HY 2026
00:00
Start Quiz
Question 101
High Yield
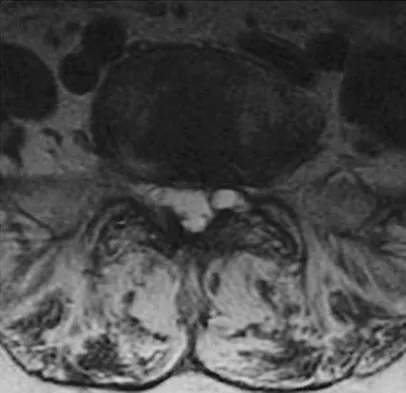
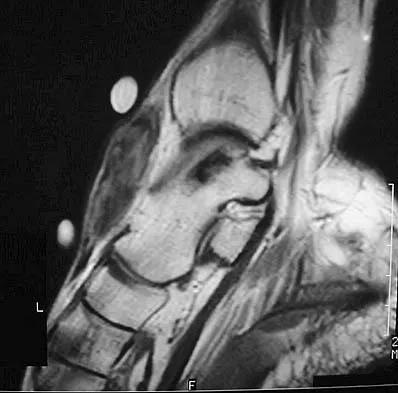
A 73-year-old woman reports a 4-month history of severe left-sided posterior buttock pain and left leg pain. The leg pain radiates into the left lateral thigh and posterior calf with cramping. Examination reveals mild difficulty with a single-leg toe raise on the left side and a diminished ankle reflex. There is also a significant straight leg raise test at 45 degrees which exacerbates symptoms. An MRI scan is shown in Figure 4. What is the most appropriate treatment at this time?
Explanation
Lumbar spinal stenosis with lumbar radiculopathy can be commonly caused by a synovial cyst arising from the facet joints. Lyons and associates reported on the surgical treatment of synovial cysts in 194 patients. Of the 147 with follow-up data, 91% reported good pain relief and 82% had improvement of their motor deficits. Epstein reported a 58% to 63% incidence of good/excellent results and a 38 to 42 point improvement on the SF-36 Physical Function Scale. It was also suggested that since the presence of a synovial cyst indicates facet pathology, possible fusion should be considered in these patients, especially those with underlying spondylolisthesis. Lyons MK, Atkinson JL, Wharen RE, et al: Surgical evaluation and management of lumbar synovial cysts: The Mayo Clinic Experience. J Neurosurg 2000;93:53-57. Khan AM, Synnot K, Cammisa FP, et al: Lumbar synovial cysts of the spine: An evaluation of surgical outcome. J Spinal Disord Tech 2005;18:127-131.
Question 102
High Yield
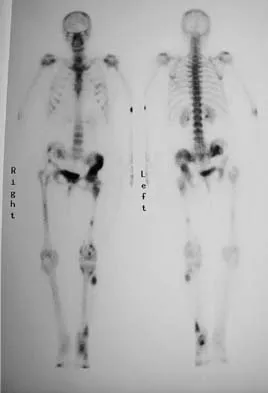
A 6-month-old child is seen in the emergency department with a spiral fracture of the tibia. The parents are vague about the etiology of the injury. There is no family history of a bone disease. In addition to casting of the fracture, initial management should include
Explanation
Unwitnessed spiral fractures should raise the possibility of child abuse, especially prior to walking age. With nonaccidental trauma being considered in the differential diagnosis, a skeletal survey is indicated to determine if there are other fractures in various stages of healing. Kempe CH, Silverman FN, Steele BF, et al: The battered-child syndrome. JAMA 1962;181:17-24.
Question 103
High Yield
Figures 4a and 4b show the radiographs of a 53-year-old woman who was injured in a fall. After initial closed reduction, what is the preferred treatment for this fracture?


Explanation
This elbow fracture-dislocation involves a radial head fracture, coronoid fracture, and ulnohumeral dislocation (terrible triad). Several algorithms exist for treatment; surgical treatment is indicated. The treatment should address the radial head. Studies have shown replacement to be superior to repair in comminuted fractures. The coronoid may be addressed in unstable cases at the time of radial head excision and replacement. Lateral ligamentous repair is carried out during closure of the lateral elbow capsule. Medial ligamentous repair also may be undertaken but usually in concert with bony repair. Hinged external fixation remains an option when instability exists following bony and soft-tissue repair. Acute ulnar nerve transposition is rarely indicated. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 104
High Yield
A 36-year-old woman has neck pain in the upper cervical region and occipital discomfort after being involved in a motor vehicle accident. Examination reveals no forehead or scalp lacerations. The neurologic examination is normal. A CT scan shows no evidence of bony injury. Figures 39a and 39b show a lateral radiograph and an MRI scan. Management should consist of


Explanation
The lateral radiograph shows 8 mm of atlantoaxial translation. In the absence of a bony injury, this represents rupture of the transverse atlantal ligament. The MRI scan reveals soft-tissue swelling posterior to the odontoid and a high intensity zone in the atlanto-dens interval consistent with acute injury. These injuries require arthrodesis because nonsurgical measures will not provide stability. Techniques for C1-2 fusion include Gallie, Brooks, or triple wiring. Transarticular screw fixation across the C1-2 articulation provides the most rigid means of fixation and the highest arthrodesis rates but is technically demanding. Anterior C2-3 arthrodesis will not address the level of instability. The normal atlanto-dens interval is 3 mm in an adult and 4 mm in a child. Kurz LT: Transverse atlantal ligament insufficiency, in Clark CR (ed): The Cervical Spine. Philadelphia, PA, Lippincott-Raven, 1998, pp 401-407.
Question 105
High Yield
A 17-year-old football player is injured during a play and reports abdominal pain that is soon followed by nausea and vomiting. What organ has most likely been injured?

Explanation
The spleen is the most common organ injured in the abdomen as the result of blunt trauma. It is also the most common cause of death because of an abdominal injury. The liver is the second most commonly injured organ. Injury to the other organs is rare. The diagnosis can be made with CT. Treatment ranges from observation to splenectomy, depending on the severity of injury. Green GA: Gastrointestinal disorders in the athlete. Clin Sports Med 1992;11:453-470.
Question 106
High Yield
A 28-year-old man sustained a shoulder dislocation 2 years ago. It remained dislocated for 3 weeks and required an open reduction. He now reports constant pain and has only 60 degrees of forward elevation and 10 degrees of external rotation. He desires to return to some sporting activities. An AP radiograph and intraoperative photograph (a view of the humeral head through a deltopectoral approach) are shown in Figures 31a and 31b. What is the best treatment option to decrease pain and improve function?

Explanation
The radiograph and intraoperative photograph show osteonecrosis with near complete head loss/collapse. A stemmed implant is more appropriate in this patient because there is very little bone to support a resurfacing implant. In a younger patient, a glenoid implant should be delayed as long as possible because of the eventual need for revision secondary to glenoid loosening and wear, especially in a young active male. The hemiarthroplasty may be converted to a total shoulder arthroplasty in the future. Levy O, Copeland SA: Cementless surface replacement arthroplasty of the shoulder: 5- to 10-year results with the Copeland mark-2 prosthesis. J Bone Joint Surg Br 2001;83:213-221.
Question 107
High Yield
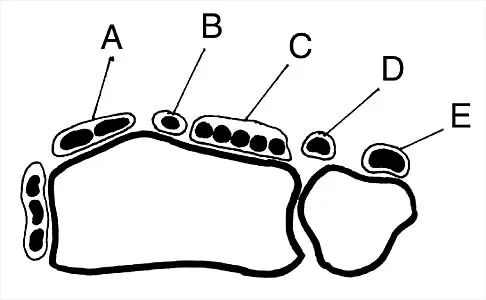
Figure 30 shows an axial cross section of extensor tendon anatomy in zone 7 of the wrist. What letter best depicts the location of the posterior interosseous nerve?
Explanation
The posterior interosseous nerve in contained in the floor of the fourth dorsal compartment of the wrist, which is labelled C in this diagram. Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 224.
Question 108
High Yield
When the great toe deviates into a valgus position, the action of the abductor hallucis muscle becomes one of
Explanation
The abductor hallucis muscle inserts together with the medial tendon of the flexor hallucis brevis into the medial base of the proximal phalanx of the great toe. When the hallux assumes a valgus position, the action of the abductor becomes one of flexion and pronation of the first metatarsal. Resch S: Functional anatomy and topography of the foot and ankle, in Myerson M (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, vol 1, pp 25-49.
Question 109
High Yield
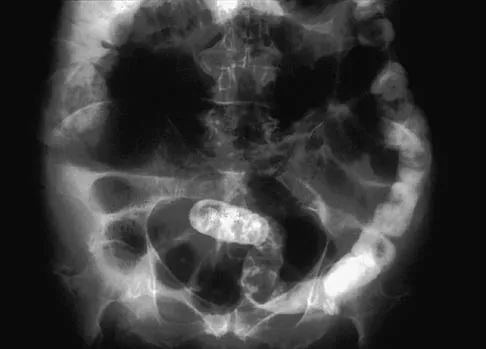
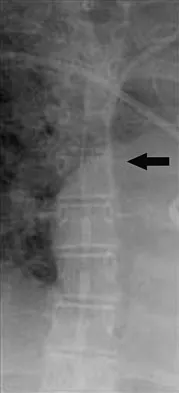
A 65-year-old woman has nausea, vomiting, and abdominal distention after undergoing total knee arthroplasty 48 hours ago. An abdominal radiograph is shown in Figure 14. Associated risk factors for this disorder include
Explanation
The prevalence of postoperative ileus associated with total joint arthroplasty has been reported to be as high as 3%. Metabolic abnormalities such as hypokalemia are believed to contribute to the onset of ileus and Ogilvie's syndrome (acute pseudo-obstruction of the colon). Prolonged bed rest also has been associated with the development of ileus and Ogilvie's syndrome. Untreated Ogilvie's syndrome can result in cecal perforation. Ileus usually is not accompanied by mechanical obstruction. Antibiotic administration and the type of anesthesia used have not been correlated with development of ileus. Administration of warfarin has been associated with elevated prothrombin time/partial thromboplastin time and international normalized ratio levels when ileus is managed with a nasogastric tube and suction. Metabolic imbalances must be corrected to reverse the ileus process. Iorio R, Healy WL, Appleby D: The association of excessive warfarin anticoagulation and postoperative ileus after total joint replacement surgery. J Arthroplasty 2000;15:220-223.
Question 110
High Yield
A 35-year-old carpenter sustained an injury to his dominant shoulder in a fall. He reports that he felt a sharp tearing sensation as he held on to a scaffold to keep from falling. Examination reveals swelling and ecchymosis down the upper arm, weakness to internal rotation, and deformity of the anterior axilla. He has good strength in external rotation and no apprehension with instability testing. Radiographs are normal. Management should consist of

Explanation
The findings are classic for a pectoralis major tendon avulsion. Deformity of the anterior axillary fold is a classic finding, and ecchymosis down the arm suggests that the injury is at the humeral attachment rather than at the musculotendinous junction. Good external rotation strength indicates that function in the supraspinatus and infraspinatus has been preserved. The treatment of choice for a tendon avulsion in a young individual is early surgical repair. Conversely, if the injury is within the muscle or at the musculotendinous junction, initial nonsurgical management is recommended. If the location of the injury cannot be determined by physical examination, then MRI of the pectoralis major can be helpful. Hanna CM, Glenny AB, Stanley SN, et al: Pectoralis major tears: Comparison of surgical and conservative treatment. Br J Sports Med 2001;35:202-206.
Question 111
High Yield
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?

