HY 2026
00:00
Start Quiz
Question 601
High Yield
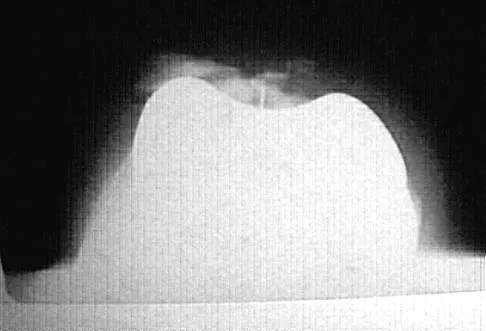
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of

Explanation
A semiconstrained prosthesis can provide excellent results in carefully selected patients. Because the radiographs show extensive joint destruction with loss of the capitellum and trochlea, a capitellocondylar total elbow (unconstrained) prosthesis is contraindicated. Elbow fusion is poorly accepted, and the radiographs show too much articular destruction for a radial head excision, synovectomy, or interposition arthroplasty to be effective. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 602
High Yield
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Explanation
The elbow usually is stable after reduction in most elbow dislocations. Ross and associates reported that supervised motion begun immediately after reduction was effective in uncomplicated dislocations. The elbow will become stiff if immobilization is applied for an extended period of time. Immediate open treatment is not indicated for a simple elbow dislocation. Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
Question 603
High Yield
A 77-year-old man with diabetes mellitus has had a nonhealing Wagner grade I ulcer under the medial sesamoid for the past 3 months. He smokes tobacco regularly. He has undergone several debridements and total contact casting. Examination reveals no palpable pulses. He has no erythema or purulence, and he is afebrile. Radiographs reveal no abnormalities. What is the best initial diagnostic test to help determine why the ulcer has failed to heal?
Explanation
The best initial test for this patient is to assess the vascular supply to the foot. An elderly smoker with diabetes mellitus has a high risk of peripheral vascular disease. Decreased weight bearing has not been successful. Although a bone scan might be helpful, it would take secondary consideration to the patient's vascular supply, especially in the absence of any acute infection. Monofilament testing would help diagnosis neuropathy, which is a root cause behind the ulcer forming, but does not prevent it from healing. The Thompson's test is used to diagnosis an Achilles tendon rupture.
Question 604
High Yield
Which of the following properties primarily provides the excellent corrosion resistance of metallic alloys such as stainless steel and cobalt-chromium-molybdenum?
Explanation
All of the metals and metallic alloys used in orthopaedic surgery obtain their corrosion resistance from an adherent oxide layer. For stainless steel and cobalt alloy, the addition of chromium as an alloying element ensures the formation of a chromium oxide passive layer that forms on the surface and separates the bulk material from the corrosive body environment. Titanium alloy achieves the same result without chromium by forming an adherent passive layer of titanium oxide. Although these layers can indeed be hard, hardness does not in and of itself provide corrosion resistance. Adding nickel to both metallic alloys adds to strength but does not influence corrosion resistance appreciably. Galvanic potential can influence corrosion but does so by differences in potential between two contacting materials; for example, stainless steel and cobalt alloy have substantially different potentials, and if they were in contact within an aqueous environment, corrosion would commence with the stainless steel becoming the sacrificial anode. Metallic carbides are important in strengthening the alloys but have no role in providing corrosion resistance. Williams DF, Williams RL: Degradative effects of the biological environment on metal and ceramics, in Ratner BD, Hoffman AS, Shoen FJ, et al (eds): Biomaterials Science. San Diego, CA, Academic Press, 1996, pp 260-265. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 190-193.
Question 605
High Yield
A 58-year-old man has anterior knee pain after undergoing total knee arthroplasty for osteoarthritis 2 years ago. He denies any history of trauma. A Merchant view is shown in Figure 20. What is the most likely cause of his pain?
Explanation
The patient has a patellar stress fracture after resurfacing in a total knee arthroplasty. Several studies have shown that over-resection of the patella to less than 12 to 15 mm increases anterior patellar surface strains to a point where the risk of fracture is increased. Increasing the patellar thickness, positioning of the femoral component, lateral releases, and component types have not been clearly associated with increased fracture risk. Reuben JD, McDonald CL, Woodard PL, Hennington LJ: Effect of patella thickness on patella strain following total knee arthroplasty. J Arthroplasty 1991;6:251-258. Hsu HC, Luo ZP, Rand JA, An KN: Influence of patellar thickness on patellar tracking and patellofemoral contact characteristics after total knee arthroplasty. J Arthroplasty 1996;11:69-80.
Question 606
High Yield
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?

Explanation
Persistent pain following an ankle sprain can present a diagnostic dilemma. All of the injuries listed should be considered in the differential diagnosis. The superficial peroneal nerve courses in the lateral compartment and exits the crural fascia 12 to 15 cm above the level of the ankle. Muscle herniation through the fascial defect has been reported to be associated with entrapment of this nerve. The fascial hiatus also may serve as a potential tether in cases of inversion injuries causing injury to the superficial peroneal nerve. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Question 607
High Yield
Nutritional rickets is associated with which of the following changes in chemical blood level?
Explanation
Nutritional rickets is associated with decreased dietary intake of Vitamin D, resulting in low levels of Vitamin D that result in decreased intestinal absorption of calcium and low to normal serologic levels of calcium. To boost serum calcium levels, there is a compensatory increase in PTH and bone resorption, leading to increased alkaline phosphatase levels. Brinker MR: Cellular and molecular biology, immunology, and genetics in orthopaedics, in Miller MD (ed): Review of Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 81-94. Pettifor J: Nutritional and drug-induced rickets and osteomalacia, in Farrus MJ (ed): Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 399-466.
Question 608
High Yield
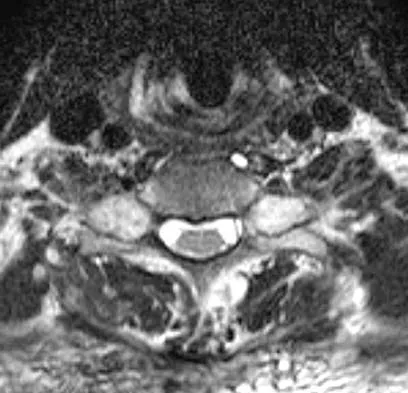
Subluxation caused by rheumatoid arthritis is most commonly seen at what level of the cervical spine?

Explanation
Approximately 65% of cervical subluxations occur at C1-C2. Of these, 50% are anterior, with the remainder being lateral and posterior. The second most common type is basilar invagination, occurring in 40% of patients. The third most common type is subaxial, occurring in 20% of patients with rheumatoid arthritis. Subluxation at more than one level is common. Boden S, Clark CR: Rheumatoid arthritis of the cervical spine, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 693. Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 609
High Yield
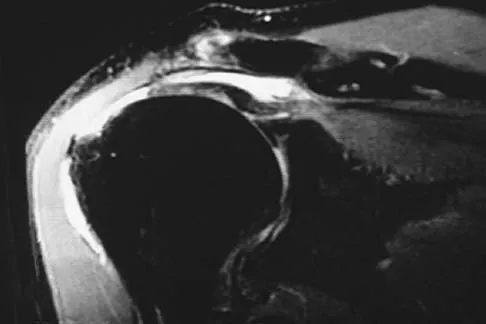
A 40-year-old woman who is an avid tennis player reports the insidious onset of progressive left shoulder pain for the past 2 months. Examination reveals full range of motion with a positive impingement sign. Strength in the supraspinatus and infraspinatus muscles is normal, although stress testing is painful. An earlier subacromial cortisone injection provided good, but only temporary relief. An AP radiograph of the left shoulder is shown in Figure 10. Management should now consist of

Explanation
The radiograph shows calcific deposits within the substance of the supraspinatus tendon. Patients with this condition are prone to recurrent bouts of acute inflammation in the shoulder. While the response to cortisone injection is often dramatic, repeated injections are not recommended because of injury to the collagen fibers. Good results have been obtained with arthroscopic evacuation of the calcium deposits. In one study, the addition of a subacromial decompression did not improve the results. Jerosch J, Strauss JM, Schmiel S: Arthroscopic treatment of calcific tendinitis of the shoulder. J Shoulder Elbow Surg 1998;7:30-37.
Question 610
High Yield
Which of the following factors can contribute to patellar subluxation following routine total knee arthroplasty?

Explanation
Excessive resection of the lateral facet of the patella can lead to subluxation. Rotational alignment of the components can have a significant impact on patellar tracking. Internal rotation of the femoral component leads to more lateral alignment of the patella within the trochlear groove. Internal rotation and medial placement of the tibial component results in lateralization of the tibial tubercle with an increase in the Q angle. Excessive valgus alignment of the mechanical axis, or insufficient correction of preoperative valgus, has a similar effect on the Q angle, and both can result in a higher rate of tracking problems.
Question 611
High Yield
Which of the following diagnostic studies best distinguishes Ewing's sarcoma from small cell osteosarcoma?

Explanation
Cytogenetics best demonstrates the 11;22 translocation characteristic of Ewing's sarcoma. The translocation also can be detected with polymerase chain reaction and fluorescent in situ hybridization. The Ewing antibody is used for immunostaining to check for cell membrane (surface) staining of a marker unrelated to the translocation; this could also help distinguish Ewing's sarcoma from small cell osteosarcoma. A bone scan will show increased uptake with both types of tumors. Although most Ewing's sarcoma tumors are diploid, some are polyploid as are most osteosarcomas. Flow cytometry is used to sort cells, sometimes based on antibody binding. LDH can be elevated in both Ewing's sarcoma and osteosarcoma and is a poor prognostic indicator when elevated. Lymph node metastases are uncommon in both of these tumors. Perotti D, Corletto V, Giardini R, Parafioriti A, Fossati-Bellani F, Luksch R: Retrospective analysis of ploidy in primary osseous and extraosseous Ewing family tumors in children. Tumori 1998;84:493-498. Riley RD, Burchill SA, Abrams KR, Heney D, Sutton AJ, Jones DR, et al: A systematic review of molecular and biological markers in tumours of the Ewing's sarcoma family. Eur J Cancer 2003;39:19-30.
Question 612
High Yield
What is the most common cause of the new onset of amenorrhea in a female endurance athlete who is not sexually active?
Explanation
Insufficient caloric intake caused by either a poor diet or an eating disorder is the most common cause for the loss of menses in a female athlete. In the face of adequate caloric intake, stress is unlikely to cause amenorrhea. Oral contraceptives control menses but do not eliminate it. Diabetes mellitus does not cause the new onset of amenorrhea. Pregnancy can be a cause in a sexually active athlete. Chromosomal abnormalities can result in delayed or absent menarche but not the onset of amenorrhea in a postmenarchal female. Constantini NW: Clinical consequences of amenorrhea. Sports Med 1994;17:213-223.
Question 613
High Yield
A 46-year-old man sustains a calcaneal fracture in a fall off a scaffold. During surgical reconstruction using an extended lateral incision, the fracture is reduced and fixed with a plate and screws. One of the posterior facet screws is found to be 5 mm out of the bone on the Harris view. What structure is most likely at risk because of this finding?
Explanation
The abductor hallucis muscle is the most medial structure. The posterior tibial tendon and the flexor digitorum longus tendon lie more cephalad to the sustentaculum tali. There is a groove under the sustentaculum for the flexor hallucis longus tendon. Subchondral lag screws placed across the posterior facet exit the medial side of the calcaneus in this groove. Just medial to the flexor hallucis longus tendon is the neurovascular bundle. A screw that is out of the bone a short distance can cause triggering of the flexor hallucis longus tendon. Patients will report loss of great toe excursion in the early postoperative period. Accurate measurement of subchondral lag screw length avoids this complication. Hollinshead WH: Anatomy for Surgeons, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 802-852. Rosenberg AS, Cheung Y: Diagnostic imaging of the ankle and foot, in Jahss MH (ed): Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991, pp 109-154.
Question 614
High Yield
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?

