HY 2026
00:00
Start Quiz
Question 1
High Yield
A 15-year-old boy who participates in track reports acute pain along the left iliac crest during a sprint. Examination reveals that the anterior superior iliac spine is nontender. The most likely diagnosis is an injury to the

Explanation
The patient has iliac apophysitis. The radiographic findings are easily overlooked but usually reveal slight asymmetric widening of the iliac crest apophysis. The apophysis is the most vulnerable structure, as it is three to five times weaker than the tendon. This is not an epiphyseal site, and injury to the muscle or the tendinous insertion to bone (enthesis) is unlikely. Clancy WG Jr, Foltz AS: Iliac apophysitis and stress fractures in adolescent runners. Am J Sports Med 1976;4:214-218. Waters PM, Millis MB: Hip and pelvic injuries in the young athlete, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 279-293. Lombardo SJ, Retting AC, Kerlan RK: Radiographic abnormalities of the iliac apophysis in adolescent athletes. J Bone Joint Surg Am 1983;65:444-446.
Question 2
High Yield
In the posterior approach to the proximal radius (proximal Thompson approach), the supinator is exposed through the interval between what two muscles?
Explanation
The proximal exposure of the radius is most often used for internal fixation of fractures, resection of tumors, or decompression of the posterior interosseous nerve beneath the supinator muscle. The supinator muscle is exposed through the interval between the extensor carpi radialis brevis and the extensor digitorum comminus muscles. This interval can be more easily palpated further distal in the forearm. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 136-146.
Question 3
High Yield
A 25-year-old professional baseball pitcher reports a 4-month history of gradually increasing medial elbow pain that occurs during the late cocking and acceleration phases of throwing. The pain occasionally refers distally along the ulnar aspect of the forearm. He denies any weakness; however, he notes occasional paresthesias. A nerve conduction velocity study demonstrates increased latency across the cubital tunnel. Management consisting of 6 weeks of rest and rehabilitation fails to provide relief as the symptoms returned when he resumed throwing. What is the best course of action?
Explanation
In the thrower's elbow, ulnar neuritis is felt to result from both chronic compression and traction on the nerve that occurs during the throwing motion. Occasionally, subluxation of the nerve also can lead to symptoms. If nonsurgical management fails to provide relief, transposition of the nerve to an anterior subcutaneous location is the surgical procedure of choice. The nerve is held in its new position by one or two fascial slings created from the fascia of the common flexor origin. Schickendantz MS: Diagnosis and treatment of elbow disorders in the overhead athlete. Hand Clin 2002;18:65-75.
Question 4
High Yield
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
In the study done by Pevny and associates, 35% of patients older than age 40 years sustained rotator cuff tears and 8% had axillary nerve palsies. All of the patients with axillary nerve palsy also had rotator cuff tears. Imaging of the rotator cuff is indicated in this age group. The incidence of recurrent instability in patients older than age 40 years is 10% to 15%. Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294. Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Question 5
High Yield
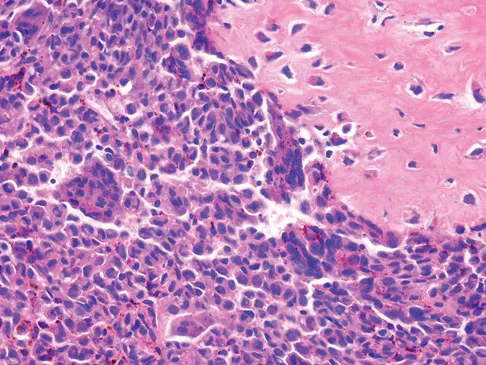
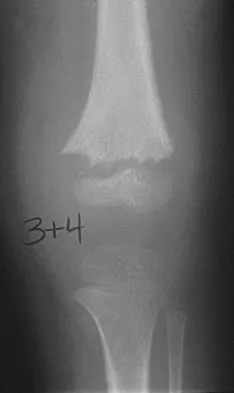
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?


Explanation
The epiphyseal location on the radiograph and MRI scan and the histologic findings of polyhedral cells separated by a chondroid matrix with pericellular, lattice-like "chicken wire" calcification all suggest chondroblastoma. Although giant cell tumors of bone typically occupy an epiphyseal location, they are rare in children and when present are often metaphyseal in skeletally immature patients. Enchondromas and osteoblastomas are generally metaphyseal and, along with giant cell tumors, have very different histology than seen here. Chondromyxoid fibromas are typically metaphyseal in location. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Question 6
High Yield
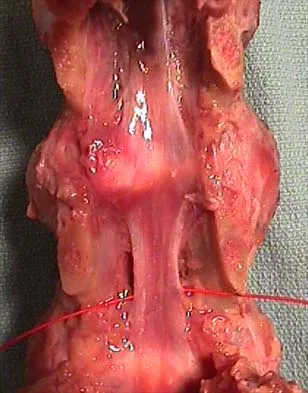
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of

Explanation
Brodsky and associates reviewed 34 cases of cervical pseudarthrosis after anterior fusion. Seventeen were treated with revision anterior fusion and 17 with posterior foraminotomy and fusion. Good results were seen in 75% of patients who underwent revision anterior surgery, but better results (94%) were seen with posterior surgery, including foraminotomy and stabilization. Tribus and associates reported treatment of 16 patients with pseudarthrosis using revision anterior debridement of the fibrous tissue and fusion with autograft and plates. There was improvement of the neck in 75% of the patients, nonunion in 19%, continued weakness in 28%, and dysphagia in 5%. Farey and associates reported on 19 patients treated with posterior foraminotomy, stabilization, and fusion with a fusion rate of 100%, resolution of arm pain in 94%, resolution of weakness in 100%, and resolution of neck pain in 75%. It would appear that posterior foraminotomy is more effective for relieving arm pain and neurologic deficits associated with pseudarthrosis. Posterior fusion has the most reliable rate of arthrodesis in this setting. Dysphagia is reported in some patients undergoing more extensive anterior dissections required for applying plates. A neck brace is unlikely to aid in healing of pseudarthrosis in a patient who underwent surgery 8 months ago. A neck brace would be most effective within the first 3 months if a delayed union is identified. Brodsky AE, Khalil MA, Sassard WR, Neuman BP: Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair. Spine 1992;17:1137-1143. Tribus CB, Corteen DP, Zdeblick TA: The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine. Spine 1999;24:860-864.
Question 7
High Yield
During the first 2 years of life, which of the following actions is most responsible for increasing structural stability of the physis?
Explanation
The zone of Ranvier provides the earliest increase in strength of the physis. During the first year of life, the zone spreads over the adjacent metaphysis to form a fibrous circumferential ring bridging from the epiphysis to the diaphysis. This ring increases the mechanical strength of the physis. The zone also helps the physis grow latitudinally. In turn, the increased width of the physis helps the physis further resist mechanical forces. The change in shape of the physis to its progressively more undulating form is also a factor in increasing physeal strength, but this occurs over a longer period of time, as the child's activity level increases. The undulations of the physis seen in some growth plates also add to stability but to a lesser extent. The other changes contribute little toward increasing physeal strength. Burkus J, Ogden J: Development of the distal femoral epiphysis: A microscopic morphological investigation of the zone of Ranvier. J Pediatr Orthop 1984;4:661-668.
Question 8
High Yield
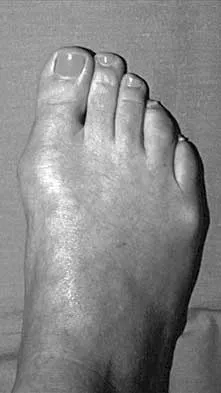
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?

Explanation
Based on her symptoms and prior shoe wear modifications, the treatment of choice is surgical correction of the hallux valgus with a chevron osteotomy. There are no data to support the use of a custom orthosis to delay the progression of a hallux valgus deformity. Steroid injection would only risk infection, as well as joint and capsule damage. Extra-depth shoes are an option; however, the patient is interested in surgical options. Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584. Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Question 9
High Yield
What normal tissue has a low signal intensity (appears black) on both T1- and T2-weighted images?
Explanation
Tendons, cortical bone, ligaments, menisci, and fibrous tissue will show low signal intensity (SI) on both T1- and T2-weighted images. Fat-containing tissues, such as subcutaneous fat and bone marrow, will show high SI on T1-weighted images and low SI on T2-weighted images. Tissues with high water content, such as joint fluid, intervertebral disk, and edema, will show low SI on T1-weighted images and high SI on T2-weighted images. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 65-70.
Question 10
High Yield
A 10-year-old boy with an L1 myelomeningocele has a low-grade fever and a swollen thigh that is warm to touch and erythematous. AP and lateral radiographs are shown in Figures 24a and 24b. Management should consist of

Explanation
Fractures of the long bones are common in patients with myelodysplasia, and the frequency of fracture increases with higher level defects. Fractures also occur following surgery and immobilization secondary to disuse osteoporosis. The response to the fracture (swelling, fever, warmth, erythema) is often confused with infection, osteomyelitis, or cellulitis. Management should consist of a short period of immobilization in a well-padded splint. Long-term casting results in further osteopenia and repeated fractures. Lock TR, Aronson DD: Fractures in patients who have myelomeningocele. J Bone Joint Surg Am 1989;71:1153-1157.
Question 11
High Yield
When performing a bunionectomy with a release of the lateral soft-tissue structures, the surgeon is cautioned against releasing the conjoined tendon that inserts along the lateral base of the proximal phalanx of the great toe. This conjoined tendon is made up of what two muscles?
Explanation
Owens and Thordardson cautioned surgeons not to release the conjoined tendon from the base of the proximal phalanx of the great toe because of an increased risk of iatrogenic hallux varus. Release of the transverse and oblique heads of the adductor hallucis is largely accomplished by releasing the soft tissue adjacent to the lateral sesamoid, without releasing tissue from the base of the proximal phalanx. The conjoined tendon is made up of the flexor hallucis brevis and the adductor hallucis. Owens S, Thordardson DB: The adductor hallucis revisited. Foot Ankle Int 2001;22:186-191.
Question 12
High Yield
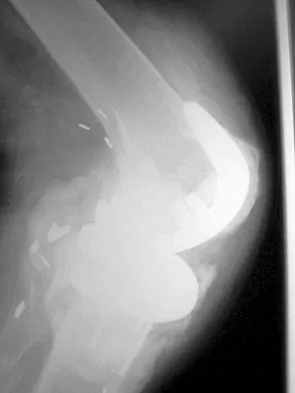
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with



Explanation
The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 13
High Yield
A full-term newborn has webbing at the knees, rigid clubfeet, a Buddha-like posture of the lower extremities, and no voluntary or involuntary muscle action at and below the knees. Radiographs of the spine and pelvis reveal an absence of the lumbar spine and sacrum. What maternal condition is associated with this diagnosis?
Explanation
The history, physical examination, and radiographic findings are consistent with type IV sacral agenesis or caudal regression syndrome. These children are born with no lumbar spine or sacrum. The T12 vertebra is often prominent posteriorly. Popliteal webbing and knee flexion contractures are common with this diagnosis. There is a higher incidence of this diagnosis when the mother has diabetes mellitus. Maternal drug abuse and alcoholism can produce phenotypically unique children but without the findings described here. Maternal idiopathic scoliosis is not associated with caudal regression syndrome. Chan BW, Chan KS, Koide T, et al: Maternal diabetes increases the risk of caudal regression caused by retinoic acid. Diabetes 2002;51:2811-2816.
Question 14
High Yield
Posterior lumbar spine arthrodesis may be associated with adjacent segment degeneration cephalad or caudad to the fusion segment. Which of the following is the predicted rate of symptomatic degeneration at an adjacent segment warranting either decompression and/or arthrodesis at mid-range follow-up (5-10 years) after lumbar fusion?
Explanation
The rate of symptomatic degeneration at an adjacent segment warranting either decompression or arthrodesis was predicted to be 16.5% at 5 years and 36.1% at 10 years based on a Kaplan-Meier analysis.
Question 15
High Yield
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?


