Question 1
A 21-year-old collegiate wrestler sustains a blow to his right eye during a match. Examination reveals anisocoria with a dilated right pupil. The globe is properly formed, and extra-occular movements and the visual field are grossly intact. What is the most likely diagnosis?


Explanation
Traumatic mydriasis occurs from a contusion to the iris sphincter. This is a transient phenomenon during which the iris fails to constrict properly, resulting in a dilated pupil. More severe trauma can result in a tear of the sphincter and permanent pupillary deformity. In association with head injury, traumatic anisocoria would be a concerning indicator of the severity of injury. Retinal detachment, lens dislocation, corneal abrasion, and traumatic hyphema are all potential results of eye injury but are not reflected by this clinical description. Brucker AJ, Kozart DM, Nichols CW, Irving MR: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby Year Book, 1991, pp 650-670.
Question 2
After making a tackle, a football player is found prone and unconscious without spontaneous respirations. Initial management should consist of
Explanation
The on-field evaluation and management of a seriously injured athlete requires that health care teams have a game plan in place and proper equipment that is readily available. The initial step, which consists of stabilizing the head and neck by manually holding them in a neutral position, is then followed by assessment of breathing, pulses, and level of consciousness. If the athlete is breathing, management should consist of mouth guard removal and airway maintenance. If the athlete is not breathing, the face mask should be removed, with the chin strap left in place. The airway must be established, followed by initiation of assisted breathing. CPR is instituted only when breathing and circulation are compromised. In the unconscious athlete or if a cervical spine injury is suspected, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated. McSwain NE, Garnelli, RL: Helmet removal from injured patients. Bull of Am Coll Surg 1997;82:42-44.
Question 3
A 23-year-old baseball pitcher who has diffuse pain along the posterior deltoid reports pain during late acceleration and follow-through. Examination of his arc of motion from external rotation to internal rotation at 90 degrees of shoulder abduction reveals a significant deficit in internal rotation when compared to the nonthrowing shoulder. Initial management should consist of
Explanation
Loss of internal rotation is common among overhead throwers and tennis players. Posterior capsular stretching can improve symptoms when accompanied by rest and gradual resumption of throwing. To avoid a false impression of improvement, cortisone injection is not recommended. Pitching through pain can cause further damage to the labrum and capsule. A sling and external rotator strengthening will not improve internal rotation. Kibler WB: Biomechanical analysis of the shoulder during tennis activities. Clin Sports Med 1995;14:79-85.
Question 4
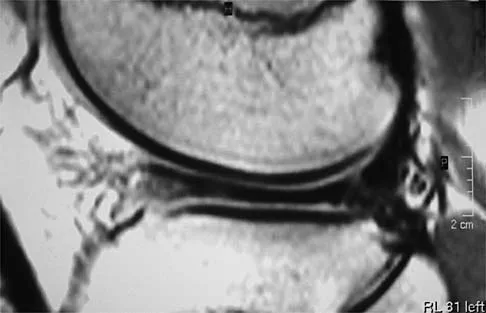
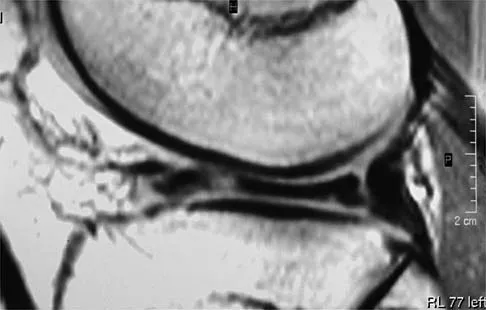
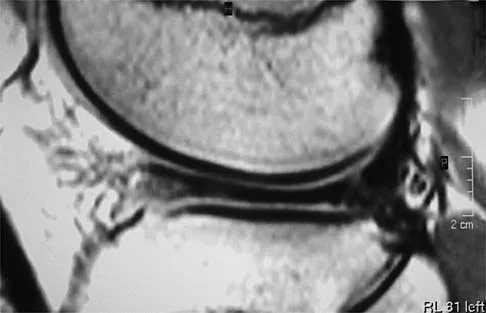
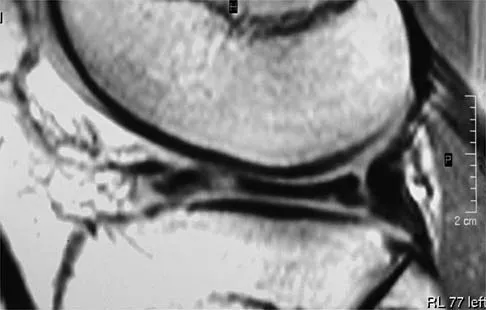
A 54-year man has left shoulder pain and weakness after falling while skiing 4 months ago. Examination reveals full range of motion passively, but he has a positive abdominal compression test and weakness with the lift-off test. External rotation strength with the arm at the side and strength with the arm abducted and internally rotated are normal. MRI scans are shown in Figures 1a and 1b. Treatment should consist of

