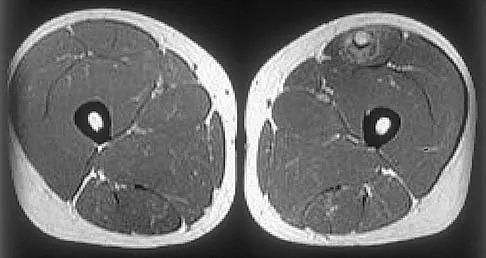
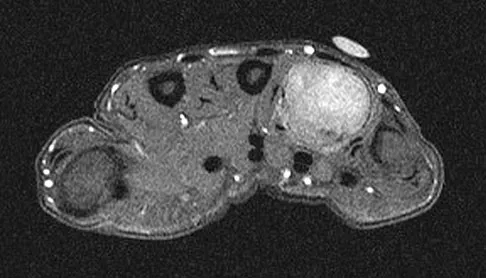
Figures 34a through 34c show an axial proton density (spin echo long TR, short TE) image, a sagittal inversion recovery (STIR) image, and a sagittal T1-weighted (short TR, short TE) image of the left thigh. What is the most likely diagnosis?


Explanation
The images reveal a region of increased signal within the rectus femoris muscle with mild, ill-defined surrounding edema. The presence of high intensity signal on the T1-weighted image favors acute blood, in this case associated with a rectus femoris muscle tear or fatty tissue. However, because of fat suppression, a fatty lesion or lipoma would be dark on STIR, rather than bright as in this image. Most foreign bodies are low intensity signal and if small, are difficult to evaluate with MRI. The lack of adjacent subcutaneous soft-tissue edema or surrounding fluid makes pyomyositis an unlikely diagnosis.
Question 816
High Yield
A 44-year-old woman has had lower extremity dysesthesias, urinary incontinence, and has been unable to walk for the past 2 days. She reports no pain or history of trauma. She notes that 3 weeks ago she missed work for 2 days because of back pain, but it resolved with rest. Examination shows decreased or absent sensation below the knees, no motor function below the knees, and decreased rectal tone. Catheterization results in a postvoid residual of 2,000 mL. Plain radiographs and MRI scans without contrast are shown in Figures 1a through 1d. What is the next most appropriate step in management?




Explanation
The patient has had a clear and sudden onset of a profound neurologic deficit. The radiographic studies suggest a lesion in the conus medullaris that appears to be intradural and intramedullary. MRI, with and without contrast, will best evaluate this mass further. The addition of gadolinium allows further evaluation of vascularity and the extent of the lesion. Eichler ME, Dacey RG: Intramedullary spinal cord tumors, in Bridwell KH, Dewald RL (eds): The Textbook of Spine Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, vol 2, pp 2089-2116.
Question 817
High Yield
What structure is most at risk for injury from a retractor against the tracheoesophageal junction during an anterior approach to the cervical spine?
Explanation
Although any of these structures can be injured by pressure from the medial blade of a self-retaining retractor, the recurrent laryngeal nerve runs cephalad in the interval between the esophagus and trachea and is vulnerable to pressure if caught between the retractor and an inflated endotracheal tube balloon. Ebraheim NA, Lu J, Skie M, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine. Spine 1997;22:2664-2667.
Question 818
High Yield
What part of the glenoid labrum has the least vascularity?
Explanation
The glenoid labrum receives its blood supply from the suprascapular, posterior humeral circumflex, and circumflex scapular arteries. The labral vessels arise from the capsular and periosteal vessels that penetrate the periphery of the labrum. The bone does not appear to be a source of vascularity. The posterior/superior and inferior labrum have a fairly robust vascular supply, whereas the anterior/superior labrum has relatively poor vascularity, which may influence the success of superior lateral repairs.
Question 819
High Yield
A 58-year-old woman has had a painless periscapular mass for the past year. An MRI scan and biopsy specimen are shown in Figures 4a and 4b. What is the most likely diagnosis?
Explanation
Elastofibroma is a rare tumor that most commonly occurs in adults who are older than age 55 years. The lesions usually grow between the chest wall and the scapula, and 10% are bilateral. Histologic analysis shows that they are composed of equal amounts of elastin and collagen with occasional fibroblasts. Briccoli A, Casadei R, Di Renzo M, Favale L, Bacchini P, Bertoni F: Elastofibroma dorsi. Surg Today 2000;30:147-152.
Question 820
High Yield
What is the main function of collagen found within articular cartilage?

Explanation
The main function of collagen in articular cartilage is to provide the tissue's tensile strength. It also immobilizes proteoglycans within the extracellular matrix. Compressive properties are maintained by proteoglycans. Cartilage metabolism is maintained by the indwelling chondrocytes. The flow of water through the tissue promotes transport of nutrients and provides a source of lubricant for the joint. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 3-44.
Question 821
High Yield
A 25-year-old carpenter falls on his outstretched arm. What physical finding best correlates with the lesion seen on the MRI scan shown in Figure 3?

Explanation
The MRI scan shows disruption of the subscapularis muscle. Subscapularis rupture is associated with weakness in internal rotation as shown with a positive lift-off test as described by Gerber and Krushell. The belly press test also has been shown to be a useful clinical test for this problem. Weakness in external rotation and abduction is more consistent with supraspinatus and infraspinatus tears. Deltoid atrophy is associated with an axillary nerve injury. Loss of biceps contour is associated with rupture of the long head of the biceps. Gerber C, Krushell RJ: Isolated rupture of the tendon of the subscapularis muscle: Clinical features in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 822
High Yield
Which of the following radiographic views best depicts a Hill-Sachs defect?

Explanation
The Stryker notch view best shows this type of defect. An outlet view helps evaluate acromial shape, a true AP shows joint space narrowing, a serendipity view evaluates the sternoclavicular joint, and a Zanca view helps evaluate the acromioclavicular joint. An internal rotation AP may also depict a Hill-Sachs defect.
Question 823
High Yield
Which of the following surgical devices employed for stabilization of the sternoclavicular joint is associated with the highest incidence of life-threatening complications?

Explanation
Numerous reports have documented serious complications including death from migration of intact or broken Kirschner wires or Steinmann pins into hilar structures such as the heart, pulmonary artery, and the aorta. Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
Question 824
High Yield
Compared with wear rates of metal-on-standard polyethylene bearings (75 to 250 um/y), the wear rate of metal-on-metal bearings for hip arthroplasty is approximately how many micrometers per year?
Explanation
Studies on older systems, as well as newer designs, have confirmed that metal-on-metal bearing surfaces undergo linear wear of 2 to 5 um per year. Ceramic bearing surfaces produced with recent technology perform even better, with a wear rate of 0.5 to 2.5 um per year. Clinical wear rates of metal-on-crosslinked polyethylene have not yet been determined. McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Question 825
High Yield
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Explanation
Chondrocytes are obtained from cartilage harvested from non-weight-bearing areas of the knee. The extracellular matrix is digested, and the chondrocytes are expanded for later transplantation. Cells implanted into a defect are secured with a flap of periosteum. Cells are expanded to obtain 20 to 50 times the original number of cells to transplant at a cell density of 3x10-7 cells/mL. There is a direct relationship between cell number and biosynthetic activity. Osteochondral lesions of up to 8 mm may be treated with autologous transplant alone; larger depth lesions should be bone grafted at the time of harvest. Mesenchymal stem cells differentiate easily into fibrous tissue, bone, and fat; conversion of mesenchymal stem cells into cartilage in vitro currently is difficult to accomplish. Goldberg and Caplan, however, were able to obtain cartilage repair using mesenchymal stem cells transplanted into defects in rabbits in vivo. In animal studies, fluorescent-labeled cells persist for at least 14 weeks, integrate with the surrounding normal margins, and become part of the repaired tissue replete with sulfated proteoglycans and type II collagen. Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am 2003;85:109-115.
Question 826
High Yield
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?

Explanation
In patients with flexion-distraction injuries of the thoracolumbar spine, 50% have associated, potentially life-threatening, visceral injuries that occasionally are diagnosed hours or even days after admission. Based on these findings, consultation with a general surgeon is recommended. Blunt and penetrating injuries to the cardiopulmonary system or aorta sometimes can be seen with this type of injury, but they are no more common than with other types of thoracolumbar fractures because of the relatively mild bony injury anteriorly. Neurologic trauma with this type of fracture is also somewhat rare. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 351-360.
Question 827
High Yield
A 40-year-old man has intractable pain following 2 years of nonsurgical management for high-grade spondylolisthesis. What is the best surgical option?

