HY 2026
00:00
Start Quiz
Question 401
High Yield
Figure 26 shows the clinical photograph of a patient who has developed a residual limb ulcer following a traumatic transtibial amputation 2 years ago. What is the preferred treatment to resolve the ulcer?

Explanation
The first step in the treatment of an amputation residual limb (stump) ulcer is local wound care and adjustment of the residual limb-prosthetic interface, as well as adjusting prosthetic alignment. Surgical revision should be undertaken only when prosthetic modification is unsuccessful. Murnaghan JJ, Bowker JH: Musculoskeletal complications, in Smith DG, Michael JW, Bowker JH (eds): Atlas of Amputations and Limb Deficiencies, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 683-700.
Question 402
High Yield
Mutations of what gene are associated with subsequent development of osteosarcoma?
Explanation
The mutation of the retinoblastoma gene has been associated with an increased prevalence of osteosarcoma. The mutation resulting in EWS-FLI1 is associated with Ewing's sarcoma. The other mutations are associated with tumor formation and proliferation but not necessarily with osteosarcoma formation. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 4. Scholz R, Kabisch H, Delling G, Winkler K: Homozygous deletion within the retinoblastoma gene in a native osteosarcoma specimen of a patient cured of a retinoblastoma of both eyes. Pediatr Hematol Oncol 1990;72:65.
Question 403
High Yield
Following an acute dislocation of the patella, the risk of a recurrent dislocation is greater if the patient has which of the following findings?

Explanation
Recurrent dislocations may follow an earlier dislocation. One study found that in patients who had a patellar dislocation between the ages of 11 to 14 years, 60% had a recurrent dislocation. The incidence of recurrent dislocation dropped to 33% in patients who had a patellar dislocation between the ages of 15 to 18 years. The authors also found that the incidence of recurrence was greater in patients who demonstrated a predisposition to dislocation as determined by evaluation of the unaffected knee. Predisposing signs included passive lateral hypermobility of the patella, a dysplastic distal third of the vastus medialis obliquis muscle, and a high and/or lateral position of the patella. A second study found that the risk of redislocation was considerably higher in patients who were in their teens at the first episode of dislocation compared to older patients. There are no studies linking either a patella baja or a bipartite patella to an increased risk of redislocation. Cash JD, Hughston JC: Treatment of acute patellar dislocation. Am J Sports Med 1988;16:244-249.
Question 404
High Yield
An 18-year-old man recently underwent an uncomplicated arthroscopic partial medial meniscectomy that was complicated by reflex sympathetic dystrophy (RSD), also termed "sympathetically maintained pain" (SMP). What is the most common finding of this condition?

Explanation
The hallmark for RSD or SMP is the presence of pain that is out of proportion to that expected for the degree of the injury. SMP often extends well beyond the involved area and is present in a nonanatomic distribution. The pain is frequently described as a burning sensation, with extreme sensitivity to light touch. Joint stiffness can be present but is a nonspecific finding. There may be cold intolerance, but this is not a cardinal symptom. Sweating actually may be increased. Osteopenia, if present, is a late finding. Lindenfeld TN, Bach BR Jr, Wojtys EM: Reflex sympathetic dystrophy and pain dysfunction in the lower extremity. Instr Course Lect 1997;46:261-268.
Question 405
High Yield
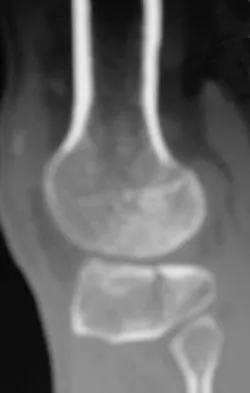
A 45-year-old male karate instructor sustained the injury shown in Figures 40a through 40c while practicing karate. The decision to proceed with surgery depends on which of the following factors?


Explanation
The most important criteria in determining the need for surgery following a nondisplaced or minimally displaced tibial plateau fracture is knee stability to varus/valgus stress. Soft-tissue injury noted on MRI may be addressed at a later time following fracture healing. This fracture pattern is amenable to nonsurgical management. Decisions regarding surgical intervention may be made up to 2 weeks after injury.
Question 406
High Yield
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
Significant elevation of the erythrocyte sedimentation rate in a patient with a painful hip arthroplasty mandates a complete work-up for infection prior to considering revision surgery. Reproducibility and reliability of ultrasonography as a diagnostic test still needs clarification. Aspiration is the easiest and most cost-effective test and should be performed prior to nuclear imaging. The latter is most valuable if the results are negative, strongly predicting the absence of infection. Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
Question 407
High Yield
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?

Explanation
The child has a near complete central physeal arrest of the distal femur and worsening limb-length discrepancy will develop. She is growing at the average rate for the population. The distal femoral physis grows at a rate of roughly 9 mm per year. Girls finish their growth at approximately age 14 years. Thus, at maturity the left leg will be 6.4 cm longer than the right. An angular deformity has not developed at this point and her arrest is central; therefore, angular deformity is unlikely to develop in any plane. Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Question 408
High Yield
What is the most prevalent adverse event associated with allogeneic blood transfusion?

Explanation
Clerical error leading to acute hemolysis and even death occurs in 1:12,000 to 1:50,000 transfusions. Bacterial contamination leading to sepsis/shock occurs in 1:1 million transfusions. HIV transmission is approximately 1:500,000 transfusions and hepatitis C is 1:103,000 transfusions. Anaphylactic reactions occur in 1:150,000 transfusions. Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Question 409
High Yield
In patients with neurofibromatosis, what is the most important sign of impending rapid progression of a spinal deformity?
Explanation
Neurofibromatosis can progress very rapidly. Rib penciling is the only singular prognostic factor. Significant progression has been observed in 87% of the curves with three or more penciled ribs. The other factors are often present but do not have a high correlation with rapid, severe progression. Crawford AH, Schorry EK: Neurofibromatosis in children: The role of the orthopaedist. J Am Acad Orthop Surg 1999;7:217-230.
Question 410
High Yield
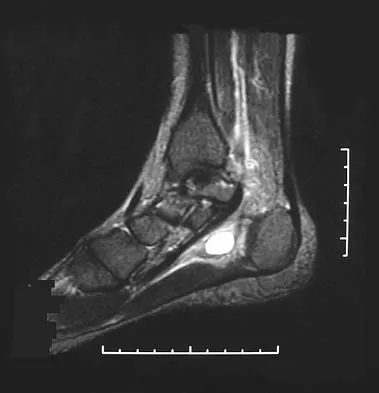
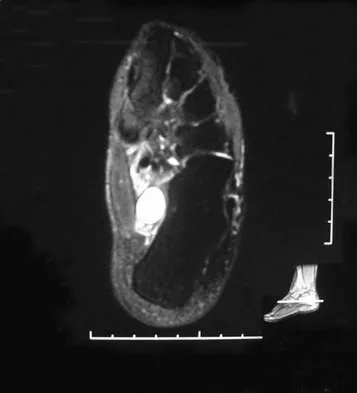
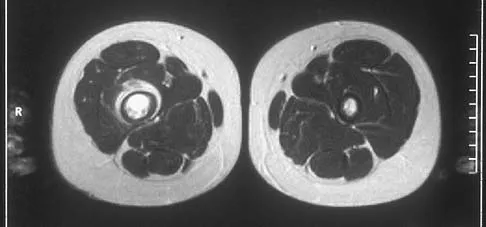
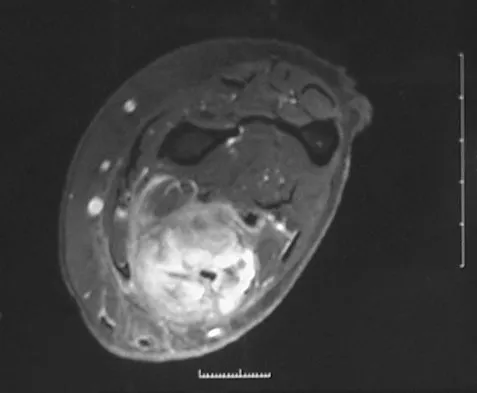
A 37-year-old woman has had intermittent paresthesias and numbness in the plantar foot for the past 6 months. She reports that the symptoms are worse with activity, and the paresthesias are beginning to awaken her at night. MRI scans are shown in Figures 6a and 6b. What is the most likely diagnosis?
Explanation
The symptoms are consistent with tarsal tunnel syndrome. Ganglion cysts are a well-known cause of tarsal tunnel syndrome. The MRI scans show a high intensity, well-circumscribed mass in the tarsal tunnel that is consistent with a fluid-filled cyst. Patients usually respond well to excision of the ganglion and resolution of the tarsal tunnel symptoms. The surrounding fat is a different signal intensity on the MRI scans, which rules out a lipoma. Synovial cell sarcoma has a heterogeneous appearance on an MRI scan. Metastatic tumors are most commonly found in the osseous structures of the foot, not the soft tissues. Rozbruch SR, Chang V, Bohne WH, et al: Ganglion cysts of the lower extremity: An analysis of 54 cases and review of the literature. Orthopedics 1998;21:141-148. Llauger J, Palmer J, Monill JM, et al: MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics 1998;18:1481-1498.
Question 411
High Yield
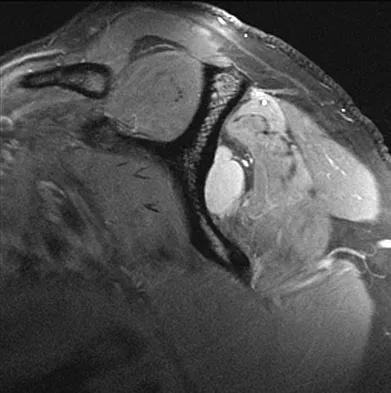
A 62-year-old man with a long history of right shoulder pain and weakness is scheduled to undergo hemiarthroplasty. Based on the radiographs shown in Figures 6a through 6c, what preoperative factor will most affect postoperative functional outcome?



