HY 2026
00:00
Start Quiz
Question 301
High Yield
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of


Explanation
The patient has grade IV heterotopic ossification with the limb in an abnormal nonfunctional position. Treatment should consist of excision of the bone to restore hip motion and prophylaxis to prevent recurrent formation. The best time to excise the bone is controversial, with no conclusive evidence supporting early or late excision. Pellegrini VD Jr, Koniski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 302
High Yield
A previously asymptomatic 12-year-old girl sustained a direct blow to the right lateral knee from a baseball bat. Examination reveals an area of ecchymosis and tenderness over the lateral thigh. The patient can walk without pain, but range of motion of the knee causes discomfort. Plain radiographs of the knee are shown in Figures 11a and 11b. To address the bone lesion, management should consist of


Explanation
The plain radiographs reveal a pedunculated osteochondroma with a fracture. There is a bony growth in the metaphysis of a long bone, on a stalk that is directed away from the nearby epiphysis. On the AP view, the host cortical and medullary bone are shown as "blending" with lesional bone. There is also a fracture through the lesion. Based on these radiographic findings, the diagnosis is an osteochondroma; therefore, initial management of an acute fracture of an osteochondroma is symptomatic treatment alone. Additional imaging studies are not indicated in this patient. At times it may be difficult to distinguish a sessile osteochondroma from a parosteal osteosarcoma. In the latter case, the host medullary bone and lesion bone are not confluent. A CT scan may be helpful to distinguish if the host medullary and cortical bone are confluent with the lesion.
Question 303
High Yield
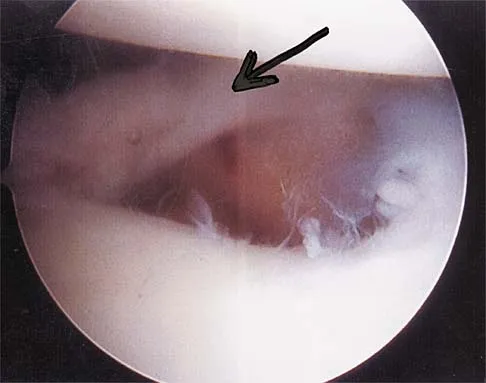
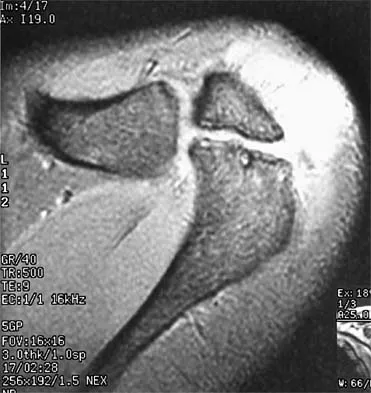
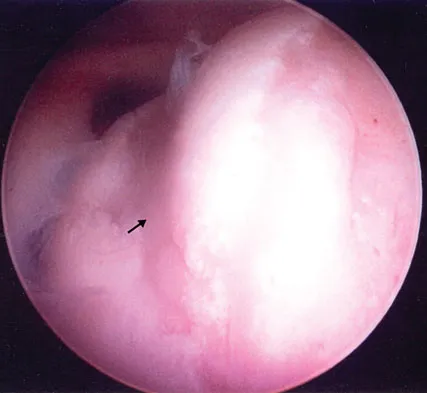
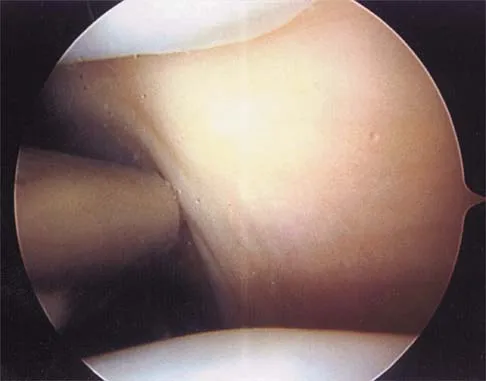
A patient has right shoulder pain. Figure 1a shows a gadolinium-enhanced transverse MRI scan at the level of the coracoid. Figure 1b shows an arthroscopic view of the anterior structures from a posterior portal. These images reveal which of the following findings?

Explanation
The area shown in the arthroscopic view and MRI scan is referred to as a Buford complex and represents a normal labral variant. It consists of a thickened, cord-like middle glenohumeral ligament, a superior labral attachment of the middle glenohumeral ligament just anterior to the biceps tendon, and absence of the anterosuperior labrum. This combination of findings can be confusing and may simulate labral pathology. Mistaken repair of the lesion back to the glenoid rim can result in significant loss of external rotation. A Bankart lesion would be located at the inferior anterior glenoid rim. The subscapularis is seen anterior to the labrum. Normal variations that occur in the anterosuperior labrum can simulate pathology. Gusmer PB, Potter HG, Schatz JA, et al: Labral injuries: Accuracy of detection with unenhanced MR imaging of the shoulder. Radiology 1996;200:519-524. Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 47-63.
Question 304
High Yield
A 20-year-old collegiate football player who sustained blunt head trauma during the first half of a game is emotional and confused. During the halftime intermission, his affect, memory, and disorientation are totally resolved and have returned to preinjury baseline. The only residual finding is a very mild headache. He wants to play the second half. What is the most appropriate course of action?
Explanation
There is almost universal acceptance that an athlete may return to play after blunt head trauma only if he or she is totally asymptomatic. Mild residual symptoms are considered an absolute contraindication for return to play. Returning to play after a cardiovascular challenge or sport-specific activities is permitted on the pretext that the athlete is totally asymptomatic prior to these maneuvers. Neuropsychiatric testing is being used more frequently to monitor residual cognitive effects after head trauma. It has not been used as a return to play criterion. Garrick J (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 29-48.
Question 305
High Yield
Where is the watershed zone for tarsal navicular vascularity?

Explanation
The central one third has been established as the watershed zone by angiographic studies, and has been borne out in clinical conditions involving the navicular, such as stress fractures and osteonecrosis. These findings account for the susceptibility to injury at this level. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 239-242.
Question 306
High Yield
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of

Explanation
The MRI scans show a mesoacromion with tendonopathy of the supraspinatus. The history and physical findings indicate that the patient has a symptomatic os acromiale. Simple excision of the unstable os acromiale has not yielded consistently good results. Meticulous internal fixation using tension banding with cannulated screws and autologous bone grafting has shown good results for this problem. Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Question 307
High Yield
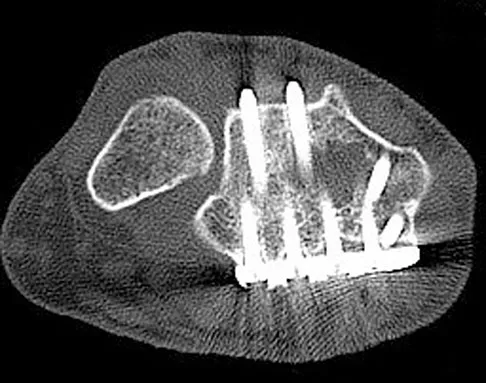
A patient is treated with volar plating for a distal radius fracture. The CT scan shown in Figure 15 is obtained after union of the fracture because the patient reports ongoing symptoms. The prominent hardware is most likely injuring what tendon?
Explanation
Extensor tendon injuries have been reported after volar plating of distal radius fractures. The CT scan shows prominent dorsal hardware a few millimeters ulnar to Lister's tubercle. The second compartment, the ECRL and ECRB, is radial to Lister's tubercle. The ECU runs along the distal ulna. The contents of the fourth dorsal compartment run just ulnar to Lister's tubercle. The EDC tendon is likely irritated in this patient. The EPB runs along the radial border of the radius and is well away from prominent hardware. Benson EC, Decarvalho A, Mikola EA, et al: Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res 2006;451:218-222.
Question 308
High Yield
Why is tendon considered an anisotropic material?
Explanation
Anisotropic materials have mechanical properties that vary based on the direction of loading. The relative values of Young's modulus for tendon, ligament, and bone are not relevant to isotropy. The mechanical properties of tendon do change with preconditioning, but this change is related to viscoelasticity. The intrinsic mechanical properties of tendon do vary with the rate of loading, but this variance is related to viscoelasticity. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 134-180.
Question 309
High Yield
An 11-year-old boy has right shoulder pain and has been unwilling to use the arm after throwing a baseball in a Little League game 3 weeks ago. Examination reveals upper arm and shoulder tenderness with swelling. A radiograph and MRI scan are shown in Figures 27a and 27b. Management should consist of


Explanation
The radiograph is consistent with a unicameral (simple) bone cyst. The MRI scan reveals that the cyst is juxtaposed to the physis and therefore can be classified as active (latent cysts are more than 1 cm away from the physis). Active cysts are treated with aspiration and steroid injection, although repeated injections may be necessary. Curettage and bone grafting results in more reliable healing but may lead to growth arrest in active cysts. Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 945-946.
Question 310
High Yield
Figure 7 shows the AP radiograph of a 60-year-old man who has had pain in the thigh for past 6 months. History reveals that he underwent hip replacement 1 year ago. The radiographic changes are most likely the result of what process?

Explanation
The arrows in the radiograph point to circumferential radiolucencies that strongly support the diagnosis of septic loosening. Radiolucent lines that occur in such a short time are also typical of an infection. Garvin KL, Hanssen AD: Infection after total hip arthroplasty: Past, present, and future. J Bone Joint Surg Am 1995;77:1576-1588.
Question 311
High Yield
An otherwise healthy 25-year-old man sustained a wound with a 1-cm by 1.5-cm soft-tissue loss over the volar aspect of the middle phalanx of his middle finger. After appropriate debridement and irrigation, the flexor digitorum profundus tendon and neurovascular bundles are visible. The wound should be treated with a

Explanation
The wound described indicates loss of soft tissue directly to the level of the tendon, precluding use of skin grafts if excursion of the tendon is desired. A cross-finger flap is ideal for small wounds on the volar aspect of digits. A thenar flap is suitable for tip injuries. A lateral arm flap will not reach the fingers. A Moberg flap is limited to distal injuries of the thumb. Kappel DA, Burech JG: The cross-finger flap: An established reconstructive procedure. Hand Clin 1985;1:677-683.
Question 312
High Yield
Baseball pitchers who have internal impingement will most likely demonstrate what changes in range of motion?