Explanation
Circumferential fusion is the preferred choice for patients undergoing revision surgery following failed posterolateral fusions for isthmic spondylolisthesis as well as for those patients having primary surgery for high-grade isthmic spondylolisthesis.
Question 828
High Yield
A 2-year-old boy has complete absence of the sacrum and lower lumbar spine. What is the most likely long-term outcome if no spinal pelvic stabilization is performed?

Explanation
Without stabilization, progressive kyphosis will develop between the spine and pelvis. The kyphosis progresses to the point that the child must use his or her hands to support the trunk, and therefore is unable to use his or her hands for other activities. Neck extension contracture does not usually develop. Neurologic deficit, including sexual dysfunction, is generally present at birth and static. Tachdjian MO: The spine: Congenital absence of the sacrum and lumbosacral vertebrae (lumbosacral agenesis), in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 3, p 2228.
Question 829
High Yield
A 45-year-old woman has had intense pain in her foot for the last 3 days. She also reports a mild fever and difficulty with shoe wear. Examination reveals a swollen, slightly erythematous warm foot with tenderness at the great toe metatarsophalangeal joint and pain with passive motion of the joint. An AP radiograph is shown in Figure 13. Which of the following will best aid in determining a definitive diagnosis?

Explanation
The patient has gouty arthropathy of the first metatarsophalangeal joint. This definitive diagnosis is achieved with aspiration of the joint and polarized light microscopy that shows needle-shaped negatively birefringent monosodium urate crystals. Differential diagnoses of infectious arthritis and pseudogout are also definitively made through joint aspiration. Although rheumatoid arthritis is a possibility, a serum rheumatoid factor is not always diagnostic and a patient with rheumatoid arthritis may have concomitant gouty arthritis. The radiographic findings are not typical of diabetes mellitus or of a patient with Charcot arthropathy. Wise CM, Agudelo CA: Diagnosis and management of complicated gout. Bull Rheum Dis 1998;47:2-5.
Question 830
High Yield
What nerve is at greatest risk when developing the superficial plane between the tensor fascia lata and sartorious during the anterior (Smith-Peterson) approach to the hip?
Explanation
The lateral femoral cutaneous nerve pierces the fascia between the tensor fascia lata and the sartorius approximately 2.5 cm distal to the anterosuperior iliac spine and is at risk when the interval is defined. The superior gluteal and femoral nerves define the internervous plane between the tensor fascia lata and the sartorius and are not at risk for injury. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia, PA, JB Lippincott, 1984, pp 302-316.
Question 831
High Yield
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of

Explanation
Periosteal new bone formation is a warning sign of prosthetic infection. Indomethacin may prevent heterotopic ossification if given early enough; however, it is irrelevant in this patient. A C-reactive protein and a sed rate are useful screening studies that add to the predictive value of the radiographs and may be performed routinely if sepsis is suspected. A bone scan obtained 4 months after surgery would show increased uptake in all cases. If results of a sed rate and C-reactive protein are normal, then a biopsy should be considered to rule out a neoplasm.
Question 832
High Yield
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Explanation
The patient has a posterolateral rotatory instability (PLRI) of the elbow that is most likely the result of iatrogenic injury to the lateral ulnar collateral ligament, the main ligament implicated in PLRI. The anterior band of the medial collateral ligament is implicated in valgus instability. Injury to the radial nerve is unlikely, and the lateral radial collateral ligament makes less of a contribution to elbow stability than does the ulnar component. While the origin of the extensor carpi radialis brevis may contribute to elbow stability, it is not as important a stabilizer as the lateral ulnohumeral ligament. O'Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
Question 833
High Yield
In surgically treating hand and finger infections in patients with diabetes mellitus, what factor is associated with higher amputation rates?
Explanation
Patients with diabetes mellitus are prone to infection, and surgical treatment of their infections frequently requires multiple procedures. The triad of poor wound healing, chronic neuropathy, and vascular disease contributes to the increased infection rate. Studies have demonstrated increased amputation rates in patients with diabetes mellitus who have renal failure or deep polymicrobial or gram-negative infections. Gonzalez MH, Bochar S, Novotny J, et al: Upper extremity infections in patients with diabetes mellitus. J Hand Surg Am 1999;24:682-686. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 834
High Yield
An 11-year-old boy stepped on a nail and sustained a puncture to the right forefoot 6 days ago. He was wearing tennis shoes at the time of injury. Treatment in the emergency department consisted of local debridement and tetanus prophylaxis; a radiograph was negative for foreign body, chondral defect, or fracture. He was discharged with a 3-day prescription of amoxicillin and clavulanate. The patient now has increasing pain and tenderness at the puncture site. What is the best course of action?
Explanation
The initial treatment consisting of oral antibiotics was appropriate but with progressive symptoms, surgical debridement is necessary. Ciprofloxacin is contraindicated in children, and at this stage, oral antibiotics are inadequate. Intravenous antibiotics may be necessary, but surgical debridement is paramount. Failure to respond to the initial management precludes further observation. Riegler HP, Routson T: Complications of deep puncture wounds of the foot. J Trauma 1979;19:18-22.
Question 835
High Yield
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?

Explanation
C-reactive protein declines rapidly as the clinical picture improves. Failure of the C-reactive protein to decline after 48 to 72 hours of treatment should indicate that treatment may need to be altered. Blood culture is positive only 50% of the time and will be negative soon after antibiotics are administered, even if treatment is not progressing satisfactorily. WBC count is highly variable and poorly correlated with treatment. The ESR rises rapidly but declines too slowly to guide treatment. Radiographic findings may not change but can take up to 2 weeks to show changes.
Question 836
High Yield
The great medullary artery, also known as the Adamkiewicz artery, originates from which of the following arteries?
Explanation
The great medullary artery originates as a direct or indirect branch of the left posterior intercostal artery, usually between T8 and T12. It becomes intradural and crosses over one to three disk spaces before turning to the midline where it anastomoses with the anterior spinal artery. Injury to this artery can result in devastating ischemia of the lower spinal cord. Lu J, Ebraheim NA, Biyani A, Brown JA, Yeasting RA: Vulnerability of great medullary artery. Spine 1996;21:1852-1855.
Question 837
High Yield
A 51-year-old woman with no preoperative neurologic deficit is undergoing elective anterior cervical diskectomy and fusion (ACDF) with plating and fusion for a C5-6 disk herniation with right-sided neck pain. Thirty minutes into the surgery the neurophysiologic monitoring shows a rapid drop and then loss of amplitude in the right cortical somatosensory-evoked potential waveform. All other waveforms remained normal and unchanged, including right-sided cervical (subcortical) and peripheral (Erb's point), and those from the left-sided upper extremity and both lower extremities. What is the most likely cause of the change?

Explanation
The change noted is focal and confined to the cortex, sparing the opposite side, both lower extremities, and the subcortical waveforms, making all the choices unlikely with the exception of carotid compression with focal cortical ischemia. This may be associated with poor collateral flow from the opposite hemisphere due to an incomplete circle of Willis. Drummond JC, Englander RN, Gallo CJ: Cerebral ischemia as an apparent complication of anterior cervical discectomy in a patient with an incomplete circle of Willis. Anesth Analg 2006;102:896-899.
Question 838
High Yield
Which of the following mechanisms is considered the most common cause of failure of osteoarticular allografts used for articular reconstruction?