Explanation
1b The examination findings are consistent with subscapularis muscle weakness but normal supraspinatus and infraspinatus strength. The lift-off test and abdominal compression test are specific for subscapularis function. The MRI scan reveals a chronic avulsion and retraction of the subscapularis. The transverse image reveals a normal infraspinatus muscle, and the sagittal image reveals an atrophic subscapularis. Surgical repair of the isolated subscapularis tendon is indicated. Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 31-56.
Question 5
A 17-year-old high school long distance runner is seeking advice before running a marathon for the first time. What advice should be given regarding his fluid, carbohydrate, and electrolyte intake around the time of the race?

Explanation
The goal of fluid replenishment should be to replace the sweat that has been lost. Sweat is mostly water, with a small concentration of salts and other electrolytes. Absorption is enhanced by solutions of low osmolality. Scientific research has also shown that adding carbohydrates to the drink improves athletic performance. Carbohydrates such as glucose and maltodextrins (glucose polymers) stimulate fluid absorption by the intestines. Fructose slows intestinal absorption of fluids. Drinks that are high in fructose, such as orange juice, can lead to gastrointestinal distress and osmotic diarrhea. Kirkendall D: Fluids and electrolytes, in The U.S. Soccer Sports Medicine Book. Baltimore, MD, Williams and Wilkins, 1996.
Question 6
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of


Explanation
The radial head is an important secondary stabilizer of the elbow, helping to resist valgus forces. There has been a movement toward open reduction and internal fixation of the radial head when technically feasible, especially in a relatively high-demand athlete or laborer. The examination and radiograph suggest that displacement of the fragment is great enough to create a mechanical block. Extended splinting would only serve to encourage arthrofibrosis. Early range of motion is appropriate if there is minimal displacement of the radial head fragement, it is stable, and there is no mechanical block to motion. Fragments larger than one third of the joint surface should be excised only if it is not possible to reduce and repair the fragment. Primary excision of the radial head should be avoided if possible. Complications after excision of the radial head include muscle weakness, wrist pain, valgus elbow instability, heterotopic ossification, and arthritis. Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Question 7
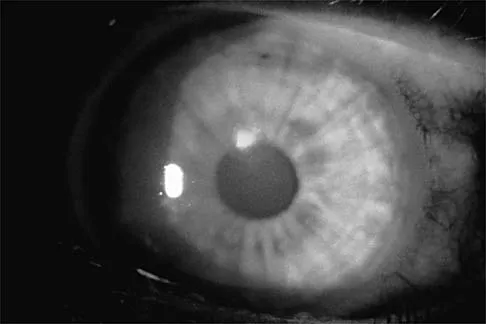
Figure 3 shows the clinical photograph of a wrestler who has an acute mass in his ear. He does not wear protective headgear. The area is mildly tender and without erythema. Management should consist of


Explanation
The patient has an auricular hematoma. This injury is typically related to blunt trauma, occuring in wrestlers who do not use protective headgear. The goal of treatment is to remove the fluid, reapproximate the perichondrium to the underlying articular cartilage, and limit reaccumulation of the fluid in attempt to prevent cartilage necrosis. Aspiration and application of a compressive dressing offers the best chance to achieve this goal. There are no signs of infection such as marked tenderness, erythema, or surrounding edema to justify antibiotic use or irrigation and debridement. The mass does not warrant excision. Kaufman BR, Heckler FR: Sports-related facial injuries. Clin Sports Med 1997;16:543-562.
Question 8
A patient with no history of patellar instability sustains a traumatic lateral patellar dislocation. What structure most likely has been torn?


