HY 2026
00:00
Start Quiz
Question 501
High Yield
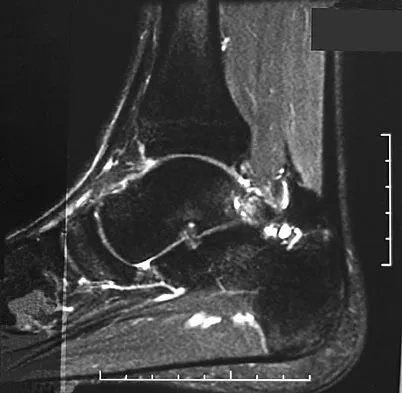
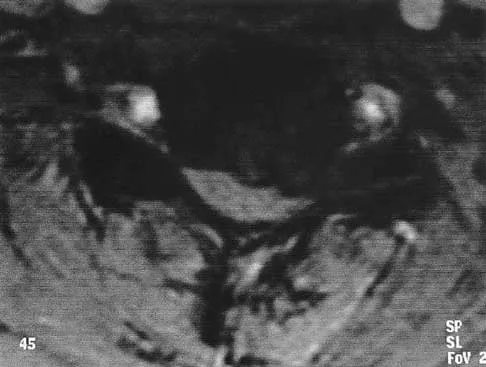
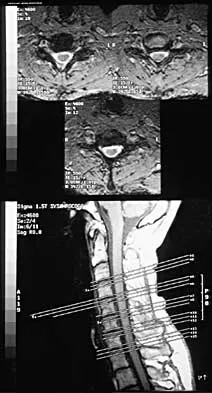
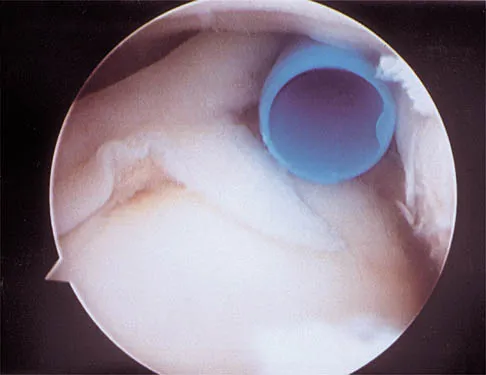
A 28-year-old professional dancer reports a 3-month history of progressive pain in the posterior aspect of the left ankle. Her symptoms are worse when she assumes the en pointe position. Examination reveals tenderness to palpation at the posterolateral aspect of the ankle posterior to the peroneal tendons which is made worse with passive plantar flexion. There is no nodularity, fluctuance, or tenderness of the Achilles tendon. The neurovascular examination is unremarkable. A lateral radiograph and MRI scan are shown in Figures 16a and 16b, respectively. Management should consist of

Explanation
The imaging studies reveal findings typical of the os trigonum syndrome. This condition results from inflammation between the os trigonum and the adjacent talus. The symptoms of posterior ankle pain are exacerbated by plantar flexion, which stresses the fibrous union between these two bones. Definitive management of the high-level athlete involves excision of the os trigonum from a medial approach, although arthroscopic excision has also been described. The os trigonum is not an intra-articular structure; therefore, ankle arthroscopy is neither diagnostic nor therapeutic. Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057. Mouhsine E, Crevoisier X, Leyvraz P, et al: Post-traumatic overload or acute syndrome of the os trigonum: A possible cause of posterior ankle impingement. Knee Surg Sports Traumatol Arthrosc 2004;12:250-253.
Question 502
High Yield
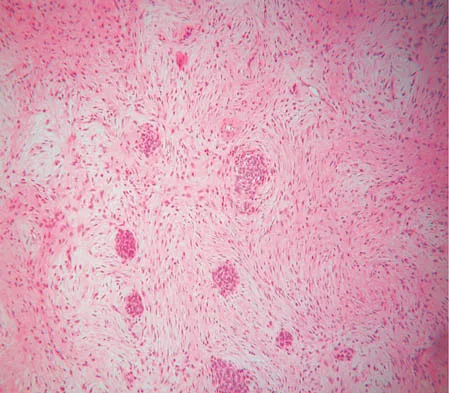
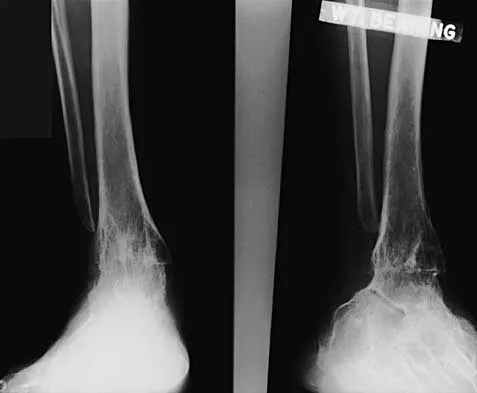
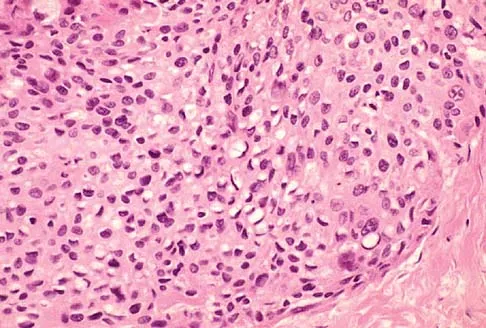
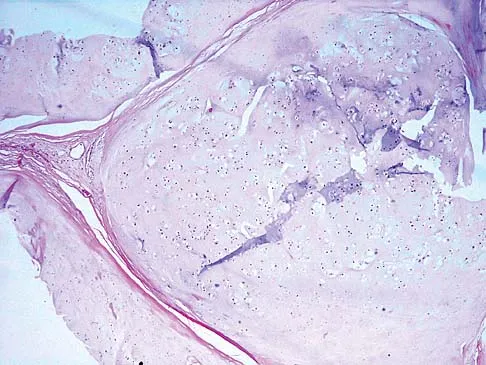
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?

Explanation
The radiograph and pathology are consistent with adamantinoma. While the mechanism underlying adamantinoma has not been identified, it is believed to be closely related to osteofibrous dysplasia, which may represent a precursor. The other diagnoses are not known to give rise to adamantinoma.
Question 503
High Yield
Which of the following best describes the resultant forces on an increased offset stem when compared with a standard offset stem?

Explanation
The increased emphasis on restoring offset in total hip arthroplasty has implications for the forces applied to the components and the fixation interfaces. Static analysis has shown that with an increased affect, joint reaction force on the articulation is decreased. When the resultant load on the hip is "out of plane" (ie, directed anterior to posterior), there is increased torsion where the stem is turned into more retroversion. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180. Hurwitz DE, Andriaacchi TP: Biomechanics of the hip, in Callaghan J, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott-Raven , 1998.
Question 504
High Yield
A paraplegic 32-year-old man was pulling himself up in bed by grasping the headboard rails when he felt a pop and immediate pain. A radiograph and CT scan are shown in Figures 2a and 2b. Based on these findings, management should consist of


Explanation
The coracoid process is an essential component of the superior shoulder suspensory complex and must be maintained. Open reduction and internal fixation is recommended if the fragment is large and displaced more than 1 cm. Froimson AI: Fracture of the coracoid process of the scapula. J Bone Joint Surg Am 1978;60:710-711.
Question 505
High Yield
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
In general, a previously healthy patient with an acute onset of nontraumatic lower back pain does not need diagnostic imaging before proceeding with therapeutic treatment. In the absence of any "red flags" during the history and physical examination, such as trauma or constitutional symptoms (ie, fevers, chills, weight loss), the appropriate treatment for acute onset lower back pain is purely symptomatic treatment including limited analgesics and early range of motion. Diagnostic imaging is not necessary unless the initial treatment is unsuccessful and symptoms are prolonged. Miller and associates suggested that the use of radiographs can lead to better patient satisfaction but not necessarily better outcomes. Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Question 506
High Yield
Figure 33 shows the venogram of a patient who has a long history of alcohol abuse. Warfarin should be used cautiously because of the interaction with which of the following factors?