Explanation
Pollak and associates found that the average SF-36 score for patients who sustained a pilon fracture was significantly lower than patients with diabetes mellitus, AIDS, hypertension, asthma, migraines, pelvic fracture, polytrauma, and AMI. Moreover, patients having undergone pilon fixation scored lower on all but three of the SF-36 scales (vitality, mental health, and emotional health).
Question 112
High Yield
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
Multidirectional instability of the shoulder is defined as symptomatic instability in two or more directions (anterior, posterior) but must include a component of inferior instability. Initial treatment should always include physical therapy and instruction in a home exercise program that emphasizes periscapular and rotator cuff strengthening to improve the dynamic stability of the glenohumeral joint. Immobilization has not been shown to be effective. Open capsular shift and arthroscopic capsular plication remain the surgical options when appropriate nonsurgical management fails (typically a minimum of 6 months of dedicated therapy and home program). Thermal capsulorrhaphy remains controversial but is not recommended by many clinicians because of reported complications including recurrent instability, axillary nerve injury, chondrolysis, and capsular injury. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908. D'Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up. Am J Sports Med 2004;32:21-33. Levine WN, Clark AM Jr, D'Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Question 113
High Yield
A 10-year-boy has had thigh pain for the past several months. He denies any history of trauma. Examination reveals no soft-tissue mass, and mild tenderness. Figures 33a and 33b show the plain radiograph and MRI scan, and the biopsy specimens are shown in Figures 33c and 33d. What is the most likely diagnosis?


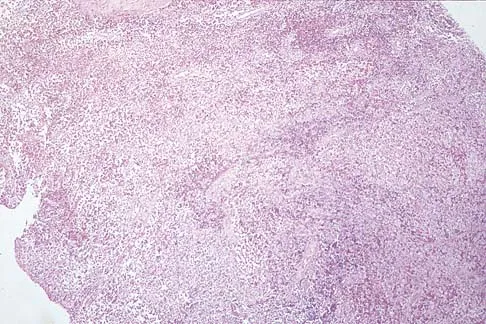
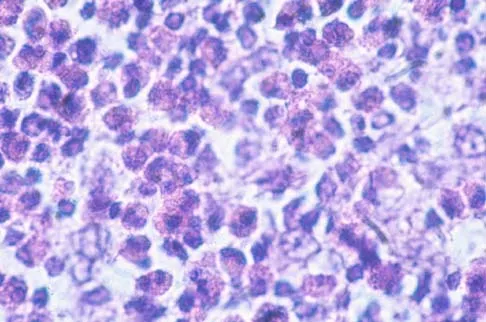
Explanation
The diagnosis is eosinophilic granuloma. The plain radiograph and MRI scan show a lesion in the midshaft of the femur. There is no soft-tissue mass. There is reactive bone about the lesion that suggests a less aggressive tumor. The histology reveals eosinophils in an otherwise bland cellular background with no evidence of mitotic figures or malignant cells to suggest sarcoma. The diagnostic elements are the amphophilic (ie, pale purple) histiocytes with cigar-shaped nuclei, some of which have linear longitudinal grooves. There is no histologic evidence of infection. Lymphoma of bone would be an unusual occurrence in this age group, and the histology is not consistent with that diagnosis.
Question 114
High Yield
What is the most appropriate treatment for a 50-year-old woman who sustains the injury shown in Figures 14a and 14b?


Explanation
This intra-articular distal humerus fracture with displacement at the joint surface is best treated with surgical fixation. The most biomechanically sound construct is two plates applied to either column 180 degrees from one another. Elbow arthroplasty is most appropriate for low demand elderly patients. Schemitsch EH, Tencer AF, Henley MB: Biomechanical evaluation of methods of internal fixation of the distal humerus. J Orthop Trauma 1994;8:468-475. McCarty LP, Ring D, Jupiter JB: Management of distal humerus fractures. Am J Orthop 2005;34:430-438.
Question 115
High Yield
A 22-year-old female collegiate javelin thrower has shoulder pain. She notes that her pain is primarily located in the posterior aspect of her shoulder, is exacerbated with throwing, and she experiences maximal tenderness in the extreme cocking phase of the throwing cycle. On examination, she reports deep posterior shoulder pain when the arm is abducted 90 degrees and maximally externally rotated to 110 degrees. This reproduces her symptoms precisely. Shoulder radiographs are normal. What is the most likely diagnosis?
Explanation
The patient has internal impingement. Internal impingement is commonly seen in overhead throwing athletes. When positioned in the extreme cocking phase of the throwing cycle, the posterior glenoid impacts the articular surface of the infraspinatus and posterior fibers of the supraspinatus tendon. This impact can cause partial-thickness rotator cuff tearing and posterosuperior labral lesions. She has no evidence of anterior shoulder instability, and her range of motion is excellent which rules out adhesive capsulitis. Subacromial impingement is identified with anterolateral shoulder pain with internal rotation in the abducted position. A full-thickness rotator cuff tear in a 22-year-old individual would require significant trauma and would likely result in pain at rest and with lifting. Meister K, Buckley B, Batts J: The posterior impingement sign: Diagnosis of rotator cuff and posterior labral tears secondary to internal impingement in overhand athletes. Am J Orthop 2004;33:412-415.
Question 116
High Yield
A 20-year-old soccer player who collapsed after a goal kick reports weakness and nausea. He appears slightly confused. Examination reveals that he is not sweating. His skin is warm and dry. The outdoor temperature is 80 degrees F (26.6 degrees C) with a relative humidity of 80%. Management should consist of
Explanation
There is a spectrum of heat-related conditions. Heat cramps are the mildest form of heat illness. In heat exhaustion, cramps are associated with headache and weakness, and the skin is pale and moist. Treatment of heat cramps or heat exhaustion consists of removing and loosening excess clothing, applying ice to the axilla and groin, ingestion of cool water, and cool water sprays. This patient demonstrates symptoms of heat stroke which is a medical emergency. The core body temperature may be as high as 106 to 110 degrees F (41.1 to 43.3 degrees C). In heat stroke, the patient may no longer be sweating, and the skin may be hot and red. The athlete is usually confused, weak, nauseated, and may have seizure activity. Central nervous system depression has been called the most important marker of heat stroke, and progresses from confusion and bizarre behavior to collapse, delirium, and coma. Bizarre behavior is often the first sign of heat stroke. The patient needs to be treated and moved to a medical facility rapidly. During transfer, IV fluids and cooling of the athlete should be initiated. The best treatment of heat-related illness appears to be prevention with adequate hydration and monitoring of conditions (temperature and humidity), with cancellation of competition when conditions do not comply with guidelines. Griffin LY: Emergency preparedness: Things to consider before the game starts. J Bone Joint Surg Am 2005;87:894-902. Barker TA, Motz HA, Gersoff WK: Environmental factors in athletic performance, in Fu FH, Stone DA (eds): Sports Injuries, ed 2. Philadelphia, PA, Lippincott, 2001, pp 67-68.
Question 117
High Yield
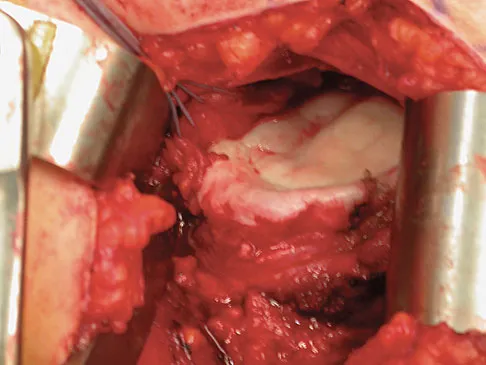
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
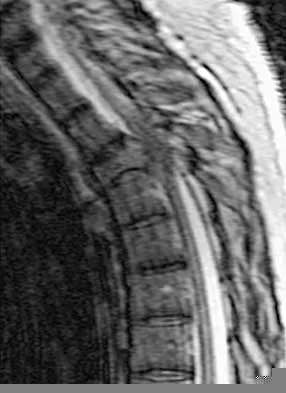
Explanation
Surgical decompression and stabilization have been shown to be the most effective means of improving neurologic function. Decompression is most reliably done from the side of the compression, which is anterior in this patient. Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Question 118
High Yield
An 83-year-old woman reports pain in her left middle finger after a minor injury. Laboratory studies show a WBC count of 7,000/mm3, an erythrocyte sedimentation rate of 3 mm/h, a uric acid of 10.4 mg/dL, and a normal serum protein electrophoresis. Radiographs are shown in Figures 49a and 49b. A core biopsy specimen is shown is Figure 49c. In addition to treatment of the finger fracture, treatment should include


Explanation
This clinical picture is most consistent with periarticular erosions from gout. The patient has multiple periarticular lytic lesions in the hand. The laboratory studies show an elevated serum uric acid level, and the biopsy specimen demonstrates acute and chronic inflammation with prominent clefts. Therefore, the preferred treatment is systemic control of her gout. Radiation therapy, chemotherapy, and/or amputation should be considered for a malignancy; however, the pathology does not demonstrate any evidence of pleomorphism, high nuclear-to-cytoplasmic ratio, nuclear atypia, or mitotic activity. Antibiotics for an infectious process is a consideration, but the minimal elevation in the WBC count and erythrocyte sedimentation rate does not support an infectious process. Wise CM: Crystal-associated arthritis in the elderly. Clin Geriatr Med 2005;21:491-511.
Question 119
High Yield
What complication is most likely to develop after right total hip arthroplasty in the patient shown in Figure 5?

Explanation
The patient has hypertrophic arthritis, which is a strong risk factor for heterotopic bone formation. The remaining complications are possible but do not have the same significant risks. Goel A, Sharp DJ: Heterotopic bone formation after hip replacement: The influence of the type of osteoarthritis. J Bone Joint Surg Br 1991;73:255-257.
Question 120
High Yield
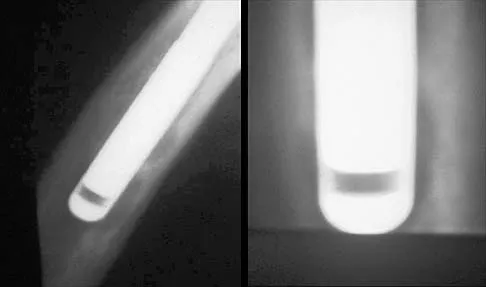
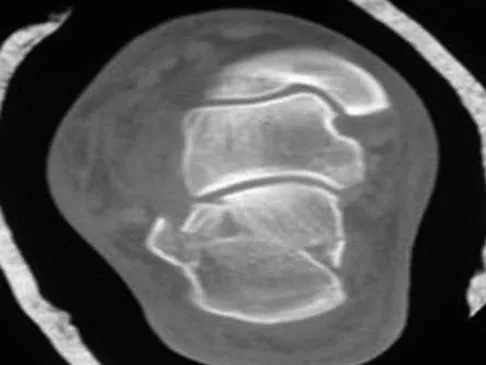
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of

Explanation
The CT scan shows a stress fracture of the olecranon. This injury is the result of repetitive abutment of the olecranon into the olecranon fossa, traction from triceps activity during the deceleration phase of the throwing motion, and impaction of the medial olecranon onto the olecranon fossa from valgus forces. Fractures may be either transverse or oblique in orientation. Initial treatment consists of rest and temporary splinting. Electrical bone stimulation may also be considered. Open fixation with a large compression screw is recommended when nonsurgical management has failed to provide relief. Ahmad CS, ElAttrache NS: Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med 2004;23:665-676.
Question 121
High Yield
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10 degrees. Initial management should consist of

Explanation
The patient has cavus feet with minimal clinical symptoms. At this stage, conservative management is preferred. The use of a molded orthosis will allow better support of the midfoot and provide cushioning of the forefoot. This will most likely result in long-term relief. In more advanced cases with forefoot callus formation, Achilles tendon lengthening or calcaneal osteotomy and Steindler stripping are effective in correcting the cavus deformity. In the presence of arthritic changes in the hindfoot, a triple arthrodesis with corrective bone resection may be necessary. Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
Question 122
High Yield
Figure 33 shows the AP and lateral radiographs of an obese 58-year-old man who underwent a cementless total hip arthroplasty 6 years ago. He reports no pain, and examination reveals a normal gait and painless hip range of motion. What is the most likely diagnosis?
Explanation
Osteolysis of an otherwise well-functioning total hip arthroplasty is a recognized complication, and its radiographic appearance is typical, as shown here. Distal osteolysis, such as that shown here, is more prevalent when there is noncircumferential sealing of the proximal femoral canal. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 175-180.
Question 123
High Yield
Figures 44a through 44c show the radiographs of an 18-year-old female soccer player who fell on her outstretched hand 1 day ago. She denies any history of wrist pain. Examination reveals tenderness at the anatomic snuffbox. Management should consist of



Explanation
The treatment of choice for proximal pole scaphoid fractures is open reduction and internal fixation with a differential pitch screw via a dorsal approach. Healing rates of 100% have been reported for these acute fractures. Casting results in slow healing, with recommendations including 16 weeks or more in a cast. Vascularized bone grafts are not indicated for acute fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg 1999;24:1206-1210.
Question 124
High Yield
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
Postoperative subscapularis detachment can be identified with a positive lift-off test that reveals weakness in internal rotation. This complication does not necessarily compromise the anterior capsule repair. The load-and-sift maneuver and articular contrast studies may be normal. Supraspinatus tests for impingement and weakness should be negative. Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 125
High Yield
Figures 46a through 46e show the radiographs of a 22-year-old man who injured his wrist in a motorcycle accident. He has no other injuries. What is the best course of action?





