HY 2026
00:00
Start Quiz
Question 701
High Yield
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?

Explanation
During transaxillary resection of the first rib, the long thoracic nerve is at risk as it passes either through or posterior to the middle scalene muscle. Injury to this nerve may occur as the result of overly aggressive retraction of the middle scalene during the procedure. Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Question 702
High Yield
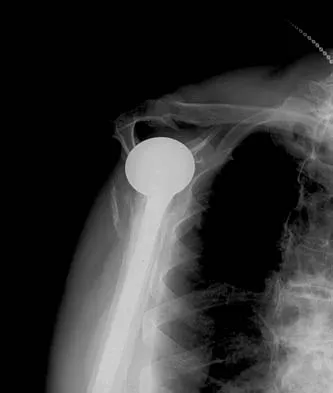
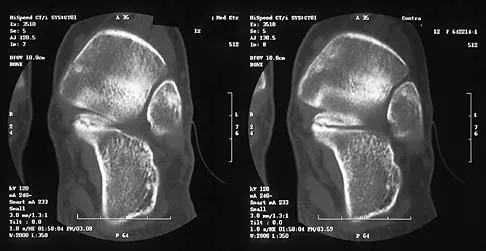
A 67-year-old man who underwent humeral head arthroplasty for a four-part fracture 6 months ago reports that he is still unable to actively elevate his arm. Rehabilitation after surgery consisted of a sling with passive range-of-motion exercises for 2 weeks and then progressed to active-assisted and strengthening exercises at 3 weeks. Radiographs are shown in Figures 28a and 28b. What is the primary cause of his inability to elevate the arm?

Explanation
The radiographs show nonunion of both the greater and lesser tuberosities. Tuberosity pull-off and nonunion remain among the most common causes of failed humeral head arthroplasty for fracture. Strict attention to securing the tuberosities to each other and to the shaft, and autogenous bone grafting from the excised humeral head will decrease the incidence of pull-off and improve healing rates. Active-assisted range-of-motion and strengthening exercises should be delayed until tuberosity healing is noted radiographically, usually at 6 to 8 weeks postoperatively. Hartsock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humeral fractures. Orthop Clin North Am 1998;29:467-475. Hughes M, Neer CS: Glenohumeral joint replacement and postoperative rehabilitation. Phys Ther 1975;55:850-858.
Question 703
High Yield
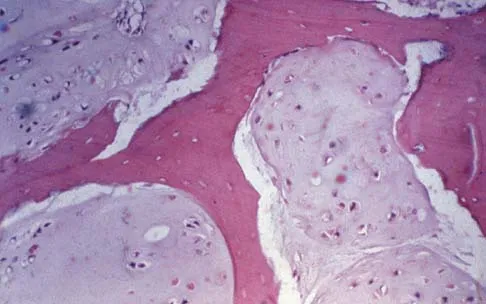
What is the dominant component of articular cartilage extracellular matrix by weight?

Explanation
Articular cartilage is a highly organized viscoelastic material, and load transmission depends on the specific composition of the extracellular matrix. Articular cartilage is devoid of neural, lymphatic, and blood vessel tissue. The extracellular matrix consists of water, proteoglycans, and collagen. Water comprises most of the wet weight (65% to 80%). Type II collagen comprises 95% of the collagen. The collagen and proteoglycan (keratan sulfate and chondroitin sulfate) matrix and its high water content are responsible for the mechanical properties of the articular cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Inst Course Lect 1998;47:487-504.
Question 704
High Yield
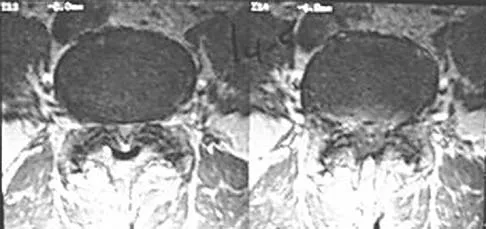
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of

Explanation
The patient has a degenerative spondylolisthesis at L4-5 with associated spinal stenosis. His symptoms are consistent with neurogenic claudication. Based on these findings, the surgical treatment of choice is decompression and posterolateral fusion. Use of instrumentation is controversial. Laminectomy alone is reserved for the patient who is frail medically. There is no role for an anterior approach or for fusion alone without decompression. Fischgrund JS, Mackay M, Herkowitz HN, et al: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 705
High Yield
When comparing mobile-bearing total knee arthroplasty (TKA) to fixed-bearing total condylar arthroplasty, the mobile-bearing procedure provides

Explanation
Survivorship is similar in the two groups. In a recent study, mobile-bearing TKAs showed a slightly higher maximum flexion than the total condylar fixed-bearing-type designs (112 degrees versus 108 degrees with no difference in recovery rate). Using a fixed-bearing or a mobile-bearing design did not seem to influence the recovery rate in early results after knee arthroplasty. Mobile-bearing arthroplasties are suggested, in theory, to offer a reduction in polyethylene wear; however, clinical studies have not yet proven this. Recovery rates have yet to be statistically seen as improved with either method. Differences in strength have not been shown. Aglietti P, Baldini A, Buzzi R, et al: Comparison of mobile-bearing and fixed-bearing total knee arthroplasty: A prospective randomized study. J Arthroplasty 2005;20:145-153. Sorrells RB: The rotating platform mobile bearing TKA. Orthopedics 1996;19:793-796.
Question 706
High Yield
A healthy 52-year-old woman is seeking professional advice about management of osteoporosis. She has no risk factors for osteoporosis. What is the best recommendation for bone health for this patient?
Explanation
Women older than age 50 years should receive daily supplementation with calcium and vitamin D to help preserve bone density. Bone mineral density testing is recommended for women age 65 years or older and postmenopausal women with at least one risk factor for osteoporotic fractures: prior fragility fracture, low estrogen levels, premature menopause, long-term secondary amenorrhea, glucocorticoid therapy, maternal history of hip fracture, or low body mass index. Hormone therapy is not approved for the treatment of osteoporosis. Gass M, Dawson-Hughes B: Preventing osteoporosis-related fractures: An overview. Am J Med 2006;119:S3-S11.
Question 707
High Yield
Which of the following is considered the most effective means of identifying an evolving motor tract injury during cervical spine surgery?
Explanation
In a study of 427 patients undergoing cervical spine surgery, 12 patients demonstrated substantial or complete loss of amplitude of the tceMEPs. Ten of those patients had complete reversal of the loss following prompt intraoperative intervention. SSEP monitoring failed to identify any changes in one of the two patients that awoke with a new motor deficit. SSEP changes lagged behind the tceMEP changes in patients in which major changes were detected by both modalities. TceMEP monitoring was 100% sensitive and 100% specific. SSEP monitoring was only 25% sensitive and 100% specific.
Question 708
High Yield
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
Prospective studies, including randomized and randomized multicenter reports, have shown that percutaneous or mini-open acute Achilles tendon repair has comparable functional results when compared to traditional open techniques. Calder and Saxby reported one superficial infection out of 46 patients with a mini-open repair; Assal and associates and Cretnik and associates had no wound complications or infections. The other complications have not proved to be less likely with the mini-open or percutaneous technique. Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170. Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Question 709
High Yield
A 13-year-old gymnast has had recurrent right elbow pain for the past year. She denies any history of trauma. Rest and anti-inflammatory drugs have failed to provide relief. Examination reveals no localized tenderness and only slight loss of both flexion and extension (10 degrees). What is the most likely diagnosis?
Explanation
Osteochondritis of the capitellum is characterized by pain, swelling, and limited motion. Catching, clicking, and giving way also can occur. It commonly affects athletes who participate in competitive sports with high stresses, such as pitching or gymnastics. Krijnen MR, Lim L, Willems WJ: Arthoscopic treatment of osteochondritis dissecans of the capitellum: Report of 5 female athletes. Arthroscopy 2003;19:210-214.
Question 710
High Yield
Which of the following findings is seen in the chest radiograph shown in Figure 13?

Explanation
Orthopaedic surgeons are often responsible for interpreting radiographs of general examinations such as the chest radiograph shown. For accurate interpretation, it is important to systematically review all of the information available on the radiograph. Using this approach, the fracture of the left proximal humerus is readily recognized. Linear air soft-tissue density at the lung periphery would suggest a pneumothorax, but this finding is not shown on the radiograph. The upper thoracic spine is well aligned. The sternoclavicular and distal clavicles are normal.
Question 711
High Yield
During cemented total hip arthroplasty, peak pulmonary embolization of marrow contents occurs when the
Explanation
Peak embolization is observed during femoral stem insertion. Embolization is also observed during acetabular preparation and hip reduction. Lewallen DG, Parvizi J, Ereth MH: Perioperative mortality associated with hip and knee arthroplasty, in Morrey BF (ed): Joint Replacement Arthroplasty, ed 3. Philadelphia, PA, Churchill-Livingstone, 2003, pp 119-127.
Question 712
High Yield
An active 47-year-old woman with rheumatoid arthritis reports forefoot pain and deformity and has difficulty with shoe wear. Examination reveals hallux valgus and claw toes. A radiograph is shown in Figure 10. What is the most appropriate surgical treatment?

Explanation
Rheumatoid arthritis commonly affects the metatarsophalangeal joints, which become destabilized with time resulting in hallux valgus and dislocated lesser claw toes. The result is metatarsalgia as the dislocated claw toes "pull" the fat pad distally. Severe hallux valgus reduces first ray load, which compounds the metatarsalgia because the load is transferred to the lesser metatarsal heads. First metatarsophalangeal arthrodesis restores weight bearing medially and corrects the painful bunion. Metatarsal head resection slackens the toe tendons to allow correction of the claw toes by whatever means necessary and decreases plantar load over the forefoot. Rheumatoid arthritis in the first metatarsophalangeal joint will continue to progress if osteotomies or a Lapidus procedure are performed. Keller resection arthroplasty increases transfer metatarsalgia and reduces push-off power during gait. Flexor-to-extensor tendon transfer of the lesser toes does not address the metatarsalgia and does not correct the dislocation of the metatarsophalangeal joint. Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 572.
Question 713
High Yield
A 36-year-old woman sustained a tarsometatarsal joint fracture-dislocation in a motor vehicle accident. The patient is treated with open reduction and internal fixation. What is the most common complication?