Explanation
Pitchers tend to have a decrease in internal rotation and an increase in external rotation. The increase in external rotation is felt to be multifactorial. An increase in humeral retroversion occurs from repeated throwing. This results in increased soft-tissue stretching and results in a posterior capsular contracture. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Question 313
High Yield
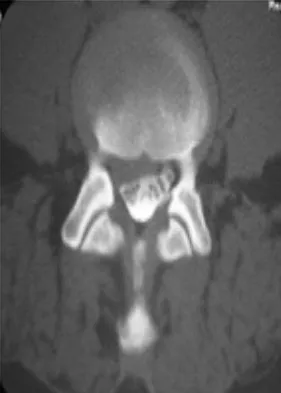
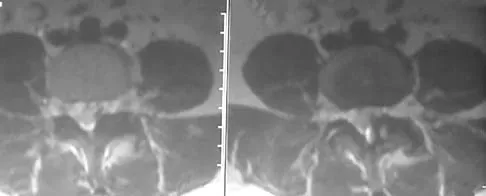
Thoracic disk herniations are most frequently found in what area of the spine?
Explanation
Although thoracic disk herniations have been reported at all levels of the thoracic spine, more than two thirds are found at T9-T12, which is the more mobile lower third of the thoracic region. Belanger TA, Emery SE: Thoracic disc disease and myelopathy, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 855-864.
Question 314
High Yield
What is the most common malignant tumor of the foot?
Explanation
Whereas chondrosarcoma is the most frequently occurring malignant bone tumor of the foot and synovial sarcoma is the most common soft-tissue foot malignancy, the most common malignant tumor overall is melanoma. It constitutes approximately 25% of lesions found on the lower extremity. Furthermore, 31% of all melanomas arise in the foot. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 11-26.
Question 315
High Yield
The first branch of the lateral plantar nerve innervates the
Explanation
The first branch of the lateral plantar nerve innervates the abductor digiti quinti, and more distal branches of the lateral plantar nerve supply the quadratus plantae and the interossei. The medial plantar nerve supplies the abductor hallucis brevis and the flexor digitorum brevis. Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Question 316
High Yield
What is the most common complication requiring reoperation after dorsal plating for a distal radius fracture?
Explanation
The most common complication of dorsal plating is extensor tenosynovitis, which often causes pain and is a frequent reason for hardware removal. Other less frequent complications include loss of reduction and extensor tendon ruptures, with flexor tendon ruptures occuring to an even lesser degree. Rozental TD, Beredjiklian PK, Bozentka DJ: Functional outcome and complications following two types of dorsal plating for unstable fractures of the distal part of the radius. J Bone Joint Surg Am 2003;85:1956-1960.
Question 317
High Yield
A 12-year-old boy sustained a grade III open tibial fracture 1 week ago and underwent multiple debridements and fracture fixation. He now has a soft-tissue defect that measures 6 cm x 6 cm, with an area of exposed bone and muscle on the distal medial leg that is a few centimeters proximal to the ankle. Management of the soft-tissue defect should now consist of

Explanation
The soft-tissue defect is in a very difficult position - the distal tibia. The defect is too distal for a gastrocnemius flap, and the exposed bone precludes an immediate skin graft. A free flap and skin graft would be required for closure. VAC is very effective in soft-tissue defects such as this one. Healthy granulation tissues form quickly. VAC can be the definitive treatment, or it can be used before skin grafting. Wet-to-dry dressings could promote granulation, but the process is hastened substantially by VAC. Amputation is not a consideration because there are no signs of infection or fracture healing problems at this time. Mooney JF III, Argenta LC, Marks MW, et al: Treatment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Orthop 2000;376:26-31.
Question 318
High Yield
A 57-year-old woman with diabetes mellitus has purulent drainage from a lateral incision after undergoing open reduction and internal fixation of a displaced ankle fracture 10 days ago. Examination reveals moderate erythema and a foul odor coming from the wound. Cultures are obtained. What is the next most appropriate step in management?
Explanation
Early postoperative wound infections after open reduction and internal fixation should be treated with aggressive debridement and maintenance of stability of the fracture. If infection persists following healing of the fracture, the hardware should be removed. Carragee EJ, Csongradi JJ, Bleck EE: Early complications in the operative treatment of ankle fractures: Influence of delay before operation. J Bone Joint Surg Br 1991;73:79-82.
Question 319
High Yield
Which of the following tumors have characteristic chromosomal translocations?

Explanation
Ewing's sarcoma has an 11;22 translocation that creates the EWS/FLI1 fusion gene, and synovial sarcoma has an X;18 translocation that creates the STT/SSX fusion gene. The other tumors do not have consistent translocations. Sandberg AA: Cytogenetics and molecular genetics of bone and soft-tissue tumors. Am J Med Genet 2002;115:189-193.
Question 320
High Yield
A 30-year-old elite marathon runner reports chronic pain over the lateral aspect of the distal right leg and dysesthesia over the dorsum of the foot with active plantar flexion and inversion of the foot. Examination reveals a tender soft-tissue fullness approximately 10 cm proximal to the lateral malleolus. The pain is exacerbated by passive plantar flexion and inversion of the ankle. There is also a positive Tinel's sign over the site of maximal tenderness. There is no motor weakness, and deep tendon reflexes are normal. Radiographs and MRI of the leg are normal. What is the next most appropriate step in management?
Explanation
The patient has entrapment of the superficial peroneal nerve against its fascial opening in the distal leg. It is typically exacerbated by passive or active plantar flexion and inversion of the foot, which leads to traction of the nerve as it exits this opening. Treatment involves release of the fascial opening to reduce this traction phenomenon. Closure of the defect will only aggravate the condition and potentially result in an exertional compartment syndrome. A four-compartment fasciotomy is only indicated for an established compartment syndrome of the leg. Styf J: Diagnosis of exercise-induced pain in the anterior aspect of the lower leg. Am J Sports Med 1988;16:165-169. Sridhara CR, Izzo KL: Terminal sensory branches of the superficial peroneal nerve: An entrapment syndrome. Arch Phys Med Rehabil 1985;66:789-791.
Question 321
High Yield
The lateral arm flap is based on what arterial supply?
Explanation
The lateral arm flap is based on the posterior radial collateral artery, a branch of the profunda brachial artery. Katsaros J, Tan E, Zoltie N: The use of the lateral arm flap in upper limb surgery. J Hand Surg 1991;16:598-604.
Question 322
High Yield
Figure 4a shows the radiograph of a 20-year-old man who has an injury to the right shoulder. Figure 4b shows an arthroscopic view (posterior portal). The arrow points to a

Explanation
The radiograph shows an anterior dislocation of the shoulder. A frequently encountered sequela of this is a compression fracture of the posterolateral humeral head, commonly referred to as a Hill-Sachs defect. The arthroscopic view of the glenohumeral joint visualizes the posterior aspect of the humeral head. In the image, the area devoid of cartilage to the right is the bare area. The indentation seen to the left is a Hill-Sachs defect. Matsen FA, Thomas SC, Rockwood CA, et al: Glenohumeral instability, in Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 611-754.
Question 323
High Yield
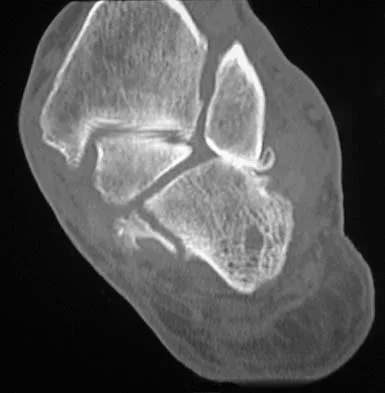
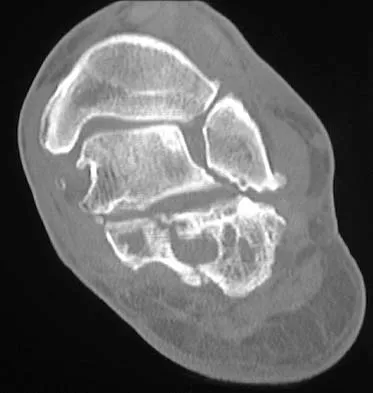
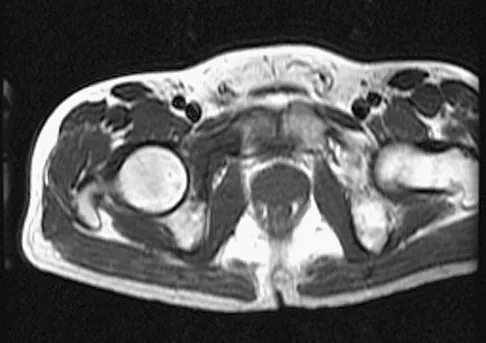
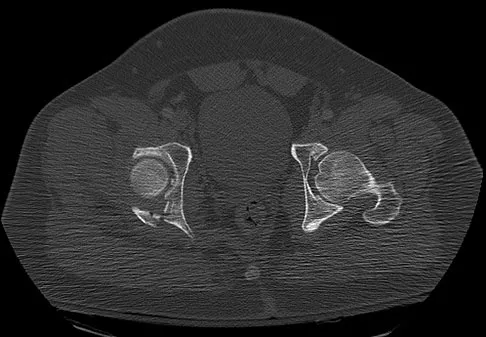
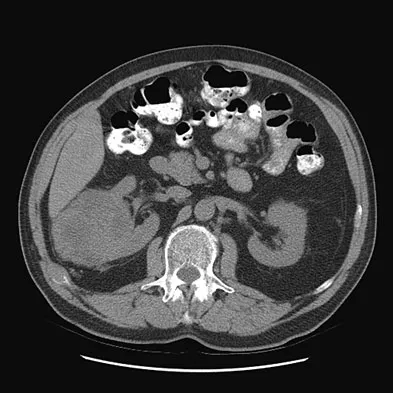
Figures 38a and 38b show the CT scans of a 64-year-old woman. What is the most likely diagnosis?
Explanation
The CT scans show large cystic lesions in the talus and calcaneus with complete subluxation of the subtalar joint, allowing the calcaneus to slide laterally until it becomes blocked by the fibula. The cause of this subluxation is severe posterior tibial tendon dysfunction. Although no fibular fracture has yet appeared, it can occur with continued stress from the calcaneus. There is, however, a pathologic fracture in the medial calcaneus through a medial degenerative cyst. The joint space is irregular and not symmetrical as would be seen in an inflammatory arthropathy. Cystic lesions are not present in the tibia. No stress fracture is seen in the talus. Coughlin MJ: Sesamoids and accessory bones of the foot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 437-499.
Question 324
High Yield
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
Distal radial physeal stress syndrome has been reported in up to 25% of nonelite gymnasts showing premature closure of the distal radial physis and distal ulnar overgrowth, producing positive ulnar variance. The diagnosis should be suspected when there is tenderness at the distal radial physis in a young gymnast. The pathology is thought to be the result of repetitive compressive stresses caused by upper extremity weight-bearing forces. The recommended treatment is 3 to 6 months of rest. Salter-Harris fractures with a distal radial epiphyseal slip are unlikely, especially in the absence of a specific traumatic event. Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Question 325
High Yield
A 67-year-old patient seen in the emergency department reports the acute onset of pain and is unable to ambulate. History reveals that the patient underwent surgical treatment for a periprosthetic femoral fracture 6 months ago. A radiograph is shown in Figure 41. What is the best treatment option at this time?

Explanation
The radiograph reveals a periprosthetic fracture at the tip of the stem with a stable cemented implant. This is classified as a Vancouver type B1 periprosthetic fracture. An attempt at internal fixation has already failed; therefore, the most predictable results would be achieved with distal fixation. After removal of the well-fixed cemented implant, the proximal bone may not be suitable for proximal fixation. Adequate bone stock is available such that an allograft prosthetic composite or a tumor prosthesis is not necessary. The best option is a long stem implant with distal fixation, which serves as an intramedullary device to restore alignment and increase the likelihood of union. Cortical onlay strut grafts are used as an adjunct to definitive fixation. Younger AS, Dunwoody I, Duncan CP: Periprosthetic hip and knee fractures: The scope of the problem. Inst Course Lect 1998;47:251-256.
Question 326
High Yield
Figures 7a and 7b show the radiographs of a 51-year-old woman who injured her left leg after falling off a stepladder. Surgical reconstruction is performed with a compression screw and side plate; the postoperative radiograph is shown in Figure 7c. Following gradual progression of weight bearing, she reports that she slipped again and placed full weight on the extremity. She now notes a new onset of increased pain in her left thigh and hip region. Follow-up radiographs are shown in Figures 7d and 7e. Reconstruction should consist of





Explanation
The initial fracture was an unstable reverse oblique intertrochanteric fracture with subtrochanteric extension. Initial fixation with a high-angled screw and side plate construct may not provide stability as well as a 95 degree fixed-angle device or a intramedullary hip screw device. The follow-up radiographs show loss of fixation and further propagation of the fracture distally. Reconstruction would best be accomplished with hardware removal and conversion to a long intramedullary nail with femoral head fixation or a 95 degree angled plate and screw device. Conversion to a longer plate does not improve the biomechanical situation at the primary fracture site. In situ bone grafting would not provide any additional stability and would not correct the deformity. The proximal femoral fracture is not amenable to retrograde nailing. Cerclage wiring will not sufficiently enhance stability and is not indicated. Bridle SH, Patel AD, Bircher M, Calvert PT: Fixation of intertrochanteric fractures of the femur: A randomized prospective comparison of a gamma nail and dynamic hip screw. J Bone Joint Surg Br 1991;73:330-334. DeLee JC: Fractures and dislocations of the hip, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green's Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1659-1825. Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Question 327
High Yield
Figure 38a shows the radiograph of a 12-year-old boy who underwent a reamed intramedullary nailing for a closed femoral shaft fracture. One year after rod removal, he reports groin pain. A current radiograph is shown in Figure 38b. The findings are most likely the result of