Explanation
The patient has a fracture-dislocation of the radiocarpal joint. Attached to the large radial styloid fragment are the extrinsic wrist ligaments to the carpus. This injury should be treated with open reduction and internal fixation of the styloid fracture. Radiolunate fusion or extrinsic ligament repair is suggested when the extrinsic ligaments are ruptured, resulting in ulnar translocation of the carpus. Dumontier C, Meyer ZU, Reckendorf G, et al: Radiocarpal dislocations: Classification and proposal for treatment: A review of twenty-seven cases. J Bone Joint Surg Am 2001;83:212.
Question 126
High Yield
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
Explanation
An infection of the shoulder is considered a surgical emergency unless there are medical reasons that a patient cannot be taken to the operating room. If cultures of wound drainage are in question, then an aspiration should be done emergently, not several days later. The hallmark of infection in any major joint is increasing pain out of proportion to what is expected. Drainage occurring 1 to 2 days after an arthroscopic procedure is not normal, and it should be aggressively treated. Delay in diagnosis can result in sepsis and on a delayed basis, postinfectious arthritis. Both the glenohumeral joint and the subacromial space require debridement and irrigation, followed by antibiotics after both areas are cultured. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213. Settecerri JJ, Pitner MA, Rock MG, Hanssen AD, Cofield RH: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5. Ward WG, Eckardt JJ: Subacromial/subdeltoid bursa abscesses: An overlooked diagnosis. Clin Orthop 1993;288:189-194.
Question 127
High Yield
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
Failure of the scalene block, necessitating general anesthesia or the immediate administration of narcotic medications, is the most common complication, occurring in 3% to 18% of patients. Cardiac arrest or cardiovascular collapse has been reported in anecdotal occurrences. Seizure that is the result of intravascular injection of local anesthetic is a rare complication, with an incidence reported of 0% to 6%. Neurologic complications, including laryngeal and phrenic nerve injuries, are rare although parathesias lasting up to 2 weeks have been reported in up to 3% of patients. Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Question 128
High Yield
Figure 9 shows a cross-sectional view of the spinal cord at the lower cervical level. Injury to the structure indicated by the black arrow will lead to what neurologic deficit?
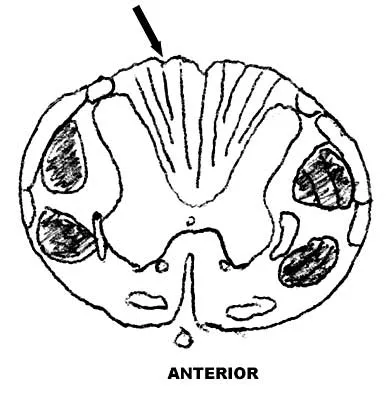
Explanation
The arrow is pointing to the posterior columns of the spinal cord that transmit position sense, vibratory sense, and proprioception. There are no motor tracts in the posterior columns. Bohlman H, Ducker T, Levine A: Spine trauma in adults, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 911.
Question 129
High Yield
Ewing's sarcoma of bone most commonly occurs in which of the following locations?
Explanation
Ewing's sarcoma typically occurs in the major long tubular bones, with the femur the most common location. The flat bones of the pelvis are the second most common location. Ewing's sarcoma occurs in the fibula but with a lower incidence than that seen in the major tubular bones. Ewing's sarcoma infrequently occurs in the metacarpals or the vertebral bodies. Simon M, Springfield D, et al: Ewing's Sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 287.
Question 130
High Yield
A 75-year-old patient returns for follow-up after undergoing bilateral total hip arthroplasty (THA). The right hip is a hybrid THA performed 12 years ago, whereas the left hip is a cementless THA performed 10 years ago. Both acetabular components are the same type, same size, and from the same manufacturer. Both femoral heads are 28-mm cobalt-chromium components. What is the most likely explanation for the advanced polyethylene wear in one hip?
Explanation
Over the past three decades, gamma irradiation and air has been the most common method of sterilizing polyethylene used in total joint arthroplasty. This method of sterilization results in breakage of the chemical bonds within the polymer. While this promotes cross-linking, it also leaves the polyethylene vulnerable to oxidation, especially if packaged in an air environment. Oxidation has been shown to decrease polyethylene's molecular weight, ultimate tensile strength, elongation, and toughness which results in a stiffer, more brittle material that is less resistant to wear. Severity of oxidation and a decrease in mechanical properties have been shown to be related to the length of time that the component is exposed to air (the shelf life). Currier and associates studied the clinical performance of gamma irradiated in air polyethylene components that had been shelf aged. They demonstrated that for the first 5 years of shelf life, polyethylene oxidized rather slowly. However, polyethylene components with a shelf life of more than 5 years would be expected to have minimal mechanical toughness and would likely fail rapidly if implanted. Bohl and associates evaluated 135 patients who had undergone total knee arthroplasty. Survivorship at 5 years was 100% for components with a shelf life of less than 4 years, 89% for components with a shelf life of 4 to 8 years, and 79% for components with a shelf life of more than 8 years. Sychterz and associates reported no correlation between shelf life and true wear rates for components with a shelf life of less than 3 years. In summary, both in vivo and in vitro data suggest that shelf life in excess of 3 to 5 years has a direct effect on wear of polyethylene. Currier BH, Currier JH, Collier JP, et al: Shelf life and in vivo duration: Impacts on performance of tibial bearings. Clin Orthop 1997;342:111-122. Bohl JR, Bohl WR, Postak PD, et al: The Coventry Award: The effects of shelf life on clinical outcome for gamma sterilized polyethylene tibial components. Clin Orthop 1999;367:28-38.
Question 131
High Yield
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most likely reveal
Explanation
Follow-up examination at 6 months revealed no statistically significant differences in quadricep or hamstring strength when comparing surgical versus nonsurgical extremities isokinetically. Therefore, the selection of autogenous hamstring or patellar tendon for ACL reconstruction should not be based solely on the assumption of the graft tissue source altering the recovery of quadricep and/or hamstring strength. Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172 Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Question 132
High Yield
A 68-year-old man reports a 1-year history of debilitating neck pain without neurologic symptoms. History reveals a C5-6 anterior diskectomy and bone grafting 10 years ago that provided good relief of arm and neck pain. Radiographs show evidence of fibrous union at C5-6, spondylotic disk narrowing at C4-5 and C6-7, and a fixed 2-mm subluxation at C3-4. Examination reveals cervical stiffness and discomfort at the extremes of movement. His neurologic examination is normal. Treatment should now consist of
Explanation
Axial pain can be difficult to manage. Pain management is not always successful, and surgical approaches may provide disappointing results unless there is discrete pathology. Whereas planning of a surgical approach should consider prior approaches and preexisting laryngeal dysfunction, no compelling case for surgical intervention can be made for this patient. Therefore, management should consist of patient education, exercise, and nonnarcotic medication. Ahn NU, Ahn UM, Andersson GB, et al: Operative treatment of the patient with neck pain. Phys Med Rehabil Clin N Am 2003;14:675-692. Algers G, Pettersson K, Hildingsson C, et al: Surgery for chronic symptoms after whiplash injury: Follow-up of 20 cases. Acta Orthop Scand 1993;64:654-656.
Question 133
High Yield
A 21-year-old man sustains multiple gunshot wounds to his right upper extremity. He can not extend his digits or his thumb but can extend and radially deviate his wrist. An injury to the radial nerve or one of its branches has most likely occurred at which of the following locations?
Explanation
In this patient, the radial nerve is most likely injured at the level of the radial neck. The radial nerve emerges from the posterior cord of the brachial plexus and travels along the spiral groove of the humerus. At the level of the lateral humeral condyle, the radial nerve branches into the posterior interosseous nerve after giving off two cutaneous branches, the superficial radial and the posterior cutaneous. The posterior interosseous nerve travels through the supinator muscle and winds around the radial neck. At this level, the posterior interosseous nerve is vulnerable to injury, particularly following fracture or penetrating trauma. Netter F: The Ciba Collection of Medical Illustrations: The Musculoskeletal System, Part 1: Anatomy, Physiology and Metabolic Disorders. West Caldwell, NJ, Ciba-Geigy Corporation, 1987, vol 8, p 53.
Question 134
High Yield
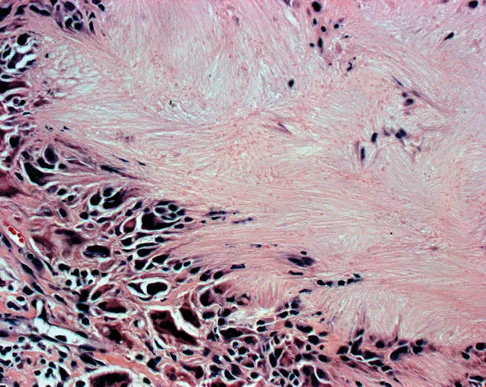
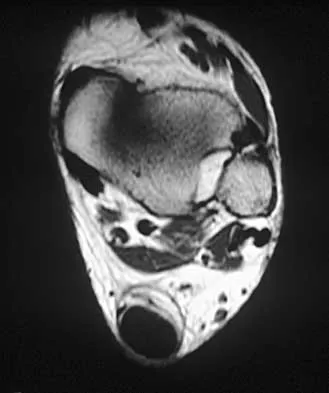
A 40-year-old man has a palpable mass over the dorsum of the ankle. He reports no history of direct trauma but notes that he sustained a laceration to the middle of his leg 6 weeks ago. Examination reveals a 4-cm x 1-cm mass. T1- and T2-weighted MRI scans are shown in Figures 12a and 12b. An intraoperative photograph and biopsy specimen are shown in Figures 12c and 12d. What is the most likely diagnosis?


Explanation
The findings are most consistent with a rupture of the anterior tibial tendon. The damaged area of tendon should be resected, followed by tendon reconstruction or tenodesis. The histology is not consistent with giant cell tumor of the tendon sheath, gout, or synovial sarcoma. Fibromatosis is characterized by a large number of spindle cells within the collagen background. Otte S, Klinger HM, Loreaz F, Haerer T: Operative treatment in case of closed rupture of the anterior tibial tendon. Arch Orthop Traum Surg 2002;122:188-190.
Question 135
High Yield
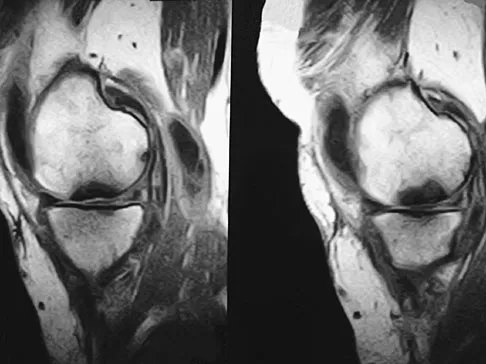
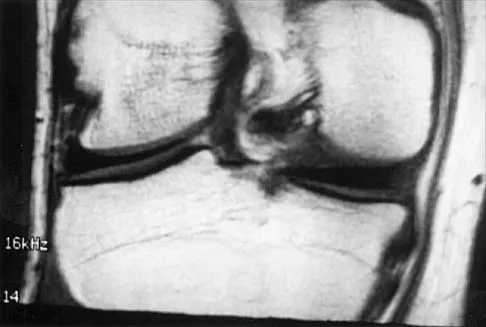
A 74-year-old woman has had acute medial right knee pain for the past 3 months. She denies any history of trauma or previous problems. Coronal and sagittal MRI scans are shown in Figures 11a and 11b. What is the most likely diagnosis?

