HY 2026
00:00
Start Quiz
Question 201
High Yield
A 21-year-old professional ballet dancer reports a painful popping sensation over her right hip joint. Examination reveals that symptoms are reproduced with hip flexion and external rotation. Which of the following studies will best confirm the diagnosis?
Explanation
The patient has snapping hip syndrome of the internal type, which is more common in ballet dancers. It is caused by the iliopsoas tendon gliding over the iliopectineal line or the femoral head. The diagnosis usually can be made by the history and physical examination. Snapping is reproduced by hip flexion and extension or flexion with external rotation and abduction. Conventional and dynamic ultrasonography will confirm the snapping structure. Radiographs occasionally show calcifications near the lesser trochanter. MRI can be used to rule out other diagnoses that can simulate snapping hip. Gruen GS, Scioscia TN, Lowenstein JE: The surgical treatment of internal snapping hip. Am J Sports Med 2002;30:607-613.
Question 202
High Yield
A 100-lb 9-year-old boy has a closed midshaft transverse femoral fracture. The oblique fracture is shortened by 3 cm with a 10-degree varus angulation. Surgical management consists of intramedullary, retrograde flexible titanium nailing. To optimize fracture stability, the surgeon should
Explanation
The technique of intramedullary nailing with titanium elastic nails is based on the concept of balanced forces across the fracture site with two equally sized nails. Implantation of the largest sized nails possible, with two equally sized nails, maximizes the stiffness at the fracture site, thereby optimizing fracture alignment and stability. Impacting the nails into the medullary canal can impact the fixation by minimizing distal purchase of the nail at the cortical insertion site. Closed reduction commonly permits bony reduction and passage of the nails; open reduction is reserved for inability to align the fracture. Luhmann SJ, Schootman M, Schoenecker PL, et al: Complications of titanium elastic nails for pediatric femur fractures. J Pediatr Orthop 2003;23:443-447. Lascombes P, Haumont T, Journeau P: Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop 2006;26:827-834.
Question 203
High Yield
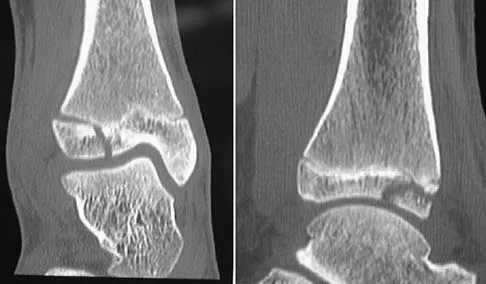
A 42-year-old woman sustained a closed, displaced talar neck fracture in a motor vehicle accident. Which of the following is an avoidable complication of surgical treatment?
Explanation
Malunion of the talus is a devastating complication that leads to malpositioning of the foot and subsequent arthrosis of the subtalar joint complex. This is considered an avoidable complication in that accurate surgical reduction will minimize its development. Posttraumatic arthritis of the subtalar joint, osteonecrosis of the talus, posttraumatic arthritis of the ankle joint, and complex regional pain syndrome all may develop as a result of the initial traumatic event and may not be avoidable despite anatomic reduction. Rockwood and Green's Fractures in Adults, ed 5. Philadelphia, PA, Lippincott, Williams and Wilkins, 2001, pp 2091-2132.
Question 204
High Yield
Which of the following is a true statement regarding thoracic disk herniations?
Explanation
Symptomatic herniations of the thoracic spine are much less common than those of the cervical or lumbar region. They tend to occur most commonly during the third to fifth decades of life and although they can be found at all levels, they are most common in the lower third near the thoracolumbar region. Posterior laminectomy and disk excision has the highest rate of neurologic deterioration and is not recommended. Multiple studies have shown that herniated thoracic disks can be found at one or more levels in 40% of asymptomatic individuals. Shah RP, Grauer JN: Thoracoscopic excision of thoracic herniated disc, in Vaccaro AR, Bono CM (eds): Minimally Invasive Spine Surgery. New York, NY, Informa Healthcare, 2007, pp 73-80.
Question 205
High Yield
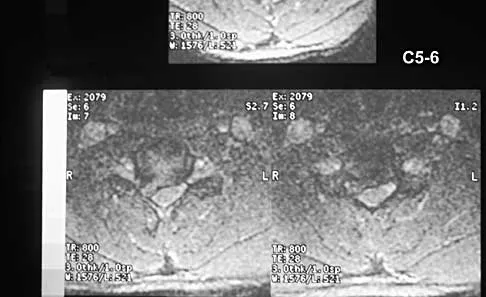
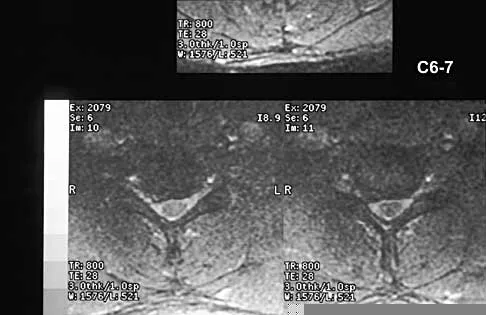
A 40-year-old carpenter has a 3-month history of right arm pain and neck pain that now leaves him unable to work. Examination reveals a positive Spurling test, weakness of the biceps, and a mildly positive Hoffman's sign on the right side. Electromyography and nerve conduction velocity studies show a right C6 deficit. Figures 27a through 27c show MRI scans that reveal two-level spondylotic disease at C5-6 and C6-7, a large herniated nucleus pulposus at C5-6, and a prominent ridge and hard disk at C6-7. Nonsurgical management fails to provide relief, so the patient elects surgical intervention. Which of the following surgical options would give the best long-term results?

Explanation
The patient has a single-level deficit by clinical examination but an adjacent level that may be pathologic. Hilibrand and associates, in a review of 374 patients with myeloradiculopathy treated with single-level or multilevel anterior cervical diskectomy and fusion, showed that 25% of patients had an occurrence of new radiculopathy or myelopathy at an adjacent level within 10 years after surgery. Reoperation rates were highest in those patients where the adjacent nonfused segment was C5-6 or C6-7. Those patients who had multilevel fusions had a lower incidence of adjacent segment disease. The authors recommended incorporating an adjacent level in the initial procedure in patients with myelopathy or radiculopathy when significant disease was noted. Posterior keyhole foraminotomy is an excellent procedure for single-level radiculopathy but is not effective in relieving myelopathy. Anterior cervical diskectomy without fusion has an increased incidence of hypermobility and neck pain on long-term follow-up. In a later review, these authors reported improved fusion rates and better clinical outcomes with the use of strut fusions instead of multilevel interbody grafts. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH: Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 1999;81:519-528. Henderson CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512.
Question 206
High Yield
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for


Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 207
High Yield
Figures 9a and 9b show the radiographs of a 12-year-old girl who has had right hip pain for the past 4 months. She reports that the pain is so severe that she is unable to walk and is now using a wheelchair. Examination reveals pain with any attempted range of motion. Management should include


Explanation
In addition to mild hip dysplasia, the radiograph shows an osteoblastic lesion of the right ilium. The patient's symptoms are much more severe than is typical for late hip dysplasia. MRI can determine the extent of the lesion in the bone and soft tissues. Following work-up and biopsy, the patient was diagnosed with Ewing's sarcoma. Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 507-518, 542-544.
Question 208
High Yield
A 13-year-old girl with hallux valgus reports pain after playing basketball. Radiographs show a hallux valgus angle of 20 degrees, an intermetatarsal angle of 11 degrees, a distal metatarsal articular angle of 10 degrees, and a congruent joint. Management should consist of
Explanation
Shoe wear modification is the most appropriate management based on the patient's age, high activity level, and relatively minor symptoms. She also has a mild hallux valgus. Normal radiographic measurements are an intermetatarsal angle of less than 9 degrees, a hallux valgus angle of less than 15 degrees, and a distal metatarsal articular angle of less than 9 degrees. Surgical procedures should be reserved for patients with more severe or progressive deformities. Stephens HM: Bunions, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1510-1519.
Question 209
High Yield
A 20-year-old man sustained a closed tibial fracture and is treated with a reamed intramedullary nail. What is the most common complication associated with this treatment?

Explanation
The most common complication is anterior knee pain (57%). The knee pain is activity related (92%) and exacerbated by kneeling (83%). Although knee pain is the most common complication, most patients rate it as mild to moderate and only 10% are unable to return to previous employment. Some authors report less knee pain with a peritendinous approach when compared to a tendon-splitting approach. In one study, nail removal resolved pain in 27%, improved it in 70%, and made it worse in 3%. The incidence of the other complications was: infection 0% to 3%, nonunion 0% to 6%, and malunion 2% to 13%. Compartment syndrome is rare after nailing. Court-Brown CM: Reamed intramedullary tibial nailing: An overview and analysis of 1106 cases. J Orthop Trauma 2004;18:96-101. McQueen MM, Gaston P, Court-Brown CM: Acute compartment syndrome: Who is at risk? J Bone Joint Surg Br 2000;82:200-203.
Question 210
High Yield
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
CT of the abdomen and pelvis is not part of the staging of osteosarcoma. Staging studies should consist of CT of the chest, radiographs of the chest and primary tumor, MRI of the primary tumor, and a bone scan. The MRI should be obtained prior to the biopsy.
Question 211
High Yield
A 14-year-old football player has had right knee pain for the past 2 months; however, he denies any history of trauma. Examination shows an abductor lurch and increased external rotation of the right lower extremity. The best course of action should be to

Explanation
Slipped capital femoral epiphysis is the most common pathology involving the hip in adolescents. While patients with acute slips may report severe pain and are unable to ambulate, those with chronic slips often have pain during ambulation, a limp, and increased external rotation of the hip. While 60% of the patients specifically report hip pain, the remainder have pain in the thigh or knee. The initial diagnostic study of choice is AP and frog-lateral radiographs of the pelvis; bilateral involvement is frequently seen. Boyer DW, Mickelson MR, Ponseti IV: Slipped capital femoral epiphysis: Long-term follow-up study of one hundred and twenty-one patients. J Bone Joint Surg Am 1981;63:85-95.
Question 212
High Yield
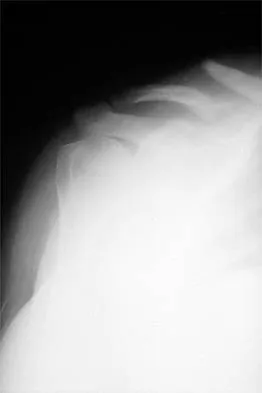
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient?


Explanation
The radiographs reveal osteonecrosis with collapse. The most reliable and durable treatment for osteonecrosis of the humeral head remains prosthetic shoulder arthroplasty. Osteonecrosis of the humeral head may be seen after the use of steroids, and there is an increasing demand for shoulder arthroplasty in young people because of the use of high-dose steroids in chemotherapy regimes for the treatment of malignant tumors. The indications for most shoulder arthrodeses today include posttraumatic brachial plexus injury, paralytic disorders in infancy, insufficiency of the deltoid muscle and rotator cuff, chronic infection, failed revision arthroplasty, severe refractory instability, and bone deficiency following resection of a tumor in the proximal aspect of the humerus. Clearly, the role of arthroscopy and related minimally invasive techniques in the treatment of humeral head osteonecrosis remains unknown. Hasan SS, Romeo AA: Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-298. Hattrup SJ: Indications, technique, and results of shoulder arthroplasty in osteonecrosis. Orthop Clin North Am 1998;29:445-451.
Question 213
High Yield
A 31-year-old woman has increasing pain and tightness in her right knee, with occasional stiffness and recurrent hemorrhagic effusions. MRI scans are shown in Figures 2a and 2b. What is the most likely diagnosis?