Explanation
Mechanical loosening and infection can occur as complications after surgery, but the most common cause of osteoarticular allograft failure is graft collapse during revascularization. Clinical rejection because of an immune response is an unusual means of failure. Meyers MH, Akeson W, Convery FR: Resurfacing of the knee with fresh osteochondral allograft. J Bone Joint Surg Am 1989;71:704-713.
Question 839
High Yield
An 8-year-old boy sustains nondisplaced midshaft fractures of the tibia and fibula after being struck by a car while he was riding his bicycle. No other injuries are noted, but the patient reports pain with passive motion of his toes. His neurovascular examination is otherwise normal. What is the best course of action?
Explanation
Pain with passive motion of the toes is a recognized early sign of increased compartment pressures. At a minimum, a baseline evaluation of the leg compartment pressures should be obtained. While it is normal for the patient to have pain related to the associated muscle contusions, any significant concerns should be addressed immediately in light of the severe consequences likely when a compartment syndrome occurs. Mubarak SJ, Owen CA, Hargens AR, et al: Acute compartment syndromes: Diagnosis and treatment with the aid of the wick catheter. J Bone Joint Surg Am 1978;60:1091-1095.
Question 840
High Yield
What joint always remains uninvolved in all stages of scapholunate advanced collapse (SLAC) deformity of the wrist?
Explanation
The development of arthritis in SLAC wrist follows a consistent pattern. Beginning at the radial styloid to the scaphoid articulation, it progresses through the entire radioscaphoid joint and the midcarpal joint. In all stages, the radiolunate joint is spared, which is the basis for a scaphoid excision and four-corner fusion performed as a motion-sparing procedure for treatment of this condition. Wyrick JD: Proximal row carpectomy and intercarpal arthrodesis for the management of arthritis. J Am Acad Orthop Surg 2003;11:277-281. Watson HK, Ballett FL: The SLAC wrist: Scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg Am 1984;9:358-365.
Question 841
High Yield
To control most spontaneous bleeding into the knee in children with hemophilia, factor VIII must be replaced to what percentage of normal?

Explanation
The knee is the most common location of spontaneous bleeding in children with hemophilia. Treatment generally requires replacement to 40% to 50% of normal. For surgery, the replacement should be to 100%. The plasma level generally rises 2% for every unit (per kg body weight) of factor VIII administered. Rodriquez-Merchan EC: Management of the orthopaedic complications of hemophilia. J Bone Joint Surg Br 1998;80:191-196.
Question 842
High Yield
An olecranon fracture-dislocation of the elbow in which the fracture line exits distal to the coronoid process is best managed by open reduction and
Explanation
Fracture-dislocations of the elbow present difficult management problems. Standard olecranon fractures normally are not associated with a dislocation; however, the surgeon needs to recognize that some fractures that have a dislocation, in particular a posterior dislocation, represent a Monteggia equivalent. These injuries are not ulnar shaft fractures because they are fractured at or just distal to the coronoid; however, because of the unstable fracture-dislocation, the forces across this reduction are high. Two Kirschner wires and a tension band wire provide inadequate fixation. Therefore, the preferred method of fixation is plate osteosynthesis with a 3.5-mm low-contact dynamic compression plate or reconstruction plate. Jupiter JP, Kellam JF: Fractures of the forearm, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 421-454. Quintero J: Fracture of the forearm, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 323-337.
Question 843
High Yield
What is the recommended insertion torque for halo pins in adults?

Explanation
Garfin and associates have shown that halo pins inserted with 8 in-lb of insertion torque results in significantly less loosening with cyclical loading than pins inserted with 6 in-lb of torque. Moreover, Botte and associates reported that 8 in-lb of torque is clinically safe and effective in lowering the incidence of pin loosening and infection. Botte MJ, Byrne TP, Garfin SR: Application of the halo device for immobilization of the cervical spine utilizing an increased torque pressure. J Bone Joint Surg Am 1987;69:750-752. Garfin SR, Lee TO, Roux RD, et al: Structural behavior of the halo orthosis pin-bone interface: Biomechanical evaluation of standard and newly designed stainless steel halo fixation pins. Spine 1986;11:977-981.
Question 844
High Yield
A 10-year-old boy with severe hemophilia A (factor VIII) sustained an injury to his right forearm 2 hours ago when a classmate fell on his arm during a scuffle. Examination reveals moderate swelling in the forearm, decreased sensation in the distribution of the median and ulnar nerves, and pain on passive extension of the fingers. What is the most appropriate sequence of treatment?
Explanation
The patient has severe hemophilia with a volar forearm hemorrhage and an emerging compartment syndrome. Therefore, it is critical to normalize the clotting deficiency as the first step in treatment. In a patient who has a factor VIII level of less than 1% and no inhibitors to factor VIII, transfusion with 4 unit/kg will typically raise the factor VIII level to 100%. Continuous transfusion can then be used to maintain this level. Compartment pressures can be safely measured after infusion of factor VIII. Because the hemorrhage is of limited duration and any surgery is considered serious in a patient with hemophilia, the compartment pressure should be measured before making a decision regarding a fasciotomy. However, it is important to note that the use of factor VIII concentrates allows both emergency and elective surgery provided that adequate hematology backup is available. Splinting the elbow and wrist in flexion reduces the pressure in the volar compartments, protects the forearm from further trauma, and makes the patient more comfortable. Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell & Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 345-391. Greene WB, McMillan CW: Nonsurgical management of hemophilic arthropathy, in Barr JS (ed): Instructional Course Lectures 38. Park Ridge, Ill, American Academy of Orthopaedic Surgeons, 1989, pp 367-381.
Question 845
High Yield
Figures 34a through 34c show the radiographs of a 51-year-old woman who injured her elbow in a fall from standing height. Examination reveals that elbow range of motion is limited by pain only. Management should consist of



Explanation
The radiographs show a small minimally displaced radial head fracture that is amenable to nonsurgical management. Early range-of-motion exercises will best restore function and minimize stiffness. A long arm cast for any length of time will result in severe elbow stiffness. Morrey BF: Radial head fracture, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 341-364.
Question 846
High Yield
Which of the following parameters is considered most important when assessing an acetabular fracture for surgical indications?
Explanation
The most important aspect in the decision for surgery in an acetabular fracture is the ability of the femoral head to remain concentrically reduced under the dome in AP and Judet oblique views of the pelvis. If this parameter is present, then the need for surgery is determined by other aspects such as fragmentation, age, incongruity, and displacement. If the head remains stable under the dome without traction, there is sufficient acetabular dome to provide stability, and nonsurgical treatment may be appropriate. Tile M: Assessment and management of acetabular fractures, in Tile M (ed): Pelvic and Acetabular Fractures, ed 2. Baltimore, MD, Williams and Wilkins, 1995, pp 305-354. Letournel E: Acetabular fractures: Classification and management. Clin Orthop 1980;151:81-106.
Question 847
High Yield
A 7-year-old girl has pain and swelling of the right elbow after falling off her bicycle. Radiographs are shown in Figure 31. What is the most appropriate initial step in management?

Explanation
Lateral condylar fractures are challenging to treat because of late displacement and development of a nonunion that may lead to valgus instability, pain, or tardy ulnar nerve palsy. Fractures such as this one with more than 2 mm of displacement on any radiographic view are prone to nonunion and should be stabilized. Fractures with less than 2 mm of displacement usually are stable and may be treated nonsurgically. In these patients, careful follow-up is recommended within several days of casting to check for fracture displacement. Arthrography or MRI may be helpful in these minimally displaced fractures. Fractures with an intact articular cartilage surface, such as noted on these studies, are unlikely to displace further. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425. Attarian DE: Lateral condyle fractures: Missed diagnoses in pediatric elbow injuries. Mil Med 1990;155:433-434. Flynn JC: Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J Pediatr Orthop 1989;9:691-696.
Question 848
High Yield
A 75-year-old woman who fell on her right knee now reports pain and is unable to bear weight. History reveals that she underwent total knee arthroplasty on the right knee 6 years ago. Radiographs are shown in Figure 5. Management should now consist of

Explanation
The radiographs show a loose femoral component with an associated medial condyle distal femoral fracture. The treatment of choice is open reduction and internal fixation with revision of the femoral component because of the femoral component loosening. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. McLaren AC, DuPont JA, Schroeber DC: Open reduction internal fixation of supracondylar fractures above total knee arthroplasties using the intramedullary supracondylar rod. Clin Orthop 1994;302:194-198.
Question 849
High Yield
A 14-year-old boy reports pain in the distal thigh. He denies any history of trauma. Examination reveals tenderness and swelling of the distal thigh without effusion. A radiograph and CT scan are shown in Figures 10a and 10b. A biopsy specimen is shown in Figure 10c. Management should consist of


Explanation
Based on these findings, the patient has an aneurysmal bone cyst. Frequently, fluid-fluid levels can be detected on MRI or CT images. The histologic results show a lesion that consists of cavernous spaces filled with blood. The lining of the cavity contains spindle cells, multinucleated giant cells, and reactive bone. Curettage and bone grafting is the preferred treatment method. Without treatment, these lesions can become quite large and destructive. Radiation therapy is not recommended for resectable lesions. Chemotherapy is not required for these benign lesions. Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
Question 850
High Yield
A 12-year-old boy who has had a 1-month history of right thigh pain and a limp reports worsening of the pain after a fall, and he can no longer walk or bear weight on the involved extremity. Radiographs of the pelvis reveal a slipped capital femoral epiphysis with moderate to severe displacement. While positioning the patient on the fracture table for screw fixation, partial reduction of the slip is achieved. No further reduction maneuvers are attempted, and the epiphysis is stabilized with a single cannulated screw. What complication is most likely to develop following this procedure?
Explanation
Traditional classification of slipped capital femoral epiphyses is based on the following temporal criteria: acute (symptoms that persist for less than 3 weeks); chronic (symptoms that persist for more than 3 weeks); or acute on chronic (acute exacerbation of long-standing symptoms). A newer classification differentiates between a stable slip where weight bearing is possible, and an unstable slip if it is not. Reduction of an unstable slip often occurs unintentionally with induction of anesthesia and positioning of the patient for surgery. The rate of satisfactory results is lower primarily because of a much higher incidence of osteonecrosis following internal fixation of an unstable slip. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Question 851
High Yield
Which of the following statements describing chordomas is false?