Explanation
Osteonecrosis of the femoral head is a known complication from the use of rigid intramedullary nails for femoral fractures in adolescents. When the nails are placed through the piriformis fossa, the lateral ascending vessels of the femoral neck may be injured, resulting in osteonecrosis of the femoral head in 1% to 2% of patients. Rigid reamed nails placed into the piriformis fossa are contraindicated in children with open growth plates because the physis is a barrier to blood supply and the ligamentum teres does not provide sufficient vascularity. Alternative fixation methods for femoral fractures in adolescents include external fixation and open reduction and internal fixation. Nailing through the tip of the trochanter may decrease the incidence of this serious complication. Letts M, Jarvis J, Lawton L, et al: Complications of rigid intramedullary rodding of femoral shaft fractures in children. J Trauma 2002;52:504-516. Stans AA, Morrissy RT, Renwick SE: Femoral shaft fracture treatment in patients age 6 to 16 years. J Pediatr Orthop 1999;19:222-228. Buckley SL: Current trends in the treatment of femoral shaft fractures in children and adolescents. Clin Orthop 1997;338:60-73.
Question 328
High Yield
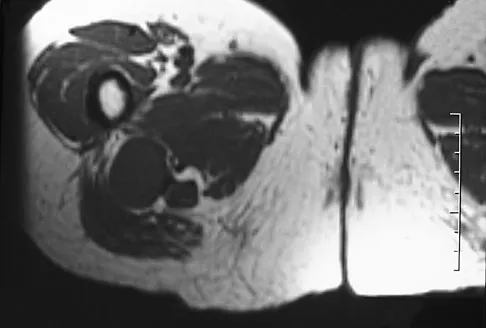
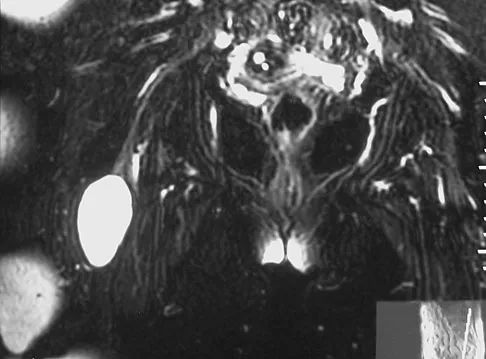
Which of the following choices best describes the fracture pattern shown in Figures 2a through 2c?



Explanation
The fracture pattern shown in the radiographs is a fracture of the posterior column. The only line interrupted on the AP pelvis is the ilioischial line. The obturator oblique view shows that the iliopectineal line is intact as is the outline of the posterior wall. The iliac oblique view shows an interruption of the ilioischial line and an intact anterior wall. Therefore, this fracture is a fracture of the posterior column. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Question 329
High Yield
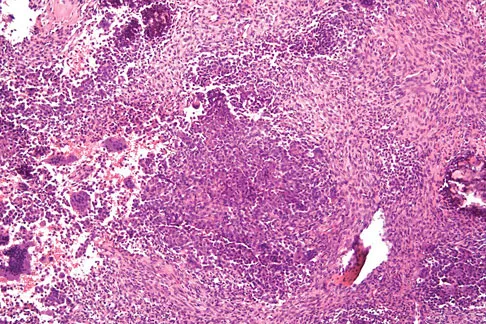
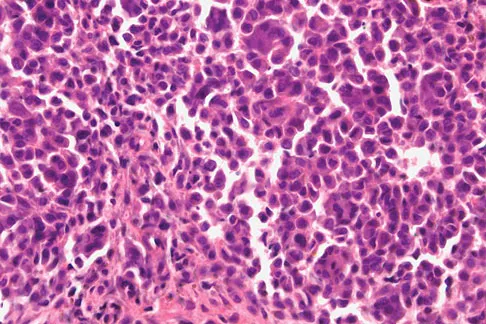
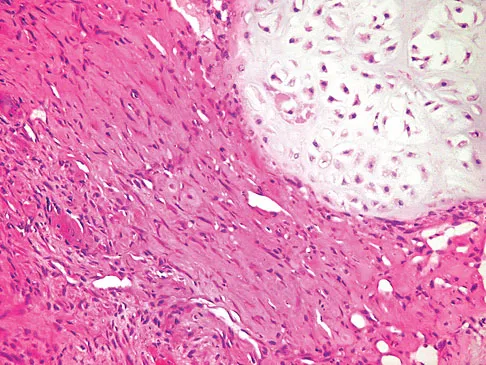
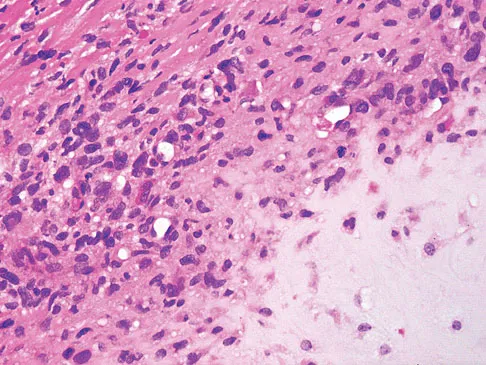
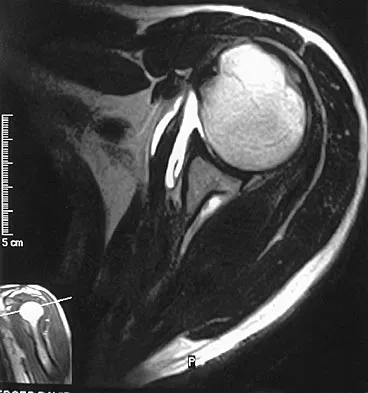
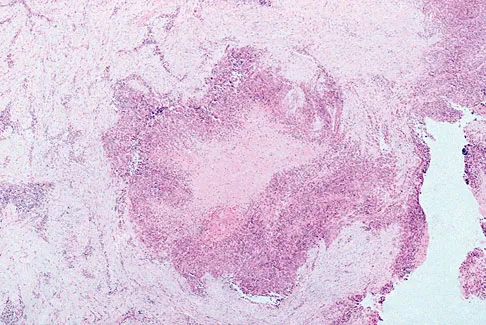
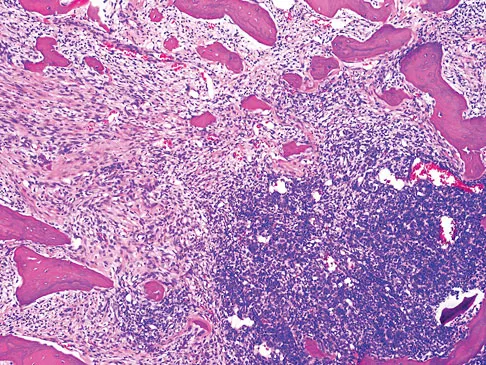
Figures 12a through 12e show the radiograph, MRI scans, and biopsy specimens of a 17-year-old boy. What is the most likely diagnosis?


Explanation
The images show an epiphyseal lesion. The MRI scan shows extensive bone edema surrounding the lesion, consistent with chondroblastoma. Histology shows polygonal chondroblasts in a cobblestone-like pattern and areas of calcification consistent with chondroblastoma. Although some giant cells are seen, the age of the patient and the polygonal chondroblasts differentiate this lesion from giant cell tumor. Clear cell chondrosarcoma is an epiphyseal lesion that occurs in an older population, and the cells have clear cytoplasm. This lesion is not producing bone on imaging or histologic specimen, eliminating osteosarcoma. Tuberculous septic arthritis can be an epiphyseal lesion, but granulomas would be seen on histology. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 103-111.
Question 330
High Yield
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of

Explanation
Excision of the affected mucoid degenerative area is considered appropriate management in the Blazina classification system. A finding of phase III indicates persistent pain with or without activities, as well as deterioration of performance. With the appearance of the mucoid degeneration and the vigorous activity level of the intercollegiate basketball player, it is unlikely that nonsurgical management will provide adequate relief. When excising the affected degenerative area, care must be taken to retain normal tendon fibers. The defect in the patellar tendon is closed with absorbable sutures, as is the paratenon. Postoperative rehabilitation involves initial mobilization extension, with progressive range-of-motion and mobilization exercises as tolerated and weight bearing as tolerated. Open chain and isokinetic exercises are delayed until full range of motion and mobility is obtained, generally within 4 weeks. A return to activities is achieved by 80% to 90% of athletes, although there may be occasional activity-related aching for 4 to 6 months after surgery. Blazina ME, et al: Jumper's knee. Orthop Clin North Am 1973;4:665. Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper's knee. Am J Sports Med 1984;12:375-380. Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Question 331
High Yield
A 45-year-old woman who recently underwent biopsy of a lymph node in the right posterior cervical triangle now finds it difficult to hold objects overhead and has diffuse aching in the right shoulder region. What is the most likely diagnosis?
Explanation
The trapezius is innervated by the spinal accessory nerve. The nerve is superficial in the area of the posterior cervical triangle and is prone to injury during dissection. Paralysis of the trapezius causes loss of scapular stability when forward flexion or abduction of the shoulder is attempted. Vastamaki M, Solonen KA: Accessory nerve injury. Acta Orthop Scand 1984;55:296-299.
Question 332
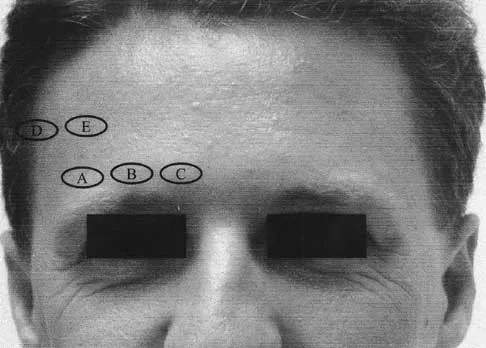
High Yield
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include "onion bulb" formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?
Explanation
The patient has HMSN-III or Dejerine-Sottas syndrome. This form of HMSN progresses very rapidly and frequently results in severe foot deformity in early childhood. The changes are progressive and are the result of muscle imbalance during growth. Balancing of the foot musculature is essential, particularly during the phases of rapid growth of the foot. However, this cannot be accomplished using the anterior tibial muscle because it is already weak and the transfer will further weaken it. Bony procedures also may be required, and tendon transfers cannot be depended on to correct bony deformity. However, these procedures can be deferred until the foot is closer to adult size. Surgeries that lead to joint arthrodesis, such as triple arthrodesis and some midfoot osteotomies, are contraindicated because the feet may lose protective sensation as the disease progresses. Fusions in insensate feet are less successful than realignment procedures that maintain mobility. Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Question 333
High Yield
A 39-year-old woman fell onto her flexed elbow and sustained a comminuted displaced radial head and neck fracture. Radiographs confirm concentric reduction of the ulnohumeral joint. Examination reveals pain with compression of the radius and ulna at the wrist. What is the best treatment for the radial head fracture?
Explanation
Patients with comminuted radial neck and head fractures and associated wrist pain have a significant injury to the elbow and forearm. Nonsurgical management is an option, but initial casting will result in stiffness and early range of motion is likely to be unsuccessful secondary to pain. Surgical treatment with open reduction and internal fixation, although possible, is technically demanding and results are unpredictable with comminuted fractures. Excision alone in the face of wrist pain may lead to radial shortening. The treatment of choice is excision and metallic radial head arthroplasty. Silastic implants have been associated with synovitis and wear debris. Furry KL, Clinkscales CM: Comminuted fractures of the radial head: Arthroplasty versus internal fixation. Clin Orthop 1998;353:40-52.
Question 334
High Yield
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?

