Question 51
A 32-year-old amateur bowler has progressive pain in the lateral aspect of the proximal forearm and elbow. Nonsurgical management consisting of a tennis elbow brace, nonsteroidal anti-inflammatory drugs, and activity modification has failed to provide relief. Examination reveals tenderness in the lateral aspect of the proximal forearm and exacerbation of symptoms with resisted finger extension. Radiographs of the elbow reveal no abnormalities. Which of the following studies will aid in diagnosis?
Explanation
It is often difficult to accurately discern between lateral epicondylitis and radial tunnel syndrome. Neither MRI nor a bone scan is likely to reveal abnormalities. Electrodiagnostic studies are often inconclusive, and radial tunnel syndrome often presents without motor weakness. The symptoms of radial tunnel syndrome are expected to improve with an injection of lidocaine into the radial tunnel; therefore, this is the test of choice in this clinical scenario. Radiographs of the wrist will not assist in making the diagnosis. Eversmann WW Jr: Entrapment and compression neuropathies, in Green DP (ed): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingston, 1993, pp 1341-1385.
Question 52
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
Failure of the scalene block, necessitating general anesthesia or the immediate administration of narcotic medications, is the most common complication, occurring in 3% to 18% of patients. Cardiac arrest or cardiovascular collapse has been reported in anecdotal occurrences. Seizure that is the result of intravascular injection of local anesthetic is a rare complication, with an incidence reported of 0% to 6%. Neurologic complications, including laryngeal and phrenic nerve injuries, are rare although parathesias lasting up to 2 weeks have been reported in up to 3% of patients. Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Question 53
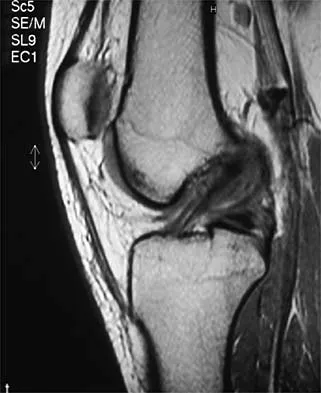
Figure 22 shows the MRI scan of a 20-year-old female basketball player who has pain over the anterior knee that interferes with her performance. Examination reveals phase III Blazina patellar tendinosis. Management should consist of

Explanation
Excision of the affected mucoid degenerative area is considered appropriate management in the Blazina classification system. A finding of phase III indicates persistent pain with or without activities, as well as deterioration of performance. With the appearance of the mucoid degeneration and the vigorous activity level of the intercollegiate basketball player, it is unlikely that nonsurgical management will provide adequate relief. When excising the affected degenerative area, care must be taken to retain normal tendon fibers. The defect in the patellar tendon is closed with absorbable sutures, as is the paratenon. Postoperative rehabilitation involves initial mobilization extension, with progressive range-of-motion and mobilization exercises as tolerated and weight bearing as tolerated. Open chain and isokinetic exercises are delayed until full range of motion and mobility is obtained, generally within 4 weeks. A return to activities is achieved by 80% to 90% of athletes, although there may be occasional activity-related aching for 4 to 6 months after surgery. Blazina ME, et al: Jumper's knee. Orthop Clin North Am 1973;4:665. Kelly DW, Carter VS, Jobe FW, Kerlan RK: Patellar and quadriceps tendon ruptures: Jumper's knee. Am J Sports Med 1984;12:375-380. Krums PE, Ryder B: Operative treatment of patella tendon disorders. Operative Techniques Sports Med 1994;2:303.
Question 54
When comparing the failure load of an evenly tensioned four-stranded hamstring tendon anterior cruciate ligament autograft to a 10-mm bone-patellar tendon-bone autograft, the hamstring graft will fail at a tension
Explanation
The failure load of an evenly tensioned four-stranded hamstring tendon autograft has been reported to be 4,500 Newtons. The failure load of a 10-mm patellar tendon autograft has been estimated at 2,600 Newtons. The intact anterior cruciate ligament failure load has been calculated at 1,725 Newtons. Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA: Arthroscopic reconstruction of the anterior cruciate ligament: A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:448-454. Hamner DL, Brown CH Jr, Steiner ME, et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Question 55
What pathology is most likely to result in failure of an arthroscopic Bankart repair?
Explanation
Recent studies have documented that an arthroscopic Bankart repair performed with good technique can produce success rates similar to an open repair. However, the results of an arthroscopic repair deteriorate significantly if there is a 25% or greater anterior-inferior glenoid rim defect (inverted pear configuration) or an engaging Hill-Sachs lesion in which the humeral head defect keys onto the glenoid rim in abduction and external rotation. If either of these entities exist or there is multidirectional instability with pathologic hyperextensible tissue laxity, an open repair is recommended. An associated SLAP lesion would not significantly affect the result of the Bankart procedure. Not infrequently, the anterior glenoid labrum is partially or completely disrupted and, in itself, is not a contraindication to arthroscopic Bankart repair. In almost all patients with predominantly unidirectional instability, some degree of capsular/anterior-inferior glenohumeral ligament attenuation is present and can be addressed during the arthroscopic repair. Burkhart SS, De Beer JF: Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.
Question 56
A 37-year-old man has had isolated chronic knee swelling for the past 6 months. He denies any history of specific trauma. Examination reveals a large effusion with a stable knee, but the remainder of the examination is normal. Plain radiographs are unremarkable. An MRI scan reveals a large effusion without meniscal injury. An arthroscopic image of the suprapatellar pouch is shown in Figure 23. What is the most likely diagnosis?