Explanation
Casali and associates provided a recent review of the treatment options for chordomas. These tumors are not radiosensitive; however, modern intensity modulated radiosurgery techniques may be of value. The combination of surgery and radiotherapy compared to surgery alone results in the same disease-free survival time. Complete surgical resection of the chondroma with clean margins offers the best survival; however, its location may make total removal impossible. Thus subtotal resection followed by radiotherapy results in better survival despite the tumor's lack of radiosensitivity.
Question 852
High Yield
A 42-year-old man sustained a fracture of the distal radius with subsequent stiffness in the ipsilateral shoulder. Despite a 6-month program of range-of-motion exercises, external rotation at the side is limited to 10 degrees. Attempts at closed manipulation are unsuccessful. Treatment should now consist of
Explanation
When external rotation at the side is limited, the most likely diagnosis is contracture of the rotator cuff interval, including the superior glenohumeral and coracohumeral ligaments. Therefore, the treatment of choice is arthroscopic release of the rotator cuff interval.
Question 853
High Yield
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
Temporary bed rest (less than 4 days) with gradual resumption of activities can be efficacious. Epidural steroid injections may be indicated for acute low back pain with radiculopathy. Acupuncture, facet joint injections, or ligamentous (sclerosant) injections are not indicated. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Question 854
High Yield
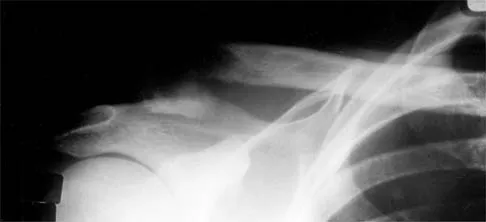
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of
Explanation
For the patient with an anterior sternoclavicular dislocation, the most appropriate initial treatment should be symptomatic. Surgical options are usually contraindicated because the incidence of intraoperative and postoperative complications is high. A deformity from an anterior sternoclavicular dislocation is usually well tolerated. Return to play is allowed when symptoms resolve. Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 477-525.
Question 855
High Yield
Which of the following is considered the best method to measure limb-length discrepancy in a patient with a knee flexion contracture?

Explanation
The most effective way to measure a limb-length discrepancy in a patient with a knee flexion contracture is a lateral CT scanogram. All the other methods listed provide inaccurate results with a knee flexion contracture because the measurements are made in the coronal plane. Aaron A, Weinstein D, Thickman D, et al: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Question 856
High Yield
An obese 10-year-old boy has had left groin pain and a limp for the past 2 months. Examination reveals decreased abduction and internal rotation. Laboratory studies show normal renal function and an elevated thyroid-stimulating hormone (TSH) level. AP and frog lateral radiographs of the pelvis are shown in Figures 30a and 30b. What is the best course of action?


Explanation
The radiographs show a grade I slipped capital femoral epiphysis (SCFE) that is classified as stable because the child is able to bear weight. The elevated TSH level indicates possible hypothyroidism. SCFE usually occurs in boys age 12 to 14 years. Because of the patient's young age and hypothyroidism, he is at increased risk for slippage of the contralateral hip; therefore, prophylactic pinning of the uninvolved side also should be considered. Because of the risk of slip progression, crutch treatment and nonsteroidal anti-inflammatory drugs are not indicated. Realignment osteotomy is not indicated for grade I SCFE. Traction to reduce the slip, followed by pinning, has been advocated for unstable slips but is not indicated here. Loder RT, Wittenberg B, DeSilva G: Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop 1995;15:349-356.
Question 857
High Yield
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?

Explanation
The findings are characteristic of hemangioma. When the hemangioma is large enough, vertical striations may be visible on plain radiographs. Axial CT scans commonly reveal a speckled appearance. Metastatic lesions are typically hypointense on T1-weighted images because they replace the fatty marrow. Bony islands, like cortical bone, are dark on T1- and T2-weighted images. Intravertebral disk herniation would have characteristics similar to the disk and be in continuity with the disk. Osteoporosis is more diffuse. Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
Question 858
High Yield
What is the most common reason for reoperation in total knee arthroplasty?

Explanation
Patellar problems currently constitute the largest number of complications after total knee arthroplasty, affecting between 8% and 35% of patients. These problems include patellar instability, fracture, component loosening, surface erosion, and pain. Malalignment, as an isolated reason for revision, is uncommon, yet it contributes to accelerated wear of the components. Joint instability affects up to 6% of patients, and the infection rate in knee arthroplasty is around 1% to 2%. Blasier RB, Matthews LS: Complications of prosthetic knee arthroplasty, in Epps CH (ed): Complications in Orthopaedic Surgery. Philadelphia, PA, JP Lippincott, 1994, pp 1066-1069. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620.
Question 859
High Yield
Examination of a 6-year-old boy who sustained a displaced Salter-Harris type II fracture of the distal radius reveals 35 degrees of volar angulation. A satisfactory reduction is obtained with the aid of a hematoma block. At the 10-day follow-up examination, radiographs show loss of reduction and 35 degrees of volar angulation. Management should now consist of

Explanation
In a 6-year-old child with a physeal fracture, the healing response 10 days after injury is so advanced that manipulation would have to be very forceful to be successful. A forceful manipulation in a patient this age increases the risk of early growth arrest and a significant disability because 80% of the growth of the radius comes from the distal physis. Because of the large contribution of growth from the distal radial physis and the angulation being in the plane of wrist motion, the potential for remodeling of this fracture is great. It is highly probable that this fracture will completely remodel in 1 to 2 years of growth. In this patient, even a "gentle" open reduction would probably require enough force that the physis would be damaged. Dimeglio A: Growth in pediatric orthopaedics, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 33-62.
Question 860
High Yield
A 22-year-old professional ballet dancer reports a 3-month history of posterior ankle pain that occurs when she changes from a flat foot to pointe (hyperplantar flexed position). Examination does not elicit the pain with forced passive plantar flexion. A radiograph is shown in Figure 8. What is the most likely cause of the pain?