Explanation
In an atrophic nonunion with a good soft-tissue envelope, adequate plating with cancellous bone graft can be used to span defects of up to 6 cm. Cortical graft from the fibula or iliac crest is not necessary. BMP-7 is a bone graft substitute and should not be used alone in this patient because the hardware is loose.
Question 16
High Yield
A patient has a displaced midshaft transverse fracture of the humerus and is neurologically intact. Following closed reduction and application of a coaptation splint, the patient cannot dorsiflex the wrist or the fingers at the metacarpophalangeal joints of the hand. What is the next most appropriate step in management?

Explanation
The answer to this question is controversial. All of the standard textbooks state that development of a radial nerve palsy during initial fracture management may represent a laceration or injury of the nerve by bone fragments at the time of manipulation; therefore, surgery should be considered. However, it appears that there is no scientific basis for this decision. A review of the available literature shows that the results were the same for patients who were observed as for those who underwent radial nerve exploration. The indications for surgical exploration include palsies associated with open fractures, irreducible closed fractures, and vascular injuries. The only other relative indication for surgical exploration is following manipulation of a Holstein-Lewis fracture (a distal third fracture of the humerus with a lateral spike). In this type of fracture, exploration may be necessary if a closed reduction leads to radial nerve palsy because the spike may lacerate or compress the nerve. Observation for return of nerve function may be appropriate for 3 months or longer prior to considering late exploration. Bostman O, Bakalim G, Vainionpaa S, Wilppula E, Patiala H, Rokkanen P: Radial palsy in shaft fracture of the humerus. Acta Orthop Scand 1986;57:316-319. Shaz JJ, Bhatti NA: Radial nerve paralysis associated with the fractures of the humerus: A review of 62 cases. Clin Orthop 1983;172:171-176.
Question 17
High Yield
Figure 2 shows the AP radiograph of an 18-year-old woman with progressive and severe right hip pain. Nonsteroidal anti-inflammatory drugs no longer control her pain. What is the next most appropriate step in management?

Explanation
A concentric hip with acetabular dysplasia in a symptomatic patient is best treated by periacetabular osteotomy. The Salter osteotomy is less optimal because the method has limited correction, is uniaxial, cannot be tailored to the deformity, and lateralizes the entire hip joint, thereby increasing the joint reactive forces. Because the hyaline cartilage of the joint is histologically normal, rotating the hyaline cartilage into an optimal position is preferable to augmenting the acetabulum with a shelf or by Chiari osteotomy. Varus intertrochanteric osteotomy has no significant role in the treatment of acetabular dysplasia. Total hip arthroplasty may be required in the future but should not be the first choice.
Question 18
High Yield
What is the most common diagnosis in a patient older than age 40 years with a destructive bony lesion?
Explanation
The most common destructive lesions in a patient older than age 40 years are, in decreasing incidence, metastatic carcinoma, multiple myeloma, lymphoma, and chondrosarcoma. Osteosarcoma is found primarily in younger patients.
Question 19
High Yield
What is the most common bacteria cultured from dog and cat bites to the upper extremity?
Explanation
To define bacteria responsible for dog and cat bite infections, a prospective study yielded a median of five bacterial isolates per culture. Pasteurella is most common from both dog bites (50%) and cat bites (75%). Pasteurella canis was the most frequent pathogen of dog bites, and Pasteurella multocida was the most common isolate of cat bites. Other common aerobes included streptococci, staphylococci, moraxella, and neisseria.
Question 20
High Yield
A 58-year-old man has persistent pain and weakness of his right shoulder after undergoing primary rotator cuff repair 1 year ago. A clinical photograph is shown in Figure 11. Which of the following factors might make functional improvement problematic with revision rotator cuff surgery?

Explanation
Functional improvement after revision rotator cuff surgery is most likely to occur in patients with an intact deltoid, good-quality rotator cuff tissue, preoperative active elevation alone to 90 degrees, and only one prior rotator cuff repair. In this patient, the compromised deltoid origin might make functional improvement less likely. Djurasovic M, Marra G, Arroyo JS, et al: Revision rotator cuff repair: Factors influencing results. J Bone Joint Surg Am 2001;83:1849-1855. Bigliani LU, Cordasco FA, McIlveen SJ, et al: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515.
Question 21
High Yield
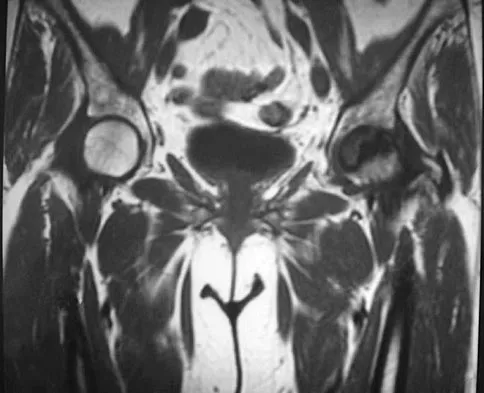
A 2-year-old child has been referred for management of congenital kyphosis. Neurologic examination is normal, and radiographs show a type I congenital kyphosis. Which of the following anomalies is seen in the MRI scan shown in Figure 6?

Explanation
There is a high incidence of intraspinal anomalies in patients with congenital scoliosis and kyphosis. Bradford and associates reported an incidence rate of 38% in 42 patients. The MRI scan shows that the filum terminale is thickened and adherent distally in the spinal canal. Although the conus is at L1, which may be normal, neurologic dysfunction may occur with further growth. There are no signals of high intensity within the cord that would suggest a syrinx. A Chiari II malformation would be found in the upper cervical region, not shown in this MRI scan. Meningocele and diastematomyelia are not present. Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 22
High Yield
Radiographs of an 80-year-old woman with back pain reveal a compression fracture. Which of the following imaging studies best evaluates the acuity of the fracture?
Explanation
The best method of evaluating the acuity of osteoporotic compression fractures is to look for edema in the vertebral body. This is best accomplished with a STIR-weighted MRI scan. Bone scans can show increased uptake at the site of fracture for many months after the fracture. T1-weighted MRI scans show loss of normal marrow fat that may not necessarily correspond with acuity of the fracture. CT scans and radiographs show fracture deformity but cannot be used to judge acuity. Phillips FM: Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 2003;28:S45-S53.
Question 23
High Yield
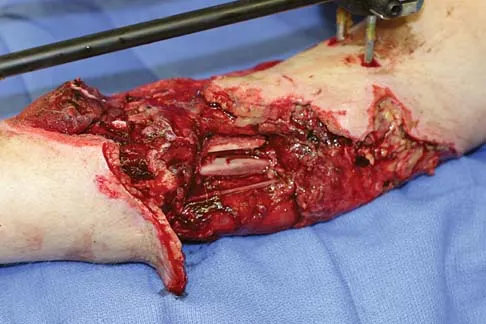
A healthy 25-year-old man sustains a grade IIIB open tibial fracture. Following appropriate debridement, irrigation, and stabilization with an external fixator, the soft-tissue injury is shown in Figure 30. What is the most appropriate definitive soft-tissue coverage procedure?
Explanation
This is a very large near circumferential defect with posterior as well as anterior skin and muscle injury. Bone is exposed. The posterior muscles cannot be rotated since they are part of the zone of injury. The bone and other poorly vascularized areas of this wound would not accept a skin graft. The best chance for limb salvage will be to obtain soft-tissue coverage with a free tissue transfer using the latissimus dorsi. Mathes SJ, Nahai F: Vascular anatomy of muscle: Classification and applications, in Mathes SJ, Nahai F (eds): Clinical Application for Muscle and Musculocutaneous Flaps. St Louis, MO, CV Mosby, 1982, p 20.
Question 24
High Yield
It has been shown that bisphosphonate-based supportive therapy (pamidronate or zoledronate) reduces skeletal events (onset or progression of osteolytic lesions) both in patients with multiple myeloma and in cancer patients with bone metastasis. The use of biphosphonate therapy has been associated with