Explanation
The history and physical examination are consistent with a monoarticular joint condition but not typical of joint sepsis. The arthroscopic appearance of brownish proliferative synovium is typical of PVNS. PVNS is a monoarticular synovial disease of unknown etiology and is treated with total synovectomy. The proliferative synovitis is not consistent with chondromalacia. Synovial cell sarcoma is an extracapsular disease. Rheumatoid arthritis typically is polyarticular, and the synovial appearance is not associated with hemosiderin deposition. Flandry FC, Hughston JC, Jacobson KE, Barrack RL, McCann SB, Kurtz DM: Surgical treatment of diffuse pigmented villonodular synovitis of the knee. Clin Orthop 1994;300:183-192.
Question 57
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
Subscapularis tears can be associated with disruption of the transverse ligament supporting the biceps. The remaining aspects of the rotator cuff, superior labrum, and capsule can be intact with this injury. Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Question 58
An 18-year-old hockey player sustains an acute anterior shoulder dislocation that requires manual reduction. At arthroscopy, the lesion shown in Figure 24 will be observed in what percent of patients?

Explanation
The clinical photograph shows an acute capsulolabral avulsion from the anterior glenoid, also referred to as a Perthes-Bankart lesion. In patients who sustain an acute dislocation that requires a manual reduction, this pathologic lesion is observed with high frequency. In several research studies, it has been visualized in 80% to 95% of patients at arthroscopy. Taylor DC, Arciero RA: Pathologic changes associated with shoulder dislocations: Arthroscopic and physical examination findings in first-time, traumatic anterior dislocations. Am J Sports Med 1997;25:306-311.
Question 59
A 22-year-old competitive volleyball player has shoulder pain, and rest and a cortisone injection have failed to provide relief. Examination reveals atrophy along the posterior scapula, but an MRI scan does not reveal a rotator cuff tear or labral cyst. What is the most likely cause for the shoulder weakness?
Explanation
Repetitive overhead slams and serves may produce a traction injury to the distal branch of the suprascapular nerve. Bankart, biceps, and superior labrum anterior and posterior injuries can occur but usually do not produce visible atrophy. Muscle avulsion is uncommon. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 60
An 11-year-old female gymnast has had gradually increasing right wrist pain for the past 6 months. Examination reveals normal range of motion and strength. Moderate tenderness is present over the distal radius. AP radiographs will most likely show
Explanation
Distal radial physeal stress syndrome has been reported in up to 25% of nonelite gymnasts showing premature closure of the distal radial physis and distal ulnar overgrowth, producing positive ulnar variance. The diagnosis should be suspected when there is tenderness at the distal radial physis in a young gymnast. The pathology is thought to be the result of repetitive compressive stresses caused by upper extremity weight-bearing forces. The recommended treatment is 3 to 6 months of rest. Salter-Harris fractures with a distal radial epiphyseal slip are unlikely, especially in the absence of a specific traumatic event. Mandelbaum BR, Bartolozzi AR, Davis CA, Teurlings L, Bragonier B: Wrist pain syndrome in the gymnast: Pathogenetic, diagnostic, and therapeutic consideration. Am J Sports Med 1989;17:305-317.
Question 61
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
Postoperative subscapularis detachment can be identified with a positive lift-off test that reveals weakness in internal rotation. This complication does not necessarily compromise the anterior capsule repair. The load-and-sift maneuver and articular contrast studies may be normal. Supraspinatus tests for impingement and weakness should be negative. Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Question 62
Figures 25a and 25b show the clinical photographs of a 19-year-old baseball outfielder who has shoulder pain after sliding headfirst into second base. He reports pain while batting, sliding, and catching. Examination reveals a posterior prominence during midranges of forward elevation, which then disappears with a palpable clunk during terminal elevation and abduction. What is the most likely diagnosis?