Explanation
The radiographs reveal osteoarthritis and proximal humeral head migration. Integrity of the rotator cuff must be questioned based on these radiographic changes. The status of the rotator cuff is the most influential factor affecting postoperative function in shoulder hemiarthroplasty. The coracoacromial ligament provides a barrier to humeral head proximal migration in the face of a rotator cuff tear. The radiographs do not indicate significant humeral head or glenoid erosion. Acromioclavicular arthritis is often asymptomatic. Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Question 412
High Yield
An 18-month-old boy has 45 degrees of kyphosis in the thoracolumbar spine secondary to type I congenital kyphosis. Examination reveals that he is neurologically intact, and an MRI scan shows no evidence of intraspinal pathology. Management should consist of

Explanation
Surgery is indicated for congenital kyphosis once the deformity reaches a certain size or if significant progression is documented. In a young patient with a relatively small deformity, the treatment of choice is isolated in situ posterior fusion and postoperative immobilization. If an adequate posterior fusion can be obtained, an epiphyseodesis effect can be generated, allowing the remaining anterior growth to cause some correction. Because there is no evidence of neurologic compression and the deformity is less than 50 degrees, anterior surgery is not indicated. There is no role for bracing in the management of congenital kyphosis. Winter RB: Congenital Deformities of the Spine. New York, NY, Thieme-Stratton, 1983, pp 229-261.
Question 413
High Yield
Figures 40a and 40b show the pre- and postoperative radiographs of an 82-year-old woman with bilateral hip pain who has had staged total hip arthroplasties. To minimize potential injury to the sciatic nerve at the time of surgery, the surgeon should


Explanation
To improve hip biomechanics and secure more suitable bone for acetabular fixation, the true acetabulum is often resurfaced in patients who have developmental dysplasia of the hip, thus lowering the hip center and lengthening the leg. Acute lengthening of more than 3 cm will place excessive tension on the sciatic nerve and require a femoral shortening to avoid sciatic nerve injury. The other maneuvers will not relieve sciatic nerve tension because of limb lengthening. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 430-431.
Question 414
High Yield
Figure 7 shows the radiograph of an 18-year-old hockey player who sustained a shoulder injury during a fall into the side boards. Examination reveals a significant prominence at the acromioclavicular joint. Management should consist of

Explanation
The radiograph shows a type V acromioclavicular separation with greater than 100% superior elevation of the clavicle. This finding implies detachment of the deltoid and trapezius from the distal clavicle. Because of severe compromise of function and potential compromise to the overlying skin, surgery is the treatment of choice for type V acromioclavicular separations. During reduction and repair, meticulous repair of the deltotrapezial fascia will also aid in securing the repair. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 415
High Yield
A 42-year-old athletic trainer has a persistent popping sensation about the lateral ankle associated with weakness and pain following a remote injury. Deficiency in what structure directly leads to this pathology?

Explanation
The patient has instability of the peroneal tendon. The superior peroneal retinaculum is the primary retaining structure preventing peroneal subluxation. It is a thickening of fascia that arises off the posterior margin of the distal 1 to 2 cm of the fibula and runs posteriorly to blend with the Achilles tendon sheath. The inferior peroneal retinaculum attaches to the peroneal tubercle of the calcaneus and is not involved in this pathology. A deficient groove in the posterior distal fibula may also be a contributing factor in the development of the condition.
Question 416
High Yield
What is the primary reason for including the ilium in the distal fixation of long instrumentation constructs in adult scoliosis?

Explanation
Studies have shown that when compared with fixation to the sacrum alone, the success rate of fusion across the lumbosacral junction increases when both the sacrum and ilium are included in the posterolateral construct. Curve correction, coronal balance, and pelvic balance are all attended to within the thoracolumbar spine and are not directly related to the pelvic fixation. Fretting and corrosion are a byproduct of metal-to-metal connections. Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.
Question 417
High Yield
A 5-year-old boy sustained an elbow injury. Examination in the emergency department reveals that he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. The radial pulse is palpable at the wrist, and sensation is normal throughout the hand. Radiographs are shown in Figures 6a and 6b. In addition to reduction and pinning of the fracture, initial treatment should include


Explanation
The findings are consistent with a neurapraxia of the anterior interosseous branch of the median nerve. This is the most common nerve palsy seen with supracondylar humerus fractures, followed closely by radial nerve palsy. Nearly all cases of neurapraxia following supracondylar humerus fractures resolve spontaneously, and therefore, further diagnostic studies and surgery are not indicated. Cramer KE, Green NE, Devito DP: Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-505.
Question 418
High Yield
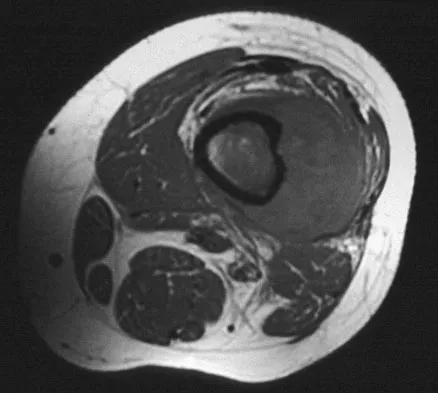
A 54-year-old woman sustained an elbow injury 3 months ago that was treated with open reduction and internal fixation. She now reports pain and limited elbow motion. Radiographs are shown in Figures 10a and 10b. Treatment should now consist of


Explanation
Radiographs reveal malunion of a Monteggia fracture-dislocation. Dislocation of the posterior radial head is caused by the malunited ulnar fracture. The deformity includes shortening with an apex posterior angulation. In the acute setting, open reduction of the radial head rarely is necessary; however, in chronic dislocations, open reduction is required. Without ulnar osteotomy, recurrent radial head dislocation is likely.
Question 419
High Yield
If a surgeon inadvertently burrs through the midlateral wall of C5 during a anterior corpectomy, what structure is at greatest risk for injury?
Explanation
The vertebral artery is contained within the vertebral foramen and thus tethered alongside the vertebral body, making it vulnerable to injury if a drill penetrates the lateral wall. The C5 root passes over the C5 pedicle and is not in the vicinity. The C6 root passes under the C5 pedicle but is posterior to the vertebral artery and is only vulnerable at the very posterior-inferior corner. The carotid artery and the vagus nerve are both within the carotid sheath and well anterior. Pfeifer BA, Freidberg SR, Jewell ER: Repair of injured vertebral artery in anterior cervical procedures. Spine 1994;19:1471-1474.
Question 420
High Yield
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should consist of

Explanation
Rupture of the pectoralis major tendon most commonly occurs during bench pressing. Wolfe and associates have shown that the most inferiorly located fibers of the sternal head lengthen disproportionately during the final 30 degrees of humeral extension during the bench press. This creates a mechanical disadvantage in the final portion of the eccentric phase of the lift; with forceful flexion of the shoulder these maximally stretched fibers may rupture. In most patients, particularly in young athletes, the treatment of choice is anatomic repair of the ruptured tendon to its insertion in the proximal humerus either with suture anchors or transosseous sutures. Following surgery, most patients experience a near normal return of strength and significant improvement in the cosmetic appearance of the deformity. While more technically challenging, repair of chronic rupture is possible and is indicated in some patients. Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Question 421
High Yield
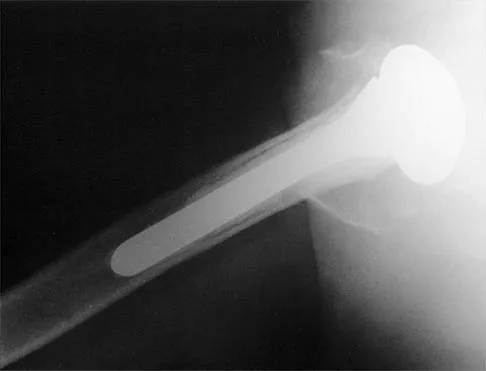
A 72-year-old woman who underwent right total hip arthroplasty 7 years ago now reports right hip pain and limb shortening. Studies for infection are negative. AP and lateral radiographs are shown in Figures 13a and 13b. What is the most appropriate management?


Explanation
Current literature supports the use of reinforcement cages for the reconstruction of failed, loosened acetabular components associated with major bone loss as seen in this patient. Although results of revision using the so-called jumbo cup with screws generally have been good, the amount of bone loss and medial wall penetration shown here and the likelihood of pelvic discontinuity precludes the use of that technique. With either technique, bone grafting of remaining defects is recommended. Sporer SM, O'Rourke M, Paprosky WG: The treatment of pelvic discontinuity during acetablular revision. J Arthroplasty 2005;20:79-84.
Question 422
High Yield
A 15-year-old girl with a midshaft fibular lesion has histologic findings consistent with Ewing's sarcoma. Following induction chemotherapy, local control typically consists of

Explanation
The current treatment regimen for Ewing's sarcoma typically involves induction chemotherapy followed by local control and further chemotherapy. Local control consists of surgery only, radiation therapy only, or a combination of the two. In bones that are easily resectable (expendable) with wide margins, surgery is usually recommended. For areas that cannot be resected (ie, large bulky pelvic tumors), radiation therapy alone is sometimes the preferred method of local control. If surgery is chosen and the margins are close, radiation therapy can be used as an adjuvant treatment. Amputation is rarely required for an isolated fibular lesion. Observation without adequate local control results in local recurrence. Nesbit ME Jr, Gehan EA, Burgert EO Jr, et al: Multimodality therapy for the treatment of primary, non-metastatic Ewing's sarcoma of the bone: A long-term follow-up of the first intergroup study. J Clin Oncol 1990;8:1664-1674.
Question 423
High Yield
A patient with Charcot-Marie-Tooth disease has a progressively rigid cavovarus foot deformity. The patient states that the pain is restricted to the forefoot, where rigid claw toe deformities have developed. Which of the following structures is primarily involved in creation of a claw toe deformity?