Explanation
The use of bisphosphonates has been recently associated with the development of osteonecrosis of the jaw. Length of exposure seems to be the most important risk factor for this complication. The type of bisphosphonate may play a role and previous dental procedures may be a precipitating factor. Bisphosphonates are a class of therapeutic agents originally designed to treat loss of bone density (ie, alendronate). The primary mechanism of action of these drugs is inhibition of osteoclastic activity, and it has been shown that these drugs are useful in diseases with propensities toward osseous metastases. In particular, they are effective in diseases in which there is clear upregulation of osteoclastic or osteolytic activity, such as breast cancer and multiple myeloma, and have developed into a mainstay of treatment for individuals with these diseases. Although shown to reduce skeletal events, there has been no improvement in patient survival. Bamias A, Kastritis E, Bamia C, et al: Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J Clin Oncol 2005;23:8580-8587. Thakkar SG, Isada C, Smith J, et al: Jaw complications associated with bisphosphonate use in patients with plasma cell dyscrasias. Med Oncol 2006;23:51-56.
Question 25
High Yield
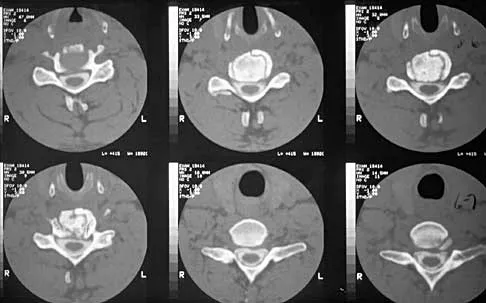
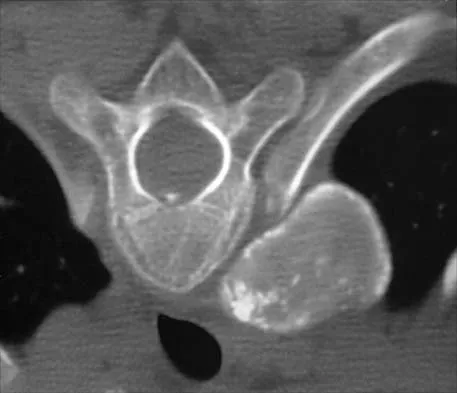
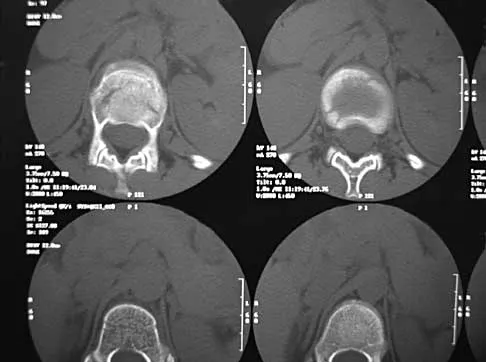
A 10-year-old girl has been referred for evaluation of a prominence at the lower cervical spine. The patient is asymptomatic, and the examination reveals no evidence of neurologic abnormality. A radiograph and CT scans are shown in Figures 12a through 12c. What is the most likely diagnosis?


Explanation
Tuberculosis is uncommon in the cervical spine but has a relatively greater incidence in young children. In a review of 40 patients with lower cervical spine involvement (C2 to C7), 24 were younger than age 10 years at presentation. In children, the disease is characterized by more extensive involvement with the formation of large abscesses. In older patients with lower cervical tuberculosis, the disease is more localized but is more likely to cause paraplegia. Four-drug antituberculosis therapy should be used. For patients with pain or neurologic dysfunction, anterior excision of diseased bone and grafting are indicated. Whether vertebral body excision and grafting should be done in an asymptomatic 10-year-old child is debatable. The CT scan shows a large "cold" abscess that is partially calcified. Hsu LC, Leong JC: Tuberculosis of the lower cervical spine (C2 to C7): A report on 40 cases. J Bone Joint Surg Br 1984;66:1-5.
Question 26
High Yield
Figure 30 shows the MRI scan of a 68-year-old woman who has left hip pain. What is the most appropriate treatment?
Explanation
The patient has a large zone of osteonecrosis of the left femoral head. The wedge-shaped zone of decreased signal intensity on the T1 image in the subchondral region of the femoral head is typical. Based on these findings, total hip arthroplasty is the most appropriate treatment. Open reduction and internal fixation will not help this condition. Incisional biopsy is indicated only if the MRI scan shows a probable neoplasm. Resection of the proximal femur is indicated only for aggressive malignancy. Arthrodesis may be considered in a younger patient but not in a 68-year-old individual. Other treatments, not listed, such as core decompression, vascularized fibular transplant, and osteotomy may be options in selected patients. Urbaniak JR, Jones JP Jr (eds): Osteonecrosis: Etiology, Diagnosis, and Treatment. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 213-223.
Question 27
High Yield
A 26-year-old man sustained an isolated injury to his left hip joint in a motor vehicle accident. Closed reduction was performed, and the postreduction radiograph is shown in Figure 29. Management should now consist of

Explanation
The patient has a posterior fracture-dislocation of the hip and following reduction, an incarcerated fragment of bone resulted in an incongruent reduction. Whereas expedient removal of the fragment is required to limit articular cartilage damage, this situation is not an emergency and the procedure may be performed when the appropriate surgical team is available and the patient is stabilized. Skeletal traction through either the femur or tibia may relieve some pressure on the joint and prevent articular damage. Nonsurgical care for incarcerated fragments is contraindicated. Tile M, Olson SA: Decision making: Non operative and operative indications for acetabular fractures, in Tile M, Helfet DL, Kellam JF (eds): Fractures of the Pelvis and Acetabulum. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 496-532.
Question 28
High Yield
Posterior sternoclavicular dislocations are most commonly associated with which of the following complications?

Explanation
Posterior sternoclavicular dislocations are commonly associated with tracheal compression, which can be a life-threatening condition requiring immediate reduction. The other listed complications are less common. Brooks AL, Henning GD: Injury to the proximal clavicular epiphysis, abstracted. J Bone Joint Surg Am 1972;54:1347-1348.
Question 29
High Yield
The artery located within the substance of the coracoacromial ligament is a branch of what artery?
Explanation
The acromial branch of the thoracoacromial artery courses along the medial aspect of the coracoacromial ligament and may be encountered when performing an open or arthroscopic subacromial decompression. Bleeding can be controlled by ligation of its branch from the thoracoacromial artery. The other arteries may be injured in other surgical exposures of the shoulder. Esch JC, Baker CL: The shoulder and elbow, in Whipple TL (ed): Arthroscopic Surgery. Philadelphia, PA, JB Lippincott, 1993, pp 65-66.
Question 30
High Yield
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?

Explanation
The patient has a midstem periprosthetic fracture, which commonly results in loosening of the prosthesis. Patients who have a large amount of bone loss may require an allograft with the surgical reconstruction. Although the patient reported a fall, her history is also consistent with preexisting loosening of the prosthesis. Chronic infection has been shown in up to 16% of these fractures; however, the patient's work-up revealed no infection. Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 31
High Yield
An otherwise healthy 45-year-old man has a 3-cm subcutaneous mass on his anterior thigh that is presumed to be a lipoma. Removal of the mass is performed in the office of his primary care physician. Pathologic evaluation shows a high-grade malignant fibrous histiocytoma. Staging reveals no evidence of metastatic disease. Management at this time should consist of
Explanation
Resection of a previously excised soft-tissue sarcoma is recommended. Reoperation is recommended after removal of malignant tumors previously believed to be benign, as approximately one half of the patients will have residual tumor in the re-excised specimen. Observation is not indicated in most patients because local recurrence is likely. Radiation therapy alone may result in long-term local control but is felt to be less effective than reoperation. Chemotherapy and radiation therapy alone are not recommended. Wide excision is the most important factor for local disease control. Radiation therapy after surgical re-excision may also decrease the risk of local recurrence. Peabody TD, Monson D, Montag A, Schell MJ, Finn H, Simon MA: A comparison of the prognoses for deep and subcutaneous sarcomas of the extremities. J Bone Joint Surg Am 1994;76:1167-1173. Giuliano AE, Eilber FR: The rationale for planned reoperation after unplanned total excision of soft-tissue sarcomas. J Clin Oncol 1985;3:1344-1348. Lewis JJ, Leung D, Espat J, Woodruff JM, Brennan MF: Effect of resection in extremity soft tissue sarcoma. Ann Surg 2000;231:655-663.
Question 32
High Yield
Figure 26 shows the radiograph of an otherwise healthy Caucasian 5-year-old boy who has a painless limp. What is the best treatment option?

Explanation
The prognosis of Legg-Perthes disease in children younger than age 6 years is good. There is no indication that surgical treatment will improve the outcome. Range-of-motion exercises to prevent contracture may be helpful. Herring JA, Kim HT, Browne R: Legg-Calve-Perthes disease: Prospective multicenter study of the effect of treatment on outcome. J Bone Joint Surg Am 2004;86:2121-2134.
Question 33
High Yield
A 12-year-old girl who has a history of frequent tripping and falling also has bilateral symmetric hand weakness, high arched feet, absent patellar and Achilles tendon reflexes, and excessive wear on the lateral border of her shoes. She reports that she has multiple paternal family members with similar deformities. She most likely has a defect of what protein?
Explanation
The girl shows clinical features of hereditary motor sensory neuropathy type 1, Charcot-Marie-Tooth disease. The most common type of this autosomal-dominant disease is due to an underlying defect in the gene coding for peripheral myelin protein-22 on chromosome 17. Many other less common mutations have been identified in this family of neuropathies. Dystrophin is a protein that is abnormal in Duchenne's muscular dystrophy, which affects males and is diagnosed earlier. Type I collagen is defective in osteogenesis imperfecta. Alpha-L-iduronidase is defective in mucopolysaccharidosis type I, Hurler's syndrome. Defective cartilage oligomeric matrix protein is associated with some forms of multiple epiphyseal dysplasia. Patel PI, Roa BB, Welcher AA, et al: The gene for the peripheral myelin protein PMP-22 is a candidate for Charcot-Marie-Tooth disease type 1A. Nat Genet 1992;1:159-165.
Question 34
High Yield
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann's sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?