Explanation
Any of the above structures may be involved in a lateral patellar dislocation. However, biomechanic studies have found that the medial patellofemoral ligament is the major soft-tissue static restraint of lateral patellar displacement, providing at least 50% of this function. Desio SM, Burks RT, Bachus KN: Soft tissue restraints to lateral patellar translation in the human knee. Am J Sports Med 1998;26:59-65. Conlan T, Garth WP Jr, Lemons JE: Evaluation of the medial soft-tissue restraints of the extensor mechanism of the knee. J Bone Joint Surg Am 1993;75:682-693.
Question 9
A 22-year-old swimmer underwent thermal capsulorrhaphy treatment for recurrent anterior subluxation. Following 3 weeks in a sling, an accelerated rehabilitation program allowed him to return to swimming in 3 1/2 months. While practicing the butterfly stroke, he sustained an anterior dislocation. He now continues to have symptoms of anterior instability and has elected to have further surgery. Surgical findings may include a


Explanation
Complications of thermal capsule shrinkage or accelerated rehabilitation include capsule ablation. Since the original surgery did not include labral reattachment, findings of a Bankart lesion or a glenoid fracture from a nontraumatic injury are unlikely. Subscapularis detachment or biceps subluxation is a postoperative complication of open repairs. Failure of early postoperative instability treatment should not produce loose bodies. Abrams JS: Thermal capsulorrhaphy for instability of the shoulder: Concerns and applications of the heat probe. Instr Course Lect 2001;50:29-36.
Question 10
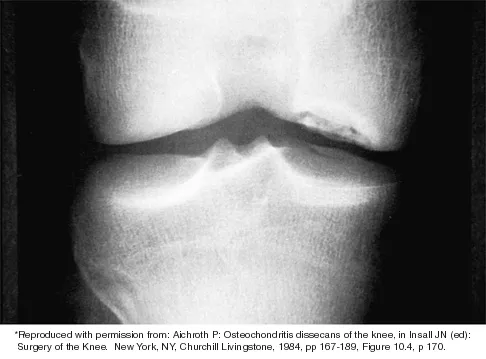
A 12-year-old boy reports knee discomfort after prolonged strenuous activities. He denies knee swelling or catching and has no pain with activities of daily living. A radiograph is shown in Figure 4. Prognosis for the pathology shown is most influenced by



Explanation
While many factors play a role in the outcome of osteochondritis dissecans, ample evidence has shown that the prognosis is most influenced by the growth status of the plates. If the growth plates are open, the chance of a successful outcome is significantly greater than if they are closed. Federico DJ, Lynch JK, Jokl P: Osteochondritis dissecans of the knee: A historical review of etiology and treatment. Arthroscopy 1990;6:190-197.
Question 11
A 70-year-old golfer has pain in her dominant shoulder. She reports that initially the pain was at night but now she is unable to play. Examination reveals weakness in external rotation and shoulder abduction. Radiographs reveal the humeral head articulating with a thin acromion. Management should consist of

Explanation
Chronic rotator cuff tears should be nonsurgically managed initially with a strengthening program. A cortisone injection may reduce inflammation. Surgery is reserved for patients who continue to have pain and lose sleep despite the use of physical therapy. Blood tests for infection or inflammation are nonspecific. Arthroscopy may play a role, but surgical replacement is reserved for advanced cases. Bokor DJ, Hawkins RJ, Huckell GH, et al: Results of nonoperative management of full-thickness tears of the rotator cuff. Clin Orthop 1993;294:103-110.
Question 12
Which of the following structures is the most important restraint to posterior subluxation of the glenohumeral joint when positioned in 90 degrees of flexion and internal rotation?