Explanation
The radiographic appearance of the joint is highly suspicious for neuropathic joint (Charcot's joint). Evidence of bone loss on both the tibial and the femoral sides may necessitate the use of metal and/or bone augments. Patients with a neuropathic joint often have excellent range of motion, and postoperative stiffness is not a problem. The main problem with these patients is instability that occurs secondary to ligamentous laxity. Use of a semiconstrained prosthesis prevents the latter complication. Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Question 335
High Yield
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of

Explanation
The radial head is an important secondary stabilizer of the elbow, helping to resist valgus forces. There has been a movement toward open reduction and internal fixation of the radial head when technically feasible, especially in a relatively high-demand athlete or laborer. The examination and radiograph suggest that displacement of the fragment is great enough to create a mechanical block. Extended splinting would only serve to encourage arthrofibrosis. Early range of motion is appropriate if there is minimal displacement of the radial head fragement, it is stable, and there is no mechanical block to motion. Fragments larger than one third of the joint surface should be excised only if it is not possible to reduce and repair the fragment. Primary excision of the radial head should be avoided if possible. Complications after excision of the radial head include muscle weakness, wrist pain, valgus elbow instability, heterotopic ossification, and arthritis. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Question 336
High Yield
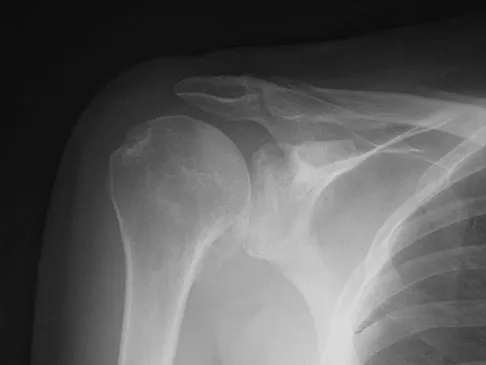
A 70-year-old man who underwent an uncomplicated large rotator cuff repair 6 months ago is now seeking a second opinion regarding persistent pain and weakness in his shoulder. Examination reveals that his incision is well healed and unreactive. The surgical report suggests that the tendons were secured back to bone with sutures through the greater tuberosity. Figure 28 shows a radiograph that was obtained 1 week ago. What is the most likely diagnosis?

Explanation
Symptoms can persist following a rotator cuff repair for a variety of reasons. In the early postoperative period, infection is the primary concern. Stiffness and loss of motion can occur because of postoperative scarring. Complex regional pain syndrome can occur but is rare, and the diagnosis is not made with a plain radiograph. This radiograph shows a superiorly migrated humeral head that articulates with the acromion, indicating that the repair has failed. While large to massive tears may fail more commonly than once thought, the clinical outcome may be satisfactory in many patients. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213.
Question 337
High Yield
Figures 37a and 37b show radiographs of a 24-year-old man who has a humeral bone lesion that was found during a screening chest radiograph. He denies any symptoms despite leading a very active lifestyle. What is the most likely diagnosis?


Explanation
The radiographs reveal a geographic, diaphyseal lesion with very subtle cortical expansion, cortical thinning, relatively sharp demarcation, and angular rather than rounded borders, suggesting a fibrous bone lesion. This lesion demonstrates the classic ground glass appearance of fibrous dysplasia. Ewing's sarcoma, metastases, and aneurysmal bone cyst all typically have a more aggressive appearance. Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Question 338
High Yield
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of

Explanation
Based on the history, examination, and radiograph, the patient has typical degenerative arthritis of the elbow. This condition is found almost exclusively in men, and there is almost universally a history of repetitive heavy use or overuse of the elbow. Patients report pain at terminal extension and usually have a flexion contracture. Radiographs reveal osteophytes on the coronoid and olecranon and in the coronoid and olecranon fossae. The osteophytes are often associated with loose bodies that sometimes are attached to the soft tissues. Treatment should consist of removal of all loose bodies and impinging osteophytes using open technique or by arthroscopy. The capsular contractures should be released at the same time. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294. Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413. Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
Question 339
High Yield
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?


Explanation
The definitive surgery would be removal of the entire resection bed, and in this case of dedifferentiated chondrosarcoma, a hemipelvectomy was performed. The MRI and CT scans show an aggressive cartilage lesion. The histology, representative of a dedifferentiated chondrosarcoma, shows a bimorphic low-grade cartilage lesion with high-grade spindle cell sarcoma. The cartilage lesion is usually an enchondroma or low-grade chondrosarcoma. The dedifferentiated portion is typically a malignant fibrous histocytoma, osteosarcoma, or fibrosarcoma. Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Question 340
High Yield
A 50-year-old man with no history of trauma reports new-onset back pain after doing some yard work the previous day. He reports pain radiating down his leg posteriorly and into the first dorsal web space of his foot. MRI scans are shown in Figures 3a through 3c. What nerve root is affected?


Explanation
The MRI scans clearly show an extruded L4-5 disk that is affecting the L5 nerve root on the left side. In addition, the L5 nerve root has a cutaneous distribution in the first dorsal web space. S1 affects the lateral foot. L4 affects the medial calf.
Question 341
High Yield
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
The enthusiasm with which dorsal rhizotomy was received led to the broadening of selection criteria with poorer results. The ideal candidate is an ambulatory 4- to 8-year-old child with spastic diplegia who does not use assistive devices or have joint contractures. The child must be old enough to actively participate in the rigorous postoperative physical therapy program. The use of the procedure in an ambulatory 16-year-old patient is less desirable because joint contractures will most likely have developed to a varying degree. The hemiplegic child is best treated by orthopaedic interventions. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29. Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Question 342
High Yield
When compared with a patient who has a subluxated hip, a patient with a dislocated hip who is undergoing acetabular reconstruction for developmental dysplasia of the hip will most likely have

Explanation
The rate of revision has been found to be significantly increased in patients with a dislocated hip preoperatively compared with patients with a subluxated hip. This may be the result of compromised acetabular bone stock. The rate of nerve palsy may be increased because of the greater degree of lengthening required to reduce the reconstructed hip. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360.
Question 343
High Yield
An obese 62-year-old man reports a 10-year history of progressive flatfoot deformity and a 3-month history of a painful callus along the plantar medial midfoot that has not improved with custom shoe wear, pedorthics, and callus care. There is no hindfoot motion, but functional ankle motion remains. He does not have diabetes mellitus. Radiographs are shown in Figures 27a and 27b. What is the best surgical option at this point?


Explanation
The deformity is long-standing, the hindfoot is immobile, and the radiographs reveal severe degenerative arthritis involving the entire hindfoot, severe deformity, and talonavicular dislocation. The "exostosis" responsible for the callus is the talar head; resection would severely destabilize the foot. Degenerative arthritis and fixed deformity preclude lateral column lengthening, medial slide calcaneal osteotomy, and talonavicular arthrodesis. Triple arthrodesis is the only viable option. Johnson JE, Yu JR: Arthrodesis techniques in the management of Stage II and III acquired adult flatfoot deformity. Instr Course Lect 2006;55:531-542.
Question 344
High Yield
The need for postoperative allogeneic blood transfusions after total hip arthroplasty has been shown to be reduced when using
Explanation
In a prospective study, 216 patients were randomized into three groups consisting of low-dose preoperative erythropoietin, high-dose preoperative erythropoietin, and placebo control. All patients were treated for 4 weeks prior to total hip arthroplasty. Both the low- and high-dose erythropoietin groups had a significantly lower rate of blood transfusions (p < 0.001) after surgery. Waddell JP: Evidence-based orthopedics. J Bone Joint Surg Am 2001;83:788.
Question 345
High Yield
A 21-year-old collegiate wrestler sustains a blow to his right eye during a match. Examination reveals anisocoria with a dilated right pupil. The globe is properly formed, and extra-occular movements and the visual field are grossly intact. What is the most likely diagnosis?
Explanation
Traumatic mydriasis occurs from a contusion to the iris sphincter. This is a transient phenomenon during which the iris fails to constrict properly, resulting in a dilated pupil. More severe trauma can result in a tear of the sphincter and permanent pupillary deformity. In association with head injury, traumatic anisocoria would be a concerning indicator of the severity of injury. Retinal detachment, lens dislocation, corneal abrasion, and traumatic hyphema are all potential results of eye injury but are not reflected by this clinical description. Brucker AJ, Kozart DM, Nichols CW, Irving MR: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby Year Book, 1991, pp 650-670.
Question 346
High Yield
A 38-year-old woman with diabetes mellitus reports a 6-week history of fever and pain localized to the right sternoclavicular joint. Local signs on examination include swelling about the joint, erythema, and increased warmth. Initial aspiration of the joint reveals Staphylococcus aureus. Radiographs reveal medial clavicular osteolysis. What is the most effective treatment at this time?
Explanation
Based on the findings, the treatment of choice is resection of the sternoclavicular joint. Antibiotic therapy, repeat aspirations, hyperbaric oxygen, and simple irrigation and debridement are generally ineffective and associated with a high rate of recurrence.
Question 347
High Yield
Figure 18a shows the clinical photograph of a 31-year-old man who has a slowly growing nodule on his right middle finger. It is minimally tender, and there is no erythema on examination. A biopsy specimen is shown in Figure 18b. What is the most likely diagnosis?

Explanation
Epithelioid sarcoma is the most common soft-tissue sarcoma in the hand and most commonly occurs in young adults. The tumors can be superficial and may become ulcerated. Deeper lesions are often attached to tendons, tendon sheaths, or fascial structures. These are usually minimally symptomatic. The biopsy specimen reveals the typical appearance of a nodular pattern with central necrosis. They can mimic a necrotizing granulomatous process. Usually there are chronic inflammatory cells along the margin of the tumor nodules. This biopsy specimen does not have the clear cells necessary for a clear cell carcinoma or sarcoma. Nora's tumor is a bizarre parosteal osteochondromatous proliferation (BPOP) first described in 1983 by the pathologist, Nora. The lesion is defined as a reactive heterotopic ossification and is mostly found in the hands or feet of adults in the third decade of life. Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 1074.
Question 348
High Yield
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of


Explanation
The patient has the classic signs of Little Leaguer's shoulder, with findings that include pain localized to the proximal humerus during the act of throwing and radiographic evidence of widening of the proximal humeral physis. Examination usually reveals tenderness to palpation over the proximal humerus, but the presence of any swelling, weakness, atrophy, or loss of motion is unlikely. The treatment of choice is rest from throwing for at least 3 months, followed by a gradual return to pitching once the shoulder is asymptomatic. Carson WG Jr, Gasser SI: Little Leaguer's shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
Question 349
High Yield
What pharmacologic agents are preferred for the treatment of symptomatic active Paget's disease?