Explanation
The patient's symptoms are typical for gouty arthropathy, and the diagnosis can only be confirmed with aspiration and visualization of the crystals. A concomitant infection also must be ruled out; therefore, it is important to obtain a cell count and culture. Colchicine may have a role in gouty management, but the diagnosis must be confirmed. Allopurinol is not effective in acute gouty arthropathy. Measurement of serum uric acid levels is often not helpful in making a definitive diagnosis. Steroid injections should be deferred until cell count and culture results indicate no accompanying infection. Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Question 615
High Yield
Figures 5a and 5b show the radiographs of an 11-year-old boy who felt a pop and immediate pain in his right knee as he was driving off his right leg to jam a basketball. Examination reveals that the knee is flexed, and the patient is unable to actively extend it or bear weight on that side. There is also a large effusion. Management should include


Explanation
Fractures through the cartilage on the inferior pole of the patella, the so-called sleeve fracture, are often difficult to diagnose because of the paucity of ossified bone visible on the radiographs. If the fracture is missed and the fragments are widely displaced, the patella may heal in an elongated configuration that may result in compromise of the extensor mechanism function. The treatment of choice is open reduction and internal fixation using a tension band wire technique to achieve close approximation of the fragments and restore full active knee extension. Heckman JD, Alkire CC: Distal patellar pole fractures: A proposed common mechanism of injury. Am J Sports Med 1984;12:424-428.
Question 616
High Yield
A 73-year-old man reports increasing back and lower extremity pain. A bone scan is shown in Figure 31. What is the most likely diagnosis?

Explanation
The bone scan reveals lesions throughout the skeleton. The patient's age, gender, and pain pattern are consistent with metastatic prostate cancer. Multiple myeloma typically does not have enough osteoblastic activity to produce this bone scan. The patient's age is not consistent with metastatic neuroblastoma (a pediatric disease). Polyostotic fibrous dysplasia may involve multiple active lesions in younger patients but does not have such a widespread distribution of lesions. Hodgkin's lymphoma can involve bone, but the widespread discrete appearance on this bone scan is most consistent with metastatic prostate cancer. In a patient with widespread bone metastases from prostate cancer, bisphosphonates may play a critical role in treatment by decreasing pain and the number of fractures. Roudier MP, Vesselle H, True LD, Higano CS, Ott SM, King SH, Vessella RL: Bone histology at autopsy and matched bone scintigraphy findings in patients with hormone refractory prostate cancer: The effect of bisphosphonate therapy on bone scintigraphy results. Clin Exp Metastasis 2003;20:171-180.
Question 617
High Yield
In an acute closed boutonniere injury, what is the most appropriate splinting technique for the proximal interphalangeal joint?

Explanation
Rupture of the central slip of the extensor mechanism and a varying degree of lateral band volar migration are the pathologic entities in an acute boutonniere injury. Splinting the proximal interphalangeal joint in full extension allows reapproximation of the central slip to the base of the middle phalanx. Distal interphalangeal joint flexion is permitted to allow movement of the lateral bands distally and dorsally, preventing contracture. Newport ML: Extensor tendon injuries in the hand. J Am Acad Orthop Surg 1997;5:59-66.
Question 618
High Yield
The medial collateral ligament complex of the elbow originates on what portion of the medial epicondyle?
Explanation
The medial collateral ligament complex of the elbow consists of three portions: the anterior bundle, the posterior bundle, and a transverse component that has little biomechanic significance. The origin of the ligament is from the central two thirds of the anteroinferior undersurface of the medial epicondyle.
Question 619
High Yield
A 30-year-old woman injured her ankle playing soccer 3 months ago. She now reports popping and pain over the lateral side of her ankle. An MRI scan is shown in Figure 33. What structure needs to be repaired to alleviate the popping?

Explanation
The symptoms and MRI scan indicate dislocated peroneal tendons. In this patient, the structure that needs to be repaired is the superior peroneal retinaculum. If the popping was coming from a torn peroneal tendon, repair would involve the peroneal longus or brevis tendon, but this is not shown in the MRI scan. The anterior talofibular ligament or the calcaneofibular ligament would need to be repaired if the patient had ankle instability due to an ankle sprain. Jones DC: Tendon disorders of the foot and ankle. J Am Acad Orthop Surg 1993;1:87-94.
Question 620
High Yield
The arrow in Figure 39 is pointing to which of the following ligaments?

Explanation
The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The scapholunate interosseous ligament stabilizes the scapholunate joint. The ulnolunate ligament originates from the base of the ulnar styloid and inserts in the lunate. The ulnotriquetral ligament originates from the base of the ulnar styloid and inserts on the triquetrum. The ulnolunate and the ulnotriquetral ligaments are important stabilizers to the ulnar side of the wrist. The short radiolunate ligament originates on the volar ulnar margin of the distal radius and inserts in the ulnar margin of the lunate. Berger RA: Ligament anatomy, in Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist, Diagnosis and Operative Management. St Louis, MO, Mosby, 1998, pp 73-105.
Question 621
High Yield
A 2-year-old girl was born with the toe deformity shown in Figure 2. She has difficulty wearing shoes despite having adequate room in the toe box. Management at this time should consist of

Explanation
The patient has a congenital curly toe deformity of the third toe, and tenotomy of the toe flexors is highly effective for this problem. Stretching and taping are ineffective for this deformity. The position of the second toe is secondary; therefore, procedures on that toe are unnecessary and ineffective. The flexor to extensor transfer is a more complicated procedure that produces negligible results, or may even worsen the deformity. Resection arthroplasty is contraindicated because it causes abnormal growth of the toes. Hamer AJ, Stanley D, Smith TW: Surgery for curly toe deformity: A double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663. Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood. J Bone Joint Surg Br 1984;66:770-771.
Question 622
High Yield
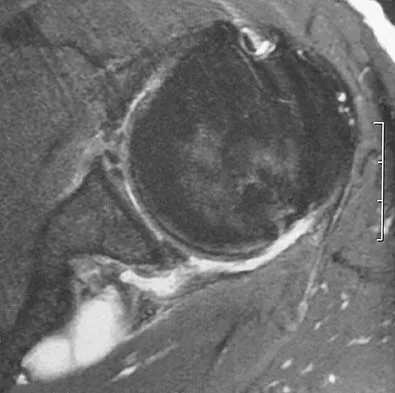
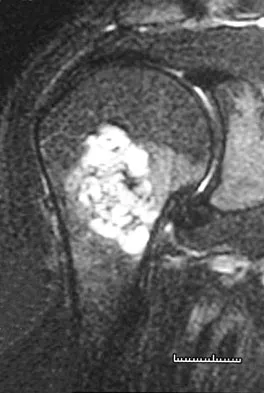
A 44-year-old recreational weight lifter reports chronic deep pain in his left shoulder that is aggravated by any pressing exercises. He also notes a painful catch in the shoulder occurring with rotational movements. Physical therapy and nonsteroidal anti-inflammatory drugs for 3 months have failed to provide relief. Examination reveals pain with O'Brien's test but no signs of instability. MRI scans are shown in Figures 4a and 4b. Treatment should now consist of
Explanation
The MRI scans show a large paralabral ganglion cyst in the spinoglenoid notch that communicates with an extensive tear of the glenoid labrum. Snyder and associates have classified superior labral tears into several subtypes that reflect the location and extent of the injury. Arthroscopic repair of the labral tear and aspiration of the ganglion cyst is the treatment of choice. Open excision of the cyst does not address the underlying problem of the labral tear. Snyder SJ, Karzel RP, Delpizzo W: SLAP lesions of the shoulder. Arthroscopy 1990;6:274-279. Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch cysts. J Shoulder Elbow Surg 2002;11:600-604. McFarland EG, Kim TK, Savino RM: Clinical assessment of three common tests for superior labral anterior-posterior lesions. Am J Sports Med 2002;30:810-815.
Question 623
High Yield
Figures 9a and 9b show the radiographs of a 4-year-old child who sustained an elbow injury. What is the most likely complication resulting from this fracture if treated in a cast?


Explanation
The radiographs show a lateral condyle fracture with 2 mm of displacement. As opposed to other pediatric elbow fractures, lateral condyle fractures have a higher incidence of nonunion. This may be due to minimal metaphyseal bone on the distal fragment, the intra-articular nature of the fracture, or from further displacement when treated nonsurgically. These fractures with 2 mm and greater of displacement should be treated with reduction and stabilization. Osteonecrosis and fishtail deformity may be seen in very rare cases of lateral condyle fractures. The incidence is certainly less than the rates of nonunion seen in nonsurgically treated fractures with 2 mm and greater of displacement. Varus malunion from overgrowth and elbow stiffness are more likely seen in fractures treated surgically. Pirker ME, Weinberg AM, Hollwarth ME, et al: Subsequent displacement of initially nondisplaced and minimally displaced fractures of the lateral humeral condyle in children. J Trauma 2005;58:1202-1207. Finnbogason T, Karlsson G, Lindberg L, et al: Nondisplaced and minimally displaced fractures of the lateral humeral condyle in children: A prospective radiographic investigation of fracture stability. J Pediatr Orthop 1995;15:422-425.
Question 624
High Yield
A 19-year-old woman reports lower back pain following a motor vehicle accident. Radiographs obtained immediately after the accident and a bone scan obtained 4 weeks later are shown in Figures 25a through 25c. The patient asks questions regarding the cause, genetics, and natural history of her condition. She should be informed that the condition was



Explanation
The radiographs show L5 spondylolysis without spondylolisthesis (slip). The bone scan is normal, indicating that the pars interarticularis fractures are not acute. The incidence of spondylolysis is approximately 5% in the general population. The lesion generally develops in children age 5 to 6 years, and there is a second peak in the adolescent population. There is a familial predisposition, with reported rates of 27% to 69% in close relatives. A recent long-term follow-up study found that 90% of the spondylolisthesis had occurred before the patient's first visit to the physician. Spondylolisthesis tends to progress during the initial growth spurt and is similar in some respects to idiopathic scoliosis. Progression of a lytic spondylolysis to spondylolisthesis in adulthood has been reported; however, this is exceedingly rare. Lauerman WC, Cain JE: Isthmic spondylolisthesis in the adult. J Am Acad Orthop Surg 1996;4:201-208. Hensinger RN: Spondylolysis and spondylolisthesis in children and adolescents. J Bone Joint Surg Am 1989;71:1098-1107. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Question 625
High Yield
What are the four most common soft-tissue sarcomas to spread via the lymph node system?