Explanation
The most common complication associated with tarsometatarsal joint injury is posttraumatic arthritis. In one series, symptomatic arthritis developed in 25% of the patients and half of those went on to fusion. In another series, 26% had painful arthritis. Initial treatment should consist of shoe modification, inserts, and anti-inflammatory drugs. Fusion is reserved for failure of nonsurgical management. Hardware failure may occur, but it is clinically unimportant. Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618. Arntz CT, Veith RG, Hansen ST Jr: Fractures and fracture-dislocations of the tarsometatarsal joint. J Bone Joint Surg Am 1988;70:173-181.
Question 714
High Yield
What does Dual Energy X-ray Absorptiometry (DEXA) testing, as a technique, measure?
Explanation
DEXA can provide data on bone mineral content and soft-tissue composition, and requires cross-sectional dimension for accuracy. DEXA provides a quantitative, not qualitative, measurement of bone mineral content and is incapable of differentiating between trabecular and cortical bone. Osteoarthritis falsely elevates the values, especially in the AP spinal analysis. Genant HK, Faulkner KG, Gluer CC: Measurement of bone mineral density: Current status. Am J Med 1991;91:49S-53S. Genant HK, Engelke K, Fuerst T, et al: Review: Noninvasive assessment of bone mineral density and stature: State of the art. J Bone Miner Res 1996;11:707-730.
Question 715
High Yield
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Explanation
Prepubescent athletes gain strength through neurogenic adaptations, including recruitment of motor units, reduced inhibition, and learned motor skills. Myogenic adaptations (muscle hypertrophy) occur after puberty and include increased contractile proteins, thickening of the connective tissue, and increased short-term energy sources such as creatine phosphate. Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Question 716
High Yield
Which of the following lesions is best suited for autologous chondrocyte implantation?
Explanation
Articular chondrocyte implantation is best performed for focal chondral defects of one area of the joint. It is not indicated for osteoarthritis. Mandelbaum BR, Brown JE, Fu F, et al: Articular cartilage lesions of the knee. Am J Sports Med 1998;26:853-861. Minas T, Nehrer S: Current concepts in the treatment of articular cartilage defects. Orthopedics 1997;20:525-538.
Question 717
High Yield
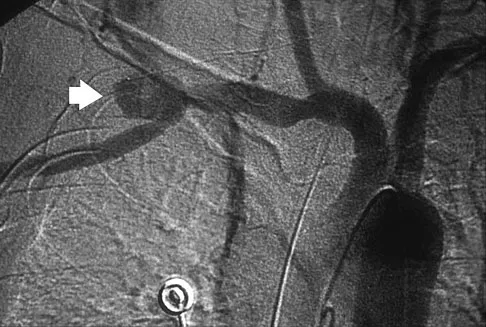
A previously healthy 65-year-old woman has a closed fracture of the right clavicle after falling down the basement stairs. Examination reveals good capillary refill in the digits of her right hand. Radial and ulnar pulses are 1+ at the right wrist compared with 2+ on the opposite side. In the arteriogram shown in Figure 36, the arrow is pointing at which of the following arteries?
Explanation
The axillary artery commences at the first rib as a direct continuation of the subclavian artery and becomes the brachial artery at the lower border of the teres major. The arteriogram reveals a nonfilling defect in the third portion of the artery just distal to the subscapular artery. The complex arterial collateral circulation in this region often permits distal perfusion of the extremity despite injury.
Question 718
High Yield
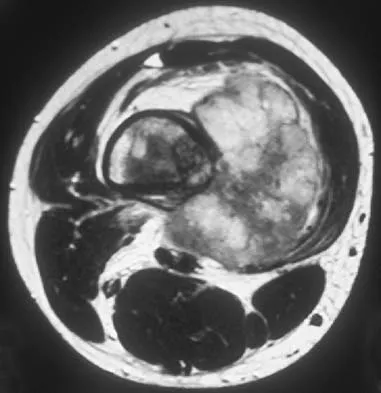
A 35-year-old woman states that she stepped on a piece of glass 6 months ago and reports numbness and shooting pain along the plantar lateral forefoot. She had previously received steroid injections in the 3 to 4 webspace. Examination reveals mild tenderness along the plantar fascia; no Tinel's sign is noted plantar medially and no Mulder's click is noted distally. An MRI scan is shown in Figure 7. What is the most likely cause of the numbness?

Explanation
The MRI scan reveals a laceration through the abductor hallucis musculature and lateral plantar nerve, producing numbness along its distribution. There is no evidence of a foreign body on the MRI scan. Baxter's nerve, or nerve to the abductor digiti quinti muscle, is the first branch off the lateral plantar nerve and impingement of this nerve typically produces a Tinel's sign along the nerve branch deep to the abductor hallucis muscle. Interdigital neuroma would be suggested by the presence of a Mulder's click. A digital nerve laceration would exhibit isolated numbness more distally. Baxter DE, Pfeffer GB: Treatment of chronic heel pain by surgical release of the first branch of the lateral plantar nerve. Clin Orthop Relat Res 1992;279:229-236.
Question 719
High Yield
Examination of an obese 3-year-old girl reveals 30 degrees of unilateral genu varum. A radiograph of the involved leg with the patella forward is shown in Figure 10. Management should consist of

Explanation
The clinical scenario describes infantile tibia vara (Blount's disease). The radiograph shows severe deformity with the characteristic Langenskiold stage 3 changes of the medial proximal tibial metaphysis that distinguish it from physiologic bowing. The preferred treatment is proximal tibiofibular osteotomy with acute correction into slight valgus to unload the damaged area of the physis. This method provides the best results in patients younger than age 4 years. Continued observation would result in progressive deformity. Bracing is most effective in younger children with less severe deformity. Lateral proximal tibial hemiepiphysiodesis relies on growth of the injured medial physis for correction and would result in severe tibial shortening in this young child. Complete epiphysiodesis also produces severe shortening and requires multiple lengthening procedures. Johnston CE II: Infantile tibia vara. Clin Orthop 1990;255:13-23.
Question 720
High Yield
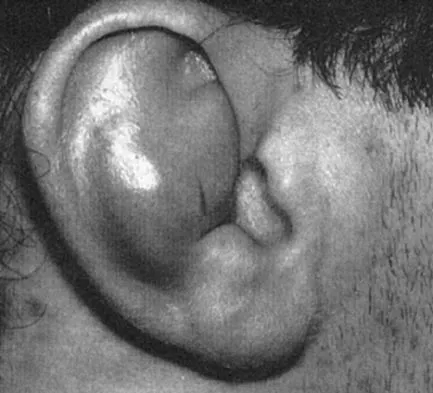
Figures 5a and 5b show the radiograph and MRI scan of a patient who has severe mechanical neck pain but no neurologic problems. Biopsy and work-up show the lesion to be a solitary plasmacytoma. Treatment should consist of


Explanation
Plasmacytoma is very sensitive to radiation therapy and given the complexity of the resection and complications of surgery in the given location, radiation therapy is preferred. However, the patient has clear loss of bony structural integrity, and resultant instability would persist even with tumor irradiation; therefore, posterior stabilization is warranted. Chemotherapy and bone marrow transplant are reserved for systemic disease with multiple myeloma. Corwin J, Lindberg RD: Solitary plasmacytoma of bone vs. extramedullary plasmacytoma and their relationship to multiple myeloma. Cancer 1979;43:1007-1013.
Question 721
High Yield
A 14-year-old boy has an anteromedial distal thigh mass. A radiograph and MRI scan are shown in Figures 39a and 39b. An open biopsy of the mass should include

Explanation
Biopsy of the soft-tissue component is often diagnostic. Alternatively, in centers with pathologists familiar with bone tumors, needle biopsy is usually successful. The principles of biopsy of bone tumors include avoiding contamination of uninvolved structures and compartments, taking the most direct path to the tumors, making an excisable biopsy tract, and obtaining diagnostic tissue. Transverse biopsy incisions should be avoided because they hinder the definitive surgical procedure. Peabody TD, Simon MA: Making the diagnosis: Keys to a successful biopsy in children with bone and soft-tissue tumors. Orthop Clin North Am 1996;27:453-459. Mankin HJ, Mankin CJ, Simon MA: The hazards of the biopsy, revisited. Members of the Musculoskeletal Tumor Society. J Bone Joint Surg Am 1996;78:656-663.
Question 722
High Yield
A 15-year-old female field hockey player sustains a blow to the mouth from a hockey stick. Three front teeth are knocked out and shown in Figure 4. In addition to calling a dentist immediately, what is the next best step in management?
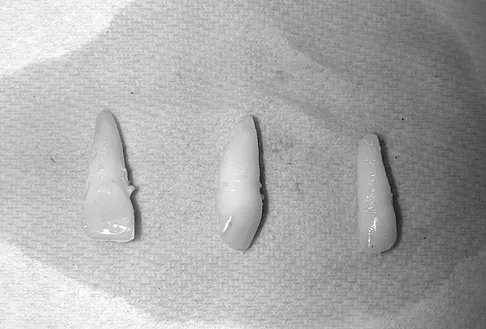
Explanation
Tooth avulsions can occur in contact or collision sports. An avulsed tooth is a medical emergency. The likelihood of survival of the tooth depends on the length of time that the tooth is out of the socket and the degree to which the periodontal ligament is damaged. The tooth should be handled only by the crown end and not the root end. It can be rinsed of debris with water or normal saline solution. The tooth should not be brushed or cleaned otherwise. During transport, the tooth must be kept moist. An avulsed tooth can be transported in whole milk, saliva, sterile saline solution, or commercially available kits with physiologic buffer solutions. The tooth and the athlete should be transported to the dentist for reinsertion as soon as possible and preferably within an hour. Krasner P: Management of sports-related tooth displacements and avulsions. Dent Clin North Am 2000;44:111-135. Sullivan JA, Anderson SJ (eds): Care of the Young Athlete. Rosemont IL, American Academy of Orthopaedic Surgeons, Elk Grove Village, IL, American Academy of Pediatrics, 2000, p 190.
Question 723
High Yield
A 25-year-old student sustains the injury shown in Figures 13a through 13c after falling off a curb. Initial management should consist of



Explanation
The radiographs reveal a fracture entering the 4-5 intermetatarsal articulation, consistent with a zone 2 injury. This classically is also referred to as a Jones fracture. The history and radiographic findings indicate this is an acute fracture, which guides management. A zone 1 fracture enters the fifth tarsometatarsal joint, and a zone 3 fracture is a proximal diaphyseal fracture distal to the 4-5 articulation. Initial management is usually nonsurgical and consists of non-weight-bearing in a short leg cast. This method has been shown to result in a better healing rate compared to weight bearing as tolerated. Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
Question 724
High Yield
Figures 45a and 45b show the radiographs of a 14-year-old boy who sustained a distal radius fracture while playing hockey. After 1 year the patient is asymptomatic. Follow-up and comparison radiographs and an MRI scan are shown in Figures 45c and 45d. What is the next most appropriate step in management?



Explanation
The patient sustained a growth plate fracture of the distal radius and ulna. Although treated with closed reduction and casting, the follow-up radiographs demonstrate shortening of the radius in comparison to the ulna, and the MRI scan confirms thinning of the distal radius growth plate and bony bars consistent with a growth arrest. At this time, the discrepancy in length is too minor to consider lengthening of the radius; in addition, excision of a physeal bar with minimal growth potential is not likely to restore the gross discrepancy. Ulnar styloid fractures are rarely symptomatic and do not require treatment in the asymptomatic patient. Closure of the distal ulna growth plate will prevent further discrepancy between the radius and ulna. Vanheest A: Wrist deformities after fracture. Hand Clin 2006;22:113-120.
Question 725
High Yield
Figures 3a and 3b show the current radiographs of a 58-year-old man who underwent total knee arthroplasty with a cruciate ligament sparing prosthesis 7 years ago. Examination reveals boggy synovitis and moderate pain, particularly anteriorly. Management should consist of


Explanation
The patient has symptoms of synovitis that are most likely the result of the release of particles from the tibial polyethylene. While observation may be warranted in a completely asymtomatic knee, some intervention is indicated for this patient as there is clear radiographic evidence of lysis in both the tibia and femur. The decision about the extent of the revision should be made at the time of surgery. A limited incision technique is not indicated. Grafting (or using graft substitute) the defect is the most appropriate approach for treating the osteolytic lesions. While a posterior stabilized prosthesis might be the solution, surgical findings might dictate otherwise.
Question 726
High Yield
The use of posting (a wedge added to the medial or lateral side of an insole) is useful to balance forefoot or hindfoot malalignment. Assuming normal subtalar joint pronation, what is the maximum amount of recommended hindfoot posting?