Explanation
Spontaneous osteonecrosis of the medial femoral condyle is seen in the MRI scans, and is most common in women older than age 60 years. Although usually present in the weight-bearing portion of the medial femoral condyle, spontaneous osteonecrosis has also been described involving the lateral femoral condyle and patella. Most patients are seen postcollapse, and the treatment of choice is arthroplasty. Optimal treatment in precollapse stages is controversial. Kidwai AS, Hemphill SD, Griffiths HJ: Spontaneous osteonecrosis of the knee reclassified as insufficiency fracture. Orthopedics 2005;28:236,333-336. Soucacos PN, Xenakis TH, Beris AE, et al: Idiopathic osteonecrosis of the medial femoral condyle: Classification and treatment. Clin Orthop 1997;341:82-89.
Question 136
High Yield
What is the second most common primary bone malignancy in children?

Explanation
Ewing's sarcoma is the second most common bone tumor in children with an incidence of three per one million Caucasian children younger than 21 years of age. Ewing's sarcoma is rare in African Americans. Osteosarcoma is the most common bone tumor in children. Rhabdomyosarcoma is the most common soft-tissue sarcoma in children. Fibrosarcoma is a rare primary bone tumor most commonly seen in adults. Adamantinoma is a rare primary bone malignancy also most commonly seen in adults in the tibia. Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 195.
Question 137
High Yield
A 30-year-old patient has acetabular dysplasia and moderate secondary osteoarthrosis. Which of the following studies will best help predict the success of periacetabular osteotomy?
Explanation
Improvement in the appearance of the hip joint on functional radiographic evaluation (abduction/adduction views) has been shown to be predictive of outcome following joint preserving surgery. CT and MRI findings have not been shown to be predictive of outcome.
Question 138
High Yield
A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed to provide relief. Examination reveals tenderness in the lateral aspect of the proximal forearm and exacerbation of symptoms with resisted finger extension. Radiographs of the elbow reveal no abnormalities. Which of the following studies will aid in diagnosis?
Explanation
It is often difficult to accurately discern between lateral epicondylitis and radial tunnel syndrome. Neither MRI nor a bone scan is likely to reveal abnormalities. Electrodiagnostic studies are often inconclusive, and radial tunnel syndrome often presents without motor weakness. The symptoms of radial tunnel syndrome are expected to improve with an injection of lidocaine into the radial tunnel; therefore, this is the test of choice in this clinical scenario. Radiographs of the wrist will not assist in making the diagnosis. Eversmann WW Jr: Entrapment and compression neuropathies, in Green DP (ed): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingston, 1993, pp 1341-1385.
Question 139
High Yield
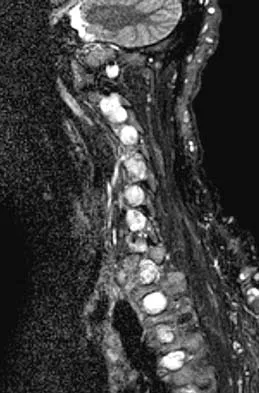
A 65-year-old man with ankylosing spondylitis sustains an extension injury to his cervical spine. Two days later, a progressive neurologic deficit develops at the C6 level. An MRI scan is shown in Figure 1. What is the most likely diagnosis?

Explanation
It is common for patients with ankylosing spondylitis to sustain extension-type fractures, typically near the cervicothoracic junction. These fractures can be minimally displaced, making them difficult to diagnose. In addition, the vertebral bodies are vascular and their canals are relatively enclosed, making them vulnerable to epidural bleeding. The MRI scan shows an epidural hematoma posteriorly compressing the cord. Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142. Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spine fracture and spinal stenosis in ankylosing spondylitis. J Neurosurg 1982;57:609-616.
Question 140
High Yield
What is the most common indication for revision following unconstrained elbow arthroplasty?

Explanation
Instability following unconstrained elbow arthroplasty occurs in 10% of patients. Subluxation is twice as common as frank dislocation; however, only 20% of these patients undergo revision. Instability following unconstrained elbow arthroplasty can be caused by component malposition or ligament insufficiency. King GJ, Itoi E, Niebur GL, et al: Motion and laxity of the capitellocondylar total elbow prosthesis. J Bone Joint Surg Am 1994;76:1000-1008.
Question 141
High Yield
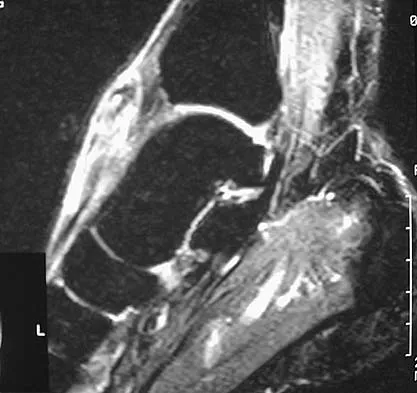
A 35-year-old woman who runs long distance has had posterior calf tenderness for the past 3 months. A clinical photograph is shown in Figure 10a, and MRI scans are shown in Figures 10b and 10c. Management at this point should consist of


Explanation
The initial treatment for peritendinitis should consist of calf stretching in an eccentric mode and physical therapy. In a recent study, this treatment has been found superior to surgical debridement in nonextensive peritendinitis and pantendinitis. A non-weight-bearing cast, while useful in reducing inflammation, will result in calf atrophy and poorly organized collagen repair. Cortisone is contraindicated because of the danger of tendon damage. Tendon debridement at this stage is not indicated. Alfredson H, Pietila T, Jansson P, Lorentzon R: Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med 1998;26:360-366.
Question 142
High Yield
Figure 1 shows the radiograph of a patient who underwent a total knee revision with a posterior stabilized mobile-bearing prosthesis and now has recurrent knee dislocations. What is the most likely cause?

Explanation
The patient has a posterior stabilized total knee revision, and the femoral component has dislocated over the tibial polyethylene cam/post. This usually indicates a loose flexion gap, or "flexion instability." A loose flexion gap can occur due to undersizing of the femoral component, anteriorization of the femoral component, excessive distal augmentation of the distal femur, or collateral ligament insufficiency, especially if combined with posterior capsular insufficiency. Isolated laxity of the extension gap (with a well-balanced flexion gap) causes varus/valgus instability, but it rarely causes the femoral component to "jump" the tibial cam of a posterior stabilized tibial insert. Malrotation of the components may cause patellar instability or a rotational instability of the tibiofemoral joint but should not cause a frank posterior dislocation of the tibia, unless combined with other errors of balancing. Although a mobile-bearing total knee arthroplasty may be more sensitive to errors in balancing than a fixed-bearing total knee arthroplasty, this complication does not reflect a faulty prosthetic design. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 173-186, 227-249.
Question 143
High Yield
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
Neurologic injury after shoulder replacement is relatively uncommon, occurring in 4% of shoulders in one large series. The importance of identifying and protecting the musculocutaneous and axillary nerves cannot be overemphasized; it is especially critical during revision arthroplasty when the normal anatomic relationships have been distorted. The long deltopectoral approach leaving the deltoid attached to the clavicle was found to be significant in the development of postoperative neurologic complications. A correlation was found between surgical time and postoperative neurologic complications, with long surgical times being associated with more neurologic complications. The presumed mechanism of injury is traction on the plexus that occurs during the surgery. A neurologic injury after total shoulder arthroplasty usually does not interfere with the long-term outcome of the arthroplasty itself; it is best managed by protective measures with passive range of motion of the involved extremity. Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 144
High Yield
A 22-year-old college baseball pitcher reports the recent onset of anterior and posterosuperior shoulder pain in his throwing shoulder. Examination shows a 15-degree loss of internal rotation, tenderness over the coracoid, and a positive relocation test. Radiographs are normal, and an MRI scan without contrast shows no definitive lesions. A rehabilitation program is prescribed. Which of the following regimens should be initially employed?
Explanation
Throwing athletes, particularly pitchers, have a high incidence of shoulder pain. Recent evidence suggests that posteroinferior capsular tightness and scapular dyskinesis may play a substantial role in the pathologic cascade, culminating in the development of articular surface rotator cuff tears and tearing of the posterosuperior labrum. These patients have posterosuperior shoulder pain primarily. Furthermore, these athletes are susceptible to a muscular fatigue syndrome, the SICK (Scapular malposition, Inferior medial border prominence, Coracoid pain and malposition, and dysKinesis of scapular movement) scapula syndrome. This patient has an internal rotation deficit and tenderness over the coracoid. The internal rotation deficit is addressed by stretching the posterior capsule. The tenderness over the coracoid has been attributed to a contracture of the pectoralis minor tendon secondary to scapular malposition. The initial phase of the rehabilitation regimen is directed at stretching the posterior capsule and pectoralis minor tendon. Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part III. Arthroscopy 2003;19:641-661.
Question 145
High Yield
A 9-year-old child sustains a proximal tibial physeal fracture with a hyperextension mechanism. What structure is at most risk for serious injury?
Explanation
The most serious injury associated with proximal tibial physeal fracture is vascular trauma. The popliteal artery is tethered by its major branches near the posterior surface of the proximal tibial epiphysis. During tibial physeal displacement, the popliteal artery is susceptible to injury. Injuries to the other structures are less common.
Question 146
High Yield
One of the serious potential complications of repair of distal biceps tendon ruptures is limited pronation and supination as a result of synostosis. What surgical approach and technique presents the highest risk for development of this complication?

Explanation
The risk of synostosis is imminent with any technique for repairing a distal biceps tendon rupture. However, the risk is quite low for all approaches that avoid exposure of the ulna, including the muscle-splitting two-incision technique.
Question 147
High Yield
The natural history of cervical spondylolytic myelopathy is best described as
Explanation
The natural history of cervical myelopathy has been described by Lees and Turner as exacerbations of symptoms followed by often long periods of static or deteriorating function (or very rarely improvement). This stepwise pattern of decreasing function has been corroborated by Clarke and Robinson. These authors described long periods of stable neurologic function, sometimes lasting for years, in about 75% of their patients. In the majority of the patients, however, the condition deteriorated between quiescent streaks. About 20% of their patients showed a slow, steady progression of symptoms and signs without a stable period, and 5% had rapid deterioration of neurologic function. Emery SF: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388. Lees F, Turner JA: The natural history and prognosis of cervical spondylosis. Brit Med J 1963;2:1607-1610.
Question 148
High Yield
The spring ligament of the foot connects what two bones?
Explanation
The spring ligament is also known as the calcaneonavicular ligament and connects the calcaneus to the navicular. This ligament supports the talar head and is an important anatomic supporting structure of the medial longitudinal arch of the foot. Choi K, Lee S, Otis JC, et al: Anatomical reconstruction of the spring ligament using peroneus longus tendon graft. Foot Ankle Int 2003;24:430-436.
Question 149
High Yield
Figure 15a shows the radiograph of a patient who has a chondrosarcoma of the acetabulum. Bone scans are shown in Figures 15b and 15c. Numerous soft subcutaneous masses are present. A clinical photograph of the hand is shown in Figure 15d. What is the most likely diagnosis?