Explanation
Recent medical literature supports the use of bisphosphonates as the treatment of choice for active Paget's disease.
Question 350
High Yield
A 19-year-old college cross-country runner is amenorrheic and has recurrent stress fractures. Long-term management should consist of
Explanation
The triad of menstrual dysfunction, disordered eating, and stress fracture is well recognized in women who participate in endurance sports. The best treatment remains to be determined, but at present, the combination of oral contraceptives to regulate menses, an increased intake of calcium and vitamin D, as well as nutritional counseling, is the recommended treatment for decreased bone mass related to exercise-induced amenorrhea. Nattiv A, Armsey TD Jr: Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
Question 351
High Yield
A 68-year-old woman undergoes a complicated four-level anterior cervical diskectomy and fusion at C3-7 with iliac crest bone graft and instrumentation for multilevel cervical stenosis. Surgical time was approximately 6 hours and estimated blood loss was 800 mL. Neuromonitoring was stable throughout the procedure. The patient's history is significant for smoking. The most immediate appropriate postoperative management for this patient should include

Explanation
Airway complications after anterior cervical surgery can be a catastrophic event necessitating emergent intubation for airway protection. Multilevel surgeries requiring long intubation and prolonged soft-tissue retraction as well as preexisting comorbidities may predispose a patient to postoperative airway complications. Sagi and associates reported that surgical times greater than 5 hours, blood loss greater than 300 mL, and multilevel surgery at or above C3-4 are risk factors for airway complications. In surgical procedures with the aforementioned factors, serious consideration should be given to elective intubation for 1 to 3 days to avoid urgent reintubation. Sagi HC, Beutler W, Carroll E, et al: Airway complications associated with surgery on the anterior cervical spine. Spine 2002;27:949-953. Epstein NE, Hollingsworth R, Nardi D, et al: Can airway complications following multilevel anterior cervical surgery be avoided? J Neurosurg 2001;94:185-188.
Question 352
High Yield
Which of the following findings best describes the acetabular fracture shown in Figure 38?
Explanation
The CT scan shows a posterior wall fracture with impaction of the articular surface and a free fragment within the joint. Proper treatment of this injury requires not only reduction and fixation of the posterior wall fragment but also removal of the free fragment and elevation of the depressed articular segment. Letournel E, Judet R: Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer Verlag, 1993.
Question 353
High Yield
A 54-year-old woman reports worsening pain in her buttock, especially when sitting for long periods of time. She has occasional pain and paresthesias radiating down her posterior leg. She has no significant medical history. MRI scans are shown in Figures 15a and 15b and a biopsy specimen is shown in Figure 15c. What is the most likely diagnosis?
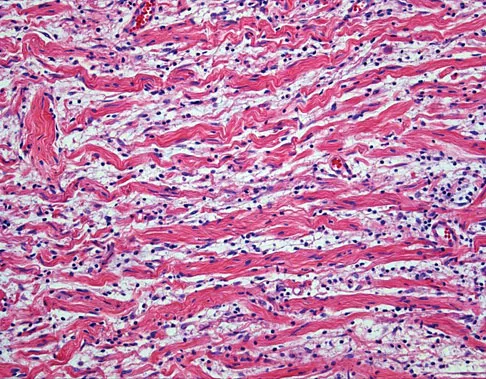
Explanation
The biopsy specimen shows a wavy collagenous matrix with elongated cells; this is most consistent with neurofibroma. The patient has a mass in the region of the sciatic nerve. Imaging characteristics, homogeneous and very low signal on T1-weighted and very high signal on the T2-weighted sequences, are consistent with a myxoid-type lesion. These include myxoma, myxoid sarcomas, and nerve sheath tumors. Campanacci M: Bone and Soft Tissue Tumors, ed 2. New York, NY, Springer-Verlag, 1999, pp 1135-1136
Question 354
High Yield
The flap shown in the clinical photograph seen in Figure 51 is based on what arterial supply?

Explanation
The groin flap is based on the superficial circumflex iliac artery, an axial flap that has been a mainstay of providing soft-tissue coverage of the upper extremity. Flaps as large as 35 cm in length and 15 cm in width have been reported. An advantage of the flap is that when used as a pedicle flap, the donor site can be closed directly. A disadvantage of the flap is that it can be quite bulky and can have a thick layer of subcutaneous fat. The superficial circumflex iliac artery travels lateral and superficial to the fascia and below and parallel to the inguinal ligament. It is helpful to elevate the fascia at the medial border of the sartorius muscle to include the deep and superficial branches of the artery for improved flap survival. McGregor IA, Jackson IT: The groin flap. Br J Plast Surg 1972;25:3-9.
Question 355
High Yield
Which of the following is considered the best cementless acetabular reconstruction method when planning for total hip arthroplasty in a patient with developmental dysplasia of the hip (DDH)?

Explanation
Anatomic positioning of the acetabular component has been shown to be the optimal position for reconstruction of the acetabulum in total hip arthroplasty for DDH. The use of medialized component positioning has been shown to be successful at maximizing the host bone coverage and minimizing the use of bone graft to structurally support the acetabular component. A small acetabular component can be used successfully as long as the femoral head is also reduced in size to maintain the thickness of the acetabular polyethylene. High and lateral positioning for the acetabular reconstruction will result in an increase in the joint reaction forces. In addition, a high and lateral placement will not provide adequate bone to stabilize the reconstruction. Numair J, Joshi AB, Murphy JC, Porter ML, Hardinge K: Total hip arthroplasty for congenital dysplasia or dislocation of the hip: Survivorship analysis and long-term results. J Bone Joint Surg Am 1997;79:1352-1360. Dorr LD, Tawakkol S, Moorthy M, Long W, Wan Z: Medial protrusio technique for placement of a porous-coated, hemispherical acetabular component without cement in a total hip arthroplasty in patients who have acetabular dysplasia. J Bone Joint Surg Am 1999;81:83-92.
Question 356
High Yield
A 46-year-old woman who was involved in a motor vehicle accident reports a 4-month history of right-sided lower back pain and pain radiating into the right thigh. The patient underwent an extensive 3-month course of physical therapy and now is dependent on narcotic medication for pain control. Epidural injection therapy has failed to improve her symptoms. Examination is significant for weakness of hip flexion in the seated position and for decreased sensation to light touch in the medial anterior thigh region. Straight leg raise is negative, but the femoral stretch test reproduces anterior thigh pain. A CT myelogram image, at L3-L4, is shown in Figure 3. What is the most appropriate management at this time?
Explanation
The CT scan reveals a right-sided lateral disk protrusion at L3-4 that has been symptomatic for more than 4 months despite appropriate nonsurgical management. Relative surgical indications include persistent radiculopathy despite an adequate trial of nonsurgical management, recurrent episodes of sciatica, persistent motor deficit with tension signs and pain, and pseudoclaudication caused by underlying stenosis. Whereas studies have shown improvement in patients with sciatica from a lumbar disk herniation treated either nonsurgically or surgically, those undergoing surgical treatment had an overall greater improvement of symptoms. Weinstein JN, Lurie JD, Tosteson TD, et al: Surgical vs nonoperative treatment for lumbar disk herniation: The Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA 2006;296:2451-2459.
Question 357
High Yield
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
The patient has spinal muscular atrophy, type 2. This type is intermediate in severity between the Werdnig-Hoffmann type (type 1) and the Kugelberg-Welander type (type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive. Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Question 358
High Yield
Figures 20a and 20b show the AP and lateral radiographs of a 62-year-old man who has had hip pain for the past 3 weeks. Figure 20c shows a CT scan of the abdomen and pelvis. A needle biopsy specimen is shown in Figure 20d. Preoperative management should include which of the following?


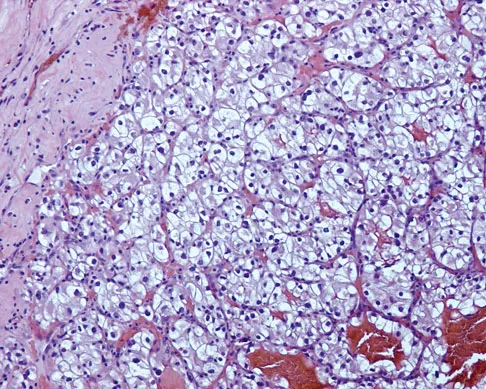
Explanation
The histology shows findings consistent with metastatic renal cell carcinoma. Renal cell carcinoma metastases are extremely vascular. Preoperative embolization helps minimize the amount of blood loss during curettage of these lesions. Chatziioannou AN, Johnson ME, Pneumaticos SG, et al: Preoperative embolization of bone metastases from renal cell carcinoma. Eur Radiol 2000;10:593-596.
Question 359
High Yield
Figure 26a shows the radiograph of a 55-year-old woman who has pain in her right leg after falling. Laboratory studies reveal an elevated alkaline phosphatase level. A biopsy specimen from the proximal tibia is shown in Figure 26b. What is the most likely diagnosis?

Explanation
Paget's disease of bone is a metabolic disorder of bone remodeling. The normally coupled process of bone resorption and deposition is lost, resulting in excessive localized bone resorption and compensatory increased bone formation. Pagetic bone tends to be more brittle; therefore, it is susceptible to pathologic fractures and subsequent deformities. Lander PH, Hadjipavlou AG: A dynamic classification of Paget's disease. J Bone Joint Surg Br 1986;68:431-438.
Question 360
High Yield
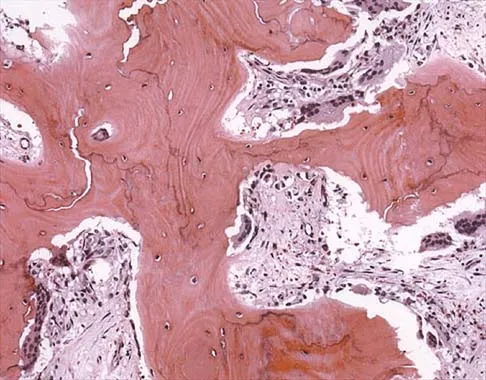
An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T1-weighted MRI scan with contrast, an angiogram, and histologies are shown in Figures 9c through 9f. What is the most likely diagnosis?


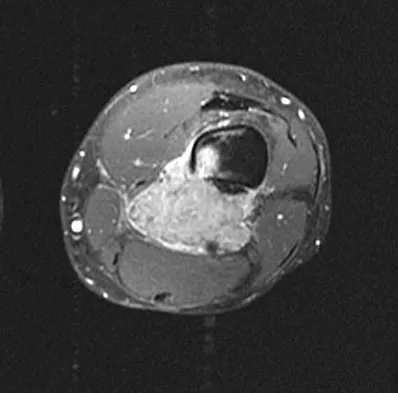
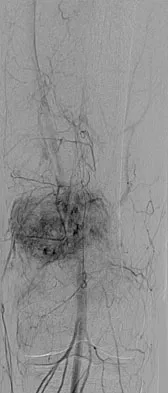
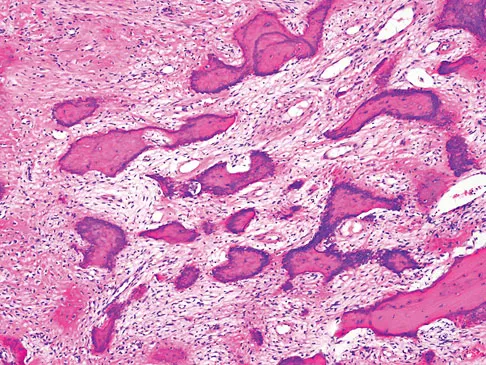
Explanation
Dedifferentiated parosteal osteosarcoma designates high-grade transformation of conventional low-grade parosteal osteosarcoma. Unlike conventional parosteal osteosarcoma, where wide surgical excision alone is considered adequate treatment, patients with dedifferentiated osteosarcoma are treated with neoadjuvant chemotherapy and wide local resection. Recognition of dedifferentiated areas with angiography can localize the area that should be biopsied and thus render an accurate diagnosis. Percutaneous biopsy of hypervascular areas should prompt the administration of chemotherapy and wide local excision to optimize patient outcome. Sheth DS, Yasko AW, Raymond AK, et al: Conventional and dedifferentiated parosteal osteosarcoma: Diagnosis, treatment, and outcome. Cancer 1996;78:2136-2145.
Question 361
High Yield
Based on the radiograph shown in Figure 4, the innervation of what muscle is most at risk with total hip arthroplasty?

Explanation
The radiograph reveals a Crowe IV deformity in a patient with developmental dysplasia of the hip. If hip arthroplasty is performed, then some degree of limb lengthening is anticipated. Excessive limb lengthening can result in sciatic nerve palsy in these patients. The peroneal branch of the sciatic nerve is most often affected. Of the muscles listed, only the extensor hallucis longus is innervated by the peroneal branch of the sciatic nerve. Eggli S, Hankemayer S, Muller ME: Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br 1999;81:843-845.
Question 362
High Yield
What is the reported failure rate for surgical treatment of a Morton's neuroma?