Explanation
Generally, patients cannot tolerate more than 5 degrees of hindfoot posting. Donatelli RA, Hurlbert C, Conaway D, et al: Biomechanics foot orthotics: A retrospective study. J Orthop Sports Phys Ther 1988;10:205-212. Michaud TM: Foot Orthoses and Other Forms of Conservative Foot Care. Baltimore, MD, Williams & Wilkins, 1993, pp 61-65, 186.
Question 727
High Yield
The quadrilateral space in the shoulder contains which of the following structures?

Explanation
The quadrilateral or quadrangular space of the shoulder is formed laterally by the humerus, proximally by the subscapularis (and teres minor viewed from posterior), distally by the teres major, and medially by the long head of triceps. The posterior humeral circumflex artery and axillary nerve pass through it. The axillary artery is more proximal. The radial nerve and profunda brachii pass through a triangular space more inferior. The circumflex scapular artery passes through a triangular space more medial. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, pp 205-206.
Question 728
High Yield
A 21-year-old collegiate female cross-country athlete reports right hip pain that begins about 12 miles into a run, followed by pain resolution when she discontinues running. However, each time she tries to resume a running program, she experiences recurrence of pain deep in the anterior groin. A plain radiograph and MRI scan are shown in Figures 8a and 8b. Management should consist of

Explanation
The history is consistent with a stress fracture. Findings on the plain radiograph are marginal, but the MRI scan shows evidence of stress reaction in the medial neck of the femur (compression side). A lesion on the compression side is not normally at risk for displacement and usually can be managed nonsurgically. A bone scan would further identify the lesion but is not necessary. A skeletal survey and chest radiograph are used in staging a tumor. Radioisotope injection and guided biopsy are sometimes used for osteoid osteomas. Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 729
High Yield
What mechanism is associated with the spontaneous resorption of herniated nucleus pulposus?
Explanation
Nonsurgical modalities remain the mainstay for treatment of herniated disks. Spontaneous resorption of herniated disks frequently is detected by MRI. Marked infiltration by macrophages and neovascularization are observed on histologic examination of herniated disks, and the resorption is believed to be related to this process. Many cytokines such as vascular endothelial growth factor, tumor necrosis factor-alpha, and metalloproteinases have been implicated in this process, but none has been found to be singularly responsible. Haro H, Kato T, Kamori H, et al: Vascular endothelial growth factor (VEGF)-induced angiogenesis in herniated disc resorption. J Orthop Res 2002;20:409-415.
Question 730
High Yield
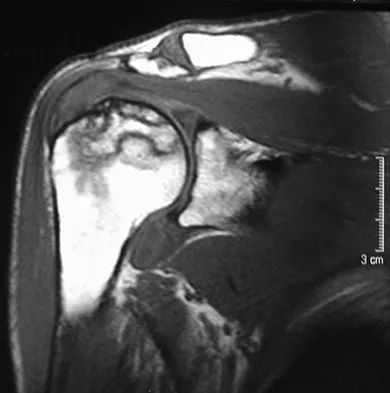
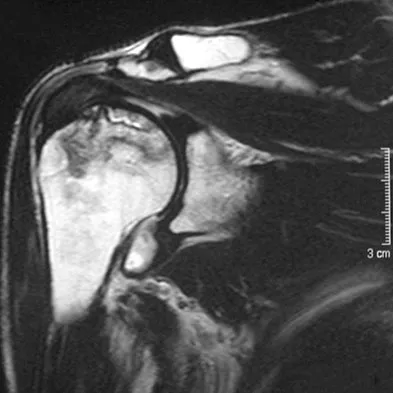
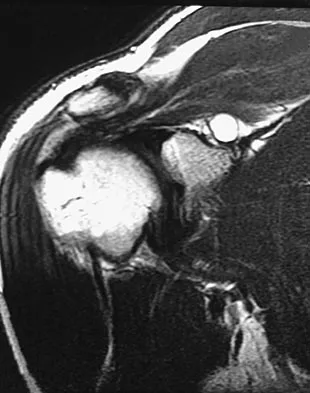
A 72-year-old woman who fell on her right shoulder while using a treadmill is now unable to elevate her right arm. An MRI scan is shown in Figure 7. What is the most likely diagnosis?

Explanation
The MRI scan reveals a large chronic rotator cuff tear with retraction and fatty infiltration atrophy of the supraspinatus and infraspinatus tendons. This tear is responsible for the patient's severe weakness and inability to elevate the arm.
Question 731
High Yield
A 35-year-old man has had a mass on the bottom of his foot for the past 6 months. He reports that initially the mass was exquisitely painful but now is minimally tender. Examination reveals a 2.5- x 2.0-cm firm, noncompressible, nonmobile mass contiguous with the plantar fascia in the distal arch. The mass is particularly prominent with passive dorsiflexion of the ankle and toes. What is the best course of action?
Explanation
The history is most consistent with a plantar fibroma. The nodules typically are located within the substance of the plantar aponeurosis. The clinical appearance is usually diagnostic without the need for advanced imaging studies. While the lesion may be prominent and painful to direct palpation, the anatomic location is usually off of the weight-bearing surface. Observation with or without an accommodative orthotic is the treatment of choice. Recurrence is common following attempted excision. Sammarco GJ, Mangone PG: Classification and treatment of plantar fibromatosis. Foot Ankle Int 2000;21:563-569.
Question 732
High Yield
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of

Explanation
The patient has a displaced fracture of the apophysis of the olecranon for which most authorities recommend surgical treatment. In older children, stability of the reduction may be achieved by the use of two parallel medullary Kirschner wires and a figure-of-8 tension band loop of either stainless steel wire or absorbable suture. The use of an absorbable suture does not require removal of the implant. Absorbable suture alone is best used in very young patients who have this type of injury. An intramedullary screw would pose an unnecessary risk of future growth disturbance. A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma. Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033. Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Question 733
High Yield
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of
Explanation
Loss of internal rotation is common among overhead throwers and tennis players. Posterior capsular stretching can improve symptoms when accompanied by rest and gradual resumption of throwing. To avoid a false impression of improvement, cortisone injection is not recommended. Pitching through pain can cause further damage to the labrum and capsule. A sling and external rotator strengthening will not improve internal rotation. Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Question 734
High Yield
A 14-year-old boy reports progressive right wrist pain. Radiographs are shown in Figure 3a, and a photomicrograph is shown in Figure 3b. What is the most likely diagnosis?

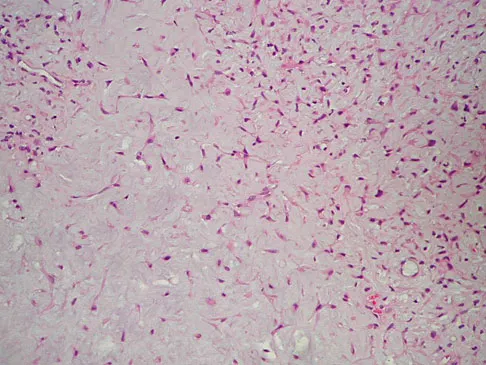
Explanation
The radiographs show a benign-appearing, well-defined lytic lesion with a thin rim of surrounding reactive bone. The photomicrograph shows spindle cells with a myxoid cartilaginous matrix. These findings are diagnostic of chondromyxoid fibroma. This is a rare, benign tumor that usually causes pain and can be locally aggressive. Lersundi A, Mankin HJ, Mourikis A, et al: Chondromyxoid fibroma: A rarely encountered and puzzling tumor. Clin Orthop Relat Res 2005;439:171-175.
Question 735
High Yield
After making a tackle, a football player is found prone and unconscious without spontaneous respirations. Initial management should consist of

Explanation
The on-field evaluation and management of a seriously injured athlete requires that health care teams have a game plan in place and proper equipment that is readily available. The initial step, which consists of stabilizing the head and neck by manually holding them in a neutral position, is then followed by assessment of breathing, pulses, and level of consciousness. If the athlete is breathing, management should consist of mouth guard removal and airway maintenance. If the athlete is not breathing, the face mask should be removed, with the chin strap left in place. The airway must be established, followed by initiation of assisted breathing. CPR is instituted only when breathing and circulation are compromised. In the unconscious athlete or if a cervical spine injury is suspected, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated. McSwain NE, Garnelli, RL: Helmet removal from injured patients. Bull of Am Coll Surg 1997;82:42-44.
Question 736
High Yield
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include

Explanation
The patient has a cyclops lesion. This is a nodule of fibroproliferative tissue that originates from either drilling debris from the tibial tunnel or remnants of the ACL stump; more rarely it is the result of broken graft fibers. The treatment of choice is excision of the nodule and, if needed, additional notchplasty. Marked improvements in function and symptoms have been noted after removal of the extension block and resumption of a rehabilitation program. Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Question 737
High Yield
A 57-year-old man has had right ankle pain for the past 10 months following an injury that went untreated. Radiographs are shown in Figures 30a through 30c. Management should consist of



Explanation
The radiographs reveal a malunited distal fibular fracture with shortening. Because there appears to be an adequate cartilage space within the ankle joint, the role of reconstruction would be to prevent arthrosis and the need for ankle arthrodesis, as well as to decrease symptoms. The treatment of choice is restoration of fibular length, alignment, and rotation with osteotomy plating, and bone grafting as needed. There is no indication for ligament reconstruction of a mechanically stable ankle, and tibial shortening osteotomy will not assist in correcting the deformity. Cast immobilization may assist with improvement of symptoms but will not correct the overall process. Determination of fibular length is best done by comparing the talocrural angle of the injured side with the uninjured side. The goal is to perfectly reduce the talus in the ankle mortise. Marti RK, Raaymakers EL, Nolte PA: Malunited ankle fractures: The late results of reconstruction. J Bone Joint Surg Br 1990;72:709-713. Geissler W, Tsao A, Hughes J: Fractures and injuries of the ankle, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 2201-2206.
Question 738
High Yield
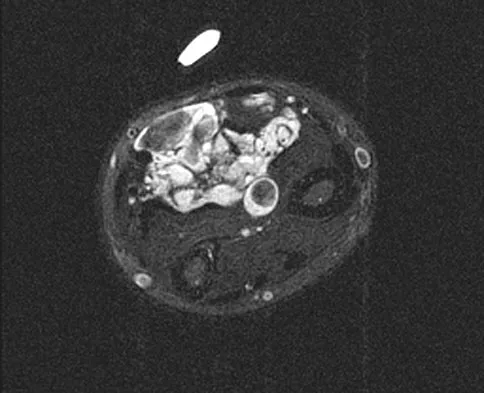
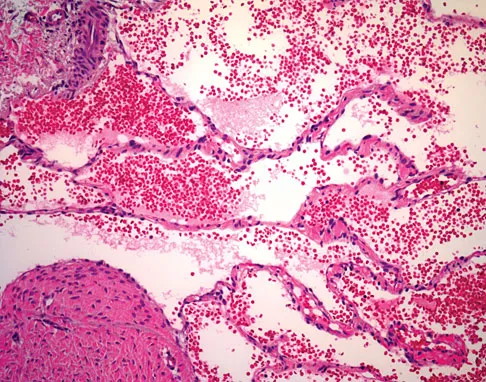
A 7-year-old girl has had a painful forearm for the past 2 months. Examination reveals fullness on the volar aspect of the forearm. Radiographs and an MRI scan are shown in Figures 42a through 42c. Biopsy specimens are shown in Figures 42d and 42e. What is the most likely diagnosis?