Explanation
The most common causes of posterior ankle pain in ballet dancers are flexor hallucis longus tenosynovitis and os trigonum syndrome. Flexor hallucis longus tenosynovitis differs from a symptomatic os trigonum by the absence of pain with forced plantar flexion and the presence of pain with resisted plantar flexion of the great toe. The pain is often felt in the posterior ankle and can be associated with a snapping or triggering sensation. Os trigonum syndrome commonly occurs in ballet dancers who perform in a position of extreme plantar flexion. The pain occurs from entrapment of the os trigonum between the posterior portion of the talus and calcaneus. Hamilton WG, Geppert MJ, Thompson FM: Pain in the posterior aspect of the ankle in dancers: Differential diagnosis and operative treatment. J Bone Joint Surg Am 1996;78:1491-1500.
Question 861
High Yield
During the early swing phase of the normal gait cycle, what lower extremity muscle is primarily contracting?
Explanation
Electromyography during walking reveals the tibialis anterior muscle is active during early swing, allowing the foot to clear the ground. All of the other muscles are quiet, as the limb moves forward through space with minimal muscular effort. The other muscles are primarily active during weight acceptance or push-off. Gage JR: An overview of normal walking. Instr Course Lect 1990;39:291-303.
Question 862
High Yield
What type of thoracolumbar spinal injury is associated with an increased risk of neurologic deterioration following admission to the hospital?
Explanation
Gertzbein's Scoliosis Research Society Morbidity and Mortality report noted that neurologic deterioration developed in approximately 16% of patients who were hospitalized with fracture-dislocations of the thoracolumbar spine, a particular concern with rotational burst fractures (AO type C). Patients with standard burst fractures and Chance fractures had a markedly lower incidence of neurologic involvement and tended to remain neurologically stable. Gertzbein SD: Neurologic deterioration in patients with thoracic and lumbar fractures after admission to the hospital. Spine 1994;19:1723-1725.
Question 863
High Yield
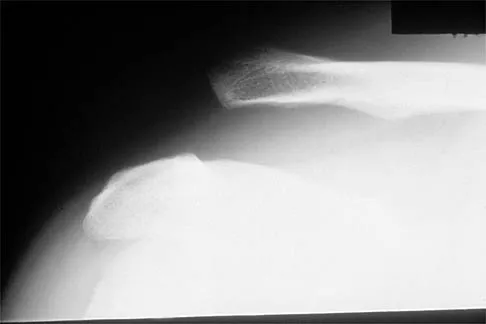
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of
Explanation
The radiograph shows a displaced type II distal clavicle fracture with nonunion. Because the patient's symptoms are minimal, the injury can be treated like a grade III acromioclavicular separation. Present management should consist of ice, anti-inflammatory drugs, activity modification, and perhaps physical therapy. If nonsurgical management fails to provide relief, the surgical options are varied with no uniformity in the literature regarding surgical treatment of this injury. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 864
High Yield
A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm3. What is the most common organism in this scenario?

Explanation
The most common bacterial etiologic agent following varicella is group A beta-hemolytic streptococcus. The other organisms are much less common. Staphylococcus aureus is the most common bone infection organism. Staphylococcus epidermidis is increasingly a bone infection organism. Group B streptococcus occurs more commonly in newborns. Kingella kingae is a common joint pathogen but is not as common following varicella. Schreck P, Schreck P, Bradley J, et al: Musculoskeletal complications of varicella. J Bone Joint Surg Am 1996;78:1713-1719.
Question 865
High Yield
A 68-year-old man fell off a 20-foot mountain cliff and was seen in the emergency department the following morning. A radiograph is shown in Figure 12. He is a nonsmoker with medical comorbidities of hypertension and hypercholesterolemia that is well controlled with medicine and diet. Capillary refill and sensation are intact distally and the patient is able to move his toes with mild discomfort. Serosanguinous fracture blisters are present laterally, and the foot is swollen and red. What is the most appropriate management?

Explanation
Whereas a patient age of older than 50 years used to be a contraindication for open reduction and internal fixation of displaced intra-articular calcaneal fractures, new data suggest that the presence of associated medical comorbidities that affect wound healing such as smoking, diabetes mellitus, and peripheral vascular disease are more relevant to postoperative functional outcome. Surgical treatment of Sanders II and III displaced intra-articular calcaneal fractures with initial Bohler angles of > 15 degrees results in better outcomes as compared to nonsurgical management. Indications for primary fusion might include Sanders IV fractures in which articular congruity or Bohler angles cannot be restored. Given the condition of the soft tissues at presentation, delayed fixation is recommended. Herscovici D Jr, Widmaier J, Scaduto JM, et al: Operative treatment of calcaneal fractures in elderly patients. J Bone Joint Surg Am 2005;87:1260-1264. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744.
Question 866
High Yield
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
The recurrent laryngeal nerve provides innervation to the vocal cords and was the most common neurologic injury reported in a series of 36,000 patients. The nerve is felt to be more vulnerable during a right-sided approach because of its anatomic course. A recent study has also suggested a role for increased endotracheal cuff pressures in this nerve injury. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 867
High Yield
Figure 3 shows the clinical photograph of a wrestler who has an acute mass in his ear. He does not wear protective headgear. The area is mildly tender and without erythema. Management should consist of
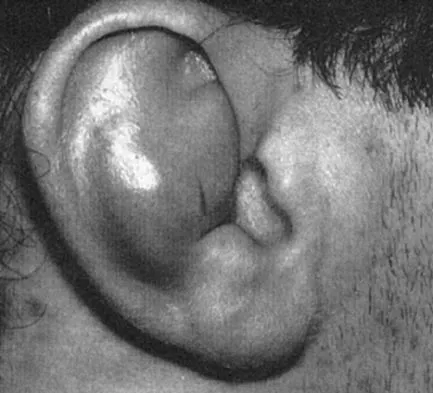
Explanation
The patient has an auricular hematoma. This injury is typically related to blunt trauma, occuring in wrestlers who do not use protective headgear. The goal of treatment is to remove the fluid, reapproximate the perichondrium to the underlying articular cartilage, and limit reaccumulation of the fluid in attempt to prevent cartilage necrosis. Aspiration and application of a compressive dressing offers the best chance to achieve this goal. There are no signs of infection such as marked tenderness, erythema, or surrounding edema to justify antibiotic use or irrigation and debridement. The mass does not warrant excision. Kaufman BR, Heckler FR: Sports-related facial injuries. Clin Sports Med 1997;16:543-562.
Question 868
High Yield
A 22-year-old college quarterback is tackled and sustains a reducible first carpometacarpal dislocation. What is the recommended treatment?
Explanation
When comparing closed reduction and pinning to ligament reconstruction, the reconstruction group had slightly better abduction and pinch strength. The volar oblique ligament usually tears off the first metacarpal in a subperiosteal fashion. In this young patient, motion-sparing procedures are preferred. Simonian PT, Trumble TE: Traumatic dislocation of the thumb carpometacarpal joint: Early ligamentous reconstruction versus closed reduction and pinning. J Hand Surg Am 1996;21;802-806.
Question 869
High Yield
Examination of a 25-year-old man who was injured in a motor vehicle accident reveals a fracture-dislocation of C5-6 with a Frankel B spinal cord injury. He also has a closed right femoral shaft fracture and a grade II open ipsilateral midshaft tibial fracture. Assessment of his vital signs reveals a pulse rate of 45/min, a blood pressure of 80/45 mm Hg, and respirations of 25/min. A general surgeon has assessed the abdomen, and a peritoneal lavage is negative. His clinical presentation is most consistent with what type of shock?

Explanation
Assessment of the acutely injured patient follows the Advanced Trauma Life Support protocol. Cervical cord injury is often associated with a disruption in sympathetic outflow. Absent sympathetic input to the lower extremities leads to vasodilatation, decreased venous return to the heart, and subsequent hypotension. With hypotension, the physiologic response of tachycardia is not possible because of the unopposed vagal tone. This results in bradycardia. Patient positioning, fluid support, pressor agents, and atropine are used to treat neurogenic shock.
Question 870
High Yield
Figures 3a and 3b show the current radiographs of a 59-year-old woman who has pain and deformity after undergoing bunion surgery 1 year ago. Nonsurgical management has failed to provide relief. Treatment should now consist of


Explanation
The hallux varus seen in this patient is most likely the result of a combination of causes. Based on the degenerative changes and the significant shortening of the first metatarsal relative to the second metatarsal, a metatarsophalangeal arthrodesis is the treatment of choice. The other surgical approaches are not expected to provide a satisfactory result. Coughlin MJ, Mann RA: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby-Year Book, 2000, pp 150-269.
Question 871
High Yield
Based on the appearance of the imaging studies shown in Figures 11a through 11c, what structure has most likely been injured?



Explanation
The radiographs reveal marked lateral subluxation of the patella in a patient who has recurrent patellar instability. The medial patellofemoral ligament is the main restraint to lateral subluxation of the patella. Boden BP, Pearsall AW: Patellofemoral instability: Evaluation and management. J Am Acad Orthop Surg 1997;5:47-57.
Question 872
High Yield
In addition to pain, which of the following factors are considered most predictive of the risk of pathologic fracture?
Explanation
While guidelines for predicting fracture risk are at best imprecise, the scoring system by Mirels (pain, anatomic location, and pattern of bony destruction) has been shown to be most predictive of fracture risk. Functional pain, peritrochanteric location, and lytic bone destruction are the greatest risk factors for pathologic fracture. The factors of patient weight, age, soft-tissue mass, and location within bone are all of lesser importance. Frassica FJ, Frassica DA, McCarthy EF, Riley LH III: Metastatic bone disease: Evaluation, clinicopathologic features, biopsy, fracture risk, nonsurgical treatment, and supportive management. Instr Course Lect 2000;49:453-459.
Question 873
High Yield
The recurrent motor branch of the median nerve innervates which of the following muscles?
Explanation
The recurrent motor branch of the median nerve supplies the thenar muscles (abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis) that are primarily responsible for thumb opposition. The nerve can be injured in carpal tunnel release. A branch of the nerve also supplies the first lumbrical. The adductor pollicis and the interossei are supplied by the ulnar nerve. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Question 874
High Yield
A 28-year-old man has had a 2-year history of progressive lateral ankle pain. History reveals that he underwent a triple arthrodesis at age 13 for a tarsal coalition. The pain has been refractory to braces, custom inserts, and nonsteroidal anti-inflammatory drugs. Weight-bearing radiographs of the ankle and foot are shown in Figures 3a through 3d. Surgical management should include which of the following?