Explanation
Chondrosarcomas associated with diffuse bone lesions (enchondromas) are characteristic of Ollier's disease. When accompanied by subcutaneous masses (hemangiomas), the condition is called Maffucci's syndrome. Multiple hereditary exostosis is characterized by diffuse osteochondromas. McCune-Albright syndrome is characterized by polyostotic fibrous dysplasia with cafe-au-lait spots and precocious puberty. Neurofibromatosis can have associated bone lesions but is not associated with chondrosarcomas. Sun TC, Swee TC: Chondrosarcoma in Maffucci's syndrome. J Bone Joint Surg Am 1985;67:1214-1219. Schwartz HS, Zimmerman NB, Simon MA, et al: The malignant potential of enchondromatosis. J Bone Joint Surg Am 1987;69:269-274.
Question 150
High Yield
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be

Explanation
Isolated palsy of the infraspinatus portion of the suprascapular nerve is common in volleyball players and is seen frequently in the throwing arm of baseball players. The exact cause is not known, but it may be the result of either tethering or traction on the nerve at the spinoglenoid notch. Synovial cysts in the spinoglenoid notch also can be a cause, but the patient's negative MRI findings rule out that entity. Because many isolated nerve palsies of the infraspinatus branch are asymptomatic, initial management should always be nonsurgical. Surprisingly, many athletes with this injury can participate fully in sports. Surgical treatment with decompression at the notch is unpredictable and generally is indicated only if nonsurgical management fails. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 151
High Yield
A 26-year-old man has recurrent right knee pain. Figures 9a and 9b show consecutive sagittal T2-weighted MRI scans, and Figure 9c shows a coronal T1-weighted MRI scan. What is the most likely diagnosis?


Explanation
A discoid meniscus is a large disk-like meniscus. It is seen in the lateral meniscus in 3% of the population; a discoid medial meniscus is much less common. It can be identified on the coronal view by noting meniscal tissue extending into the tibial spine at the intercondylar notch. The average width of a normal meniscus is less than 11 mm. A bow-tie appearance should not be seen on more than two consecutive sagittal images because the conventional thickness of the sagittal slices is 3 mm and the interval between two consecutive slices is 1.5 mm. Two sagittal slices will cover a 9-mm thickness. A discoid meniscus can be diagnosed on the sagittal views by noting a bow-tie appearance on more than two consecutive images. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 152
High Yield
Which of the following findings is a prerequisite for a high tibial valgus osteotomy for medial compartment gonarthrosis?

Explanation
The indications for high tibial valgus osteotomy include a physiologically young age, arthritis confined to the medial compartment, 10 to 15 degrees of varus alignment on weight-bearing radiographs, a preoperative arc of motion of at least 90 degrees, flexion contracture of less than 15 degrees, and a motivated, compliant patient. Contraindications include lateral compartment narrowing of the articular cartilage, lateral tibial subluxation of greater than 1 cm, medial compartment bone loss, ligamentous instability, and inflammatory arthritis. Naudie D, Bourne RB, Rorabeck CH, Bourne TT: The Insall Award: Survivorship of the high tibial valgus osteotomy. A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
Question 153
High Yield
Figure 30 shows the AP radiograph of a 9-month-old girl who has been referred for evaluation of unequal leg lengths. Examination reveals symmetrical abduction of the hips. When the hips are flexed 90 degrees, the right knee height is greater than the left knee. The girth of the right thigh and calf is larger than the contralateral side. There are no cutaneous lesions, and examination of the spine is normal. The infant is moving all extremities equally and spontaneously. Management should consist of

Explanation
Hemihypertrophy or hemihypotrophy is usually idiopathic, and either the leg or the entire side of the body may be involved. In the infant or young child, it is often difficult to determine which side is abnormal if the condition is mild. Because of the association of Wilms' tumor with hemihypertrophy, these patients should undergo a yearly renal ultrasound until at least age 5 years. Other conditions that may exhibit hemihypertrophy include Klippel-Trenaunay-Weber syndrome, Proteus syndrome, and neurofibromatosis. In this patient, the mild hemihypertrophy is idiopathic. Because of the normal spinal examination and absence of neurologic findings, an MRI scan is unnecessary. The absence of clinical and radiographic evidence of hip dysplasia makes both an ultrasound of the hips and application of a Pavlik harness unnecessary. Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont Ill, American Academy of Orthopaedic Surgeons, 1996, pp 185-193. Sponseller PD: Localized disorders of bone and soft tissue, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 305-344.
Question 154
High Yield
A 30-year-old man falls off a 7-foot ladder and sustains the injury seen in the radiograph and the CT scan shown in Figures 39a and 39b. Medical history is negative. Management of this injury should include which of the following?

Explanation
A Sanders type 2 intra-articular calcaneus fracture in a young healthy nonsmoker is best treated with open reduction and internal fixation. Whereas nonsurgical management is an option, Buckley and associates have shown that these fractures have a better outcome with surgical care. Percutaneous fixation is reserved for tongue-type fractures and subtalar arthrodesis is used in some type 4 fractures. External fixation has not been shown to be advantageous in closed fractures. Buckley R, Tough S, McCormack R, et al: Operative compared with nonoperative treatment of displaced intra-articular calcaneal fractures: A prospective, randomized, controlled multicenter trial. J Bone Joint Surg Am 2002;84:1733-1744. Sanders R: Displaced intraarticular fractures of the calcaneus. J Bone Joint Surg Am 2000;82:225-250.
Question 155
High Yield
Figures 34a and 34b show the axial and sagittal MRI scans of a 36-year-old man who reports the insidious onset of pain in the right shoulder. What is the most appropriate description of the acromial morphology?

Explanation
The MRI scans reveal a meso os acromiale with edema at the site in a skeletally mature patient. Sher JS: Anatomy, biomechanics, and pathophysiology of rotator cuff disease, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, p 23.
Question 156
High Yield
Figure 34 shows the standing AP radiograph of a 2-year-old girl who has a left bowleg deformity. Her mother states that she first noticed the problem when the child began walking at age 10 months, and the deformity has worsened over the past 6 months. Examination reveals a definite lateral thrust of the knee during the stance phase of gait. Management should consist of

Explanation
Infantile tibia vara is a developmental condition characterized by a varus angulation of the proximal end of the tibia that is caused by a growth disturbance of the proximal medial physis. In a study of 42 affected extremities in 24 children younger than age 3 years, it was found that daytime ambulatory brace treatment favorably altered the natural history of tibia vara. Another study of 27 patients with stage II Langenskiöld disease found a success rate of 70% (improved alignment without the need for osteotomy) using brace treatment. These authors also noted that children with unilateral disease were more likely to obtain correction of the deformity compared with those with bilateral disease. In this patient, observation is not warranted because untreated tibia vara has a significant risk for progressive worsening. Osteotomy is best reserved for those patients who, despite bracing, do not show satisfactory clinical and radiographic improvement by age 4 years. Elevation of the medial tibial plateau is a treatment option for older patients who have more advanced disease. An MRI scan would not provide any useful clinical information at this time. Zionts LE, Shean CJ: Brace treatment of early infantile tibia vara. J Pediatr Orthop 1998;18:102-109. Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount's disease. J Pediatr Orthop 1998;18:374-380.
Question 157
High Yield
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of

Explanation
The dislocation is between the medial and middle cuneiform. Although the first and second tarsometatarsal joints are aligned, there is a gap between the cuneiforms. The radiograph shows a Lisfranc dislocation variant. In a healthy active individual, open reduction and internal fixation yields the best results. The reestablishment of the normal arch and medial column support with anatomic reduction is critical to obtaining the best possible outcome from these injuries. Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int 2002;23:922-926.
Question 158
High Yield
A 7-year-old child is unresponsive, tachycardic, and has a systolic blood pressure of 50 mm Hg after being struck by a car. The patient is intubated and venous access is obtained. The secondary survey reveals an unstable pelvis. Despite adequate resuscitation, the patient continues to be hemodynamically unstable. What is the best course of action?
Explanation
The patient is hemodynamically unstable, so any treatment should be aimed at stabilization. Airway, breathing, and circulation are the most important areas to control initially; the patient has been intubated and has adequate venous access. Despite fluid resuscitation, the child remains hypotensive, indicating continued blood loss. With an unstable pelvic fracture there can be significant hemorrhage. Decreasing the pelvic volume can decrease blood loss related to the pelvic fracture. This can be done in the emergency department by applying a pelvic sling. Other means of decreasing pelvic volume include a pelvic clamp, a simple anterior frame pelvic external fixator, or a simple sheet tied around the pelvis. These maneuvers may stabilize the patient so that further evaluation and treatment can be undertaken. All of the other choices will delay stabilization and should be postponed until the patient is stabilized. Torode I, Zieg D: Pelvic fractures in children. J Pediatr Orthop 1985;5:76-84. Eichelberger MR, Randolph JG: Pediatric trauma-initial resuscitation, in Moore EE, Eisman B, Van Way CE (eds): Critical Decisions in Trauma. St Louis, MO, CV Mosby, 1984, p 344.
Question 159
High Yield
An otherwise healthy 57-year-old woman has limited range of motion and moderate effusion after undergoing total knee arthroplasty 6 months ago. One of two cultures of joint aspirate reveals methicillin-resistant Staphylococcus epidermidis. Management should now consist of
Explanation
The rapidly increasing prevalence of infection from Staphylococcus epidermidis has made this the most frequently cultured organism. In most patients, the infection occurred intraoperatively, thereby resulting in a chronic infection if not detected within the first 6 weeks after surgery. Irrigation of the joint may be successful during this time in 60% of patients, but the most successful treatment is extirpation for 6 weeks, followed by delayed reimplantation. This approach may result in a salvage rate of as high as 90% in some patients. Drancourt M, Stein A, Argenson JN, et al: Oral rifampin plus ofloxacin for treatment of staphylococcus-infected orthopedic implants. Antimicrob Agents Chemother 1993;37:1214-1218. Duncan CP, Beauchamp C: A temporary antibiotic-loaded joint replacement system for the management of complex infections involving the hip. Orthop Clin North Am 1993;24:751-759.
Question 160
High Yield
Figure 37 reveals a periprosthetic fracture around a cemented femoral stem in an 81-year-old patient with Paget's disease and mild coagulopathy. What is the most appropriate reconstructive management on the femoral side?

Explanation
This is an example of a Vancouver B3 periprosthetic fracture that consists of a fracture around a loose femoral stem with poor proximal bone support. Therefore, open reduction and internal fixation is not an option. PFR is an excellent choice for elderly inactive patients with poor femoral bone stock. The surgery can be performed in an expeditious manner, which is very important in a patient with mild coagulopathy. Impaction allografting and APC are both options for younger patients who have bone stock that needs to be restored. The results of revision arthroplasty using proximally coated stems, especially under these circumstances, are poor. Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304. Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.
Question 161
High Yield
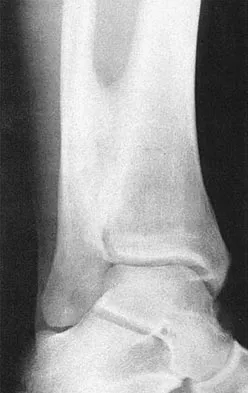
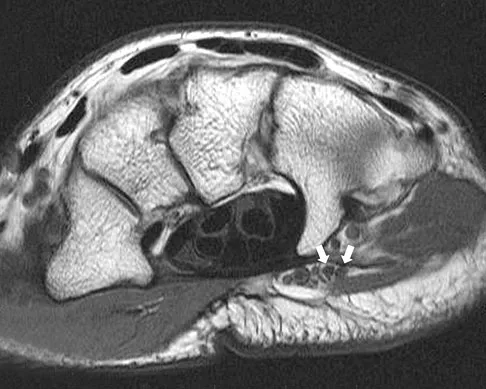
Figures 5a and 5b show axial and coronal MRI images of the left ankle of a patient with lateral ankle pain. What is the most likely diagnosis?

Explanation
The figures show a longitudinal split within the peroneus brevis tendon as it courses posterior to the fibula. The peroneus longus tendon has been driven between the medial and lateral components of the peroneus brevis tendon. Peroneal split syndrome is a cause of lateral ankle pain but may be less asymptomatic in the elderly. It may be associated with tendon subluxation following a tear of the superior peroneal retinaculum.
Question 162
High Yield
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 163
High Yield
A 56-year-old woman who underwent axillary node dissection 4 months ago now reports shoulder pain, weakness of forward elevation, and obvious winging of the scapula. What structure has been injured?
Explanation
The long thoracic nerve, which innervates the serratus anterior, is prone to injury because of its superficial location along the chest wall. The long thoracic nerve is derived from the roots of C5, C6, and C7. The spinal accessory nerve innervates the trapezius, and the thoracodorsal nerve innervates the latissimus dorsi. The posterior cord of the brachial plexus provides the axillary and the radial nerves. Hollinshead WH: Anatomy for Surgeons: The Back and Limbs, ed 3. Philadelphia, PA, Harper and Row, 1982, pp 259-340.
Question 164
High Yield
Which of the following is the preferred treatment for symptomatic localized pigmented villonodular synovitis (PVNS) of the knee?