Explanation
Soft-tissue sarcomas most frequently metastasize to the lung, but certain histologic types have a predilection for the lymph node system as well. Rhabdomyosarcoma, clear cell sarcoma, epithelioid sarcoma, and synovial sarcoma are four of the most common types to spread in this fashion. Careful evaluation and/or sentinel lymph node biopsy plays a role in disease staging and prognosis. Riad S, Griffin AM, Liberman B, et al: Lymph node metastasis in soft-tissue sarcoma in an extremity. Clin Orthop Relat Res 2004;426:129-134.
Question 626
High Yield
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?

Explanation
Dense pods of ingrowth into the porous coating of cementless ingrowth sockets are seen. Channels through the non-ingrown portion allow access to the trabecular bone of the ilium. Polyethylene wear debris can enter these areas through screw holes. Expansile, lytic lesions can result, which can become large without compromising implant fixation. Loosening is late and results from catastrophic loss of bone. A well-fixed acetabular component with a modular design, a well-designed locking mechanism, and a good survivorship history is a candidate for exchange of the liner and grafting of the osteolytic lesion. Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265. Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
Question 627
High Yield
A 40-year-old woman reports the atraumatic onset of severe knee pain and swelling after undergoing an uncomplicated elective cholecystectomy 1 week ago. She denies any history of diabetes mellitus or HIV but has had occasional episodes of mild knee pain and swelling that have always responded to nonsteroidal anti-inflammatory drugs. Radiographs are shown in Figures 5a and 5b. A knee aspiration yields a WBC count of 35,000/mm3. The aspirate should also yield which of the following findings?


Explanation
The radiographs reveal chondrocalcinosis of the menisci. This is caused by calcium pyrophosphate crystals, which are weakly positive birefringent rhomboid-shaped crystals. Frequently, this condition is asymptomatic; however, routine abdominal surgery may cause precipitation of these crystals and pain. Gout, which is caused by strongly negative birefringent needle-shaped sodium urate crystals, is not associated with chondrocalcinosis and is rare in younger women. Gross blood is uncommon without trauma. Infection is not likely in a healthy patient who underwent uncomplicated surgery. Fisseler-Eckhoff A, Muller KM: Arthroscopy and chondrocalcinosis. Arthroscopy 1992;8:98-104.
Question 628
High Yield
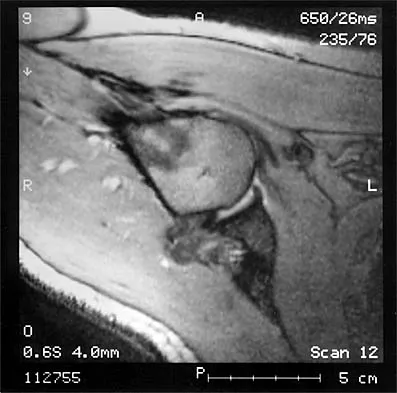
Figures 10a through 10c show the plain radiograph and MRI scans of a 41-year-old man who has right hip pain. What is the most likely diagnosis?


Explanation
Transient osteoporosis is a self-limited painful but reversible disorder. Although first described in pregnant women, it is more common in young to middle-aged men. The radiograph shows loss of mineralization in the right hip relative to the left side. There is no osseous destruction or cortical expansion typical of metastasis or giant cell tumor. The process is confined to the femoral side of the joint unlike rheumatoid arthritis, which would be centered in the joint. Osteonecrosis is better defined with sharp but irregularly shaped margins, and there is no double-line sign. The MRI scans reveal diffuse edema in the femoral head and neck that is atypical for osteonecrosis. Transient osteoporosis may recur in the same or opposite hip.
Question 629
High Yield
Figure 6 shows the radiograph of a 14-year-old baseball player who felt a pop and had an immediate onset of pain in his elbow after a hard throw from the outfield. The best course of action should be to

Explanation
The valgus stress at the elbow caused by throwing strains the medial collateral ligament. The medial epicondyle, on which the ligament inserts, is the last ossification center to fuse to the distal humerus, and acute avulsion of the medial epicondyle can occur in adolescents. If the elbow is allowed to heal in a displaced position, valgus instability and loss of elbow extension may result. Valgus instability is especially problematic for the throwing athlete. Surgical treatment with rigid internal fixation is the treatment of choice for displaced medial epicondyle avulsion fractures. Valgus instability is prevented, and the rigid fixation allows for early range of motion. Case SL, Hennrikus WL: Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med 1997;25:682-686.
Question 630
High Yield
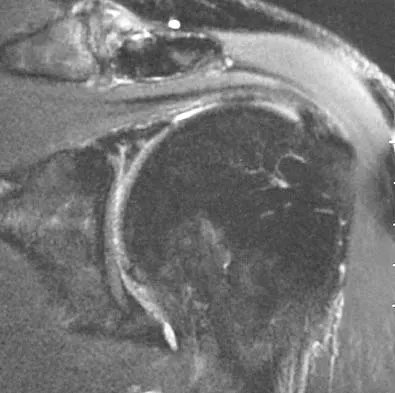
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?
Explanation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity. Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower's shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49. Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 631
High Yield
Figures 9a and 9b show the radiographs of a 28-year-old woman who sustained a head injury and a closed injury, without soft-tissue compromise, to her right lower extremity in a motor vehicle accident. Appropriate management of the foot injury should include


Explanation
The displaced talar neck fracture should be treated with open reduction and internal fixation using screws. Closed reduction and casting will not maintain position, and percutaneous pinning is not able to maintain reduction to allow union. External fixation and amputation are not necessary for this injury unless there is severe soft-tissue loss.
Question 632
High Yield
Examination of a 4-year old child with obstetrical palsy reveals weak deltoids, pectoralis major strength of 4-5, and normal hand function. External rotation of the shoulder is limited. What is the most appropriate surgical procedure to restore external rotation?
Explanation
Transfer of the latissimus dorsi and teres major to the posterior rotator cuff will restore external rotation and some abduction. The procedure should be performed in children who are approximately age 4 years, following spontaneous recovery and prior to significant stiffness. External rotation osteotomy is more appropriate for an older child. Fusion should not be performed until skeletal maturity. Distal biceps rerouting restores pronation for a supination deformity. Latissimus dorsi and teres major transfer to the subscapularis would accentuate the internal rotation. In younger patients without significant bony deformity, a subscapularis slide or lengthening can restore external rotation. Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L'Episcopo transfers in obstetrical palsy: A retrospective review of twenty cases. J Pediatr Orthop 1990;10:442-444.
Question 633
High Yield
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show


Explanation
The patient has a slipped capital femoral epiphysis (SCFE) at a younger than average age (average age 13.5 years for boys and 12.0 years for girls); therefore, an etiology that is not idiopathic must be considered. Hypothyroidism can result in a SCFE, but these children typically fall into the category of less than the 10th percentile for height. SCFE may develop in children with a growth hormone deficiency who have undergone hormonal replacement. Osteodystrophy caused by chronic renal failure may result in a SCFE, but the bone quality is markedly osteopenic on radiographs and the children are chronically ill with both low height and weight percentiles. An elevated estrogen level results in physeal closure and is protective to physeal slippage. Therefore, this child will most likely have normal laboratory values. Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Question 634
High Yield
A 35-year-old male laborer with isolated posttraumatic degenerative arthritis of the right hip undergoes the procedure shown in Figure 8. What is the most appropriate position of the right lower extremity?

Explanation
The primary indication for hip arthrodesis is isolated unilateral hip disease in a young, active patient. Avoiding abductor damage and preserving proximal femoral anatomy are imperative to allow conversion to a future total hip arthroplasty. Optimal positioning is 30 degrees of flexion to allow swing-through. Neutral abduction and adduction and slight external rotation allow the most efficient gait while allowing sufficient support in stance. A small degree of adduction is acceptable for a successful hip arthrodesis. Callaghan JJ, Brand RA, Pedersen DR: Hip arthrodesis: A long term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Question 635
High Yield
Figure 26 shows the MRI scan of a 60-year-old man who has had groin pain for the past 2 months. The patient reports pain with ambulation, and examination reveals an antalgic gait. He denies any history of steroid or alcohol abuse. Plain radiographs are normal. Management should include
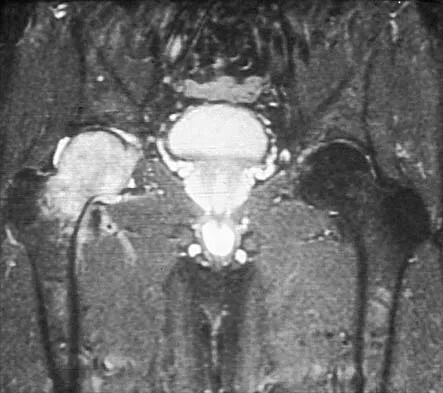
Explanation
The patient has transient osteoporosis of the hip. Transient osteoporosis is usually a self-limited condition that is most frequently seen in women in the third trimester of pregnancy and in men in the sixth decade of life. Transient osteoporosis is best treated with protected weight bearing.
Question 636
High Yield
A 9-year-old boy has a painless enlarged mass on the dorsum of his hand. Figures 14a through 14d show the clinical photograph, radiographs, and biopsy specimen. What is the most likely diagnosis?