Explanation
The radiographs reveal phleboliths on the volar side of the forearm consistent with hemangioma. The MRI scan reveals a rather well-circumscribed in size, irregular in shape, intramuscular soft-tissue mass in the volar aspect of the distal right forearm within the flexor group musculature. The mass demonstrates heterogeneous mixed signal intensity in both T1- and T2-weighted sequences with increased signal intensity on the T1, suggesting fat within the tumor, typical of hemangioma. The postgadolinium-enhanced sequences demonstrate heterogeneous enhancement. The MRI findings are consistent with a soft-tissue hemangioma. Garzon M: Hemangiomas: Update on classification, clinical presentation and associate anomalies. Cutis 2000;66:325-328.
Question 739
High Yield
A 15-year-old boy falls from his bicycle and sustains an injury to his elbow. Prereduction radiographs are shown in Figure 12a. Closed reduction is performed without difficulty and postreduction radiographs are shown in Figure 12b. What is the next most appropriate step in treatment?


Explanation
Elbow dislocations in children are rare injuries and usually result from a fall on an outstretched arm. The incidence of these injuries increases as patients age and concurrently the incidence of supracondylar humerus fractures decreases. In adolescent patients, simple elbow dislocations are treated with splint immobilization and the initiation of physical therapy once comfortable. The practitioner must be aware of structures that may get caught in the joint on reduction. These include the median nerve as well as the medial epicondyle. In this patient, the radiographs reveal a medial epicondyle fracture. Postreduction radiographs show the joint to be incongruous secondary to intra-articular displacement. At this point, the most appropriate treatment is to perform an open reduction and repair of the medial epicondyle fragment. Rasool MN: Dislocations of the elbow in children. J Bone Joint Surg Br 2004;86:1050-1058.
Question 740
High Yield
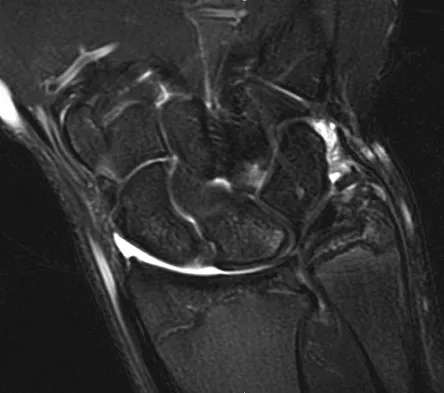
An MRI arthrogram of the elbow is shown in Figure 6. Based on these findings, what is the most likely diagnosis?

Explanation
MRI arthrography is the imaging study of choice for evaluation of medial collateral ligament injuries. Carrino JA, Morrison WB, Zou KH, et al: Noncontrast MR imaging and MR arthrography of the ulnar collateral ligament of the elbow: Prospective evaluation of two-dimensional pulse sequences for detection of complete tears. Skeletal Radiol 2001;30:625-632.
Question 741
High Yield
Which of the following treatment regimens for thromboembolic prophylaxis meets the American College of Chest Physicians Guidelines for 10-day treatment after total hip arthroplasty and total knee arthroplasty?

Explanation
Only three thromboembolic treatment protocols have reached Grade 1A status for the American College of Chest Physicians Guidelines for thromboembolic prophylaxis after total hip arthroplasty and total knee arthroplasty. Grade 1A evidence shows a clear benefit/risk improvement with supportive data from randomized clinical trials, which are strongly applicable in most clinical circumstances. Warfarin is recommended but at an INR level of 2 to 3. Low-molecular-weight heparin and fondaparinox are also acceptable treatment options. Aspirin, adjusted dose unfractionated heparin, and elastic compressive stockings are not recommended as stand-alone options. Colwell C: Evidence based guidelines for prevention of venous thromboembolism: Symposia. Proceedings of the 2005 AAOS Annual Meeting. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-18.
Question 742
High Yield
Figures 5a and 5b show the radiographs of a 56-year-old man who was seen in the emergency department following a twisting injury to his left ankle. Examination in your office 3 days later reveals marked swelling and diffuse tenderness to palpation about the ankle and leg. What is the next most appropriate step in management?


Explanation
The radiographs show an isolated posterior malleolus fracture which, given the injury mechanism, is highly suspicious for a Maisonneuve injury. As with any suspected extremity injury, radiographs including the joints above and below the level of injury are acutely indicated. Although MRI may reveal a ligamentous injury to the ankle and CT may show asymmetry of the ankle mortise or syndesmosis, both studies are considerably more costly and are not indicated in the absence of a complete radiographic work-up. Technetium bone scan is nonspecific and would be of limited value in this instance, as would repeat radiographs of the ankle. Walling AK, Sanders RW: Ankle fractures, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 1973-2016.
Question 743
High Yield
A patient who sustained a knife wound to the axilla 4 months ago now has profound interosseous wasting and generalized hand weakness. A brachial plexus injury is likely at which of the following locations in Figure 29?
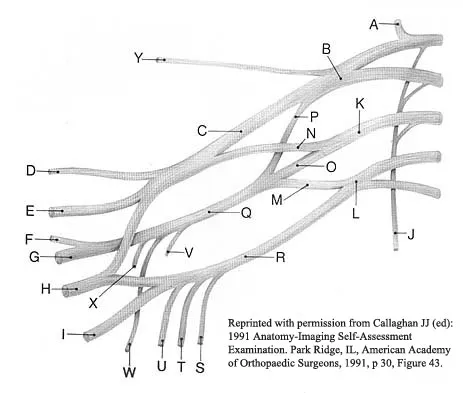
Explanation
Penetrating sharp wounds in proximity to major nerve or vascular structures should always be acutely explored. Because this patient did not seek treatment for a potentially treatable injury, interosseous wasting implies injury to the C8 and T1 nerve roots that contribute to ulnar nerve function. The most likely location for the brachial plexus injury is the location marked L or the inferior trunk. A wrist drop that is the result of radial nerve dysfunction would be expected with an injury at K or O. An upper brachial plexus palsy with loss of elbow flexion and shoulder abduction would be expected with an injury at B. A loss of elbow flexion alone would be expected following an injury at C. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, pp 28-29. Wolock B, Millesi H: Brachial plexus-applied anatomy and operative exposure, in Gelberman RH (ed): Operative Nerve Repair and Reconstruction. Philadelphia, PA, JB Lippincott, 1991, vol 2, pp 1255-1272.
Question 744
High Yield
Figure 35 shows the radiograph of a 12-year-old boy who fell off a snowmobile and landed on his left shoulder. He has a closed injury. Management should consist of

Explanation
Proximal humeral fractures in children are classified as metaphyseal or Salter-Harris type I or II fractures, and most of these fractures are treated with closed methods. Eighty percent of the growth of the humerus comes from the proximal physis; therefore, tremendous remodeling potential is present. Indications for open reduction include open fractures or severely displaced fractures in adolescents with minimal growth remaining. Acceptable limits of reduction in adolescent proximal humeral fractures include bayonet apposition and angulation of less than 35 degrees. Common blocks to reduction in adolescents include the biceps tendon and periosteum. For this fracture, use of a shoulder sling without reduction will lead to healing and an excellent result as the proximal humerus remodels. Kohler R, Trillaud JM: Fracture and fracture separation of the proximal humerus in children: Report of 136 cases. J Pediatr Orthop 1983;3:326-332. Beaty JH: Fractures of the proximal humerus and shaft in children. Instr Course Lect 1992;41:369-372. Dobbs MB, Luhmann SL, Gordon JE, et al: Severely displaced proximal humeral epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Beringer DC, Weiner DS, Noble JS, et al: Severely displaced proximal humeral epiphyseal fractures: A follow-up study. J Pediatr Orthop 1998;18:31-37.
Question 745
High Yield
Free flap coverage for severe trauma to the upper extremity has the fewest complications when performed within what time period after injury?
Explanation
Flap necrosis and infection rates are lowest if free flap coverage is performed within 72 hours of injury. Delays beyond 72 hours are associated with a higher rate of complications. Godina M: Early microsurgical reconstruction of complex trauma of the extremities. Plast Reconstr Surg 1986;78:285-292.
Question 746
High Yield
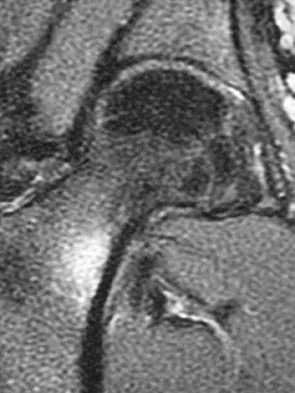
A 15-year-old girl who swims the breaststroke has had hip pain after training excessively for a national level competition. Based on the MRI scans shown in Figures 5a through 5c, what is the most likely diagnosis?
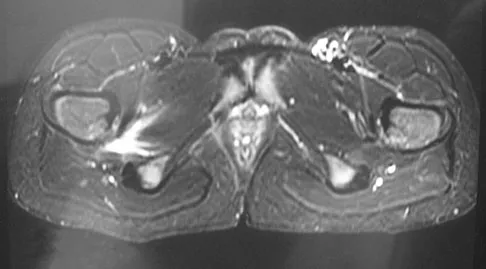

Explanation
The MRI scans reveal open physes but no evidence of a slipped capital femoral epiphysis, labral tear, or acetabular dysplasia. The femoral neck does not show evidence of a fracture. The muscle tear seen on the right side lies near the musculotendinous junction of the external rotators of the hip at the level of the lesser trochanter, representing the obturator externus. This is consistent with the forced motion required for the breaststroke kick. Grote K, Lincoln TL, Gamble JG: Hip adductor injury in competitive swimmers. Am J Sports Med 2004;32:104-108.
Question 747
High Yield
Figure 12 shows the radiograph of a 15-year-old boy with cerebral palsy who has pain at the first metatarsophalangeal joints. He is a community ambulator. Management consisting of accommodative shoes has failed to provide relief. What is the treatment of choice?