Explanation
PVNS is a rare inflammatory granulomatous condition of unknown etiology, and causes proliferation of the synovium of joints, tendon sheaths, or bursa. The disorder occurs most commonly in the third and fourth decades but can occur at any age. MRI provides excellent delineation of the synovial disease. Characteristic features of PVNS on MRI include the presence of intra-articular nodular masses of low signal intensity on T1- and T2-weighted images and proton density-weighted images. Synovial biopsy should be performed if there is any doubt of the diagnosis. Total synovectomy (open or arthroscopic) is required for the diffuse form, although recurrence is common. Rheumatoid arthritis and synovial chondromatosis are not typically associated with hemorrhagic effusions. De Ponti A, Sansone V, Malchere M: Result of arthroscopic treatment of pigmented villonodular synovitis of the knee. Arthroscopy 2003;19:602-607. Chin KR, Barr SJ, Winalski C, et al: Treatment of advanced primary and recurrent diffuse pigmented villonodular synovitis of the knee. J Bone Joint Surg Am 2002;84:2192-2202.
Question 214
High Yield
What is the most frequent complication of both lateral closing wedge high tibial osteotomy and medial opening wedge osteotomy?

Explanation
Scuderi and associates reported on patellar height after a high tibial osteotomy. Eighty-nine percent of the patellae, as measured by the Insall-Salvati index, and 76.3 percent, as measured by the Blackburne-Peel index, were observed to be lowered. More recently, Wright and associates reported a 64% incidence of patella baja in patients undergoing a medial opening wedge osteotomy. The incidence of intra-articular fracture during medial opening wedge osteotomy has been reported to be as high as 11% by Hernigou and associates, whereas the incidence of intra-articular fracture during lateral closing wedge high tibial osteotomy has been reported to be 10% to 20% by Matthews and associates. The incidence of peroneal nerve palsy with a lateral closing wedge high tibial osteotomy ranges from 0% to 20%, according to Marti and associates, whereas the incidence of peroneal palsy following a medial opening wedge osteotomy has been reported to be 15.7% by Flierl and associates. The exact incidence of compartment syndrome after a high tibial osteotomy is not known; however, it does not reach the level of patella baja. The incidence of deep infection after a lateral closing wedge high tibial osteotomy ranges from 0% to 4% according to Billings and associates. Scuderi GR, Windsor RE, Insall JN: Observations on patellar height after proximal tibial osteotomy. J Bone Joint Surg Am 1989;71:245-248. Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005;13:279-289. Hernigou P, Medevielle D, Debeyre J, et al: Proximal tibial osteotomy for osteoarthritis with varus deformity: A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354. Matthews LS, Goldstein SA, Malvitz TA, et al: Proximal tibial osteotomy: Factors that influence the duration of satisfactory function. Clin Orthop 1988;229:193-200. Marti CB, Gautier E, Wachtl SW, et al: Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 2004;20:366-372. Marti RK, Verhigan RA, Kerkhoffs GM, et al: Proximal tibial varus osteotomy: Indications, technique, and five to twenty-one-year results. J Bone Joint Surg Am 2001;83:164-170. Flierl S, Sabo D, Hornig K, et al: Open wedge high tibial osteotomy using fractioned drill osteotomy: A surgical modification that lowers the complication rate. Knee Surg Sports Traumatol Arthrosc 1996;4:149-153.
Question 215
High Yield
Which of the following best characterizes the antigenicity of allograft bone?
Explanation
Cell surface glycoproteins present in the heterogeneous population of the cells within the graft are primarily responsible for the antigenicity. Macromolocules of the matrix have also been implicated. Cryopreserved grafts have less antigenicity than fresh. Freezing, freeze-drying, or chemical sterilization and antigen extraction of the bone allograft have all been shown to reduce the antigenicity of the graft. Freeze-drying of retroviral-infected cortical bone and tendon does not inactivate retrovirus. Immunosuppression has been shown to decrease response. Hematopoietic elements along with osteogenic, chondrogenic, fibrous, and vascular cells have been shown to be antigenic. Crawford MJ, Swenson CL, Arnoczky SP, et al: Lyophilization does not inactivate infectious retrovirus in systemically infected bone and tendon allografts. Am J Sports Med 2004;32:580-586. Stevenson S, Li XQ, Davy DT, et al: Critical biological determinants of incorporation of non-vascularized cortical bone grafts: Quantification of a complex process and structure. J Bone Joint Surg Am 1997;79:1-16.
Question 216
High Yield
Figures 12a and 12b show the radiographs of a 50-year-old patient who reports acute knee pain after sustaining a twisting injury while playing tennis. Examination is unremarkable. The next most appropriate step in management should consist of


Explanation
The radiographs show localized diffuse cortical thickening that is characteristic of melorheostosis. The condition may be monostotic or it may involve many bones in one extremity (monomelic) in the distribution of a sclerotome. Bone scans will show increased uptake at the site or sites of skeletal involvement. Long tubular bones are most commonly involved. Melorheostosis is usually asymptomatic and requires no treatment. On rare occasions, there may be associated soft-tissue contractures. Dorfman H, Czerniak B: Bone Tumors. St Louis, MO, Mosby Inc, 1998, pp 1105-1107. Campbell CJ, Papademetriou T, Bonfiglio M: Melorheostosis: A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am 1968;50:1281-1304.
Question 217
High Yield
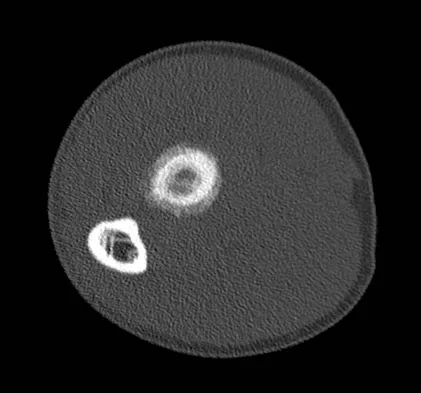
Figure 7 shows the CT scan of a 25-year-old soccer player who has had posterior ankle pain with plantar flexion for the past 2 years. Immobilization has failed to provide relief. He is ambulatory. Management should consist of
Explanation
An os trigonum is usually asymptomatic, but this accessory bone has been associated with persistent posterior ankle pain, which has been described as os trigonum syndrome. This usually affects athletes and ballerinas. Forced plantar flexion leads to impingement of the os trigonum against the posterior tibial plafond, and flexor hallucis tendinitis may develop. It may be difficult to differentiate a fractured trigonal process from the os trigonum. MRI may reveal bone marrow edema that may aid in the diagnosis of os trigonum syndrome. Steroid injections may lead to tendon rupture. The results of excision of a symptomatic os trigonum through a posteromedial or lateral approach are favorable, with a rapid return to full function. The main complication of this procedure is sural nerve injury with a lateral approach. Hedrick MR, McBryde AM: Posterior ankle impingement. Foot Ankle Int 1994;15:2-8.
Question 218
High Yield
A 32-year-old woman sustained an injury to her left upper extremity in a motor vehicle accident. Examination reveals a 2-cm wound in the mid portion of the dorsal surface of the upper arm and deformities at the elbow and forearm; there are no other injuries. Her vital signs are stable, and she has a base deficit of minus 1 and a lactate level of less than 2. Radiographs are shown in Figures 9a and 9b. In addition to urgent debridement of the humeral shaft fracture, management should include


Explanation
With a severe injury to the upper extremity, the best opportunity for achieving a good functional result for a floating elbow is immediate debridement of the open fracture, followed by internal fixation of the fractures. The ability to do this depends on the patient's physiologic status. In this patient, the procedure is acceptable because she has normal vital signs and no chest or abdominal injuries, and normal physiologic parameters (base excess and lactate) show adequate peripheral perfusion. The surgical approaches will be determined by the associated injury patterns and open wounds. In this patient, the humerus was debrided and stabilized through a posterior approach as was the medial condyle fracture. The ulna was fixed through an extension of the posterior incision and the radius through a separate dorsal approach. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 219
High Yield
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
Gradual dessication of the disk begins in the third decade as glycosaminoglycan levels within the nucleus begin to decline. The original water content of 88% decreases to 70% in the sixth decade and beyond. As glycosaminoglycan content decreases, there is a corresponding increase in noncollagen glycoprotein. Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868. Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
Question 220
High Yield
A 7-year-old boy has a limp with pain and tenderness over the distal right femur. Radiographs are shown in Figures 5a and 5b. Based on these findings, what is the best course of action?


Explanation
The patient has a nonossifying fibroma, and the symptoms suggest that there is significant weakening of the cortex and/or microfracture; therefore, biopsy, curettage, and bone grafting is the treatment of choice. Based on the size of the lesion and the presence of symptoms, observation is likely to result in pathologic fracture. A biopsy will further weaken the bone unless combined with curettage and bone grafting. Radiation therapy is not used in the treatment of nonossifying fibroma and is rarely used in any benign condition affecting skeletally immature individuals. Steroid injection has been used in the treatment of unicameral bone cysts and in Langerhan's cell histiocytosis but not for nonossifying fibroma. Dormans, JP, Pill SG: Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr Course Lect 2002;51:457-467.
Question 221
High Yield
A 13-year-old girl is referred for a painful progressive valgus deformity of the right knee. Examination reveals an antalgic gait with an obvious valgus deformity. The right distal femur has a palpable, tender mass with erythema and warmth. Figures 4a and 4b show a clinical photograph and a radiograph. Management should consist of


Explanation
The radiograph shows a pathologic fracture through a destructive lesion of the distal femur metaphysis with osteolytic and osteoblastic features. The lateral cortex is destroyed, and there is periosteal new bone formation. These findings are consistent with malignancy, most likely an osteogenic sarcoma. Patients with suspected malignant tumors are best managed by surgeons with specific expertise in orthopaedic oncology. The biopsy of a malignant lesion should be deferred to the surgeon who is capable of definitive management of the patient. Enneking W: Principles of musculoskeletal oncologic surgery, in Evarts C (ed): Surgery of the Musculoskeletal System. New York, NY, Churchill Livingston, 1990.
Question 222
High Yield
A 40-year-old man with an acetabular chondrosarcoma has a small soft-tissue mass. Treatment should consist of

Explanation
The treatment of choice for pelvic chondrosarcoma is wide resection via an internal hemipelvectomy. Chondrosarcoma requires surgical resection for control and does not respond to traditional chemotherapy or external beam radiation. Hip arthroplasty with acetabular reconstruction and curettage and cementation of the lesion are intralesional procedures that result in a higher incidence of local recurrence of tumor. Pring M, Weber KL, Unni K, Sim FH: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642.
Question 223
High Yield
A 17-year-old girl who initially presented as a child with multiple skeletal lesions, café-au-lait spots, and precocious puberty now has bone pain. A recent bone scan reveals multiple areas of increased scintigraphic uptake, including bilateral proximal femurs. A radiograph is shown in Figure 19. Besides activity modification, what is the next best line of treatment for decreasing her pain?

