Question 51
Figure 24 shows the radiograph of a 10-year-old boy who sustained a valgus injury to the knee. Examination reveals grade III medial laxity. Initial management should consist of


Explanation
Based on the mechanism of injury and findings of medial laxity, the most likely diagnosis is injury to either the growth plate or the medial collateral ligament. With the open physeal plate, this area of injury is presumed present until proven otherwise; therefore, stress radiographs should be obtained before implementing any treatment or ordering more extensive and expensive tests. DeLee JC: Ligamentous injury of the knee, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, vol 3, pp 406-432. Clanton TO, DeLee JC, Sanders B, Neidre A: Knee ligament injuries in children. J Bone Joint Surg Am 1979;61:1195-1201.
Question 52
A right-handed 14-year-old pitcher has had a 3-month history of shoulder pain while pitching. Examination reveals full range of motion, a mildly positive impingement sign, pain with rotational movement, and no instability. Plain AP radiographs of both shoulders are shown in Figures 25a and 25b. Management should consist of




Explanation
25b The patient has the classic signs of Little Leaguer's shoulder, with findings that include pain localized to the proximal humerus during the act of throwing and radiographic evidence of widening of the proximal humeral physis. Examination usually reveals tenderness to palpation over the proximal humerus, but the presence of any swelling, weakness, atrophy, or loss of motion is unlikely. The treatment of choice is rest from throwing for at least 3 months, followed by a gradual return to pitching once the shoulder is asymptomatic. Carson WG Jr, Gasser SI: Little Leaguer's shoulder: A report of 23 cases. Am J Sports Med 1998;26:575-580.
Question 53
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
Several studies have identified a complete proximal avulsion of the hamstring muscles as an injury that leads to significant long-term disability, with a high percentage of athletes who must permanently restrict their activities following nonsurgical management. Early surgical repair and prolonged rehabilitation have yielded consistently better results than nonsurgical management. Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Question 54
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Explanation
Prepubescent athletes gain strength through neurogenic adaptations, including recruitment of motor units, reduced inhibition, and learned motor skills. Myogenic adaptations (muscle hypertrophy) occur after puberty and include increased contractile proteins, thickening of the connective tissue, and increased short-term energy sources such as creatine phosphate. Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Question 55
Following an episode of transient quadriplegia in contact sports, an athlete's return to play is absolutely contraindicated when
Explanation
Return to play decisions after traumatic spinal or spinal cord injury are not always clear-cut and often must be made on a patient-by-patient basis. The Torg ratio has been found to have low sensitivity in patients with large vertebral bodies. Abnormal electromyographic studies can persist in the face of normal function and do not define spinal injury. Duration of quadriplegia is not related to anatomic pathology. Findings on MRI scans or contrast-enhanced CT scans consistent with stenosis include lack of a significant cerebrospinal fluid signal around the cord, bony or ligament hypertrophy, or disk encroachment. Based on these findings, return to play should be avoided. Cantu RC, Bailes JE, Wilberger JE Jr: Guidelines for return to contact or collision sport after a cervical spine injury. Clin Sports Med 1998;17:137-146. Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ: Normal cervical spine morphometry and cervical stenosis in asymptomatic professional football players: Plain film radiography, multiplanar computer tomography, and magnetic resonance imaging. Spine 1991;16:178-186.
Question 56
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Explanation
Because there is a significant possibility that the patient may have a fracture of the lateral process of the talus, there is some disagreement as to the best radiographic study to identify this injury. A CT scan is an appropriate diagnostic tool to visualize the fracture and identify any displacement. Displaced lateral process fractures are best treated surgically. Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder's foot and ankle. Am J Sports Med 1998;26:271-277.
Question 57
A 24-year-old man who plays golf noted the immediate onset of pain on the ulnar side of his hand and has been unable to swing a club for the past 6 weeks after striking a tree root with his club during his golf swing. Examination reveals full motion of the wrist, diminished grip strength, and tenderness over the hypothenar region. A CT scan of the hand and wrist is shown in Figure 26. Management should consist of