Explanation
Multiple hereditary exostosis and enchondroma commonly present as multiple lesions in the hand. Multiple hereditary exostosis consists of cartilage capped bony exostoses arising from the metaphyseal end of rapidly growing bones. Osteosarcoma and chondrosarcoma rarely appear as multiple lesions. Fracture callus can exhibit enchondral ossification that is usually circumferential, but the radiographic findings are not consistent with fracture. Porter DE, Emerton ME, Villanueva-Lopez F, Simpson AH: Clinical and radiographic analysis of osteochondromas and growth disturbance in hereditary multiple exostoses. J Pediatr Orthop 2000;20:246-250.
Question 637
High Yield
A patient who underwent a high tibial osteotomy (HTO) is now scheduled to undergo total knee arthroplasty (TKA). When compared with a patient undergoing primary TKA without a prior HTO, the patient should be advised to expect a higher incidence of
Explanation
Conversion TKA following a previous HTO can be successful; however, it is associated with poorer clinical results when compared with other primary TKAs. There is an increased likelihood of poor range of motion that is partially affected by patella infera created from the osteotomy. Patella infera also results in difficulty with surgical exposure. There has been no reported increase in the rate of infection, fracture, or loosening.
Question 638
High Yield
What is the most common clinically significant preventable complication secondary to the treatment of a displaced talar neck fracture?
Explanation
The most important consequence of a displaced talar neck fracture after closed or open treatment is malunion. Because displacement of the talar neck is associated with displacement of the subtalar joint, any malunion leads to intra-articular incongruity or malalignment of the subtalar joint. Varus malunion is common when there is comminution of the medial talar neck. This results in pain, osteoarthritis, and hindfoot deformity that requires further treatment. Because of these complications, it is imperative that all displaced talar neck fractures are reduced anatomically; fragmented fractures may require bone grafting to maintain the length and rotation of the neck. Tile M: Fractures of the talus, in Schatzker J, Tile M (eds): Rationale of Operative Fracture Care, ed 2. Berlin, Springer-Verlag, 1996, pp 563-588. Daniels TR, Smith JW, Ross TI: Varus malalignment of the talar neck: Its effect on the position of the foot and on subtalar motion. J Bone Joint Surg Am 1996;78:1559-1567.
Question 639
High Yield
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most influenced by

Explanation
While many factors play a role in the outcome of osteochondritis dissecans, ample evidence has shown that the prognosis is most influenced by the growth status of the plates. If the growth plates are open, the chance of a successful outcome is significantly greater than if they are closed. Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Question 640
High Yield
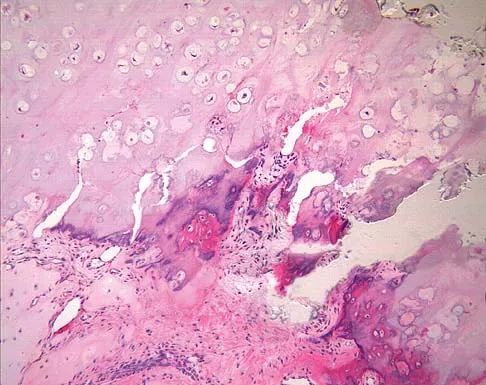
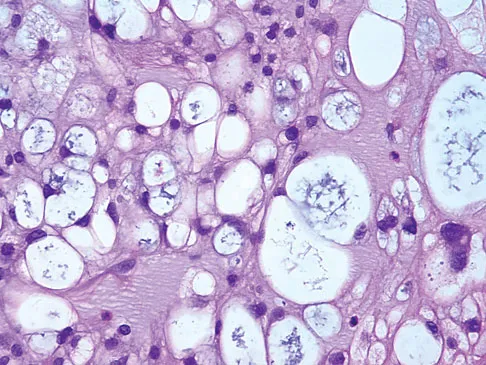
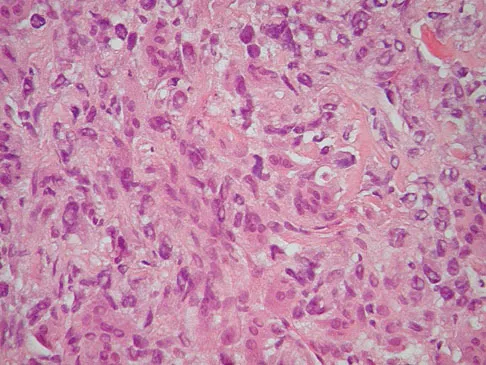
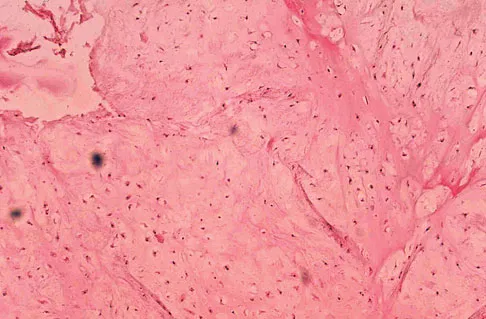
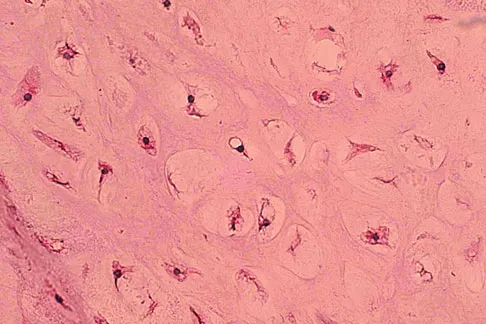
The biopsy specimens seen in Figures 55a and 55b are from a lytic lesion in the sacrum of a 58-year-old man. What is the most likely diagnosis?
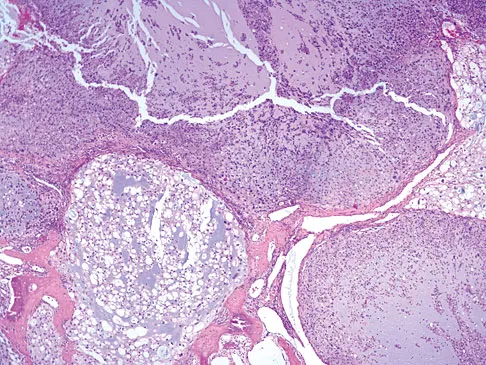
Explanation
The lesion is a chordoma and the other listed choices can be eliminated based on the histology. Many tumors can occur in the sacrum including chordoma, multiple myeloma, giant cell tumor, aneurysmal bone cyst, and metastatic disease. The histology in this patient shows a lobulated lesion on low power with fibrous septae separating the lobules. At higher magnification, the cells have eosinophilic vacuolated cytoplasm and are called physaliferous cells. Chordoma is a low-grade neoplasm that most commonly occurs in the sacrum and rarely in the base of the skull. The diagnosis is often delayed. Chordoma is thought to originate from notochordal remnants. Chordoma typically occurs in the midline and has an associated soft-tissue mass. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 372. Fuchs B, Dickey ID, Yaszemski MJ, et al: Operative management of sacral chordoma. J Bone Joint Surg Am 2005;87:2211-2216.
Question 641
High Yield
Which of the following describes the correct proximal to distal progression of the annular and cruciform pulleys of the digits?
Explanation
The correct progression of the annular and cruciform pulley in the digits is A1, A2, C1, A3, C2, A4, C3. The two cruciform pulleys are collapsible elements adjacent to the more rigid annular pulleys of the flexor tendon sheath. This arrangement enables unrestricted flexion of the proximal interphalangeal joint. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 176-186.
Question 642
High Yield
A 21-year-old woman who was wearing a seat belt sustained an injury of the thoracolumbar junction in a motor vehicle accident. The AP radiograph shows widening between the L1 and L2 spinous processes, and the CT scan shows the empty facet sign at this level. The initial evaluation should include

Explanation
The patient has a flexion-distraction injury of the thoracolumbar spine that is often associated with wearing a seat belt. The fracture has a high risk of associated intra-abdominal injury; therefore, the initial evaluation should include a CT of the abdomen. The most common visceral injury is to the bowel. Smith WS, Kaufer H: Patterns and mechanisms of lumbar injuries associated with lap seat belts. J Bone Joint Surg Am 1969;51:239-254.
Question 643
High Yield
Degenerative spondylolisthesis of the cervical spine is most commonly seen at which of the following levels?
Explanation
Degenerative spondylolisthesis of the cervical spine is seen almost exclusively at C3-4 and C4-5; this is in contrast to degenerative changes, which are most commonly seen at C5-6 and C6-7. Tani T, Kawasaki M, Taniguchi S, et al: Functional importance of degenerative spondylolisthesis in cervical spondylotic myelopathy in the elderly. Spine 2003;28:1128-1134.
Question 644
High Yield
A 24-year-old woman was struck by a mini van in a parking lot and sustained a closed segmental tibia fracture that was treated with an intramedullary nail the following morning. Follow-up examinations reveal a slowly progressive clawing of all five toes, a progressive equinocavovarus contracture, and the patient is unable to perform a single heel rise on the affected limb. At 1 year after surgery, the patient now has a 10-degree equinus contracture that is not relieved with knee flexion. Treatment should now consist of
Explanation
This is an example of a missed deep posterior compartment syndrome that typically presents 6 months after the injury with progressive clawing due to necrosis, scarring, and contracture of the posterior tibial tendon, flexor digitorum longus, and flexor hallucis longus. Treatment consists of debridement of necrotic muscle and scar tissue with corresponding tendon excision. After debridement and posterior capsule release, if the equinus is relieved with knee flexion, a gastrocnemius slide may be performed. Otherwise, the lengthening should be at the level of the Achilles tendon. Bracing will not address the claw toes. Hansen ST Jr: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott Williams & Wilkins, 2000, pp 212-213. Manoli A II, Smith DG, Hansen ST Jr: Scarred muscle excision for the treatment of established ischemic contracture of the lower extremity. Clin Orthop Relat Res 1993;292:309-314.
Question 645
High Yield
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of

Explanation
It is not uncommon for patients with ankylosing spondylitis to sustain extension-type fractures, most typically of the cervicothoracic junction. These fractures can appear nondisplaced or minimally displaced initially, making them difficult to diagnose. Because there is no mobility between vertebrae, fractures tend to occur more like those of a transverse fracture of a long bone. In addition, the vertebral bodies are vascular and their canals are relatively enclosed, making them vulnerable to epidural bleeding. The MRI scan reveals an epidural hematoma located posteriorly on the cord; therefore, the treatment of choice is surgical evacuation and a posterior laminectomy. Because of the intrinsic instability of such fractures at the time of the laminectomy, internal fixation and stabilization with a posterior fusion is warranted. A simple laminectomy will only increase instability, and control is unlikely with halo vest immobilization. An anterior procedure will not effectively treat the problem given the location of the hematoma. Consideration can be given to methylprednisolone and observation; however, this will not eradicate the problem. Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Question 646
High Yield
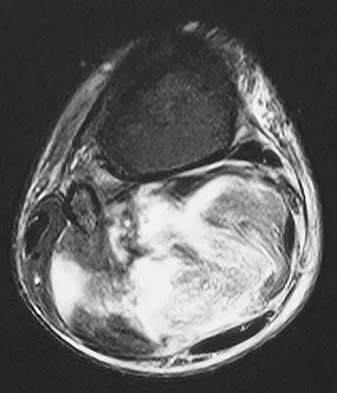
Figures 13a and 13b show the MRI scans of a 70-year-old patient who has a posterior calf mass. Examination reveals that the mass extends to the midcalf level. A biopsy specimen reveals a high-grade soft-tissue sarcoma. Metastatic work-up shows no lesions. Management should consist of

Explanation
Soft-tissue sarcomas generally are treated with radiation therapy and wide surgical resection. In this patient, involvement of most of the posterior calf compartment and circumferential involvement of the posterior tibial and peroneal neurovascular bundle makes limb salvage impractical. Any attempt at wide surgical resection would leave a poorly functioning limb with questionable surgical margins. A high below-knee amputation would be the best option. Radiation therapy alone is contraindicated. Lindberg RD, Martin RG, Romsdahl MM, et al: Conservative surgery and post-operative radiotherapy in 300 adults with soft tissue sarcoma. Cancer 1981;47:2391-2397. Sim FT, Frassica FS, Frassica DA: Soft tissue tumors: Diagnosis, evaluation, and management. J Am Acad Orthop Surg 1994;2:202-211.
Question 647
High Yield
A 45-year-old man reports right shoulder pain with overhead activities only. Figures 47a through 47d show the radiographs, bone scan, and MRI scan of a lesion of the proximal shoulder. What is the most appropriate treatment?



