Question 76
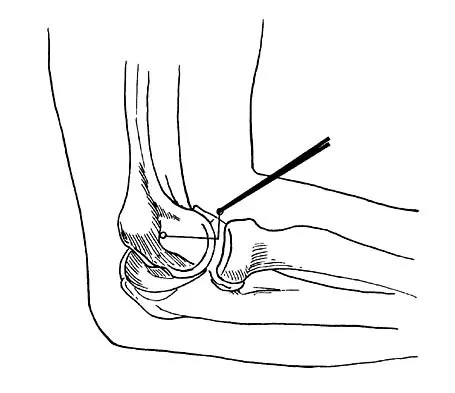
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
The radial nerve is only 4 mm from the anterolateral portal, while the median nerve is 11 mm away from the anteromedial portal. The ulnar nerve is only at risk on the medial side of the elbow. Anterior and posterior interosseous nerves are more distal within the forearm and are not in danger during portal placement. O'Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Question 77
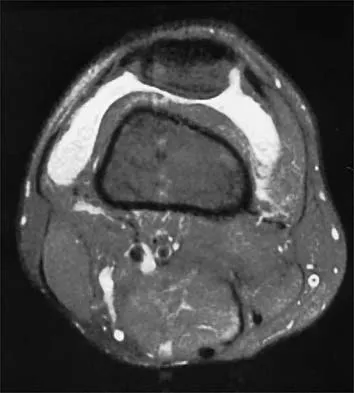
A 39-year-old man has anterior shoulder pain after landing on his abducted left shoulder while playing softball. Examination reveals a stable glenohumeral joint, pain on passive external rotation of greater than 25 degrees, and pain and weakness on belly press (Napoleon's) test. An MRI scan is shown in Figure 32. To provide maximum pain relief and return of function, management should include
Explanation
The examination and MRI scan confirm a subscapularis rupture and dislocation of the long head of the biceps tendon. The greatest return of function will result from repair of the subscapularis and tenodesis of the biceps tendon. Physical therapy alone will result in inadequate healing of the subscapularis and will not address the biceps tendon. While biceps tenotomy is an option, it will not provide the same level of pain relief and return of function as a tenodesis in a young, active man. There is no evidence for a supraspinatus tear. Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Question 78
A 37-year-old racquet player had dominant shoulder pain for 1 year, and cortisone injections provided only temporary relief. Because MRI findings did not reveal a rotator cuff tear, he underwent arthroscopic treatment including subacromial decompression and spur removal below the distal clavicle. Three years following surgery, he now reports that the pain has returned. What is the most likely cause of his pain?
Explanation
Co-planing the distal clavicle may lead to painful acromioclavicular joints in up to 35% of patients; this is felt to be related to destabilizing the distal clavicle. Intra-articular diagnosis of synovitis, degenerative joint disease, and superior labrum anterior and posterior lesions would have been identified at initial arthroscopy (not necessarily seen in open surgery). Ganglions are seen on MRI. Fischer BW, Gross RM, McCarthy JA: Incidence of acromioclavicular joint complications after arthroscopic subacromial decompression. Arthroscopy 1999;15:241-248. Hazel RM, Tasto JP, Klassen J: Arthroscopic subacromial decompression: A 9-year follow-up. Arthroscopy 1998;14:419.
Question 79
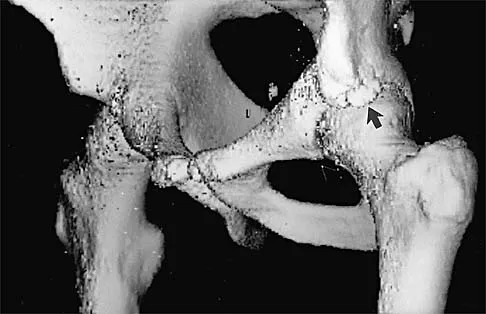
Figure 33 shows the radiograph of a 28-year-old avid golfer who has chronic right wrist pain. Management should consist of
Explanation
The patient's chronic symptoms are associated with a fracture of the base of the hook of the hamate; therefore, the treatment of choice is simple excision of the fracture fragment, with reasonable expectations of functional return. Acute fractures may be difficult to treat because of the high incidence of nonunion, but once nonunion is discovered, nonsurgical management usually is unsuccessful. Bone grafting may be a surgical alternative, but successful outcomes with percutaneous fixation or trephination of the fibrous union have not been reported. Geissler WB: Carpal fractures in athletes. Clin Sports Med 2001;20:167-188.
Question 80
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 81
Which of the following best describes athletic pubalgia?