Explanation
Localized PVNS is a variant of the disease process where the synovial proliferation occurs in one area and usually presents as a discrete mass. It has been effectively treated with complete excision. This may be performed arthroscopically or with arthrotomy. Complete synovectomy and radiation therapy are unnecessary to eradicate the localized form of PVNS. Tyler WK, Vidal AF, Williams RJ, et al: Pigmented villonodular synovitis. J Am Acad Orthop Surg 2006;14:376-385.
Question 165
High Yield
After humeral head replacement for four-part fractures, what is the most commonly reported difficulty?

Explanation
Results show that patients who underwent humeral head replacement for fracture almost routinely report pain relief, but functional reports vary. The most commonly reported difficulty is the use of weight in the overhead position with wide variation in active elevation. Factors found to affect active elevation include age, humeral offset, greater tuberosity positioning, and four-part (as compared with three-part) fractures. Goldman RT, Koval KJ, Cuomo F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and fourth-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4:81-86.
Question 166
High Yield
Clinical evidence suggests that grafts for replacing a torn anterior cruciate ligament often stretch after surgery. What is the most probable mechanism for this behavior?
Explanation
The stretching of the graft occurs over time as the graft is loaded. Time-dependent deformation under load is called creep and is common in viscoelastic materials such as ligament tissue. Creep can occur under both static and cyclic load conditions; time-dependent deformation will occur as long as load is applied to the tissue. Similarly, when a graft is initially tensioned to a given deformation at surgery, the load generated in the graft will decrease over time; this behavior is called stress relaxation and also is indicative of a viscoelastic material. Water content may affect the viscoelastic properties by changing the friction between collagen fibers, but studies have shown little difference in water content between grafts and normal ligaments. Fatigue failures may manifest themselves through damage to the ligament tissue, but this would require higher loads than are routinely experienced by grafts. Elastic stretch is recoverable and, therefore, does not contribute to a permanent stretch. Similarly, gross failure at the attachment would not cause a stretch, but rather a catastrophic instantaneous instability. Boorman RS, Thornton GM, Shrive NG, et al: Ligament grafts become more susceptible to creep within days after surgery. Acta Orthop Scand 2002;73:568-574. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 596-609.
Question 167
High Yield
Which of the following symptoms are most commonly associated with piriformis syndrome?
Explanation
Piriformis syndrome is best characterized by localized posterior hip pain and radicular symptoms in the sciatic distribution because of compression of the piriformis muscle on the sciatic nerve. Weakness in hip extension is not a characteristic finding, nor is pain with hip abduction or flexion. Hypesthesia of the lateral thigh would be more characteristic of a lesion of the lateral femoral cutaneous nerve. Radiating medial thigh pain would suggest hip joint pathology or upper lumbar nerve root irritation. Weakness in internal rotation is not a characteristic feature, and hypesthesia of the perineum would suggest possible involvement of the pudendal nerve. Byrd JWT: Thigh, hip, and pelvis, in Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy, ed 2. Philadelphia, PA, WB Saunders, 2002, pp 114-139.
Question 168
High Yield
A 52-year-old woman reports mild pain localized to the left sternoclavicular joint. History is notable for chronic renal failure requiring dialysis for the last 5 years. A clinical photograph, chest radiograph, and bone scan are shown in Figures 58a through 58c. What is the most likely diagnosis?


Explanation
Spontaneous swelling with the appearance of joint subluxation may be associated with an acute, subacute, or chronic bacterial infection of the sternoclavicular joint. Common causes of infection include bacteremia, rheumatoid arthritis, alcoholism, intravenous drug use, and chronic debilitating diseases. Subclavian vein catheterization and renal dialysis can predispose patients to sepsis and osteomyelitis of the sternoclavicular joint. Renoult B, Lataste A, Jonon B, et al: Sternoclavicular joint infection in hemodialysis patients. Nephron 1990;56:212-213.
Question 169
High Yield
Figure 10 shows the radiograph of a 7-year-old patient who has a bilateral Trendelenburg limp and limited range of hip motion but no pain. His work-up should include

Explanation
The radiograph shows bilateral flattening of the femoral heads with mottling and "fragmentation" suggestive of Legg-Calve-Perthes disease. However, when these changes occur bilaterally and are symmetric, multiple epiphyseal dysplasia or spondyloepiphyseal dysplasia should be suspected. Skeletal survey will show irregularity of the secondary ossification centers. With these conditions, there is no true osteonecrosis and no evidence that orthotic or surgical "containment" will alter the outcome of progressive degenerative arthritis. Cardiac anomalies and coagulopathies are not associated with the epiphyseal dysplasias. Crossan JF, Wynne-Davies R, Fulford GE: Bilateral failure of the capital femoral epiphysis: Bilateral Perthes disease, multiple epiphyseal dysplasia, pseudoachondroplasia, and spondyloepiphyseal dysplasia congenita and tarda. J Pediatr Orthop 1983;3:297-301.
Question 170
High Yield
What structure is located immediately posterior to the capsule at the posterior cruciate ligament tibial insertion?
Explanation
The popliteal artery lies just posterior to the posterior cruciate ligament tibial insertion, separated only by the posterior capsule of the knee. When performing a posterior cruciate ligament reconstruction, this artery is at risk for injury during creation of the tibial tunnel. Jackson DW, Proctor CS, Simon TM: Arthroscopic assisted PCL reconstruction: A technical note on potential neurovascular injury related to drill bit configuration. J Arthroscopy 1993;9:224-227.
Question 171
High Yield
Which is the best initial study for the diagnostic evaluation of diskogenic low back pain?

Explanation
Radiography is the best initial study for the evaluation of diskogenic low back pain. The normal degenerative process can be evaluated. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain should also be evaluated. The other tests may be beneficial but represent later imaging options.
Question 172
High Yield
A 24-year-old woman has a spleen laceration and hypotension. Radiographs reveal a pulmonary contusion and a displaced mid-diaphyseal fracture of the femur. The trauma surgeon clears her for stabilization of the femoral fracture. What technique will offer the least potential for initial complications?

Explanation
A concern in the multiply injured patient who has a pulmonary contusion is the potential for further pulmonary compromise because of embolization of marrow, blood clot, or fat during manipulation of the medullary canal. Recent evidence has shown that the presence of a lung injury is the most important determining factor in future deterioration. However, despite the lung injury and its potential consequences, this patient's femur fracture needs stabilization. Because damage control in the multiply injured patient requires a technique that can be performed rapidly and consistently, the treatment of choice is application of an external fixator. By placing two pins above and below the fracture and with longitudinal traction, the fracture is quickly realigned and stabilized. This allows the patient to be resuscitated and treated at a later date when definitive management of the fracture can be carried out. There is little difference between plate fixation and intramedullary nailing. Bosse MJ, MacKenzie EJ, Riemer BL, et al: Adult respiratory distress syndrome, pneumonia, and mortality following thoracic injury and a femoral fracture treated with either intramedullary nailing with reaming or with a plate: A comparative study. J Bone Joint Surg Am 1997;79:799-809. Scalea TM, Boswell SA, Scott JD, Mitchell KA, Kramer ME, Pollak AN: External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: Damage control orthopedics. J Trauma 2000;48:613-623.
Question 173
High Yield
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?

Explanation
The cervical spine may be involved in a child with polyarticular or systemic JRA; fusion or instability can occur. Radiographic assessment of the cervical spine should include lateral flexion-extension views. The potential exists for spinal cord injury during intubation or positioning in the presence of an unstable cervical spine. Limitations of the TMJ and micrognathia may affect ease of intubation and administration of anesthesia via a mask. If the TMJ and jaw are involved, some patients may have dental findings such as dental caries and even abscesses which can affect surgery. Some children, particularly those with systemic arthritis, may be taking corticosteroids long-term and may need stress dosing with complex surgeries. Although it is important to routinely check for uveitis and iritis in children with JRA, this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA. Cassity JT, Petty RE (eds): Textbook of Pediatric Rheumatology, ed 5. Philadelphia, PA, WB Saunders, 2005. Ilowite N: Current treatment of juvenile rheumatoid arthritis. Pediatrics 2002;109:109-115. Ruddy S, Harris ED, Sledge CB (eds): Kelley's Textbook of Rheumatology, ed 6. Philadelphia, PA, WB Saunders, 2001.
Question 174
High Yield
A 26-year-old woman who noted right-sided lumbosacral pain 10 days ago while vacuuming now reports that the pain has intensified. She denies any history of back problems. No radicular component is present, and her neurologic examination is normal. The next most appropriate step in management should consist of

Explanation
The initial management of a lumbar strain should consist of 2 to 3 days of bed rest when symptoms are severe, activity restrictions, and nonsteroidal anti-inflammatory drugs. It has been estimated that 60% to 80% of the adult population experiences back pain, with 2% to 5% affected yearly. Spontaneous improvement generally will occur within 4 weeks. Further study is indicated by the presence of radiculopathy, weakness, trauma, or suspicion of malignancy. Bigos S, Boyer O, Braen GR, et al: Acute low back pain in adults: Clinical practice guideline No. 14. AHCPR Publication No. 95-0642. Rockville, MD, Agency for Health Care Policy and Research, Public Health Service, US Department of Health and Human Services, December, 1994.
Question 175
High Yield
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of


Explanation
The patient has a displaced femoral neck fracture. Although the treatment remains controversial, most clinicians advocate either a closed or open reduction in younger active patients. Achieving an anatomic reduction is necessary to avoid loss of reduction, nonunion, or osteonecrosis. An acceptable reduction may have up to 15 degrees of valgus angulation and 10 degrees of posterior angulation. Parallel multiple screws or pins are the most common method of internal fixation. Prosthetic replacement is generally reserved for older and less active individuals. Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Question 176
High Yield
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist's office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?

Explanation
The privacy rules do not require an individual's written authorization for certain permitted or required uses and disclosures of the medical records. Patient or parental authorization is not required for disclosures for certain purposes related to treatment, payment, or health care operations. Specifically, HIPAA does not require a covered entity to obtain patient authorization for many of the health care industry's most fundamental activities such as providing care. Carroll R: Risk Management Handbook for Health Care Organizations, ed 4. Hoboken, NJ, Jossey-Bass, 2003, p 1142.
Question 177
High Yield
A 24-year-old woman fell from a horse and landed on her outstretched right arm. Radiographs reveal an elbow dislocation with a type II coronoid fracture and a nonreconstructable comminuted radial head fracture. What is the most appropriate management?

Explanation
The combination of an elbow dislocation and a fracture of the radial head and coronoid is known as a terrible triad injury. To restore elbow stability, each injury must be addressed. The nonreconstructable radial head fracture requires implant arthroplasty. Open reduction and internal fixation of the coronoid is also necessary as is repair of the lateral collateral ligament complex which is usually avulsed from the lateral epicondyle region. Ring D, Quintero J, Jupiter JB: Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg Am 2002;84:1811-1815. Ring D, Jupiter JB, Zilberfarb J: Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-551.
Question 178
High Yield
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
A knock-out mouse to the Vitamin D receptor would cause loss of vitamin D function, resulting in rickets. Renal failure would not occur; although Vitamin D is converted from 25 (OH) D to 1,25 (OH) D in the kidney, the active hormone acts on the gut and bone. Osteopetrosis can be seen as the phenotype for the c fos knock-out mouse; the Jansen-type metaphyseal dysplasia phenotype results from overactivation of the PTH/PTHrp receptor. Although compensatory hyperparathyroidism would occur, excessive PTH would not be able to rescue the skeletal loss and instead phosphoturia and phosphotasia would result. Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Question 179
High Yield
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?