Explanation
The figures show a lesion of the proximal humerus consistent with an enchondroma. The lesion is calcified on the radiographs. There is no cortical destruction, significant endosteal scalloping, or soft-tissue mass. The bone scan shows mild uptake in the area of the proximal humerus, and the T2-weighted MRI scan shows a lesion with high uptake, suggesting a lesion with high water content. A CT scan could also be obtained to rule out bone destruction or periosteal reaction. Pain with overhead activities is likely related to the rotator cuff. A biopsy is unlikely to add information because of inherent difficulties interpreting low-grade cartilaginous lesions. Curettage and grafting and en bloc resection are excessive treatments for a benign lesion that is apparently asymptomatic. Observation with a follow-up radiograph in 3 to 6 months is appropriate. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 648
High Yield
During particle-induced osteolysis around implants, what cell secretes most of the interleukin-6 (IL-6)?
Explanation
During osteolysis, IL-6 is secreted by fibroblasts in the membrane surrounding the prosthesis. IL-6 also can be secreted by osteoblasts in other settings, but they are not the predominant source of IL-6 in particle-induced osteolysis. The remaining cells are not major sources of IL-6.
Question 649
High Yield
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the

Explanation
The patient has primary scapular-trapezius winging. This condition can be caused by blunt trauma to the relatively superficial spinal accessory nerve that is located in the floor of the posterior cervical triangle in the subcutaneous tissue. Other causes of injury include penetrating trauma, traction, or surgical injury. With trapezius winging, the shoulder appears depressed and laterally translated because of an unopposed serratus anterior. This contrasts with primary serratus anterior winging, which is caused by injury to the long thoracic nerve. In this condition, the scapula assumes a position of superior elevation and medial translation, and the inferior angle is rotated medially. The thoracodorsal nerve supplies the latissimus dorsi and is not involved in primary scapular winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 650
High Yield
The arrow in Figure 11 points toward a finding consistent with which of the following?

Explanation
The finding of a unilateral absent pedicle is often referred to as a winking owl sign and is a manifestation of pedicle destruction from metastatic disease. As the vertebral body is destroyed from the neoplastic process, it extends into the pedicle and destroys the cortical rim that normally creates the oval ring of the pedicle on an AP image. McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Question 651
High Yield
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
Because there is a significant possibility that the patient may have a fracture of the lateral process of the talus, there is some disagreement as to the best radiographic study to identify this injury. A CT scan is an appropriate diagnostic tool to visualize the fracture and identify any displacement. Displaced lateral process fractures are best treated surgically. Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder's foot and ankle. Am J Sports Med 1998;26:271-277.
Question 652
High Yield
An 18-year-old football halfback reports that he had immediate right knee pain after being tackled 1 week ago. Examination now reveals moderate tenderness over the proximal medial tibia and lateral joint and normal cruciate stability. In evaluating the integrity of the posterolateral knee structures, what is the most reliable examination finding?
Explanation
The most reliable test for a relatively isolated posterolateral complex (PLC) injury is the asymmetric tibial external rotation or "dial test." It can be performed with the patient prone or supine. When greater than 10 degrees of external rotation at 30 degrees of flexion is present when compared with the opposite knee, it indicates significant damage to the posterolateral structures. Asymmetric external rotation, which is also present at 90 degrees of flexion, indicates injury to the posterior cruciate ligament (PCL) as well. Varus laxity may indicate significant damage to both the PLC and PCL. Approximately 35% of the normal population may have a reverse pivot shift when examined under anesthesia; therefore, it is considered a less specific test. The external rotation/recurvatum and posterolateral drawer tests are adjunctive in assessing isolated posterolateral laxity but are not thought to be as reliable. Veltri DM, Warren RF: Isolated and combined posterior cruciate injuries. J Am Acad Orthop Surg 1993;1:67-75.
Question 653
High Yield
At the L4-5 level, what is the location of the S2-5 nerve roots in relationship to the L5 and S1 nerve roots?
Explanation
The nerve roots of S2-5 are positioned dorsally and in the midline relative to the L5 and S1 nerve roots. The L5 nerve root is located lateral to S1 as it prepares to exit under the L5 pedicle. The S1 nerve root is located lateral and ventral to the S2-5 nerve roots. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 3-17.
Question 654
High Yield
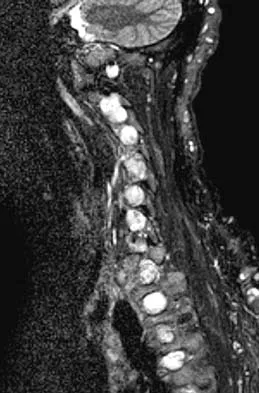
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?
Explanation
Muliple neurofibromas result in marked foraminal enlargement as seen on the sagittal MRI scan. Collagen disorders leading to dural ectasia may show similar enlargement, but none of these is listed as a possible answer. Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 655
High Yield
Figure 10 shows the radiograph of a 9-year-old girl who injured her left lower leg after being thrown from a horse. Examination reveals no other injuries. Which of the following forms of management will provide the lowest rate of complications and the earliest return to function?

Explanation
Because the patient has a transverse midshaft fracture with no evidence of comminution, the treatment of choice is closed reduction and stabilization with flexible intramedullary nails. Transverse fractures treated with an external fixator heal with poor callus and have a high refracture rate. In addition, the pin tracks produce undesirable and excessive scarring. Femoral pin traction is safe and effective but results in considerable muscle wasting and a slow return to function. Interlocking nails run the risk of greater trochanteric growth disturbance and/or osteonecrosis of the femoral head in this age group. Plate fixation, while effective, requires considerable tissue dissection with large scar formation. It also requires a rather extensive dissection for later plate removal. Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Question 656
High Yield
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of

Explanation
Asymptomatic spondylolysis in a child or adolescent should be observed for the possible development of spondylolisthesis, but no other active intervention is needed. The initial treatment of choice for symptomatic spondylolysis includes rest and activity modifications, nonsteroidal anti-inflammatory drugs, physical therapy, bracing, and casting. Immobilization with a TLSO or pantaloon spica cast may permit healing of an acute pars fracture. Rarely, surgical treatment may be necessary. Surgical options include posterolateral L5-S1 fusion or direct repair of the pars defect. Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis. J Pediatr Orthop 1989;9:538-540.
Question 657
High Yield
A 53-year-old patient is seen in the emergency department after sustaining a fall onto her left hip. A current radiograph is shown in Figure 40. What is the best treatment option?

Explanation
The patient has sustained a Vancouver B2 periprosthetic femoral fracture (a femoral fracture that occurs around or just distal to a loose stem, with adequate proximal bone stock). The stem is no longer fixed to proximal bone; therefore, retention of the femoral component is not recommended. Nonsurgical management is contraindicated because of the high risk of nonunion and malunion with significant component settling in the distal fragment and leg shortening. Revision femoral arthoplasty must attain distal fixation in adequate host bone, which is usually successful with a porous-coated cylindrical stem. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 658
High Yield
Figures 36a and 36b show the radiographs of a 3-year old child who has a congenital upper extremity deformity. Which of the following features would be a major contraindication to a centralization procedure?


Explanation
The patient has bilateral absent radii or radial clubhand. Patients who lack elbow flexion take advantage of the hand position to reach their mouths, and a centralization procedure would take away that ability. This procedure can be performed on patients with partial to complete absence of the radius. A hypoplastic thumb can be addressed at a staged procedure; it does not represent a contraindication to centralization. Complete thumb absence can be addressed by pollicizing the index ray. Green DP: Operative Hand Surgery, ed 2. New York, NY, Churchill Livingstone, 1988, pp 269-271.
Question 659
High Yield
Which of the following is considered the most predictive factor in determining whether a patient will need a blood transfusion after total knee arthroplasty?
Explanation
Multiple studies have shown that the preoperative hemoglobin level is the most predictive factor in determining whether a transfusion will be necessary after total hip or total knee arthroplasty. Studies have not shown any correlation with the other options. Salido JA, Marin LA, Gomez LA, Zorrilla P, Martinez C: Preoperative hemoglobin levels and the need for transfusion after prosthetic hip and knee surgery: Analysis of predictive factors. J Bone Joint Surg Am 2002;84:216-220. Sculco TP, Gallina J: Blood management experience: Relationship between autologous blood donation and transfusion in orthopedic surgery. Orthopedics 1999;22:S129-S134.
Question 660
High Yield
A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh. Passive movement of the hip appears to elicit tenderness and very limited hip motion. A radiograph of the pelvis shows mild subluxation of the left hip. The next step in evaluation should consist of
Explanation
The diagnosis of bone and joint sepsis in a newborn is difficult because of the relative lack of obvious signs and symptoms. Fever is usually absent. A study of 34 newborns with osteomyelitis identified prematurity and delivery by cesarean section as predisposing factors. In that study, the most common clinical findings were pseudoparalysis, local swelling, and pain on passive movement. Because early diagnosis is so important, any infant who exhibits these findings should be suspected as having bone or joint sepsis. Once the area of involvement is identified, aspiration is mandatory. In newborns who have an infection about the hip, radiographs may reveal subluxation. In this patient, septic arthritis must be ruled out by aspiration of the hip. Developmental dysplasia of the hip is not painful and is not accompanied by localized swelling. If no purulent material is obtained at the time of hip aspiration, an arthrogram should be obtained to rule out epiphysiolysis of the proximal femur. Because the area of involvement has been identified by clinical examination, a gallium scan or MRI scan of the spine is not indicated. Knudsen CJ, Hoffman EB: Neonatal osteomyelitis. J Bone Joint Surg Br 1990;72:846-851.
Question 661
High Yield
A 13-year-old boy hyperextends his knee while playing basketball and reports a pop that is followed by a rapid effusion. A lateral radiograph is shown in Figure 4. Initial management consists of attempted reduction with extension, with no change in position of the fragment. What is the next most appropriate step in management?