Explanation
Warfarin acts by inhibiting clotting factors II, VII, IX, X. The actual mechanism of action is by inhibition of hepatic enzymes, vitamin K epoxide, and perhaps vitamin K reductase. This inhibition results in lack of carboxylation of vitamin K-dependent proteins (II, VII, IX, X). The anticoagulant effect of warfarin can be reversed with vitamin K or fresh-frozen plasma. The use of alcohol may lead to liver dysfunction and an even more limited margin of available factors. Lieberman JR, Wollaeger J, Dorey F, et al: The efficacy of prophylaxis with low-dose warfarin for prevention of pulmonary embolism following total hip arthroplasty. J Bone Joint Surg Am 1997;79:319-325.
Question 507
High Yield
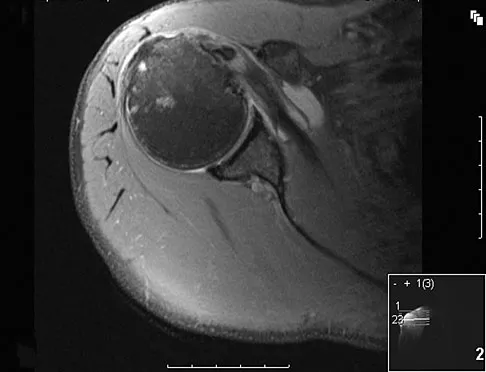
A 50-year-old man reports left shoulder pain and weakness after undergoing a lymph node biopsy in his neck 2 years ago. Examination reveals winging of the left scapula. Electromyography shows denervation of the trapezius. Surgical treatment for this condition involves
Explanation
The muscle transfer procedure most commonly performed for trapezius paralysis is the Eden-Lange procedure. Trapezius paralysis in this patient is secondary to iatrogenic injury to the spinal accessory nerve during lymph node biopsy. In this procedure, the levator scapulae and rhomboid minor and major muscles are transferred laterally. Pectoralis transfer to the inferior border of the scapula is used as a dynamic transfer for serratus anterior winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325. Langenskiold A, Ryoppy S: Treatment of paralysis of the trapezius muscle by Eden-Lange operation. Acta Orthop Scand 1973;44:383-388.
Question 508
High Yield
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
The maximum stress in a bone occurs at the periosteal surface (the greatest distance from the center of the bone). The magnitude of the stress is equal to the magnitude of the applied moment (M) multiplied by the distance to the surface (roughly the radius of the bone, r) divided by the area moment of inertia (I), so that stress = Mr/I. Of the possible answers, only area moment of inertia of the cross section contains any of these three items. The stress can also depend on the length of the bone, but it cannot be determined without knowing the location at which the bending load is applied, information that was not given in the problem. The type of structural support may influence local stresses where the support contacts the bone, but it has little effect on the maximum stress in the bone. The cross-sectional area is not as important as the area moment of inertia because the stress is not evenly distributed over the cross-section. Plastic modulus is a material property, not a geometric or structural property, and it does not affect stress. Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Question 509
High Yield
A 24-year-old woman who has hypotension, a head injury, and who experienced a poor response to resuscitation has been taken to the operating room for a splenectomy. Following abdominal surgery she remains unstable with increasing pulmonary respiratory pressures and decreasing oxygen saturation. She has a transverse mid-diaphyseal fracture of the tibia with a 4-cm laceration and soil-contaminated muscle in the wound. Based on these findings, management should consist of
Explanation
Because the patient is critically ill and requires expeditious care, stabilization of the long bone fracture is required, but definitive care of the fracture should be postponed. The treatment of choice at this time is irrigation with 12 L of saline solution, followed by debridement and nondefinitive stabilization with a simple four-pin external frame to regain axial and rotational alignment. When the patient's condition is more stable, more definitive care can be performed. Bosse MJ, Kellam JF: Orthopaedic management decisions in the multiple trauma patient, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 151-164. Weresh MJ, Stover MD, Bosse MJ, Jeray K, Kellam JF: Pulmonary gas exchange during intramedullary fixation of femoral shaft fractures. J Trauma 1999;46:863-868.
Question 510
High Yield
What structure is considered the single most important soft-tissue restraint to anterior-posterior stability of the sternoclavicular joint?
Explanation
In a cadaver ligament sectioning study, the posterior capsular ligament was considered the most important structure for anterior-posterior stability of the sternoclavicular joint. The anterior capsular ligament also helps prevent anterior displacement but not to the same degree as the posterior ligament. The interclavicular ligament provides little support for anteroposterior translation. Spencer EE, Kuhn JE, Huston LJ, et al: Ligamentous restraints to anterior and posterior translation of the sternoclavicular joint. J Shoulder Elbow Surg 2002;11:43-47.
Question 511
High Yield
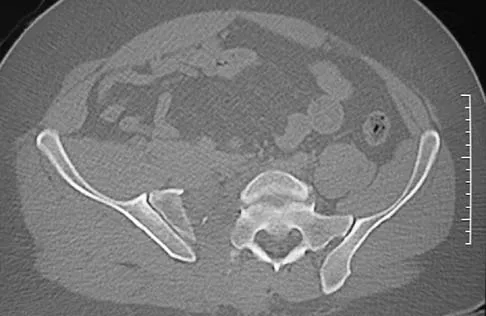
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
Iliosacral screws have gained popularity for posterior stabilization of pelvic ring disruptions, but complications attributed to incorrect placement are a clinical problem. The L5 nerve root is at greatest risk and is in closest proximity to a malpositioned screw (exiting the sacrum). The L4 root is more anterior at this level. The S1 root is still intraosseous at this level and is at risk but not from the screw exiting anteriorly at this level. The arteries are at risk but are more anterior and are at less risk than the L5 nerve root.
Question 512
High Yield
A 45-year-old man who underwent an ankle arthrodesis reports that for the first 6 years he had significant pain relief after the fusion healed. However, he now has increasing pain in the sinus tarsi. AP and lateral radiographs are shown in Figures 8a and 8b. What is the most likely cause of the patient's symptoms?

Explanation
The patient has a solid ankle fusion radiographically. With a tibiotalar arthrodesis, the adjacent joints (subtalar and transverse tarsal) take additional stress. Over time, progressive degenerative arthritis will occur in these adjacent joints, often necessitating further surgery. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631.
Question 513
High Yield
A 2-day-old infant has the hyperextended knee deformity shown in Figure 7. No other deformities are found on examination. A radiograph shows that the ossified portion of the proximal tibia is slightly anterior to that of the distal femur. Management should consist of
Explanation
Congenital dislocation of the knee is an uncommon deformity that varies in presentation from simple hyperextension to complete anterior dislocation of the tibia on the femur. Treatment varies with the age at presentation and the severity of the deformity. Most authors recommend early nonsurgical management. A recent study of 24 congenital knee dislocations in 17 patients found that satisfactory results were obtained in most instances using closed treatment. Based on their findings, the authors concluded that immediate reduction or serial casting should be performed when the patient is seen early after birth. If the patient is seen late and correction cannot be achieved by serial casting, traction followed by closed or open reduction may be necessary. Early percutaneous quadriceps recession has been described for complex congenital knee dislocations associated with underlying disorders, such as arthrogryposis and Ehlers-Danlos syndrome. Ko JY, Shih CH, Wenger DR: Congenital dislocation of the knee. J Pediatr Orthop 1999;19:252-259. Johnson E, Audell R, Oppenheim WL: Congenital dislocation of the knee. J Pediatr Orthop 1987;7:194-200.
Question 514
High Yield
Which of the following muscles attaches to the coracoid process of the scapula?
Explanation
The insertion of the pectoralis minor is on the base of the coracoid process. The coracoid helps define the interval between the subscapularis and supraspinatus muscles but neither attaches to it. The coracobrachialis and short head of biceps attach to the tip of the coracoid but are not listed as options. The long head of the biceps attaches to the supraglenoid tubercle. The serratus arises from the vertebral border of the scapula. Jobe CM: Anatomy and surgical approaches, in Jobe FW (ed): Operative Techniques in Upper Extremity Sports Injuries. St Louis, MO, Mosby, 1996, pp 140-142.
Question 515
High Yield
What is the most common complication following interscalene nerve block for shoulder surgery?
Explanation
All of these complications have been documented after interscalene nerve block. Other serious complications such as cardiac arrest and respiratory distress have also been noted. However, the most common complication after interscalene nerve block appears to be temporary paresthesia to the hand that can occur in up to 2.3% of the patients. Bishop JY, Sprague M, Gelber J, et al: Interscalene regional anesthesia for shoulder surgery. J Bone Joint Surg Am 2005;87:974-979.
Question 516
High Yield
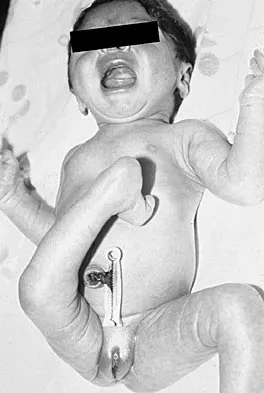
Figure 6 shows the clinical photographs of a newborn who underwent a colostomy for an imperforate anus. Examination shows extended knees, flexed hips, and equinovarus feet. Dimpling is noted over the buttocks. Patients with these findings differ from patients with myelodysplasia in that they

Explanation
The patient has sacral agenesis. Clinical signs include the classic dimpling over the buttocks and the characteristic lower extremity deformities. Imperforate anus is often associated with this disorder. Although motor function correlates with the level of vertebral defect, sensation is usually intact. This is important therapeutically, because patients are not as prone to pressure sores as are those with myelodysplasia. Kyphosis may develop in many patients with lumbosacral agenesis, but lordosis is unusual. Latex allergy and progressive neural deterioration may occur in patients with either myelodysplasia or sacral agenesis but is more common in the former.
Question 517
High Yield
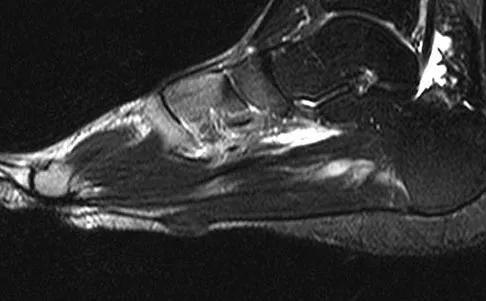
Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing total contact casts. The deformity does not correct passively. Dorsalis pedis and posterior tibial pulses are palpable. The patient is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. The ulcer is currently healed. What is the best option to prevent recurrent ulceration and infection?


Explanation
This is a nonplantigrade deformity in a patient with a Charcot foot deformity. Longitudinal studies have shown that recurrent ulceration/infection is likely unless the deformity is corrected. Achilles tendon lengthening is advised for simple forefoot ulcers. The current approach to this problem is best managed with surgical correction of the deformity, Achilles tendon lengthening, and therapeutic footwear. Bevan WP, Tomlinson MP: Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ank Int 2008;29:568-573. Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Question 518
High Yield
Figures 35a and 35b show the axial T2-weighted and coronal T1-weighted MRI scans of a patient who has enlargement of the right thigh. What is the most likely diagnosis?
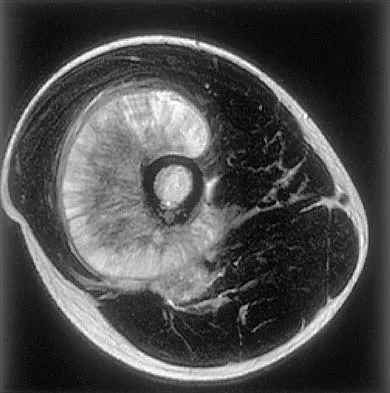
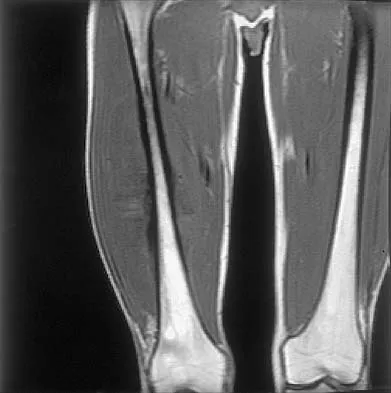
Explanation
The images show a large, almost circumferential, mass surrounding the diaphysis of the femur. The intramedullary signal is normal with minimal cortical destruction, both findings that should be abnormal in conventional osteosarcoma and Ewing's sarcoma. There are very low-signal striations representing osteoid formation that would have a sunburst radiographic pattern. This indicates an osteogenic lesion. Myositis ossificans is not indicated because studies would reveal zonal ossification starting in the periphery rather than the more central pattern seen in this patient. This appearance is typical for periosteal osteosarcoma.
Question 519
High Yield
Which of the following structures is most vulnerable during a medial sesamoidectomy of the hallux?
Explanation
The plantar-medial cutaneous nerve is at risk with the surgical approach to the medial sesamoid. It is found directly underlying an incision made at the junction of the glabrous skin of the hallux and must be identified before the approach can proceed. Transection will result in a painful neuroma that impinges on the plantar-medial surface of the toe and cause problems with shoe wear. The only other structure that lies near the surgical field is the abductor hallucis tendon which lies dorsal to the incision.
Question 520
High Yield
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?

Explanation
A prospective randomized study of patients with degenerative spondylolisthesis and spinal stenosis by Herkowitz and Kurz showed significantly improved clinical outcomes in patients who also received a lumbar arthrodesis. Patients with a laminectomy at an adjacent level do not have improved outcomes with an arthrodesis. Minimal lumbar scoliosis does not require arthrodesis. Arthrodesis is indicated in cases where there is removal of more than 50% of the facets bilaterally but not with an associated foraminal stenosis. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-807.
Question 521
High Yield
In revision total hip arthroplasty, an acetabular reconstruction cage is best indicated for which of the following patterns of bone loss?