Explanation
McCune-Albright syndrome is the combination of polyostotic fibrous dysplasia, café-au-lait lesions, and endocrine dysfunction. The most common endocrine presentation is precocious development of secondary sexual characteristics. Compared with bone lesions in patients without polyostotic disease, the skeletal lesions in patients with the syndrome tend to be larger, more persistent, and associated with more complications. Bisphosphonate therapy has been shown in several studies to decrease the pain associated with the skeletal lesions of fibrous dysplasia. DiCaprio MR, Enneking WF: Fibrous dysplasia: Pathophysiology, evaluation and treatment. J Bone Joint Surg Am 2005;87:1848-1864.
Question 224
High Yield
A 63-year-old woman who sustained a distal radial fracture 2 months ago now reports that she is unable to achieve active extension of the thumb at the interphalangeal joint. What type of trauma may lead to this clinical finding?
Explanation
Nondisplaced distal radial fractures have a higher rate of spontaneous rupture of the extensor pollicis longus tendon. The extensor mechanism is felt to impinge on the tendon following a nondisplaced fracture and causes either a mechanical attrition of the tendon or a local area of ischemia in the tendon. Helal B, Chen SC, Iwegbu G: Rupture of the extensor pollicis longus tendon in undisplaced Colles' type of fracture. Hand 1982;14:41-47.
Question 225
High Yield
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?
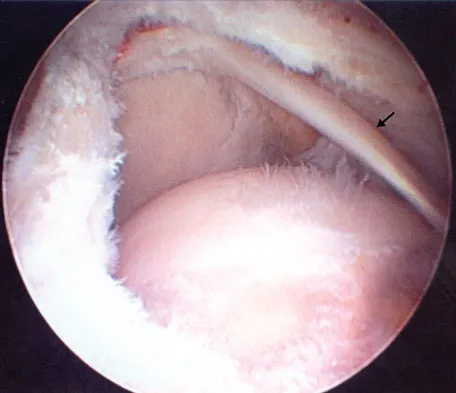
Explanation
This view from the lateral portal shows a full-thickness rotator cuff tear. The glenohumeral joint can be visualized through this tear. The glenoid, labrum, and biceps tendon attaching to the superior aspect of the glenoid are easily viewed from this portal, and the arrow is pointing to the biceps tendon. Arthroscopic rotator cuff repair can be performed while visualizing from this portal and using anterior and posterior working portals. Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principles of techniques, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Question 226
High Yield
For the athlete performing heavy exercise, the magnitude of core temperature and heart rate increase is most proportional to

Explanation
Studies examining the impact of graded water debt have clearly shown that the magnitude of core temperature and heart rate increase accompanying work are proportional to the magnitude of water debt at the onset of exercise. Though added thermal burden from hot climates is a factor, it appears to be less significant. Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524. Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Question 227
High Yield
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?
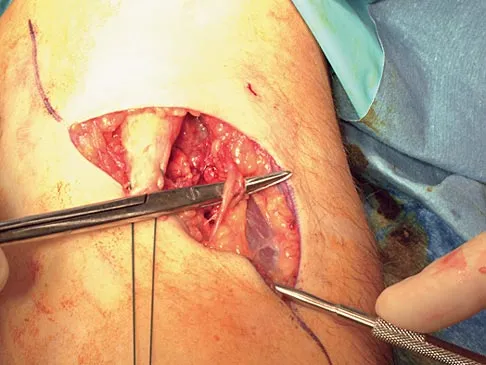
Explanation
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach. Kelly EW, Morrey BF, O'Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Question 228
High Yield
A patient with rheumatoid arthritis with both ankle and subtalar involvement was treated as shown in Figures 11a and 11b. What complication is unique to this type of fixation?


Explanation
The interlocking screws at the proximal end of the rod can act as a stress riser and lead to fracture. Postoperative pain at this level should prompt inclusion of this diagnosis in the differential. Removing the screws following bone union can decrease the chances of this occurring. A short rod that avoids the diaphyseal area may also be beneficial. Rotatory deformity is controlled by the perpendicularly oriented distal transfixion screws. Talar osteonecrosis would be unusual since the dissection can be minimized with an intramedullary rod. Any type of hardware can fail if the construct does not lead to a solid arthrodesis. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 236-237. Thordarson DB, Chang D: Stress fractures and tibial cortical hypertrophy after tibiotalocalcaneal arthrodesis with an intramedullary nail. Foot Ankle Int 1999;20:497-500.
Question 229
High Yield
A 42-year-old man sustained the periprosthetic fracture shown in Figures 19a and 19b. The femoral component is well fixed. What is the next most appropriate step in management?

Explanation
The patient has a periprosthetic fracture below the femoral stem. The component is porous coated and well fixed. Open reduction and internal fixation, leaving the stem in place, can be performed when bone quality is good. Plating with or without allograft struts and supplemental cerclage fixation generally is acceptable. If the component is loose, revision to a longer device is recommended with appropriate stabilization of the fracture using the aforementioned methods. If bone loss has occurred, allograft supplementation or a tumor prosthesis may be indicated. Fractures located well below the stem tip can be treated without regard for the prosthesis. Closed reduction and bracing is not associated with good results for periprosthetic femoral fractures. Retrograde intramedullary nailing is not appropriate for this fracture. Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Question 230
High Yield
Which of the following articulation couplings shows the lowest coefficient of friction as tested in the laboratory?
Explanation
Alumina ceramic is highly biocompatible when used as a biomaterial for joint arthroplasty implants. It has been shown to have good hardness, low roughness, and excellent wettability, therefore resulting in very low friction. However, it is expensive and limited reports have shown the problem of fracture on impact. The exact role for ceramic articulations is unknown at present. Cuckler JM, Bearcroft J, Asgian CM: Femoral head technologies to reduce polyethylene wear in total hip arthroplasty. Clin Orthop 1995;317:57-63.
Question 231
High Yield
The anticoagulant effect of the low-molecular-weight heparins (LMWH) is mediated by the binding affinity of antithrombin III to which of the following coagulation factors?

Explanation
Standard heparin mediates its anticoagulant effect largely through its interaction with antithrombin III. A conformational change in antithrombin III occurs that markedly accelerates its ability to inactivate the coagulation enzymes thrombin factor (II), factor Xa, and factor IXa. In contrast, LMWHs do not contain the necessary saccharide units to bind thrombin and antithrombin III simultaneously. The anticoagulant effect of LMWHs involves binding of antithrombin III to factor Xa.
Question 232
High Yield
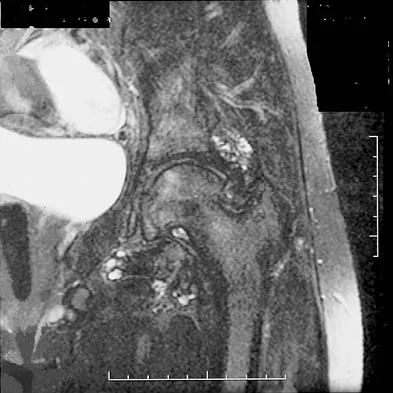
Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?
Explanation
In pediatric patients who have pain and recurrent hemarthrosis in the knee, hemangioma is often seen as an internal derangement of the knee, and long delays in diagnosis are common. An MRI scan is noninvasive and will best aid in diagnosis. In this patient, the MRI scan shows a hemangioma with no evidence of meniscal injury or discoid meniscus. Hemophilia is unlikely because the patient is female. The presence of hemarthrosis makes JRA an unlikely diagnosis.
Question 233
High Yield
A 10-year-old boy who is active in soccer has had activity-related heel pain for the past 3 months. Examination reveals tenderness over the posterior heel and a tight Achilles tendon. Radiographs demonstrate a 2-cm cyst in the anterior body of the calcaneus. His physes have not closed. Based on these findings, what is the most appropriate management?

Explanation
The most likely diagnosis is Sever's disease, which is considered either an apophysitis or a para-apophyseal stress fracture. It is common in athletic children and is associated with a tight Achilles tendon. Cast immobilization may be necessary if activity reduction fails. Calcaneal cysts are quite common and do not require any further diagnostic testing or treatment unless they occupy the full width of the calcaneus or one third of the length of the calcaneus. Ogden JA, Ganey TM, Hill JD, et al: Sever's injury: A stress fracture of the immature calcaneal metaphysis. J Ped Orthop 2004;24:488-492.
Question 234
High Yield
What is the typical MRI signal intensity of bone marrow affected by acute osteomyelitis?

Explanation
The classic MRI findings of osteomyelitis are a decrease in the normally high signal intensity of marrow on T1-weighted images and normal or increased signal intensity on T2-weighted images. This is the result of replacement of marrow fat by inflammatory cells and edema, which causes lower signal intensity than fat on T1-weighted images and higher signal intensity than fat on T2-weighted images. The addition of gadolinium to a T1-weighted sequence reveals increased signal intensity in the hyperemic marrow. Unger E, Moldofsky P, Gatenby R, et al: Diagnosis of osteomyelitis by MR imaging. Am J Roentgenol 1988;150:605-610. Dormans JP, Drummond DS: Pediatric hematogenous osteomyelitis: New trends in presentation, diagnosis and treatment. J Am Acad Orthop Surg 1994;2:333-341.
Question 235
High Yield
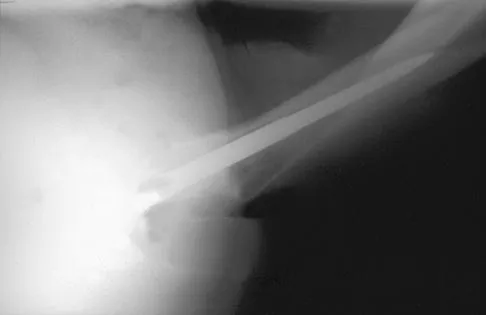
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 236
High Yield
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?


Explanation
The floating elbow is best managed with early open reduction and internal fixation of the humeral and forearm fractures, followed by early range of motion. These fractures predispose the elbow to stiffness, and early range of motion is recommended. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 237
High Yield
A 42-year-old woman with a long-standing history of rheumatoid arthritis undergoes total shoulder arthroplasty for persistent pain that has failed to respond to nonsurgical management. Intraoperative radiographs reveal an oblique, minimally displaced fracture of the greater tuberosity. Based on these findings, what is the best course of action?