Explanation
Adequate decompression of the cervical cord can be achieved in a variety of ways depending on the pathoanatomy of the compression, but kyphosis is a relative contraindication to laminectomy alone. For laminectomy to be effective, the lordosis must be maintained so the cord can displace posteriorly away from the anterior structures. In addition, removing the posterior tension band increases the probability that the kyphosis will progress, therefore increasing the force against the front of the cord as it tents across the kyphosis. Albert TJ, Vaccaro A: Postlaminectomy kyphosis. Spine 1998;23:2738-2745. Truumees E, Herkowitz HN: Cervical spondylotic myelopathy and radiculopthy. Instr Course Lect 2000;49:339-360.
Question 35
High Yield
Figures 25a and 25b show the radiographs of a 66-year-old man who has had a long history of bilateral painful flatfoot deformities. Examination reveals that his foot is partially correctable passively, albeit with discomfort, and he has an Achilles tendon contracture. An ankle-foot orthosis has failed to provide relief. Treatment should now consist of


Explanation
The patient has a pronounced deformity with pain and degenerative arthritis; therefore, triple arthrodesis is the treatment of choice. Gastrocnemius or Achilles tendon lengthening may be a necessary adjunct to the triple arthrodesis, but alone is inadequate to allow for correction. Because the ankle-foot orthosis has failed to provide relief, a UCBL is not likely to help. Osteotomy procedures are designed for lesser deformities and well-preserved joints. Nunley JA, Pfeffer GB, Sanders RW, et al (eds): Advanced Reconstruction: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 115-120.
Question 36
High Yield
A 45-year-old man seen in the emergency department reports a 1-week history of worsening low back pain and a progressive neurologic deficit in the S1 distribution. Examination reveals 2/5 strength in the gastrocnemius. Laboratory studies show a WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 74 mm/h. Radiographs of the lumbosacral spine show narrowing of the L5-S1 disk space, with irregularity of the end plates. A sagittal T2-weighted MRI scan is shown in Figure 8. Definitive management should consist of

Explanation
The history, physical examination, laboratory, and radiographic findings are most consistent with an infectious process. When there are signs of neurologic compromise, surgery is generally recommended. This is an anterior process, and anterior column debridement is necessary, followed by stabilization. Anterior or posterior stabilization is a reasonable option, but posterior decompression alone is unlikely to adequately reverse the process and may lead to segmental kyphosis. Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 165-189.
Question 37
High Yield
Figures 45a and 45b show the radiographs of a 40-year-old woman with rheumatoid arthritis who is unable to straighten her ring and little fingers. Examination reveals that the fingers can be passively corrected, but she is unable to actively maintain the fingers in extension. Management should consist of


Explanation
The patient has extensor tendon ruptures at the level of the wrist that are the result of synovitis at the distal radioulnar joint (Vaughn-Jackson syndrome). Extensor indius proprius transfer appropriately matches strength and excursion of the ruptured extensor digiti quinti and extensor digitorum communis tendons. An extensor tenosynovectomy with distal radioulnar joint resection decreases the synovitis, which if left untreated may cause additional tendon ruptures. Radial head resection is used for posterior interosseous nerve compression secondary to radial head synovitis, and in this patient only two fingers are involved, which rules out this diagnosis. Dynamic splinting is not indicated for ruptured tendons. Metacarpophalangeal arthroplasties and imbrication of the sagittal bands are used for metacarpophalangeal arthritis and extensor tendon subluxation. If this was the problem, the patient should be able to maintain the fingers in extension after they are passively extended. Total wrist arthrodesis prevents the tenodesis effect, thus limiting effective tendon excursion and making the proposed transfer less effective. Feldon P, Terrono AL, Nalebuff EA, et al: Rheumatoid arthritis and other connective tissue diseases: Tendon ruptures, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 1669-1684. Moore JR, Weiland AJ, Valdata L: Tendon ruptures in the rheumatoid hand: Analysis of treatment and functional results in 60 patients. J Hand Surg Am 1987;12:9-14.
Question 38
High Yield
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child's ability to walk in the future?
Explanation
For the parachute test, the examiner holds the child prone and then lowers the child rapidly toward the floor. The parachute reaction is normal or positive if the child reaches toward the floor. The Moro or startle reflex should not be present beyond age 6 months. Asymmetric tonic neck reflex, extensor thrust, and absent foot placement are abnormal findings at any age. Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Question 39
High Yield
A 6-year-old African-American boy with sickle cell disease has had pain and limited use of his right arm for the past 3 days. History reveals that he sustained a humeral fracture approximately 3 years ago. A lateral radiograph is shown in Figure 25. Based on these findings, a presumptive diagnosis of chronic osteomyelitis is made. What are the two most likely organisms?

Explanation
The risk of Salmonella osteomyelitis is much greater in patients with sickle cell disease than the general population. The exact reason for this increased risk is still unclear, but it appears to be associated with an increased incidence of gastrointestinal microinfarcts and abscesses. Both Staphylococcus aureus and Salmonella have been mentioned as the most prevalent causative organisms. Piehl FC, David RJ, Prugh SI: Osteomyelitis in sickle cell disease. J Pediatr Orthop 1993;13:225-227. Givner LB, Luddy RE, Schwartz AD: Etiology of osteomyelitis in patients with major sickle hemoglobinopathies. J Pediatr 1981;99:411-413. Epps CH Jr, Bryant DD III, Coles MJ, Castro O: Osteomyelitis in patients who have sickle-cell disease: Diagnosis and management. J Bone Joint Surg Am 1991;73:1281-1294.
Question 40
High Yield
When performing a long fusion to the sacrum in an osteopenic patient in whom optimal sagittal balance is restored, which of the following is a benefit of extending the distal fixation to the pelvis, rather than the sacrum alone?

Explanation
In osteopenic individuals, even those with excellent obtained or maintained balance, long instrumented fusions to the sacrum impart a high degree of strain, and the sacrum may fail in a transverse fracture or fracture-dislocation pattern. The risk of proximal functional kyphosis is unrelated to distal fixation as are coronal plane correction and rod contouring. Pubic ramus fractures have been shown to be associated with both fixation to the sacrum alone as well as to the ilium.
Question 41
High Yield
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?

Explanation
Excessive flexion gap tightness can be addressed with a variety of techniques; including: (a) recess and release the posterior cruciate ligament; (b) resect a posterior slope in the tibia; (c) avoid an oversized femoral component that moves the posterior condyles more distally; (d) resect more posterior femoral condyle and use a smaller femoral component placed more anteriorly; and (e) release the tight posterior capsule and balance the collateral ligaments.
Question 42
High Yield
Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include

Explanation
The radiographs show massive subsidence of the lateral side of the tibia with severe tibial bone loss and a fractured proximal fibula. Reconstruction should consist of a large metal or bony lateral tibial augmentation, and a stem long enough to bypass the defect is required. The femoral and tibial components are articulating without any remaining polyethylene medially; therefore, the femoral component is damaged and needs revision. The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250. Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Question 43
High Yield
Compared to similar patients who do not donate autologous blood, patients with normal baseline hemoglobin who donate autologous blood prior to undergoing primary total hip arthroplasty are likely to

Explanation
Billote and associates compared patients with normal baseline hemoglobin levels who did and did not donate autologous blood prior to total hip arthroplasty. No patients received allogeneic blood perioperatively, and the autologous donors had significantly lower hemoglobin levels at the time of surgery and in the recovery room. Of the autologous donors, 69% received an autologous transfusion. The authors concluded that autologous donation was unnecessary in patients undergoing primary total hip arthroplasty who had a normal hemoglobin. Billote D, Glisson SN, Green D, Wixson RL: A prospective, randomized study of preoperative autologous donation for hip replacement surgery. J Bone Joint Surg Am 2002;84:1299-1304.
Question 44
High Yield
An 18-year-old football player lands on a flexed knee and ankle after being tackled. Examination reveals increased external rotation and posterior translation and varus at 30 degrees of flexion, which decreases as the knee is flexed to 90 degrees. What is the most likely diagnosis?
Explanation
The flexed knee and ankle mechanism of injury can result in a PCL and/or posterolateral corner injury. The examination reveals an isolated injury to the posterolateral corner (arcuate, popliteus, posterolateral capsule). This results in increased posterior translation and external rotation, as well as varus that is most notable at 30 degrees of flexion and decreases as the knee is further flexed to 90 degrees. Combined PCL and posterolateral corner injuries are characterized by increasing instability as the knee is flexed to 90 degrees from 30 degrees, while isolated PCL tears show the greatest degree of instability at 90 degrees of flexion. A rupture of the quadriceps tendon would not affect anterior or posterior stability, whereas an isolated rupture of the lateral collateral ligament, which is a rare injury, is characterized by varus instability at 30 degrees of knee flexion without posterior translation. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Question 45
High Yield
A 36-year-old nurse has had redness, pain, and small vesicles on the pulp of her middle finger for the past 3 days. Management should consist of
Explanation
Small vesicles on the fingers of a health care worker suggest a herpetic infection, and the management of choice is observation. Incision and drainage may result in a bacterial infection. Marsupialization is used in the treatment of a chronic paronychia. Calcium gluconate is used for hydrofluoric acid burns, and copper sulfate is used for white phosphorus burns. Fowler JR: Viral Infections. Hand Clin 1989;5:613-627.
Question 46
High Yield
A 23-year-old man sustains a unilateral jumped facet with an isolated cervical root injury in a motor vehicle accident. Acute reduction results in some initial improvement of his motor weakness. Over the next 48 hours, examination reveals ipsilateral loss of pain and temperature sensation in his face, limbs, and trunk, as well as nystagmus, tinnitus, and diplopia. What is the most likely etiology for these changes?
Explanation
The patient is showing signs of vertebral artery stroke. The signs of Wallenberg syndrome include those listed above, as well as contralateral loss of pain and temperature sensation throughout the body, an ipsilateral Horner's syndrome, dysphagia, and ataxia. Vertebral artery injuries are not unusual in significant cervical facet injuries. A lesion in the cervical spinal cord is not associated with these symptoms, and an intracranial hemorrhage from trauma is unlikely to present in this manner. Young PA, Young PH: Basic Clinical Neuroanatomy. Baltimore, MD, Williams and Wilkins, 1997, pp 242-243. Hauop JS, et al: The cause of neurologic deterioration after acute cervical spinal cord injury. Spine 2001;26:340-346.
Question 47
High Yield
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?