Explanation
Acetabular cage reconstruction is indicated in severe disruption of acetabular bone stock when a cementless acetabular component cannot be stabilized in intimate contact with a sufficient bed of structurally sound and viable host bone, with or without a structural graft. Cages are used in pelvic discontinuity where they provide a bridge between the ilium and the ischium, while supporting a cemented cup. All of the other scenarios are amenable to achieving an adequate rim fit for a cementless component, using a jumbo cup if necessary. Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Question 522
High Yield
A 58-year-old woman with rheumatoid arthritis and a severe hindfoot valgus deformity now reports recurrent lateral ankle pain. Examination reveals pain over the fibula and sinus tarsi, with a valgus hindfoot that is passively correctable. Despite the use of an ankle-foot orthosis, this is the second time this problem has occurred. Radiographs and a clinical photograph are shown in Figures 28a through 28c. What is the next most appropriate step in treatment?



Explanation
Excessive hindfoot valgus can lead to abutment between the calcaneus and fibula. This valgus force can lead to a stress fracture of the distal fibula. Surgery may be required if an insufficiency fracture recurs despite orthotic management. Of the choices listed, a subtalar arthrodesis is most likely to achieve rebalancing of the foot at the level of the deformity. Stephens HM, Walling AK, Solmen JD, Tankson CJ: Subtalar repositional arthrodesis for adult acquired flatfoot. Clin Orthop 1999;365:69-73
Question 523
High Yield
What is the most frequent late complication of cementless fixation in total knee arthroplasty?

Explanation
The incidence of osteolysis, particularly around fixation screws in the tibia, can be as high as 30%. Stable femoral component fixation is generally maintained. Infection, subluxation of the patella, and stiffness can occur with either cemented or cementless fixation. Peters PC, Engh GA, Dwyer KA, Vinh TN: Osteolysis after total knee arthroplasty without cement. J Bone Joint Surg Am 1992;74:864-876.
Question 524
High Yield
A 14-year-old boy who is right handed reports right shoulder pain. Radiographs show a lucent lesion of the proximal humeral epiphysis with a narrow zone of transition. Results of an open biopsy confirm the presence of a chondroblastoma. Based on these findings, the next most appropriate step in management should consist of

Explanation
The patient has a chondroblastoma of the proximal humerus; therefore, the treatment of choice is curettage and bone grafting. Surgical resection of the proximal humerus is not indicated in the initial treatment of an intraosseous chondroblastoma. Mirra JM: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, pp 589-623.
Question 525
High Yield
A previously asymptomatic 14-year-old girl sustained a twisting injury to her ankle. Radiographs are shown in Figures 2a and 2b. Management should consist of


Explanation
The radiographs show a well-defined, irregular, eccentric lesion in the distal tibia metaphysis with a thin sclerotic margin. The radiographs are diagnostic of nonossifying fibroma, a common entity in this age group and in this location. No further work-up is indicated. The patient was asymptomatic prior to the injury and the lesion is small and thus not worrisome for an impending pathologic fracture; therefore, no treatment is indicated beyond observation. The natural history of these lesions is to gradually ossify as the patient reaches skeletal maturity. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 69-75.
Question 526
High Yield
Which of the following is an important factor in performing a proper biopsy?

Explanation
There are a number of important technical details in performing a biopsy. Incisions should always be longitudinal in the extremity. Good hemostasis is important in avoiding contamination from hematoma. The approach should avoid neurovascular structures, and go through a single muscle belly when possible. Although a frozen section should be obtained to ensure adequate viable tissue has been obtained, definitive diagnosis is not necessary at the time of the frozen section. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 197-215.
Question 527
High Yield
A sentinel event is defined as an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. What is the most common sentinel event related to spine surgery?
Explanation
Patient safety and prevention of medical errors is a major focus of recent national advocacy groups. Analysis has shown that the most common sentinel event in spine surgery is surgery on the wrong level. Therefore, it is recommended that every patient have the surgical site signed, the level of surgery marked intraoperatively, and a radiograph taken. Surgery on the wrong level is most likely to occur in single-level decompressive procedures. Wong DA, Watters WC III: To err is human: Quality and safety issues in spine care. Spine 2007;32:S2-S8.
Question 528
High Yield
A 47-year-old woman falls and sustains a direct blow to her middle finger. She notes pain and swelling and is unable to move the proximal interphalangeal (PIP) or distal interphalangeal (DIP) joints. Radiographs are shown in Figures 8a through 8c. Proper management should consist of



Explanation
The oblique nature of the fracture and extension of the fracture to the condyles implies an unstable fracture. Lag screw fixation provides an excellent chance of union, and the ability to start early range of motion. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green's Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 281.
Question 529
High Yield
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be
Explanation
Although the patient has a large herniated nucleus pulposus, the pain has decreased from 10/10 to 3/10 over a 4-week period and the patient is now free of any neurologic symptoms. It is quite likely that further nonsurgical management will continue to resolve his symptoms. In the absence of any neurologic deficits, there is no evidence that the patient is at significant risk for paralysis. Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
Question 530
High Yield
What is the most appropriate indication for replantation in an otherwise healthy 35-year-old man?

Explanation
Vascular anastamoses are exceedingly difficult with amputations distal to the nail fold as the digital vessels bifurcate or trifurcate at this level, and little functional benefit is gained compared to other means of soft-tissue coverage. Single digit amputations, other than the thumb, are a relative contraindication for replantation. Replantations at the level of the proximal phalanx lead to poor motion of the proximal interphalangeal joint. In a healthy active adult, an amputation through the wrist is an appropriate situation to proceed with a replantation. A transverse forearm amputation is a good indication with a warm ischemia time of less than 6 hours. Urbaniak JR: Replantation, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1085.
Question 531
High Yield
Which of the following benign bone lesions can develop lung metastases?
Explanation
Although considered benign bone lesions, lung metastases can develop in giant cell tumors and chondroblastomas. These often can be treated with multiple thoracotomies, resulting in long-term survival. Roberts PF, Taylor JG: Multifocal benign chondroblastomas: Report of a case. Hum Pathol 1980;11:296-298.
Question 532
High Yield
Ulnohumeral distraction interposition arthroplasty is considered the most appropriate treatment for which of the following patients?

Explanation
Distraction interposition arthroplasty is indicated for the treatment of both rheumatoid and posttraumatic arthritis and is reserved for younger patients who are not suitable candidates for total elbow arthroplasty. Although less reliable than prosthetic replacement, distraction interposition arthroplasty is a useful option in the treatment of young, high-demand patients with elbow arthritis. It is rarely indicated in the presence of polyarticular inflammatory arthritis but may be of value in those patients in whom the disease is limited primarily to the elbow. Isolated radiocapitellar arthritis can be successfully treated with radial head resection, although caution should be exercised if there is evidence of instability. Osteoarthritis is best treated with ulnohumeral arthroplasty. Cheng SL, Morrey BF: Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82:233-238.
Question 533
High Yield
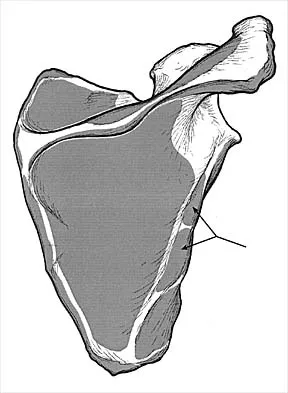
Which of the following nerves innervates the muscle that originates from the middle third of the dorsal surface of the lateral border of the scapula, as shown in Figure 7?
Explanation
Teres minor originates from the middle third of the dorsal surface of the lateral border of the scapula. It is supplied by the axillary nerve (C5). Williams PL, Warwick R, Dyson M, Bannister LH: Myology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 611-615.
Question 534
High Yield
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the

Explanation
The radiographs show fractures of the coronoid and radial head. The medial collateral ligament has been avulsed from the ulnar insertion, and there is a valgus opening on the medial side. The lateral collateral ligament is always disrupted in elbow dislocations and fracture-dislocations that occur secondary to falls. This is known as the terrible triad injury (dislocation and fractures of the coronoid and radial head); it has a very poor prognosis because of its propensity for recurrent or persistent instability and late arthritis. The principle in treating this injury is to repair all of the injured parts or protect them with a hinged external fixator until they heal. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 535
High Yield
What is the most common presenting sign or symptom in an adult with lumbar pyogenic infection?
Explanation
Pain is very common but is often nonspecific; therefore, the diagnosis of spinal infection is often delayed. Fever and sepsis can occur but are not common. Neurologic manifestations also can occur but are absent in most patients. In findings reported by Carragee, the urinary tract is a common source for hematogenous spinal infection, but the source was found in only 27% of 111 patients. Direct inoculation during spinal surgery is uncommon. Carragee EJ: Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am 1997;79:874-880. Frazier DD, Campbell DR, Garvey TA, et al: Fungal infections of the spine: Report of eleven patients with long-term follow-up. J Bone Joint Surg Am 2001;83:560-565.
Question 536
High Yield
A 45-year-old man undergoes an anterior cervical diskectomy and fusion at C5-6 and C6-7 with instrumentation. During the first postoperative visit at 1 week, the patient reports difficulty swallowing and mild anterior cervical tightness. The anterior wound is benign and the patient denies any dyspnea or shortness of breath. A postoperative radiograph is seen in Figure 25. What is the most appropriate management at this time?

Explanation
The radiograph shows significant prevertebral soft-tissue swelling following a two-level anterior cervical diskectomy and fusion. The incidence of dysphagia 2 years after anterior cervical spine surgery is 13.6%. Risk factors for long-term dysphagia after anterior cervical spine surgery include gender, revision surgeries, and multilevel surgeries. The use of instrumentation, higher levels, or corpectomy versus diskectomy did not significantly increase the prevalence of dysphagia. Lee and associates demonstrated that while dysphagia after anterior cervical spine surgery is a common early finding, it generally decreases significantly by 6 months with nonsurgical management. A minority of patients experience moderate or severe symptoms by 6 months after the procedure. Female gender and multiple surgical levels have been identified as risk factors for the development of postoperative dysphagia. Lee MJ, Bazaz R, Furey CG, et al: Risk factors for dysphagia after anterior cervical spine surgery: A two-year prospective cohort study. Spine J 2007;7:141-147.
Question 537
High Yield
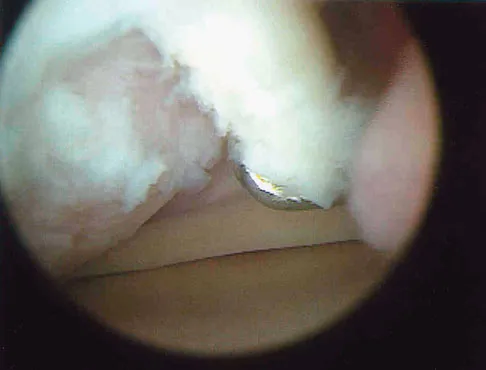
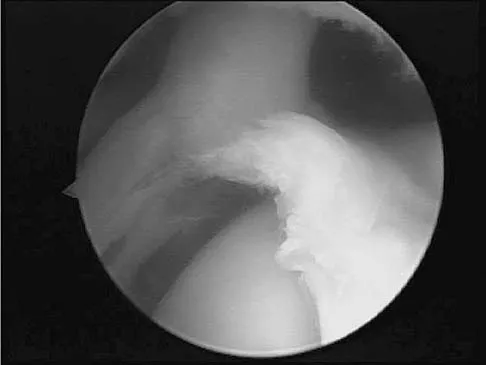
Which of the following anatomic structures is often difficult to visualize during elbow arthroscopy?