Explanation
Fractures of the hook of the hamate frequently are not identified in the acute phase. Because the fracture can be difficult to see on plain radiographs, the lack of findings can lead to a painful nonunion. A carpal tunnel view may show the fracture, but a CT scan will best detect the injury. Immobilization is the treatment of choice and will result in union in most patients unless the diagnosis is delayed. However, excision of the fragment may be necessary for patients who have nonunion, persistent pain, or ulnar nerve palsy. Carroll RE, Lakin JF: Fracture of the hook of the hamate: Acute treatment. J Trauma 1993;34:803-805.
Question 58
An 18-year-old football player sustains a contact injury to his right lower leg, and radiographs show a closed transverse fracture of the middle third of the tibia. Based on the clinical examination, a compartment syndrome is suspected. When measuring compartment pressures, the highest tissue pressure is recorded how many centimeters proximal or distal to the fracture site?
Explanation
Measurements of compartment pressures in patients with tibial fractures and compartment syndrome reveal that the highest tissue pressures are recorded at the level of the fracture or within 5 cm of the fracture. Tissue pressures show a statistically significant decrease when they are recorded at increasing distances proximal and distal to the site of the highest pressure recorded. To reliably determine the location of the highest tissue pressure in patients with tibial fractures, measurements should be obtained, at a minimum, in both the anterior and deep posterior compartments at the level of the fracture, as well as at locations proximal and distal. The highest tissue pressure recorded should serve as a basis for determining the need for fasciotomy. Heckman MM, Whitesides TE Jr, Grewe SR, Rooks MD: Compartment pressure in association with closed tibial fractures: The relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am 1994;76:1285-1292.
Question 59
A 50-year-old patient who plays tennis sustained the deformity shown in Figure 27 following a high volley. Further diagnostic work-up should include
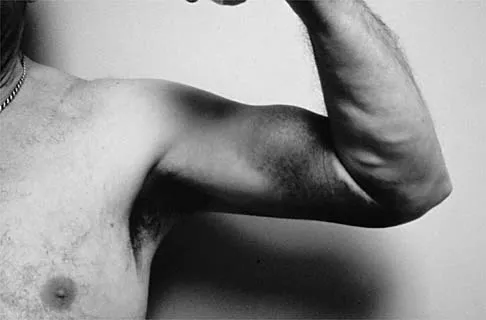

Explanation
The patient has a rupture of the long head of the biceps; however, patients older than age 45 years are at greater risk of having an associated rotator cuff tear. An MRI scan should be ordered to avoid missing concomitant rotator cuff pathology. While patients may report pain radiating down the arm at the time of the tendon rupture, an EMG is not indicated. The short head of the biceps is intact and needs no further work-up, even though the muscle descends in most cases. The anterior labrum can be injured but is not associated with this deformity. Neer CS II, Bigliani LU, Hawkins RJ: Rupture of the long head of the biceps related to the subacromial impingement. Orthop Trans 1977;1:114.
Question 60
A 16-year-old ice hockey player is struck on the chest by the puck. He skates a few strides and then collapses. What is the most likely diagnosis?
Explanation
Sudden cardiac arrest following a blow to the chest in young athletes has been termed "commotio cordis." It is most common in Little League and other youth projectile sports (eg, ice hockey, lacrosse). The cause, although not completely determined, is most likely an arrhythmia related to the impact in a vulnerable time in the cardiac cycle. Resuscitation has proven to be exceedingly difficult, resulting in a high mortality rate. Maron BJ, Strasburger JF, Kugler JD, Bell BM, Brodkey FD, Poliac LC: Survival following blunt chest impact-induced cardiac arrest during sports activities in young athletes. Am J Cardiol 1997;79:840-841.
Question 61
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of