Explanation
The reported failure rate is in the range of 15%, which may be the result of incorrect diagnosis, improper web space selection, or formation of a stump neuroma. Therefore, the procedure should be approached with caution, measures should be taken to ensure that the diagnosis is accurate, and nonsurgical options should be exhausted. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
Question 363
High Yield
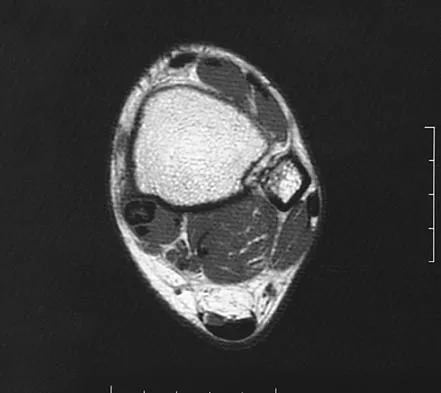
Atraumatic neuropathy of the suprascapular nerve usually occurs at what anatomic location?
Explanation
The suprascapular nerve passes through the suprascapular notch and the spinoglenoid notch before innervating the infraspinatus muscle. At both locations, the suprascapular nerve is prone to nerve compression, which often results from a ganglion cyst. The other anatomic locations are not associated with suprascapular nerve impingement. Romeo AA, Rotenberg DD, Bach BR: Suprascapular neuropathy. J Am Acad Orthop Surg 1999;7:358-367.
Question 364
High Yield
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient's symptoms at this time?
Explanation
Although many hematologic and electrolyte abnormalities may be present in a patient with advanced metastatic cancer, an elevated serum calcium level is most commonly associated with confusion. Treatment with hydration, diuretics, and bisphosphonates is recommended. Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
Question 365
High Yield
Examination of a supine patient in which the hip is abducted, externally rotated, and flexed is referred to as
Explanation
During Patrick's test, also known as the FABER test, the flexed, abducted, and externally rotated hip is positioned to isolate sacroiliac pathology. Back pain with this test is not considered diagnostic. With Kernig's sign, the spinal cord is placed on stretch, eliciting root or meningeal irritation by forcibly flexing the patient's head and neck with his or her hands clasped behind the head. For Lasegue's sign, the patient performs a straight leg raise with the immobile hip already held in flexion. The femoral stretch test can be performed in the prone position or side lying, but the hip is held in extension while the knee is flexed, testing for femoral neuritis. Watkins RG: History, physical examination, and diagnostic tests for back and lower extremity problems, in Watkins RG (ed): The Spine in Sports. St Louis, MO, Mosby, 1996, Chapter 7.
Question 366
High Yield
Figure 33a shows a line drawing of a normal hemipelvis. The anterior acetabular rim is bold. Figure 33b illustrates a hemipelvis with a crossover sign, which is indicative of what acetabular pathology?
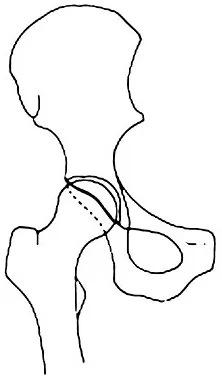
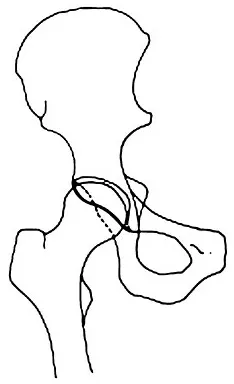
Explanation
In a normal AP pelvis radiograph, the anterior rim of the acetabulum runs medially and distally, diverging from the posterior rim which runs much more vertically. In excessive acetabular retroversion, the anterior rim (bold line in Figure 33b) and posterior rim start laterally, and as these lines progress medially and distally, the anterior line crosses the posterior line. This predisposes to femoral acetabular impingement. Reynolds D, Lucas J, Klaue K: Retroversion of the acetabulum: A cause of hip pain. J Bone Joint Surg Br 1999;81:281-288.
Question 367
High Yield
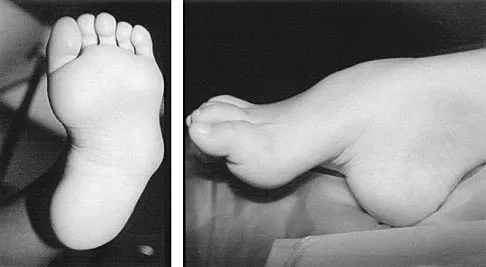
A 7-month-old girl has had a severe flatfoot deformity since birth. The talar head is prominent in the medial plantar arch of the foot. No other deformities of the spine or extremities are present. Motor and sensory examinations of the extremities are normal. Figures 37a through 37c show simulated weight-bearing AP and lateral radiographs and a planter flexion lateral view. What is the most likely diagnosis?



Explanation
Congenital vertical talus is a fixed dorsal dislocation of the talonavicular joint with equinus of the ankle joint. The AP radiograph shows valgus of the midfoot and an increased talocalcaneal angle; the lateral radiograph shows a vertically positioned talus and equinus of the ankle joint, and the plantar flexion lateral view shows that the talonavicular joint does not reduce. A line drawn through the long axis of the talus passes below the long axis of the first metatarsal. Initial management should consist of serial casting to stretch the dorsal soft-tissue structures; surgery eventually will be required to reduce the talonavicular joint. The differential diagnosis of congenital vertical talus includes pes calcaneovalgus, flexible pes planus, and peroneal spastic flatfoot. Pes calcaneovalgus, flexible pes planus, congenital short Achilles tendon, and peroneal spastic flatfoot would not show resistent dorsal dislocation of the navicular on the plantar flexion view. Kodros SA, Dias LS: Single-stage surgical correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Question 368
High Yield
A 32-year-old woman with systemic lupus erythematosus treated with methotrexate and oral corticosteroids reports right groin pain with ambulation and night pain. Examination reveals pain with internal and external rotation and flexion that is limited to 105 degrees because of discomfort. Laboratory studies show a serum WBC of 9.0/mm3 and an erythrocyte sedimentation rate of 35 mm/h. Figures 5a and 5b show AP and lateral radiographs of the right hip. Further evaluation should include


Explanation
The radiographs show Ficat and Arlet stage 2 osteonecrosis. The femoral head remains round, and there are sclerotic changes in the superolateral quadrant. Patients with systemic lupus erythematosus are at risk for osteonecrosis because of prednisone use and the underlying metabolic changes associated with the condition (hypofibrinolysis and thrombophilia). MRI is the best diagnostic method for detecting osteonecrosis, with a greater than 98% sensitivity and specificity. For this patient, an MRI can assess the contralateral hip for any involvement and can quantify the extent of the lesion. Mont MA, Jones LC, Sotereanos DG, Amstutz HC, Hungerford DS: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 369
High Yield
An 82-year-old woman reports activity-related knee pain. History reveals that she underwent total knee arthroplasty 16 years ago. AP and lateral radiographs and a bone scan are shown in Figures 38a through 38c. What is the most likely diagnosis?



Explanation
The radiographs reveal a large femoral metaphyseal lytic lesion with well-defined borders. Joint space narrowing medially is consistent with polyethylene wear. The most likely diagnosis is particle-mediated osteolysis. Metastatic tumors and primary sarcomas adjacent to an arthroplasty are extremely rare. In addition, malignant tumors and infection would more likely reveal a destructive lesion with poorly defined borders and increased uptake on a bone scan. Stress shielding with massive bone loss has not been described in knee arthroplasty literature, although this entity has been observed in fully porous-coated femoral implants in total hip arthroplasty. Robinson EJ, Mulliken BD, Bourne RB, et al: Catastrophic osteolysis in total knee replacement: A report of 17 cases. Clin Orthop Relat Res 1995;321:98-105. Archibeck MJ, Jacobs JJ, Roebuck KA, et al: The basic science of periprosthetic osteolysis. Instr Course Lect 2001;50:185-195.
Question 370
High Yield
A 58-year-old woman with rheumatoid arthritis has progressive neck pain, upper extremity and lower extremity weakness, and difficulty with fine motor movements. Examination reveals hyperreflexia with mild to moderate objective weakness but the patient has no difficulty with ambulation for short distances. What is the most important preoperative imaging finding that predicts full neurologic recovery with surgical stabilization?
Explanation
Boden and associates' article presents compelling evidence that patients with rheumatoid arthritis and neurologic deterioration in C1-2 instability are more likely to achieve some improvement if the posterior atlanto-dens interval is greater than 10 mm on preoperative studies. All the patients in their series who had neurologic deterioration and a preoperative posterior atlanto-dens interval of greater than 14 mm achieved complete motor recovery. Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297. Boden SD, Clark CR: Rheumatoid arthritis of the cervical spine, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Question 371
High Yield
A 48-year-old woman with rheumatoid arthritis reports increasing elbow pain for the past 6 months. History reveals that she underwent total elbow arthroplasty 7 years ago. A peripheral WBC count, erythrocyte sedimentation rate, and C-reactive protein studies are normal. An AP radiograph is shown in Figure 5. What is the next most appropriate step in management?

Explanation
Pain relief is excellent after total elbow arthroplasty and is comparable to the results found with hip and knee arthroplasty. The failure of total elbow arthroplasty in the treatment of rheumatoid arthritis can be the result of infection, aseptic loosening, instability, and bearing surface wear. The radiographic findings shown here are consistent with bushing wear in a linked device. The bushings can be changed before continued wear results in osteolysis and implant loosening. If the implants become loose, then reimplantation is necessary. Resection arthroplasty is not indicated if the components are well fixed. Elbow arthrodesis is not indicated in patients with rheumatoid arthritis. Gill DR, Morrey BF: The Coonrad-Morrey total elbow arthroplasty in patients who have rheumatoid arthritis: A ten to fifteen-year follow-up study. J Bone Joint Surg Am 1998;80:1327-1335.
Question 372
High Yield
A 16-year-old high school student undergoes a routine preparticipation physical examination at the beginning of the school year. Examination reveals marked laxity of both shoulders but only mild generalized laxity in other joints. The load and shift test allows for anterior humeral translation to the glenoid rim and posterior humeral translation beyond the glenoid rim. The sulcus sign is present. What is the next most appropriate step in management?
Explanation
This patient has shoulder laxity without apprehension. Because there is a wide range of normal laxity in asymptomatic shoulders, the physician should inform the student of these findings, recommend shoulder strengthening exercises, and allow unrestricted sports participation unless symptoms develop. Harryman DT, Sidles JA, Harris SL, Matsen FA III: Laxity of the normal glenohumeral joint: A quantitative in vivo assessment. J Shoulder Elbow Surg 1992;1:66-76. Hawkins RJ, Bokor RJ: Clinical evaluation of shoulder problems, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 186. McFarland EG, Campbell G, McDowell J: Posterior shoulder laxity in asymptomatic athletes. Am J Sports Med 1996;24:468-471.
Question 373
High Yield
A 47-year-old man with Charcot-Marie-Tooth (CMT) disease was treated with a fifth metatarsal head resection for a symptomatic bunionette 2 years ago. What is the most likely complication seen at this time?