Explanation
25b A headfirst slide with the arm extended can injure the posterior shoulder. Winging of the scapula is dynamic and is considered a compensatory effort to prevent subluxation; it is not related to nerve injury. Posterior glenohumeral subluxation can be present during the initiation of a bat swing. Rotator cuff function, interval tears, and superior labrum tears can be painful but do not produce winging. Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Question 63
A soccer player who sustained a twisting injury to the right ankle while making a cut is unable to bear weight and has diffuse tenderness over the anterior and lateral aspects of the ankle. Examination also shows a positive squeeze test. Plain radiographs and a stress radiograph are shown in Figures 26a through 26c. Radiographs of the leg and knee are normal. What is the most appropriate management?


Explanation
26b 26c The mechanism of injury, physical examination, and radiographs indicate a "high" ankle sprain with disruption of the distal tibiofibular ligaments and interosseous membrane. These injuries typically involve pronation and external rotation forces. In addition, recovery is significantly delayed, often requiring 6 to 8 weeks to heal. Radiographs obtained months after recovery often show calcification within the distal syndesmosis, which is not typically symptomatic. This patient has gross instability, resulting in a high incidence of chronic diastasis and subluxation leading to impaired function. Treatment should consist of reduction and stabilization with a transsyndesmotic screw because this injury demonstrates a widened syndesmosis. Boytim MJ, Fisher DA, Neumann L: Syndesmotic ankle sprains. Am J Sports Med 1991;19:294-298.
Question 64
When compared with the normal anterior cruciate ligament (ACL), placement of an anterior cruciate ligament graft in the over-the-top position on the femoral side has what effect on its function?
Explanation
The placement of ACL graft with respect to its femoral and tibial attachments has a significant effect on its function. Evidence has shown that if the graft is placed in the over-the-top position, the graft will become lax in flexion and more taut with extension. Conversely, if the graft is placed too anterior on the femoral side, it will tighten in flexion and become lax in extension. Azar FM: Revision anterior cruciate ligament reconstruction. Instr Course Lect 2002;51:335-342. Draganich LF, Hsieh YF, Sherwin SH, et al: Intra-articular anterior cruciate ligament graft placement on the average most isometric line on the femur: Does it reproducibly restore knee kinematics? Am J Sports Med 1999;27:329-334.
Question 65
An 11-year-old boy has right shoulder pain and has been unwilling to use the arm after throwing a baseball in a Little League game 3 weeks ago. Examination reveals upper arm and shoulder tenderness with swelling. A radiograph and MRI scan are shown in Figures 27a and 27b. Management should consist of


Explanation
27b The radiograph is consistent with a unicameral (simple) bone cyst. The MRI scan reveals that the cyst is juxtaposed to the physis and therefore can be classified as active (latent cysts are more than 1 cm away from the physis). Active cysts are treated with aspiration and steroid injection, although repeated injections may be necessary. Curettage and bone grafting results in more reliable healing but may lead to growth arrest in active cysts. Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 945-946.
Question 66
A 37-year-old recreational tennis player undergoes surgery for tennis elbow. Following surgery, she describes clicking and popping on the lateral aspect of the elbow. A lateral pivot shift test is positive. What is the most likely cause of her symptoms?
Explanation
The patient has a posterolateral rotatory instability (PLRI) of the elbow that is most likely the result of iatrogenic injury to the lateral ulnar collateral ligament, the main ligament implicated in PLRI. The anterior band of the medial collateral ligament is implicated in valgus instability. Injury to the radial nerve is unlikely, and the lateral radial collateral ligament makes less of a contribution to elbow stability than does the ulnar component. While the origin of the extensor carpi radialis brevis may contribute to elbow stability, it is not as important a stabilizer as the lateral ulnohumeral ligament. O'Driscoll SW, Morrey BF: Surgical reconstruction of the lateral collateral ligament, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 169-182.
Question 67
An 18-year-old football halfback reports that he had immediate right knee pain after being tackled 1 week ago. Examination now reveals moderate tenderness over the proximal medial tibia and lateral joint and normal cruciate stability. In evaluating the integrity of the posterolateral knee structures, what is the most reliable examination finding?
Explanation
The most reliable test for a relatively isolated posterolateral complex (PLC) injury is the asymmetric tibial external rotation or "dial test." It can be performed with the patient prone or supine. When greater than 10 degrees of external rotation at 30 degrees of flexion is present when compared with the opposite knee, it indicates significant damage to the posterolateral structures. Asymmetric external rotation, which is also present at 90 degrees of flexion, indicates injury to the posterior cruciate ligament (PCL) as well. Varus laxity may indicate significant damage to both the PLC and PCL. Approximately 35% of the normal population may have a reverse pivot shift when examined under anesthesia; therefore, it is considered a less specific test. The external rotation/recurvatum and posterolateral drawer tests are adjunctive in assessing isolated posterolateral laxity but are not thought to be as reliable. Veltri DM, Warren RF: Isolated and combined posterior cruciate injuries. J Am Acad Orthop Surg 1993;1:67-75.
Question 68
Figures 28a through 28d show the radiographs and MRI scans of a 20-year-old basketball player who sustained an inversion injury to his right ankle. Management should consist of