Explanation
The patient has a moderately displaced distal diaphyseal fracture of the fifth metatarsal, and the most appropriate treatment is brief immobilization and symptomatic management. Attempts at closed reduction are unlikely to appreciably alter the position of the fracture. Surgical techniques for either reduction of the fracture or fixation have not been shown to result in improved functional outcomes. O'Malley MJ, Hamilton WG, Munyak J: Fractures of the distal shaft of the fifth metatarsal: "Dancer's Fracture." Am J Sports Med 1996;24:240-243. DeLee JC: Fractures and dislocations of the foot, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1465-1703.
Question 62
A 22-year-old volleyball player has atrophy of the infraspinatus muscle. This deficit is the result of entrapment of what nerve?
Explanation
Suprascapular deficits, as the result of repetitive forceful internal rotation with overhead ball striking, occur in the spinoglenoid notch. Compression interferes with distal suprascapular nerve innervation to the infraspinatus, while allowing the supraspinatus to function normally. A scapular notch entrapment of this nerve would involve both the supraspinatus and the infraspinatus. The axillary, dorsal scapular, and subscapular nerves do not affect the infraspinatus. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 63
Figure 29 shows the radiograph of a 25-year-old woman who has had a 3-month history of ankle pain after sustaining an inversion injury to the ankle. She reports occasional catching, but no sense of instability. Examination reveals ligament stability. Management should consist of


Explanation
Osteochondral lesions of the talar dome can have a traumatic or nontraumatic etiology. Most authors site a probable traumatic etiology for lateral lesions. Stage I and II lesions, which are composed of compressed subchondral bone or a partial detached osteochondral fragment, can be treated initially in a non-weight-bearing short leg cast for 6 weeks. Stage III medial lesions can also be treated in the same manner. If symptoms persist, the treament of choice is debridement of the fracture, curettage of the lesion, and drilling of the subchondral bone. This treatment also applies to lateral stage III and all stage IV lesions. If the fragment is at least one third of the size of the talar dome, management should consist of open reduction and internal fixation. In patients with more chronic lesions (4 to 6 months of persistent pain), the threshold to proceed with surgery is lower, even in a stage II lesion. Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 205-226.
Question 64
A 19-year-old college cross-country runner is amenorrheic and has recurrent stress fractures. Long-term management should consist of
Explanation
The triad of menstrual dysfunction, disordered eating, and stress fracture is well recognized in women who participate in endurance sports. The best treatment remains to be determined, but at present, the combination of oral contraceptives to regulate menses, an increased intake of calcium and vitamin D, as well as nutritional counseling, is the recommended treatment for decreased bone mass related to exercise-induced amenorrhea. Nattiv A, Armsey TD Jr: Stress injury to bone in the female athlete. Clin Sports Med 1997;16:197-224.
Question 65
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of



Explanation
30b The MRI scans show a mesoacromion with tendonopathy of the supraspinatus. The history and physical findings indicate that the patient has a symptomatic os acromiale. Simple excision of the unstable os acromiale has not yielded consistently good results. Meticulous internal fixation using tension banding with cannulated screws and autologous bone grafting has shown good results for this problem. Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Question 66
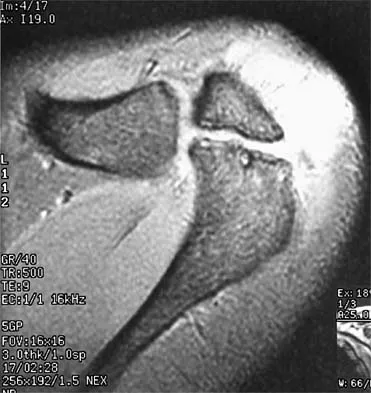
A 39-year-old competitive cyclist sustains an injury to her left hip in a fall. Gadolinium arthrography, with an accompanying MRI scan, is shown in Figure 31. A cleft, or defect, identified by the arrow, indicates a detachment of the