Explanation
Athletic pubalgia refers to a distinct syndrome of lower abdominal and adductor pain that is mostly commonly seen in high performance male athletes. This condition must be distinguished from others such as painful inflammation of the symphysis pubis, referred to as osteitis pubis. Symptoms attributable to the iliopsoas tendon are most commonly associated with snapping of the tendon. Stress fracture of the pubic ramus may cause symptoms in this area, but it is usually confirmed by imaging studies. Neurapraxia of the pudendal nerve is associated with pressure from the seat in cycling sports and also as a complication associated with traction during surgical procedures. Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Question 82
Figures 34a and 34b show the radiographs of a 28-year-old man who fell on his outstretched arm with significant force while mountain biking. The nerve deficit most likely to occur would result in weakness of

Explanation
34b The patient has a Monteggia fracture-dislocation (proximal ulnar fracture and radial head dislocation). The posterior interosseous nerve branch of the radial nerve is the most likely to be injured and could result in weakness of thumb extension and finger metacarpal extension. Considerably less likely are injuries to the more proximal radial nerve branches supplying the extensor carpi radialis longus and brevis, resulting in weak wrist extension; the ulnar nerve supplying the digital intrinsics, resulting in weak finger abduction; the anterior interosseous branch of the median nerve, resulting in weakness of the flexor pollicis longus; and the distal median nerve, resulting in weakness of thumb opposition. Bado JL: The Monteggia lesion. Clin Orthop 1967;50:71-86.
Question 83
Which of the following activities can improve posterior capsular contractures?
Explanation
Posterior capsule stretching is performed in the cross-chest and behind the back positions. Stretching in internal rotation in the abducted shoulder will further stretch the posterior capsule. Wide grip stretch, and anterior capsule and strengthening exercises will not necessarily stretch the capsule. Ellenbacher TS: Shoulder internal and external rotation strength and range of motion of highly-skilled junior tennis players. Isokinetic Exercise Sci 1992;2:1-8.
Question 84
Figure 35 shows the radiograph of a 35-year-old weightlifter who has had pain with overhead lifts for the past 7 months. Cortisone injections in the acromioclavicular joint provided only temporary relief. A bone scan reveals increased activity of the acromioclavicular joint. Treatment should now consist of

Explanation
Osteolysis of the distal clavicle is common in weightlifters; therefore, distal clavicle excision is the treatment of choice. A subacromial decompression alone would not alleviate the acromioclavicular joint symptoms. Interval closure, biceps degeneration, and superior labrum anterior and posterior repair would limit superior migration but would not explain the abnormal bone scan. Thermal capsular shrinkage does not have a role here. Flatow EL, Cordasco FA, McCluskey GM, Bigliani LU: Arthroscopic resection of the distal clavicle via a superior portal: A critical quantitative radiographic assessment of bone removal. Arthroscopy 1990;6:153-154.
Question 85
Following reconstruction of the anterior cruciate ligament (ACL), which of the following rehabilitation exercises has the greatest potential to harm the graft?
Explanation
Isometric quadriceps contraction between 15 and 30 degrees of flexion creates significant strain in the ACL and potential damage to the reconstructed graft. Isolated quadriceps contraction with knee flexion of greater than 60 degrees, hamstring contraction at any angle of knee flexion, and active knee motion between 35 and 90 degrees of flexion create substantially less strain in the properly implanted ACL graft. Beynnon BD, Gleming BC, Johnson RL, Nichols CE, Renstrom PA, Pope MH: Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. Am J Sports Med 1995;23:24-34.
Question 86
A young active patient with a complete isolated posterior cruciate ligament (PCL) tear undergoes a double bundle PCL reconstruction. The tensioning pattern of the anterolateral (AL) and posteromedial (PM) bundles most likely to reproduce the most normal knee kinematics would be to tension
Explanation
During flexion and extension of the normal knee, the AL bundle of the PCL is taut in flexion, and the PM bundle is taut when the knee is near extension. The AL bundle is approximately two times larger at its midsubstance, stiffer, and has a higher ultimate load than the PM bundle. In vitro testing has demonstrated that by tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 0 degrees of flexion, essentially normal knee kinematics are restored. Tensioning the AL bundle at 45 degrees of flexion and the PM bundle at 0 degrees of flexion would result in increased laxity with flexion at 90+ degrees. Tensioning the AL bundle at 90 degrees of flexion and the PM bundle at 45 degrees of flexion would result in increased laxity near extension. Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin T, Woo SL: Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med 2000;28:144-151.