Explanation
The ulnar collateral ligament is often difficult to visualize during elbow arthroscopy. It can be seen clearly in only 10% to 30% of elbow arthroscopies. All of the other structures should be easily and thoroughly seen and palpated during elbow arthroscopy. Johnson LL: Arthroscopic Surgery: Principles and Practice. St Louis, MO, CV Mosby, 1988.
Question 538
High Yield
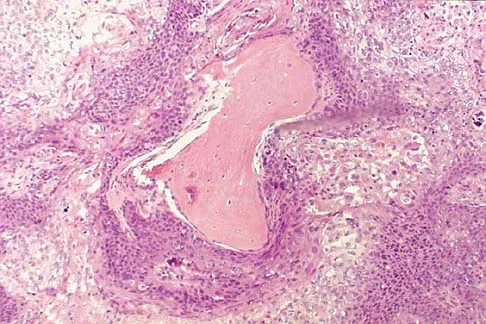
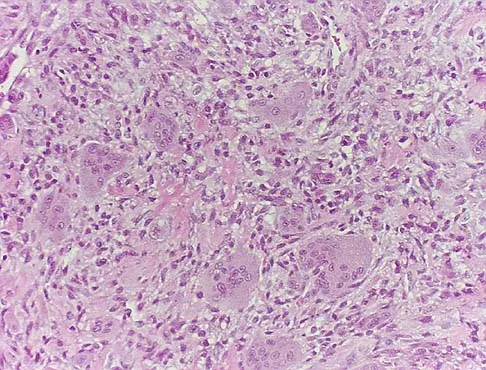
A 69-year-old man has a painful slow-growing lesion of the distal phalanx of his thumb. History reveals that he has had chronic osteomyelitis of the thumb for the past 12 years. The radiograph and biopsy specimens are seen in Figures 9a through 9c. Treatment should consist of

Explanation
The diagnosis is squamous cell carcinoma. The radiograph shows a destructive lesion, and the histologic slides demonstrate squamous cells invading bone. The preferred treatment for squamous cell carcinoma is wide resection; however, in this location a wide margin can be achieved only with amputation. Overall survival in patients with squamous cell carcinoma secondary to chronic osteomyelitis is not significantly worse than that expected for age-matched controls. Dell PC: Hand, in Simon MA, Springfield D (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 405-420.
Question 539
High Yield
Which of the following substances is least likely to affect the success of bone union after lumbar arthrodesis?
Explanation
Much attention has been given to the use of supplemental postoperative analgesia with nonsteroidal anti-inflammatory drugs (NSAIDs), and a significant reduction in narcotic use has been recorded. However, a high failure rate of arthrodesis has been associated with the use of postoperative NSAIDs. Glassman and associates reported 29 cases of pseudarthrosis in 167 patients when ketorolac was used as a postoperative analgesic, whereas only five fusion failures were noted in 121 patients not using ketorolac. Indomethacin and ibuprofen have been shown to adversely affect bone formation in clinical and animal trials. Nicotine has also been shown in a number of studies to decrease the fusion rate. Oxycodone hydrochloride is a synthetic morphine and does not affect the fusion process. Glassman SD, Rose SM, Dimar JR, Puno RM, Campbell MJ, Johnson JR: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838. Deguchi M, Rapoff AJ, Zdeblick TA: Posterolateral fusion for isthmic spondylolisthesis in adults: Analysis of fusion rate and clinical results. J Spinal Disord 1998;11:459-464.
Question 540
High Yield
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?

Explanation
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate. Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
Question 541
High Yield
A 64-year-old man with a history of metastatic lung cancer reports increasing right hip pain over the period of several months. Radiographs are shown in Figures 3a and 3b. Initial management should consist of


Explanation
The patient has lung cancer metastatic to the right proximal femur. The lesion is large, has destroyed a portion of the cortex, and involves the peritrochanteric region. All of these findings put the patient at high risk for pathologic fracture. The lesion is amenable to intramedullary fixation in the form of some type of reconstruction nail. Chemotherapy alone will not restore the bone stock. Given the extent of the lesion, radiation therapy, chemotherapy, or embolization will not prevent fracture. A proximal femoral replacement would be indicated in patients with bone destruction extending into the femoral head and neck. Bisphosphonates may diminish the risk of subsequent lesions but are not sufficient to treat this high-risk lesion. Radiation therapy should be given postoperatively to prevent further bone destruction.
Question 542
High Yield
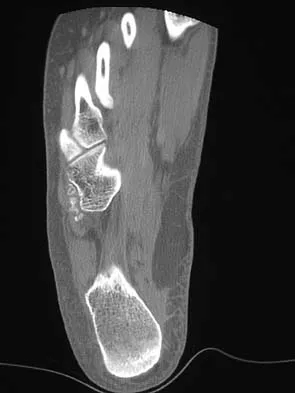
The oblique radiograph of the foot and the CT scan shown in Figures 10a and 10b show a patient whose symptoms have failed to respond to rest and non-steroidal anti-inflammatory drugs. What is the best course of action?

Explanation
The radiograph and MRI scan show elongation and fragmentation of the os peroneum. Although casting, orthoses, and steroid injection may relieve symptoms, excision of the os peroneum and primary repair when necessary, with or without tenodesis of the peroneus longus to the peroneus brevis, have been shown to produce excellent results. Haddad SL: Disorders of tendons: Peroneal tendon dysfunction, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 812-817.
Question 543
High Yield
Figures 10a and 10b show the clinical photograph and MRI scan of a plantar foot lesion. If excisional biopsy is performed, what is the most likely complication?

Explanation
The MRI scan shows plantar fibromatosis. The treatment is usually nonsurgical. If surgery is indicated, wide local excision with excision of the entire plantar fascia is usually indicated. The main problem with simple excision of the lesion is the high chance of recurrence. The other listed complications are those that are a result of the wide local excision. Aluisio FV, Mair SD, Hall RL: Plantar fibromatosis: Treatment of primary and recurrent lesions and factors associated with recurrence. Foot Ankle Int 1996;17:672-678.
Question 544
High Yield
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?


Explanation
The stretched peroneus brevis muscle and tendon follow anterior to the fibula and are most likely incarcerated with reduction. The anterior talofibular ligament is too small to prevent reduction of the ankle joint itself. The extensor digitorum brevis originates from the talus; therefore, it is not involved in the tibiotalar joint. The posterior tibial tendon lies medially and would not be interposed into the ankle joint. Similarly, the anterior tibialis tendon also would not be involved. Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Question 545
High Yield
A 47-year-old woman has an asymptomatic pelvic mass that was discovered on routine gynecologic examination. A radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 7a through 7d. Metastatic work-up is negative. Treatment should consist of



Explanation
The imaging studies show a chondrosarcoma; therefore, surgical treatment is indicated. There is no role for intralesional treatment of an exophytic lesion, particularly in the pelvis. Even obtaining a biopsy specimen risks intrapelvic contamination, although many surgeons would still perform a biopsy prior to a resection to confirm the diagnosis. Chondrosarcoma is considered resistant to both radiation therapy and chemotherapy; therefore, radiation therapy generally is not used except for unresectable lesions. Chemotherapy would be used only for metastatic disease or in patients with high-grade chondrosarcoma. The grade would not be known until after resection, and in this patient, the histology slide showed a grade I neoplasm. Chemotherapy would not be used preoperatively because a cartilage tumor is unlikely to shrink, and in this patient, the lesion is resectable. Springfield DS, Gebhardt MS, Mcguire MH: Chondrosarcoma: A review. J Bone Joint Surg Am 1996;78:141-149.
Question 546
High Yield
A 29-year-old man reports a 2-week history of severe neck pain after being struck sharply on the back of the head and neck while moving a refrigerator down a flight of stairs. Initial evaluation in the emergency department revealed no obvious fracture and he was discharged in a soft collar. Neurologic examination is within normal limits, and radiographs taken in the office are shown in Figures 21a through 21c. Subsequent MRI scans show intra-substance rupture of the transverse atlantal ligament. What is the most appropriate treatment option at this time?



Explanation
Dickman and associates classified injuries of the transverse atlantal ligament into two categories. Type I injuries are disruptions through the substance of the ligament itself. Type II injuries render the transverse ligament physiologically incompetent through fractures and avulsions involving the tubercle of insertion of the transverse ligament on the C1 lateral mass. Type I injuries are incapable of healing without supplemental internal fixation. Type II injuries can be treated with a rigid cervical orthosis with a success rate of 74%. Surgery may be required for type II injures that fail to heal with 3 to 4 months of nonsurgical management. Findlay JM: Injuries involving the transverse atlantal ligament: Classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery 1996;39:210.
Question 547
High Yield
A 30-year-old man has had a 3-day history of severe, incapacitating lower back pain without radiation. He reports improvement with rest. He denies any history of trauma, has no constitutional symptoms, and his neurologic examination is normal. What is the best course of action?
Explanation
There are no red flags in the history or examination to warrant MRI. Limited bed rest (less than 3 days) has been shown to be more beneficial to early recovery compared with prolonged bed rest (more than 7 days). No data support the use of epidural or facet steroid injections for acute low back pain.
Question 548
High Yield
A 78-year-old patient undergoing revision total knee arthroplasty has bone loss throughout the knee at the time of revision. A distal femoral augment is used to restore the joint line. One month after surgery, the patient reports pain and is unable to ambulate. A lateral radiograph is shown in Figure 34. What is the most likely etiology of this problem?

Explanation
Instability is a leading cause of failure following total knee arthroplasty. Instability can present as global instability, extension gap (varus/valgus) instability, or flexion gap (anterior/posterior) instability. Treatment options are numerous based on the exact pathology. The radiograph reveals anterior/posterior instability with dislocation consistent with flexion gap instability. A loose flexion gap can allow the femoral component to ride above the tibial cam post mechanism, resulting in dislocation. Distal femoral augments treat extension gap instability, whereas tibial augments can treat both flexion and extension gap instability. Posterior condyle augments at the distal femur can also be used to treat flexion gap instability. Flexion gap instability is further aggravated by extension mechanism incompetence. Note the excessively thin patella on the lateral radiograph. Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. McAuley J, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty. Inst Course Lect 2004;53:237-241.
Question 549
High Yield
Figure 2a shows the radiograph of a 48-year-old man who was involved in a motorcycle accident. A CT scan is shown in Figure 2b. The patient underwent pelvic angiography for persistent hypotension despite resuscitation. What vessel is most likely to be injured?