Explanation
The risk of intraoperative fracture in osteoporotic bone in patients with rheumatoid arthritis is significant. Fractures most often occur during humeral head dislocation and positioning for canal reaming. If the fracture occurs at the greater tuberosity, cerclage suture fixation of the tuberosity fracture with autogenous cancellous bone graft from the resected humeral head is the treatment of choice. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 215-225.
Question 238
High Yield
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include

Explanation
The patient has severe acetabular protrusio, a condition that is frequently associated with Marfan syndrome. An echocardiogram is necessary to rule out the most serious consequence of this syndrome, aortic root widening, which can lead to aortic valve dysfunction or fatal aortic rupture. An electromyogram may be indicated for Charcot-Marie-Tooth disease, which is associated with acetabular dysplasia, but not protrusio. The renal ultrasound, the MRI scan, and the biopsy would be of no value in this patient. Protrusio can also be seen in patients with osteogenesis imperfecta and juvenile rheumatoid arthritis. Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Question 239
High Yield
What patient factor is predictive of better outcomes for surgical management of a displaced calcaneal fracture compared to nonsurgical management?
Explanation
A recent randomized trial of surgical versus nonsurgical management of calcaneal fractures showed that patients who were on workers' compensation did poorly with surgical care. These patients had less favorable outcomes regardless of their initial management. Factors such as age, smoking, and vasculopathies compromise skin healing, leading to greater surgical risks. The best results were obtained in patients who are younger than age 40 years, have unilateral injuries and are injured during noncompensable activities. Women tend to do better with surgery than men. Howard JL, Buckley R, McCormack R, et al: Complications following management of displaced intra-articular calcaneal fractures: A prospective randomized trial comparing open reduction internal fixation with nonoperative management. J Orthop Trauma 2003;17:241-249.
Question 240
High Yield
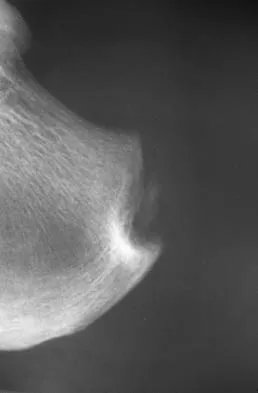
A 65-year-old man has chronic Achilles insertional tendinitis that is refractory to nonsurgical management. A radiograph is shown in Figure 9. Preoperative counseling should include a discussion of the realistic duration of postoperative recovery. You should inform the patient that his expected recovery will last

Explanation
An older patient with calcaneal enthesopathy may take a year or more to recover after tendon debridement and calcaneal ostectomy. Young patients, and those with purely tendon pathology, may recover more quickly. McGarvey WC, Palumbo RC, Baxter DE, et al: Insertional Achilles tendinitis: Surgical treatment through a central tendon splitting approach. Foot Ankle Int 2002;23:19-25.
Question 241
High Yield
Which of the following is considered the most appropriate shoe modification following transmetatarsal amputation?
Explanation
Most patients who undergo transmetatarsal amputation do not require custom shoe wear or an orthosis above the ankle. A molded toe filler is used to prevent excessive shear that can lead to ulceration. Use of a soft toe filler without stiffening of the sole results in excessive flexibility from the shortened lever arm, which reduces the efficiency of gait. A firm footplate or carbon fiber base adds rigidity to aid in push-off. A rocker bottom also may be added to the shoe. Philbin TM, Leyes M, Sferra JJ, Donley BG: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Question 242
High Yield
A 35-year-old woman who underwent open reduction and internal fixation of a calcaneal fracture 14 months ago reports pain that has failed to respond to nonsurgical management. Examination reveals limited painful subtalar motion but no hindfoot deformity. A lateral radiograph is shown in Figure 6. Surgical reconstruction is best accomplished with

Explanation
The patient has posttraumatic subtalar joint arthrosis that developed following a calcaneal fracture. Because there is no hindfoot deformity, in situ subtalar joint arthrodesis is the treatment of choice. Calcaneal osteotomy or distraction bone block arthrodesis is beneficial in patients with severe talar dorsiflexion or malunion of the calcaneal body. Triple arthrodesis is not warranted without changes at the transverse tarsal joint, and typically even with injury into the calcaneocuboid joint, this joint is often asymptomatic. Pantalar arthrodesis is not indicated as the pathology is occurring at the subtalar joint and not in the ankle joint. Sanders R: Fractures and fracture-dislocations of the calcaneus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1422-1464. Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Question 243
High Yield
A 26-year-old woman sustained a nondisplaced femoral neck fracture and treatment consisted of use of percutaneous cannulated screws. At her 3-month follow-up visit, she reports hip pain and is unable to ambulate. A radiograph is shown in Figure 1. What is the next most appropriate treatment?

Explanation
Femoral neck fracture nonunion is a challenging problem for orthopaedic surgeons. Vertical fractures are more prone to nonunion due to shear stress rather than compressive forces across the fracture site. Several authors have suggested these fractures are more common in young adults due to injury type and bone composition. It is widely regarded that an effort should be made to salvage the femoral head if vascularity remains. The most common method to treat this complication is valgus intertrochanteric osteotomy of the femur. This functionally makes a vertical fracture more horizontal, converting shear into compressive forces. It also helps correct the varus position of the fracture nonunion. Hartford JM, Patel A, Powell J: Intertrochanteric osteotomy using a dynamic hip screw for femoral neck nonunion. J Orthop Trauma 2005;19:329-333.
Question 244
High Yield
A patient who is an observant Jehovah's Witness requires major surgery for scoliosis that will likely result in significant blood loss. Which of the following might the patient consider allowing the surgical team to use?

Explanation
Jehovah's Witnesses will not accept the transfusion of blood or blood products such as packed red or white cells, platelets, or plasma. However, many Jehovah's Witnesses will accept the use of a cell saver in a "closed circuit." Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Question 245
High Yield
One advantage of using onlay strut allograft in femoral revision surgery is that it can

Explanation
Onlay grafts can provide more structural support than morcellized grafts. They are more easily incorporated into the host femur than bulk segmental total femur allografts; however, the incorporation is never complete. The use of onlay grafts is principally directed at addressing segmental defects of the femur; their use can be applied with either cementless or cement fixation of the femoral stem. Emerson RH Jr, Malinin TI, Cuellar AD, Head WC, Peters PC: Cortical strut allografts in the reconstruction of the femur in revision total hip arthroplasty: A basic science and clinical study. Clin Orthop 1992;285:35-44. Pak JH, Paprosky WG, Jablonsky WS, Lawrence JM: Femoral strut allografts in cementless revision total hip arthroplasty. Clin Orthop 1993;295:172-178.
Question 246
High Yield
A study is conducted to measure the difference in bone mineral density between postmenopausal women taking a drug treatment versus those taking a placebo. What is the most important result to be reported from this study?
Explanation
A complete answer necessarily includes the means and standard deviations of bone mineral density in both groups. Given these, which are the basic results of the study, the P-value can be calculated if desired. All of the other options preclude assessment of the actual data, that is, the information collected by the study. P-values and confidence intervals should be perceived as additional information, which help to assess the certainty of relating the study's findings to the general population, but they should not be reported instead of the results (ie, the means and standard deviations).
Question 247
High Yield
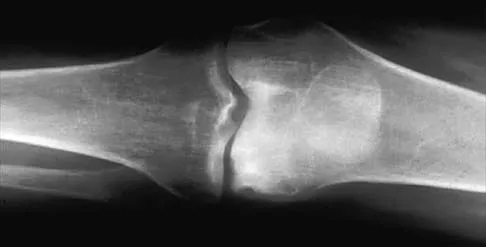
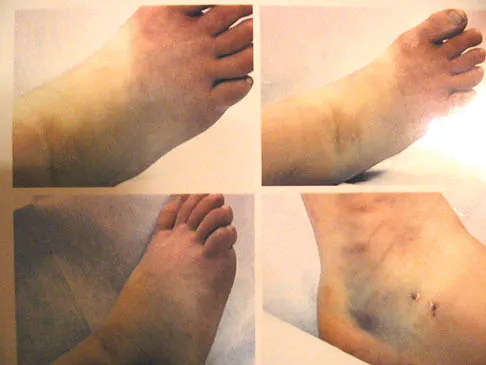
The condition shown in Figures 9a and 9b is most likely the result of


Explanation
The clinical photograph and radiograph show gout, which is the result of urate deposition in the joint and soft tissues. Radiographs frequently reveal periarticular erosions. The crystals are intracellular and negatively birefringent under the polarized microscope. Treatment for acute flares include colchicines, indomethacin, and corticosteroids (including injections). Medications such as allopurinol help prevent recurrent flares. Tophi such as that seen in this patient are often confused with and associated with infection. Wortmann RL, Kelley WM: Crystal-induced inflammation: Gout and hyperuricemia, in Harris ED, Budd RC, Firestein GS, et al (eds): Kelley's Textbook of Rheumatology, ed 7. New York, NY, Elsevier Science, 2005, pp 1402-1429. Trumble TE (ed): Hand Surgery Update 3: Hand, Elbow, & Shoulder. Rosemont, IL, American Society for Surgery of the Hand, 2003, pp 433-457.
Question 248
High Yield
Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?

Explanation
The radius of curvature of the distal femur is greater over the distal aspect of the lateral femoral condyle than the distal aspect of the medial femoral condyle. As the femur rolls posteriorly during early knee flexion, both condyles undergo similar angular changes equal to the amount of flexion. With a similar amount of angular rotation, the sphere with the larger radius experiences greater net rollback, producing a pivoting motion. Although the anterior cruciate ligament plays a role in producing tibial rotations, the posterior cruciate ligament does not play a significant role in producing such rotations. Similarly, the tibial tubercle does not play a significant role in producing normal rotations of the femur relative to the tibia. The popliteus may also play a role in producing rotational pivots, as might differential laxity of the medial and lateral collateral ligaments in early knee flexion. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.
Question 249
High Yield
Figures 9a and 9b show the spinal radiographs of a 3-year-old child with short limb dwarfism. The lateral radiograph is obtained with maximal lumbar extension. Management should consist of