Explanation
28b 28c 28d Osteochondral fractures involving the talar dome have been classified based on radiographic and MRI findings. A nondisplaced and incomplete fracture may be treated effectively with a short leg cast and no weight bearing for 6 weeks. This patient has a complete, separated, and displaced osteochondral fragment involving the midlateral talar dome that will most likely cause pain, mechanical symptoms, and effusion if treated nonsurgically. In addition, there is very little bone remaining on the fragment, making the likelihood of healing with open reduction and internal fixation problematic. The treatment of choice includes arthroscopy, removal of the loose fragment, curettage or drilling of the base, and a rehabilitation program that emphasizes peroneal strengthening, range of motion, and proprioceptive training. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Question 69
A 19-year-old rugby player has severe knee pain after being injured in a game 2 weeks ago. Examination reveals a knee effusion, limited motion, and increased 3+ Lachman's test and anterior drawer. There is also increased external rotation at 30 degrees of knee flexion when the patient is placed in the prone position. Based on these findings, which of the following actions would most likely increase the risk of anterior cruciate ligament (ACL) reconstruction failure?
Explanation
The patient has a combined ACL and posterolateral corner injury. Failure to diagnose and treat an injury of the posterolateral corner in a patient who has a tear of the anterior or posterior cruciate ligament can result in failure of the reconstructed cruciate ligament. The tibial external rotation test is best performed with the patient in the prone position. A 10-degree side-to-side difference of external rotation at 30 degrees of knee flexion indicates injury to the posterolateral corner. Acute grade III isolated or combined injuries of the posterolateral corner are best treated early by direct repair or by augmentation or reconstruction of all injured ligaments. Postoperative arthrofibrosis after an ACL reconstruction has been observed with preoperative deficiencies of knee motion. Veltri DM, Warren RF: Posterolateral instability of the knee. J Bone Joint Surg Am 1994;76:460-472.
Question 70
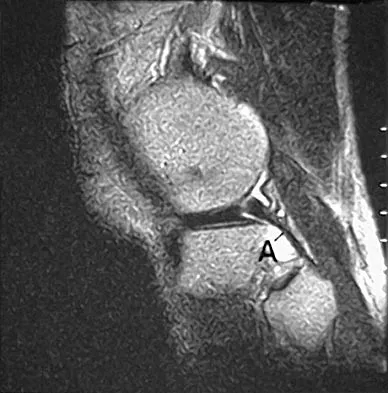
The primary function of structure "A" in Figure 29 is to limit
Explanation
The primary function of the popliteofibular ligament is to resist posterolateral rotation of the tibia on the femur, although it also secondarily resists varus angulation and posterior displacement of the tibia on the femur. The posterior cruciate ligament resists posterior tibial displacement, especially at 90 degrees of flexion. The lateral collateral ligament primarily resists varus displacement at 30 degrees of flexion but also resists posterolateral rotatory displacement with flexion that is less than approximately 50 degrees. The anterior and posterior cruciate ligaments resist varus displacement (along with the lateral collateral ligament) at 0 degrees of flexion. The anterior cruciate ligament primarily resists anterolateral displacement of the tibia on the femur. Sugita T, Amis AA: Anatomic and biomechanical study of the lateral collateral and popliteofibular ligaments. Am J Sports Med 2001;29:466-472.
Question 71
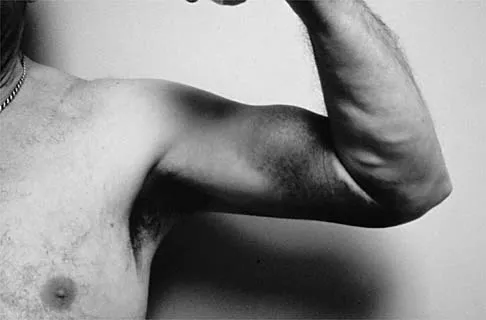
While lifting weights, a patient feels a pop in his arm. He has the deformity shown in Figure 30. If left untreated, the patient will have the greatest deficiency in