Explanation
The pelvic injury is a severe anterior-posterior compression III or Tile C injury. The vessel most likely injured is the superior gluteal artery, but several arterial bleeding sources are likely. Vertical shear injuries can also injure this vessel, but it is much less common. When arterial injury follows a lateral compression injury, it is usually related to injury of a more anterior vessel like the obturator artery or a branch of the external iliac artery. O'Neill PA, Riina J, Sclafani S, et al: Angiographic findings in pelvic fractures. Clin Orthop 1996;329:60-67.
Question 550
High Yield
A 46-year-old man has incomplete paraplegia after being involved in a motor vehicle accident. The CT scan shown in Figure 5 reveals marked canal compromise. What is the most appropriate management to improve neurologic status?

Explanation
According to a study by the Scoliosis Research Society, the use of anterior decompression is most predictable for improving neurologic status. This is particularly true of bowel and bladder functional loss. Laminectomy is contraindicated because it further destabilizes the spine. Posterior instrumentation and indirect reduction through distraction and ligamentotaxis only incompletely decompress the compromised canal and are successful only if performed within 48 hours of injury. While some improvement may occur with closed management, the amount of recovery is less than that achieved with surgical decompression. A posterior approach and instrumentation may be added to the anterior decompression based on the characteristics of associated injuries to the posterior element. Gertzbein SD: Scoliosis Research Society multicenter spine fracture study. Spine 1992;17:528-540. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-215.
Question 551
High Yield
A patient with rheumatoid arthritis has an unstable pseudarthrosis after undergoing C1-2 posterior fusion. No neurologic deficits are noted, and repair with posterior transarticular fixation screws and a posterior wiring technique at C1-2 is planned. Which of the following preoperative studies offers the best visualization?
Explanation
Dickman and associates reported a greater than 10% incidence of vertebral artery anomalies at the C1-2 junction that would preclude the use of either unilateral or bilateral transarticular screw placement. They noted that 13 of 105 patients had a high-riding transverse foramen that precluded bilateral screw placement. In another series, 17 of 94 patients had unilateral high-riding transverse foramina and three had bilateral anomalies. Thin-cut CT with sagittal reconstructions offers the best visualization of the anomalous position of the vertebral artery. They noted that single screw placement in combination with posterior C1-2 fusion was an effective means to secure C1-2 stability. MRI gives excellent visualization of soft tissues and spinal cord compression but is not as clear as thin-cut CT for visualization of the vertebral artery foramina. Vertebral artery angiography is an invasive study with an inherent potential for complications. Electromyography does not correlate with vertebral artery anatomy. Paramore CG, Dickman CA, Sonntag VK: The anatomic suitability of the C1-2 complex for transarticular screw fixation. J Neurosurg 1996;85:221-224. Dickman CA, Sonntag VK: Posterior C1-C2 transarticular screw fixation for atlantoaxial arthrodesis. Neurosurgery 1998;43:275-280.
Question 552
High Yield
A 47-year-old woman has a right bunion that has been symptomatic despite modifications in shoe wear. She requests surgical correction. An AP radiograph is shown in Figure 37. Treatment should consist of

Explanation
Because the radiograph reveals an intermetatarsal angle of greater than 15 degrees and an incongruent metatarsophalangeal joint, the treatment of choice is a proximal first metatarsal osteotomy with distal soft-tissue realignment. A distal chevron procedure would not correct this degree of deformity. A Keller procedure is reserved for a less active elderly individual. Arthrodesis is appropriate for a patient with advanced arthritis of the metatarsophalangeal joint. The double osteotomy is reserved for the congruent metatarsophalangeal joint with hallux valgus. Coughlin MJ, Carlson RE: Treatment of hallux valgus with an increased distal metatarsal articular angle: Evaluation of double and triple first ray osteotomies. Foot Ankle Int 1999;20:762-770.
Question 553
High Yield
Figure 7 shows the radiograph of a 64-year-old man who has neck pain and weakness of the upper and lower extremities following a motor vehicle accident. Examination reveals 3/5 quadriceps and 4/5 hip flexors but no ankle dorsiflexion or plantar flexion. His intrinsics are 1/5, with finger flexors of 3/5. He is awake, alert, and cooperative. Management should consist of

Explanation
In patients with facet dislocations and an incomplete neurologic deficit, early decompression of the canal via reduction of the dislocation generally is considered safe if the patient is alert and can cooperate. However, patients who cannot cooperate with serial neurologic examinations during the reduction are at risk for increased deficit secondary to herniated nucleus pulposus, and MRI should be performed prior to either closed or open reduction. Star AM, Jones AA, Cotler JM, et al: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Question 554
High Yield
An 18-month-old child sustains a crush amputation of the tip of the index finger. Bone is exposed, but the nail is intact. Management should consist of

Explanation
Children have a much greater capacity to heal soft-tissue injuries than adults. Most crush or avulsion fingertip amputations in children, particularly those younger than age 2 years, can be treated with serial dressing changes, even with bone exposed. Das SK, Brown HG: Management of lost finger tips in children. Hand 1978;10:16-27.
Question 555
High Yield
The relocation test is most reliable for diagnosing anterior subluxation of the glenohumeral joint when
Explanation
The relocation test is most accurate when true apprehension is produced with the arm in combined abduction and external rotation and then relieved when posterior pressure is placed on the humeral head. Pain with this test is a less specific response and may occur with other shoulder disorders such as impingement.
Question 556
High Yield
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings?

Explanation
Treatment of shoulder instability with thermal devices has lead to numerous complications including recurrent instability, chondrolysis, stiffness, and capsular necrosis. This patient's findings are consistent with a heat-induced axillary nerve injury. Normal radiographs exclude extensive chondrolysis. Levine WN, Bigliani LU, Ahmad CS: Thermal capsulorrhaphy. Orthopedics 2004;27:823-826.
Question 557
High Yield
A 20-year-old patient has foot pain. A radiograph and T1-weighted MRI scan are shown in Figures 8a and 8b. A biopsy specimen is shown in Figure 8c. Treatment should consist of


Explanation
Giant cell tumors occur near articular surfaces in young adults. The histology shows abundant giant cells with nuclei resembling the surrounding cells. Although the MRI scan shows soft-tissue involvement, curettage is still the preferred treatment. Chemotherapy is not necessary for benign lesions, and amputation is too aggressive. Cementation, phenol, and cryosurgery (liquid nitrogen) are all acceptable local adjuvants to curettage. Packing the cavity with bone graft rather than cement is also acceptable. Dahlin DC, Unni KK: Bone Tumors: General Aspects and Data on 8,542 Cases. Springfield, IL, Charles C. Thomas, 1986.
Question 558
High Yield
A newborn girl with an isolated unilateral dislocatable hip is placed in a Pavlik harness with the hips flexed 100 degrees and at resting abduction. Figure 23 shows an ultrasound obtained 2 weeks later. What is the next step in management?
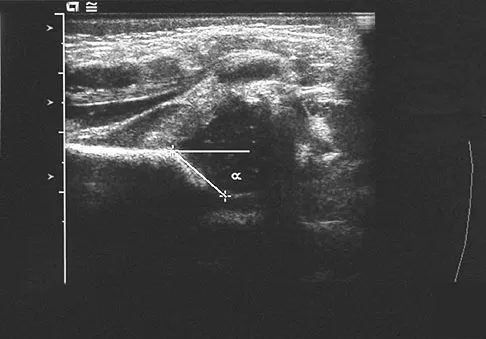
Explanation
The infant has a well-positioned hip in the Pavlik harness and treatment should be continued in the current position. The success rate is over 90% with the use of this device for a dislocatable hip. Ultrasound is a useful tool to confirm appropriate positioning of the cartilaginous femoral head during treatment. If the femoral head is not reduced after 2 to 3 weeks in the harness, this mode of treatment should be abandoned. Forceful extreme abduction can cause osteonecrosis of the femoral epiphysis and should be avoided. Closed reduction, arthrography, and spica casting are indicated if the hip cannot be maintained in a reduced position with the harness. Lehmann HP, Hinton R, Morello P, et al: Developmental dysplasia of the hip practice guideline: Technical report. Committee on Quality Improvement, and Subcommittee on Developmental Dysplasia of the Hip. Pediatrics 2000;105:E57.
Question 559
High Yield
A patient reports persistent anterior shoulder pain following a forceful external rotation injury to the shoulder. An MRI scan is shown in Figure 4. The patient remains symptomatic despite 3 months of nonsurgical management. Treatment should now consist of
Explanation
The MRI scan reveals a subscapularis tear with a biceps that is out of the groove. Treatment in this patient is most predictable if the subscapularis is repaired. The biceps should either be tenodesed or tenotomized since it is unstable. Recentering of the biceps has been found to be unpredictable. Treatment of these lesions has been shown to have better results if the biceps is either released or tenodesed. This prevents recurrent biceps symptoms that can be source of surgical failure. Edwards TB, Walch G, Sirvenaux F, et al: Repair of tears of the subscapularis: Surgical technique. J Bone Joint Surg Am 2006;88:1-10. Deutsch A, Altcheck DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 560
High Yield
Varus intertrochanteric osteotomy for coxa valga commonly produces which of the following results?
Explanation
The greater trochanter is raised as a by-product of varus osteotomy, and a temporary abductor lag and lurch is common for 6 months following surgery. In the absence of hip joint subluxation, varus intertrochanteric osteotomy has no effect on the center edge angle of Wiberg. Varus osteotomy typically increases femoral offset, thereby improving the abductor lever arm and reducing the hip joint reaction force. Even without taking a wedge, varus osteotomy always produces some degree of shortening.
Question 561
High Yield
The use of a screw between the clavicle and the coracoid process to maintain the clavicle and acromioclavicular (AC) joint in a reduced position is a treatment option for AC joint separations. Screw removal is generally recommended after soft-tissue healing. What effect does this rigid coracoclavicular fixation have on shoulder kinematics?
Explanation
This issue has been debated since Inman published his classic study on clavicular rotation in 1944. Subsequently, it has been shown by several authors that the clinical evaluation of patients with either coracoclavicular screws in place or with arthrodesis of the coracoclavicular reveals little to no loss of shoulder motion. This is most likely the result of synchronous motion of the scapula and clavicle in shoulder movements. Flatow EL: The biomechanics of the acromioclavicular, sternoclavicular, and scapulothoracic joints. Instr Course Lect 1993;42:237-245. Kenedy JC, Cameron H: Complete dislocation of the acromioclavicular joint. J Bone Joint Surg Br 1954;36:202-208. Rockwood CA Jr, Williams GR, Young CD: Disorders of the acromioclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 483-553.
Question 562
High Yield
Which of the following is considered a specific advantage of using COX-2 inhibitors over COX-1 inhibitors?
Explanation
Inflammation is mediated through two isoforms of cyclooxygenase that convert arachidonic acid to prostaglandins. Selectivity, but not specificity, is one of the unique characteristics of this process that has been able to provide more protection from the effects of gastric mucosal alterations using the COX-2 selective inhibitors. The use of COX-1 selective inhibitors is associated with side effects such as ulcerative conditions and platelet interference, both of which have been difficult to control in the past until the advent of the COX-2 inhibitors. PGE2 inhibition by COX-1 in the intestinal track can then be bypassed, thereby reducing ulceration complications associated with use of nonsteroidal anti-inflammatory drugs. Lane JM: Anti-inflammatory medications: Selective COX-2 inhibitors. J Am Acad Orthop Surg 2002;10:75-78. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002.
Question 563
High Yield
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?