Explanation
The posterior band of the inferior glenohumeral ligament is the most important restraint to posterior subluxation of the glenohumeral ligament with the shoulder in 90 degrees of flexion and internal rotation. With the shoulder in external rotation, the subscapularis is an important stabilizer to posterior subluxation. When the shoulder is in neutral rotation, the coracohumeral ligament is the primary stabilizer. The middle glenohumeral ligament functions primarily to resist anterior translation of the shoulder in the midrange of abduction. The supraspinatus muscle and tendon have relatively little contribution to anterior and posterior translation of the glenohumeral joint. Blasier RB, Soslowsky LJ, Malicky DM, Palmer ML: Posterior glenohumeral subluxation: Active and passive stabilization in a biomechanical model. J Bone Joint Surg Am 1997;79:433-440.
Question 13
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?

Explanation
Based on these findings, the most likely diagnosis is a rotator cuff injury and probable tear; therefore, MRI is the study of choice. CT is preferred for articular fractures. A bone scan is nonspecific and can identify inflammation or occult fracture. Joint aspiration is not likely to identify an effusion. Physical therapy and a functional capacity examination are used to identify weakness during recovery prior to a return to work or sports. Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Question 14
In the arthroscopic photograph shown in Figure 5, the structure labeled "A" functions primarily as a restraint to translation of the humeral head in what direction?


Explanation
The superior glenohumeral ligament identified as "A" in the figure functions primarily as a restraint to inferior glenohumeral translation of the adducted arm. The middle glenohumeral ligament is highly variable and pooly defined in up to 40% of the population and functions to restrain anterior translation of the externally rotated arm in the midrange of abduction. The anterior band of the inferior glenohumeral ligament is the primary restraint to anterior/inferior translation of the head with the shoulder abducted to 90 degrees and in maximum external rotation. Ticker JB, Bigliani LU, Soslowskiy LJ, et al: Inferior glenohumeral ligament: Geometric and strain-rate dependent properties. J Shoulder Elbow Surg 1996;5:269-279.
Question 15
During the anterior approach for repair of a distal biceps tendon rupture, what structure, shown under the scissors in Figure 6, is at risk for injury?

Explanation
The most commonly injured neurovascular structure during an anterior approach for the repair of a distal biceps tendon rupture is the lateral antebrachial cutaneous nerve. This structure is located lateral to the biceps tendon and in a superficial location just deep to the subcutaneous layer. The antecubital vein is medial and superficial with the brachial artery and median nerve also medial to the biceps tendon but deep to the common flexors. The posterior interosseous nerve is deep within the supinator muscle and can be injured in the deep dissection or through the posterior approach when using a two-incision approach. Kelly EW, Morrey BF, O'Driscoll SW: Complications of repair of the distal biceps tendon with the modified two-incision technique. J Bone Joint Surg Am 2000;82:1575-1581.
Question 16
Which of the following variables has been shown to have the greatest influence on the higher rate of anterior cruciate ligament (ACL) tears in women when compared to men for similar sports?

Explanation
All of the variables have been proposed as possible causes for the increased incidence of ACL tears in women versus men. The general differences in the level of neuromuscular training however, specifically conditioning and muscle strength, have been shown to play the greatest role. Harmon KJ, Ireland ML: Gender differences in noncontact anterior cruciate ligament injuries. Clin Sports Med 2000;19:287-302. Arendt EA: Knee injury patterns among men and women in collegiate basketball and soccer. Am J Sports Med 1995;23:694-701.
Question 17
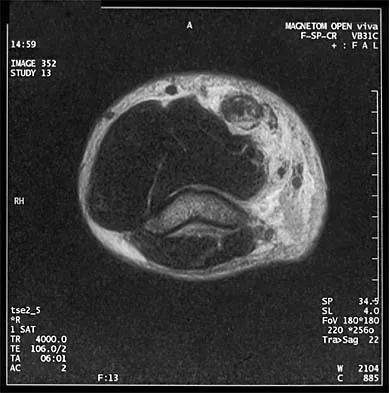
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?