Explanation
The patient has a valgus-supination triple arthrodesis malunion. Weight-bearing radiographs show excessive residual valgus through the subtalar joint, producing lateral subfibular impingement, and residual forefoot abduction and midfoot supination through the talonavicular joint, lateralizing the weight-bearing forces through the foot. The deformity is best managed with a medial displacement calcaneal osteotomy and transverse tarsal derotational osteotomy. Ankle arthroscopy and lateral ligament reconstruction are indicated in the event of ligament instability. Tendon transfer, lateral column lengthening, and heel cord lengthening are used for treatment of adult flatfoot from posterior tibial tendon insufficiency. Ankle arthrodesis and ankle arthroplasty are not indicated in this patient because the lateral ankle symptoms are the result of the underlying deformity in the hindfoot, the patient is young, and the ankle joint is relatively normal. Haddad SL, Myerson MS, Pell RF IV: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis. Foot Ankle Int 1997;18:489-499.
Question 875
High Yield
A 25-year-old woman has significant pain and swelling in her left ankle after falling off her bicycle. Examination reveals that she is neurovascularly intact. Radiographs are shown in Figures 33a through 33c. What is the next most appropriate step in management?



Explanation
The radiographs show a displaced ankle fracture with widening of the syndesmosis. Open reduction and internal fixation is indicated with fixation of the mortise with syndesmotic screws. Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Question 876
High Yield
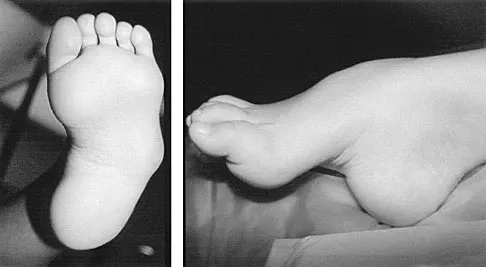
Figures 8a and 8b show the clinical photograph and radiograph of a 4-month-old infant who has a left foot deformity. Examination reveals that the foot deformity is an isolated entity, and the infant has no known neuromuscular conditions or genetic syndromes. Which of the following studies will best confirm the diagnosis?


Explanation
The clinical photograph shows a rocker-bottom deformity, and the lateral radiograph suggests a congenital vertical talus deformity. A lateral radiograph of the foot in maximum plantar flexion is needed to demonstrate the fixed position of the deformity with malalignment of the talar-metatarsal axis. A fixed dislocation of the navicular on the talus differentiates a congenital vertical talus from the oblique talus with talonavicular subluxation. Kumar SJ, Cowell HR, Ramsey PL: Vertical and oblique talus. Instr Course Lect 1982;31:235-251. Kodros SA, Dias LS: Single-stage correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Question 877
High Yield
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of

Explanation
Fractures of the hook of the hamate frequently are not identified in the acute phase. Because the fracture can be difficult to see on plain radiographs, the lack of findings can lead to a painful nonunion. A carpal tunnel view may show the fracture, but a CT scan will best detect the injury. Immobilization is the treatment of choice and will result in union in most patients unless the diagnosis is delayed. However, excision of the fragment may be necessary for patients who have nonunion, persistent pain, or ulnar nerve palsy. Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Question 878
High Yield
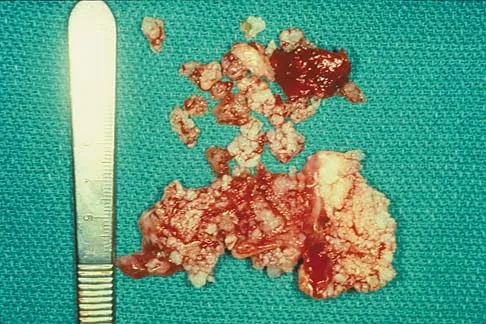
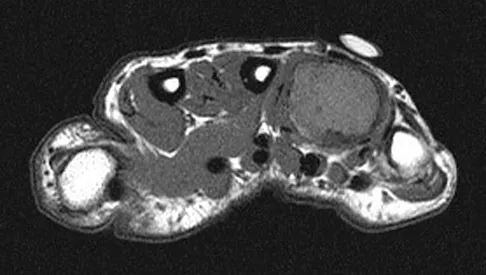
A 51-year-old male truck driver has had progressive left hip pain for more than 2 years, and he reports that the pain has become severe in the past 9 months. He is now unable to work because of the pain. Examination reveals that range of motion of the hip is limited to 95 degrees of flexion, 0 degrees of internal rotation, and 20 degrees of external rotation. The plain radiograph, MRI scan, and intraoperative gross photographs are shown in Figures 9a through 9d. Management should consist of



Explanation
The diagnosis is synovial chondromatosis. While the plain radiograph fails to show any calcifications, the MRI scan shows an intra-articular mass that involves the capsule. Grossly multiple granular cartilage nodules are seen. Management should consist of removing all loose bodies along with the synovial membrane.
Question 879
High Yield
Immobilization of human tendons leads to what changes in structure and/or function?
Explanation
Recent in vivo and in vitro experiments demonstrate that immobilization of tendon decreases its tensile strength, stiffness, and total weight. Microscopically, there is a decrease in cellularity, overall collagen organization, and collagen fibril diameter.
Question 880
High Yield
A 26-year-old man has had hand pain and progressive swelling in the knuckle for the past several months. He denies any trauma to the hand. The ring finger metacarpophalangeal joint is tender, and there is loss of motion in the digit. Figure 32a shows the radiograph and Figures 32b through 32d show the T1-weighted, T2-weighted, and gadolinium MRI scans, respectively. What is the most likely diagnosis?


Explanation
The radiograph reveals a subchondral lesion in the metacarpophalangeal joint that is lytic and expansile. The MRI scans show a mass that is moderate in intensity on the T2-weighted image and has some gadolinium uptake. There are no cystic components in this lesion. The subchondral location and expansile nature are highly suggestive of giant cell tumor of bone. A lesion with this appearance might also represent an aneurysmal bone cyst, given the amount of expansion present. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 113-118.
Question 881
High Yield
An intoxicated 68-year-old man fell at home. Examination reveals abrasions on his forehead, 2/5 weakness of his hand intrinsics and finger flexors, and 4/5 strength of the deltoid, biceps, and triceps bilaterally. Lower extremity motor function is 5/5. Sensory examination to pain and temperature is diminished in his hands but intact in his lower extremities. Deep tendon reflexes are depressed in all four extremities, but perianal sensation and rectal tone are intact. Foley catheterization yields 700 mL of urine. Radiographs of the cervical spine reveal multilevel spondylosis without fracture or subluxation. An MRI scan reveals high-intensity signal change within the cord substance at C5. What is the most likely diagnosis?