Explanation
Paletta and Laskins performed a retrospective study of the results of TKA with cement in 22 patients who had a previous patellectomy. Nine of the patients had insertion of a posterior cruciate ligament-substituting implant. Thirteen patients had insertion of a posterior cruciate ligament-sparing implant. The 5-year postoperative knee scores were 89 for the posterior cruciate ligament-substituting knee versus 67 for the posterior cruciate ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Question 48
High Yield
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include
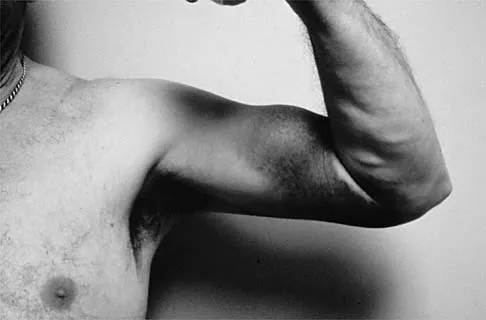
Explanation
The patient has a rupture of the long head of the biceps; however, patients older than age 45 years are at greater risk of having an associated rotator cuff tear. An MRI scan should be ordered to avoid missing concomitant rotator cuff pathology. While patients may report pain radiating down the arm at the time of the tendon rupture, an EMG is not indicated. The short head of the biceps is intact and needs no further work-up, even though the muscle descends in most cases. The anterior labrum can be injured but is not associated with this deformity. Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Question 49
High Yield
What is the primary indication for performing a total wrist arthroplasty in a patient with painful rheumatoid arthritis?
Explanation
The most conservative indications for a total wrist arthroplasty are to spare motion on one side and to improve activities of daily living. Component loosening, dislocation, and wound problems are frequent. Suitable patients can be of various ages, wrist motion, and radiographic stages of arthritis. Ipsilateral total elbow arthroplasty, type III degenerative changes of the wrist, age older than 55, and limited range of motion are neither primary indications nor contraindications to a total wrist arthroplasty. Divelbiss BJ, Sollerman C, Adams BD: Early results of the universal total wrist arthroplasty in rheumatoid arthritis. J Hand Surg Am 2002;27:195-204. Vicar AJ, Burton RI: Surgical management of rheumatoid wrist-fusion or arthroplasty. J Hand Surg Am 1986;11:790-797.
Question 50
High Yield
A 67-year-old retired steelworker was involved in a motor vehicle accident and sustained a midcervical spinal cord injury. Radiographs and MRI scans reveal severe cervical stenosis and spondylosis without fractures or dislocations. Neurologic examination reveals an ASIA C spinal cord impairment with greater motor involvement of the upper extremities than the lower extremities. What is the probability that the patient eventually will become ambulatory?
Explanation
The patient sustained an incomplete spinal cord injury known as central cord syndrome. Central cord syndrome characteristically has disproportionate involvement of the upper extremities with the lower extremities being relatively spared. It is most commonly seen after cervical injuries in elderly patients with spondylosis and spinal stenosis, often without fracture. Penrod and associates noted that 23 of 59 patients with central cord syndrome (ASIA C and D) ultimately walked. The poorest prognosis, however, was in ASIA C patients older than age 50, in which only 40% walked. Penrod LE, Hegde SK, Ditunno JF Jr: Age effect on prognosis for functional recovery in acute, traumatic central cord syndrome. Arch Phys Med Rehab 1990;71:963-968.
Question 51
High Yield
In the radiograph shown in Figure 42, the fracture pattern around this well-fixed stem is classified as Vancouver type

Explanation
The Vancouver classifications describes periprosthetic hip fractures in the following way. Type A fractures are in the trochanteric region. Type B1 fractures occur around the stem or at the tip in the face of a well-fixed stem. These are usually treated with open reduction and internal fixation, usually including struts, cable, and/or cable plates. Type B2 fractures occur in the same region with a loose stem. Type B3 fractures occur with a loose stem where the proximal bone is of poor quality and/or severely comminuted. Type C fractures occur well below the stem. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 149-154. Parvizi J, Rapuri VR, Purtill JJ, et al: Treatment protocol for proximal femoral periprosthetic fractures. J Bone Joint Surg Am 2004;86:8-16.
Question 52
High Yield
Figure 36 shows an AP radiograph of a 65-year-old man who reports activity-related groin pain. History reveals that he underwent total hip arthroplasty 12 years ago. What is the most likely diagnosis?

Explanation
The AP radiograph demonstrates extensive periacetabular osteolysis. The central hole eliminator has dissociated from the shell and migrated into a lytic defect in the ischium. In a retrieval study, most periacetabular osteolytic lesions had a clear communication pathway with the joint space. Lesions with communication to the joint via several pathways or through a central dome hole (as in this patient) were larger and more likely to be associated with cortical erosion. Although periprosthetic tumors have been described, they are rare and particle-induced inflammation around a prosthesis does not seem to increase the risk for carcinogenesis. Visuri T, Pulkkinen P, Paavolainen P: Malignant tumors at the site of total hip prosthesis: Analytic review of 46 cases. J Arthroplasty 2006;21:311-323. Bezwada HP, Shah AR, Zambito K, et al: Distal femoral allograft reconstruction for massive osteolytic bone loss in revision total knee arthroplasty. J Arthroplasty 2006;21:242-248.
Question 53
High Yield
A 17-year-old woman seen in the emergency department reports right knee pain and swelling that has progressively worsened over the past several weeks. Radiographs are shown in Figures 31a and 31b. What is the most likely diagnosis?


Explanation
The radiographs reveal a blastic lesion of the proximal tibial metaphysis with cortical destruction, mineralization extending into the soft tissue laterally, indistinct margins, and destruction of the normal trabecular pattern. In this age group, with this aggressive appearance, osteosarcoma is the most likely diagnosis. Chondroblastoma and giant cell tumor are generally geographic and lytic. Chondrosarcoma is rare in this age group and would likely be a secondary lesion from an underlying chondroid tumor that is not present here. Whereas infection can have a wide variety of appearances, it tends to be more lytic in the acute presentation. Sanders TG, Parsons TW: Radiographic imaging of musculoskeletal neoplasia. Cancer Control 2001;8:221-231.
Question 54
High Yield
What neurovascular structure is at greatest risk when creating a proximal anterolateral elbow arthroscopy portal?
Explanation
The radial nerve is 4 to 7 mm from the anterolateral portal, which is placed 1 cm anterior and 3 cm proximal to the lateral epicondyle. The posterior interosseous nerve can lie 1 to 14 mm from the portal site. Andrews JR, Carson WG: Arthroscopy of the elbow. Arthroscopy 1985;1:97-107.
Question 55
High Yield
A skeletally mature 15-year-old girl who was thrown from the car in a rollover accident sustained the injuries shown in Figures 23a through 23d. Examination reveals no neurologic deficit, but the patient has moderate posterior spinal tenderness at the level of the injury. What is the most appropriate treatment?



Explanation
The majority of patients with thoracolumbar burst fractures without neurologic deficit can be effectively treated with a TLSO or a hyperextension body cast. Indications for surgery are neurologic deficit and/or significant deformity (greater than 50% loss of anterior vertebral body height or marked kyphosis). Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Question 56
High Yield
A 22-year-old college football player reports shortness of breath and dyspnea after a tackle. Examination reveals tachypnea, tachycardia, the trachea is shifted to the right, and there are decreased breath sounds on the left lung fields. The first line of treatment on the field should be
Explanation
The patient has a tension pneumothorax. This is a life-threatening emergency where air is trapped between the pleura and the lung, which prevents expansion of the lung. This causes hypoxia and cardiopulmonary compromise. The first line of treatment is to place a needle into the second intercostal space in the midclavicular line. The athlete should then be transported to the emergency department for chest tube placement. The athlete cannot return to play, and resuscitation is not necessary because he has not gone into cardiopulmonary arrest. Amaral JF: Thoracoabdominal injuries in the athlete. Clin Sports Med 1997;16:739-753.
Question 57
High Yield
An 18-year-old woman sustains a twisting injury of the knee while skiing. Figures 7a and 7b show the radiograph and coronal MRI scan of the knee. In addition to the injury shown, what is the most likely associated injury?


Explanation
The MRI scan shows a Segond fracture, which is a small avulsion of the lateral joint capsule from the anterolateral aspect of the proximal tibia. It is almost always associated with anterior cruciate ligament rupture and often with a tear of either the medial or lateral meniscus. Goldman AB, Pavlov H, Rubenstein D: The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol 1988;151:1163-1167. Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the knee. Am J Sports Med 2005;33:131-148.
Question 58
High Yield
What is the main mechanism for nutrition of the adult disk?
Explanation
Disk nutrition occurs via diffusion through pores in the end plates. The disk has no direct blood supply, and the anulus is not porous to allow diffusion. The dorsal root ganglion does not provide blood supply to the disc. Biyani A, Andersson GB: Low back pain: Pathophysiology and management. J Am Acad Orthop Surg 2004;12:106-115. Urban JG, Holm S, Maroudas A, et al: Nutrition of the intervertebral disc: Effect of fluid flow on solute transport. Clin Orthop 1982;170:296-302.
Question 59
High Yield
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
Passive stretching is contraindicated during rehabilitation as it may potentiate the severity of the myositis ossificans. Electrical stimulation, iontophoresis, isometric exercise, and ice/heat contrast are not known to exacerbate this process. Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Question 60
High Yield
A 60-year-old man with diabetes mellitus is referred for evaluation of nonhealing ulcers of his left foot. Nonsurgical management has failed to provide relief, and a below-the-knee amputation is being considered. Which of the following studies best predicts successful amputation wound healing?
Explanation
The TcPO2 measures the O2 delivering capacity of the local vasculature. Values above 40 mm Hg have been shown to correlate with positive healing potential. The hemoglobin A1c is a good indicator of long-term glucose levels; however, it has no direct correlation with wound healing potential. Serum albumin is an indirect measure of nutritional status, and deficiencies in nutrition must be addressed before any surgery. Adequate hemoglobin levels are also necessary to promote adequate oxygenation to the amputation site. The ankle-brachial index may be falsely elevated as a result of calcified vessels in patients with diabetes mellitus. Wyss CR, Harrington RM, Burgess EM, et al: Transcutaneous oxygen tension as a predictor of success after amputation. J Bone Joint Surg Am 1988;70:203-207.
Question 61
High Yield
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?

Explanation
In the early 1990s, a transition was made from a two-incision ACL reconstruction to a single-incision ACL reconstruction, and there was concern over divergence of the femoral screws. It was shown radiographically that approximately 5% of the time, divergence of the screw was greater than 15 degrees from the bone plug. In a bovine model, there was significant loss of pull-out strength with an increase in divergence from 15 degrees to 30 degrees. Therefore, attempts should be made to minimize divergence to 15 degrees or less. Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Question 62
High Yield
A 55-year-old woman with type I diabetes mellitus has a chronic ulcer over the dorsum of her right foot and reports forefoot pain. Examination reveals 1- x 2-cm nondraining ulcer over the dorsum of the foot. The patient has 1-2+ pain with compression of the foot and ankle. She has a weakly palpable posterior tibial pulse and an absent dorsalis pedis pulse. There is no erythema, cellulitis, or drainage. Radiographs are normal. Which of the following diagnostic studies should be obtained?
Explanation
The presence of a dorsal ulcer in the presence of weak or absent pulses strongly suggests the possibility of arterial insufficiency. The best initial noninvasive study to assess for ischemia is the Doppler arterial study. A determination of the vascular status is of a greater priority than an assessment for infection or neuropathy because of the location and presentation of the ulcer. If ankle pressures are less than 45 mm Hg, there is a high risk that these lesions will not heal without revascularization. Wagner FW Jr: The dysvascular foot: A system for diagnosis and treatment. Foot Ankle 1981;2:64-122.
Question 63
High Yield
A 61-year-old woman has increasing pain in her left great toe. She states that she has had discomfort for years but now has pain with all shoe wear. A radiograph is shown in Figure 35. To provide the most predictable pain-free result, treatment should consist of