Explanation
Diseases such as Charcot-Marie-Tooth result in spasticity to the extrinsic flexor tendons. This results in hyperflexion of the proximal and distal interphalangeal joints of the involved toe, as well as hyperextension at the metatarsophalangeal joint. The tendon often becomes contracted with progressive equinus of the ankle. Correction of ankle equinus exaggerates the claw toe deformity. The interosseous tendon plays no role in the etiology of a claw toe but may become contracted in later stages of the disease. Laxity of the volar plate may precipitate a claw toe deformity in a nonspastic situation. In patients with a head injury, claw toe deformities are generally the result of overactivity of the extensor tendons. Keenan MA, Gorai AP, Smith CW, Garland DE: Intrinsic toe flexion deformity following correction of spastic equinovarus deformity in adults. Foot Ankle 1987;7:333-337. Pichney GA, Derner R, Lauf E: Digital "V" arthrodesis. J Foot Ankle Surg 1993;32:473-479.
Question 424
High Yield
The radiographic feature seen in Figure 37 that best indicates a slow-growing process is the
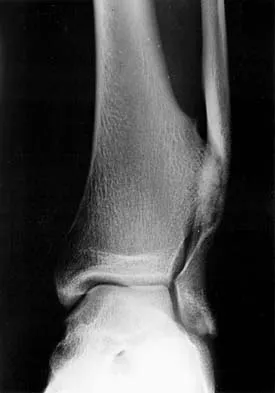
Explanation
For the fibula (or any bone) to bow, a long-standing process needs to be present. Pressure from a rapid process would cause erosion, not allowing the bone to remodel. The other features are helpful confirmatory findings but also may be associated with aggressive processes. In this patient, the fibular deformity is caused by a sessile osteochondroma of the tibia. Lodwick GS, Wilson AJ, Farrell C, Virtama P, Dittrich F: Determining growth rates of focal lesions of bone from radiographs. Radiology 1980;134:577-583.
Question 425
High Yield
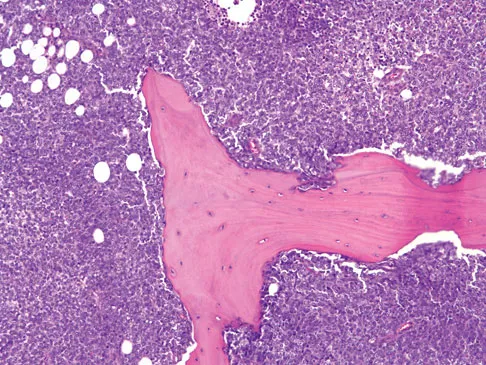
A 10-year-old boy with a history of retinoblastoma now reports right knee pain. AP and lateral radiographs are shown in Figures 3a and 3b. What is the most likely diagnosis?


Explanation
The radiographs show a bone-producing lesion in the femoral diaphysis. The radiographic appearance of small round cell tumors is more permeative with an elevated periosteum and no matrix production. The appearance of this lesion is most consistent with osteosarcoma. Patients who carry the Rb gene are predisposed to osteosarcoma. However, Ewing's sarcoma, primitive neuroectodermal tumor, and osteomyelitis can all occur in this location. Unni KK: Dahlin's Bone Tumors: General Aspects and Data on 11,087 Cases, ed 5. Philadelphia, PA, Lippincott-Raven, 1996, pp 143-160.
Question 426
High Yield
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4 degrees F (37.4 degrees C), and examination reveals that abduction of the left hip is limited to 30 degrees. Laboratory studies show a WBC of 11,000/mm3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of

Explanation
The most likely diagnosis is transient synovitis. Initial management should consist of bed rest and serial observation to rule out atypical septic arthritis of the hip. In an unreliable family situation, hospitalization for bed rest and observation may be indicated. Other disorders such as proximal femoral osteomyelitis, leukemia, juvenile rheumatoid arthritis, pelvic osteomyelitis, diskitis, and arthralgia secondary to other inflammatory disorders should be considered. However, these disorders are unlikely because of the paucity of abnormal clinical signs exhibited by the patient. On the other hand, transient synovitis of the hip in children is a diagnosis of exclusion; other possibilities should be explored if the patient's symptoms do not follow a typical course and resolve in 4 to 21 days.
Question 427
High Yield
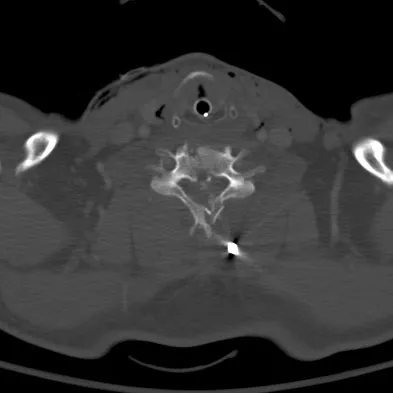
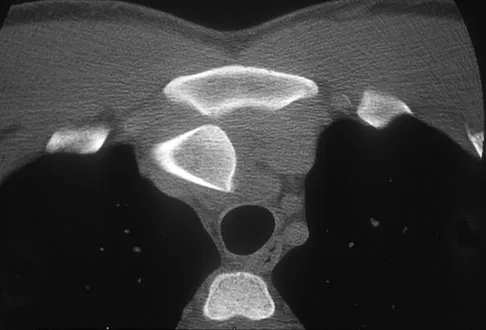
Figure 11a shows the clinical photograph of a 46-year old woman who reports a 3-week history of pain and a "lump" at the base of her neck. She is otherwise in good health and denies any trauma. A 3-D reconstruction CT is shown in Figure 11b. What is the most likely diagnosis?


Explanation
Spontaneous subluxation of the sternoclavicular joint occurs without any significant trauma. It is usually accentuated by placing the extremity in an overhead position. Discomfort usually resolves within 4 to 6 weeks with nonsurgical management. Rockwood CA, Wirth MA: Disorders of the sternoclavicular joint, in Rockwood CA, Matsen FA, Wirth MA, et al (eds): The Shoulder. Philadelphia, PA, WB Saunders, 2004, vol 2, pp 1078-1079.
Question 428
High Yield
An 11-year-old girl has had pain in the medial arch of her foot for the past 3 months. She reports that pain is present even with daily activities such as walking to class at school, and ibuprofen provides some relief. She denies any history of trauma. Examination reveals a flexible pes planus with focal tenderness over a prominent tarsal navicular tuberosity. Radiographs show a prominent accessory navicular. Management should consist of

Explanation
The patient has the classic symptoms, examination findings, and radiographs for a painful accessory navicular. Initial treatment should always be nonsurgical, specifically cast immobilization. Surgery should be reserved for those patients who fail nonsurgical management. Corticosteroids should not be injected into a posterior tibial tendon or insertion point because they can weaken the tendon and possibly cause tendon rupture. Triple arthrodesis and biopsy have no role in the management of a painful accessory navicular.
Question 429
High Yield
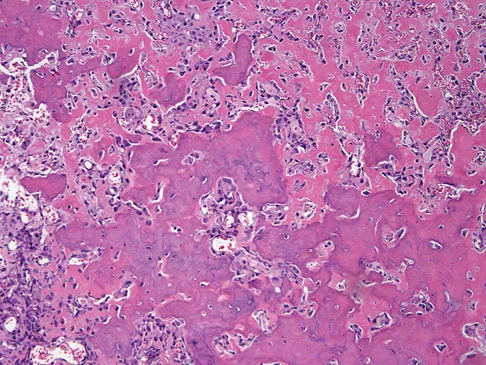
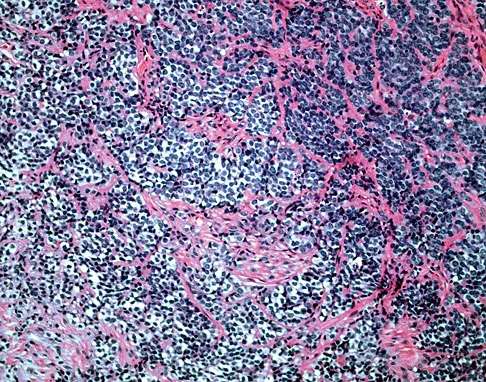
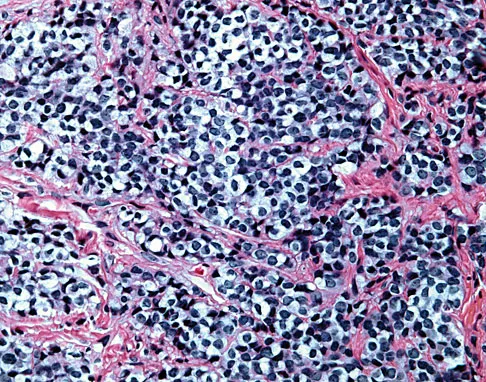
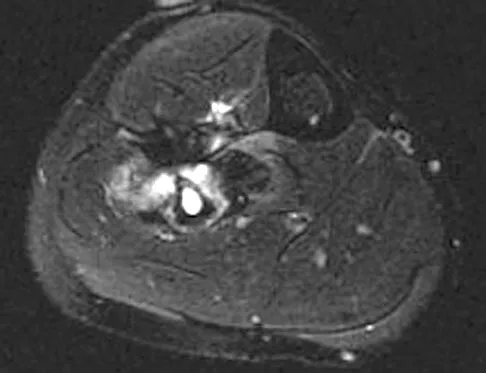
A 47-year-old woman has had a 1-month history of left hip and medial thigh pain that is exacerbated by sitting. Laboratory studies show a total protein level of 8.2 g/dL (normal 6.0 to 8.0) and an immunoglobulin G (IGG) level of 2,130 mg/dL (normal 562 to 1,835). A radiograph, CT scan, and biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?


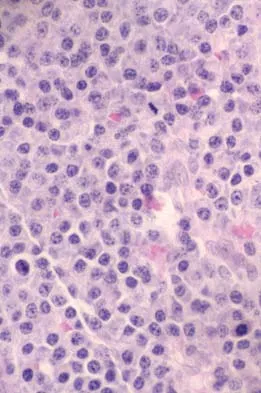
Explanation
The laboratory studies and histology are both consistent with myeloma. Infection should show white blood cells other than plasma cells on histology. Lymphoma would show lymphocytes, not plasma cells. The lack of bone formation on the imaging studies and the lack of osteoid on histology rule out osteosarcoma. The cells have too much cytoplasm and nuclear chromatin to be Ewing's sarcoma cells.
Question 430
High Yield
What is the most common location for localized pigmented villonodular synovitis (PVNS) to occur?

Explanation
Localized PVNS is a form of the disease in which synovial proliferation is restricted to one area of a joint and causes the formation of a small mass-like lesion. The true incidence of this is unknown but is probably less common than the diffuse form of the disease. PVNS presents as a usually painful discrete mass. The anterior compartment of the knee is the most common location. Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis. J Am Acad Orthop Surg 2006;14:376-385.
Question 431
High Yield
A 19-year-old woman fell onto her nondominant hand 6 weeks ago. Radiographs are shown in Figures 37a and 37b. A decision has been made to treat this fracture surgically. What is the best approach to treat this fracture?


Explanation
Displaced fractures of the scaphoid are best treated with compression screw fixation. Proximal third fractures (as in this patient) are optimally approached via a dorsal approach to ensure proper reduction and compression. Fractures of the scaphoid waist can be approached either by a volar or a dorsal approach. Kirschner wire fixation is limited to proximal pole fractures that are too small to accommodate the trailing head of a compression screw. Retting ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole fractures. J Hand Surg Am 1999;24:1206-1210.
Question 432
High Yield
A soccer player who sustained a twisting injury to the right ankle while making a cut is unable to bear weight and has diffuse tenderness over the anterior and lateral aspects of the ankle. Examination also shows a positive squeeze test. Plain radiographs and a stress radiograph are shown in Figures 26a through 26c. Radiographs of the leg and knee are normal. What is the most appropriate management?