Question 87
Accurate evaluation of the upper portion of the subscapularis muscle is best accomplished with active internal rotation
Explanation
Internal rotators of the shoulder include the subscapularis, pectoralis major, teres major, and latissimus dorsi muscles. The subscapularis has two portions, with the upper portion receiving its innervation from the upper subscapular nerve (C5) and the lower portion from the lower subscapular nerve (C5-6). The two tests commonly performed to isolate the internal rotation to the subscapularis muscle are the lift-off test and the belly press test. Electromyographic findings have shown the lift-off test to be more accurate for the lower portion of the subscapularis and the belly press test to be more sensitive for the upper portion. Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ: Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med 1998;26:210-220.
Question 88
During what phase of the throwing motion is the highest torque measured across the glenohumeral joint?
Explanation
Electromyography is used to evaluate muscular firing patterns about the shoulder during the throwing sequence. The rotator cuff muscles and biceps are relatively inactive during the acceleration phase, whereas the pectoralis major, serratus anterior, latissimus dorsi, and subscapularis show highest activity. By contrast, deceleration is accomplished by the rotator cuff musculature and the larger trunk muscles acting in concert to slow down the arm. It is during this phase of follow through that the highest torque is measured secondary to eccentric muscle contraction. Jobe FW, Moynes DR, Tibone JE, Perry J: An EMG analysis of the shoulder in pitching: A second report. Am J Sports Med 1984;12:218-220. Pappas AM, Zawacki RM, Sulliva TJ: Biomechanics of baseball pitching: A preliminary report. Am J Sports Med 1985;13:216-222.
Question 89
Figure 36 shows the radiograph of a 28-year-old man who injured his shoulder in a motocross race. Management should consist of

Explanation
Fractures of the distal one third of the clavicle have a high incidence of delayed union (45% to 67%) and nonunion (22% to 33%) with nonsurgical management. Surgical stabilization with tension band techniques or a combination of plate and screw techniques is indicated, especially in young, active patients. In this patient, significant displacement of the fracture implies injury to the coracoclavicular ligaments with a higher risk of delayed union or nonunion. Various surgical treatments have been recommended, but the use of smooth wires is not indicated because of the potential for hardware migration. Jupiter JB, Ring D: Fractures of the clavicle, in Ianotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott, Williams and Wilkins, 1999, pp 709-736.
Question 90
Figure 37 shows the radiograph of a 21-year-old collegiate basketball player who has had mild midfoot aching for the past 4 months. What is the best course of action?

Explanation
A stress fracture of the navicular is considered a high-risk injury because of the incidence of nonunion. If identified early, cast immobilization with no weight bearing is appropriate. However, this patient is a high-caliber athlete who has had symptoms for 4 months. Therefore, surgery is recommended to expedite recovery and optimize the chance of healing. Meyer SA, Saltaman CL, Albright JP: Stress fractures of the foot and ankle. Clin Sports Med 1993;12:395-413. Kahn JM, Fuller PJ, Burkner PD, et al: Outcome of conservative and surgical management of navicular stress fractures in athletes: Eighty-six cases proven with computerized tomography. Am J Sports Med 1992;20:657-666.
Question 91
A 17-year-old high school gymnast who has peripatellar knee pain has been unable to practice on a consistent basis for the past 3 years. She denies any specific injury events. Physical therapy for modalities, quadriceps strengthening, and hamstring stretching provide temporary relief. A trial of patellar taping significantly reduces her pain. Examination reveals an 15-degree Q angle, moderate lateral facet tenderness, negative patellar apprehension, and the inability to evert the patella. Radiographs show a moderate lateral patellar tilt. Treatment should now consist of
Explanation
The patient has patellofemoral stress and a tight lateral retinaculum that has failed to respond to nonsurgical management; therefore, the most appropriate treatment includes an arthroscopic lateral retinacular release. A patellar restraining brace may aggravate the peripatellar pain by increasing pressure on the lateral facet. There is no evidence of patellar instability or significant malalignment; therefore, medial retinacular repair or a tibial tubercle transfer is not indicated. A modified Maquet tibial tubercle elevation would be considered only for significant patellofemoral arthrosis. Gambardella RA: Techical pitfalls of patellofemoral surgery. Clin Sports Med 1999;18:897-903.