Explanation
Because the patient has a hallux valgus with increased intermetatarsal and hallux valgus angles and advanced degenerative arthritis of the joint, arthrodesis of the first metatarsophalangeal joint will provide the most predictable pain-free result. An attempt to correct the bunion with a bunionectomy or osteotomy would most likely fail. The hallux valgus and advanced degenerative changes put the foot beyond the indications for a cheilectomy. Long-term results with silicone arthroplasty have been disappointing. Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Question 64
High Yield
A 35-year-old woman with type 1 diabetes mellitus has been treated for the past 2 years at a wound care center for persistent bilateral fifth metatarsal head ulcers. Management has consisted of shoe wear modifications, treatment with multiple enzymatic ointments, and a fifth metatarsal head resection on the left side. Physical examination reveals intact pulses, minimal ankle dorsiflexion, neutral hindfoot, and a persistent ulcer under the fifth metatarsal heads. What treatment will best help heal the ulcers?
Explanation
The patient likely has a significant Achilles contracture that causes her to always bear more weight on her forefoot. A gastrocnemius recession takes the ankle out of plantar flexion and she will be able to return to a normal gait and reduce the pressures on her forefoot. A forefoot amputation is a salvage option. The other choices are appropriate; however, the patient has had this problem for 2 years and she has already had multiple attempts at shoe wear modification. Laughlin RT, Calhoun JH, Mader JT: The diabetic foot. J Am Acad Orthop Surg 1995;3:218-225.
Question 65
High Yield
At the level of the midcalf, the plantaris tendon is found at which of the following locations?
Explanation
The plantaris tendon is often harvested to augment a tendon reconstruction. The origin of the plantaris muscle is on the posterolateral aspect of the distal femur, and the muscle lies lateral to the tibial nerve and the posterior tibial artery. The tendon then courses posteriorly between the soleus and the medial head of the gastrocnemius. Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3. Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 475.
Question 66
High Yield
A 7-year-old boy is seen in the emergency department with an isolated and displaced supracondylar humerus fracture and absent radial and ulnar pulses. Despite a moderately painful attempt at realignment, examination reveals that his hand remains pulseless. What is the next most appropriate step in management?
Explanation
Displaced supracondylar humerus fractures in children may have associated vascular compromise. Decreased blood flow may be due to vessel injury, entrapment within the fracture site, kinking from fracture displacement, or from vessel spasm. Optimal initial treatment in the emergency department includes gentle realignment of the limb and vascular assessment. Angiography is not required in isolated injuries as the level of the vessel compromise is always at the site of the fracture. When blood flow is not restored, the next best step in treatment is to proceed urgently to the operating room. A formal closed reduction and pinning is performed, and then the vascular status is reassessed. Exploration and vascular repair is required if the hand is cool, white, and without pulses. Ay S, Akinci M, Kamiloglu S, et al: Open reduction of displaced pediatric supracondylar humeral fractures through the anterior cubital approach. J Pediatr Orthop 2005;25:149-153. Sabharwal S, Tredwell SJ, Beauchamp RD, et al: Management of pulseless pink hand in pediatric supracondylar fractures of humerus. J Pediatr Orthop 1997;17:303-310.
Question 67
High Yield
A player on a professional football team sustains a knee injury and is diagnosed with an anterior cruciate ligament rupture. When employed as the team physician, your ethical obligation is to inform
Explanation
When you are employed as a team physician, you are obligated to inform the players and the team organization of all athletically relevant medical issues. This differs significantly from the normal rule of patient confidentiality. If the player came to see you and you were not the team physician, you may not inform the team unless the player so desires. As the team physician, you are not obligated to inform the media. Tucker AM: Ethics and the professional team physician. Clin Sports Med 2004;23:227-241.
Question 68
High Yield
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?

Explanation
The tibia has grown into valgus secondary to the proximal fracture. This occurs in about one half of these injuries, and maximal deformity occurs at 18 months postinjury. The deformity gradually improves over several years, with minimal residual deformity. Therefore, treatment at this age is unnecessary as there is a high rate of recurrence and complications regardless of technique. The valgus deformity is not a result of physeal injury or growth arrest. Medial proximal tibial hemiepiphysiodesis is an excellent method of correcting the residual deformity but is best reserved until close to the end of growth. Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482. McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 69
High Yield
What vessel is marked with an asterisk in Figure 44?
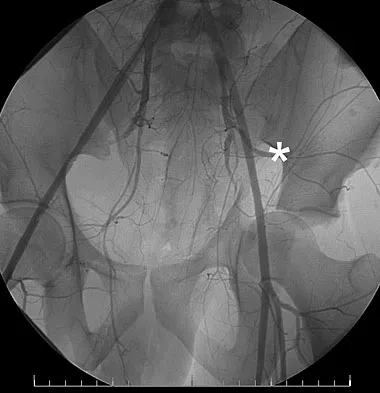
Explanation
The superior gluteal artery is a branch of the posterior division of the internal iliac artery and exits the pelvis through the greater sciatic notch. It can be injured as a result of a pelvic ring fracture or acetabular fracture that has a fracture of the posterior column. Agur AM, Dalley AF (eds): Grant's Atlas of Anatomy, ed 12. Philadelphia, PA, Lippincott Williams and Wilkins, 2008.
Question 70
High Yield
What is the most common complaint in patients with a developmental radial head dislocation?
Explanation
Developmental dislocation of the radial head most frequently presents as a painless mass over the posterior aspect of the elbow. Patients do not have feelings of elbow subluxation but may report pain or clicking. Limitation of motion is most frequently found in the pronation and supination arc rather than in flexion and extension. Lloyd-Roberts GC, Bucknill TM: Anterior dislocation of the radial head in children-etiology: Natural history and management. J Bone Joint Surg Am 1977;58:402.
Question 71
High Yield
A collegiate football player who sustained a blow to the head during the first quarter of a game is confused for several minutes after the hit but does not lose consciousness. He had two similar episodes in games earlier in the season. When should he be allowed to return to play?
Explanation
Using the traditional concussion grading scale, the patient sustained a grade I concussion because he did not lose consciousness and his abnormal cognitive level lasted less than 1 hour. If this was the player's first concussion, theoretically he could return to play later in the game provided that he had no confusion, headache, or associated symptoms. However, because it was the third concussion for the year, participation in contact sports should be terminated for the season. Guskiewwicz KM, Barth JT: Head injuries, in Schenk RC Jr (ed): Athletic Training and Sports Medicine. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 143-167.
Question 72
High Yield
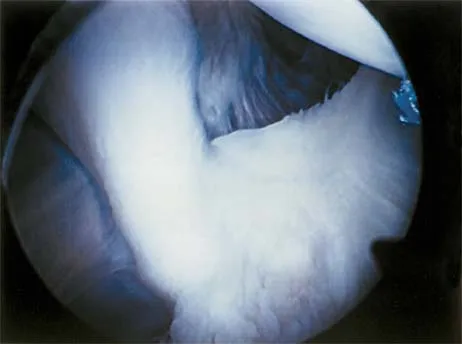
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of

Explanation
Subscapularis tendon tears are being recognized with increasing frequency, and the mechanism of injury involves hyperabduction and external rotation. The patient will have anterior shoulder pain and may report a sensation of instability. Examination will reveal anterior shoulder tenderness over the lesser tuberosity and bicipital groove, and the Gerber lift-off test usually is positive. The MRI scan shown here reveals an intact anterior labrum. The subscapularis tendon is avulsed and retracted, with no evidence of the biceps tendon within the groove; this implies dislocation of the biceps, a common accompanying feature of a subscapularis tear. This injury is also recognized as a complication after open anterior shoulder stabilizations where the subscapularis has been incised as part of the approach. Therefore, the appropriate management involves repair of the subscapularis. The injury does not represent a recurrence so immobilization or revision stabilization, which may be reasonable treatment for recurrent instability, is not indicated. The findings are not consistent with a superior labral tear. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 73
High Yield
Which of the following types of iliac osteotomy provides the greatest potential for increased coverage?
Explanation
The degree of acetabular dysplasia and the age of the child are important considerations when choosing what type of osteotomy to perform. The ability to obtain concentric reduction is a prerequisite of all osteotomies that redirect the acetabulum. Procedures that cut all three pelvic bones allow more displacement and, therefore, correction of acetabular dysplasia. The closer the osteotomy is to the acetabulum, the greater the coverage of the femoral head. Compared with the other acetabular osteotomies, the Ganz periacetabular osteotomy provides the greatest potential for correcting acetabular deficiency because there are no bone or ligamentous restraints to limit correction, but it has the disadvantage of being a technically demanding procedure. The amount of coverage provided by the Salter osteotomy is limited. Millis MB, Poss R, Murphy SB: Osteotomies of the hip in the prevention and treatment of osteoarthritis, in Eilert RE (ed): Instructional Course Lectures XLI. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1992, pp 145-154.
Question 74
High Yield
A 70-year-old golfer has pain in her dominant shoulder. She reports that initially the pain was at night but now she is unable to play. Examination reveals weakness in external rotation and shoulder abduction. Radiographs reveal the humeral head articulating with a thin acromion. Management should consist of

Explanation
Chronic rotator cuff tears should be nonsurgically managed initially with a strengthening program. A cortisone injection may reduce inflammation. Surgery is reserved for patients who continue to have pain and lose sleep despite the use of physical therapy. Blood tests for infection or inflammation are nonspecific. Arthroscopy may play a role, but surgical replacement is reserved for advanced cases. Bokor DJ, Hawkins RJ, Huckell GH, et al: Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
Question 75
High Yield
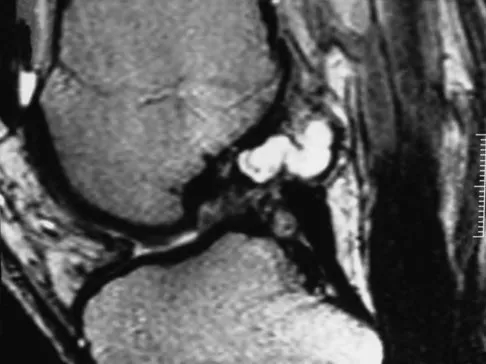
A 21-year-old soccer player reports pain and is unable to straighten his knee following an acute injury during a game. He is unable to continue to play. An MRI scan is shown in Figure 3. What is the next most appropriate step in management?