Explanation
Avulsion fractures of the tibial spine are rare injuries that result from rapid deceleration or hyperextension of the knee in skeletally immature individuals. This injury is the equivalent of ruptures of the anterior cruciate ligament in adults. These fractures are classified as types 1 through 3. Type 1 is a minimally displaced fracture, type 2 fractures have an intact posterior hinge, and type 3 fractures have complete separation. The radiograph demonstrates a completely displaced, or type III, tibial spine avulsion. Surgical reduction is indicated in type 2 fractures that fail to reduce with knee extension and in all type 3 fractures. Reduction may be arthroscopic or open, with fixation of the bony fragment using a method that maintains physeal integrity and prevents later growth arrest. Preferred techniques would be with suture or an intra-epiphyseal screw Wiley JJ, Baxter MP: Tibial spine fractures in children. Clin Orthop 1990;255:54-60. Mulhall KJ, Dowdall J, Grannell M, et al: Tibial spine fractures: An analysis of outcome in surgically treated type III injuries. Injury 1999;30:289-292. Owens BD, Crane GK, Plante T, et al: Treatment of type III tibial intercondylar eminence fractures in skeletally immature athletes. Am J Orthop 2003;32:103-105.
Question 662
High Yield
Which of the following factors are considered prognostic of survival in patients with soft-tissue sarcomas?
Explanation
The factors that are independently prognostic of patient survival are tumor size, tumor grade, and tumor depth (ie, subfascial versus superficial). These factors are the basis for the American Joint Committee on Cancer staging criteria. Patient age and neurovascular invasion are not prognostic. Surgical margin is prognostic for local recurrence but not conclusively for patient survival or metastasis. Metastatic disease is also predictive of survival. Cheng EY, Thompson RC Jr: New developments in the staging and imaging of soft-tissue sarcomas. Instr Course Lect 2000;49:443-451.
Question 663
High Yield
A 19-year-old female long-distance runner has an incomplete tension-side femoral neck stress fracture. Management should consist of
Explanation
Unlike compression-side stress fractures, tension-side stress fractures on the superior side of the femoral neck are at a very high risk of displacement, even if the patient is not bearing weight. It is highly recommended to treat these fractures like acute fractures and to proceed with internal fixation emergently. Once the fracture has displaced, the prognosis is poor in terms of returning to sports, even when reduced and internally fixed. Nonsurgical management, such as limited weight bearing and low-impact activities, works very well for other lower extremity stress fractures. A training program evaluation (shoes, tracks, schedule) is always indicated for all patients with stress fractures.
Question 664
High Yield
A 30-year-old farmer undergoes replantation of an above-the-elbow amputation. What form of management is most important following this surgery?
Explanation
After major limb replantation, the occurrence of ischemic rhabdomyonecrosis can result in lactic acidosis and myoglobulinemia. These complications can be limited by rapid repair of the arterial supply, potentially using a shunt before skeletal stability. Repair of the venous system should be performed after repair of the artery. High volume fluid replacement will maintain a diuresis, thus limiting the complications from myoglobulinemia. Wood MB: Replantations about the elbow, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 1985, pp 472-480.
Question 665
High Yield
Which of the following best describes the course of the median nerve at the elbow?
Explanation
The median nerve courses superficial to the ulnar artery, deep to the fibrous arch of the superficialis muscle, and deep to the superficial head of the pronator teres muscle. The median nerve lies within the interval between the flexor digitorum superficialis muscle and the flexor digitorium muscle as it progresses toward the wrist. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 666
High Yield
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of

Explanation
Monteggia fractures in children must be recognized. Early appropriate treatment is much easier than delayed reconstruction for a missed radial head dislocation. In younger children, attempts should be made to reduce the ulna fracture and radial head dislocation with traction and manual manipulation. Anterior Monteggia fractures are the most common, and in this variety the radius is much better stabilized in elbow flexion. Posterior Monteggia fractures are less common and may be managed in elbow extension. Closed reduction is much more successful in younger children; ulnar fixation with a rod or plate may be needed in older patients with unstable fractures. Annular ligament repair is rarely needed in the acute fracture. Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554. Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
Question 667
High Yield
Which of the following factors is most closely associated with early postoperative migration of "stand-alone" lumbar interbody fusion cages?
Explanation
Postoperative migration of lumbar interbody fusion cages is a rare complication. It is most commonly seen after placement of the cages through a posterior approach, with instability of the final construct. It is not associated with the design of the cage, the type of graft used, or a resultant pseudarthrosis. McAfee PC: Interbody fusion cages in reconstructive operations on the spine. J Bone Joint Surg Am 1999;81:859-880.
Question 668
High Yield
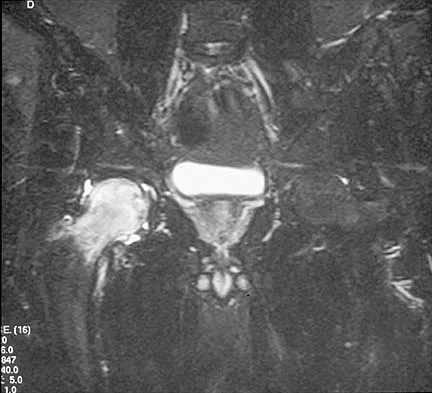
A 21-year-old patient has had pain and a marked decrease in active and passive shoulder motion after having had a seizure 2 months ago as the result of alcohol abuse. Current AP and axillary radiographs and a CT scan are shown in Figures 26a through 26c. Management should consist of



Explanation
Open reduction and subscapularis and lesser tuberosity transfer into the defect is the treatment of choice in young individuals who have defects that involve between 20% to 45% of the head. Disimpaction and bone grafting is an option in injuries that are less than 3 weeks old. Closed reduction 2 to 3 months after injury usually is unsuccessful and increases the risk of fracture or neurovascular injury. Total shoulder arthroplasty is reserved for defects of greater than 50% or with associated glenoid surface damage. Hemiarthroplasty should be avoided in young individuals unless 50% or more of the head is involved. Gerber C: Chronic locked anterior and posterior dislocations, in Warner JJ, Iannotti JP, Gerber C (eds): Complex and Revision Problems in Shoulder Surgery. Philadelphia, PA, Lippincott-Raven, 1997, pp 99-113.
Question 669
High Yield
A woman with a neck and chest tumor has weakness in the biceps and paresthesias in the thumb. Brachioradialis and infraspinatus function are normal. The lesion is affecting which of the following structures?

Explanation
The lateral cord terminates as the musculocutaneous nerve and also contributes sensory fibers to the median nerve. Involvement of the C6 root or upper trunk could potentially cause weakness of the infraspinatus and the brachioradialis. The middle trunk and the posterior cord do not contribute motor fibers to the thumb or sensory fibers to the thumb.
Question 670
High Yield
A 2-year-old girl has had a swollen right knee for the past 7 weeks. There is no history of significant trauma, and she has not had a fever or been ill. Her parents report that she is stiff in the morning but otherwise does not report pain. A CBC count and erythrocyte sedimentation rate are normal. Treatment with naproxen at appropriate doses for the past 2 weeks has resulted in some improvement. Radiographs show only soft-tissue swelling. Examination reveals a healthy-appearing child with a warm and swollen right knee that is only slightly tender but lacks full extension by 20 degrees. What is the next most appropriate step in management?
Explanation
Up to 30% of children with juvenile rheumatoid arthritis (increasingly known now as juvenile idiopathic arthritis or JIA) already have potentially damaging uveitis at the time of diagnosis. This patient has typical oligoarticular JRA (JIA) and therefore is at significant risk for uveitis. MRI, radioisotope scanning, or an ACE level most likely would not provide additional useful diagnostic information because intra-articular derangement, osteomyelitis, or sarcoidosis are all unlikely. Arthrocentesis and triamcinolone hexacetonide joint injection might be indicated if continued use of nonsteroidal medication does not result in improvement, but should be held off for at least an additional 4 to 6 weeks to see if continued use of naproxen results in control of the arthritis. Wolf MD, Lichter PR, Ragsdale CG: Prognostic factors in the uveitis of juvenile rheumatoid arthritis. Ophthalmology 1987;94:1242. Cassidy JT, Petty RE: Textbook of Pediatric Rheumatology. Philadelphia, PA, WB Saunders, 2001, p 220.
Question 671
High Yield
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?

Explanation
The patient's right upper extremity is held in the "head waiter's" posture with the shoulder internally rotated, the elbow extended, and the wrist in flexion. The Erb type of obstetrical brachial plexus palsy involves the C5 and C6 nerve root, and occasionally, as in this child, the C7 nerve root. Obstetrical palsy is a traction injury, and is associated with a high birth weight, shoulder dystocia, cephalopelvic disproportion, or the use of forceps. Erb palsy is four times more common than injury to the entire plexus or injury to the C8 and T1 nerve roots. It results from the shoulder being depressed while the head and neck are laterally rotated, extended, and tilted in the opposite direction. Most patients recover wrist extension and elbow flexion. Patients with residual weakness of shoulder external rotation and abduction will benefit from release of the pectoralis major, latissimus dorsi, and teres major, with transfer of the latissimus dorsi and the teres major to the posterosuperior aspect of the rotator cuff. Recent studies using arthrograms and CT scans have shown a higher incidence of posterior glenoid deficiency and posterior subluxation than that observed with plain radiographs. The posterior subluxation or dislocation can be effectively reduced by tendon release and transfer procedures. Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Question 672
High Yield
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
Ford and associates studied 81 high school basketball players and found that females landed with greater total valgus knee loading and a greater maximum valgus knee angle than male athletes. Hewett and associates reported in a study of 205 female athletes that those with increased dynamic valgus and high abduction loads were at increased risk of anterior cruciate ligament injury. Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
Question 673
High Yield
What is the most consistent finding regarding glenohumeral kinematics in patients with symptomatic tears of the rotator cuff?
Explanation
Normal glenohumeral kinematics are represented by ball-and-socket modeling when the rotator cuff is intact. This is true for motion that involves more than 30 degrees of abduction. In patients with shoulder pain and symptomatic rotator cuff tears, superior translation occurs with abduction beyond 30 degrees. This is quite evident in massive tears but is seen consistently to a lesser degree with smaller tears. Yamaguchi K, Sher JS, Anderson WK, et al: Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
Question 674
High Yield
A 9-year-old girl reports progressive right knee pain. Radiographs are shown in Figures 59a and 59b. Work-up reveals no other sites of disease. Low- and high-power photomicrographs are shown in Figures 59c and 59d. What is the most appropriate treatment?


Explanation
This classic case of osteosarcoma illustrates the typical radiographic and histologic characteristics of this disease. The radiographs show an aggressive-appearing lesion of the distal femur. The lesion has both lytic and blastic areas. Periosteal reaction is present in the form of a Codman's triangle. The radiographs are highly suggestive of osteosarcoma. The photomicrographs show malignant spindle cells that produce osteoid, thus confirming the diagnosis of osteosarcoma. Treatment of osteosarcoma is multimodal including multi-agent chemotherapy and surgery (wide resection or amputation). Bacci G, Ferrari S, Bertoni F, et al: Long-term outcome for patients with nonmetastatic osteosarcoma of the extremity treated at the Instituto Ortopedico Rizzoli according to the Instituto Ortopedico Rizzoli/osteosarcoma-2 protocol: An updated report. J Clin Oncol 2000;18:4016-4037. Bielack SS, Kempf-Bielack B, Delling G, et al: Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J Clin Oncol 2002;20:776-790.
Question 675
High Yield
A 10-year-old boy has had wrist pain for the past 3 months. He denies any history of trauma. He reports mild tenderness associated with a palpable mass. A radiograph and biopsy specimens are shown in Figures 52a through 52c. What is the most likely diagnosis?