Explanation
The patient has kyphosis in association with achondroplasia. The AP radiograph shows decreased interpedicular distance at the lower lumbar vertebrae, a feature considered to be a distinctive sign of achondroplasia. Most patients with achondroplasia have kyphosis, and this usually resolves spontaneously. When the fixed component is greater than 30 degrees, however, brace treatment is recommended. Spinal fusion is seldom required.
Question 250
High Yield
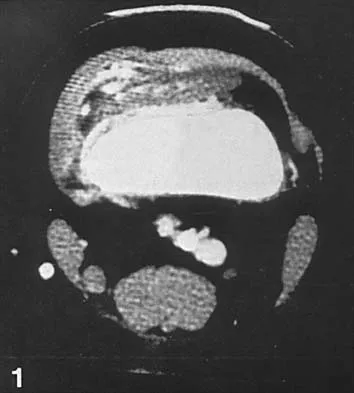
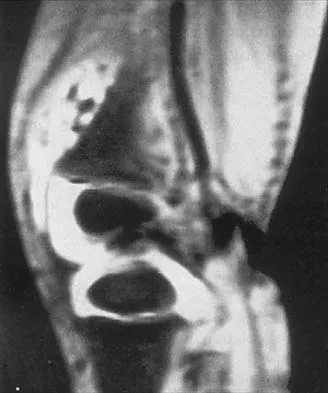
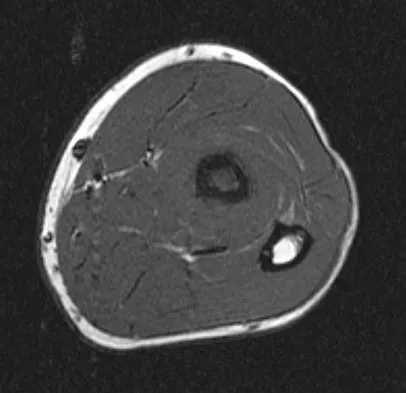
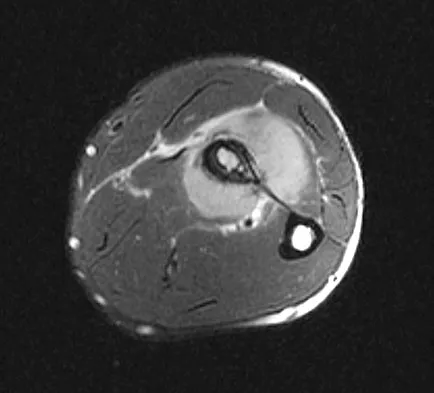
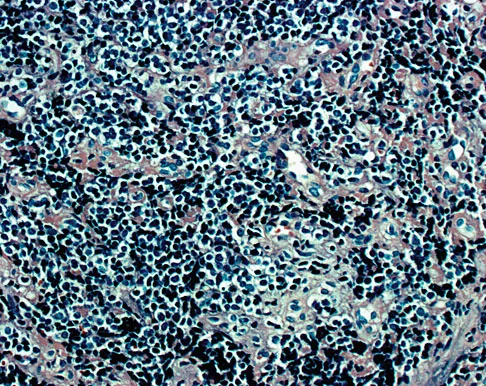
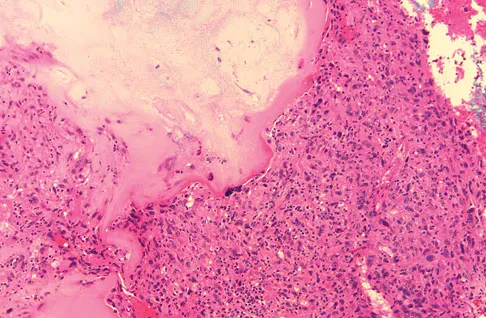
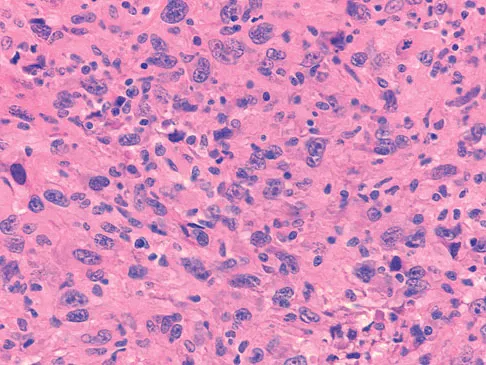
Figures 1a through 1c show the radiograph and MRI scans of a 16-year-old patient who has a painful hip. Examination reveals a significant limp, limited abduction and internal rotation, and severe pain with internal rotation and adduction. A biopsy specimen is shown in Figure 1d. What is the deposited pigment observed in this condition?


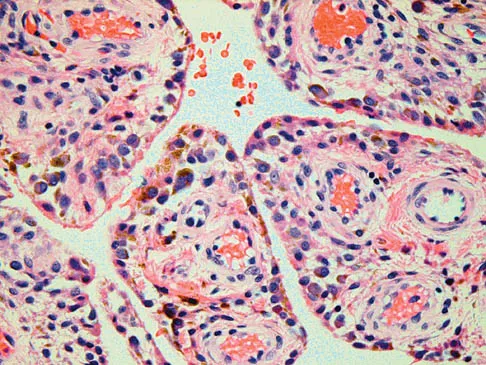
Explanation
Pigmented villonodular synovitis (PVNS) is a synovial proliferative disorder that remains a diagnostic difficulty. The most common clinical features are mechanical pain and limited joint motion. On radiographs, the classic finding is often a large lesion, associated with multiple lucencies. Other findings may include a normal radiographic appearance, loss of joint space, osteonecrosis of the femoral head, or acetabular protrusion. MRI is the imaging modality of choice and will show the characteristic findings of a joint effusion, synovial proliferation, and bulging of the hip. The synovial lining has a low signal on T1- and T2-weighted images, secondary to hemosiderin deposition. Copper deposition occurs in patients with Wilson's disease, which mainly affects the liver. Bhimani MA, Wenz JF, Frassica FJ: Pigmented villonodular synovitis: Keys to early diagnosis. Clin Orthop 2001;386:197-202.
Question 251
High Yield
During a retroperitoneal approach to the L4-5 disk, what structure must be ligated to safely mobilize the common iliac vessels toward the midline from laterally and gain exposure?

Explanation
To mobilize the common iliac vessels across the midline, the iliolumbar vein must be ligated. It has a short trunk and can be torn if mobilization is attempted without ligation. It is the only branch off the common iliacs (there are no arterial branches) prior to the terminal branches, the internal (hypogastric) and external iliacs. The middle sacral vessels run distally from the axilla of the bifurcation and are a factor when accessing the L5-S1 disk. Baker JK, Reardon PR, Reardon MJ, et al: Vascular injury in anterior lumbar surgery. Spine 1993;18:2227-2230.
Question 252
High Yield
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20 degrees. Management should consist of
Explanation
Indications for surgical treatment of spondylolisthesis include pain and/or progression of deformity. Specifically, surgery is necessary when there is persistent pain or a neurologic deficit that fails to respond to nonsurgical therapy, there is significant slip progression, or the slip is greater than 50%. For patients with mild spondylolisthesis, in situ posterolateral L5-S1 fusion is adequate. In patients with more severe slips (greater than 50%), extension of the fusion to L4 offers better mechanical advantage. Postoperative immobilization may be achieved with instrumentation, casting, or both. In patients with a slip angle of greater than 45 degrees, reduction of the lumbosacral kyphosis with instrumentation or casting is desirable to prevent slip progression. Laminectomy alone is contraindicated in a child. Nerve root decompression is indicated if radiculopathy is present clinically. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Question 253
High Yield
An 11-year-old girl sustained an injury to her right foot when a 500-lb headstone fell on it. The headstone was removed after 3 minutes. Radiographs show multiple midfoot fractures. Examination reveals severe pain that is worse with passive toe motion. Clinical photographs are shown in Figure 28. Management should consist of
Explanation
The patient has a classic history and examination for an acute compartment syndrome of the foot. CT, MRI, or stress radiographs are not necessary prior to emergent fasciotomies of the foot. These studies can be performed after the initial fasciotomies to determine the best long-term management of the fractures. There are nine compartments in the foot. These are decompressed through three incisions (two on the dorsal foot and one medially). A short leg cast does not address the compartment syndrome and could be limb threatening with excessive swelling in a circumferential cast. It is preferable to splint severe crush injuries rather than apply a cast. Fulkerson E, Razi A, Tejwani N: Review: Acute compartment syndrome of the foot. Foot Ankle Int 2003;24:180-187.
Question 254
High Yield
Turf toe typically involves injury to which of the following structures of the great toe?
Explanation
The term turf toe includes a range of injuries of the capsuloligamentous complex of the first metatarsophalangeal joint with or without osteochondral fracture of the first metatarsal head or one of the sesamoids. The mechanism of injury is hyperextension. Clanton TO, Butler JE, Eggert A: Injuries to the metatarsophalangeal joints in athletes. Foot Ankle 1986;7:162-176.
Question 255
High Yield
The spread of malignant cells to the vertebrae is often through
Explanation
In 1940, Batson described a valveless plexus of veins that extend from the dural venous sinuses of the skull to the sacrum. This system permits retrograde blood flow and enables tumor cells to enter vertebral bodies at multiple levels. Increased intra-abdominal pressure will enhance this retrograde blood flow.
Question 256
High Yield
What neurovascular structure is most at risk when performing an inside-out repair of the posterior horn of the medial meniscus?
Explanation
The saphenous nerve is located on the posterior medial aspect of the knee and must be protected when performing an inside-out repair of the medial meniscus. The peroneal nerve is most at risk with lateral meniscal repairs. The other structures usually are not at risk with meniscal repair. Cannon WD Jr, Morgan CD: Meniscal repair: Arthroscopic repair techniques. Instr Course Lect 1994;43:77-96.
Question 257
High Yield
A 32-year-old man who sustained a tarsometatarsal (Lisfranc) injury 3 years ago now reports increasing pain in the left foot. Orthotics, nonsteroidal anti-inflammatory drugs, and injections have provided only temporary relief. Examination reveals swelling and tenderness over the tarsometatarsal joints. Radiographs show advanced arthrosis of the first and second tarsometatarsal joints. Management should now include

Explanation
The patient has advanced arthrosis of the midfoot, and orthotic management has failed to provide relief. Therefore, the treatment of choice is midfoot arthrodesis. Shock wave treatment has not been shown to be beneficial for arthritis. An ankle-foot orthosis would not be appropriate based on findings of a normal ankle joint. Triple arthrodesis would not be helpful because the hindfoot joint is not affected in a Lisfranc injury. Sangeorzan BJ, Veith GR, Hansen ST Jr: Salvage of Lisfranc's tarsometatarsal joints by arthrodesis. Foot Ankle 1990;10:193-200.
Question 258
High Yield
A 45-year-old man who has had recurrent pain and swelling of the left Achilles tendon insertion for the past 10 years reports that physical therapy and activity modification have provided relief in the past. He now has continued pain despite these efforts. He also reports occasional bouts of dysuria that he attributes to a history of prostatitis. He also notes recent eye irritation that he attributes to allergies. A lateral heel radiograph is shown in Figure 33. Which of the following laboratory studies would best aid in diagnosis?
Explanation
Reiter's syndrome is a seronegative spondyloarthropathy characterized most commonly by a triad of asymmetric arthritis, urethritis, and uveitis. Tendon ensethopathies can also be present. It is most often seen in men and is associated with a positive HLA-B27 marker. Rheumatoid arthritis does not usually present with these features; more commonly it causes forefoot pain and synovitis of the metatarsophalangeal joints. A CBC count with differential would be helpful in a situation of possible infection. The urethral swab would help to diagnose a gonococcal infection which can cause a monoarticular septic arthritis. Antiphospholipid antibody is associated with a hypercoaguable state and increased risk of deep venous thrombosis.
Question 259
High Yield
What type of nerve palsy is most common following elbow arthroscopy?

Explanation
Transient ulnar nerve palsy is the most common palsy following elbow arthroscopy. The ulnar nerve is most frequently affected, followed by the radial nerve. Injury to the other nerves has been reported but less frequently. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
Question 260
High Yield
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?

Explanation
The patient has a periprosthetic fracture around a loose cemented femoral component. The proximal bone stock is poor; therefore, this fracture may be categorized as Vancouver 3-B. Hip arthrodesis and resection arthroplasty provide suboptimal results, particularly for ambulatory patients. Although impaction allografting may be an option to restore the bone stock in a younger patient, the latter procedure will be very difficult to perform when the proximal bone is poor in quality and fractured. Cementing another component into this wide femur is not an option. The best option for revision of the femoral component in this elderly patient is proximal femoral replacement arthroplasty. Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Question 261
High Yield
A 55-year-old woman who underwent a left total hip arthroplasty 8 months ago using a modified Hardinger approach reports a persistent painless limp. Examination reveals that when she is not using a cane, she lurches to the left during weight bearing on the left lower extremity. An AP radiograph is shown in Figure 29. Which of the following hip muscle groups should be strengthened to improve the gait abnormality?