Explanation
Central cord syndrome is characterized by greater neurologic involvement of the upper extremities than the lower extremities. This is typically seen in older patients with cervical spondylosis without associated bony injury or joint subluxation. The prognosis for recovery is fair. Patients with Brown-Sequard syndrome have an ipsilateral motor deficit and contralateral loss of pain and temperature. Prognosis for recovery depends on the mechanism of injury, which is often of a penetrating nature. Anterior cord syndrome results from anterior compression such as occurs with a burst or teardrop fracture of the vertebral body; patients have bilateral motor loss, pain, and temperature loss with preservation of proprioception and vibratory sensation (posterior column function). The prognosis for recovery is generally poor. Posterior cord syndrome is rare and is associated with loss of posterior column function (proprioception and vibration). Northrup BE: Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott-Raven, 1998, pp 541-549.
Question 882
High Yield
Which of the following is considered a major characteristic of hyaluronate?
Explanation
Hyaluronate is a naturally occurring compound that is the backbone of the central core of the proteoglycan aggregate. Cartilage is made of two principal tissue structures. The connective tissue component includes collagen, which forms the framework for structural strength and elasticity. The proteoglycan aggregate provides a unique property of water incorporation and friction reduction capabilities. Hyaluronate forms the base or central core of the aggregate on which a link protein binds a protein core. Chondroitin sulfate and keratin sulfate are then bound to this protein core, forming the terminal extension of the aggregate. Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 69-78. Felson DT: Osteoarthritis. Rheum Dis Clin North Am 1990;16:499-512.
Question 883
High Yield
A 28-year-old man sustains the closed injury shown in Figures 3a through 3c after falling 8 feet while rock climbing. Management should consist of



Explanation
The radiographs show a comminuted talar body fracture. The goal of treatment is to minimize the risks of posttraumatic arthrosis of the ankle and subtalar joint and to maintain vascularity. Open reduction and internal fixation with an attempt at anatomic reduction will lead to improved outcomes. Attempting to repair this fracture via an arthrotomy only is extremely difficult, and the addition of a medial malleolar osteotomy is warranted. A limited anterior lateral arthrotomy with minimal soft-tissue stripping may assist with fixation of anterior-lateral and lateral fragments and allow better assessment of reduction of the major fracture line. Nonsurgical care would lead to inadequate reduction and increased risk of both ankle and hindfoot arthrosis. Talectomy and primary ankle and hindfoot arthrodesis should not be performed as primary surgical reconstructive options in this closed injury pattern. Sanders R: Fractures and fracture-dislocations of the talus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1465-1518.
Question 884
High Yield
Which of the following factors is a significant predictor of reoperation following open reduction and internal fixation of intertrochanteric fractures with a sliding-compression hip-screw device?
Explanation
As shown by Palm and associates from the Hip Fracture Study group, the integrity of the lateral femoral cortex in intertrochanteric hip fractures is a significant predictor of reoperation. Baumgartner and associates have shown that a tip-apex distance of greater than 25 mm is associated with a high risk of femoral head cut-out. Lastly, intertrochanteric hip fractures can be described as standard obliquity or reverse obliquity when describing the fracture pattern. Mechanistically, a reverse obliquity pattern is important to recognize because it reflects the presence or absence of a lateral buttress to which the proximal fracture fragment may compress. Palm H, Jacobsen S, Sonne-Holm S, et al: Integrity of the lateral femoral wall in intertrochanteric hip fractures: An important predictor of a reoperation. J Bone Joint Surg Am 2007;89:470-475. Sadowski C, Lübbeke A, Saudan M, et al: Treatment of reverse oblique and transverse intertrochanteric fractures with use of an intramedullary nail or a 95 degrees screw-plate: A prospective, randomized study. J Bone Joint Surg Am 2002;84:372-381.
Question 885
High Yield
An adult with a distal humeral fracture underwent open reduction and internal fixation. What is the most common postoperative complication?
Explanation
Most patients lose elbow range of motion after open reduction and internal fixation of a distal humeral fracture. Ulnar nerve dysfunction, nonunion, and infection all occur less commonly. Webb LX: Distal humerus fractures in adults. J Am Acad Orthop Surg 1996;4:336-344.
Question 886
High Yield
Based on the MRI scan shown in Figure 6, the abnormal signal is seen in what carpal bone?
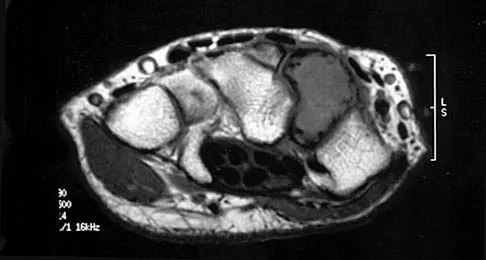
Explanation
The MRI scan reveals an abnormal signal in the trapezoid, which lies adjacent to the capitate in the distal carpal row. The tumor is a giant cell tumor of bone. Cooney WP, Linscheid RL, Dobyns JH: The Wrist: Diagnosis and Operative Treatment. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 278-282. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2238-2240. bar based on these measurements is shown in Figure 54d. Initial treatment should consist of 1- bony bar resection and distal fibula epiphysiodesis. 2- bony bar resection and corrective osteotomy. 3- bony bar resection and physiodesis of the opposite distal tibial physis. 4- corrective osteotomy and a limb-lengthening procedure. 5- corrective osteotomy and physiodesis of the opposite distal tibial physis. 2 54a 54b 54c 54d Mapping of a physeal bar from biplane polytomography or CT helps to identify lesions that should be treated surgically and aids in planning the surgical approach and resection. Criteria for surgical excision are at least 2 years of longitudinal growth remaining and involvement of no more than 50% of the physis. Osteotomy is required if angular deformity is greater than 20 degrees. Although this physeal bar is large, it is slightly less than 50% of the total area of the physis. Limb lengthening in this case should be reserved for failure of bar resection. Physiodesis of the opposite distal tibia at this age would result in disproportionate shortening of both tibiae. Carlson WO, Wenger DR: A mapping method to prepare for surgical excision of a partial physeal arrest. J Pediatr Orthop 1984;4:232-238.
Question 887
High Yield
A 32-year-old man sustained a fracture of his upper arm in a motor vehicle accident. Radiographs are shown in Figure 32. Because of other associated injuries, surgical stabilization is chosen. What technique will result in the least complications and the best outcome?

Explanation
Most humeral fractures will heal with nonsurgical functional brace management. When the initial pain has subsided in a coaptation splint, the patient is converted to a functional brace and allowed to use the arm for activities. The fracture should heal within 6 weeks to 12 weeks with acceptable results. Surgery is indicated if there is vascular injury, open injury, floating elbow, chest injury, bilateral humeral fractures, or if a reduction cannot be obtained or maintained. The surgical treatment of choice is either antegrade reamed locked intramedullary nailing or plate osteosynthesis. Plate osteosynthesis appears to offer better results with respect to union, function, and risk of complications. Schemitsch EH, Bhandari M: Fractures of the humeral shaft, in Browner BD: Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1481-1511.
Question 888
High Yield
The transverse diameter of the pedicle is most narrow at which of the following levels?

Explanation
Of the levels given, T5 has the most narrow pedicle in anatomic studies. One study in patients with scoliosis did note that T7 on the concave side was more narrow than T5, but T7 is not listed here as a possible answer. O'Brien MF, Lenke LG, Mardjetko S, et al: Pedicle morphology in thoracic adolescent idiopathic scoliosis: Is pedicle fixation an anatomically viable technique? Spine 2000;25:2285-2293.
Question 889
High Yield
A patient who underwent open reduction and internal fixation of an olecranon fracture 2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?


Explanation
The radiographs do not show an articular malunion. Treatment is directed at the soft-tissue contracture and should begin with formal physical therapy and static progressive splinting. Radiation therapy is effective in the perioperative period and is indicated when ectopic bone formation is a concern. Morrey BF: The posttraumatic stiff elbow. Clin Orthop Relat Res 2005;431:26-35.
Question 890
High Yield
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
Of the incomplete spinal cord injuries, Brown-Sequard syndrome has the best prognosis for ambulation. Central cord syndrome has a variable recovery. Anterior cord syndrome has the worst prognosis, with motor recovery rare below the level of the injury. Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Question 891
High Yield
An 8-year-old boy is diagnosed with acute onset cauda equina syndrome. A radiograph, MRI scans, and a biopsy specimen are shown in Figures 57a through 57d. What is the most appropriate treatment?