Explanation
The mechanism of injury, physical examination, and radiographs indicate a "high" ankle sprain with disruption of the distal tibiofibular ligaments and interosseous membrane. These injuries typically involve pronation and external rotation forces. In addition, recovery is significantly delayed, often requiring 6 to 8 weeks to heal. Radiographs obtained months after recovery often show calcification within the distal syndesmosis, which is not typically symptomatic. This patient has gross instability, resulting in a high incidence of chronic diastasis and subluxation leading to impaired function. Treatment should consist of reduction and stabilization with a transsyndesmotic screw because this injury demonstrates a widened syndesmosis. Boytim MJ, Fisher DA, Neumann L: Syndesmotic ankle sprains. Am J Sports Med 1991;19:294-298.
Question 433
High Yield
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of


Explanation
Immediate repair of the tuberosity and rotator cuff is recommended on identifying the avulsion or nonunion. Revising the humeral component to increase tension and length will overtighten the cuff and increase the chance of tuberosity pull-off. The glenoid is uninvolved and should not be replaced. Attempts to strengthen the rotator cuff will be unsuccessful because the insertions are no longer attached to the humerus when the tuberosities avulse. Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
Question 434
High Yield
When treating thoracic disk herniations, which of the following surgical approaches has the highest reported rate of neurologic complications?
Explanation
Numerous surgical approaches have been used for thoracic diskectomy, including the most recent VATS. One of the first approaches described, posterior laminectomy, involves manipulation of the spinal cord, which the other approaches avoid. The posterior approach had dismal results, including further neurologic deterioration and even paralysis. Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864. Benjamin V: Diagnosis and management of thoracic disc disease. Clin Neurosurg 1983;30:577-605. Russell T: Thoracic intervertebral disc protrusion: Experience of 67 cases and review of the literature. Br J Neurosurg 1989;3:153-160.
Question 435
High Yield
What is the known manner in which the growth hormone-insulin-like growth factor-I (GH-IGF-I) system functions to stimulate bone growth?
Explanation
IGF-I, formerly known as somatomedin-C, possibly acts by both paracrine and endocrine hormone pathways. The products of the GH-IGF-I system induce proliferation without maturation of the growth plate and thus induce linear skeletal growth. The action of the thyroid hormone axis is via an active metabolite that enters target cells and signals a nuclear receptor to stimulate both proliferation and maturation of the growth plate. Increased amounts of the active steroid hormone metabolite promote proliferation and maturation of the growth plate. Calcitonin inhibits bone resorption. Binder G, Grauer ML, Wehner AV, et al: Outcome in tall stature: Final height and psychological aspects in 220 patients with and without treatment. Eur J Pediatr 1997;156:905-910. Wang J, Zhou J, Cheng CM, et al: Evidence supporting dual, IGF-I-independent and IGF-I-dependent, roles for GH in promoting longitudinal bone growth. Endocrinol 2004;180:247-255.
Question 436
High Yield
Anabolic steroid use has which of the following effects on serum lipoprotein levels?

Explanation
The use of anabolic steroids causes a decrease in high-density lipoprotein levels but has no effect on low-density lipoprotein levels. An abnormally low high-density lipoprotein level should alert the physician to the possibility of steroid use in an athlete. Hartgens F, Rietjens G, Keizer HA, et al: Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a). Br J Sports Med 2004;38:253-259.
Question 437
High Yield
What is the most common complication of halo vest immobilization in adults?
Explanation
Although pin loosening generally has not been considered a major problem, it has been cited as the most common complication in two published series of halo vest complications. The other possible complications are all significantly less common. Baum JA, Hanley EN Jr, Pullekines J: Comparison of halo complications in adults and children. Spine 1989;14:251-252. Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
Question 438
High Yield
Commotio cordis is best treated with
Explanation
Commotio cordis is a rare but catastrophic condition that is caused by blunt chest trauma. It results in cardiac fibrillation and is universally fatal unless immediate defibrillation is performed. Although case reports of successful use of the chest thump maneuver exist, the best method of treatment is cardiac defibrillation. IV fluids, epinephrine, and albuterol inhalers are used to treat dehydration, anaphylactic shock, and bronchospasm respectively, and are not effective in the treatment of commotio cordis. McCrory P: Commotio cordis. Br J Sports Med 2002;36:236-237.
Question 439
High Yield
A comparison of dural tears repaired with suture alone and those treated by suture with fibrin glue supplementation will reveal which of the following findings?
Explanation
Animal studies assessing the influence of fibrin glue supplementation have detected a markedly greater inflammatory response at the site of application. An increased incidence of infection and delays in healing were not noted. Cain JE Jr, Rosenthal HG, Broom MJ, Jauch EC, Borek DA, Jacobs RR: Quantification of leakage pressures after durotomy repairs in the canine. Spine 1990;15:969-970.
Question 440
High Yield
An otherwise healthy 57-year-old man has persistent, severe hip pain after undergoing total hip arthroplasty 3 months ago. What is the next most appropriate step in management?

Explanation
Any patient who is severely symptomatic this quickly after surgery must be evaluated for infection. Loosening is also a possible cause, but infection must be ruled-out. Bone scans are not helpful at this early postoperative stage. Normal laboratory values argue strongly against infection, but when abnormal, need to be supplemented with a hip aspiration. Aspiration remains the most selective and sensitive measure, especially when linked to a WBC count of the synovial tissues in the joint. There is no indication for an antiobiotic trial because it may make future culture sensitivity more difficult. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993; 24: 751-759.
Question 441
High Yield
A 25-year-old laborer sustains a transverse fracture of the proximal 25% of the scaphoid. CT reconstructions reveal a 1-mm fracture gap. What is the most appropriate treatment?
Explanation
A higher risk of nonunion and the need for prolonged immobilization is seen after nonsurgical management of proximal pole fractures of the scaphoid. Because of the relatively poor blood supply of the proximal pole, surgical treatment with a compression screw is advocated for fractures of the proximal third of the scaphoid. Clay NR, Dias JJ, Costigan PS, et al: Need the thumb be immobilized in scaphoid fractures? A randomised prospective trial. J Bone Joint Surg Br 1991;73:828-832.
Question 442
High Yield
A radiograph, MRI scans, and a biopsy specimen of a 9-year-old boy with thigh pain are shown in Figures 37a through 37d. Management should consist of


Explanation
The patient has Ewing's sarcoma. Management options for local tumor control include radiation therapy, resection, or a combination; however, in this patient wide resection is preferred over radiation therapy. Radiation therapy is associated with damage to the growth plate, pathologic fracture, radiation-induced sarcomas, and a local recurrence rate of approximately 10% to 12%. Radiation therapy is used for positive margins, unresectable tumors, or for tumors that have a poor response to chemotherapy. Amputation is not necessary since the tumor is resectable. Chemotherapy has improved overall survival rates to over 60% of patients. Sailer SL: The role of radiation therapy in localized Ewing' sarcoma. Semin Radiat Oncol 1997;7:225-235. Shankar AG, Pinkerton CR, Atra A, Ashley S, Lewis I, Spooner D, et al: Local therapy and other factors influencing site of relapse in patients with localised Ewing's sarcoma. United Kingdom Children's Cancer Study Group (UKCCSG). Eur J Cancer 1999;35:1698-1704. Carrie C, Mascard E, Gomez F, Habrand JL, Alapetite C, Oberlin O, et al: Nonmetastatic pelvic Ewing sarcoma: Report of the French society of pediatric oncology. Med Pediatr Oncol 1999;33:444-449.
Question 443
High Yield
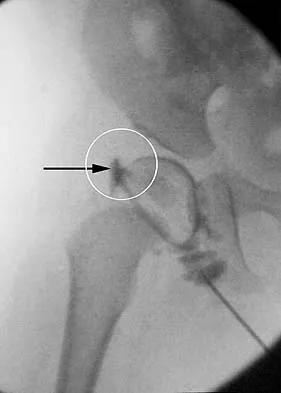
Figure 36 shows the hip arthrogram of a newborn. Which of the following structures is enclosed by the circle?
Explanation
The structure enclosed by the circle is the acetabular labrum. It is visible as the white point of tissue outlined by the darkly radiopaque contrast. The appearance of the contrast surrounding the sharp white point of a normal labrum is called the "rose thorn sign." The limbus is the term reserved for a rounded, infolded labrum seen with arthrography. The pulvinar is the fatty tissue seen in the empty acetabulum when the hip is dislocated. The ligamentum teres is seen as a white stripe outlined by contrast coursing from the central acetabulum to the dislocated femoral head. The transverse acetabular ligament courses across the inferior portion of the acetabulum and is not clearly seen with arthrography. Herring JA: Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, vol 1, pp 532-533.
Question 444
High Yield
A 41-year-old man who plays golf regularly has had ulnar-sided wrist pain for the past several days after striking a tree root with a golf club. Examination reveals significant pain with resisted flexion of the ring and small fingers and tenderness over the hook of the hamate. Which of the following radiographic views would be most helpful in identifying the pathology of this injury?

Explanation
The history and examination findings suggest an acute fracture of the hook of the hamate. The radiographic study considered most helpful in identifying this type of fracture is the carpal tunnel view. PA and lateral views of the wrist will not adequately visualize the hook of the hamate. Bruerton's view is intended for the assessment of the metacarpophalangeal joints. Pathology would not be suspected in the scaphoid, metacarpals, or the phalanges, so the scaphoid view and the PA, lateral, and oblique views of the hand would not be helpful. Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, p 855.
Question 445
High Yield
A 72-year-old woman who sustained a cerebrovascular accident 9 months ago now has a fixed elbow flexion contracture of 80 degrees. Management should consist of

Explanation
A flexion contracture of the elbow is commonly seen in hemiplegic patients following cerebrovascular accidents. Spasticity and myostatic contracture of the joint are both causative factors. In patients with a flexion deformity of less than 90 degrees, musculocutaneous neurectomy is recommended, followed by serial casting to treat any residual deformity. At 9 months after injury, physical therapy will not significantly improve motion. Nerve blocks may be used in the early stages of recovery to facilitate therapy and serial casting.
Question 446
High Yield
Figure 8a shows the clinical photograph of an 83-year-old woman who has an enlarging left forearm mass. MRI scans are shown in Figures 8b and 8c. What is the next most appropriate step in management?