Explanation
While other surgeries have provided some success, first metatarsophalangeal joint arthrodesis has the highest overall success rate compared to other surgeries in ambulatory and nonambulatory children with cerebral palsy. The recurrence rate is unacceptably high with the other procedures listed above. In contrast, neurologically normal children are amenable to osteotomies and soft-tissue procedures. Davids JR, Mason TA, Danko A, et al: Surgical management of hallux valgus deformity in children with cerebral palsy. J Pediatr Orthop 2001;21:89-94.
Question 748
High Yield
Figure 39 shows the radiograph of a 4-month old infant who has been undergoing weekly casting since birth for a congenital equinovarus deformity. Management should now consist of

Explanation
The radiograph shows the development of a rocker-bottom foot deformity. A rocker-bottom foot occurs in the treatment of clubfoot when casting is continued in the presence of a very tight gastrocnemius-soleus complex and an uncorrected hindfoot. While there are some preliminary reports on using Botox injection and continued casting for the equinus deformity, most authors recommend posterior or posterior medial release. Percutaneous tenotomy has been recently recommended with the resurgence of the Ponsetti technique. Lehman WB, Atar D: Complications in the management of talipes equinovarus, in Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 135-136. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 927-935.
Question 749
High Yield
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of



Explanation
Tarsal coalitions commonly present in the preadolescent age group as a rigid, planovalgus foot. Small coalitions of the calcaneonavicular joint or the middle facet of the talocalcaneal joint can be excised with interposition of fat or muscle tissue. Isolated calcaneocuboid joint coalitions are very rare. This patient has an associated large talocalcaneal coalition; therefore, resection is contraindicated. Surgery is warranted after failure of nonsurgical management, and because of the involvement of two joints, the only viable option for the severely symptomatic foot is triple arthrodesis. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 750
High Yield
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include

Explanation
In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
Question 751
High Yield
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?

Explanation
Excision of the fracture fragment typically leads to rapid return to function. Fixation techniques are difficult to perform because of the size of the bone; hardware prominence is common. Nerve deficits are not typically noted in this injury. The motor branch of the ulnar nerve in Guyon's canal must be protected during the surgical approach. Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Question 752
High Yield
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of

Explanation
The patient has a stable bony fracture that will heal with immobilization in a rigid collar. Flexion-extension radiographs may be obtained at 6 weeks to verify that there is no instability; mobilization may then be begun.
Question 753
High Yield
A 58-year-old woman with a history of severe asthma and long-term prednisone use reports a progression of chronic shoulder pain for the past 6 months. Radiographs and MRI scans are shown in Figures 30a through 30d. What is the most likely diagnosis?


Explanation
The patient has osteonecrosis of the humeral head. The radiographs show increased density in the superior subchondral region of the humeral head. The MRI scans reveal a central collapse of the humeral head. The patient's history of severe asthma and long-term prednisone use predisposes her to this condition. The MRI scans show no evidence of a full- or partial-thickness rotator cuff tear. Without a history of fevers, chills, or other systemic signs or symptoms, there is no indication of septic arthritis. The radiographs do not reveal periarticular erosions, commonly seen in rheumatoid arthritis. Matsen FA III, Rockwood CA Jr, Wirth MA, et al: Glenohumeral arthritis and its management, in Rockwood CA Jr, Matsen FA III (eds): Rockwood and Matsen The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 871-874.
Question 754
High Yield
A 24-year-old man who works at a local oyster and clam farm sustained a laceration on his hand at work. Examination reveals a cellulitic index finger without evidence of tenosynovitis. After appropriate irrigation and debridement, what antibiotic is most appropriate?
Explanation
Injuries involving brackish water and shellfish can have devastating consequences caused by Vibrio vulnificus infections. Patients may have a severe invasive infection, with three main clinical features: primary septicemia, wound infection, and gastroenteritis. Antibiotic administration is crucial because mortality rates of up to 50% have been observed with Vibrio septicemia. The current recommendation is to give a third-generation cephalosporin such as ceftazadime. Chiang SR, Chuang YC: Vibrio vulnificus infection: Clinical manifestations, pathogenesis, and antimicrobial therapy. J Microbiol Immunol Infect 2003;36:81-88.
Question 755
High Yield
Figure 36 shows the radiograph of a patient who has hip pain and is unable to ambulate. What is the most appropriate management for this patient?

Explanation
The patient has a periprosthetic fracture of the greater trochanter - Vancouver A. The reason for the fracture of the greater trochanter is the extensive periarticular osteolysis that has occurred as a result of polyethylene wear. The latter is demonstrated by eccentric seating of the large femoral head in the acetabulum. The most appropriate management is to reverse the osteolysis process, which involves exchange of the acetabular liner with or without revision of the other components depending on their fixation and position. The greater trochanter can also be fixed during revision surgery. Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Question 756
High Yield
A 35-year-old patient has right hip pain. Figures 34a and 34b show the coronal MRI scan and the biopsy specimen. What is the most likely diagnosis?


Explanation
Alcohol abuse, steroids, Caisson disease, sickle cell disease, and radiation therapy are the leading causes of nontraumatic osteonecrosis of the femoral head. Arlet J: Nontraumatic avascular necrosis of the femoral head: Past, present, and future. Clin Orthop 1992;277:12-21.
Question 757
High Yield
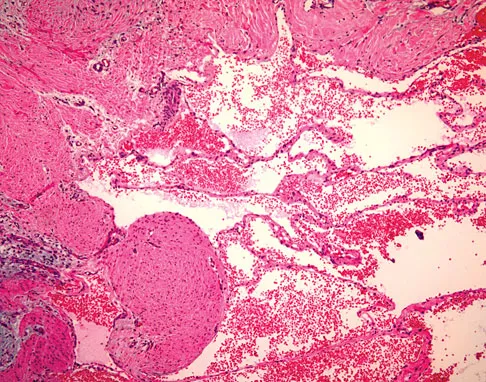
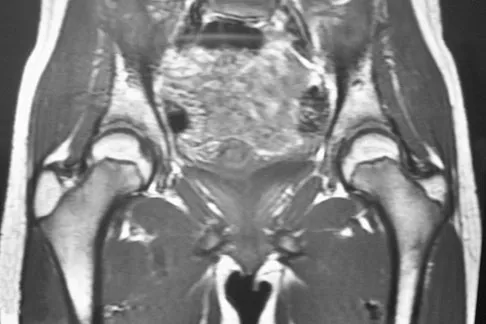
A 43-year-old woman has an enlarging mass in the left groin. A radiograph, CT scan, and a biopsy specimen are shown in Figures 42a through 42c. Treatment should consist of

Explanation
The patient has a pelvic chondrosarcoma. The radiograph shows a lytic bone lesion emanating from the left inferior pubic ramus and extending into the soft tissues. Punctate calcifications are revealed on the radiograph and CT scan. The histology is consistent with a malignant cartilage lesion. Appropriate treatment for a pelvic chondrosarcoma is wide resection. In this location, wide resection of the ischiopelvic region (type 3 internal hemipelvectomy) is the treatment of choice. A type 2 internal hemipelvectomy involves resection of the periacetabular region. A type 1 internal hemipelvectomy involves resection of the ilium. No reconstruction is required for a type 3 resection. A classic hemipelvectomy is not necessary because the tumor can be removed with an adequate margin while maintaining the neurovascular structures and hip joint. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642. Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, Romsdahl MM: Chondrosarcoma of the pelvis: Prognostic factors for 67 patients treated with definitive surgery. Cancer 1996;78:745-750.
Question 758
High Yield
A 22-year-old woman injures her neck in a motor vehicle accident. Examination reveals no sensory or motor function below T8. Radiographs and an MRI scan show a burst fracture at T7. Forty-eight hours later, the bulbocavernosus reflex is present but there is no evidence of motor or sensory recovery in the lower extremities. What is the most likely diagnosis?

Explanation
Spinal shock typically ends after 48 hours with the return of reflexes, including the bulbocavernosus reflex. Lack of motor or sensory recovery in the lower extremities with the return of reflexes generally indicates a complete cord syndrome. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Question 759
High Yield
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?

Explanation
The photomicrograph demonstrates a wedge-shaped infarct with femoral head collapse; therefore, the diagnosis is osteonecrosis of the femoral head. Perthes disease and osteoarthritis do not involve a wedge-shaped defect. Tuberculosis of the hip joint results in greater destruction of the articular cartilage. Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.
Question 760
High Yield
A 63-year-old man with type I diabetes mellitus who underwent open forefoot amputation now has a high fever, and an elevated WBC count and blood glucose levels. Repeat laboratory studies the day after surgery show a WBC count of 9,500/mm3, a serum albumin level of 1.9 g/dL, and a total lymphocyte count of 1,900/mm3. Examination reveals that he is afebrile, and his blood glucose level is now normal. An ultrasound Doppler of the dorsalis pedis artery shows an ankle-brachial index of 0.6. A transcutaneous partial pressure measurement of oxygen at the ankle joint shows a level of 38 mm Hg. What is the best course of action?

Explanation
This patient appears to have adequate blood supply to heal a Syme's ankle disarticulation but is currently malnourished because of the systemic infection, and is likely to progress to wound failure. Therefore, the initial management of choice is culture-specific antibiotic therapy, open wound management, and nutritional supplementation. If his serum albumin rises to a minimum of 2.5 gm/dL, he can undergo elective Syme's ankle disarticulation. If the serum albumin does not rise within a short period of time, he should undergo transtibial amputation.
Question 761
High Yield
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
The steel shank is a flat 1-inch steel strip placed between layers of the shoe to extend the foot lever and prevent deformity at the toe break seen following a partial first ray amputation. A rocker sole may be added as well to facilitate transition from foot flat to the toe-off phase of gait. Proper shoe fit is important, but "snug" fitting shoes in a patient with peripheral neuropathy and likely fluctuations in volume from intermittent swelling are to be avoided. A custom shoe is an unnecessary expense. The patient has at least 10 degrees of dorsiflexion at the ankle with an intact anterior tibialis muscle; therefore, catching the sole on carpeting should not be a problem. Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Question 762
High Yield
A 15-year-old boy has a mass at the knee. Radiographs show an aggressive tumor involving the proximal tibia, and biopsy findings reveal a high-grade osteosarcoma. Staging studies show that the tumor impinges on the neurovascular bundle. The tumor enlarges during preoperative chemotherapy. Management should now consist of

Explanation
Limb salvage procedures have become the usual treatment for even high-grade osteosarcomas. However, tumors associated with pathologic fracture, tumors encasing the neurovascular bundle, and tumors that enlarged during preoperative therapy and are adjacent to the neurovascular bundle require amputation.
Question 763
High Yield
What acetabular procedure for developmental dysplasia of the hip does not require a concentric reduction of the femoral head in the acetabulum?
Explanation
All of the reorientation innominate osteotomies require a concentric reduction of the hip. The Staheli shelf procedure may be performed even with the hip subluxated, but it is a salvage procedure that covers a portion of the femoral head with capsular fibrocartilage rather than hyaline cartilage. Staheli LT, Chew DE: Slotted acetabular augmentation in childhood adolescence. J Pediatr Orthop 1992;12:569-580.
Question 764
High Yield
The posterior horn of the medial meniscus receives its primary blood supply from what artery?
Explanation
The middle genicular artery supplies the posterior capsule and intracapsular structures (anterior cruciate ligament, posterior cruciate ligament, posterior horns of the meniscus). The medial and lateral inferior geniculates anastomose anteriorly to form a capillary network to supply the fat pad, synovial cavity, and patellar tendon. The lateral superior and inferior genicular arteries supply the lateral retinaculum. Insall J, Scott WN: Anatomy, in Surgery of the Knee, ed 3. Philadelphia, PA, Churchill Livingstone, 2001, pp 64-70.
Question 765
High Yield
What is the most common secondary malignancy arising in pagetic bone?