Explanation
The radiograph reveals densities within the articular cartilage of the knee commonly referred to as chondrocalcinosis. The term chondrocalcinosis refers to the presence of calcium-containing crystals detected as radiodensities in cartilage. Calcium-containing crystals other than calcium pyrophosphate dihydrate may also deposit in articular cartilage and menisci, producing both radiographically detectable densities in cartilage and joint inflammation or degeneration. Hemochromatosis, alkaptonuria (ochronosis), and Wilson's disease are characterized by cellular deposition of iron, calcium, and copper ions, respectively, into various tissues including articular cartilage and can give this appearance. Septic arthritis does not usually cause chondrocalcinosis. Klippel JH (ed): Primer on the Rheumatic Diseases, ed 11. Atlanta, GA, Arthritis Foundation, 1997, pp 226-229 and 328-331.
Question 564
High Yield
Figures 32a and 32b show the radiographs of an active 13-year-old boy who has persistent left thigh pain and a limp despite a trial of protected weight bearing. Management should consist of


Explanation
The plain radiographs show an eccentric metaphyseal lesion involving a long bone in a skeletally immature patient. The lesion is longer than it is wide, with distinctly lobular outer edges that are sclerotic. These findings are characteristic of a nonossifying fibroma. Small asymptomatic lesions may be followed clinically. Larger lesions that occupy greater than two thirds of the width of the shaft and are located in areas of high mechanical stress such as the femur are more prone to fracture than smaller lesions. Pain is often a sign of impending fracture or the presence of a small fracture that may not be apparent on radiographs. The natural history of the lesion is to resolve over a period of years. The procedure that would allow the patient to return to contact sports is curettage and bone grafting. Intralesional steroid injection has been advocated in the treatment of unicameral bone cysts and eosinophilic granuloma but not nonossifying fibromas. En block resection is not indicated for a benign lesion. Low-dose radiation therapy has been used for eosinophilic granuloma but not for nonossifying fibromas. Walker RN, Green NE, Spindler KP: Stress fractures in skeletally immature patients. J Pediatr Orthop 1996;16:578-584.
Question 565
High Yield
The use of radiation therapy is most effective in metastatic bone disease from which of the following tumors?
Explanation
Both myeloma and lymphoma are more responsive to radiation therapy. The other types of tumors are relatively more resistant to radiation. Doses of 25 to 50 Gy (2,500 to 5,000 cGy) are usually sufficient for myeloma and lymphoma, while carcinomas frequently require a higher dosage. Large cell lymphoma of bone is usually of B-cell origin and is treated with chemotherapy and radiation therapy. Simon MA, Springfield DS, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 683.
Question 566
High Yield
A 14-year-old girl has a painful hallux valgus deformity that has not responded to shoe modifications. Figure 21 shows a standing AP radiograph. What is the most appropriate surgical procedure?

Explanation
The radiograph reveals an increased first-second intermetatarsal angle and a congruent metatarsophalangeal joint with an abnormal distal metatarsal articular angle. Correction of both of these abnormalities requires a proximal and distal first metatarsal osteotomy. Coughlin M: Juvenile bunions, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 297-339.
Question 567
High Yield
A 20-year-old football player has immediate pain in the midfoot and is unable to bear weight after an opposing player lands on the back of his plantar flexed foot. AP and lateral radiographs are shown in Figures 4a and 4b. Management should consist of


Explanation
The history and radiographs indicate a Lisfranc fracture-dislocation of the foot. The radiographs show the classic "fleck sign," which is an avulsion of the Lisfranc ligament from the base of the second metatarsal. Most authors recommend open reduction and internal fixation of this injury. Closed reduction can be attempted, but anatomic reduction is unlikely because of the interposed bone fragments and soft tissues. Standard radiographs are not reliable in identifying 1 to 2 mm of subluxation of the tarsometatarsal joint. The tarsometatarsal joint has a poor tolerance to even mild subluxation, and the resulting decrease in joint contact area increases the likelihood of posttraumatic arthritis. Open reduction with the joint visible allows more anatomic reduction and internal fixation of larger osteochondral fragments or excision of smaller interposed fragments. Bellabarba C, Sanders R: Dislocations of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, vol 2, pp 1539-1558.
Question 568
High Yield
In a locking plate screw construct, axial forces are borne by which of the following?
Explanation
In a traditional plate system, fracture security depends on the friction between the plate and the underlying bone. Bicortical fixation will decrease the toggle and improve stability. Locking plates absorb axial forces transmitted from the screws. Such plates do not require plate compression against the bone, thus preserving periosteal blood supply. Nana AD, Joshi A, Lichtman DM: Plating of the distal radius. J Am Acad Orthop Surg 2005;13:159-171.
Question 569
High Yield
A 45-year-old woman awakens with the acute onset of burning left shoulder pain that radiates toward the axilla. She denies any history of trauma. On examination, she is unable to abduct her arm but has full passive shoulder motion. Her sensation is intact. Cervical spine examination reveals full range of motion and a negative Spurling's test. Radiographs and MRI studies are normal for the cervical spine and shoulder. What is the most likely diagnosis?

Explanation
The definition of brachial neuritis or Parsonage-Turner syndrome is a rare disorder of unknown etiology that causes pain or weakness of the shoulder and upper extremity. The loss of active motion excludes cervical C6-7 radiculopathy and impingement. A normal MRI scan and full passive motion exclude a rotator cuff tear and adhesive capsulitis, respectively. Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
Question 570
High Yield
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?


Explanation
An increased density of the talar body compared to the distal tibia following fracture of the talar neck is highly suggestive of vascular compromise of the talar body. Subchondral osteopenia of the talus at 6 to 8 weeks (Hawkins sign) is a favorable sign but does not eliminate the possibility of osteonecrosis. Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Question 571
High Yield
Total hip arthroplasty in a patient with a long-standing hip fusion on the contralateral side is most likely to result in
Explanation
Contralateral total hip arthroplasty in patients with hip fusions results in a 40% higher rate of mechanical failure and loosening. During gait, motion of the contralateral hip is increased and more time is spent bearing weight on that hip. In patients with hip fusions, gait efficiency is only 53%, with a greater rate of oxygen consumption. Garvin KL, Pellicci PM, Windsor RE, et al: Contralateral total hip arthroplasty or ipsilateral total hip arthroplasty in patients who have long-standing fusion of the hip. J Bone Joint Surg Am 1989;71:1355-1362. Gore DR, Murray MP, et al: Walking patterns of men with unilateral surgical hip fusion. J Bone Joint Surg Am 1975;57:759-765.
Question 572
High Yield
Figure 12a shows the clinical photograph of a 36-year-old man who has left shoulder pain and dysfunction after undergoing a lymph node biopsy 2 years ago. The appearance of the shoulder during abduction and a wall push-up maneuver is shown in Figures 12b and 12c, respectively. Which of the following procedures provides the best pain relief and function?



Explanation
Injury to the spinal accessory nerve can occur after penetrating trauma to the shoulder. Blunt trauma may also cause loss of trapezius function. Most commonly, surgical dissection in the posterior triangle of the neck, such as lymph node biopsy, may expose the nerve to possible damage. Surgical repair of the nerve may be considered up to 1 year after injury; after this time muscle transfer is usually associated with a better functional outcome. Steinman SP, Spinner RJ: Nerve problems in the shoulder, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1013-1015.
Question 573
High Yield
In a patient who has rheumatoid arthritis with acetabular protrusion, what is the best biomechanical position for the cup with respect to the preoperative center of rotation?

Explanation
Acetabular protrusion in patients with rheumatoid arthritis moves the center of hip rotation medially and posteriorly. Positioning of the acetabular component in a patient with protrusion is best accomplished in the normal (anterior and inferior) position and not in a protruded position. This has been shown both clinically and in a finite-element analysis. Any medial positioning will produce impingement of the prosthesis neck on the rim, and superior placement produces improper hip mechanics. Crowninshield RD, Brand RA, Pedersen DR: A stress analysis of acetabular reconstruction in protrusio acetabuli. J Bone Joint Surg Am 1983;65:495-499.
Question 574
High Yield
Figures 36a and 36b show the radiographs of a 48-year-old woman who smokes cigarettes and sustained a segmental femoral shaft fracture in a motor vehicle accident 9 months ago. Initial management consisted of stabilization with a reamed statically locked intramedullary nail. She now reports lower leg pain that increases with activity. In addition to advising the patient to quit smoking, management should include


Explanation
The patient has an oligotrophic nonunion of the distal femoral fracture. Although the proximal fracture appears incompletely united, it was stable at exchange nailing. The treatment of choice is exchange reamed nailing to at least 2 mm above the nail in place. Bone grafting is debatable. Recent studies have shown a 70% to 75% success rate with exchange nailing only, so in nonhypertrophic nonunions, bone grafting can be considered. Nonsurgical management consisting of observation or external stimulation runs the risk of implant failure. Plate fixation is acceptable but is considered a second choice because of the need to consider stabilization of the proximal fracture until union is achieved. Also, plate fixation definitely requires bone grafting. Webb LX, Winquist RA, Hansen ST: Intramedullary nailing and reaming for delayed union or nonunion of the femoral shaft: A report of 105 consecutive cases. Clin Orthop 1986;212:133-141. Weresh MJ, Hakanson R, Stover MD, et al: Failure of exchange reamed intramedullary nailing for ununited femoral shaft fractures. J Orthop Trauma 2000;14:335-338.
Question 575
High Yield
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
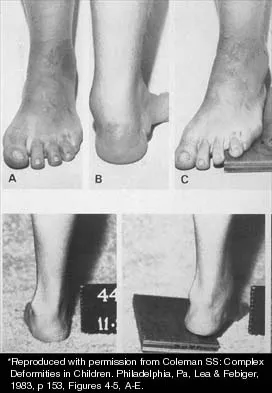
Explanation
The clinical photographs show a patient with a type I hereditary sensory motor neuropathy who has cavus feet with a flexible hindfoot. The Coleman block test shows that the hindfoot corrects into valgus. To prevent progressive cavus, patients with this condition may benefit from soft-tissue releases at a younger age while the foot is flexible. Once there is fixed deformity, combined soft-tissue and bone procedures usually are necessary. Metatarsal osteotomies will correct the cavus, but will do nothing for the drop foot. Transfer of the extensor hallucis longus to the neck of the first metatarsal and modified transfer of the extensor digitorum longus to the dorsum of the foot will prevent further claw toes and improve foot dorsiflexion. Anterior transfer of the posterior tibialis tendon will also aid in dorsiflexion. Calcaneal osteotomy should be reserved for fixed hindfoot varus that does not correct with block testing, and triple arthrodesis should be avoided as long as possible because the long-term outcome is poor. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245. Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Question 576
High Yield
A 67-year-old woman is seen in the emergency department after falling at home. Radiographs before and after treatment are shown in Figures 49a and 49b, respectively. Which of the following best explains the 8-week postinjury clinical findings seen in Figure 49c?