Explanation
The history and MRI findings indicate the presence of anterior tibiotalar osteophytes. This is frequently observed in soccer, rugby, and football athletes who play on grass or turf surfaces and repetitively push off and change directions. Examination may reveal an effusion but no loss of subtalar motion. A positive external rotation (Klieger) test is described as pain at the distal ankle with external rotation of the foot and is observed in patients with syndesmosis sprains. This patient may have an increased anterior drawer because of a history of sprains; however, this finding is not specific for anterior impingement of tibiotalar osteophytes. The most specific finding on physical examination is pain with forced dorsiflexion. Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Question 18
A 21-year-old collegiate female cross-country athlete reports right hip pain that begins about 12 miles into a run, followed by pain resolution when she discontinues running. However, each time she tries to resume a running program, she experiences recurrence of pain deep in the anterior groin. A plain radiograph and MRI scan are shown in Figures 8a and 8b. Management should consist of



Explanation
8b The history is consistent with a stress fracture. Findings on the plain radiograph are marginal, but the MRI scan shows evidence of stress reaction in the medial neck of the femur (compression side). A lesion on the compression side is not normally at risk for displacement and usually can be managed nonsurgically. A bone scan would further identify the lesion but is not necessary. A skeletal survey and chest radiograph are used in staging a tumor. Radioisotope injection and guided biopsy are sometimes used for osteoid osteomas. Boden BP, Osbahr DC: High-risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 19
A 21-year-old football player who sustained a direct blow to the posterior hindfoot while making a cut is unable to bear weight on the injured foot. Examination reveals tenderness and swelling of the great toe metatarsophalangeal (MTP) joint. Radiographs are shown in Figures 9a and 9b. What is the most likely diagnosis?



Explanation
9b Turf toe occurs in collision and contact sports in which the athlete pushes off to accelerate or change direction and there is hyperextension of the great toe MTP joint. Typically, there is also axial loading of the posterior hindfoot, which increases the hyperextension of the MTP joint. The most common presentation is pain and swelling of the MTP joint and inability to hyperextend the joint without significant symptoms. With significant force, fractures of the sesmoids and plantar soft tissues can occur. The radiographs do not show a dislocation of the great toe MTP joint because it is concentrically located on both radiographs. However, the radiographs show a fracture of the lateral sesamoid or a diastasis of a bipartite lateral sesamoid. The medial sesamoid is also proximal indicating a rupture of the plantar (volar) plate. Therefore, the most likely diagnosis is a fracture of the lateral sesamoid with rupture of the plantar plate leading to proximal migration of the proximal fragment of the lateral sesamoid and the medial sesamoid. Rodeo SA, et al: Diastasis of bipartite sesamoids of the first metatarsophalangeal joint. Foot Ankle 1993;l4:425-434.
Question 20
Examination of an 18-year-old professional soccer player who was forcefully kicked across the shin while attempting a slide tackle reveals a marked effusion and limited motion of the knee. The tibia translates 12 mm posterior to the femoral condyles when the knee is held in 90 degrees of flexion. There is no posteromedial or posterolateral instability. Management should consist of
Explanation
The patient has an acute grade III posterior cruciate ligament injury. The majority of grade I and II injuries can be treated with protected weight bearing and quadriceps rehabilitation, and most patients can return to sports within 2 to 4 weeks. In contrast, grade III injuries require immobilization in full extension for 2 to 4 weeks to protect the posterior cruciate ligament and the other posterolateral structures presumed to be damaged. The mainstay of postinjury rehabilitation for all posterior cruciate ligament injuries is quadriceps strengthening exercises, which have been shown to counteract posterior tibial subluxation. Miller MD, Bergfeld JA, Fowler PJ, Harner CD, Noyes FR: The posterior cruciate ligament injured knee: Principles of evaluation and treatment. Instr Course Lect 1999;48:199-207.
Question 21
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?



Explanation
A compression or burst injury occurs with vertical loading of the spine, such as from a blow to the vertex with the neck flexed (eg, spear tackling in football). This leads to vertebral end plate fractures before disk injury. At higher forces, the entire vertebra and disk may explode into the spinal canal. Analysis has shown this to be the major mechanism of cervical fracture, dislocation, and quadriplegia. With the normal head-up posture, the cervical spine has a gentle lordotic curve, and forces transmitted to the head are largely dissipated in the cervical muscles. When the neck is flexed, the cervical spine becomes straight, with the vertebral bodies lined up under one another. This allows for minimal dissipation of the impact forces to be absorbed by the neck muscles. Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532. Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Question 22
A 17-year-old high school football player injures his right ankle during a game. Examination reveals swelling and a closed ankle deformity, with normal foot circulation and sensation. Radiographs are shown in Figures 10a and 10b. In addition to closed reduction, management should include