Explanation
The incidence of malignant transformation or the formation of a secondary malignancy in pagetic bone is estimated to be less than 1%. Osteosarcoma is the most common secondary malignancy, followed by fibrosarcoma and chondrosarcoma. Ewing's sarcoma arising in pagetic bone has not been reported. Grimer RJ, Carter SR, Tillman RM, et al: Osteosarcoma of the pelvis. J Bone Joint Surg Br 1999;81:796-802.
Question 766
High Yield
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
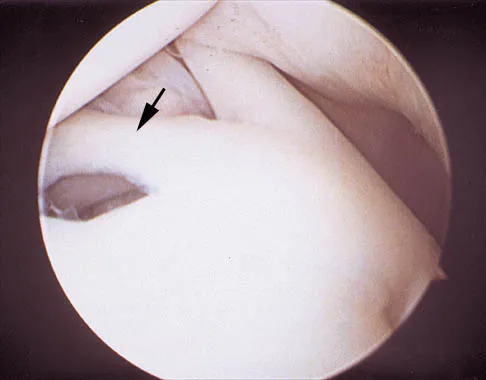
Explanation
The photograph shows a normal variant that is a sublabral hole beneath the anterosuperior labrum. In some instances, the labrum will become confluent with the middle glenohumeral ligament as a stout band. Because this variant is not abnormal, no treatment is necessary. Securing this portion of the labrum to the capsule may tighten the middle glenohumeral ligament complex and restrict external rotation of the arm. Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Question 767
High Yield
A 9-year-old boy sustained a traumatic brain injury and right lower extremity trauma in an accident involving a motor vehicle and a pedestrian. Initial evaluation in the emergency department reveals an obtunded patient who is breathing spontaneously and withdraws appropriately to painful stimuli. After initial resuscitation and stabilization, a CT scan reveals a right parietal intracranial hemorrhage. Radiographs of the swollen right thigh are shown in Figures 32a and 32b. Management of the fractured femur should ultimately consist of


Explanation
A child with a traumatic brain injury generally achieves significant neurologic recovery and has a more favorable prognosis than an adult. Early stabilization of fractures facilitates transportation of the child for diagnostic tests and decreases the incidence of shortening and malunion. Surgical treatment of the fracture is indicated when cerebral perfusion pressure has stabilized. Casting or traction is not the most appropriate treatment of a femoral fracture in a child of this age with a brain injury. Fracture reduction is difficult to maintain if the brain injury leads to spasticity, and transportation within the hospital for tests is more difficult. Insertion of a reamed antegrade intramedullary nail inserted at the piriformis fossa is associated with a small risk of osteonecrosis of the femoral head. The transverse femoral fracture in this patient is ideally suited for stabilization with flexible intramedullary nails. Ligier and associates treated 123 femoral shaft fractures in children with flexible intramedullary nails, including 35 patients with head injury. In one patient with hemiplegia and a urinary tract infection, a deep wound infection developed, necessitating nail removal. The remaining patients all healed without major complications. Heinrich and associates treated 78 diaphyseal femoral fractures with flexible intramedullary nails, including 14 with head injury. No major complications were reported and all fractures healed. Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 83-95. Ligier JN, Metaizeau JP, Prevot J, et al: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77. Heinrich MS, Drvaric DM, Darr K, et al: The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: A prospective analysis. J Pediatric Orthop 1994;14:501-507.
Question 768
High Yield
When performing a posterior cruciate ligament reconstruction with a tibial inlay-type approach, what is the approximate anatomic distance of the popliteal artery from the screws used for fixation of the bone block?
Explanation
Miller and associates reported the results of a cadaveric study of the vascular risk of a posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. The average distance from the screw to the popliteal artery was 21.1 mm (range, 18.1 mm to 31.7 mm). Other approaches, such as the transtibial tunnel technique which involves drilling an anterior-posterior tunnel, have also been studied in cadavers. Matava and associates noted that increasing flexion reduces but does not completely eliminate the risk of arterial injury during arthroscopic posterior cruciate ligament reconstruction. However, this study did not use the small, medial utility incision recommended by Fanelli and associates, which creates an interval for the surgeon's finger between the medial gastrocnemius and the posteromedial capsule so that any migration of the guidepin can be palpated and changed prior to any injury to the posterior neurovascular bundle. Matava MJ, Sethi NS, Totty WG: Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: Implications for posterior cruciate ligament reconstruction. Arthroscopy 2000;16:796-804. Miller MD, Kline AJ, Gonzales J, et al: Vascular risk associated with posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique. J Knee Surg 2002;15:137-140.
Question 769
High Yield
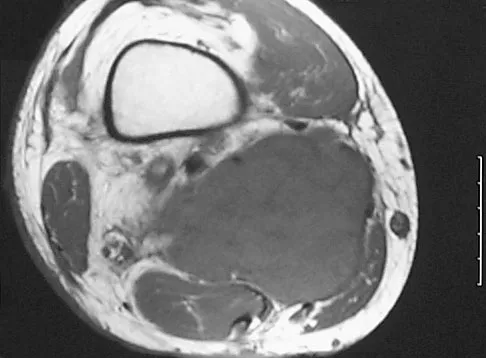
A 22-year-old professional baseball catcher has posterior shoulder pain and severe external rotation weakness with the arm in adduction. Radiographs are normal. MRI scans are shown in Figures 15a through 15c. Management should consist of
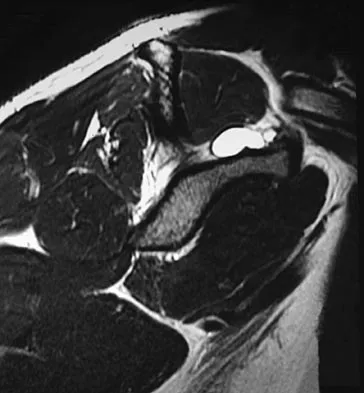

Explanation
The MRI scans reveal a large posterior paralabral cyst associated with a posterior-superior labral tear. The cyst appears as a well-defined, smoothly marginated mass with low signal intensity on T1-weighted MRI scans and with high signal intensity on T2-weighted MRI scans. MRI also reveals changes in the supraspinatus and infraspinatus muscles secondary to denervation, including decreased muscle bulk and fatty infiltration. MRI has the added advantage, compared with other imaging modalities, of detecting intra-articular lesions, such as labral tears, which are frequently associated with ganglion cysts of the shoulder. In this case of a professional baseball player with a space-occupying lesion causing nerve compression with an associated labral tear, the treatment of choice is arthroscopic decompression of the cyst and repair of the tear. Acromioplasty would not address the primary pathology in this patient. Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Question 770
High Yield
A 26-year-old man is brought to the emergency department unresponsive and intubated after being found lying on the side of the road. He has a Glasgow Coma Scale score of 6. A chest tube has been inserted on the right side of the chest for a pneumothorax. An abdominal CT scan reveals a small liver laceration and minimal intraperitoneal hematoma. A pneumatic antishock garment (PASG) is on but not inflated. He has bilateral tibia fractures. A pelvic CT scan shows an anterior minimally displaced left sacral ala fracture and left superior and inferior rami fractures. He has received 2 L of saline solution and 4 units of blood but remains hemodynamically unstable. What is the next most appropriate step in management?

Explanation
There is no identifiable thoracic, abdominal, or long bone source of ongoing bleeding. The patient has a lateral compression Burgess-Young type I pelvic ring injury. This injury does not increase the pelvic volume because it is not unstable in external rotation. Application of a PASG, a pelvic clamp, or an external fixator may be helpful if the patient has a pelvic injury that is unstable in external rotation or translation but would be of little use in this injury pattern. Persistent hemodynamic instability after administration of 4 units of blood is the decision point where most authors would recommend angiography and embolization. If the pelvis is unstable in external rotation or translation, inflation of the PASG trousers or application of an external fixator is recommended before angiography. Attributing the hemodynamic instability to the head injury before ruling out the pelvis as a source is not indicated. Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: Effective classification system and treatment protocols. J Trauma 1990;30:848-856. Evers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: Priorities in management. Arch Surg 1989;124:422-424.
Question 771
High Yield
What is the correct order of the elastic modulus of the following materials from greatest to least?

Explanation
In Young's modulus of elasticity, E is a measure of the stiffness of a material and its ability to resist deformation. In the elastic region of the stress-stain curve, E = stress/strain. The moduli of elasticity for these materials are alumina ceramic = 380 Gigapascals (GPa), cobalt-chromium = 210 GPa, stainless steel = 190 GPa, titanium = 116 GPa, and PMMA = 1.1 to 4.1 GPa. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 182-215.
Question 772
High Yield
The incidence of osteosarcoma is highest in what age group?

Explanation
The peak incidence of osteosarcoma occurs in the second decade, followed by the third decade. Up to 75% of all cases of osteosarcoma occur in patients between 10 and 25 years. It rarely occurs after age 30. Affected women tend to be younger than affect men. Osteosarcoma associated with Paget's disease or in radiation-induced osteosarcoma occurs in an older population. Simon M, Springfield D, et al: Osteogenic Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 266. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989.
Question 773
High Yield
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should

Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Question 774
High Yield
Which of the following clinical disorders is the result of a mutation in fibroblast growth factor recepter 3 (FGFR3)?
Explanation
Camptomelic dysplasia is caused by a heterozygous loss of function of the Sox9 gene. The alternatives have genetic causes, but are not linked to Sox9. Cleidocranial dysplasia is related to a defect in Cbfa-1 (Osf-2, Runx2). Schmid metaphyseal chondrodysplasia is related to Type X collagen. Fibrous dysplasia is related to a defect in the alpha subunit of stimulatory guanine-nucleotide-binding protein (Gs). Achondroplasia is related to a defect in fibroblast growth factor receptor 3. Wagner T, Wirth J, Meyer J, et al: Autosomal sex reversal and camptomelic dysplasia are caused by mutations in and around the SRY-related gene SOX9. Cell 1994;79:1111-1120. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 111-131.
Question 775
High Yield
Mechanical reduction of the pain associated with the condition shown in Figure 6 can be accomplished through the use of a cane on the contralateral side. Similarly, if this patient must carry any type of load in his or her arms, it should be carried

Explanation
Patients with diseased hips often must carry objects while walking, yet they are rarely instructed on which hand to use. The patient should be directed to carry the object on the ipsilateral side, just the opposite of the side he or she would use a cane. The cane pushes up on the weight of the body so that when the patient is carrying a load, the weight in the hand on the same side as the hip pushes up on the weight of the body, but now the patient has the fulcrum of the hip in between. Tan and associates mathematically determined the hip forces that result when a load is carried in the ipsilateral hand versus the contralateral hand. Using a free-body diagram of a single-leg supported stance, they found that when a load was carried in the contralateral hand, the resultant forces on the hip were increased considerably. Conversely, when the weight was carried in the ipsilateral hand, the forces were actually lower than when no weight was carried at all. Therefore, carrying a weight on the opposite side resulted in hip forces that were substantially greater than when the weight was carried on the same side.
Question 776
High Yield
An elderly patient falls and sustains an extension injury to the neck that results in upper extremity weakness, spared perianal sensation, and lower extremity spasticity. These findings best describe what syndrome?
Explanation
These finding indicate central cord syndrome, and injury that is more common in the older population who have some degree of spondylosis. The physiologic insult can be a central spinal hematoma with resultant hematomyelia. Bowel and bladder functional return has a good prognosis, unlike the upper extremity motor loss. Cauda equina syndrome generally involves injury at the lumbar levels, with some degree of lower extremity motor loss. Posterior cord syndrome is characterized by preservation of motor function below the level of injury and position/vibratory sensory loss. Brown-Sequard syndrome, which is often produced by a penetrating injury, results in contralateral hypalgesia and ipsilateral weakness. Anterior cord syndrome has a poor prognosis for functional return; lower extremity findings include loss of light touch, sharp/dull, and temperature sensations below the level of injury, as well as motor function. Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Question 777
High Yield
During a transperitoneal approach to the L5-S1 interspace, care must be taken to protect the superior hypogastric plexus from injury. Which of the following techniques reduces the risk of neurologic injury?