Explanation
The modified Hardinger approach includes a partial anterior trochanteric osteotomy creating a trochanteric wafer (as seen on the radiograph) that is displaced anterior and medial in continuity with the gluteus medius and vastus lateralis. Failure of abductor reattachment, migration of the trochanter, nonunion of the osteotomy site, and excessive splitting of the gluteus medius muscle causing injury to the inferior branch of the superior gluteal nerve can result in weakness of the abductor mechanism. Abductor strength should be evaluated with the patient lying on the opposite side and elevating the affected limb. Although slight weakness may manifest itself as a limp only after prolonged muscular activity, significant weakness results in a constant limp without associated discomfort. Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 512-526.
Question 262
High Yield
An 20-year-old elite college football player has ecchymosis, swelling, and pain on the lateral side of his foot after a game. Radiographs are shown in Figures 31a through 31c. Management should consist of


Explanation
Metaphyseal-diaphyseal junction fractures of the fifth metatarsal require careful evaluation. In athletes, early intervention with a 4.5-mm intramedullary screw correlates with an earlier return to activity. One study examining the failure of surgically managed Jones fractures revealed that use of anything other than a 4.5-mm malleolar screw for internal fixation correlated with failure. Glasgow MT, Naranja RJ Jr, Glasgow SG, et al: Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: The Jones fracture. Foot Ankle Int 1996;17:449-457.
Question 263
High Yield
Figures 32a and 32b show the radiographs of a 13-year-old right hand-dominant boy who sustained a closed Salter-Harris type II fracture of the proximal humerus during a hockey game. The shoulder has significant swelling, but is neurovascularly intact. What treatment offers the best chance of reestablishing normal shoulder motion?


Explanation
The patient has a significantly angulated proximal humerus fracture with a high degree of varus angulation, and rotational malalignment is likely. Failure to correct the varus angulation will result in permanent loss of shoulder abduction because the patient's age limits bony remodeling. These fractures are inherently unstable due to the inability to control the proximal fracture alignment. Shoulder spica casts have a high rate of redisplacement after treatment. Adequate open or closed reduction and pin fixation in the operating room optimizes alignment and all but eliminates the chance of redisplacement. Dobbs MB, Luhmann SJ, Gordon JE, et al: Severely displaced proximal humerus epiphyseal fractures. J Pediatr Orthop 2003;23:208-215. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, p 701.
Question 264
High Yield
Which of the following methodologies has been proven to be effective in reducing the use of homologous blood transfusion following total hip arthroplasty (THA)?

Explanation
A variety of methodologies have been used to decrease the need for homologous blood transfusions following THA. Some of the effective strategies include preoperative donation of autologous units, intraoperative salvage and recycling, preoperative injection of erythropoietin, and regional anesthesia. Cementless fixation and use of wound drains have been shown to increase the blood loss with THA. Huo MH, Paly WL, Keggi KJ: Effect of preoperative autologous blood donation and intraoperative and postoperative blood recovery on homologous blood transfusion requirement in cementless total hip replacement operation. J Am Coll Surg 1995;180:561-567. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 265
High Yield
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome?



Explanation
The patient has a displaced burst fracture. Fusion with instrumentation has shown better results than casting alone. Posterior fusion with instrumentation, with sagittal plane correction, yields the best results. Decompression occurs indirectly with correction of the kyphosis. Anterior decompression is unnecessary. Lalonde F, Letts M, Yang JP, et al: An analysis of burst fractures of the spine in adolescents. Am J Orthop 2001;30:115-120. Clark P, Letts M: Trauma to the thoracic and lumbar spine in the adolescent. Can J Surg 2001;44:337-345.
Question 266
High Yield
Figure 24 shows the radiograph of a 10-year-old boy who sustained a valgus injury to the knee. Examination reveals grade III medial laxity. Initial management should consist of

Explanation
Based on the mechanism of injury and findings of medial laxity, the most likely diagnosis is injury to either the growth plate or the medial collateral ligament. With the open physeal plate, this area of injury is presumed present until proven otherwise; therefore, stress radiographs should be obtained before implementing any treatment or ordering more extensive and expensive tests. DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 406-432. Clanton TO, DeLee JC, Sanders B, Neidre A: Knee ligament injuries in children. J Bone Joint Surg Am 1979;61:1195-1201.
Question 267
High Yield
Patients with rheumatoid arthritis may exhibit an increase in viral load for which of the following viruses?
Explanation
Rheumatoid arthritis (RA) is a complex multisystem disorder. It has been suggested that patients with RA have an impaired capacity to control infection with Epstein-Barr virus. Epstein-Barr virus has oncogenic potential and is implicated in the development of some lymphomas. Recent publications provide evidence for an altered Epstein-Barr virus-host balance in patients with RA who have a relatively high Epstein-Barr virus load. Large epidemiologic studies confirm that lymphoma is more likely to develop in patients with RA than in the general population. The overall risk of development of lymphoma has not risen with the increased use of methotrexate or biologic agents. Histologic analysis reveals that most lymphomas in patients with RA are diffuse large B cell lymphomas, a form of non-Hodgkin lymphoma. Epstein-Barr virus is detected in a proportion of these. Patients with RA do not have prevalence for infection with any of the other mentioned viruses. Callan MF: Epstein-Barr virus, arthritis, and the development of lymphoma in arthritis patients. Curr Opin Rheumatol 2004;16:399-405.
Question 268
High Yield
A 19-year-old man has had pain and swelling in his left forearm for the past 8 months. Laboratory studies show a mildly elevated WBC count and erythrocyte sedimentation rate. Radiographs are shown in Figures 58a and 58b, a CT scan is shown in Figure 58c, and T1- and T2-weighted MRI scans are shown in Figures 58d and 58e, respectively. A biopsy specimen is shown in Figure 58f. Immunohistochemistry demonstrates that the lesion is negative for leukocyte common antigen (CD34). What is the most common cytogenetic translocation associated with this lesion?


Explanation
The imaging studies show a permeative lytic destructive lesion in the proximal radius with "hair-on-end" periosteal reaction and a large soft-tissue mass most consistent with Ewing's sarcoma. The pathology reveals monotonous sheets of "round blue" cells. This limits the differential diagnosis to primary lymphoma of bone versus Ewing's sarcoma. These are best differentiated by immunohistochemistry, cytogenetics, and flow cytometry. Lymphoma of bone is typically CD34 positive and CD99 negative; whereas, the reverse is true of Ewing's sarcoma, CD34 negative and CD99 positive. The most common cytogenetic translocation with Ewing's sarcoma is 11; 22; 21; 22 and 7; 22 translocations have also been reported in Ewing's sarcomas. The X; 18 translocation is most commonly associated with synovial cell sarcomas; the 12; 22 translocation is most commonly associated with clear cell sarcomas; the 2; 13 translocation is most commonly associated with alveolar rhabdomyosarcomas, and the 12; 16 translocation is most commonly associated with myxoid liposarcomas. Flow cytometry is used to characterize the cell types of lymphomas. Womer R: The cellular biology of bone tumors. Clin Orthop Relat Res 1991;262:12-21. Yamaguchi U, Hasegawa T, Morimoto Y, et al: A practical approach to the clinical diagnosis of Ewing's sarcoma/primitive neuroectodermal tumour and other small round cell tumours sharing EWS rearrangement using new fluorescence in situ hybridisation probes for EWSR1 on formalin fixed, paraffin wax embedded tissue. J Clin Pathol 2005;58:1051-1056.
Question 269
High Yield
When performing a Weil osteotomy of a lesser metatarsal, the desired angle of the saw cut should be approximately
Explanation
Appropriate orientation of the saw cut when performing a Weil osteotomy is approximately parallel with the plantar surface of the foot. This is done in an effort to minimize plantar displacement of the capital fragment. The removal of additional bone from the osteotomy site either by removing a separate wafer of bone or using a thicker saw blade has also been described to minimize plantar displacement of the distal fragment. Trnka H, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Question 270
High Yield
In the upright standing position, approximately what percent of the vertical load is borne by the lumbar spine facet joints?

Explanation
Direct measurement and finite element modeling results show that approximately 20% of the vertical load is borne by the posterior structures of the lumbar spine in the upright position. Adams MA, Hutton WC: The effect of posture on the role of the apophyseal joints in resisting intervertebral compressive forces. J Bone Joint Surg Br 1980;62:358-362.
Question 271
High Yield
What is the most common surgical cause of the foot deformity shown in Figure 9?

Explanation
The radiograph shows a hallux varus deformity. Iatrogenically acquired hallux varus is most often the result of excessive lateral soft-tissue release, sesamoidectomy, or both. It also can be caused by a medial tibial sesamoid subluxation in conjunction with excessive postoperative dressing application, overcorrection of the intermetatarsal angle, or excessive medial eminence resection. Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Question 272
High Yield
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of
Explanation
The patient has a symptomatic painful atrophic midclavicular nonunion, and the treatment of choice is rigid internal fixation with a dynamic compression plate and autogenous bone grafting. A tension band effect is desired and achieved by placing the plate superiorly. Excellent success rates of 90% to 100% have been reported using this technique. Intramedullary screw fixation without bone grafting has a decreased success rate. Partial claviculectomy is not a preferred option. Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Question 273
High Yield
A 73-year-old man stepped off a street curb and felt a crack in his left hip. He is now unable to bear weight. A radiograph is shown in Figure 54a. Biopsy specimens are shown in Figures 54b and 54c. What is the most likely diagnosis?

Explanation
The biopsy specimens reveal a high-grade spindle cell lesion adjacent to an area of benign cartilage. This is consistent with a dedifferentiated chondrosarcoma. The radiograph shows a pathologic fracture through a lesion characterized by calcification within the left greater trochanter. Distal to the area of calcification, there is a more osteolytic, destructive appearance. Synovial sarcoma has a biphasic appearance histologically with areas of glandular differentiation that stain positive with keratin. Metastatic prostate cancer, although osteoblastic in appearance, would have a glandular histologic appearance. There is no cartilage in these lesions. Classic low-grade chondrosarcoma does not have an area of high-grade pleomorphic spindle cells within the lesion. A periosteal osteosarcoma is a surface-based lesion with a sunburst radiographic pattern. Although there may be cartilage in the lesion histologically, there are also malignant cells producing osteoid. Dedifferentiated chondrosarcoma is an aggressive, high-grade variant of chondrosarcoma. Wold LE, Adler CP, Sim FH, et al: Atlas of Orthopedic Pathology, ed 2. Philadelphia, PA, WB Saunders, 2003, p 269.
Question 274
High Yield
Figure 11 shows the radiograph of a 2-year-old child with marked genu varum and tibial bowing. Based on these findings, what is the best initial course of action?

Explanation
The radiograph shows multiple wide physes, consistent with a diagnosis of rickets. A low serum phosphorous level and an elevated alkaline phosphatase level are the hallmarks in diagnosing familial hypophosphatemic Vitamin D-resistant rickets. Serum calcium is usually normal or low normal. This disease is inherited as an X-linked dominant trait and usually presents at age 18 to 24 months. The disease results from a poorly defined problem with renal phosphate transport in which normal dietary intake of vitamin D is insufficient to achieve normal bone mineralization. Renal tubular dysfunction is associated with urinary phosphate wasting. Treatment involves oral phosphate supplementation, which can cause hypocalcemia and secondary hyperparathyroidism. To prevent associated problems, high doses of Vitamin D are administered. While obtaining a scanogram may be clinically indicated in an associated limb-length discrepancy, and subsequent corrective surgery may be indicated, either of these choices would not be the first course of action. An orthosis may slow the progression of genu varum in this disorder but is less important than establishing the correct diagnosis to begin pharmacologic treatment. This amount of varum and tibial bowing far exceeds the normal limits of physiologic genu varum. Skeletal dysplasias usually are not associated with abnormal laboratory values. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743.
Question 275
High Yield
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?