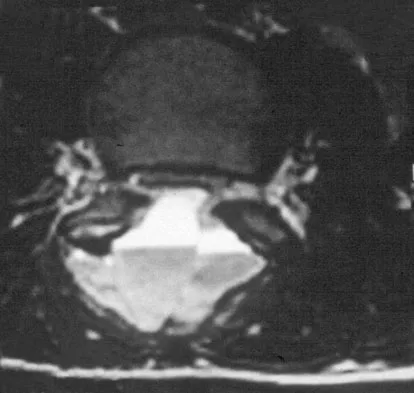
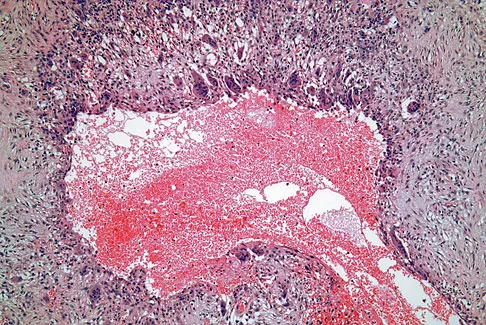
Explanation
The findings are consistent with an aneurysmal bone cyst. The MRI scan demonstrates a lesion involving the posterior elements of the vertebrae with fluid-fluid levels and neural compression. Fibrovascular tissue with multinucleated giant cells surrounding a vascular lake is seen on the histology. The most appropriate treatment is a marginal resection of the involved posterior elements. Although the recurrence rate can be as high as 25% to 30%, wide surgical resection could result in permanent neurologic injury and is not necessary. Aspiration and steroid injection have been advocated but would not relieve the nerve compression in this patient. Radiation therapy and chemotherapy are not indicated. Mankin HJ, Hornicek FJ, Ortiz-Cruz E, et al: Aneurysmal bone cyst: A review of 150 patients. J Clin Oncol 2005;23:6756-6762.
Question 892
High Yield
Figures 1a and 1b show the clinical photograph and oblique radiograph of a 52-year-old man who has plantar first metatarsal pain. A felt pad in the shoe proximal to the area of pain has failed to provide relief. Management should now consist of


Explanation
The patient has a discrete callus that overlies a prominent medial sesamoid. Calluses typically occur in response to increased pressure on the skin. Initial treatment should be directed at reducing local pressure with a felt pad. Sesamoid shaving is indicated if the felt pad fails to provide relief. Sesamoidectomy should be reserved for refractory callus given the potential complications of transfer metatarsalgia or callus and hallux valgus. A first metatarsal dorsiflexion osteotomy is more appropriate for a diffuse callus that fails to respond to nonsurgical management. Cryoablation and topical salicylic acid are appropriate for plantar warts, which have a rougher appearance with multiple, small black spots in the lesion. Mann RA, Wapner KL: Tibial sesamoid shaving for treatment of intractable plantar keratosis. Foot Ankle 1992;13:196-198.
Question 893
High Yield
Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?

Explanation
Stiffness following total knee arthroplasty can be a disabling condition. There are many reasons for loss of knee motion following total knee arthroplasty. Technical errors, such as overstuffing of the patella, malpositioning of the components, and ligamentous imbalance, are all known to result in stiffness following total knee arthroplasty. In some patients with a possible genetic predisposition, aggressive arthrofibrosis may develop and result in loss of knee motion. In any patient who has deteriorating knee motion, particularly after revision arthroplasty, deep infection should be ruled out. Although on occasion surgical intervention may be required to address knee stiffness, the outcome of revision surgery is poor if no reason for stiffness can be determined. Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.
Question 894
High Yield
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
Repetitive overhead slams and serves may produce a traction injury to the distal branch of the suprascapular nerve. Bankart, biceps, and superior labrum anterior and posterior injuries can occur but usually do not produce visible atrophy. Muscle avulsion is uncommon. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 895
High Yield
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?

Explanation
Unopposed action of the tibialis anterior with weakness of the peroneus longus will lead to a dorsal bunion and supination deformity. Overpull of the gastrocnemius-soleus complex and posterior tibialis with weakness of the peroneus brevis will cause equinovarus deformity. A strong posterior tibialis with weakness of the peroneals will cause varus of the hindfoot. Unopposed peroneus brevis and incompetence of the posterior tibialis will lead to a flatfoot deformity. The etiology of a cavus foot is complex, but findings usually include a contracted plantar fascia and weakness of the tibialis anterior. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 289-302.
Question 896
High Yield
In the most common condition causing a winged scapula, which of the following nerves is affected?
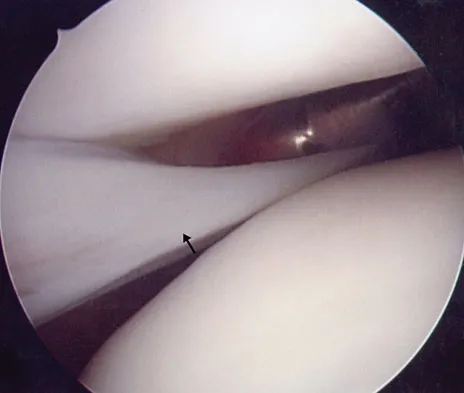
Explanation
A winged scapula is most often associated with Parsonage-Turner syndrome, a condition thought to be due to an inflammatory or immune-mediated mechanism. Certain muscles are predisposed, particularly the serratus anterior muscle innervated by the long thoracic nerve. Other less common nerve lesions (eg, the spinal accessory and dorsal scapular nerves) may also cause winged scapulae. Kline DG, Hudson AR: Nerve Injuries: Operative Results for Major Nerve Injuries, Entrapments and Tumors. Philadelphia, PA, WB Saunders, 1995.
Question 897
High Yield
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?


Explanation
The images demonstrate a L5 selective root block as it exits the L5-S1 foramen. This root block best helps relieve pain or paresthesias in the L5 distribution, which is the dorsal first web space and the great toe. The lateral foot is an S1 distribution and would need to be blocked through the posterior first sacral foramen. The anterior shin and thigh represent the L4 root which exits a level above this at the L4-5 foramen. A stocking distribution is nonanatomic and not indicative of a specific root. Magee D: Principles and concepts, in Orthopaedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Question 898
High Yield
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of


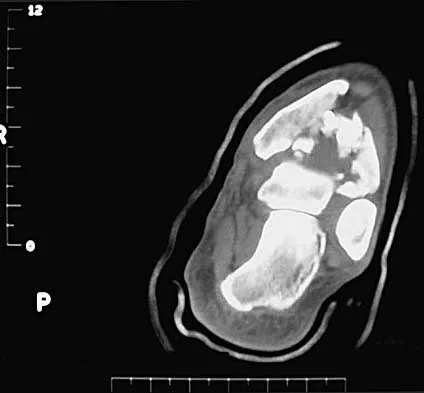
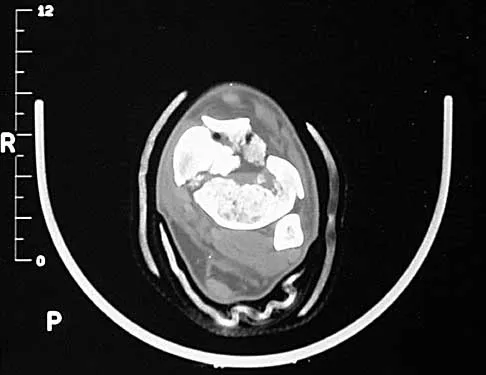
Explanation
The patient has a severe high-energy injury from axial loading to the left ankle and distal tibia. This is a closed injury, but the soft tissues are injured and severely swollen. Initial treatment should focus on skeletal stabilization, and incisions directly over the fracture area should be avoided until soft-tissue stabilization has occurred. Immediate spanning external fixation with plans for a delayed reconstruction as needed for the joint surface is the treatment of choice. Closed reduction and application of a constrictive long leg cast may lead to increased risk of tissue necrosis. Immediate open procedures to internally fix the fracture add the risks of soft-tissue necrosis and are to be avoided. Percutaneous plating may be one of the delayed fixation options but should not be used immediately. Primary ankle arthrodesis is not indicated. Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265. Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Question 899
High Yield
A 45-year-old tennis player undergoes surgery for chronic lateral epicondylitis. After returning to play, he notes increasing lateral elbow pain with mechanical catching and locking. Examination shows positive supine posterolateral rotatory instability. What ligament has been injured?
Explanation
The patient has sustained an iatrogenic injury to the lateral ulnar collateral ligament. This injury has been reported after lateral approaches to the elbow. The orbicular, annular, and lateral radial collateral ligaments have a much less important role in lateral elbow stability. The anterior band of the ulnar collateral ligament is on the medial side of the elbow and is important for valgus stability. O'Driscoll SW, Bell DF, Morrey BF: Posterolateral rotatory instability of the elbow. J Bone Joint Surg Am 1991;73:440-446.
Question 900
High Yield
A 32-year-old woman has left second toe dactylitis (sausage toe). Radiographs show a "pencil in cup" distal interphalangeal joint deformity. Examination reveals that subtalar motion is markedly reduced. What is the most likely diagnosis?

Explanation
The patient's clinical picture is considered the classic presentation for psoriatic arthritis. The other answers are not applicable for the constellation of findings. Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 1691-1693.