Explanation
The radiograph shows a benign-appearing cortically based lesion eroding the underlying cortex, producing a saucer-shaped defect typical of a periosteal chondroma. The histology shows benign-appearing neoplastic cartilage. Although enchondroma would have the same histologic appearance, radiographs generally show a lesion with a central medullary epicenter. The benign-appearing histology does not support chondrosarcoma. Chondromyxoid fibroma will generally show histologic elements of its fibrous and myxoid components. Chondroblastoma typically demonstrates histologic findings of polyhedral cells separated by a chondroid matrix with pericellular, lattice-like "chicken wire" calcification. Schajowicz F: Tumors and Tumorlike Lesions of Bone: Pathology, Radiology, and Treatment, ed 2. Berlin, Springer-Verlag, 1994, pp 147-151.
Question 676
High Yield
An 18-month-old child with obstetrical palsy has a maximum external rotation as shown in Figure 34. The parents should be advised that without surgical treatment the likelihood that glenoid dysplasia will develop is approximately what percent?

Explanation
Based on the available literature, the probability of development of glenoid dysplasia in the setting of a significant limitation of external rotation is close to 70%. Humeral dysplasia is also likely and can be managed surgically. Efforts are being made to identify procedures that will prevent glenoid dysplasia and help maintain function. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667. Waters PM, Smith GR, Jaramillo D: Glenohumeral deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:668-677.
Question 677
High Yield
A 67-year-old woman has had pain in the area of the metatarsal heads and toes bilaterally for the past 18 months. She describes a diffuse discomfort and a constant burning sensation. She notes that the area feels swollen. Examination reveals that her pulses are normal, and there is no frank swelling or focal tenderness. What is the most likely diagnosis?
Explanation
Patients with peripheral neuropathy will often initially see an orthopaedic surgeon and report symptoms of burning, numb, dead, or wooden feet. A simple diagnostic evaluation with a tuning fork (to test vibratory sensibility) or use of the Semmes-Weinstein monofilaments will help make the diagnosis. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 113-121.
Question 678
High Yield
Figure 33 shows the CT scan of a 40-year-old man who injured his left shoulder while skiing. What structure is attached to the bony fragment?
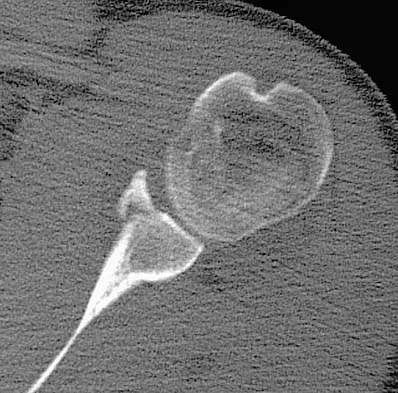
Explanation
The scan reveals a bony Bankart lesion. The anterior band of the inferior glenohumeral ligament is the major restraint to anterior translation of the humeral head and is usually injured with anterior shoulder dislocations. It inserts onto the glenoid labrum at the anteroinferior aspect of the glenoid rim. The labrum most frequently avulses from the glenoid (Bankart lesion), but occasionally the bony attachment is avulsed. O'Brien SJ, Neves MC, Arnoczky SP, et al: The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sports Med 1990;18:449-456.
Question 679
High Yield
A 75-year-old woman notes a slowly enlarging mass in the right anterior thigh. Her medical history is significant only for hypertension. An MRI scan of her thigh is shown in Figures 60a through 60d. Which of the following surgical margins is the most appropriate for removal of this lesion?
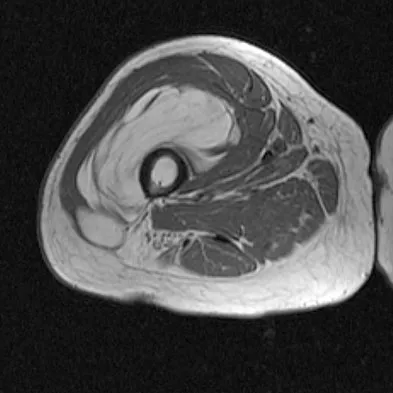
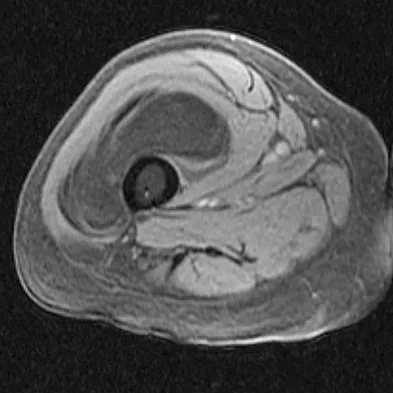
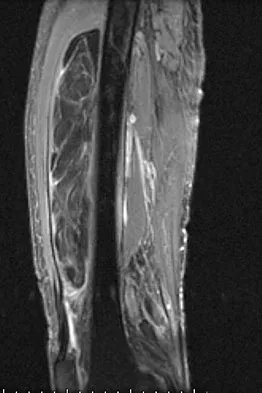
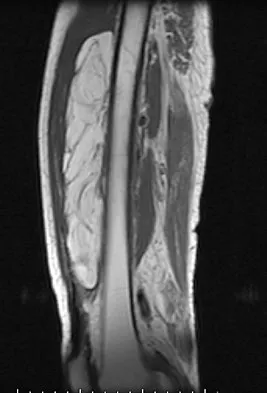
Explanation
The patient has a large deep anterior thigh mass that has imaging characteristics of mature fat. Intramuscular lipomas are effectively treated with marginal resections with very low recurrence rates. Large lipomas often have small amounts of intralesional signal changes frequently representing trapped muscle fibers and do not necessitate more extensive margins. Gaskin CM, Helms CA: Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas): Results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol 2004;182:733-739.
Question 680
High Yield
Figures 23a and 23b show the MRI scans of a 50-year-old woman who has increasing gait disturbance. She reports three falls in the past week. Examination reveals hyperreflexia, motor weakness in the biceps and triceps, and a positive Hoffman's sign. What is the most appropriate treatment plan?

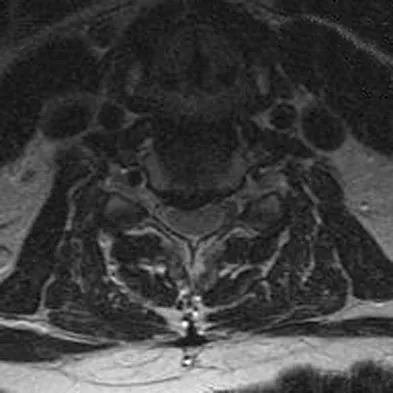
Explanation
The patient has obvious signs of progressive myelopathy. Based on her significant physical examination findings, nonsurgical management will not significantly impact her outcome. Cervical decompression alone is contraindicated in patients with cervical kyphosis such as seen here. Anterior cervical fusion is the best option. Emery SE, Bohlman HH, Bolesta MJ, et al: Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy: Two to seventeen-year follow-up. J Bone Joint Surg Am 1998;80:941-951. Ferguson RJ, Caplan LR: Cervical spondylotic myelopathy. Neurol Clin 1985;3:373-382.
Question 681
High Yield
A 63-year-old woman reports giving way of the knee and pain after undergoing primary total knee arthroplasty (TKA) 1 year ago. Examination reveals that the knee is stable in full extension but has gross anteroposterior instability at 90 degrees of flexion. The patient can fully extend her knee with normal quadriceps strength. Studies for infection are negative. AP and lateral radiographs are shown in Figures 12a and 12b, respectively. What is the appropriate management?
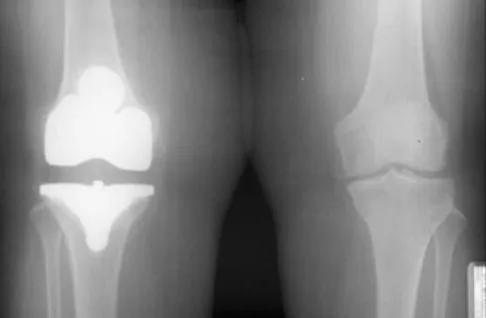

Explanation
The radiographs show posterior flexion instability that is the result of a flexion-extension gap imbalance and posterior cruciate ligament incompetence after a posterior cruciate ligament-retaining TKA. The femur is anteriorly displaced on the tibia, with lift-off of the femoral component from the tibial polyethylene. Revision to a larger femoral component will address the larger flexion gap relative to the extension gap, and a posterior stabilized implant will address the posterior cruciate ligament insufficiency. Pagnano and associates, reporting on a series of painful TKAs previously diagnosed as pain of unknown etiology, showed that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant. Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
Question 682
High Yield
A 78-year-old woman undergoes her third lumbar decompression and fusion from L3 to L5 without complication. On the morning of postoperative day 3, examination reveals painless, flaccid weakness of both lower extremities. She also has an absent bulbocavernous reflex and a mild saddle paresthesia. MRI scans of the lumbar spine are shown in Figures 26a and 26b. What is the most appropriate management at this time?
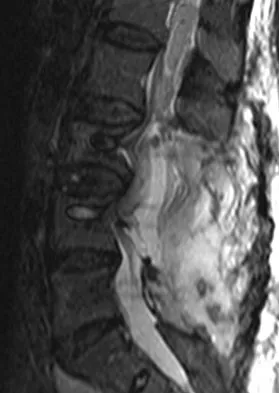
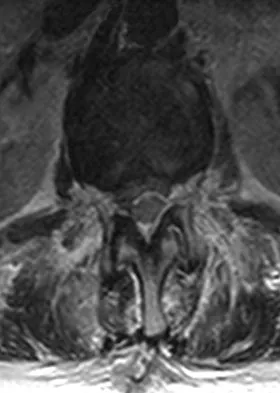
Explanation
The MRI scans reveal a large postoperative hematoma causing significant thecal compression. An epidural hematoma with neurologic deficit is a surgical emergency requiring immediate evacuation of the hematoma. Although the incidence of postoperative epidural hematomas is rare, the consequences of a missed diagnosis can be catastrophic. Early recognition and evacuation are essential in preserving or restoring neurologic function. Uribe and associates attributed delayed postoperative hematomas to previous multiple lumbar surgeries as a possible contributing factor. Yi S, Yoon do H, Kim KN, et al: Postoperative spinal epidural hematoma: Risk factor and clinical outcome. Yonsei Med J 2006;47:326-332.
Question 683
High Yield
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?
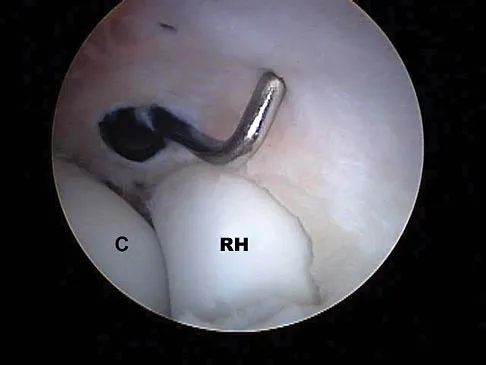
Explanation
The image shows a view of the radiocapitellar joint from an anterior medial portal. The radial nerve lies on the elbow capsule at the midportion of the capitellum. It is at risk for injury when capsular excision is performed in this region. Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 684
High Yield
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15 degrees), anatomic varus of greater than 10 degrees, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
Question 685
High Yield
Which of the following actions best enhances performance when an athlete is participating in a 10K race?
Explanation
Proper hydration prior to an athletic event is the most important determinant of performance. It is virtually impossible to keep pace with fluid loss during an athletic competition. When a net loss of fluid occurs and the athlete is properly prehydrated, this fluid loss will not adversely affect performance. It is not necessary to load up on carbohydrates prior to a 10K race, or to replace calories burned during the race. Hyponatremia can develop in ultra-endurance athletes, especially marathoners, if they hydrate without replacing electrolytes lost through sweating; however, this is highly unlikely for a 10K race. Newmark SR, Toppo FR, Adams G: Fluid and electrolyte replacement in the ultramarathon runner. Am J Sports Med 1991;19:389-391.
Question 686
High Yield
Which of the following is considered an important component in treating the lesion shown in Figure 56?