Explanation
Several studies have shown that sitting ability by age 2 years is highly prognostic of walking. Molnar and Gordon reported that children not sitting independently by age 2 years had a poor prognosis for walking. Wu and associates reported that children sitting without support by age 2 years had an odds ratio of 26:1 of walking compared with those unable to sit. This was far higher than the odds ratios for cerebral palsy location, motor dysfunction, crawling, creeping, scooting, or rolling. Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Question 276
High Yield
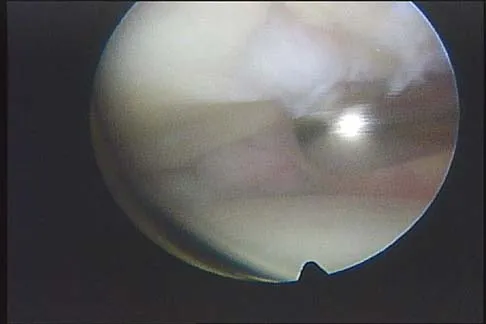
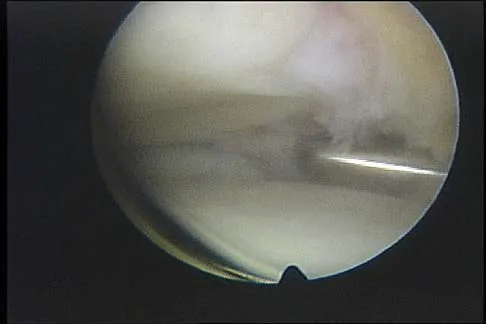
The arthroscopic views shown in Figures 31a and 31b reveal extensive synovitis in the anterolateral corner of the ankle overlying a band of tissue sometimes implicated in soft-tissue impingement of the ankle following a chronic sprain injury. This band is a portion of the
Explanation
The arthroscopic views show the lateral side of the ankle as demonstrated by the presence of the tibiofibular articulation. As is typical in chronic anterolateral impingement, synovitis overlies the anteroinferior band of the tibiofibular ligament, the most distal portion of the anterior syndesmosis. Hypertrophic scar formed on or in this ligament can impinge on the lateral margin of the talar dome and has been associated with chronic anterolateral ankle pain. Bassett FH III, Gates HS III, Billys JB, et al: Talar impingement by the anteroinferior tibiofibular ligament: A cause of chronic pain in the ankle after inversion sprain. J Bone Joint Surg Am 1990;72:55-59.
Question 277
High Yield
A 16-year-old ice hockey player is struck on the chest by the puck. He skates a few strides and then collapses. What is the most likely diagnosis?
Explanation
Sudden cardiac arrest following a blow to the chest in young athletes has been termed "commotio cordis." It is most common in Little League and other youth projectile sports (eg, ice hockey, lacrosse). The cause, although not completely determined, is most likely an arrhythmia related to the impact in a vulnerable time in the cardiac cycle. Resuscitation has proven to be exceedingly difficult, resulting in a high mortality rate. Maron BJ, Strasburger JF, Kugler JD, Bell BM, Brodkey FD, Poliac LC: Survival following blunt chest impact-induced cardiac arrest during sports activities in young athletes. Am J Cardiol 1997;79:840-841.
Question 278
High Yield
A 55-year-old man who works as a carpenter reports chronic right anterior shoulder pain and weakness. Examination reveals 90 degrees of external rotation (with the arm at the side) compared to 45 degrees on the left side. His lift-off examination is positive, along with a positive belly press finding. An MRI scan reveals a chronic, retracted atrophied subscapularis tendon. What is the most appropriate management of his shoulder pain and weakness?
Explanation
Chronic subscapularis tendon ruptures preclude primary repair. In such instances, subcoracoid pectoralis major tendon transfers may improve function and diminish pain. The subcoracoid position of the transfer allows redirection of the pectoralis major in a direction recreating the vector of the subscapularis tendon. Shoulder fusion is a salvage procedure, and corticosteroid injection may reduce pain but will not improve function. Jost B, Puskas GJ, Lustenberger A, et al: Outcome of pectoralis major transfer for the treatment of irreparable subscapularis tears. J Bone Joint Surg Am 2003;85:1944-1951.
Question 279
High Yield
Figure 2 shows the lateral radiograph of an 8-year-old boy who sustained an acute injury to the elbow after falling down the stairs. Management should consist of

Explanation
The patient has a flexion-type olecranon fracture, and the integrity of the extensor mechanism is disrupted. With this degree of displacement, closed reduction and extension casting would not be adequate. The strongest construct is an oblique screw across the fracture site, with a tension band. Healing is rapid in this age group; therefore one of the heavy absorbable sutures can be used as the tension band. Two parallel pins with the stainless steel tension band wire (AO technique) can be used but requires wire dissection for removal. Once the fracture is healed, the single screw can be removed easily with only a small incision. The presence of the screw, across the apophysis, has not been shown to produce any significant growth disturbance. Use of a large intramedullary screw would not be advisable because of the small size of the proximal fragment. Murphy DF, Greene WB, Gilbert JA, Dameron TB Jr: Displaced olecranon fractures in adults: Biomechanical analysis of fixation methods. Clin Orthop 1987;224:210-214.
Question 280
High Yield
Nonsurgical management of pectoralis major tears is likely to result in weakness of glenohumeral
Explanation
Nonsurgical management is considered for proximal tears as well as partial tears in some individuals. Surgical management is often not appropriate in older or sedentary patients. However, patients treated nonsurgically will have a significant cosmetic defect, as well as weakness in adduction and internal rotation. Schepsis AA, Grafe MW, Jones HP, et al: Rupture of the pectoralis major muscle: Outcome or repair of acute and chronic injuries: Am J Sports Med 2000;28:9-15.
Question 281
High Yield
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of
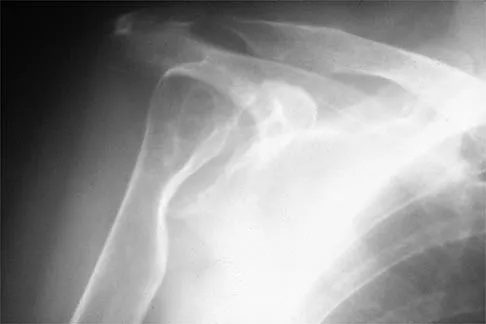
Explanation
Because the patient has end-stage rheumatoid arthritis with glenoid and rotator cuff deficiency, humeral arthroplasty is the treatment of choice. When a patient has an intact rotator cuff and there is sufficient glenoid bone stock to implant a glenoid component, total shoulder arthroplasty is the preferred method because it appears to provide more predictable pain relief. Glenohumeral arthrodesis is generally avoided when there is a functional deltoid or rotator cuff. Open synovectomy is appropriate in early rheumatoid disease before articular changes are present. Anterior acromioplasty with coracoacromial ligament resection is avoided in patients with rheumatoid arthritis because this procedure compromises the coracoacromial arch and may result in anterosuperior instability. Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337. Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271. Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Question 282
High Yield
An 18-year-old gymnast has had a 1-year history of foot pain. Examination reveals medial midfoot tenderness without swelling. Non-weight-bearing in a cast for 6 weeks has failed to provide relief. An axial CT scan of the midfoot is shown in Figure 20. What is the optimal treatment for this condition?
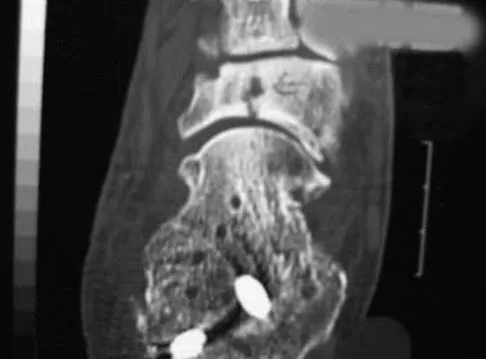
Explanation
Stress fractures of the navicular are often seen in running and jumping sports. Whereas most individuals heal with nonsurgical management consisting of 6 weeks of casting, this gymnast has had pain for 1 year and nonsurgical management has failed. Open reduction with bone grafting is the preferred treatment. Quirk RM: Stress fractures of the navicular. Foot Ankle Int 1998;19:494-496.
Question 283
High Yield
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic
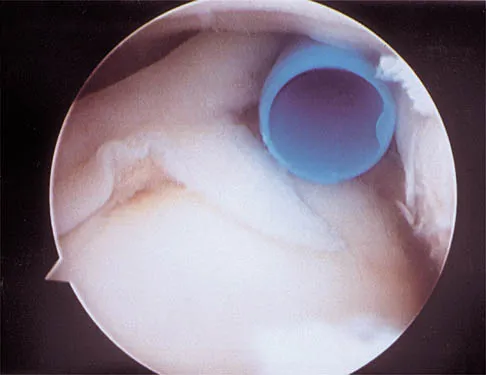
Explanation
The lesion is a variation of a type I superior labrum anterior and posterior lesion; therefore, appropriate treatment is simple debridement. Biceps tenodesis or release is not indicated because the biceps tendon and anchor are intact. There is no indication for labral repair or capsulorraphy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Question 284
High Yield
The radiograph shown in Figure 54 reveals that the plate on the second metacarpal is acting in what manner?

Explanation
There are four ways in which a plate acts: compression, tension bend, bridge or spanning, and buttress. Since there is no cortical contact with the large span of comminution, this plate is acting as a bridge plate. A bridge plate is defined as when the plate is used as an extramedullary splint attached to the two main fragments, leaving the comminution untouched.
Question 285
High Yield
Based on the radiographic findings shown in Figure 41, which of the following wrist ligaments is most likely disrupted?

Explanation
The radiograph shows a diastasis of the scapholunate interval, caused by certain failure of the scapholunate interosseous ligament. The lunotriquetral interosseous ligament stabilizes the lunotriquetral joint. The long radiolunate ligament originates in the volar radius and inserts in the lunate. The short radiolunate ligament originates on the ulnar margin of the radius and inserts on the ulnar margin of the lunate. The ulnolunate ligament originates at the ulnar styloid base and inserts on the volar aspect of the lunate. Linscheid RL, Dobyns JH, Beabout JW, et al: Traumatic instability of the wrist: Diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632. Mayfield JK, Johnson RP, Kilcoyne RK: Carpal dislocations: Pathomechanics and progressive perilunar instability. J Hand Surg Am 1980;5:226-241.
Question 286
High Yield
A 20-year-old man sustains the injury shown in Figures 1a and 1b in a motorcycle accident. In addition to a prompt closed reduction, his outcome might be optimized by


Explanation
Lateral subtalar dislocations, which are less common than medial subtalar dislocations, are high-energy injuries that are frequently associated with small osteochondral fractures. It is generally recommended that large fragments be internally fixed, and small fragments entrapped within the joint be excised. Although arthrosis frequently occurs after this injury and is the most common long-term complication, primary subtalar arthrodesis is not indicated. A talar neck fracture is not evident on the radiographs, and lateral subtalar dislocation usually does not lead to instability.
Question 287
High Yield
Which of the following findings is considered a contraindication for posterior decompression (with or without fusion) for myelopathy?