Explanation
Retrograde ejaculation is the sequela of superior hypogastric plexus injury. This structure needs protection, especially during anterior exposure of the L5-S1 disk space. Only blunt dissection should be used, and use of monopolar electrocautery should be avoided. If possible, preserve and retract the middle sacral artery. Once the iliac veins are isolated, blunt dissection is begun along the course of the medial edge of the left iliac vein, reflecting the prevertebral tissues toward the patient's right side. The dissection goes from left to right because the parasympathetic plexus is more adherent on the right side.
Question 778
High Yield
Figure 6 shows the lateral radiograph of a 22-year-old woman who has painful Scheuermanns's kyphosis in the middle and lower thoracic spine. When planning surgical correction using instrumentation, the distal aspect of the instrumentation should ideally extend to the

Explanation
Posterior constructs for Scheuermann's kyphosis ideally should extend from the most superior to the most inferior aspect of the Cobb angulation. However, the most distal fusion level must be in a stable or lordotic position to avoid the development of junctional kyphosis. Lowe reported that failure to incorporate the first lordotic segment of the lumbar spine is associated with a higher risk of junctional kyphosis. The first lordotic segment of the lumbar spine is typically at least one level below the distal aspect of the curve as measured by the Cobb technique and most commonly is in the upper part of the lumbar spine. Lowe TG: Scheuermann's disease. Orthop Clin North Am 1999;30:475-487.
Question 779
High Yield
A 46-year-old man fell 20 feet and sustained the injury shown in Figure 3. The injury is closed; however, the soft tissues are swollen and ecchymotic with blisters. The most appropriate initial management should consist of

Explanation
Although this is a fracture of the medial and lateral malleoli, the degree of displacement and comminution of the medial dome indicate that this injury is similar to a pilon fracture. Initial management should consistent of stabilization to allow for soft-tissue healing. The use of temporizing spanning external fixation should be the initial step, followed by limited or more extensive open reduction and internal fixation when the soft-tissue status will allow. Initial placement in either a short or long leg cast does not provide the needed stability and does not allow for care and monitoring of soft tissues. In addition, maintaining reduction of the talus may be very difficult. Immediate open reduction and internal fixation through an injured soft-tissue envelope adds the risk of difficulties with incision healing and a higher risk of deep infection. In the acute setting, a primary ankle fusion through this soft-tissue envelope is not indicated. Marsh JL, Bonar S, Nepola JV, et al: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509. Wyrsch B, McFerran MA, McAndrew M, et al: Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 1996;78:1646-1657.
Question 780
High Yield
Figures 4a through 4c show the radiographs, CT scans, and T1-weighted MRI scan of a 19-year old man who has had increasing right hip pain and decreasing range of motion for the past several years. He also reports intermittent "locking" of the hip. What is the most likely diagnosis?


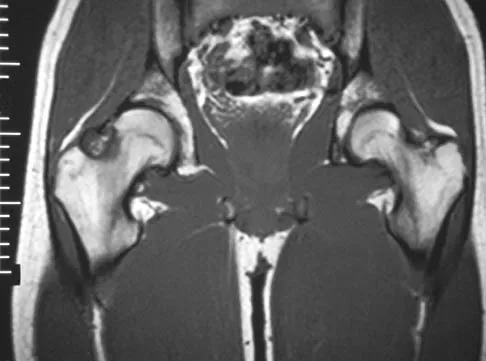
Explanation
The radiographs reveal small ossified masses around the femoral neck. The CT scans also show these masses and suggest that they are separate from the underlying cortex of the femoral neck, although they abut it. The MRI scan does not reveal significant marrow changes in the proximal femur apart from some mild reactive changes immediately adjacent to the nodules. These findings suggest a synovial or joint-based disorder as opposed to a primary bone tumor. The most likely diagnosis is synovial osteochondromatosis, which is consistent with the patient's mechanical symptoms. Crotty JM, Monu JU, Pope TL Jr: Synovial osteochondromatosis. Radiol Clin North Am 1996;34:327-342.
Question 781
High Yield
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?

Explanation
The patient has symptoms typical of Raynaud's phenomenon secondary to underlying vascular disease. The next most appropriate step in the management of this patient should be to perform contrast angiography on the involved upper extremity to look for proximal or distal arterial lesions or insufficiencies. MRI and contrast CT are not as specific as angiography for the identification of vascular lesions of the upper extremity. Although patients with primary Raynaud's vasospastic disease can have normal angiographic findings, they typically are younger than age 40 years, are female, and have normal results on an Allen test. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Question 782
High Yield
Figures 44a and 44b show the radiographs of a 28-year-old woman who has had progressive hip pain for the past 3 months. What is the most likely diagnosis?


Explanation
The patient has multiple hereditary exostoses and a secondary chondrosarcoma arising from a proximal femoral exostosis. The radiograph of the knee shows multiple osteochondromas typical in a patient with multiple hereditary exostoses. Patients with this diagnosis are at an increased risk for malignant degeneration of an osteochondroma. The lateral radiograph of the hip shows a bony lesion emanating from the anterior aspect of the femoral neck that is not well defined in the surrounding soft tissues. There are punctate calcifications and a large soft-tissue mass. The most likely diagnosis is a secondary chondrosarcoma developing from a benign osteochondroma. An enchondroma is an intramedullary benign cartilage lesion. Ollier's disease and Maffucci's syndrome involve multiple enchondromas. Scarborough M, Moreau G: Benign cartilage tumors. Orthop Clin North Am 1996;27:583-589.
Question 783
High Yield
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of

Explanation
The prognosis for most patients with Osgood-Schlatter disease is good. When the secondary ossification center unites with the main body of the tibial tubercle, the patellar tendon has a more rigid anchor, and heterotopic ossification and its associated reaction often become quiescent. However, even after closure of the growth plates, some patients have persistent symptoms. Excision of the ossicle and prominence of the tibial tuberosity decompresses the patellar tendon and allows most patients to resume sports activities. Nonsurgical modalities are ineffective. Better results have been reported after excision than after drilling of the tubercle. Excision of the ossicle is not indicated prior to skeletal maturity because symptoms will resolve in most patients when the secondary ossification center unites. Flowers MJ, Bhadreshwar DR: Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J Pediatr Orthop 1995;15:292-297.
Question 784
High Yield
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?


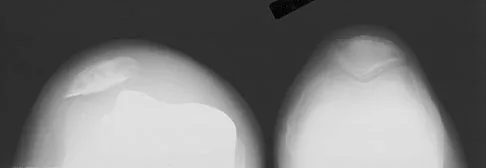
Explanation
The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first. Kelly MA: Extensor mechanism complications in total knee arthroplasty. Instr Course Lect 2004;53:193-199. Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Question 785
High Yield
A 20-year-old basketball player reports a 6-month history of right groin pain that radiates into his testicles with activities of daily living. He denies any history of trauma. Examination reveals tenderness about the groin, and he has full hip range of motion. The abdomen is soft. Radiographs are normal. Nonsurgical management has consisted of rest and physical therapy, but he continues to have pain. What is the next step in management?
Explanation
Sports hernias may be one of the most common causes of groin pain in athletes. Resisted hip adduction is painful in the case of groin disruption. Radiation of pain into the testicles and/or adductor region is often present. Sports hernias are associated with weakening of the posterior inguinal wall. In contrast with sports hernias, traditional or classic hernias can be readily detected on physical examination. Diagnostic imaging studies are not helpful and only serve to help exclude other diagnoses. Systemic high-dose steroids or sacroiliac joint injections have no role in treatment. High success rates have been reported for laparoscopic hernia repair in athletes. Kluin J, den Hoed PT, van Linschoten R, et al: Endoscopic evaluation and treatment of groin pain in the athlete. Am J Sports Med 2004;32:944-949. Genitsaris M, Goulimaris I, Sikas N: Laparoscopic repair of groin pain in athletes. Am J Sports Med 2004;32:1238-1242.
Question 786
High Yield
Figure 8 shows the radiograph of a 72-year-old man who has had severe pain in the left hip for the past 3 weeks. History reveals alcohol abuse. The next most appropriate step should consist of

Explanation
The radiograph reveals destruction of the femoral head with loss of the articular cartilage. These findings are consistent with an infected hip, and aspiration will confirm the diagnosis. Although the patient could have advanced osteonecrosis, typically the cartilage interval is maintained and such destruction is rarely associated with osteonecrosis.
Question 787
High Yield
Which of the following nerves is susceptible to entrapment near the calcaneal attachment site of the plantar fascia and can mimic or co-exist with plantar fasciitis?

Explanation
The first branch of the lateral plantar nerve is susceptible to entrapment beneath the deep fascia of the adductor hallucis muscle adjacent to the calcaneal attachment of the plantar fascia. This can be a cause of chronic heel pain. Additionally, the nerve is vulnerable to injury by a blind dissection in releasing the plantar fascia. The dorsal cutaneous branch of the superficial peroneal nerve supplies sensation to the dorsum of the foot. The medial calcaneal branch of the posterior tibial nerve lies in the subcutaneous tissues and innervates the skin of the heel. It is vulnerable to injury from skin incisions on the medial side of the heel. The lateral branch of the medial plantar nerve forms the second and third common digital nerves. Entrapment of the proper medial plantar nerve can occur at the master knot of Henry. This is well distal to the calcaneal attachment of the plantar fascia, and the pain usually radiates more distally in the arch, separate from heel pain. The communicating branch of the fourth common digital nerve crosses to the third common digital nerve. Therefore, the third common digital nerve receives supply from both the lateral and medial plantar nerves. This dual supply has been implicated in the increased incidence of digital neuroma of the third common digital nerve. Bordelon RL: Heel pain, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 837-857. Mann RA, Baxter DE: Diseases of the nerves, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 543-574.
Question 788
High Yield
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?

Explanation
A compression or burst injury occurs with vertical loading of the spine, such as from a blow to the vertex with the neck flexed (eg, spear tackling in football). This leads to vertebral end plate fractures before disk injury. At higher forces, the entire vertebra and disk may explode into the spinal canal. Analysis has shown this to be the major mechanism of cervical fracture, dislocation, and quadriplegia. With the normal head-up posture, the cervical spine has a gentle lordotic curve, and forces transmitted to the head are largely dissipated in the cervical muscles. When the neck is flexed, the cervical spine becomes straight, with the vertebral bodies lined up under one another. This allows for minimal dissipation of the impact forces to be absorbed by the neck muscles. Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532. Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Question 789
High Yield
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 790
High Yield
During primary total knee arthroplasty, what is the maximum distance the joint line can be raised or lowered before poor motion, joint instability, and increased chance of revision occur?