Explanation
The history and findings are consistent with a diagnosis of a sprain of the medial collateral ligament (MCL) of the elbow; therefore, contrast-enhanced MRI is considered the most sensitive and specific study for accurately showing this injury. Arthroscopic visualization of the MCL is limited to the most anterior portion of the anterior bundle only; complete inspection of the MCL using the arthroscope is not possible. CT without the addition of contrast is of no value in this situation. Use of a technetium Tc 99m bone scan is limited to aiding in the diagnosis of occult fracture, a highly unlikely injury in this patient. There are no clinical indications for electromyography. Timmerman LA, Andrews JR: Undersurface tear of the ulnar collateral ligament in baseball players: A newly recognized lesion. Am J Sports Med 1994;22:33-36. Timmerman LA, Schwartz ML, Andrews JR: Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation of 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-32.
Question 180
High Yield
The force generated by a muscle is most highly dependent on its
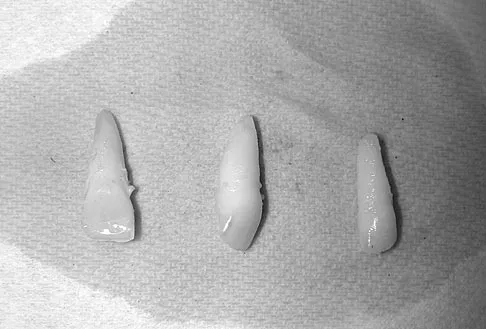
Explanation
The cross-sectional area of a muscle determines to a great extent the force generated by the muscle. The force of a muscle contraction is controlled by the amount of myofibrils that contract; the greater the amount of contracting myofibrils, the greater the force of contraction. Fiber types have less to do with the force of contraction and more to do with the duration and speed of contraction. Muscle length affects contraction force through the Blix curve. The morphology of a muscle can affect the cross-sectional area by varying the angle of the fibers in relation to the force vector. Conditioning mostly affects duration and fatigability. Buckwalter JA, Mow VC, Ratcliffe A: Restoration of injured or degenerated articular cartilage. J Am Acad Orthop Surg 1994;2:192-201.
Question 181
High Yield
An axial T1-weighted MRI scan of the pelvis is shown in Figure 13. The arrow is pointing to what muscle?
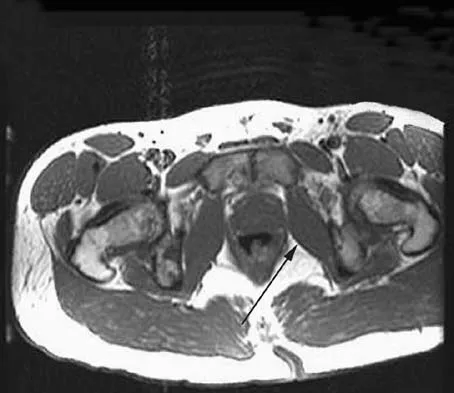
Explanation
The obturator internus muscle originates from the internal pelvic wall and passes laterally through the lesser sciatic foramen, banking around the ischium below the sacrospinous ligament before inserting on the medial aspect of the greater trochanter. Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, Ogose A (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Question 182
High Yield
A 5-year-old boy has had right hip pain and a limp for the past 3 months. Examination of the right hip reveals irritability and restricted abduction and internal rotation. AP and lateral radiographs of the hips are shown in Figures 31a and 31b. Initial management should consist of


Explanation
A favorable prognosis can be expected in up to 70% of children with Legg-Calve-Perthes disease who are younger than age 6 years. Containment treatment has not been shown to alter the outcome in this age group. The goals of treatment in this patient are to reduce pain (synovitis), restore motion, and improve function. Symptomatic treatment modalities include bed rest, traction, crutches, activity modification, and nonsteroidal anti-inflammatory drugs. Herring JA: The treatment of Legg-Calve-Perthes disease: A critical review of the literature. J Bone Joint Surg Am 1994;76:448-458.
Question 183
High Yield
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis?


Explanation
The patient has a traumatic rotator cuff tear. The history of the fall, the weakness on examination, and normal radiographic findings make a traumatic rotator cuff tear the most likely diagnosis. An MRI scan can be obtained to further evaluate the integrity of the rotator cuff. The axillary radiograph shows a reduced, nondislocated total shoulder arthroplasty. His radiographs show a well-seated humeral stem and no signs of loosening. The glenoid is a cemented all-polyethylene component with no evidence of radiolucent lines surrounding the cemented pegs. The polyethylene glenoid component is radiolucent; however, the space between the metallic humeral head and the glenoid bone is the thickness of the polyethylene glenoid component. If the humeral head were directly against the glenoid bone, then catastrophic fracture of the glenoid would be the working diagnosis. Hattrup SJ, Cofield RH, Cha SS: Rotator cuff repair after shoulder replacement. J Shoulder Elbow Surg 2006;15:78-83.
Question 184
High Yield
During excision of a Baker cyst, the base or stalk is usually found between the

Explanation
Although there are several bursae in the posterior portion of the knee, the most prevalent one with a connection to the knee joint is the one in the interval between the semimembranosus and the medial head of the gastrocnemius muscle. The popliteus muscle and posterior cruciate ligament, the posterior cruciate ligament and lateral gastrocnemius muscle, and the medial gastrocnemius muscle and posterior cruciate ligament are all too lateral and uncommon. The semitendinosus and medial head of the gastrocnemius muscles do not come in contact in the posterior aspect of the knee. Resnick D: Diagnosis of Bone and Joint Disorders, ed 3. Philadelphia, PA, WB Saunders, 1995, p 379.
Question 185
High Yield
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?

Explanation
The radiograph shows tuberosity malposition. The effect of improper prosthetic placement has also been associated with poor outcomes. However, the malposition of the tuberosity seen on the radiograph clearly explains loss of motion in this patient. It has been demonstrated that the functional results after hemiarthroplasty for three- and four-part proximal humeral fractures appear to be directly associated with tuberosity osteosynthesis. The most significant factor associated with poor and unsatisfactory postoperative functional results was malposition and/or migration of the tuberosities. Factors associated with a failure of tuberosity osteosynthesis in a recent study were poor initial position of the prosthesis, poor position of the greater tuberosity, and women older than age 75 years (most likely with osteopenic bone). Greater tuberosity displacement has been identified by Tanner and Cofield as being the most common complication after prosthetic arthroplasty for proximal humeral fractures. Furthermore, Bigliani and associates examined the causes of failure after prosthetic replacement for proximal humeral fractures and found that although almost all failed cases had multiple causes, the most common single identifiable reason was greater tuberosity displacement. Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748. Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.
Question 186
High Yield
A 43-year-old woman is referred after excisional biopsy of a cutaneous soft-tissue mass from her left shoulder. Based on the biopsy specimens shown in Figures 44a and 44b, what is the best course of action?
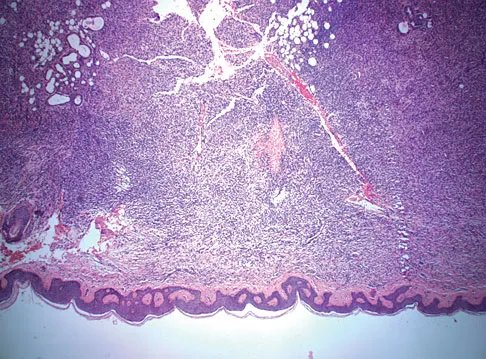
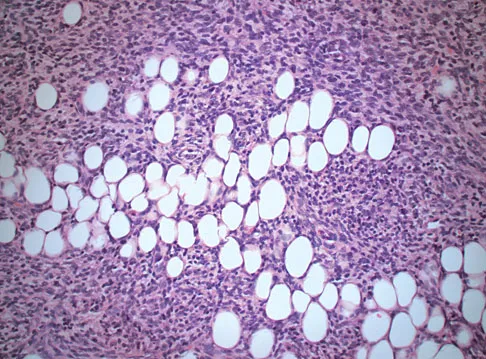
Explanation
Dermatofibrosarcoma protuberans (DFSP) is a rare superficial sarcoma that is frequently misdiagnosed at presentation. It is frequently excised prior to suspecting that the lesion is a sarcoma and if not appropriately treated with tumor bed resection to obtain wide margins, these lesions have a high incidence of local recurrence. It is recommended that the wide excision include the deep fascia and a 2.5- to 3-cm cuff of normal-appearing skin. Distant disease spread is rare and usually occurs in the face of a multiply recurrent lesion. Despite the apparent gross circumscription of these lesions, the tumor diffusely infiltrates the dermis and subcutaneous tissues. A characteristic histologic finding can be seen in the deep margins of the tumor where it intricately interdigitates with normal fat. Lindner NJ, Scarborough MT, Powell GJ, et al: Revision surgery in dermatofibrosarcoma protuberans of the trunk and extremities. Eur J Surg Oncol 1999;25:392-397.
Question 187
High Yield
A 6-year-old boy presents with a mass and a lucent lesion involving the tibial shaft as seen in Figure 17a. The mass is mildly tender to palpation. The bone scan is focally hot in the tibia. Biopsy specimens are shown in Figures 17b and 17c. What is the most likely diagnosis?

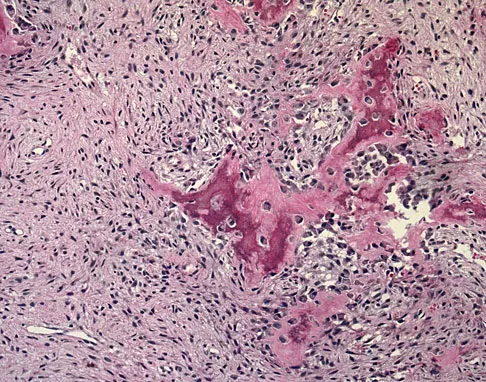
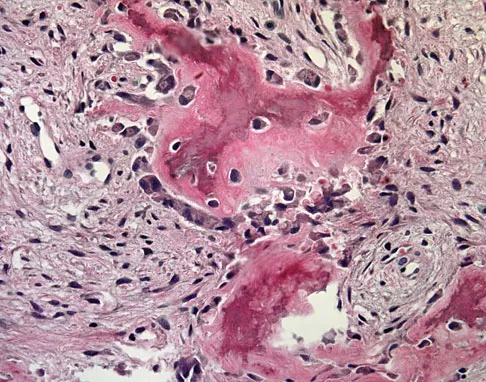
Explanation
Osteofibrous dysplasia frequently presents at a very young age, usually less than 10 years. In most patients, it involves the anterior cortex of the tibial shaft and minor anterior bowing of the tibia is frequently seen. The lesion is unpredictable in nature, but local recurrence is very high in patients who undergo surgery before 15 years of age. Campanacci M, Laus M: Osteofibrous dysplasia of the tibia and fibula. J Bone Joint Surg Am 1981;63:367-375.
Question 188
High Yield
At the time of the revision surgery shown in Figure 14, the acetabular component was found to be stable. Polyethylene exchange with a standard ultra-high molecular weight polyethylene liner and grafting was performed. The patient is at significantly increased risk for

Explanation
Maloney and associates reported a 35% increased risk of pelvic osteolysis after total hip arthroplasty with a porous-coated acetabular component without cement. All components were stable at the time of revision. Only liners were exchanged and debridement of the granuloma with or without bone graft was performed. No defects progressed and one third of the lesions were no longer visible on radiographs, regardless of bone grafting. Unfortunately, despite the technical ease of many of these types of revisions, the dislocation rate for these cases is significant. Precautions should be taken postoperatively, and patients should be educated about this risk preoperatively. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 411-424. Boucher HR, Lynch C, Young AM, et al: Dislocation after polyethylene liner exchange in total hip arthroplasty. J Arthroplasty 2003;18:654-657.
Question 189
High Yield
Which of the following factors is most commonly associated with mechanical failure of a cemented total hip arthroplasty?