Explanation
Patients older than age 40 years at the time of initial anterior dislocation have low rates of redislocation; however, 15% of these patients experience a rotator cuff tear. Moreover, there is a dramatic increase (up to 40%) in the incidence of rotator cuff tears in patients older than age 60 years. Axillary nerve injury may occur but is less common than rotator cuff tear. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 273-284.
Question 577
High Yield
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for

Explanation
Flexion contractures are the most common complication of elbow dislocations. About 15% of patients lose more than 30 degrees of flexion. The risk of contracture is proportional to the duration of immobilization. Elbows should be moved within the first few days after reduction. The splinting is for comfort and protection only while the pain subsides. Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249. Linscheid RL, O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452. O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Question 578
High Yield
A 22-year-old skier reports painful range of motion in the left thumb after falling forward on his outstretched hand while holding his ski pole. Examination of the left thumb reveals increased AP laxity and 45 degrees of valgus laxity at the metacarpophalangeal (MCP) joint. Examination of the right thumb shows 25 degrees of valgus laxity at the MCP joint. Radiographs are normal. Management should consist of
Explanation
The patient has a complete tear of the ulnar collateral ligament as defined by MCP joint laxity of greater than 30 degrees (or 15 degrees greater laxity compared with the opposite side). Primary repair is the treatment of choice because displacement of the ligament superficial to the adductor aponeurosis (Stener lesion) must be corrected. Any volar plate injury can be addressed during repair of the ulnar collateral ligament.
Question 579
High Yield
Which of the following is considered an advantage of arthroscopic distal clavicle excision compared with open distal clavicle excision?

Explanation
Arthroscopic versus open distal clavicle excision has the advantage of allowing evaluation of the glenohumeral joint arthroscopically prior to moving into the subclavicular and subacromial space to perform the distal clavicle excision. This can be of value in both confirming the diagnosis as well as avoiding diagnostic errors. Berg and Ciullo showed that in 20 patients who underwent open distal clavicle excision that resulted in failure, 15 of those patients had a superior labral anterior posterior (SLAP) lesion. Of these 15 patients who had the lesion treated surgically, 9 went on to a good to excellent result after the surgery was performed arthroscopically. Fewer complications, lower infection rate, and decreased surgical time have not been documented in the literature. Arthroscopic technique sacrifices the inferior acromioclavicular ligament and preserves the superior acromioclavicular ligament. Berg EE, Ciullo JV: The SLAP lesion: A cause of failure after distal clavicle resection. Arthroscopy 1997;13:85-89.
Question 580
High Yield
A 15-year-old high school soccer player collides with an opponent and is unconscious when the trainer arrives on the field. He is conscious within 15 seconds, breathing appropriately, and denies any headache, neck pain, or nausea. It is his first head injury. Provided that the athlete is free of symptoms, when should he be allowed to return to athletic activity?

Explanation
The loss of consciousness indicates a grade 2 concussion, which necessitates a 4-week period out of sport. The last week prior to return must be symptom-free and the athlete should not have symptoms in practice. Cantu RC: Return to play guidelines after a head injury. Clin Sports Med 1998;17:45-60.
Question 581
High Yield
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
Explanation
According to Morgan and associates, a type II SLAP lesion can create or is associated with a superior instability pattern. They suggest that this can exist without a co-existing anteroinferior instability pattern. They reported that repair of the SLAP lesion alone resulted in satisfactory outcomes in 90% of patients and a return to throwing in more than 90% of pitchers. The arthroscopic findings in this patient do not support a diagnosis of anteroinferior laxity or instability; therefore, thermal capsular shift or capsular placation is not necessary. Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565. Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Question 582
High Yield
A 30-year-old patient has wrist pain. A radiograph and biopsy specimen are shown in Figures 34a and 34b. What is the most likely diagnosis?

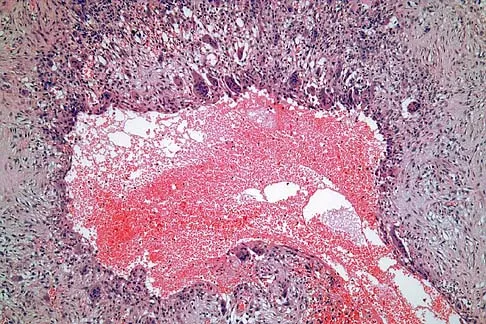
Explanation
Aneurysmal bone cysts typically present as radiolucent lesions with an expansile remodeled cortex. The histologic appearance consists of blood-filled lakes surrounded by a benign lining that contains fibroblasts, giant cells, and hemosiderin. Although the other lesions are in the radiographic differential diagnosis, these histologic findings indicate an aneurysmal bone cyst. Bieselker JL, Marcove RC, Huvos AG, Mike V: Aneurysmal bone cyst: A Clinico-pathologic study of 66 cases. Cancer 1973;26:615.
Question 583
High Yield
Which of the following structures is the most important restraint to posterior subluxation of the glenohumeral joint when positioned in 90 degrees of flexion and internal rotation?
Explanation
The posterior band of the inferior glenohumeral ligament is the most important restraint to posterior subluxation of the glenohumeral ligament with the shoulder in 90 degrees of flexion and internal rotation. With the shoulder in external rotation, the subscapularis is an important stabilizer to posterior subluxation. When the shoulder is in neutral rotation, the coracohumeral ligament is the primary stabilizer. The middle glenohumeral ligament functions primarily to resist anterior translation of the shoulder in the midrange of abduction. The supraspinatus muscle and tendon have relatively little contribution to anterior and posterior translation of the glenohumeral joint. Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML: Posterior glenohumeral subluxation: Active and passive stabilization in a biomechanical model. J Bone Joint Surg Am 1997;79:433-440.
Question 584
High Yield
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
Alternative bearing surfaces in THA have received much attention in recent years as more and more hip arthroplasties are being performed on younger patients with hip arthritis. The two most popular nonmetal-on-polyethylene bearing surfaces are metal-on-metal and ceramic-on-ceramic. There are arguments supporting the use of either, but ceramic bearings have been shown to have a theoretic increased risk of fracture compared with cobalt-chromium. This has been shown to be clinically relevant with zirconium ceramics. Newer alumina ceramics are being produced with lower porosity and grain size and with higher density and purity, resulting in lower fracture risk but still greater than that of cobalt-chromium. Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
Question 585
High Yield
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?


Explanation
While difficult to appreciate on the AP radiograph of the shoulder, the increased physeal signal demonstrated on the axial MRI scan is consistent with a nondisplaced growth plate fracture. A comparison radiograph of the left shoulder also could be considered and the injured shoulder evaluated for physeal widening. Proximal humeral fractures in children are somewhat unusual, representing less than 1% of all fractures seen in children and only 3% to 6% of all epiphyseal fractures. Physeal injuries are classified according to the Salter-Harris classification scheme. Salter-Harris type I fractures represent approximately 25% of physeal injuries to the proximal humerus in adolescents. The proximal humeral physis is responsible for 80% of the longitudinal growth of the humerus; therefore, there is tremendous potential for remodeling of fractures in this region. Management for nondisplaced Salter-Harris type I fractures is limited to a short period of immobilization followed by a gradual return to activities as clinical symptoms resolve. Curtis RJ, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 991-1007.
Question 586
High Yield
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury. Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Question 587
High Yield
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?


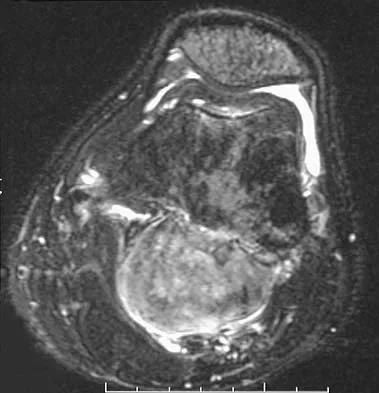
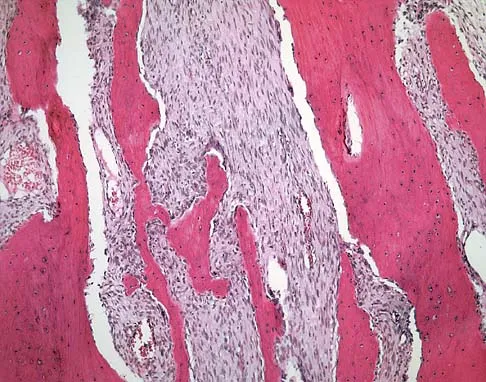
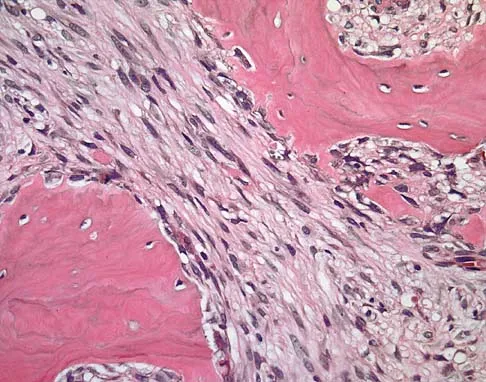
Explanation
The patient has parosteal osteosarcoma. The posterior aspect of the distal femur is the typical location for this variant of osteogenic sarcoma. The imaging studies indicate a surface lesion with no involvement of the adjacent intramedullary canal. The histologic appearance is that of a low-grade fibroblastic osteosarcoma, consisting of relatively mature bone and a bland fibroblastic stroma lacking cytologic atypia and mitotic activity. A cartilaginous component is also frequently seen. Classic osteosarcoma typically has a more aggressive radiologic and histologic appearance. Sessile osteochondromas, while common behind the knee, have a presence of hematopoietic marrow and fat. The cartilage found in the associated cartilaginous cap is oriented. Chondrosarcomas are more typical in an older age group and have a histologic pattern consisting of malignant chondroid. Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
Question 588
High Yield
Following a radial nerve neurapraxia at or above the elbow, return of muscle function can be expected to start at the brachioradialis and return along which of the following progressions?