Explanation
10b The examination and radiographs reveal a closed fracture-dislocation of the ankle with tibiofibular diastasis. Immediate fixation of the medial malleolus and plating of the fibula are indicated. If residual tibiofibular diastasis occurs with lateral translation of the fibula after plating, a syndesmotic screw is placed to stabilize the syndesmosis. Ankle fracture-dislocations associated with a proximal fibular fracture (Maisonneuve fracture) require syndesmotic fixation, but the fibula is not plated. Unstable ankle fractures require surgical treatment. If swelling is severe (fracture blisters, loss of skin wrinkling), a compressive splint is applied and surgery is delayed for 5 to 7 days. Browner BD, Jupiter JB, Levine AM, Trafton PG: Skeletal Trauma. Philadelphia, PA, WB Saunders, 1992, pp 1887-1957.
Question 23
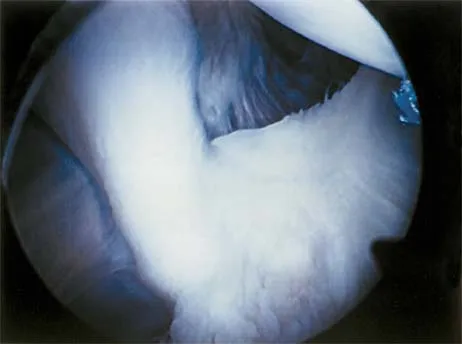
Figure 11 shows a consecutive sequence of MRI scans obtained in a 12-year-old boy who has had increasing lateral knee pain and catching for the past 6 months. Examination reveals pain localized to the lateral joint line. Range-of-motion testing reveals a 5-degree lack of full extension on the involved side. Plain radiographs and laboratory values are within normal limits. What is the most appropriate management?

Explanation
Discoid menisci are rare causes of lateral knee pain in children. Various etiologies have been proposed, including failure of central absorption of the developing meniscus and hereditary transmission. Patients with discoid menisci have pain, clicking, and locking with a loss of active extension on range-of-motion testing. Classification of discoid menisci according to the Watanabe classification include complete, incomplete, and Wrisberg ligament type. The Wrisberg variant contains an abnormal posterior meniscal attachment. MRI is the diagnostic tool of choice, revealing a thick, flat meniscus generally seen in three consecutive MRI images. Symptomatic knees are often associated with a meniscal tear or degeneration and are managed with arthroscopic partial excision to a more normal shape (saucerization). Vandermeer RD, Cunningham FK: Arthroscopic treatment of the discoid lateral meniscus: Results of long-term follow-up. Arthroscopy 1989;5:101-109.
Question 24
A collegiate football player who sustained a blow to the head during the first quarter of a game is confused for several minutes after the hit but does not lose consciousness. He had two similar episodes in games earlier in the season. When should he be allowed to return to play?

Explanation
Using the traditional concussion grading scale, the patient sustained a grade I concussion because he did not lose consciousness and his abnormal cognitive level lasted less than 1 hour. If this was the player's first concussion, theoretically he could return to play later in the game provided that he had no confusion, headache, or associated symptoms. However, because it was the third concussion for the year, participation in contact sports should be terminated for the season. Guskiewwicz KM, Barth JT: Head injuries, in Schenk RC Jr (ed): Athletic Training and Sports Medicine. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 143-167.
Question 25
For the athlete performing heavy exercise, the magnitude of core temperature and heart rate increase is most proportional to


Explanation
Studies examining the impact of graded water debt have clearly shown that the magnitude of core temperature and heart rate increase accompanying work are proportional to the magnitude of water debt at the onset of exercise. Though added thermal burden from hot climates is a factor, it appears to be less significant. Latzka WA, Montain SJ: Water and electrolyte requirements for exercise. Clin Sports Med 1999;18:513-524. Montain SJ, Sawka MN, Latzka WA, et al: Thermal and cardiovascular strain from hypohydration: Influence of exercise intensity. Int J Sports Med 1998;19:87-91.
Finish Exam?
You cannot change answers after submitting.