Explanation
CMT is characterized by a cavovarus foot position that increases weight-bearing stresses along the lateral border. Removal of the fifth metatarsal head carries the risk of creating a transfer lesion at the fourth metatarsal head, particularly with a cavovarus foot. Claw toes are common in CMT, but the fifth toe would be flail in this situation. Ulceration is unlikely given the lack of underlying bone. Peroneal atrophy is associated with CMT but would not be a complication of this procedure. Charcot arthropathy is a neuropathic process frequently seen in individuals with diabetes mellitus. Kitaoka HB, Holiday AD Jr: Metatarsal head resection for bunionette: Long-term followup. Foot Ankle 1991;11:345-349.
Question 374
High Yield
Examination of a 9-year-old girl who injured her left elbow in a fall reveals tenderness and swelling localized to the medial aspect of the elbow. Motor and sensory examinations of the hand are normal, and circulation is intact. A radiograph is seen in Figure 28. Management should consist of

Explanation
Avulsion fractures of the medial epicondyle are caused by a valgus stress applied to the immature elbow and usually occur in children between the ages of 9 and 14 years. Long-term studies have shown that isolated fractures of the medial epicondyle with between 5 to 15 mm of displacement heal well. Brief immobilization (1 to 2 weeks) in a long arm cast or splint yields results similar to open reduction and internal fixation. Fibrous union of the fragment is not associated with significant symptoms or diminished function. Surgical excision of the fragment yielded the worst results in one study and should be avoided. Open reduction is best reserved for those injuries in which the medial epicondylar fragment becomes entrapped in the elbow joint during reduction and cannot be extracted by closed manipulation. Farsetti P, Potenza V, Caterini R, Ippolito E: Long-term results of treatment of fractures of the medial humeral epicondyle in children. J Bone Joint Surg Am 2001;83:1299-1305.
Question 375
High Yield
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45-degree lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
There are several indications for extending adult scoliosis fusions to the sacrum, rather than stopping in the lower lumbar spine. These indications include posterior column deficiencies at L5-S1, such as spondylolysis and laminectomy, and deformities extending to the sacrum, such as fixed tilt of L5-S1 or sagittal imbalance. MRI signal changes in the L5-S1 disk do not preclude stopping the fusion at L5. Some surgeons use diskography or diagnostic facet blocks to evaluate the integrity of the L5-S1 level prior to stopping the fusion at L5. Long scoliosis fusions stopping at L5 have a significant risk of failure, highlighting the importance of careful selection of fusion levels. Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629. Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Question 376
High Yield
What is the optimum position of immobilization of the foot and ankle immediately after Achilles tendon repair to maximize skin perfusion?
Explanation
Achilles tendon tension is not affected by knee position when the ankle is in 20 degrees to 25 degrees of plantar flexion. Skin perfusion overlying the Achilles tendon is maximal in 20 degrees of plantar flexion and is reduced beyond 20 degrees of plantar flexion. Neutral flexion or any amount of dorsiflexion compromises the repair.
Question 377
High Yield
An adult patient has a closed humeral fracture that was treated nonsurgically and a concomitant radial nerve injury. Six weeks after injury, electromyography shows no evidence of recovery. Management should now consist of
Explanation
In patients with radial nerve injuries with closed humeral fractures, it has been reported that 85% to 95% spontaneously recover. Based on this premise, most surgeons favor expectant management of these injuries. Even if there is no evidence of recovery at 6 weeks, repeat electromyography at 12 weeks is advocated. If there is no clinical or electromyographic signs of recovery at 6 months, exploration is recommended. If the nerve is in continuity at the time of exploration, nerve action potentials are useful in helping determine the need for neurolysis, excision, and grafting, or if excision and repair is the best option. Pollock FH, Drake D, Bovill EG, et al: Treatment of radial neuropathy associated with fractures of the humerus. J Bone Joint Surg Am 1981;63:239-243.
Question 378
High Yield
A 22-year-old right hand-dominant man who fell off his motorcycle onto the tip of his right shoulder 2 weeks ago now reports pain and difficulty raising his right arm. Examination reveals tenderness and gross movement over the lateral scapular spine and severe weakness during resisted abduction. A radiograph and 3D-CT scan are shown in Figures 24a and 24b. What is the next most appropriate step in management?


Explanation
The patient has a displaced scapular spine fracture that has resulted in shoulder weakness from a poor deltoid lever arm. The downward tilt may lead to subacromial impingement and rotator cuff dysfunction. Open reduction and internal fixation would best allow normal deltoid and shoulder function. Bone stimulators and abduction bracing may lead to healing but in a malunited position. Arthroscopic acromioplasty and fragment excision should be avoided. Ogawa K, Naniwa T: Fractures of the acromion and the lateral scapular spine. J Shoulder Elbow Surg 1997;6:544-548.
Question 379
High Yield
Which of the following nerves travels with the deep palmar arch?
Explanation
The ulnar nerve divides alongside the pisiform, and the deep branch supplies the three hypothenar muscles and crosses the palm with the deep palmar arch to supply the two ulnar lumbricals, all interossei, and finally the adductor pollicis. The superficial branch supplies the ulnar digital branches to the small and ring fingers. The median nerve branches are more superficial in the palm near the superficial palmar arch. Last RJ: Anatomy: Regional and Applied, ed 6. London, England, Churchill Livingstone, 1978, p 109.
Question 380
High Yield
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?
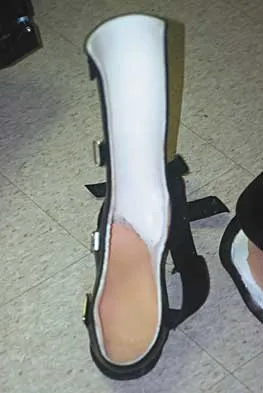
Explanation
The most likely diagnosis is a stress fracture of the calcaneus and is supported by the history of running, female gender, and amenorrhea. Reproducing pain with medial and lateral compression of the heel also supports the diagnosis. A bone scan or MRI would most likely confirm the diagnosis. Plantar fasciitis would result in pain on the bottom of the heel with point tenderness. The lack of other areas of involvement or other symptoms does not support a seronegative inflammatory arthritis. Tarsal tunnel syndrome and peripheral neuropathy are unlikely because of the normal neurologic examination. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Question 381
High Yield
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
For a pediatric patient without mechanical symptoms, initial management of an osteochondral defect lesion that is not detached should consist of casting in flexion. Failure to respond to several weeks or months of nonsurgical management may warrant surgical treatment.
Question 382
High Yield
During a posterior approach to the glenoid with retraction as shown in Figure 33, care should be taken during superior retraction to avoid injury to which of the following structures?
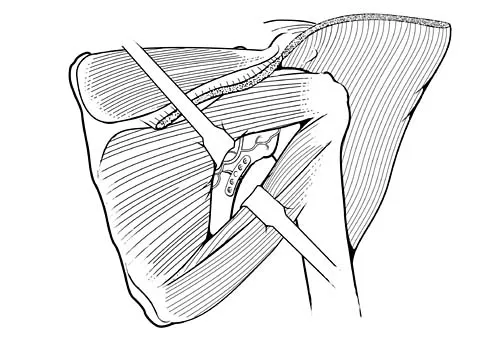
Explanation
During a posterior approach to the shoulder for either a scapular fracture, glenoid fracture, or posterior shoulder pathology, the interval between the teres minor and infraspinatus is split. Excessive superior retraction on the infraspinatus, or excessive dissection superomedially under the infraspinatus muscle and tendon can cause injury to the suprascapular nerve and/or artery. During dissection in this interval, the axillary artery and axillary nerve are well protected. A branch of the circumflex scapular artery ascends between the teres minor and infraspinatus muscle, but it is at risk during dissection on the scapula in the mid portion of the interval and not during superior retraction. The profunda brachii artery is not present in this interval. Jerosch JJ, Greig M, Peuker ET, et al: The posterior subdeltoid approach: A modified access to the posterior glenohumeral joint. J Shoulder Elbow Surg 2001;10:265-268. Judet R: Surgical treatment of scapular fractures. Acta Orthop Belg 1964;30:673-678.
Question 383
High Yield
Figure 29 shows the radiograph of a 25-year-old woman who has had a 3-month history of ankle pain after sustaining an inversion injury to the ankle. She reports occasional catching, but no sense of instability. Examination reveals ligament stability. Management should consist of

Explanation
Osteochondral lesions of the talar dome can have a traumatic or nontraumatic etiology. Most authors site a probable traumatic etiology for lateral lesions. Stage I and II lesions, which are composed of compressed subchondral bone or a partial detached osteochondral fragment, can be treated initially in a non-weight-bearing short leg cast for 6 weeks. Stage III medial lesions can also be treated in the same manner. If symptoms persist, the treament of choice is debridement of the fracture, curettage of the lesion, and drilling of the subchondral bone. This treatment also applies to lateral stage III and all stage IV lesions. If the fragment is at least one third of the size of the talar dome, management should consist of open reduction and internal fixation. In patients with more chronic lesions (4 to 6 months of persistent pain), the threshold to proceed with surgery is lower, even in a stage II lesion. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Question 384
High Yield
A previously asymptomatic 40-year-old man injures his shoulder in a fall. Examination shows that he is unable to lift the hand away from his back while maximally internally rotated. An axial MRI scan of the shoulder is shown in Figure 14. What is the most likely diagnosis?

Explanation
The MRI scan shows detachment of the subscapularis from its insertion on the lesser tuberosity. The examination finding is consistent with a positive lift-off test, also indicating a tear of the subscapularis. Lyons RP, Green A: Subscapularis tendon tears. J Am Acad Orthop Surg 2005;13:353-363.
Question 385
High Yield
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Explanation
The patient has an upper plexus palsy (Erb palsy) with severe shoulder contracture. While physical therapy for stretching is the treatment of choice to prevent contracture in the newborn, it is unlikely to be of benefit in the older child with an established contracture. Contracture release alone or in combination with muscle transfers can improve the cosmetic appearance, and in the case of a mild deformity, may also improve function. These procedures are less likely to help when there is deformity of the shoulder joint or when arthritic changes are present. The procedure of choice for an older child with joint deformity is rotational osteotomy of the proximal humerus because it can improve cosmesis and function, even in the face of joint deformity. Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537. Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L'Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Question 386
High Yield
A 45-year-old man reports that he awoke 2 weeks ago with severe pain in his right arm. Examination reveals weakness in the biceps, brachialis, and wrist extensors. There is decreased sensation in the thumb and index finger and a diminished brachioradialis reflex. Assuming this patient has a posterolateral herniated nucleus pulposus, what level is involved?

Explanation
This is a classic C6 nerve injury, and it is most likely the result of a herniated nucleus pulposus at C5-6. The C5 nerve root controls the elbow flexors, shoulder abductors, and external rotators. The C7 nerve root controls the elbow extensors, wrist pronators, and the triceps reflex. Standaert CJ: The patient history and physical examination: Cervical, thoracic and lumbar, in Herkowitz HN, Garfin SR, Eismont FJ, et al (eds): Rothman-Simeone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, vol 1, pp 171-186.
Question 387
High Yield
A 60-year-old man reports that he has had shoe pressure pain over his right great toe for several years but has minimal discomfort when barefoot or in sandals. A clinical photograph and radiographs are shown in Figures 1a through 1c. Management should consist of



Explanation
Some patients have minimal symptoms associated with hallux rigidus despite significant radiographic evidence of osteoarthritis. This patient's symptoms are primarily related to shoe pressure from the exostosis and can be managed with extra-depth shoe wear. Smith RW, Katchis SD, Ayson LC: Outcomes in hallux rigidus patients treated nonoperatively: A long-term follow-up study. Foot Ankle Int 2000;21:906-913.
Question 388
High Yield
An 11-year-old boy sustained an injury to his arm in gym class. He denies prior pain in the arm. Radiographs are shown in Figures 48a and 48b. What is the next most appropriate step in the management of this lesion?


Explanation
This radiolucent lesion with a "fallen leaf sign" is typical for a unicameral bone cyst(UBC). The most appropriate treatment is to allow the fracture to heal with clinical and radiographic observation. Curettage and bone grafting is not the best initial management for UBC. Wide resection is not indicated for UBC. The proximal humerus is the most common site for UBC. While staging studies consisting of MRI, bone scan, and CT of the chest are appropriate for lesions suspected of being malignant, the classical appearance of this UBC is such that this work-up is not necessary initially. Following fracture healing, aspiration and injection of the cyst may be indicated. Dormans JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Question 389
High Yield
The peroneus tertius is a commonly used landmark for arthroscopic portal placement. What is the function of this tendon?