Question 92
An active 55-year-old man who felt a sudden pop in the left heel while playing tennis 6 months ago was diagnosed with an ankle sprain around the time of injury. He now reports calf atrophy and severe weakness with running. Examination reveals a palpable defect in the Achilles tendon and only trace passive ankle flexion when the calf is squeezed. At the time of surgery, an Achilles tendon defect of 6 cm cannot be approximated. Surgical management of the Achilles tendon should include
Explanation
Chronic or neglected Achilles tendon ruptures can present a surgical problem. Ideally, end-to-end apposition of tendon should be attempted, but this should be accomplished without placing the foot in marked equinus. A defect of greater than 5 cm requires the use of a tendon transfer either alone or in combination with a V-Y advancement of the gastrocnemius. Because of its proximity to the Achilles tendon and its strength as a plantar flexor, the flexor hallucis longus is an ideal choice for this task. Studies have shown that early active range-of-motion exercises after an Achilles tendon repair is beneficial for tendon healing and improved clinical outcomes. Myerson M: Achilles tendon ruptures. Instr Course Lect 1999;48:219-230.
Question 93
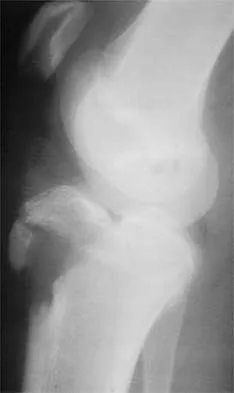
Figures 38a and 38b show the AP and lateral radiographs of a 12-year-old baseball pitcher who has pain in his right dominant elbow. Management should consist of
Explanation
38b The patient has a stress fracture of the olecranon; therefore, the most appropriate management is modification of activities below the threshold of symptoms to allow for healing. Ultrasound provides no benefit, and immobilization is not necessary. MRI is not necessary because there is no associated ligamentous injury. Arthroscopy is not indicated. Cabanela ME, Morrey BF: Fractures of the olecranon, in Morrey BF (ed): The Elbow and Its Disorders. Philadelphia, PA, WB Saunders, 2000, pp 365-379.
Question 94
What is the most reproducible landmark for the accurate anatomic placement of the tibial tunnel for an anterior cruciate ligament (ACL) reconstruction?
Explanation
The anterior border of the PCL is the most accurate and reproducible landmark for appropriate placement of the tibial tunnel for an ACL reconstruction. The central sagittal insertion point of the ACL is consistently 10 to 11 mm anterior to the anterior border of the PCL ligament. The anterior border of the tibia is not well visualized and does not serve as a reference point. While the posterior border of the anterior horn of the lateral meniscus could be used as a reference point, it has twice the variability of the PCL reference point. The posterior border of the tibia is difficult to identify and has greater variability than the PCL relative to the AP dimension of the proximal tibial surface. The anterior horn of the medial meniscus is also more variable than the PCL. Hutchinson MR, Bae TS: Reproducibility of anatomic tibial landmarks for anterior cruciate ligament reconstructions. Am J Sports Med 2001;29:777-780.
Question 95
A 20-year-old football player sustains a dorsiflexion external rotation injury to his right ankle. During sideline evaluation, which of the following findings best indicates a syndesmosis ankle sprain without diastasis?
Explanation
The inability to single leg hop is considered the best indicator of a syndesmosis ankle sprain without diastasis. Tenderness along the syndesmosis, the deltoid, or over the anterior talofibular ligament or anterior distal tibia/fibula may present later, following the initial injury. The squeeze test and tenderness with dorsiflexion and external rotation may be positive but often are not present initially. The best determinant for prediction of return to play is the amount of tenderness along the syndesmosis, measured from the distal fibula up the syndesmosis. Nussbaum ED, Hosea TM, et al: Prospective evaluation of syndesmosis ankle sprains without diastasis. Am J Sports Med 2001;29:31-35. Miller CD, Shelton WR, Barrett GR, et al: Deltoid and syndesmosis ligament injury of the ankle without fracture. Am J Sports Med 1985;23:746-750.
Question 96
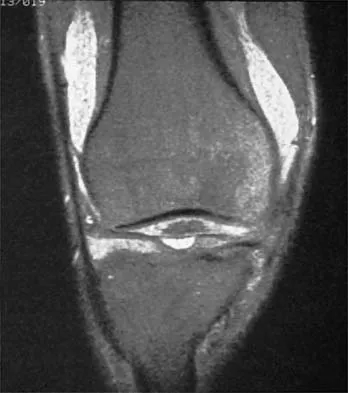
A 20-year-old college baseball pitcher reports the insidious onset of medial elbow pain. Examination reveals medial elbow tenderness, a normal neurologic examination, and no obvious valgus laxity. Plain radiographs are normal. MRI scans are shown in Figures 39a and 39b. Management should consist of


Explanation
39b Throwers and in particular, pitchers, are prone to high valgus loads to the elbow. A constellation of medial elbow pathology can develop, including medial epicondylitis, ulnar nerve neuritis, medial ulnar collateral ligament injuries, and posteromedial osteophytes of the olecranon. The MRI scans show significant increases in signal intensing as well as fiber disruption of the medial collateral ligament, indicating a complete tear. The common flexor origin shows a homogeneous signal and normal morphology. Therefore, excision of posterior osteophytes and debridement of the common flexor origin are not indicated. Likewise, this patient's symptoms do not indicate ulnar nerve pathology; therefore ulnar nerve transposition is not indicated. Primary repair of medial collateral ligament tears of the elbow lead to unpredictable results with an unacceptable rate of reoperation. The most predictable result in treating this high-demand athlete is reconstruction of the medial collateral ligament with autogenous tissue. Norris TR (ed): Athletic Injuries of the Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 311-323.