Explanation
Any large (greater than 5 cm), deep, heterogeneous mass in the extremities should be considered a sarcoma until proven otherwise. Sarcomas are rare, and without a high index of suspicion, the lesions may be misdiagnosed or there may be a delay in diagnosis. Needle biopsies can obtain sufficient tissue for diagnosis and are associated with less morbidity than open biopsy. Marginal resections or excisional biopsies should be reserved for a few select benign lesions and locations. Damron TA, Beauchamp CP, Rougraff BT, et al: Soft-tissue lumps and bumps. Instr Course Lect 2004;53:625-637.
Question 447
High Yield
Thermal capsulorrhaphy of the inferior glenohumeral ligament can cause iatrogenic injury to which of the following nerves?
Explanation
The axillary nerve courses from anterior to posterior just below the inferior shoulder capsule. Thermal energy applied to the inferior aspect of the shoulder capsule can result in injury to this nerve. Wong KL, Williams GR: Complications of thermal capsulorrhaphy of the shoulder. J Bone Joint Surg Am 2001;83:151-155.
Question 448
High Yield
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
Radiographic findings in patients with rheumatoid arthritis include symmetric joint space narrowing, periacetabular and femoral head erosions, and diffuse periarticular osteopenia. In advanced stages, protrusio acetabuli is a common finding. Ranawat and associates have shown a rate of superior femoral head migration of 4.5 mm per year and medial (axial) migration of 2.5 mm per year. Asymmetric joint space narrowing is a classic radiographic finding of degenerative arthrosis. Sacroiliac joint ankylosis commonly occurs in ankylosing spondylitis. Hip synovitis is a pathologic diagnosis, not a radiographic finding. Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Question 449
High Yield
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 450
High Yield
An obese patient undergoing total knee arthroplasty is at increased risk for which of the following complications?
Explanation
The rate of wound complications is significantly increased after total knee arthroplasty in obese patients. Knee scores and the rate of aseptic loosening or patellar subluxation do not appear to be significantly altered. Winiarsky R, Barth P, Lotke P: Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am 1998;80:1770-1774. Stern SH, Insall JN: Total knee arthroplasty in obese patients. J Bone Joint Surg Am 1990;72:1400-1404.
Question 451
High Yield
Type II collagen in nondiseased adult human articular cartilage has a half-life that is generally
Explanation
Type II collagen in articular cartilage is amazingly stable. This is important to know because matrix homeostasis generally is associated with minimal synthesis and degradation of type II collagen. Passive glycation has a consistent rate and occurs over decades. The relative amount of glycation in cartilage with age has been used as a measure of stability. Also, the rate of racemization of aspartic acid from the L to D form occurs spontaneously at a very slow rate. The relative stability of collagen can be estimated by calculating the percentage of D aspartic acid per dry weight of type II collagen. Maroudas A, Palla G, Gilav E: Racemization of aspartic acid in human articular cartilage. Connect Tissue Res 1992;28:161-169.
Question 452
High Yield
A healthy 16-year-old boy has had increasing pain in the right knee for the past 3 months. Examination reveals warmth and swelling around the distal femur. Radiographs and an MRI scan are shown in Figures 51a through 51c, and a biopsy specimen is shown in Figure 51d. What is the most likely diagnosis?



Explanation
The radiographs show a bone-producing lesion in the distal femoral metaphysis in this case of classic osteosarcoma presenting in the most common location, the distal femur. The coronal MRI scan reveals a marrow-occupying lesion with extension into the soft tissues. The histology shows osteoid production by pleomorphic cells consistent with an osteosarcoma. Ewing's sarcoma is a bone tumor characterized by uniform small blue cells on histology. Rhabdomyosarcoma is the most common childhood soft-tissue sarcoma. Osteomyelitis has an inflammatory appearance on histology. Malignant fibrous histiocytoma of bone has a lytic radiographic appearance and a pleomorphic storiform pattern without osteoid on histology. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 179.
Question 453
High Yield
Which of the following conditions precludes performing a tendon transfer?
Explanation
Several conditions must be met before a tendon transfer has the potential to correct a dynamic deformity. If the target joint cannot be passively corrected to neutral, it indicates that a static joint contracture or bony deformity exists that cannot be corrected with a dynamic tendon transfer. While in-phase muscles are best, out-of-phase muscles are often the only muscles available for transfer. Tendon transfer should pull in a straight line to avoid tethering and late failure. Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. St Louis, MO, Mosby, 2003, pp 1283-1287.
Question 454
High Yield
A 27-year-old man now reports dorsiflexion and inversion weakness after an automobile collision 6 months ago in which compartment syndrome developed isolated to the anterior and deep posterior compartments. Examination reveals the development of a progressive cavovarus deformity, but the ankle and hindfoot remain flexible. In addition to Achilles tendon lengthening, which of the following procedures is most likely to improve the motor balance of his foot and ankle?

Explanation
Compartment syndrome of the anterior and deep posterior compartments results in anterior tibialis and posterior tibialis tendon weakness, respectively. Furthermore, the long flexors to the hallux and lesser toes will be weak as well. The intact peroneus longus overpowers the weak anterior tibialis tendon, resulting in plantar flexion of the first metatarsal, cavus, and hindfoot varus. Therefore, transferring the peroneus longus to the dorsolateral midfoot reduces the first metatarsal plantar flexion torque, and possibly augments ankle dorsiflexion torque. Hansen ST: Functional Reconstruction of the Foot and Ankle. Philadelphia, PA, Lippincott, Williams & Wilkins, 2000, pp 433-435.
Question 455
High Yield
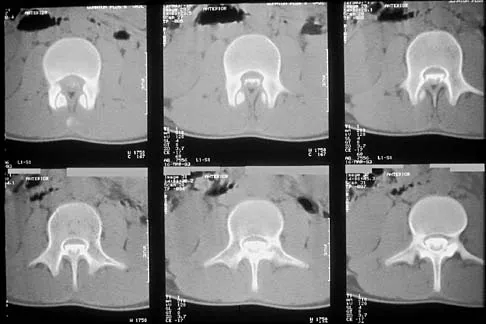
Figures 27a through 27c show the radiographs and CT scan of a 27-year-old man who sustained a low-velocity gunshot wound to the neck. He is quadriplegic (ASIA A), hemodynamically stable, and does not have drainage from his wound. After initial resuscitation and stabilization, the cervical spine and spinal cord injuries are best managed by


Explanation
Although the spinal canal has been penetrated, the lateral masses are intact bilaterally with only partial destruction of the vertebral body and penetration of the lamina on one side, thus the cervical spine is not unstable and surgical stabilization is not indicated. Dural repair is not indicated since there is no external cerebrospinal fluid leakage. Surgical treatment should be based on the need to treat extraspinal pathology only. Bono CM, Heary RF: Gunshot wounds to the spine. Spine J 2004;4:230-240.
Question 456
High Yield
A Trendelenburg gait is most likely to be seen in association with

Explanation
A Trendelenburg gait results from weakness of the gluteus medius, which is innervated by the L5 nerve root. A paracentral disk herniation at L4-L5 most commonly results in an L5 radiculopathy and thus weakness of the gluteus medius. A paracentral herniation at L5-S1 most commonly affects the S1 nerve root. A paracentral herniation at L3-L4, a central herniation at L3-L4, and a far lateral herniation at L4-L5 all affect the L4 root. Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 457
High Yield
A patient has a displaced complex intra-articular distal humeral fracture. What factor is considered most important when deciding on what surgical approach to use?

Explanation
When managing a complex intra-articular fracture, it is imperative that there is adequate visualization of the joint; this usually means an extensile approach. At the elbow, this is usually through a transolecranon osteotomy. The recent addition of a muscle-sparing approach as described by Bryan and Morrey has gained popularity, but it is difficult to maintain soft-tissue viability and it may put the ulnar nerve at risk. A triceps-splitting approach, which can be used for simple single articular splits into the joint where extra-articular reduction is available, is possible and good results have been reported. To date, there is minimal data on these alternative approaches for comminuted intra-articular distal humeral fractures. McKee MD, Mehne DK, Jupiter JP: Fractures of the distal humerus: Part II, in Browner BD, Jupiter JP, Levine AM, Trafton P (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1483-1522 McKee MD, Wilson TL, Winston L, Schemitsch EH, Richards RR: Functional outcome following surgical treatment of intra-articular distal humeral fractures through a posterior approach. J Bone Joint Surg Am 2000;82:1701-1707. Patterson SD, Bain GI, Mehta JA: Surgical approaches to the elbow. Clin Orthop 2000;370:19-33.
Question 458
High Yield
What is the function of the rotator cuff during throwing?

Explanation
The coupled action of the rotator cuff prevents superior migration and controls anterior and posterior translation by depressing the humeral head. Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Question 459
High Yield
Which of the following is considered the most useful screening method for the evaluation of protective foot sensation in a patient with diabetes mellitus?
Explanation
Patients with diabetes mellitus should be screened for the presence of protective foot sensation. In the absence of protective foot sensation, patients are at increased risk for the development of neuropathic ulcerations and neuropathic arthropathy. The most reliable screening tool for the presence of protective sensation is the ability to feel the 5.07 Semmes-Weinstein monofilament. Pinzur MS, Shields N, Trepman E, Dawson P, Evans A: Current practice patterns in the treatment of Charcot foot. Foot Ankle Int 2000;21:916-920.
Question 460
High Yield
A 45-year-old man has severe pain in both feet after his boots become wet while hunting. Examination 3 hours after the onset of symptoms reveals that his feet are cold to touch and the skin appears blanched. Management should consist of
Explanation
The patient has frostbite involving both feet. Rapid rewarming in a protected environment is the initial treatment. A footbath with water at 104.0 degrees F to 107.6 degrees F (40 degrees C to 42 degrees C) is ideal. This facilitates a uniform rewarming of the involved tissue. The other choices are less than ideal. Appliances such as heating pads provide uneven heating and may actually burn the skin. Pinzur MS: Frostbite: Prevention and treatment. Biomechanics 1997;4:14-21.
Question 461
High Yield
A 61-year-old man reports right hip pain and limited motion after undergoing total hip arthroplasty for posttraumatic arthritis 1 year ago. Figure 6 shows an AP radiograph of the pelvis. To improve motion and relieve pain, management should consist of