Explanation
The patient has a locked knee that cannot be fully extended. This is most likely the result of the mechanical block of a bucket-handle tear that has flipped into the notch. Also, the pain may be so severe that the muscle spasm prevents the knee from straightening out. When the patient is anesthetized, the muscle spasm relaxes and the meniscus can be reduced out of the notch. Arthroscopy is the treatment of choice. A meniscal repair is usually possible in large bucket-handle tears because the meniscus is torn in the red-red zone where most of the vascular supply is located. If the handle portion is badly frayed or damaged, a partial meniscectomy should be performed. The classic finding on MRI is a "double PCL sign." This is due to the flipped portion of the meniscus in the notch. Critchley IJ, Bracey DJ: The acutely locked knee: Is manipulation worthwhile? Injury 1985;16:281-283.
Question 76
High Yield
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?

Explanation
Based on these findings, the most likely diagnosis is a rotator cuff injury and probable tear; therefore, MRI is the study of choice. CT is preferred for articular fractures. A bone scan is nonspecific and can identify inflammation or occult fracture. Joint aspiration is not likely to identify an effusion. Physical therapy and a functional capacity examination are used to identify weakness during recovery prior to a return to work or sports. Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Question 77
High Yield
The posterior cord of the brachial plexus terminates into what two main branches?
Explanation
The posterior cord of the brachial plexus terminates into the radial and axillary nerves. The lateral cord terminates in branches to the musculocutaneous and the lateral root of the median nerve. The medial cord terminates in branches to the ulnar and medial roots of the median nerve.
Question 78
High Yield
What letter in Figure 33 marks the correct starting point for a transiliac pelvic screw?
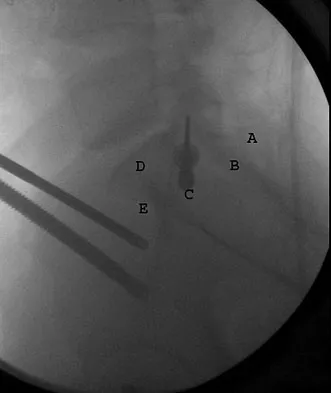
Explanation
Iliosacral screws cannot always be placed safely due to variations in pelvic anatomy. Transiliac bars are an alternative method for fixation but are placed using an open technique. A screw can be placed percutaneously through both iliac wings posterior to the posterior border of the sacrum. The starting point is visualized using a lateral C arm shot and is located on the posterior iliac crest at about the level of the S1 body where the crest has its largest area posterior to the sacrum. This area is labeled A in the figure, B represents the sacral canal, C is S1, D is the area cephalad to the iliocortical density, and E is the anterior border of the sacrum. The radiograph demonstrates a well-placed sacroiliac screw. Moed BR, Fissel BA, Jasey G: Percutaneous transiliac pelvic fracture fixation: Cadaver feasibility study and preliminary clinical results. J Trauma 2007;62:357-364.
Question 79
High Yield
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient?

Explanation
The next step in the management of this injury is completion of the shoulder trauma series. An axillary radiograph, which can be quickly performed in the emergency department, must be obtained to accurately assess the humeral head relationship to the glenoid. If difficulty is encountered, a "Velpeau" axillary may be substituted. If that fails to elucidate the status of the glenohumeral joint, a CT scan should be obtained.
Question 80
High Yield
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?

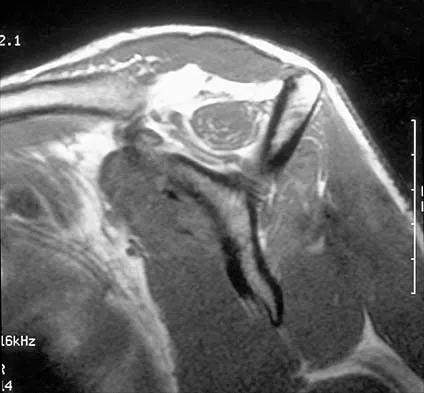
Explanation
The sagittal image reveals increased signal and decreased size of the supraspinatus and infraspinatus muscles, indicating muscle atrophy. The rotator cuff tendon signal is normal. The subscapularis and teres minor muscles are unaffected. Muscular dystrophy and thoracic outlet syndrome would be expected to have a more global effect. Although muscular atrophy can occur in the setting of a rotator cuff tear, the coronal image shows an intact supraspinatus. The suprascapular nerve supplies the supraspinatus and infraspinatus muscles. Therefore, suprascapular nerve entrapment would result in atrophy of these muscles with sparing of the surrounding musculature. Any lesion within the suprascapular notch, including neoplastic disease, a venous varix, or neuroma, can place pressure on the suprascapular nerve. Suprascapular nerve entrapment most commonly results from extension of a paralabral cyst or ganglion, often with associated labral pathology. Spinal accessory nerve disruption would show trapezius muscle atrophy. Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
Question 81
High Yield
Which of the following nerves is most likely responsible for symptoms associated with plantar fasciitis?

Explanation
The first branch of the lateral calcaneal nerve innervates the abductor digiti minimi. It is reported to be trapped at the interval between the abductor hallucis and the quadratus plantae muscles.
Question 82
High Yield
A 13-year-old boy has pain and a firm mass in his left knee. A radiograph and MRI scan are shown in Figures 2a and 2b, and a biopsy specimen is shown in Figure 2c. Based on these findings, what is the most likely diagnosis?


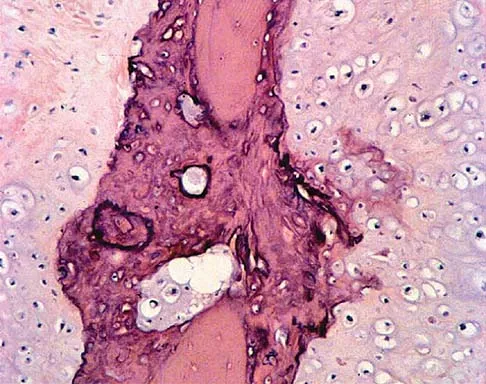
Explanation
The most likely diagnosis is osteosarcoma. The imaging studies show an aggressive primary tumor of bone, and the histology slide shows a typical chondroblastic osteosarcoma, with osteoid deposited along the surface of bone trabeculae. Ewing's sarcoma histologically consists of small round blue cells. Osteochondroma and periosteal chondroma can occur near the knee but have different radiographic and histologic patterns. Chondrosarcoma rarely occurs in children. Simon M, Springfield D, et al: Osteogenic sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 267.
Question 83
High Yield
A 14-year-old patient with an L3 myelomeningocele underwent anterior and posterior spinal fusion for a curve of 50 degrees. Follow-up examination 1 week after the procedure now reveals persistent drainage from the posterior wound. Results of laboratory cultures show Streptococcus viridans, Staphylococcus aureus, and Enterococcus. In addition to IV antibiotics, surgical irrigation, and debridement, management should include
Explanation
The rate of wound infections has dramatically decreased with the routine use of prophylactic antibiotics. Factors known to increase the risk of infection include instrumentation, prolonged surgical time, excessive blood loss, poor perioperative nutritional status, a history of surgery, and a history of infection. The use of allograft does not result in an increased rate of infection. Adequate treatment requires early diagnosis and intervention. Temperature elevation and persistent wound drainage are highly suspicious for infection. An erythrocyte sedimentation rate and a WBC are not useful in diagnosis unless serial examinations show rising levels. Patients should be taken to the operating room where the entire wound can be reopened, irrigated, and debrided. Bone graft can be washed and replaced. Hardware should not be removed. The wound should be closed over suction drains. IV antibiotics should be given for a period of at least 10 days, followed by 6 weeks orally. Leaving the wound open to granulate with dressing changes results in prolonged hospitalization, inadequate treatment of the infection, and a poor cosmetic result. Lonstein JE: Complications of treatment, in Bradford DS, Lonstein JE, Moe JH, et al (eds): Moe's Textbook of Scoliosis and Other Spinal Deformities, ed 2. Philadelphia, Pa, WB Saunders, 1987, p 476.
Question 84
High Yield
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?


Explanation
The patient has a posterior shoulder dislocation. The AP radiograph shows overlapping of the humeral head on the glenoid. The scapular Y view shows his humeral articular surface posterior to the glenoid. The posterior shoulder dislocation is frequently missed because the patient is comfortable in the "sling" position with the arm adducted and internally rotated across the abdomen. The marked restriction in external rotation on examination raises the suspicion of a posterior dislocation, adhesive capsulitis, or glenohumeral osteoarthritis. The posterior dislocation is diagnosed based on the radiographic findings. An axillary view or CT is recommended to better evaluate the dislocation. Robinson CM, Aderinto J: Posterior shoulder dislocations and fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Question 85
High Yield
Which of the following is considered the most common complication of the impaction grafting technique for femoral revision surgery?
Explanation
Impaction grafting technique for femoral revision surgery has become increasingly popular over the past decade. This technique is designed to address cavitary deficiencies of the femur. The femoral stem is inserted with cement fixation. Its clinical efficacy has not been shown to be superior to extensively porous-coated stems. Early subsidence of the stem has been reported in more than 50% of the patients. However, loss of fixation has occurred infrequently (5%) in reported series conducted by experienced surgeons. It has not been shown to have a higher infection rate. Gie GA, Linder L, Ling RS, Simon JP, Slooff TH, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Question 86
High Yield
Which of the following factors is associated with the worst prognosis in soft-tissue sarcomas?
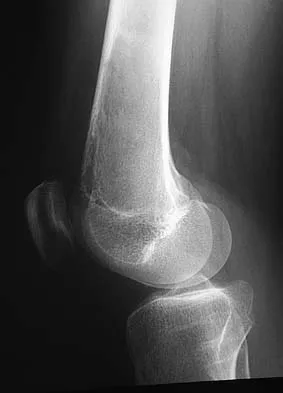
Explanation
Although factors such as a high-grade tumor and large size are associated with decreased survival, the presence of metastases carries the worst prognosis. Good results are very rare when metastases are present. Soft-tissue sarcomas, as a whole, respond poorly to chemotherapy, leading to a poor prognosis when metastases are present. Collin C, Goobold J, Hadju SI, Brennan MF: Localized extremity soft tissue sarcoma: An analysis of factors affecting survival. J Clin Oncol 1987;5:601-612.
Question 87
High Yield
Based on the findings shown in Figures 22a and 22b, corrective surgery to obtain maximal safe correction and optimal instrumentation fixation should be performed at which of the following locations?