Explanation
Mucoid cysts are commonly associated with DIP joint arthritis. Two treatment options are commonly used: (1) aspiration/drainage and injection of corticosteroid and (2) surgical excision. When performing the surgery, excision of the bony osteophytes about the DIP joint is helpful in achieving a cure. There are no reports of significant benefit with nail removal or partial ligament or extensor tendon resection. Some authors have advocated skin excision and rotational flaps for wound coverage, but this is somewhat controversial. Rizzo M, Beckenbaugh RD: Treatment of mucous cysts of the fingers: Review of 134 cases with minimum 2-year follow-up evaluation. J Hand Surg Am 2003;28:519-524.
Question 687
High Yield
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include

Explanation
Typically, posterior spinal fusion to the pelvis is recommended for patients with spinal muscular atrophy and advanced scoliosis. Examination for lower extremity muscle contractures is important because the contractures may interfere with good sitting balance. Anterior release and fusion usually are not advised. Diaphragmatic pacing is not indicated because diaphragm function usually is not affected. Patients with spinal muscular atrophy usually are not ambulatory or only marginally ambulatory at the time of scoliosis surgery; therefore, gait analysis usually is not relevant. While a muscle biopsy may have a role in the diagnosis of this disorder, it plays no subsequent role in determining life expectancy or the value of spinal surgery. Daher YH, Lonstein JE, Winter RB, Bradford DS: Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 1985;5:391-395.
Question 688
High Yield
A 28-year-old woman who is training for the New York Marathon reports pain in the posteromedial aspect of her right ankle. Examination reveals tenderness just posterior to the medial malleolus. Radiographs are normal. An MRI scan is shown in Figure 3. What is the most likely diagnosis?

Explanation
Any of the above conditions is credible with a limited history. The MRI scan unequivocally shows the stress fracture in the distal tibia. Most tibial stress fractures can be managed with rest and immobilization. Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 689
High Yield
What is the most common contracture deformity of the spastic shoulder secondary to a cerebrovascular accident?

Explanation
The resultant spasticity and weakness (paresis) following a cerebrovascular accident leads to muscle imbalance that commonly results in contracture of the shoulder in adduction, internal rotation, and varying degrees of forward flexion. In addition, the elbow is usually flexed and the forearm pronated. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 690
High Yield
A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in

Explanation
The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures. Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Question 691
High Yield
A 25-year-old woman undergoes surgical treatment of a displaced proximal humeral fracture via a deltopectoral approach. At the first postoperative visit, she reports a tingling numbness along the anterolateral aspect of the forearm. What structure is most likely injured?
Explanation
Sensation along the anterolateral aspect of the forearm is supplied by the lateral antebrachial cutaneous nerve, the terminal branch of the musculocutaneous nerve. The musculocutaneous nerve can be injured by proximal humeral fractures or dislocations, and is also at risk during surgical exposure if excessive retraction is placed on the conjoint tendon. The musculocutaneous nerve enters the conjoint tendon 1 cm to 5 cm distal to the coracoid process. McIlveen SJ, Duralde XA, D'Alessandro DF, et al: Isolated nerve injuries about the shoulder. Clin Orthop 1994;306:54-63.
Question 692
High Yield
A patient who sustained injuries in a motorcycle accident 30 minutes ago has significant motor and sensory deficits corresponding to a C6 level of injury. A lateral radiograph obtained during the initial on-scene evaluation reveals bilateral jumped facets at C5-C6; this appears to be an isolated injury. The patient is awake and alert. The next step in management of the dislocation should consist of
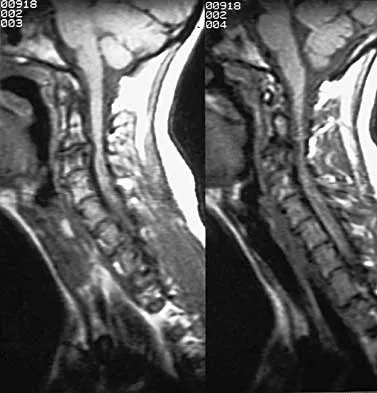
Explanation
Surgical open reduction may increase the neurologic deficit if a disk herniation exists. Evidence from animal studies suggests that rapid decompression of the spinal cord may improve recovery. Serially increasing traction weight to reduce the dislocation has been shown to be safe when used in patients who are awake. Indications for MRI include patients who are unable to cooperate with serial examinations, the need for open reduction, and progression of deficit during awake reduction. Delamarter RB, Sherman J, Carr JB: Pathophysiology of spinal cord injury: Recovery after immediate and delayed decompression. J Bone Joint Surg Am 1995;77:1042-1049. Star AM, Jones AA, Cotler JM, Balderston RA, Sinha R: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Question 693
High Yield
An 8-year-old boy reports ankle pain after striking the ground with the medial aspect of his foot while attempting to kick a soccer ball. Radiographs reveal slight distal tibial physeal widening but no other abnormalities. In treating this injury, which of the following associated conditions is most likely present but may be missed without careful evaluation?

Explanation
Malrotation of the foot is frequently overlooked in this clinical setting. This can be judged by evaluating and comparing the transmalleolar axes of the affected and unaffected legs. The rotation occurs through the physis and frequently is not recognized until the patient has been walking for a few months. The other conditions are not expected to occur in the clinical setting described. Phan VC, Wroten E, Yngve DA: Foot progression angle after distal tibial physeal fractures. J Pediatr Orthop 2002;22:31-35.
Question 694
High Yield
A 23-year-old woman falls from a bicycle and sustains a right knee injury. Figures 12a through 12d show radiographs and MRI scans of the knee. What is the most likely diagnosis?




Explanation
The radiographs and MRI scans both show an avulsion of the anterior cruciate ligament, which has been described by Meyers and McKeever in three different fracture patterns. Type I fractures are nondisplaced or have minimal displacement of the anterior margin. Type II fractures have superior displacement of their anterior aspect with an intact posterior hinge. Type III fractures are completely displaced. Although the injury is visible on the radiographs, it is more subtle in adults than children. Thus, MRI is helpful in clarifying this injury in adults. Open or arthroscopic reduction and internal fixation is recommended for type II and type III fractures that do not respond to closed reduction. Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684. Wiss DA, Watson JT: Fractures of the tibial plateau, in Rockwood CA, Green DP, Bucholz RW, et al (eds): Rockwood and Green's Fractures in Adults. Philadelphia, PA, Lippincott-Raven, 1996, pp 1920-1953.
Question 695
High Yield
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of

Explanation
The patient has subtalar arthrosis, a loss of heel height with anterior ankle impingement. The mechanics of the ankle are impaired, and dorsiflexion is painful and limited. The talar declination angle is measured by drawing a line through the longitudinal axis of the talus and the plane of support of the foot on a weight-bearing lateral radiograph. Anterior impingement is suggested with any value below 20°. By performing a distraction arthrodesis through the subtalar joint, the normal declination of the talus is reestablished, eliminating the anterior ankle impingement. Tibiotalocalaneal fusion would be inappropriate because the patient does not have arthritic symptoms in the ankle. Ankle arthroscopy or in situ arthrodesis would not reestablish appropriate ankle mechanics, and the osteophytes would be prone to redevelop. Lateral wall ostectomy may help with impingement at the level of the fibula or the lateral ankle but would provide no benefit to anterior ankle impingement. Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Question 696
High Yield
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of

Explanation
The radiograph shows developmental dysplasia of the hip with the hip reduced and congruent. The treatment of choice is a periacetabular osteotomy because it can improve hip biomechanics and prolong the function of the hip joint. This procedure should be performed prior to the development of severe degenerative changes. Observation will not alter the patient's natural history or the biomechanics of the hip. A total hip arthroplasty should be delayed until severe degenerative changes are present. A Chiari osteotomy is a salvage osteotomy used for a noncongruent subluxated hip. A Pemberton osteotomy requires an open triradiate cartilage; therefore, it is not an option in an adult. Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Question 697
High Yield
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of

Explanation
Following a CVA and with the resumption of upright posture, downward subluxation of the glenohumeral joint may occur. Although usually painless, some patients may report pain secondary to stretching of the brachial plexus. This is the result of flaccid paralysis of the deltoid muscle, and it will persist until some motor tone or spasticity returns to the shoulder girdle musculature. Early sling support and range-of-motion exercises to prevent contracture will provide the best relief. Surgical procedures are not indicated. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 698
High Yield
A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In addition to closed reduction, management should include


Explanation
The examination and radiographs reveal a closed fracture-dislocation of the ankle with tibiofibular diastasis. Immediate fixation of the medial malleolus and plating of the fibula are indicated. If residual tibiofibular diastasis occurs with lateral translation of the fibula after plating, a syndesmotic screw is placed to stabilize the syndesmosis. Ankle fracture-dislocations associated with a proximal fibular fracture (Maisonneuve fracture) require syndesmotic fixation, but the fibula is not plated. Unstable ankle fractures require surgical treatment. If swelling is severe (fracture blisters, loss of skin wrinkling), a compressive splint is applied and surgery is delayed for 5 to 7 days. Browner BD, Jupiter JB, Levine AM, Trafton PG: Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 1887-1957.
Question 699
High Yield
A 36-year-old woman is brought to the emergency department intubated and sedated following a motor vehicle accident. She is moving her upper and lower extremities spontaneously. She cannot follow commands. CT scans are shown in Figures 7a through 7c. The initial survey does not reveal any other injuries. Initial management of the cervical injury should consist of immediate



Explanation
The patient has a bilateral facet dislocation of C6-C7 with preservation of at least some neurologic function. Urgent reduction is necessary. However, because she is sedated and unable to follow commands, an MRI scan is necessary before any closed or open posterior reduction to look for an associated disk herniation. If a disk herniation is present, it must be removed prior to any reduction maneuver to prevent iatrogenic neurologic injury. It is very unlikely that this injury can be reduced with an open anterior procedure alone. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 189-199.
Question 700
High Yield
Compared with cobalt-chromium, the biomechanical properties of titanium on polyethylene articulation in total hip replacement result in

Explanation
The surface hardness of titanium is low compared with that of cobalt-chromium alloys. Titanium articulations are easily scratched, resulting in a significantly increased rate of wear and debris production. The wear and resulting lysis can also result in an increased rate of loosening. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Agins HJ, Alcock NW, Bansal M, et al: Metallic wear in failed titanium-alloy total hip replacements: A histological and quantitative analysis. J Bone Joint Surg Am 1988;70:347-356.