Explanation
The patient has symptomatic grade IV Brooker heterotopic ossification. Once the bone has matured, it can be excised. Surgical excision should be combined with postoperative irradiation to avoid recurrence. Pharmacologic and irradiation intervention are not successful beyond the perioperative period unless they are combined with surgical excision of mature heterotopic ossification. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 462
High Yield
Which of the following is considered a physiologic effect of anemia?
Explanation
The expected physiologic effects of anemia include an increased heart rate and increased cardiac output. The coronary blood flow requirement increases. There is a decrease in peripheral resistance and blood viscosity.
Question 463
High Yield
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
The contents of the anterior tarsal tunnel are the extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, and the deep peroneal nerve. The term "anterior tarsal tunnel syndrome" is used to specifically describe the compression of the deep peroneal nerve under the inferior extensor retinaculum. With nerve compression, patients report a burning sensation across the dorsum of the foot with paresthesias in the first web space. There also may be wasting and weakness of the extensor digitorum brevis. Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Question 464
High Yield
Examination of a 10-year-old girl with a hypoplastic breast and atrophic pectoralis major may also reveal which of the following findings?
Explanation
Poland's syndrome has four main features: 1) short digits as the result of absence or shortening of the middle phalanx; 2) syndactyly of the short digits usually consisting of a simple, complete type; 3) hypoplasia of the hand and forearm; and 4) absence of the sternocostal head of the pectoralis major on the same side. Wilson MR, Louis DS, Stevenson TR: Poland's syndrome: Variable expression and associated anomalies. J Hand Surg 1988;13:880-882.
References:
- Poland A: Deficiency of the pectoralis muscle. Guys Hosp Rep 1841;6:191.
Question 465
High Yield
A 32-year-old man has posttraumatic arthritis after undergoing open reduction and internal fixation of a left acetabular fracture. A total hip arthroplasty is performed, and the radiograph is shown in Figure 18. What is the most common mode of failure leading to revision in this group of patients?

Explanation
Acetabular component loosening has been reported as the most common mode of failure following total hip arthroplasty in patients with a previous acetabular fracture. Following acetabular fracture and subsequent open reduction and internal fixation, the bone quality and vascularity are compromised, thus reducing the success rate of acetabular component cementless fixation. Jimenez ML, Tile M, Schenk RS: Total hip replacement after acetabular fracture. Orthop Clin 1997;28:435-446.
Question 466
High Yield
The major blood supply to the cruciate ligaments arises from which of the following structures?

Explanation
The major blood supply to the cruciate ligaments arises from the ligamentous branches of the middle genicular artery. Few terminal branches of the inferior genicular artery contribute to the blood supply. The synovial plexus and sheath covering the cruciate ligaments are also supplied by branches of the middle genicular artery. The blood supply to the cruciate ligaments is predominately of soft-tissue origin. There is no significant osseous vascular contribution to the ligaments. Arnoczky SP: Anatomy of the anterior cruciate ligament. Clin Orthop 1983;172:19-25.
Question 467
High Yield
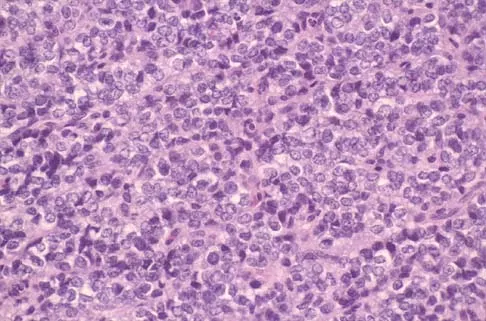
A 16-year-old boy has had left knee pain and swelling after sustaining a minor twisting injury while playing basketball 2 weeks ago. Figures 5a through 5e show the radiograph, MRI scans, and biopsy specimens. What is the most likely diagnosis?


Explanation
The imaging studies and histology are most consistent with Ewing's sarcoma. Tuberculosis can show small round blue cells on histology (lymphocytes associated with chronic infection) but would more typically involve the knee joint and periarticular bone. Osteosarcoma and MFH do not have small round blue cells histologically. Sissons HA, Murray RO, Kemp HBS: Orthopaedic Diagnosis. Berlin, Springer-Verlag, 1984, pp 254-256.
Question 468
High Yield
A 40-year-old patient who has a type II odontoid fracture is placed in a halo vest for 12 weeks; however, current radiographs show no evidence of healing. The next most appropriate step in management should consist of

Explanation
Because nonsurgical managment has failed and a significant number of type II odontoid fractures will go on to a nonunion, the salvage treatment of choice is posterior fusion at C1-2. Odontoid screws are contraindicated in patients with a chronic nonunion, which this patient has at the end of 3 months. Montesano PX: Anterior and posterior screw and plate techniques used in the cervical spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1743-1761. Bohler J: Anterior stabilization for acute fractures and non-unions of the dens. J Bone Joint Surg Am 1982;64:18-27.
Question 469
High Yield
A 40-year-old unrestrained passenger reports chest wall pain after a motor vehicle accident. Which of the following structures is most important in preventing the injury shown in Figure 33?
Explanation
Through cadaveric study, Spencer and associates measured anterior and posterior translation of the sternoclavicular joint. The study demonstrated that the posterior sternoclavicular joint capsule is the most important structure for preventing both anterior and posterior translation of the sternoclavicular joint. Gilot GJ, Wirth MA, Rockwood CA: Injuries to the sternoclavicular joint, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott, Williams and Wilkins, 2006, vol 2, pp 1373-1374.
Question 470
High Yield
An 83-year-old woman with diabetes mellitus has a history of recurrent infection over the medial aspect of her great toe and has had a painless bunion for the past 45 years. Shoe wear modifications have failed to provide relief. Pedal pulses are palpable. Figures 30a and 30b show the clinical photograph and radiograph. Management should now consist of


Explanation
The presence of recurrent breakdown over the medial eminence despite shoe wear modifications is an indication for surgery. A number of factors must be considered when deciding on an appropriate course of treatment. These include age, activity level, joint congruency, joint degeneration, and the patient's symptoms and expectations. The indications for a simple bunionectomy are rather limited. In this patient, the goal of surgery is to alleviate the recurrent infection by removal of a large medial eminence. Because the bunion is painless and long-standing, it does not warrant treatment. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 123-134.
Question 471
High Yield
A 32-year-old runner has pain in the medial arch that radiates into the medial three toes. He reports the presence of pain only when running. Examination reveals normal hindfoot alignment. There is a weakly positive Tinel's sign over the posterior tibial nerve. Tenderness is noted with palpation over the plantar medial area in the vicinity of the navicular tuberosity. What is the most likely diagnosis?
Explanation
The examination findings reveal that there is specific involvement of the medial plantar nerve by the distribution of the pain medially. The symptoms exclude the possibility of plantar fasciitis and anterior tibial tendinitis. Sinus tarsi syndrome would produce anterolateral symptoms rather than medial symptoms. Rask MR: Medial plantar neurapraxia (jogger's foot): Report of three cases. Clin Orthop 1978;134:193-195. Murphy PC, Baxter DE: Nerve entrapment of the foot and ankle in runners. Clin Sports Med 1985;4:753-763.
Question 472
High Yield
The presence of S100B tumor marker typically corresponds with which of the following as being the most likely source of the metastasis?
Explanation
Advances in development of new tumor markers and techniques of antigen retrieval have enhanced the sensitivity and reliability of identifying the primary source of metastasis. New markers such as CK7, CK20, CA125, and thyroid transcription factor-1 (TTF-1) can help to determine the origin of an adenocarcinoma or aid in the recognition of other tumors. In patients who do not have an obvious primary site of disease or screening radiographs, these new markers can help focus the search for and guide the treatment of the underlying lesion. CA125 is positive in patients with ovarian cancer, CK7 is positive in patients with breast and lung carcinoma, and CK20 is indicative of colon carcinoma if the CK7 marker is negative. Gastrointestinal stromal tumor (GIST) is positive for CD117 (c-kit) and CD34, whereas 75% of bronchogenic carcinomas are positive for TTF-1. Histochemical staining of the S100 protein family has been used for many years in the diagnosis of malignant melanoma. Recent markers HMB-45, MART-1, and Melan-A have proved to be useful in diagnosis of melanoma. S100B protein has been implicated in downregulation of p53 (oncosuppressor gene). Harpio R, Einarsson R: S100 proteins as cancer biomarkers with focus on S100B in malignant melanoma. Clin Biochem 2004;37:512-518.
Question 473
High Yield
A 42-year-old college professor reports persistent pain at the hypothenar eminence 9 months after falling from his bicycle. Initial radiographs were reportedly normal. Use of a wrist splint for the last 2 months has failed to provide relief. A radiograph obtained by his primary care physician prior to referral is seen in Figure 31. What is the most appropriate treatment?

Explanation
The oblique radiograph of the wrist reveals a displaced fracture of the pisiform that usually occurs following a direct blow or sudden contraction of the flexor carpi ulnaris tendon. Persistent pain secondary to pisotriquetral incongruity and degenerative arthritis warrants pisiform excision, which does not compromise wrist flexion strength. Pisiform fractures are usually missed on routine radiographic views. An oblique or carpal tunnel view can be helpful in visualizing the pisotriquetral joint.
Question 474
High Yield
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
This injury pattern is one of a direct trauma to the mid aspect of the foot. Without additional forces involved, capsular ligamentous injury is not anticipated; therefore, the injury should be a stable pattern. Treatment should consist of protected weight bearing as tolerated in a walking boot or walking cast. Surgical intervention with open reduction and internal fixation, percutaneous pinning, or open reduction and internal fixation with primary tarsometatarsal joint fusion is not indicated with this pattern of injury. The use of external bone stimulation in this acute fracture setting is not indicated. With injuries to the midfoot area where the exact mechanism of injury is uncertain, there should be a high index of suspicion for an associated injury to the tarsometatarsal joint, and standing radiographs or stress radiographs should be obtained. Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Question 475
High Yield
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in

Explanation
Prophylactic stabilization of impending fractures does not directly affect the overall survival rate, but it does improve factors related to intraoperative and postoperative complications and decreased recovery time. Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Question 476
High Yield
Which of the following patient factors is associated with recurrent radicular pain following lumbar diskectomy for sciatica?
Explanation
A large annular defect at the site of a lumbar disk herniation is associated with persistent radicular pain postoperatively. Large sequestered herniations and a positive SLR preoperatively correlate with good outcomes after diskectomy. Neither symptoms of more than 3 months' duration nor preoperative epidural steroid injections correlate with postoperative results after diskectomy. Carragee EJ, Han MY, Suen PW, et al: Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment type and anular competence. J Bone Joint Surg Am 2003;85:102-108.
Question 477
High Yield
Figures 28a and 28b show AP and lateral radiographs of the knee. Based on these findings, which of the following structures has most likely been injured?