Explanation
The clinical photograph and radiograph show an iatrogenic flatback deformity with loss of the normal lumbar lordosis. The safest correction for this malalignment typically is performed away from the spinal cord in the midlumbar spine, most commonly at L2 or L3. The more distal the correction is performed, the more sagittal plane translation of the C7 plumb line with respect to the posterior sacrum. Performing the osteotomy too distally, however, makes it difficult to obtain adequate distal fixation. Shufflebarger HL, Clark CE: Thoracolumbar osteotomy for postsurgical sagittal imbalance. Spine 1992;17:S287-S290.
Question 88
High Yield
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include

Explanation
The patient has a displaced radial neck fracture. Displaced radial neck fractures with angulation of more than 30 to 45 degrees require reduction. Methods of attempted closed reduction include wrapping the arm with an Esmarch's bandage and applying direct pressure over the maximum deformity of the radial head. More aggressive methods include a Kirschner wire used as a joystick or intramedullary reduction as described by the Metaizeau technique. Open reduction should be avoided because of complications such as stiffness or osteonecrosis. Indications for open reduction are irreducible displacement of more than 45 degrees with severe restriction of forearm rotation. Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop 2000;20:7-14. Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39. Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Question 89
High Yield
Which of the following factors is most likely to be associated with prolonged survival of total knee arthroplasty?
Explanation
In a survivorship study of 9,200 total knee arthroplasties, Rand and Ilstrup identified four independent variables associated with a significantly lower risk of failure: primary total knee arthroplasty, diagnosis of rheumatoid arthritis, age of 60 years or older, and use of a condylar prosthesis with a metal-backed tibial component. Other clinical studies report the use of a posterior stabilized prosthesis to be comparable to a total condylar prosthesis with retained posterior cruciate ligament. Rand JA, Ilstrup DM: Survivorship analysis of total knee arthroplasty: Cumulative rates of survival of 9200 total knee arthroplasties. J Bone Joint Surg Am 1991;73:397-409. Stern SH, Insall JN: Posterior stabilized prosthesis: Results after follow-up of nine to twelve years. J Bone Joint Surg Am 1992;74:980-986.
Question 90
High Yield
What region of the spine is most susceptible to changes in the vascular supply to the spinal cord during an anterior approach?
Explanation
The thoracic spinal cord is characterized by a variable and, at times, complicated blood supply. The artery of Adamkiewicz, also known as the great anterior medullary artery, most typically arises off the left side of the aorta between T8 and T12. It represents the sole medullary blood supply to the thoracic spine. When this artery is divided or injured, the blood supply to the thoracic cord may be interrupted. It is important to avoid electocautery of blood vessels within or near the thoracic foramen because this is a site of important, albeit limited, collateral circulation. Sharma M, Anderson FC: Spinal vascular lesions, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 301-306.
Question 91
High Yield
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?

Explanation
The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 92
High Yield
A 25-year-old farm worker sustained a grade III open fracture of the midshaft of the left tibia after falling from a ladder. Which of the following antibiotic regimens is best for this patient?

Explanation
Patients who sustain grade III open fractures that are related to a farm environment require ampicillin or penicillin for Clostridium coverage. Holton PD, Mader J, Nelson CL, Osmon DR, Patzakis MJ: Antibiotics for the practicing orthopaedic surgeon. Instr Course Lect 2000;341:36-42.
Question 93
High Yield
Which of the following studies best increases the ability to diagnose femoral neck fractures in patients with femoral shaft fractures?

Explanation
Tornetta and associates and Yang and associates found that nearly half of all femoral neck fractures associated with femoral shaft fractures were being missed at their institution. On the basis of the delayed diagnosis of these injuries, a best-practice protocol was developed by the attending trauma surgeons for the evaluation of the femoral neck in patients with a femoral shaft fracture. This protocol includes a preoperative AP internal rotation radiograph of the hip, a fine-cut (2-mm) CT scan through the femoral neck (as a part of the initial trauma scan), and an intraoperative fluoroscopic lateral evaluation of the hip just prior to fixation of the femoral shaft. In addition, postoperative AP and lateral radiographs of the hip are made in the operating room to specifically evaluate the femoral neck before the patient is awakened. They found that fine-cut CT (2 mm was the best screening tool in this group of patients) identified 12 of the 13 fractures, whereas 8 of the 13 fractures were visible on the dedicated preoperative AP internal rotation hip radiographs. Tornetta P III, Kain MS, Creevy WR: Diagnosis of femoral neck fractures in patients with a femoral shaft fracture: Improvement with a standard protocol. J Bone Joint Surg Am 2007;89:39-43.
Question 94
High Yield
A 25-year-old competitive skier sustains a twisting injury to the right ankle while skiing. She is unable to continue the activity secondary to severe lateral ankle pain. Examination reveals ecchymosis and fullness over the lateral malleolus with pain and weakness on active ankle dorsiflexion and external rotation. There is no medial-sided pain. Neurovascular examination is normal. An AP radiograph and MRI scan are shown in Figures 17a and 17b, respectively. Management should consist of

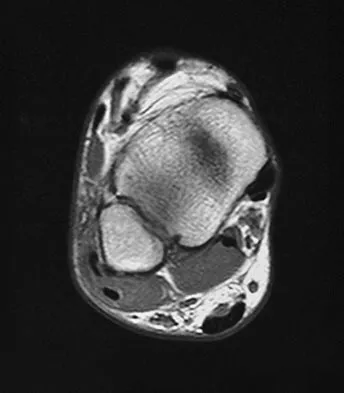
Explanation
The MRI scan shows a dislocated peroneus brevis tendon with disruption of the peroneal retinaculum. This injury is commonly seen in skiers and is the result of peroneal contraction with the ankle everted and dorsiflexed. Nonsurgical management is rarely successful; therefore, repair of the peroneal retinaculum is the treatment of choice. Eckert WR, Davis EA Jr: Acute rupture of the peroneal retinaculum. J Bone Joint Surg Am 1976;58:670-672. Murr S: Dislocation of the peroneal tendons with marginal fracture of the lateral malleolus. J Bone Joint Surg Br 1961;43:563-565.
Question 95
High Yield
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals
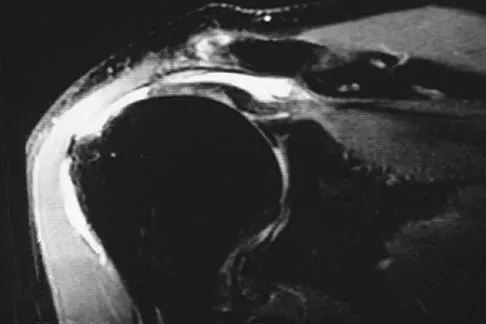
Explanation
The MRI scan reveals a full-thickness rotator cuff tear with retraction and increased signal in the subacromial space indicating joint fluid. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Question 96
High Yield
The risk of local recurrence after surgical resection of a soft-tissue sarcoma is most closely related to

Explanation
A positive margin is most closely related to subsequent local recurrence. The other factors cited, including the size and site of the tumor, may be related to local recurrence; however, they are more commonly prognostic because of the difficulty in obtaining wide surgical margins about large or proximal tumors. Radiation therapy has been noted to decrease the incidence of recurrence but is not felt to be as important as the surgical margin. The grade of the tumor has more influence on the prevalence of metastatic disease than the incidence of local recurrence. Lewis JJ, Leung D, Heslin M, Woodruff JM, Brennan MF: Association of local recurrence with subsequent survival in extremity soft tissue sarcoma. J Clin Oncol 1997;15:646-652.
Question 97
High Yield
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of

Explanation
An exercise program to strengthen the deltoid and remaining rotator cuff will most likely offer the best results. Revision rotator cuff surgery yields better results in decreasing pain than improving strength and function, and this patient has only minimal pain. Tendon transfers, involving the use of the latissimus dorsi or teres major, have been used when the rotator cuff is deemed irreparable but are not indicated in elderly patients with minimal symptoms. Bigliani LU, Cordasco FA, McIlveen SJ, Musso ES: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515. DeOrio JK, Cofield RH: Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-567.
Question 98
High Yield
Based on the type of articulation shown in Figure 32, wear is not affected by which of the following factors?

Explanation
Wear in total hip arthroplasty is a very complex phenomenon. The radial mismatch of the femoral head to the acetabular component has been shown in multiple studies to be a significant factor in wear. The mismatch can neither be too small nor too large. When the mismatch is too small, seizing of the implants can occur. When the mismatch is too large, contact stresses increase and produce exceptionally high wear. The ideal radial mismatch should be approximately 50 microns. Surface roughness and ball sphericity are two items that are extremely important with respect to wear. High carbon content has been shown to decrease wear. This device has a very large head-to-neck ratio, so impingement-related wear is unlikely. Amstutz HC, Grigoris P: Metal on metal bearings in hip arthroplasty. Clin Orthop 1996;329:S11-S34. Amstutz HC, Campbell P, McKellop H, et al: Metal on metal total hip replacement workshop consensus document. Clin Orthop 1996;329:S297-S303.
Question 99
High Yield
What are the most common portals for arthroscopic surgery of the ankle?

Explanation
The most commonly used portals are the anterolateral, anteromedial, and posterolateral portals. They have been shown to be the safest areas for portal placement, allowing no penetration of neurovascular structures. All the other portals involve placing another structure at risk. The anterocentral portal is close to the deep peroneal nerve and anterior tibular artery. The trans-Achilles portal is not recommended because of its limited utility and potential to injure the Achilles tendon. The posteromedial portal is too close to the posterotibial artery and nerve, the flexor hallucis longus and flexor digitorum longus tendons, and the branches of the calcaneal nerve. Stetson WB, Ferkel RD: Ankle arthroscopy: I. Technique and complications. J Am Acad Orthop Surg 1996;4:17-23.
Question 100
High Yield
A 9-year-old girl has pain over the fifth toe that is aggravated by shoe wear. Clinical photographs are shown in Figures 28a and 28b. Treatment of this deformity should consist of


Explanation
The major obstacle to overcome in the surgical treatment of this cock-up deformity is recurrence. Dorsal releases can be performed; however, chronic dislocation of the fifth MTP joint usually needs to be addressed with plantar release as well. Chronic dorsal soft-tissue contractures may be overcome with translation of the toe into a plantar-based incision, as described originally by Cockin and accredited to Butler. This is the treatment of choice. Resection of the proximal phalanx improves symptoms but induces a secondary deformity; this procedure is usually reserved for skeletally mature individuals. Black GB, Grogan DP, Bobechko WP: Butler arthroplasty for correction of adducted fifth toe: A retrospective study of 36 operations between 1968 and 1982. J Pediatr Orthop 1985;5:439-441. Paton RW: V-Y plasty for correction of varus fifth toe. J Pediatr Orthop 1990;10:248-249.