Explanation
The area indicated by the arrow represents gadolinium contrast extending into a separation between the lateral labrum and its acetabular attachment. This can be a traumatic detachment, but occasionally a cleft may be present as a normal variant of the labral morphology. The capsular attachment of the iliofemoral ligament is peripheral to the labrum. The pulvinar is the common name applied to the fat and overlying synovium contained within the acetabular fossa above the ligamentum teres. The zona orbicularis is a circumferential thickening of the capsule around the femoral neck, and the retinacular vessels travel within the capsular synovium up the femoral neck to supply the femoral head. Petersilge CA, Haque MA, Petersilge WJ, Lewin JS, Lieberman JM, Buly R: Acetabular labral tears: Evaluation with MR arthrography. Radiology 1996;200:231-235. Czerny C, Hofmann S, Neuhold A, et al: Lesions of the acetabular labrum: Accuracy of MR imaging and MR arthrography in detection and staging. Radiology 1996;200:225-230.
Question 67
A cortisone injection in the subacromial space will most likely result in
Explanation
A cortisone injection in the subacromial space will most likely result in elevated blood glucose levels in patients with type I diabetes mellitus. Patients should be warned of this potential complication. Cortisone does not have an effect on instability or proprioception, and a single injection would not affect osteoporosis. Repetitive injections or injection into the tendon itself could accelerate rupture of the biceps tendon. Matsen FA III, Arntz CT: Subacromial impingement, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 623-646.
Question 68
A high school athlete reports the sudden onset of low back pain while performing a dead lift. Examination reveals a lumbar paraspinal spasm and a positive straight leg raising test. The deep tendon reflexes, motor strength, and sensation in the lower extremeties are normal. The radiographs are normal. If symptoms persist for more than a few weeks, management should consist of
Explanation
In adolescents, a lumbar herniated disk is characterized by a paucity of clinical findings; a positive straight leg raising test may be the only consistent positive finding. This may result in a long period of nonsurgical management that fails to provide relief. Activities that place a significant shear load on the lumbar spine, such as the dead lift, are associated with an increased risk of central disk herniation. When an adolescent who lifts weights has a history of low back pain that fails to respond to a short period of active rest, an MRI scan is the study of choice to evaluate for a lumbar herniated disk. Epstein JA, Epstein NE, Marc J, Rosenthal AD, Lavine LS: Lumbar intervertebral disk herniation in teenage children: Recognition and management of associated anomalies. Spine 1984;9:427-432.
Question 69
A 22-year-old skier reports painful range of motion in the left thumb after falling forward on his outstretched hand while holding his ski pole. Examination of the left thumb reveals increased AP laxity and 45 degrees of valgus laxity at the metacarpophalangeal (MCP) joint. Examination of the right thumb shows 25 degrees of valgus laxity at the MCP joint. Radiographs are normal. Management should consist of
Explanation
The patient has a complete tear of the ulnar collateral ligament as defined by MCP joint laxity of greater than 30 degrees (or 15 degrees greater laxity compared with the opposite side). Primary repair is the treatment of choice because displacement of the ligament superficial to the adductor aponeurosis (Stener lesion) must be corrected. Any volar plate injury can be addressed during repair of the ulnar collateral ligament.
Question 70
Which of the following structures is most commonly involved in lateral epicondylitis?
Explanation
The most common specific site of involvement is the origin of the extensor carpi radialis brevis. It is usually caused by overuse activities, such as the eccentric overload exhibited during a backhand in tennis. In most patients, the characteristic friable, grayish tissue described as angiofibroblastic hyperplasia or hyaline degeneration is seen at the extensor carpi radialis brevis origin. Nirschl RP: Elbow tendinosis/tennis elbow. Clin Sports Med 1992;11:851-870.
Question 71
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most likely reveal
Explanation
Follow-up examination at 6 months revealed no statistically significant differences in quadricep or hamstring strength when comparing surgical versus nonsurgical extremities isokinetically. Therefore, the selection of autogenous hamstring or patellar tendon for ACL reconstruction should not be based solely on the assumption of the graft tissue source altering the recovery of quadricep and/or hamstring strength. Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172 Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Question 72
A quarterback sustains a rough tackle after which he appears confused, has a dazed look on his face and an unsteady gait on standing. He denies loss of consciousness. Reexamination within 10 minutes is normal, the patient is lucid, and he wants to return to play. The coach and the player should be advised that he may
Explanation
The patient has a grade I (mild) concussion that can result in confusion and disorientation, without loss of consciousness. This concussion syndrome is completely reversible, with no long-term sequelae. Athletes who sustain a grade I concussion may return to play after 15 minutes if there are no lingering symptoms, such as headache or vertigo. A grade II concussion is characterized by loss of consciousness of less than 5 minutes. With this type of injury, the athlete can return to play in 1 week, if asymptomatic. If a grade III (severe) concussion is sustained, the athlete should avoid contact for a minimum of 1 month before considering a return to competition. A grade III concussion is characterized by a loss of consciousness of greater than 5 minutes or posttraumatic amnesia of greater than 24 hours. A CT scan is not indicated in a grade I injury. An athlete who sustains three grade I or grade II concussions, or two grade III concussions may not return to play for the season. Torg JS, Gennarelli TA: Head and cervical spine injuries, in DeLee JC, Drez D Jr (eds): Orthopaedic Sports Medicine Principles & Practice. Philadelphia, PA, WB Saunders, 1994, vol 1, pp 417-462.
Question 73
The bone avulsion shown in Figure 32 has a high correlation with tearing of the