Explanation
Although cervical instability is a contraindication to posterior decompression alone, segmental instability in the myelopathic cervical spine can be addressed with concomitant posterior fusion with instrumentation. Cervical lordosis represents the ideal scenario for posterior decompressive procedures for myelopathy (laminectomy and laminoplasty) because compression from anterior osteophytes, if present, is relieved as the spinal cord migrates posteriorly. The anteroposterior diameter of the spinal canal does not have an impact on the selection of surgical approach. Posterior unroofing-type procedures in kyphotic cervical spines, however, are ineffective because anterior impingement on the spinal cord will remain; therefore, kyphosis of more than 10 degrees is considered a contraindication for posterior decompression. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 288
High Yield
The MRI scan shown in Figure 24 reveals a right-sided herniated nucleus pulposus at L4-5 in a patient with pain in the right leg. Administration of a caudal epidural steroid injection provides immediate relief. Over the next week he notes generalized weakness of the lower extremities and has one episode of urinary incontinence. What is the next most appropriate step in management?

Explanation
Whenever a patient's condition changes following a test or a procedure, the physician must determine the cause. A steroid flare reaction will not cause incontinence or weakness of the lower extremities. An L4-5 diskectomy may alleviate the problem if the right-sided L4-5 disk herniation is the etiology of the symptoms. However, it is unlikely that a right-sided disk herniation alone will cause a cauda equina syndrome. Possible etiologies include a further extrusion of a disk fragment at L4-5 that now obliterates the spinal canal, a disk herniation at another level, or an epidural abscess following injection of corticosteroids through a caudal approach. In the presence of a possible infection, myelography should not be performed from a lumbar puncture. The fastest and least invasive way to make an appropriate diagnosis is to obtain an MRI of the lumbar spine. In this patient, the MRI revealed an epidural abscess that was compressing the cauda equina. Because of the large dose of steroids that were injected, the patient did not manifest symptoms such as fevers and chills until late in the course. Knight JW, Cordingley JJ, Palazzo MG: Epidural abscess following epidural steroid and local anaesthetic injection. Anaesthesia 1997;52:576-578.
Question 289
High Yield
Compared to metal-on-polyethylene total hip bearing surfaces, the debris particles generated by metal-on-metal articulations are

Explanation
Retrieval studies have shown that the debris particles produced by metal-on-metal articulations in total hip arthroplasty are several orders of magnitude smaller and may be up to 100 times more numerous than those found with metal-on-polyethylene articulations. Davies AP, Willert HG, Campbell PA, et al: An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements. J Bone Joint Surg Am 2005;87:18-27.
Question 290
High Yield
A professional pitcher reports pain localized to the medial aspect of his throwing elbow. History reveals that he was pitching in a playoff game and heard and felt a pop in his elbow. MRI reveals a complete ulnar-sided avulsion of the medial collateral ligament (MCL). Examination reveals valgus instability and ulnar nerve involvement. What recommendations should be made based on the patient's desire to return to sport?
Explanation
Injuries to the MCL usually result from repetitive high valgus stress on the medial aspect of the elbow joint due to overhead throwing or racquet sports. Excessive stresses during the late cocking and acceleration phase of throwing can injure the anterior band of the MCL. Clinically, the injuries may present as chronic or acute, and a pop may be noted in the latter. Associated ulnar nerve involvement is common. Valgus instability is present in about 25% of patients. Patients typically are athletes who participate in throwing and have localized medial elbow pain and tenderness along the course of a ligament that extends from the medial epicondyle of the distal humerus to the sublime tubercle of the ulna. Surgical reconstruction is the procedure of choice in an athlete desiring a return to a high level of throwing. Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy. Philadelphia, PA, WB Saunders, 1995, p 230. Arendt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, p 227.
Question 291
High Yield
A Canale view best visualizes which of the following structures?

Explanation
The Canale view, which visualizes the talar neck, is taken with the ankle in maximum plantar flexion and the foot pronated 15 degrees. The radiograph is directed at a 75 degree angle from the horizontal plane in the anteroposterior plane. The Broden view, which is different from the Canale view, is best for imaging the posterior facet of the subtalar joint. Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Question 292
High Yield
A 62-year-old woman with soft-tissue calcifications and telangiectasia has severe pain in the left index, middle, ring, and little fingers. History reveals that she does not smoke. The clinical history and arteriogram shown in Figure 6 are consistent with which of the following conditions?

Explanation
The arteriogram shows generalized disease of all vascular structures. Even though the image was obtained following an infusion of nitroglycerin, little flow is present to the fingers. Based on the history of soft-tissue calcifications and telangiectasia, the most likely diagnosis is CREST (chondrocalcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly and telangiectasias). The arteriogram reveals Raynaud's phenomenon or the "R" component of CREST. Buerger's disease, or thromboangiitis obliterans, is strongly associated with a history of smoking. Hypothenar hammer syndrome involves repetitive trauma to the ulnar artery at the wrist, resulting in well-defined filling defects in the superficial palmar arch of the hand. Although not well visualized in this patient, the superficial arch is narrowed, showing no evidence of aneurysmal dilation. Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
Question 293
High Yield
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery?

Explanation
The magnitude of the curve at the time of the peak height velocity is the most prognostic sign in relationship to surgery. More than 70% of curves that measure more than 30 degrees at this time are likely to reach surgical range. Little DG, Song KM, Katz D, et al: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Question 294
High Yield
A 25-year-old woman has had continuous pain after falling on her outstretched wrist 12 weeks ago. A current radiograph is shown in Figure 11. Management should consist of

Explanation
The patient has a scaphoid fracture with cystic resorption of the distal aspect of the midthird of the scaphoid. This fracture is unlikely to heal without intervention. Percutaneous pinning, closed manipulation, and bone grafting will not restore alignment. Treatment requires restoration of scaphoid length, bone grafting, and internal fixation to obtain healing with normal alignment. Cooney WP, Linscheid RL, Dobyns JH, Wood MB: Scaphoid nonunion: Role of anterior interpositional bone grafts. J Hand Surg Am 1988;13:635-650. Fernandez DL: A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 1984;9:733-737. Stark HH, Rickard TA, Zemel NP, Ashworth CR: Treatment of ununited fractures of the scaphoid by illiac bone grafts and Kirschner-wire fixation. J Bone Joint Surg Am 1988;70:982-991.
Question 295
High Yield
A cortisone injection in the subacromial space will most likely result in
Explanation
A cortisone injection in the subacromial space will most likely result in elevated blood glucose levels in patients with type I diabetes mellitus. Patients should be warned of this potential complication. Cortisone does not have an effect on instability or proprioception, and a single injection would not affect osteoporosis. Repetitive injections or injection into the tendon itself could accelerate rupture of the biceps tendon. Matsen FA III, Arntz CT: Subacromial impingement, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 623-646.
Question 296
High Yield
A 28-year-old man who sustained an ankle fracture in a motor vehicle accident underwent open reduction and internal fixation 3 months ago. He continues to report significant ankle pain with ambulation. Radiographs are shown in Figure 26. What is the next most appropriate step in management?

Explanation
The patient sustained a bimalleolar ankle fracture with a syndesmosis disruption. The initial open reduction and internal fixation did not successfully reduce the distal tibiofibular joint. The patient may need a derotational distraction osteotomy of the fibula to reduce the syndesmosis. The other procedures do not address the primary problem of the fibular malunion and syndesmosis malreduction. There is no radiographic evidence of significant arthritis; therefore, ankle arthrodesis is not indicated.
Question 297
High Yield
A 74-year-old man has had worsening left shoulder pain for the past 3 years. Extensive nonsurgical management has provided only minimal relief. Examination reveals limitations in motion due to pain but good rotator cuff strength. Radiographs are shown in Figures 53a and 53b. What surgical procedure is most appropriate?


Explanation
The patient has end-stage shoulder arthritis with posterior glenoid erosion and large humeral osteophyte formation. Since the rotator cuff is likely intact, the reverse total shoulder arthroplasty is unnecessary. All the remaining procedures may provide symptomatic relief in appropriate patients; however, for most patients, total shoulder arthroplasty has been associated with the most predictive pain relief and functional improvements. Bryant D, Litchfield R, Sandow M, et al: A comparison of pain, strength, range of motion, and functional outcomes after hemiarthroplasty and total shoulder arthroplasty in patients with osteoarthritis of the shoulder: A systemic review and meta-analysis. J Bone Joint Surg Am 2005;87:1947-1956. Edwards TB, Kadakia NR, Boulahia A, et al: A comparison of hemiarthroplasty and total shoulder arthroplasty in the treatment of primary glenohumeral osteoarthritis: Results of a multicenter study. J Shoulder Elbow Surg 2003;12:207-213.
Question 298
High Yield
An 18-year-old football player sustains a contact injury to his right lower leg, and radiographs show a closed transverse fracture of the middle third of the tibia. Based on the clinical examination, a compartment syndrome is suspected. When measuring compartment pressures, the highest tissue pressure is recorded how many centimeters proximal or distal to the fracture site?
Explanation
Measurements of compartment pressures in patients with tibial fractures and compartment syndrome reveal that the highest tissue pressures are recorded at the level of the fracture or within 5 cm of the fracture. Tissue pressures show a statistically significant decrease when they are recorded at increasing distances proximal and distal to the site of the highest pressure recorded. To reliably determine the location of the highest tissue pressure in patients with tibial fractures, measurements should be obtained, at a minimum, in both the anterior and deep posterior compartments at the level of the fracture, as well as at locations proximal and distal. The highest tissue pressure recorded should serve as a basis for determining the need for fasciotomy. Heckman MM, Whitesides TE Jr, Grewe SR, Rooks MD: Compartment pressure in association with closed tibial fractures: The relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am 1994;76:1285-1292.
Question 299
High Yield
Which of the following is considered the lowest level that a standard thoracolumbosacral orthosis (TLSO) can immobilize?

Explanation
Without more distal immobilization such as a thigh extension, the lower two lumbar segments generally show the same or even increased mobility with a TLSO. White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 475-509.
Question 300
High Yield
Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reveals a normal neurologic examination, and the patient reports no discomfort with the cast and crutches. Management should now include


Explanation
Stable fractures and minimally displaced fractures in children can and should be treated by closed methods. Because loss of reduction is common, alignment of tibia fractures must be monitored closely for the first 3 weeks after cast application. This is most easily handled in a cooperative patient by cast wedging. Some children require application of a second cast under general anesthesia 2 to 3 weeks after injury, particularly if the subsidence of swelling has caused the cast to loosen. Surgical indications include the presence of soft-tissue injuries, unstable fracture patterns, fractures associated with compartment syndrome, and the child with multiple injuries. Surgical options in children include percutaneous pins, external fixation, plates and screws, and intramedullary nails. Heinrich SD: Fractures of the shaft of the tibia and fibula, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1340-1346.