Explanation
The peroneus tertius, although absent in 10% of the population, originates on the distal third of the extensor surface of the fibula and inserts onto the base of the fifth metatarsal, possibly extending to the fascia over the fourth interosseous space. The muscle is located in the anterior compartment of the leg and is innervated by the deep peroneal nerve. The tendon produces dorsiflexion and eversion when walking and can be used as an insertion point during tendon transfers to assist dorsiflexion. This tendon is peculiar to humans and is a proximally migrated deep extensor of the fifth toe. Joshi SD, Joshi SS, Athavale SA: Morphology of the peroneus tertius muscle. Clin Anat 2006;19:611-614. Williams PL, Bannister LH, Berry MM, et al (eds): Gray's Anatomy, ed 38. London, Churchill Livingston, 1995, p 883.
Question 390
High Yield
What is the primary limiting membrane and mechanical support for the periphery of the physis?

Explanation
The perichondrial fibrous ring of La Croix acts as a limiting membrane that provides mechanical support for the bone-cartilage junction of the growth plate. It is continuous with the ossification groove of Ranvier, which contributes chondrocytes for the increase in width of the growth plate. The zone of provisional calcification lies at the bottom of the hypertrophic zone and is the site of initial calcification of the matrix. It is quite weak and usually is the cleavage plane for fractures; therefore, it does not qualify as mechanical support. The last intact transverse septum separates the zone of provisional calcification from the primary spongiosa and provides no real support to the physis. The primary spongiosa is the part of the metaphysis nearest the physis. Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
Question 391
High Yield
A 68-year-old woman who sustained a closed distal tibia fracture 2 years ago was initially treated with an external fixator across the ankle for 12 weeks, followed by intramedullary nailing of the fibula and lag screw fixation of the tibia. She continued to report persistent pain so she was treated with a brace and a bone stimulator. She now reports pain in her ankle. Examination reveals ankle range of motion of 8 degrees of dorsiflexion to 25 degrees of plantar flexion. She is neurovascularly intact. Current radiographs are shown in Figures 9a through 9c. What is the next most appropriate step in management?



Explanation
The patient has a nonunion of the distal fifth of the tibia. The nonunion appears to be oligotrophic, somewhere between atrophic and hypertrophic. Management requires stabilization and stimulation of the local biology, which can be accomplished with open reduction and internal fixation with bone grafting. Bracing or casting does not provide enough stability. Ultrasound bone stimulation has been shown to speed fresh fracture repair but is not indicated in nonunions. The distal segment is too short for intramedullary nailing. A fibular osteotomy alone would increase instability and, even with prolonged casting, would be unlikely to lead to successful repair. Carpenter CA, Jupiter JB: Blade plate reconstruction of metaphyseal nonunion of the tibia. Clin Orthop 1996;332:23-28. Lonner JH, Siliski JM, Jupiter JB, Lhowe DW: Posttraumatic nonunion of the proximal tibial metaphysis. Am J Orthop 1999;28:523-528. Stevenson S: Enhancement of fracture healing with autogenous and allogeneic bone grafts. Clin Orthop 1998;355:S239-S246.
Question 392
High Yield
A football lineman who sustained a traumatic injury while blocking during a game now reports that his shoulder is slipping while pass blocking. Examination reveals no apprehension in abduction and external rotation; however, he reports pain with posterior translation of the shoulder. He has full strength in external rotation, internal rotation, and supraspinatus testing. What is the pathology most likely responsible for his symptoms?
Explanation
Traumatic posterior instability is a common finding in football players, especially in the blocking positions as well as in the defensive linemen and linebackers. A traumatic blow to the outstretched arm results in posterior glenohumeral forces. Labral detachment at the glenoid rim is common. Patients report slipping or pain with posteriorly directed pressure. Rarely do these patients have true dislocations that require reduction; however, recurrent episodes of subluxation or pain are not uncommon. Posterior repair has been shown to be successful in the treatment of traumatic instability. Bottoni CR, Franks BR, Moore JH, et al: Operative stabilization of posterior shoulder instability. Am J Sports Med 2005;33:996-1002. Williams RJ III, Strickland S, Cohen M, et al: Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-209.
Question 393
High Yield
Optimal management of the injury shown in Figure 31 should include which of the following?

Explanation
The radiograph shows a displaced calcaneal beak fracture, a tongue-type fracture variant. The fracture fragment typically includes the insertion point of the Achilles tendon, which places marked tension on the thin overlying soft-tissue envelope and can lead to full-thickness necrosis if not acutely addressed. Cast immobilization does not adequately address the increased soft-tissue tension, as the fragment will be difficult to control. Arthroscopic-assisted techniques or primary arthrodesis are not indicated because calcaneal beak fractures are typically extra-articular. Sanders RW, Clare MP: Fractures of the calcaneus, in Coughlin MJ, Mann RA, Saltzman CL (eds): Surgery of the Foot and Ankle, ed 8. Philadelphia, PA, Mosby-Elsevier, 2007, vol 2, pp 2017-2073.
Question 394
High Yield
What structure provides the major blood supply to the humeral head?
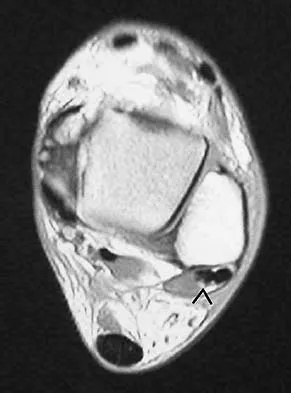
Explanation
The ascending branch of the anterior circumflex humeral artery provides the major blood supply to the humeral head. The posterior circumflex humeral artery supplies a much smaller portion of the proximal humerus. The nutrient humeral artery is the main blood supply for the humeral shaft. The thoracoacromial artery is primarily a muscular branch. The rotator cuff insertions contribute some blood supply to the tuberosities but not a major contribution. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 395
High Yield
A 16-year-old girl sustained the injury shown in Figure 7a. CT scans are shown in Figures 7b through 7d. The results of treatment of this injury have been shown to most correlate with which of the following factors?

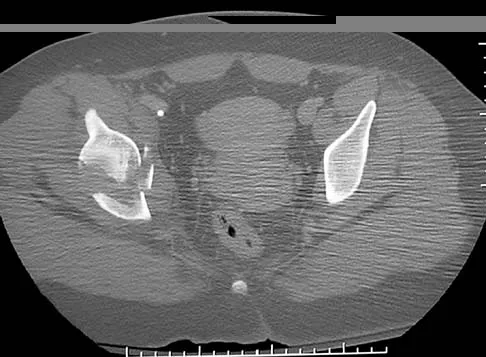

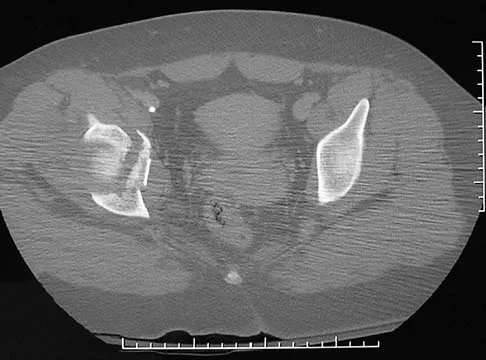
Explanation
The patient has a very low T-type acetabular fracture; however, the head is not congruent under the dome so surgical reduction is necessary. The anterior and posterior columns are displaced and will move independent from each other. The extended iliofemoral is the only approach allowing for visualization and reduction of each column. A combined anterior and posterior approach may also be used. The timing of surgery should be within the first 3 weeks of injury to optimize chances of obtaining an accurate reduction because this is an important factor in determining outcome. Letournel E, Judet R (eds): Fractures of the Acetabulum, ed 2. Berlin, Germany, Springer-Verlag, 1991.
Question 396
High Yield
Which of the following is considered the appropriate initial management protocol for an unconscious football player without spontaneous respirations?

Explanation
The on-field evaluation and management of the seriously injured athlete requires advance preparation and planning. It is imperative that the health care team have a game plan in place and the proper equipment readily available. The initial step consists of stabilizing the head and neck by manually holding the head and neck in a neutral position. Then, in the following order, check for breathing, pulses, and level of consciousness. If the athlete is breathing, simply remove the mouth guard and maintain the airway. If the athlete is not breathing, the face mask must be removed and the chin strap left in place. An open airway must be established, followed by assisted breathing. CPR is only instituted when breathing and circulation are compromised. If the athlete is unconcious or has a suspected cervical spine injury, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated. McSwain NE, Garnelli RL: Helmet removal from injured patients. Bull Am Coll Surg 1997;82:42-44. Vegso JJ, Lehman RC: Field evaluation and management of head and neck injuries. Clin Sports Med 1987;6:1-15.
Question 397
High Yield
Figure 41 shows the MRI scan of a 39-year-old man who has severe left groin and anterior thigh pain. What is the most likely diagnosis?
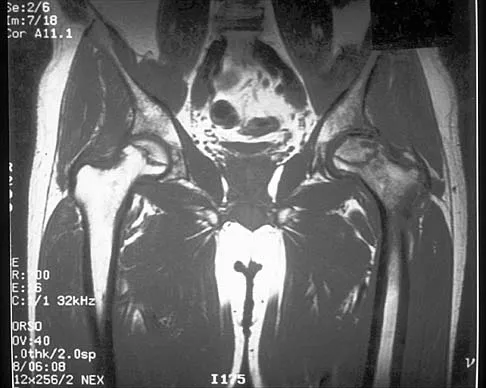
Explanation
The MRI scan shows near complete involvement of the femoral head with bone marrow changes and some collapse of the necrotic segment. This is most suggestive of osteonecrosis.
Question 398
High Yield
Where is the underlying defect in a rhizomelic dwarf with the findings shown in Figure 5?

Explanation
The radiograph shows the typical findings of achondroplasia. The defect is in fibroblast growth factor receptor 3. The pedicles narrow distally in the lumbar spine. The pelvis is low and broad with narrow sciatic notches and ping-pong paddle-shaped iliac wings. This is often called a champagne glass pelvis. Type I collagen abnormalities are typically found in osteogenesis imperfecta, and type II collagen defects are found in spondyloepiphyseal dysplasia and Kneist syndrome. COMP is defective in multiple epiphyseal dysplasia. Sulfate transport defects are seen in diastrophic dysplasia. Johnson TR, Steinbach LS: Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 809-812.
Question 399
High Yield
A 20-year-old minor league baseball pitcher is diagnosed with a symptomatic torn ulnar collateral ligament (UCL) in his pitching elbow. Nonsurgical management consisting of rest and physical therapy aimed at elbow strengthening has failed to provide relief. He has concomitant cubital tunnel symptoms that worsen while throwing. What is his best surgical option?
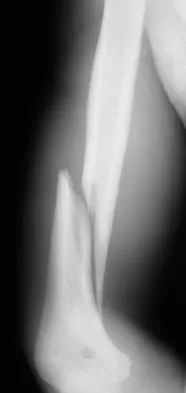
Explanation
High-level pitchers with symptomatic UCL tears require reconstruction, with autograft being the best studied graft selection. With concomitant ulnar nerve symptoms, a simultaneous ulnar nerve transposition provides good results. Ligament "repairs" and allograft reconstructions have not shown good long-term results. Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Question 400
High Yield
A 45-year-old man who is a smoker has a significant hemothorax and bilateral closed femoral fractures. On insertion of a chest tube, 1,100 mL of blood was returned. He has had 75 mL of chest tube output over the last 2 hours while being resuscitated in the ICU. His base deficit is now 2 and his urine output has been 3 mL/kg over the last hour. What is the next most appropriate step in management?

Explanation
Although this patient had a hemothorax, the bleeding has stopped and he has been resuscitated to a euvolemic status with a small base deficit and good urine output. External fixation of both femurs is an option but an unnecessary step in the treatment algorithm. Nork SE, Agel J, Russell GV, et al: Mortality after reamed intramedullary nailing of bilateral femur fractures. Clin Orthop Relat Res 2003;415:272-278.