Explanation
As described by Segond in 1987, an avulsion fracture of the lateral tibial plateau is commonly referred to as a Segond fracture. Subsequent to 1987, several authors have also found that the lateral capsular sign represents, but is not limited to, a disruption of the middle third of the lateral capsule and a tear of the anterior cruciate ligament. Bach BR, Warren RF: Radiographic indicators of anterior cruciate ligament injury, in Feagin JA (ed): The Crucial Ligaments. New York, NY, Churchill Livingston, 1988, pp 301-327. Segond P: Recherches cliniques et experimentales sur les epanchements sanguins du genou par entorse. Prog Med (Paris) 1987;7:297.
Question 74
A 21-year-old college defensive lineman sustains a minimally displaced (less than 1 mm) midthird scaphoid fracture during the first game of the season. Management should consist of
Explanation
The union rate for minimally displaced midthird scaphoid fractures is quite high with cast immobilization while allowing a return to sports. Inadequate immobilization results in a much higher nonunion rate. Early fixation and rehabilitation have been proposed for sports or positions that are not amenable to cast immobilization. While immobilization of a nondisplaced fracture results in an acceptably high union rate, there is no advantage to fixation in conjunction with immobilization in the course of healing. With adequate immobilization and protection, play restrictions until healing has occurred are unnecessary. Rettig AC, Kollias SC: Internal fixation of acute stable scaphoid fractures in the athlete. Am J Sports Med 1996;24:182-186. Rettig AC, Weidenbener EJ, Gloyeske R: Alternative management in midthird scaphoid fractures in the athlete. Am J Sports Med 1994;22:711-714.
Question 75
A 16-year-old football player sustains a direct blow to the anterior aspect of his flexed right knee. Examination reveals a contusion over the anterior tibial tubercle and a small effusion. MRI scans are shown in Figures 33a through 33c. What is the most likely diagnosis?


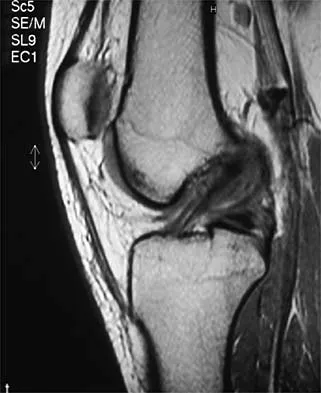



Explanation
33b 33c The MRI scans show disruption of the fibers of the PCL. Patients sustaining an isolated acute PCL injury can present with only minimal discomfort and have full range of motion. When examination reveals a contusion over the tibial tubercle and discomfort with the posterior drawer examination, with or without instability, a possible injury to the PCL should be considered. In acute injuries, the reported accuracy of MRI imaging for diagnosing PCL tears ranges from 96% to 100%. Resnick D, Kang HS: Internal Derangement of Joints: Emphasis on MRI Imaging. Philadelphia, PA, WB Saunders, 1997, pp 699-700. Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Finish Exam?
You cannot change answers after submitting.