Explanation
The radiographs show a posterior knee dislocation. Knee dislocations almost always involve rupture of both the anterior and posterior cruciate ligaments. Collateral ligament injuries also are common. Arterial, nerve, and tendon injuries each occur in less than half of knee dislocations. Schenck RC Jr, Hunter RE, Ostrum RF, et al: Knee dislocations. Instr Course Lect 1999;48:515-522.
Question 478
High Yield
Which of the following studies has the highest sensitivity and specificity in diagnosis of osteonecrosis of the femoral head?

Explanation
An MRI scan is both highly sensitive and specific for the evaluation of osteonecrosis. The measurement of increased intraosseous pressure can be technically difficult and the results have been variable. Plain radiographs can be normal early in the progression of osteonecrosis of the femoral head. The technetium Tc 99m bone scan is a very sensitive test. However, it is not specific; increased uptake can be noted in patients with arthritis, neoplastic disease, fracture, or sepsis. In addition, because of bilaterality, the frequency of false-negative scans is relatively high. Steinberg ME: Early diagnosis, evaluation, and staging of osteonecrosis, in Jackson DW (ed): Instructional Course Lectures 43. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 513-518.
Question 479
High Yield
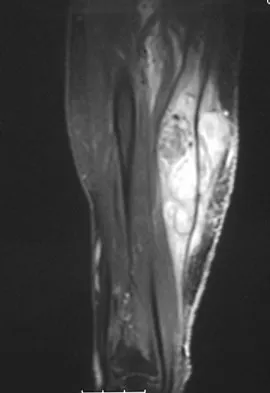
An 18-year-old boy reports increasing pain with weight bearing on his right leg and at night. Examination reveals swelling around the right midcalf. Radiographs and an MRI scan are shown in Figures 13a through 13c, and a biopsy specimen is shown in Figure 13d. What is the preferred treatment?


Explanation
The findings are consistent with Ewing's sarcoma. The radiographs reveal a lytic lesion in the diaphysis of the right fibula. There is elevation of the periosteum and evidence of a surrounding soft-tissue mass. The biopsy specimen shows diffuse small round blue cells surrounding the lamellar bone. It is the second most common malignant bone tumor in children. The most common treatment regimen consists of chemotherapy followed by surgical resection and/or radiation therapy. Surgical resection is employed when the lesion can be removed with wide margins and causes less morbidity than radiation therapy. McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 258.
Question 480
High Yield
When performing an inside-out lateral meniscal repair, capsule exposure is provided by developing the

Explanation
Capsular exposure for an inside-out lateral meniscal repair is performed by developing the interval between the iliotibial band and biceps tendon. Posterior retraction of the biceps tendon exposes the lateral head of the gastrocnemius. Posterior retraction of the gastrocnemius provides access to the posterolateral capsule. Miller DB Jr: Arthroscopic meniscus repair. Am J Sports Med 1988;16:315-320.
Question 481
High Yield
A 7-year-old girl sustains the fracture shown in Figure 29a. Casting results in uneventful healing. Ten months later, the patient has a progressive valgus deformity of the right lower extremity. A radiograph is shown in Figure 29b. Management should now consist of


Explanation
Although fractures of the proximal tibial metaphysis in young children appear innocuous, development of a progressive valgus deformity is possible despite adequate and appropriate treatment. When treating a child with this injury, it is prudent to warn the parents that a valgus deformity of the tibia may develop. The most likely cause is asymmetric growth of the proximal tibial physis. Because spontaneous angular improvement can be expected in most patients, surgery to correct these deformities should be delayed at least 2 to 3 years and should be limited to patients who have symptoms. There are no studies that document the efficacy of bracing for this deformity. Tuten HR, Keeler KA, Gabos PG, et al: Posttraumatic tibia valga in children: A long-term follow-up note. J Bone Joint Surg Am 1999;81:799-810.
Question 482
High Yield
A 14-year-old football player has had thigh pain and weakness following a full-contact scrimmage 24 hours ago. He recalls that he felt a sharp pain in his back after colliding with a much heavier player. Examination reveals that the spine is minimally tender to palpation in the upper lumbar region. Motor testing reveals quadriceps weakness bilaterally, and a reverse straight leg raising test is positive. Plain radiographs of the thoracolumbar spine are normal. A myelogram, a CT scan with contrast, and an MRI scan are shown in Figures 41a through 41c. What is the most likely diagnosis?


Explanation
Fracture of the vertebral end plate is a relatively uncommon injury that is most often seen in adolescent boys. The injury is characterized by traumatic displacement of the vertebral ring-apophysis into the spinal canal and associated disk herniation. Over one third of these injuries are seen in children with lumbar Scheuermann disease. The injury most frequently involves the midlumbar vertebra, and symptoms are often indistinguishable from those associated with a herniated disk. The injury is usually not visible on plain radiographs. The diagnosis is typically made after obtaining MRI or contrast CT scans. Treatment consists of laminotomy and excision of the osteochondral fragments. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 635-651.
Question 483
High Yield
The gluteus maximus is innervated by which of the following nerves?

Explanation
The inferior gluteal nerve supplies the gluteus maximus muscle. The superior gluteal nerve supplies the gluteus medius, gluteus minimus, and tensor fascia lata muscles. The femoral nerve supplies the quadriceps, sartorius, and pectineus muscles. The pudendal nerve is primarily a sensory nerve.
Question 484
High Yield
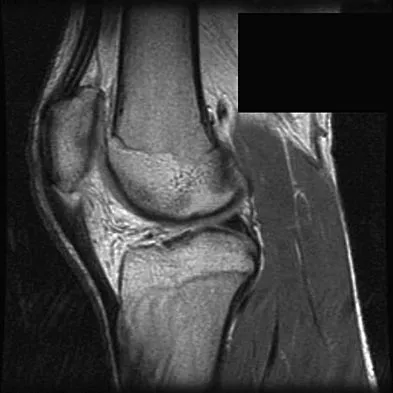
Figures 31a and 31b show the T1- and T2-weighted MRI scans of a patient's knee joint. What is the most likely diagnosis?


Explanation
The scans show a lipohemarthrosis. There is the characteristic layering of a superior zone containing fat (high signal intensity), a central zone containing serum (low signal intensity), and an inferior zone that contains red blood cells (low signal intensity). The most common cause of a lipohemarthrosis is an intra-articular fracture with leakage of marrow fat into the joint. Resnick D, Kang HS: Synovial joints, in Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 49-53.
Question 485
High Yield
The primary purpose of obtaining the radiograph shown in Figure 9 is to assess

Explanation
The radiograph shows a faux profil view of the hip. The primary purpose of this view is to evaluate anterior coverage of the femoral head. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 486
High Yield
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?
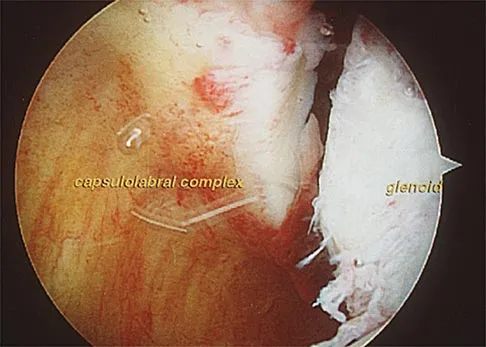
Explanation
The clinical photograph shows an acute capsulolabral avulsion from the anterior glenoid, also referred to as a Perthes-Bankart lesion. In patients who sustain an acute dislocation that requires a manual reduction, this pathologic lesion is observed with high frequency. In several research studies, it has been visualized in 80% to 95% of patients at arthroscopy. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Question 487
High Yield
The inheritance of the deformity shown in Figure 1 is most commonly
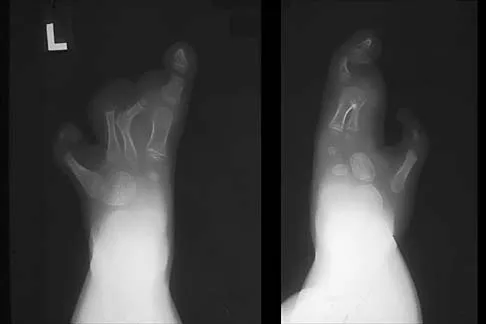
Explanation
Cleft hand and cleft foot malformations are commonly inherited as autosomal-dominant traits and are associated with a number of syndromes. An autosomal-recessive and an x-linked inheritance pattern have also been described, but these are much less common and are usually atypical. In the common autosomal-dominant condition, nearly one third of the known carriers of the gene show no hand or foot abnormalities. This is known as reduced penetrance. The disorder may be variably expressed; affected family members often exhibit a range from mild abnormalities in one limb only to severe anomalies in four limbs. Variable expressivity and reduced penetrance can cause difficulty in counseling families regarding future offspring in an affected family. Many patients have a cleft hand that may be caused by the split-hand, split-foot gene (SHFM1) localized on chromosome 7q21.
Question 488
High Yield
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
Cigarette smoking has been directly linked to pseudarthrosis in spinal fusions. The direct mechanism of action is diminished revascularization of cancellous bone graft. Additionally, a smaller area of revascularization is seen in these grafts, as well as an increased area of necrosis. Increased activity of osteoblasts would result in more bone production. Increased activity of osteocytes would not affect the fusion because osteocytes are mature bone cells.
Question 489
High Yield
The fracture shown in Figure 32 is strongly indicative of what diagnosis?

Explanation
Fractures that occur through the primary spongiosa at the subphyseal region of the metaphysis are highly specific for child abuse. On radiographic studies, the metaphyseal lucency in these injuries may appear as either the so-called "bucket-handle" or "metaphyseal corner" fracture. These fractures are not typical features of osteogenesis imperfecta or vitamin D-resistant rickets. The ingestion of lead may lead to thick, transverse bands of increased density at the distal metaphysis. Fractures in the subphyseal region of the metaphysis are not typically seen in children who have osteomyelitis. Kocher MS, Kasser JR: Orthopaedic aspects of child abuse. J Am Acad Orthop Surg 2000;8:10-20.
Question 490
High Yield
A 15-year-old boy reports feeling a pop and notes sudden giving way of the left knee while playing basketball. He has immediate pain and swelling in the knee. An AP radiograph is shown in Figure 32. A small avulsion fragment from the lateral tibial margin is the only finding. What is the most likely diagnosis?