Question 97
What is the most common arthroscopic finding of internal impingement in an overhead athlete?
Explanation
Internal impingement occurs when the articular side of the supraspinatus abrades against the posterior superior glenoid in the cocking position. Damage may include a posterior labral tear where the contact occurs, not anteriorly as in a Bankart lesion. Biceps fraying and acromion spurs are more commonly seen in extrinsic impingement. Loose bodies may occur from multiple lesions associated with instability and articular cartilage disorders but are uncommon in internal impingement. Jobe CM: Posterior superior impingement of the rotator cuff on the glenoid rim as a cause of shoulder pain in the overhead athlete. Arthroscopy 1993;9:697-699.
Question 98
A 16-year-old high school football player who sustained an acute forceful dorsiflexion ankle injury reported that he felt a pop and then noted immediate swelling over the lateral malleolus. Examination 24 hours later reveals moderate swelling and tenderness along the lateral malleolus. The external rotation, squeeze, anterior drawer, and talar tilt tests are negative. Subluxation of the peroneal tendons is palpable over the peroneal groove of the fibula. Radiographs reveal a small cortical avulsion off the distal rim of the fibula. The stress views show no instability. Initial management for this injury should include
Explanation
The patient has an acute peroneal tendon dislocation. The evaluation for syndesmotic injury and lateral ankle instability is negative. The cortical avulsion off the distal tip of the lateral malleolus, a rim fracture, is characteristic of peroneal tendon dislocations. The sensation of apprehension or frank subluxation of the peroneal tendons with active dorsiflexion of the foot while the foot is held in plantar flexion confirms the diagnosis. Based on these findings, initial management should consist of cast immobilization and protected weight bearing. If a recurrent or chronic condition develops, surgery is the most reliable treatment option. Arrowsmith SR, Fleming LL, Allman FL: Traumatic dislocations of the peroneal tendons. Am J Sports Med 1983;11:142-146.
Question 99
The essential lesion responsible for posterolateral rotatory instability of the elbow is disruption of the
Explanation
Posterolateral rotatory instability (PLRI) of the elbow represents a three-dimensional injury pattern of rotational displacement of the ulna from the trochlea and the radius from the capitellum. The ulna supinates (externally rotates) past its normal limit and the radiocapitellar joint subluxates posterolaterally, permitting the coronoid process to slide beneath the trochlea. In cadaver studies, the lateral ulnar collateral ligament has been shown to be the essential lesion responsible for PLRI. The medial collateral ligament (of which the anterior bundle is the most important) is the primary restraint to valgus instability. The posterolateral capsule and radial collateral ligament may be disrupted in a complete posterolateral dislocation but are not essential injuries for PLRI. The primary function of the annular ligament is to stabilize the proximal radioulnar joint. O'Driscoll SW, Jupiter JB, King GJW, Hotchkiss RN, Morrey BF: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738. Olsen BS, Sojbjerg JO, Dalstra M, Sneppen O: Kinematics of the lateral constraints of the elbow. J Shoulder Elbow Surg 1996;5:333-341.
Question 100
When evaluating articular cartilage, what extracellular matrix component is most closely associated with the deep calcified cartilage zone?
Explanation
Collagen type X is produced only by hypertrophic chondrocytes during enchondral ossification (growth plate, fracture callus, heterotopic ossification) and is associated with calcification of cartilage in the deep zone of articular cartilage. Collagen type I is the predominant collagen in bone, ligament, and tendon. Collagen type II is the predominant collagen in articular cartilage. Proteoglycan aggrecan and hyaluronic acid are components of the extracellular matrix and are involved in the compressive strength characteristics of articular cartilage. Buckwalter JA, Mankin HJ: Articular cartilage: Tissue design and chondrocyte matrix interactions. Instr Course Lect 1998;47:477-486.
Finish Exam?
You cannot change answers after submitting.