Explanation
Varus position of the stem is most commonly associated with failure of the cemented femoral component because of association with an inadequate cement mantle in the proximal medial and distal lateral zones. An inadequate cement mantle and obesity have been associated with increased loosening but not as frequently as a varus deformity. The influences of gender and osteoporotic bone on the outcome of cemented femoral components have not been established. Maloney WJ III: Primary cemented total hip arthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 179-189.
Question 190
High Yield
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of

Explanation
In a retrospective review of 10 patients treated with hemivertebra excision for hemivertebra in the levels of T12 to L3, the procedure was found to be safe and effective. The procedure provided an average curve correction of 67 degrees and was greatest in patients who were younger than age 4 years at the time of surgery. Long anterior and posterior fusion with instrumentation is not the treatment of choice at this age. Either anterior hemiepiphyseodesis or posterior hemiarthrodesis in this isolated hemivertebra setting would be inadequate. Brace treatment is ineffective in management of the primary curvature.
Question 191
High Yield
A 44-year-old woman has bilateral knee pain, and history reveals bilateral hip replacements. Radiographs are seen in Figure 28a, and histopathologic specimens from the total hip replacement are shown in Figures 28b and 28c. Laboratory studies reveal anemia. What is the most likely diagnosis?
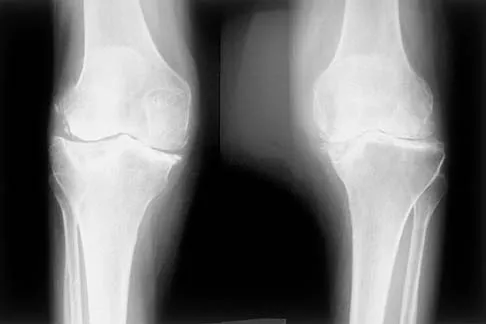
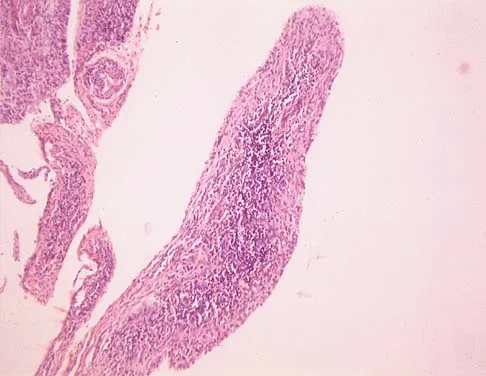
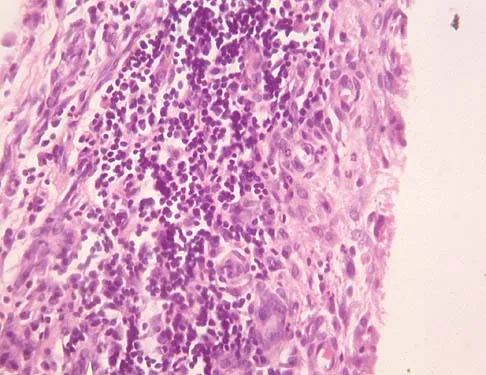
Explanation
Rheumatoid arthritis is an inflammatory arthritis that usually involves multiple joints. Radiologic findings of periarticular erosion, osteopenia, and minimal osteophyte formation favor rheumatoid arthritis over osteoarthritis. Pigmented villonodular synovitis and Charcot arthropathy are more often considered monoarticular diseases. There are no radiographic findings of Paget's disease.
Question 192
High Yield
A 12-year-old boy has severe left shoulder pain after being struck by an automobile. A chest radiograph, AP and lateral radiographs, and a CT scan with three-dimensional reconstruction of the scapula are shown in Figures 38a through 38d. Management should consist of
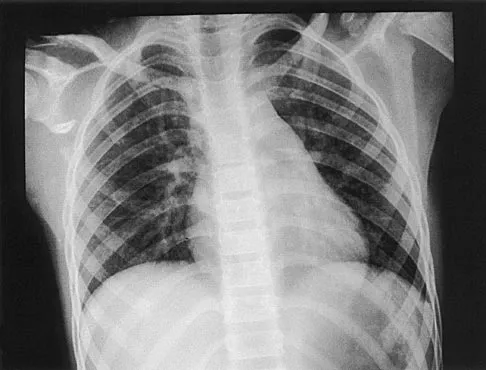


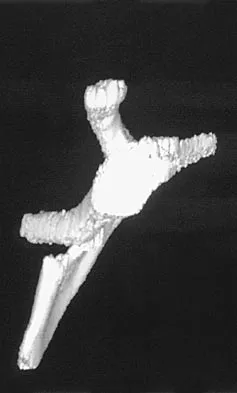
Explanation
Scapular body fractures in children are rare and are often associated with other injuries of the chest and thorax. Management is generally nonsurgical, unless the injury is open, and usually consists of support with a sling and gentle range-of-motion exercises to minimize shoulder stiffness. Green N, Swiontkowski M: Skeletal Trauma in Children, ed 2. Philadelphia, PA, WB Saunders, 1998, vol 3, pp 319-341.
Question 193
High Yield
A patient who underwent total knee arthroplasty now reports a loss of sensation in the area circled in Figure 38. This area is innervated by which of the following nerves?

Explanation
The saphenous nerve follows the saphenous vein, giving off the infrapatellar branch that crosses the knee anteriorly to supply the peripatellar skin. A longitudinal incision can interrupt the nerve, leaving the terminal distribution without sensation.
Question 194
High Yield
A 16-year-old cheerleader reports an ache in the right shoulder and arm that is worse after activity. She denies any history of acute trauma. Examination reveals a positive sulcus sign and an AP glide test with a posterior and anterior apprehension sign. To confirm a diagnosis of multidirectional instability, which of the following imaging studies is most appropriate?
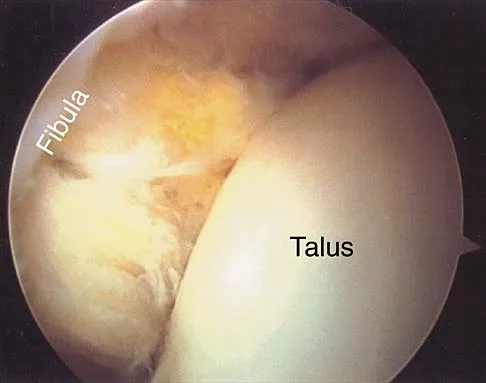
Explanation
Multidirectional instability is a common finding in young female athletes. The anatomic structures are all intact but are hypermobile; therefore, CT and bone scans and scapular Y-views are often normal. Obtaining a weighted or AP stress view while applying downward traction on the arm will document instability and hypermobility of the joint. MRI generally is not indicated in this condition. Ultrasound is used primarily for rotator cuff pathology. Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
Question 195
High Yield
Figures 3a and 3b show the inversion stress radiographs of a patient's ankle. What is the most likely ligament injury pattern?


Explanation
The radiographic findings show 30 degrees of talar tilt (severe) and 10 mm of anterior translation that typically involves laxity of both of the major lateral ligaments of the ankle (anterior talofibular and calcaneofibular). There is no evidence of deltoid laxity. Harper MC: Stress radiographs in the diagnosis of lateral instability of the ankle and hindfoot. Foot Ankle 1992;13:435-438.
Question 196
High Yield
The management of a complex multifragmentary diaphyseal fracture of either the tibia or femur has changed during the last decade. Which of the following principles of treatment is now considered less important?

Explanation
Although the original concept of internal fixation was one of anatomic reduction and stable fixation, over the past 10 to 15 years there has been a change based on the advent of intramedullary nailing and bridge plating. It is now appreciated that in a multifragmentary diaphyseal fracture, particularly of the lower extremity, the achievement of axis alignment (mechanical and anatomic axis) is all that is required. Healing will occur by callus. Relatively stable fixation is achieved through intramedullary nailing or bridge plating, providing adequate pain relief for functional aftercare. Perren SM, Claes L: Biology and mechanics of fracture management, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 7-32. deBoer P: Diaphyseal fractures: Principles, in Ruedi TP, Murphy WM (eds): AO Principles of Fracture Management. Stuttgart, Thieme, 2000, pp 93-104.
Question 197
High Yield
A 23-year-old professional baseball pitcher reports shoulder pain and decreased velocity while pitching. Physical examination reveals a side-to-side internal rotation deficit of 25 degrees. The O'Brien sign is negative; Neer and Hawkins signs are negative. Rotator cuff strength is full. Radiographs are unremarkable. What is the next step in management?

Explanation
Throwing athletes with symptomatic internal rotation deficits often benefit from an intensive posterior capsular stretching program. Patients that fail to respond to nonsurgical management may benefit from an arthroscopic posterior capsular release. Wilk KE, Meister K, Andrews JR: Current concepts in rehabilitation of the overhead throwing athlete. Am J Sports Med 2002;30:136-151.
Question 198
High Yield
Figures 1a and 1b show the sagittal T2- and T1-weighted MRI scans of a 25-year-old intravenous drug abuser who has low back pain that is increasing in intensity. Laboratory studies show a WBC count of 10,000/mm3 and an erythrocyte sedimentation rate of 80 mm/h. Blood culture is negative. Initial management consist of
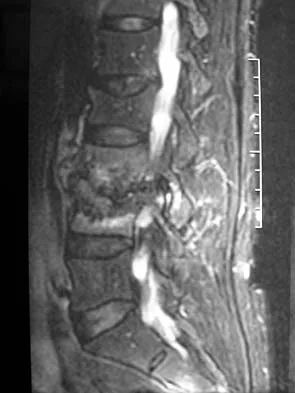

Explanation
The MRI scans show vertebral diskitis/osteomyelitis. The treatment of spinal infection in adults should be organism specific; therefore, initial management should consist of CT-guided closed biopsy prior to administration of antibiotic coverage. An open biopsy is indicated for a failed closed biopsy or failure of nonsurgical management. Although Staphylococcus aureus is the most common bacteria, a history of intravenous drug abuse raises suspicion for other organisms, including Pseudomonas. Tay BK, Deckey J, Hu SS: Spinal Infections. J Am Acad Orthop Surg 2002;10:188-197.
Question 199
High Yield
Figures 3a through 3c show the radiographs and bone scan of a patient who reports increasing pain associated with activity for the past several months. Laboratory studies show an erythrocyte sedimentation rate of 14 mm/h and a C-reactive protein level of 0.4. Aspiration is negative for infection. Management should consist of


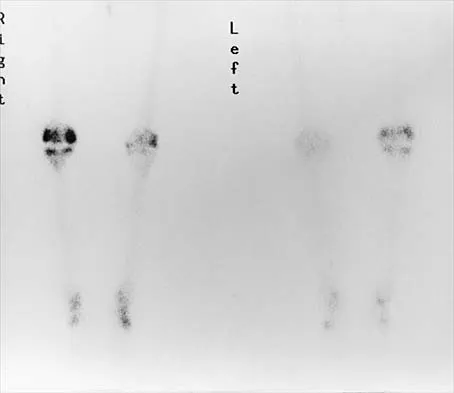
Explanation
The radiographs show polyethylene wear, but exchange of this will not necessarily provide pain relief. The presence of pain suggests the possibility of occult loosening, and the surgeon must be prepared for this option intraoperatively. There is little evidence of infection. Rand JA, Peterson LF, Bryan RS, Ilstrup DM: Revision total knee arthroplasty, in Anderson LD (ed): Instructional Course Lectures XXXV. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1986, pp 305-318.
Question 200
High Yield
Patients with patellar clunk syndrome are best managed by which of the following methods?

Explanation
Patellar clunk syndrome is usually the result of a fibrous nodule that forms on the undersurface of the distal quadriceps tendon. It may get entrapped in the intercondylar notch of the femoral component during flexion, and lead to a sudden snap as the nodule is pulled out of the notch during active extension. Nonsurgical management is rarely successful. Surgical debridement is usually curative, with only rare recurrence. More aggressive procedures such as realignment, revision, or patellectomy are usually not necessary, and are reserved for cases resistant to soft-tissue debridement. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 329. Diduch DR, Scuderi GR, Scott WN, et al: The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166-171.