Explanation
Following a radial nerve neurapraxia above the elbow, muscle recovery can be expected in a predictable pattern. Although variations will occur, the return of function or reinnervation usually occurs in the following order: brachioradialis, extensor carpi radialis longus, supinator, extensor carpi radialis brevis, extensor carpi ulnaris, extensor digitorum comminus, extensor digiti minimi, extensor indicis proprious, extensor pollicis longus, abductor pollicis longus, and extensor pollicis brevis. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System. Part 1, Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy, 1991, vol 8, p 53.
Question 589
High Yield
A 45-year-old woman has had progressive right shoulder pain for the past 6 months. She notes that the pain disrupts her sleep, she has pain at rest that requires the use of narcotic analgesics, and she has limited use of her left shoulder for most activities of daily living. History reveals the use of corticosteroids for systemic lupus erythematosus. Examination shows diminished range of motion. Radiographs of the right shoulder are shown in Figures 4a and 4b. Treatment should consist of


Explanation
Humeral arthroplasty provides excellent pain relief and function for stage IV osteonecrosis with humeral collapse. In late disease with glenoid involvement (stage V), total shoulder arthroplasty is preferred. Some authors have reported satisfactory results with core decompression of the humeral head for early stages of osteonecrosis, but results for stage IV osteonecrosis are less satisfactory when compared with those for humeral arthroplasty. Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. LePorte DM, Mont MA, Mohan V, Pierre-Jacques H, Jones LC, Hungerford DS: Osteonecrosis of the humeral head treated by core decompression. Clin Orthop 1998;355:254-260.
Question 590
High Yield
A 25-year-old semiprofessional football player sustains a hyperextension injury to the left foot. He is unable to bear weight. Examination reveals tenderness along the midfoot with swelling and plantar ecchymosis. Radiographs are negative. What is the next step in evaluation of this patient?

Explanation
The patient has a suspected Lisfranc sprain based on the plantar ecchymosis. The first step in diagnosis is a dynamic radiographic study. This should include a physician-assisted midfoot stress examination or standing weight-bearing radiographs to evaluate for displacement. There is no evidence of compartment syndrome, and a bone scan, CT, and MRI are expensive tests that are not warranted. Early JS: Fractures and dislocations of the midfoot and forefoot, in Bucholz R, Heckman JD, Court-Brown CM (eds): Rockwood and Green's Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, pp 2337-2400.
Question 591
High Yield
When considering a flexor digitorum longus tendon transfer as part of the surgical treatment in patients with symptomatic flatfoot deformity caused by posterior tibial tendon insufficiency, which of the following patients is the most appropriate candidate?
Explanation
Transfer of the flexor digitorum longus tendon is a common technique combined with other procedures to treat patients with posterior tibial tendon insufficiency. However, it is contraindicated in patients with a fixed hindfoot deformity, hypermobility, or neuromuscular compromise. It is relatively contraindicated in patients who are obese, and those older than age 60 to 70 years. Pedowitz WJ, Kovatis P: Flatfoot in the adult. J Am Acad Orthop Surg 1995;3:293-302.
Question 592
High Yield
When compared with cobalt-chromium and stainless steel implants, a titanium implant has what biomechanical properties?
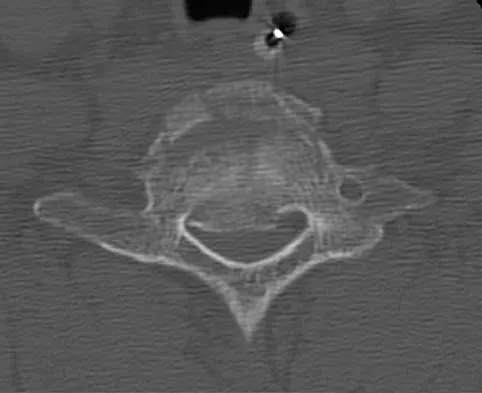
Explanation
Titanium implants are commonly used in spinal surgery, especially when MRI may be needed after implantation. Titanium implants have a lower modulus of elasticity when compared with cobalt-chromium and stainless steel implants. This is felt to allow less stress shielding for these types of implants. The other properties do not apply to titanium implants.
Question 593
High Yield
A 45-year-old recreational tennis player underwent arthroscopic decompression and mini-open repair of a small supraspinatus tendon tear 3 weeks ago after nonsurgical management failed to provide relief. He now has pain, swelling about the wound, erythema, and purulent drainage. The patient is returned to the operating room for irrigation, debridement, and cultures. What is the most common organism causing this infection?

Explanation
In a large series of mini-open rotator cuff repairs, an infection rate of at least 2% was found, with the majority of the infections caused by Propionibacterium acnes. To prevent this complication, the shoulder should be re-prepped before the mini-open incision is made to prevent bacterial contamination from the arthroscopic procedure. Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 594
High Yield
Following ankle arthroscopy performed through a posterolateral portal, a patient notes numbness on the lateral half of the heel pad of the foot. What is the most likely injured structure?
Explanation
The lateral calcaneal nerve is a branch of the sural nerve that runs along the lateral border of the Achilles tendon to innervate the lateral heel pad. Ankle arthroscopy involves posterior portals that hug the Achilles tendon to avoid the main trunks of the sural nerve and tibial nerve; however, the lateral calcaneal branch remains potentially vulnerable. The first branch of the lateral plantar nerve is actually a medial structure that partially innervates the plantar fascia and the abductor digiti quinti. The deep peroneal nerve is anterior to the ankle. Sitler DF, Amendola A, Bailey CS, et al: Posterior ankle arthroscopy: An anatomic study. J Bone Joint Surg Am 2002;84:763-769.
Question 595
High Yield
A 23-year-old man sustained an injury to his left foot when a forklift rolled over it at work. Examination reveals marked swelling of the midfoot and forefoot, with tenderness to palpation over the medial hindfoot and dorsomedial forefoot. The distal dorsalis pedis pulse is audible on Doppler examination, and his sensation is intact to touch. Radiographs are shown in Figures 33a and 33b. Management should consist of


Explanation
The best results after dislocations of the tarsometatarsal joints are seen with anatomic reduction; this is best achieved by open reduction and maintained with internal fixation with either pins or screws. Open reduction provides a means of debriding small bony fragments from the joint and allowing direct inspection of the reduction. Associated crush or shearing fractures of the cuboid or tarsal navicula are signs that suggest a Lisfranc injury. Because patients can function quite well despite the development of arthrosis in the Lisfranc joint, primary arthrodesis is not indicated in the management of this injury. Resch S, Stenstrom A: The treatment of tarsometatarsal injuries. Foot Ankle 1990;11:117-123. Schenck RC Jr, Heckman JD: Fractures and dislocations of the forefoot: Operative and nonoperative treatment. J Am Acad Orthop Surg 1995;3:70-78.
Question 596
High Yield
Immediately after undergoing lumbar instrumentation, a patient reports severe right leg pain and has 4+/5 weakness. Figure 24 shows an axial CT scan of L5. Exploratory surgery will most likely reveal
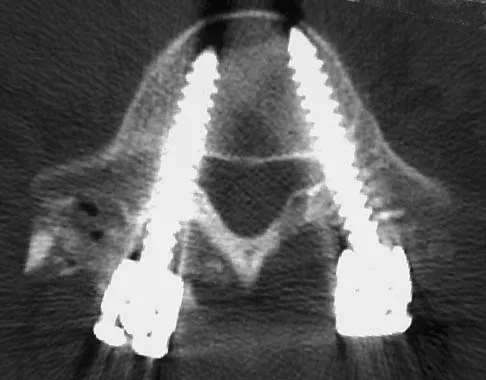
Explanation
The most common finding at exploration of an inappropriately placed pedicle screw is displacement of the nerve. Pedicle breach is common, ranging from 2% to 20%, but most are asymptomatic. All of the choices are possible, but in a large series conducted by Lonstein and associates, the authors reported that displacement of the root, most often medial, was the most common finding. Laceration, contusion, or transfixion usually was not seen. Spinal fluid leakage occurs less frequently and is not expected in the minimal broach illustrated. Esses SI, Sachs BL, Dreyzin V: Complications associated with the technique of pedicle screw fixation: A selected survey of ABS members. Spine 1993;18:2231-2238. Laine T, Lund T, Ylikoski M, et al: Accuracy of pedicle screw insertion with and without computer assistance: A randomised controlled clinical study in 100 consecutive patients. Eur Spine J 2000;9:235-240.
Question 597
High Yield
What artery provides the only direct vascularizaton to both the intraneural and extraneural blood supply of the ulnar nerve just proximal to the cubital tunnel?
Explanation
The superior ulnar collateral, inferior ulnar collateral, and posterior ulnar recurrent arteries provide consistent vascular supply to the ulnar nerve. This supply is segmental in nature. No identifiable direct anastomosis is seen between the superior ulnar collateral and the posterior ulnar recurrent arteries. The inferior ulnar collateral artery provides the only direct vascularization to the nerve and is located in the region just proximal to the cubital tunnel. The segmental nature of the blood supply to the ulnar nerve underscores the importance of its preservation during transposition.
Question 598
High Yield
The attachments of the transverse carpal ligament include which of the following structures?

Explanation
The transverse carpal ligament is the volar boundary of the carpal tunnel. It attaches to the scaphoid and trapezium radially and the pisiform and the hook of the hamate ulnarly. The ulna and trapezoid do not receive attachments of the transverse carpal ligament. Hollinshead W: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, vol 3, pp 471-472.
Question 599
High Yield
Figure 39 shows the sagittal T1-weighted MRI scan of a 27-year-old man who twisted his knee 2 weeks ago. The arrow is pointing to

Explanation
The arrow identifies a transverse dark line that represents primary trabeculae of the physeal scar. A similar finding is seen in the proximal tibia. These lines may persist indefinitely. They do not represent ongoing growth, an abnormally open physeal plate, a stress fracture, or Looser's line (fatigue fracture in osteomalacia).
Question 600
High Yield
Figures 20a and 20b show lateral and AP radiographs of a 49-year-old man who sustained a gunshot wound through the left shoulder. He reports neck pain and examination reveals weakness in all four extremities. What is the priority of evaluation?


Explanation
The projectile entered the left shoulder and traveled to the right neck; therefore, a high incidence of suspicion must be directed to the airway, great vessels of the neck, and contents of the mediastinum. Immediate assessment of airway, breathing, and circulation takes priority, followed by examination of the neurologic status and other systems, as determined by the examination findings. Subcommittee on ATLS of the American College of Surgeons Committee on Trauma 1993-1997, Spine and Spinal Cord Trauma; Advanced Trauma Life Support Student Manual, ed 6, 1997. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association and International Medical Society of Paraplegia (ASIA/IMSOP).