Explanation
Positioning of the femoral and tibial components is a common cause of early failure of total knee arthroplasty. Two modes of possible position are raising or lowering the joint line from its anatomic level. Raising or lowering the joint line beyond an established threshold can cause limited range of motion, poor patellar function, and possible instability. It has been determined that a threshold of approximately 8 mm provides consistently good results after knee arthroplasty.
Question 791
High Yield
Which of the following is associated with the use of bisphosphonates in the setting of metastatic breast cancer to the spine?
Explanation
The indications of bisphosphonate therapy in breast cancer patients range from the correction of hypercalcemia to the prevention of cancer treatment-induced bone loss. Bisphosphonates reduce metastatic bone pain in at least 50% of patients and can reduce the frequency of skeletal-related events by 30% to 40%. Osteonecrosis of the jaw could occur in up to 2.5% of breast cancer patients during long-term bisphosphonate therapy.
Question 792
High Yield
It is important to avoid which of the following exercises in the immediate postoperative period after humeral head replacement for an acute four-part fracture?

Explanation
It is critical to withhold active range of motion of the shoulder within the first 6 weeks after arthroplasty for acute fracture to prevent tuberosity avulsion. When radiographic and clinical findings show that the tuberosities are healed, active motion may be instituted, usually at 6 to 8 weeks. Immediate passive range-of-motion exercises, including external rotation with a stick, pendulum, and passive elevation, should begin within the limits of the repair on the day of surgery to prevent stiffness. Hartstock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humerus fractures. Orthop Clin North Am 1998;29:467-475.
Question 793
High Yield
A 19-year-old woman has had a painful prominence on the lateral border of her fifth metatarsal head since she was a young girl. Nonsurgical management, including the use of a wide toe box shoe, has failed to provide relief. Examination reveals a callus over the lateral prominence and on the plantar portion as well. A clinical photograph and a radiograph are shown in Figures 34a and 34b. Treatment should consist of
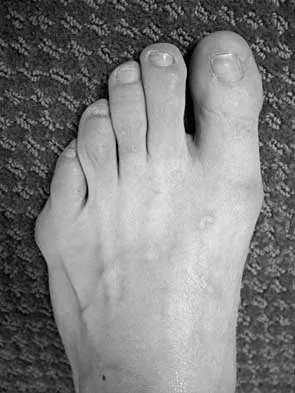

Explanation
The type of deformity described is a type 2 bunionette. There is often a congenital component to this deformity. The bowing of the fifth shaft differentiates a large intermetatarsal angle from a type 3 deformity. A distal chevron osteotomy corrects 1 degree in the intermetatarsal angle for every 1-mm shift. Because of limitations in the width of the fifth metatarsal neck, the allowable shift is generally 3 to 4 mm. This shift will not compensate for the large intermetatarsal angle. The floating osteotomy has a high rate of delayed union/nonunion and a low satisfaction rate. Metatarsal head excision has a high complication rate, including severe shortening, transfer metatarsalgia, stiffness, and pain. A more proximal procedure is necessary to correct the large intermetatarsal angle and the lateral bowing. The osteotomy of choice is a diaphyseal shaft osteotomy. Because this patient has a plantar callosity and a lateral callosity, the osteotomy is angled superiorly to elevate the fifth shaft with the shift, eliminating overload of the plantar metatarsal head and subsequent callus formation. Shereff MJ, Yang QM, Kummer FJ, Frey CC, Greenidge N: Vascular anatomy of the fifth metatarsal. Foot Ankle 1991;11:350-353. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 794
High Yield
A 55-year-old woman with a long history of low back and left lower extremity pain has failed to respond to exhaustive nonsurgical management. MRI scans show bulging and degeneration at L3-4 and L4-5 as well as a normal disk at L2-3 and L5-S1. She undergoes provocative lumbar diskography at L3-4, L4-5, and L5-S1. Post-diskography axial CT images of L3-4 and L4-5 are shown in Figures 6a and 6b, respectively. The injections at L3-4 and L4-5 produce no pain. The injection at L5-S1 produces 10/10 concordant back pain with radiation to the lower extremity. What is the most appropriate recommendation at this time?

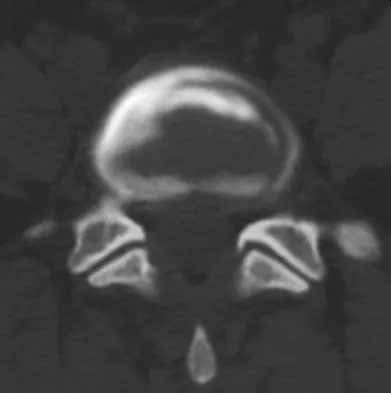
Explanation
The results of this patient's lumbar diskography are equivocal at best. The two disks most likely to be her pain generators, based on their MRI appearance, produced 10/10 pain, however it was nonconcordant and did not reproduce any of her typical left-sided radicular symptoms. The only disk that produced concordant back pain was the normal disk at the L5-S1 level and it reproduced radicular symptoms on the side opposite of her typical pain. Based on these findings, it would be difficult to select a level or levels to include in a lumbar fusion. As such, continued nonsurgical management is the safest treatment option at the current time. Brox and associates reported on a randomized clinical trial comparing lumbar fusion to cognitive intervention and exercise and found similar results in both groups, with significantly less risk in the latter. Brox JI, Sorensen R, Friis A, et al: Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913-1921.
Question 795
High Yield
What is the most common pediatric soft-tissue sarcoma?

Explanation
Soft-tissue sarcomas are the sixth most common cancer in children. Rhabdomyosarcoma is the most common type of pediatric soft-tissue sarcoma. Nearly 50% of rhabdomyosarcomas are diagnosed in children who are age 5 years or younger. Unfortunately, there has not been a significant increase in survival in children with metastatic rhabdomyosarcoma despite aggressive therapy including multiple-drug chemotherapy regimens.
Question 796
High Yield
A 68-year-old woman with metastatic breast carcinoma is seen in the emergency department. She appears lethargic, and she reports abdominal pain, nausea, and constipation. An EKG reveals a shortened QT interval. The only physical finding on examination is diffuse hyporeflexia. What is the most appropriate step in management?
Explanation
Intravenous fluid administration is the best first step to treat the hypercalcemia of malignancy. Many of these patients are dehydrated, and the increased serum calcium impairs the ability of the kidney to concentrate the urine. The decreased glomerular filtration rate secondary to the hypovolemia also leads to increased tubular resorption of calcium. The establishment of normovolemia will help promote increased urinary excretion of calcium. Lasix can also be used to help promote calciuria. Mithramycin is an antibiotic derived from Streptomyces plicatus. It is part of a group of drugs referred to as chromomycin antibiotics and is the only one of this group used clinically in the United States. It is rarely used in cancer chemotherapy because of its toxicity. A number of drug-related deaths have occurred from the use of mithramycin. Its use is now limited to the treatment of hypercalcemia associated with malignancy where it is used in lower dosage than that used for the treatment of tumors. Methotrexate has no role in the treatment of hypercalcemia of malignancy. While intravenous bisphosphonates are helpful in slowing progression of metastases and may help lower cerum calcium, they are not appropriate in the emergent treatment of hypercalcemia in the metastatic cancer patient.
Question 797
High Yield
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of

Explanation
The radiographs are classic for a Bennett's fracture, which involves a fracture of the palmar ulnar aspect of the proximal phalanx. This fracture fragment is still attached to the anterior oblique ligament. The deforming forces that cause subluxation of the base of the proximal phalanx include the pull of the abductor pollicis longus as well as the adductor pollicis. Adequate reduction can be achieved by closed reduction, percutaneous pin fixation, and casting. The fragment is too small for secure internal fixation. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Question 798
High Yield
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
With soft-tissue loss, local or free flap coverage may be necessary to treat exposed tendon and bone. However, a vacuum-assisted closure device is a good temporizing dressing. It prevents external contamination, reduces edema around the wound, increases oxygen tension in the wound, and promotes the formation of granulation tissue. The use of this negative pressure device has been described in both acute traumatic and in chronic wound scenarios. If sufficient granulation tissue forms, closure may be by split graft, avoiding a more complex coverage procedure. Immediate skin grafting over the exposed anterior tibial tendon and tibia would have a low likelihood of success. Dressing changes with sulfasalazine may be beneficial in a burn wound to assist with removal of skin slough; however, in a granulating wound, the material may be toxic to early epithelialization. Xenograft is a foreign body and should not be applied to an acute contaminated open wound. Historically, a cross-leg flap was a treatment alternative for lower extremity soft-tissue loss; however, its current applications are extremely limited. Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Question 799
High Yield
A 70-year-old woman has a preoperative anterior interscalene block prior to undergoing a total shoulder arthroplasty. After seating her in the beach chair position, she becomes acutely hypotensive. What is the most likely cause for the hypotension?
Explanation
The beach chair position may cause sudden hypotension and bradycardia as a result of the Bezold-Jarisch reflex. This reflex occurs when venous pooling and increased sympathetic tone induce a low-volume, hypercontractile ventricle, resulting in activation of the parasympathetic nervous system and sympathetic withdrawal. The reported incidence of this phenomenon associated with the sitting position is between 13% to 24%. Left untreated, the result may be cardiac arrest. Pneumothorax or central nervous system toxicity after interscalene block is rare and has an incidence of less than 0.2%. Laryngeal nerve block associated with interscalene nerve block can occur but usually results in hoarseness secondary to ipsilateral vocal cord palsy. Long T, Wass C, Burkle C: Perioperative interscalene blockade: An overview of its history and current clinical use. J Clin Anesthesia 2002;14:546-556.
Question 800
High Yield
Figure 6a shows the radiograph of a 50-year-old man who sustained an anterior dislocation of the shoulder. He undergoes closed reduction, and the postreduction radiograph is shown in Figure 6b. Management should now consist of
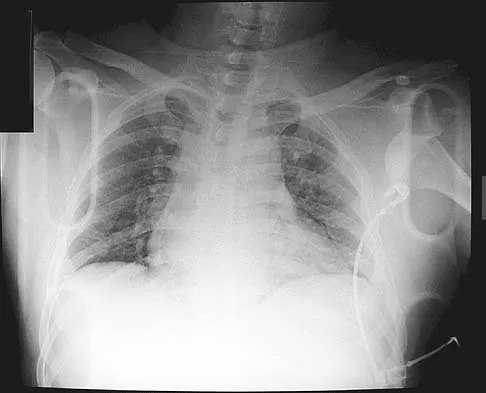

Explanation
Displaced greater tuberosity fractures often will block abduction and/or external rotation by impinging on the underside of the acromion or posterior glenoid. The indications for open reduction and internal fixation are 1 cm of displacement or 45 degrees of rotation of the tuberosity fracture. Surgical treatment has recently been recommended for 0.5 cm of tuberosity displacement. Neer CS II: Displaced proximal humeral fractures: II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 1970;52:1090-1103.