Explanation
An avulsion fracture from the lateral tibial margin carries the eponym Segond fracture and is pathognomonic for an anterior cruciate ligament (ACL) tear. The fragment is located posterior to Gerdy's tubercle and is superior and anterior to the fibular head. It represents an avulsion of the lateral capsular ligament of the knee and is caused by the same mechanism that causes the ACL tear. The pes anserinus is the insertion point of the medial hamstrings and would not be affected in a lateral avulsion injury. The posterior cruciate ligament may be seen on a lateral view if associated with an avulsion fragment, but a tear of the PCL generally cannot be diagnosed on an AP view. The insertion of the iliotibial band is broad and is unlikely to produce an avulsion injury such as that seen in the radiograph. This view is not consistent with the appearance of a lateral collateral ligament injury. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 533-557.
Question 491
High Yield
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
Although technically challenging, the Ganz periacetabular osteotomy offers advantages over other rotational pelvic osteotomies. Posterior column integrity is maintained, as is the acetabular vascular supply. Free mobility of the fragment makes large corrections in the center edge angle possible. Because of the asymmetric cuts and the need to restore anterior coverage, there is a tendency to anterior displacement of the joint while flexing the acetabulum. The procedure is commonly performed through a Smith-Petersen incision. Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 492
High Yield
A left-handed 23-year-old man who fell 5 feet from a ladder onto his left elbow sustained the closed injury shown in Figure 26. Management should consist of

Explanation
The radiographs reveal a displaced olecranon fracture. To maximize joint congruity of this intra-articular injury, open reduction and internal fixation is the treatment of choice. A tension band plate will assist with maintenance of the reduction and may aid in early range of motion because injuries to the elbow are prone to stiffness. The oblique fracture line is particularly well suited to plate fixation. Percutaneous pin fixation is unlikely to achieve anatomic joint reduction that can be obtained with open means. External immobilization will not accomplish joint reduction and will most likely lead to a nonunion. Hotchkiss RN: Fractures and dislocations of the elbow, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 929-1024. Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Question 493
High Yield
Which of the following procedures is considered most appropriate in patients with rheumatoid arthritis?

Explanation
Synovectomy of the knee prior to loss of articular cartilage has been shown to consistently relieve pain in patients with rheumatoid arthritis. Partial knee replacement will not arrest the process of joint destruction. Osteotomy of the hip has not been found to be a successful procedure in patients with rheumatoid arthritis. Hip arthrodesis should not be considered because of the multiarticular involvement in patients with rheumatoid arthritis. Core decompression of the hip has not been shown to save the femoral head because the necrosis appears to occur simultaneously with the inflammatory joint process. Granberry WM, Brewer EJ Jr: Early surgery in juvenile rheumatoid arthritis, in Calundruccio RA (ed): Instructional Course Lectures XXIII. St Louis, MO, CV Mosby, 1974, pp 32-37.
Question 494
High Yield
Figures 20a through 20d show the radiographs and MRI scans of a 59-year-old woman who has had symptoms consistent with progressive neurogenic claudication and back pain for the past 9 months. In the last 6 months, nonsurgical management consisting of nonsteroidal anti-inflammatory drugs, physical therapy, and a series of epidural steroid injections have been used; however the injections, while beneficial, have provided only temporary relief of her symptoms. What is the most appropriate management at this time?


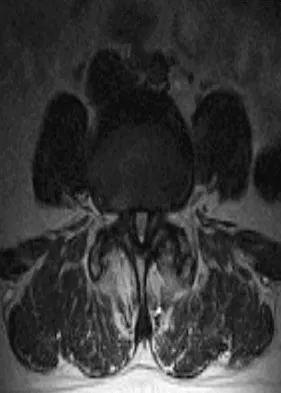

Explanation
Patients with a degenerative spondylolisthesis and severe stenosis who have failed appropriate nonsurgical management are candidates for surgical intervention. Most studies show good to excellent results in more than 85% of patients after lumbar decompression for stenosis. Atlas and associates found that at 8- to 10-year follow-up, leg pain relief and back-related functional status were greater in those patients opting for surgical treatment of the stenosis. Similarly, the decision to fuse a spondylolisthetic segment has been supported in the literature. Herkowitz and Kurz compared decompressive laminectomy alone and decompressive laminectomy with intertransverse arthrodesis in 50 patients with single-level spinal stenosis and degenerative spondylolisthesis. They demonstrated good to excellent results in 90% of the fused group compared to 44% in the nonfusion group. The decision to include instrumentation during the fusion is more controversial. Whereas the use of instrumentation has shown to improve fusion rates, it has not been conclusively shown to improve the overall clinical outcomes of patients. Atlas SJ, Keller RB, Wu YA, et al: Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the Maine lumbar spine study. Spine 2005;30:936-943. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intratransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-808.
Question 495
High Yield
What is the primary indication for performing an arthroscopic synovectomy on a patient with hemophilia that is the result of factor VIII deficiency?
Explanation
Improved medical management has changed musculoskeletal outcomes for individuals with hemophilia. Patients with severe hemophilia receiving prophylactic administration of factor VIII may never develop a target joint that requires further orthopaedic intervention. Patients with moderate hemophilia and those patients with severe hemophilia not receiving prophylactic treatment will still develop joints that have recurrent hemarthroses. When recurrent hemarthrosis continues despite optimal medical management, synovectomy is indicated. While synovectomy is predictable in its ability to decrease joint bleeding, it does not necessarily improve joint range of motion or prevent the development of hemophilic arthropathy over time. It will not reverse articular damage to the joint once it has developed. Dunn AL, Busch MT, Wyly JB; et al: Arthroscopic synovectomy for hemophilic joint disease in a pediatric population. J Pediatr Orthop 2004;24:414-426.
Question 496
High Yield
What is the most common foot deformity associated with myelomeningocele?

Explanation
All of the above can be associated with myelomeningocele, but talipes equinovarus occurs in 50% to 90% of patients with myelomeningocele. Congenital vertical talus is rarely associated with any neuromuscular diseases other than myelomeningocele but is not the most common deformity in myelomeningocele. Stans AA, Kehl DK: The pediatric foot, in Baratz ME, Watson AD, Imbriglia JE (eds): Orthopaedic Surgery: The Essentials. New York, NY, Thieme, 1999, pp 702-703.
Question 497
High Yield
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of

Explanation
Near complete correction and rebalancing of the spine can be achieved by hemivertebral resection that may be done as either a simultaneous or a staged procedure in the young patient. This eliminates the problem of future progression and possible development of compensatory curves. Nonsurgical management is not indicated in congenital scoliosis. Convex hemiepiphyseodesis is best suited for patients younger than age 5 years who have a short curve caused by fully segmented hemivertebrae that correct to less than 40 degrees with the patient supine. Hemiepiphyseodesis and isolated posterior fusion are not indicated. Bradford DS, Boachie-Adjei O: One-stage anterior and posterior hemivertibral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am 1990;72:536-540.
Question 498
High Yield
A 62-year-old patient with rheumatoid arthritis has had pain and instability of the elbow following total elbow replacement 2 years ago. A complete work-up, including aspiration and cultures, is negative. Figures 9a and 9b show the AP and lateral radiographs. Treatment should consist of


Explanation
The patient has aseptic loosening of the original semiconstrained prosthesis and significant proximal ulnar bone destruction; therefore, the treatment of choice is revision arthroplasty using a semiconstrained design. Although orthotic stabilization could be used, it will not provide long-term pain relief. Resection arthroplasty after removal of the components may lead to painful instability. Elbow arthrodesis would be difficult with the bone stock loss and is not considered the best option. Two main contraindications to the use of an unconstrained prosthesis are significant bone loss and previous use of a hinged or semiconstrained prosthesis. An ulnar allograft could be combined with the use of a semiconstrained long-stemmed ulnar prosthesis as a treatment modification. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 499
High Yield
Steroids are thought to prevent neurologic deterioration after traumatic spinal cord injury by which of the following mechanisms?
Explanation
The proposed mechanisms by which steroids such as methylprednisolone are thought to prevent neurologic deterioration by limiting secondary insult, include: decreasing the area of ischemia in the cord, reducing TNF-alpha expression and NF-kB binding activity, decreasing free radical oxidation and thus stabilizing cell and lysosomal membranes, and checking the influx of calcium into the injured cells, thus reducing cord edema. Slucky AV: Pathomechanics of spinal cord injury. Spine: State Art Rev 1999;13:409-417.
Question 500
High Yield
The acceleration of an object under the influence of a force depends directly on the mass of the object. The angular acceleration of an object under the influence of a moment depends directly on the
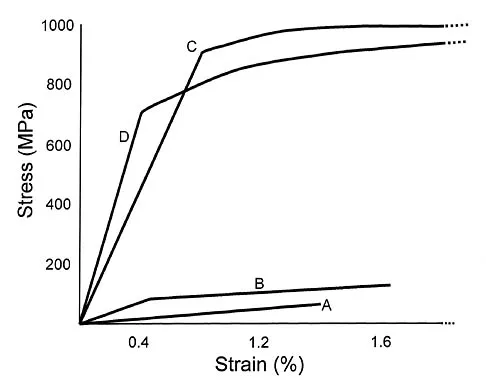
Explanation
Similar to the action of a force, a moment tends to angularly accelerate an object in a manner proportional to a quantity related to the mass of the object. The concept of a more massive object requiring a larger force to cause the same straight line acceleration is straightforward. The concept for changing angular velocity is similar but not identical. The proportional constant between the moment and the resulting angular acceleration is the mass moment of inertia, which depends not only on the mass of the object, but also its distribution. The unit of mass moment of inertia is obtained by multiplying the mass of the object by the square of the distance between an equivalent location of the center of rotation of the object and an equivalent location of the center of mass. Orthopaedic surgeons can change both the amount of mass carried by a limb and the way that the mass is distributed. For example, in applying a cast to the leg, the physician can affect the mass of the cast by the choice of casting material and by the size of the cast. As the mass moment of inertia of the limb increases (eg, by applying the cast farther down on the leg or using a heavier casting material), the patient will need to exert larger moments to angularly accelerate the leg during gait. Andriacchi T, Natarajan RN, Hurwitz DE: Musculoskeletal dynamics, locomotion, and clinical applications, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 43-47.