Explanation
The patient has a distal biceps rupture. While the distal biceps contributes to elbow flexion, its main function is forearm supination. Baker BE, Bierwagen D: Rupture of the distal tendon of the biceps brachii: Operative versus non-operative treatment. J Bone Joint Surg Am 1985;67:414-417. D'Arco P, Sitler M, Kelly J, et al: Clinical, functional, and radiographic assessments of the conventional and modified Boyd-Anderson surgical procedures for repair of distal biceps tendon ruptures. Am J Sports Med 1998;26:254-261.
Question 72
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
Passive stretching is contraindicated during rehabilitation as it may potentiate the severity of the myositis ossificans. Electrical stimulation, iontophoresis, isometric exercise, and ice/heat contrast are not known to exacerbate this process. Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Question 73
Which of the following symptoms are most commonly associated with piriformis syndrome?
Explanation
Piriformis syndrome is best characterized by localized posterior hip pain and radicular symptoms in the sciatic distribution because of compression of the piriformis muscle on the sciatic nerve. Weakness in hip extension is not a characteristic finding, nor is pain with hip abduction or flexion. Hypesthesia of the lateral thigh would be more characteristic of a lesion of the lateral femoral cutaneous nerve. Radiating medial thigh pain would suggest hip joint pathology or upper lumbar nerve root irritation. Weakness in internal rotation is not a characteristic feature, and hypesthesia of the perineum would suggest possible involvement of the pudendal nerve. Byrd JWT: Thigh, hip, and pelvis, in Miller MD, Cooper DE, Warner JJP (eds): Review of Sports Medicine and Arthroscopy, ed 2. Philadelphia, PA, WB Saunders, 2002, pp 114-139.
Question 74
A 19-year-old football player who sustained three traumatic anterior shoulder dislocations underwent surgery to repair a Bankart lesion. Nine months after surgery, examination reveals stability, elevation to 150 degrees, external rotation to 0 degrees with the elbow at his side and to 50 degrees at 90 degrees of abduction, and internal rotation to T12. If his range of motion does not improve, he is at most risk for
Explanation
Loss of external rotation can lead to degenerative joint disease following an anterior stabilization procedure. A tight anterior capsule will prevent internal impingement. Risk of thoracic outlet syndrome should not be increased. Subscapularis detachment is a risk following open anterior repair; however, a gain in external rotation would be noted. In time, this patient's shoulder may show increased posterior glenohumeral wear but should not have symptoms of recurrent subluxation unless multidirectional instability is present. Hawkins RJ, Angelo RL: Glenohumeral osteoarthrosis: A late complication of the Putti-Platt repair. J Bone Joint Surg Am 1990;72:1193-1197.
Question 75
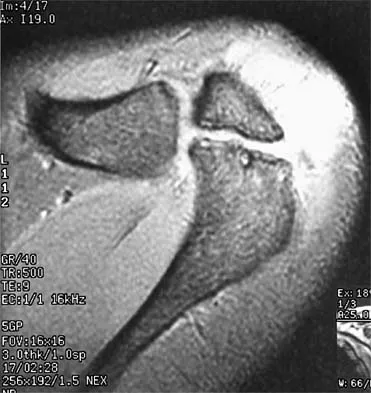
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of

Explanation
Subscapularis tendon tears are being recognized with increasing frequency, and the mechanism of injury involves hyperabduction and external rotation. The patient will have anterior shoulder pain and may report a sensation of instability. Examination will reveal anterior shoulder tenderness over the lesser tuberosity and bicipital groove, and the Gerber lift-off test usually is positive. The MRI scan shown here reveals an intact anterior labrum. The subscapularis tendon is avulsed and retracted, with no evidence of the biceps tendon within the groove; this implies dislocation of the biceps, a common accompanying feature of a subscapularis tear. This injury is also recognized as a complication after open anterior shoulder stabilizations where the subscapularis has been incised as part of the approach. Therefore, the appropriate management involves repair of the subscapularis. The injury does not represent a recurrence so immobilization or revision stabilization, which may be reasonable treatment for recurrent instability, is not indicated. The findings are not consistent with a superior labral tear. Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Finish Exam?
You cannot change answers after submitting.
