Question 51
What is the most common complication of halo vest immobilization in adults?
Explanation
Although pin loosening generally has not been considered a major problem, it has been cited as the most common complication in two published series of halo vest complications. The other possible complications are all significantly less common. Baum JA, Hanley EN Jr, Pullekines J: Comparison of halo complications in adults and children. Spine 1989;14:251-252. Garfin SR, Botte MJ, Waters RL, Nickel VL: Complications in the use of the halo fixation device. J Bone Joint Surg Am 1986;68:320-325.
Question 52
What is the most common neurologic complication following an anterior cervical diskectomy and fusion?
Explanation
The recurrent laryngeal nerve provides innervation to the vocal cords and was the most common neurologic injury reported in a series of 36,000 patients. The nerve is felt to be more vulnerable during a right-sided approach because of its anatomic course. A recent study has also suggested a role for increased endotracheal cuff pressures in this nerve injury. Flynn TB: Neurologic complications of anterior cervical interbody fusion. Spine 1982;7:536-539.
Question 53
An otherwise healthy 45-year-old woman reports the onset of severe right leg pain. Figure 20a shows an axial MRI scan of the L4-5 level, and Figure 20b shows a sagittal view with the arrow at the L4-5 level. What nerve root is the most likely source of her pain?


Explanation
20b The scans show a disk herniation in the far lateral region of the disk. In particular, the sagittal view shows the herniation adjacent to the exiting L4 nerve root. Disk herniations in this area that cause symptoms are more likely to compress the nerve exiting at the same level rather than the next most caudal level. McCulloch JA: Microdiscectomy, in Frymoyer JW (ed): The Adult Spine: Principles and Practice. New York, NY, Raven Press, 1991, vol 2, pp 1765-1783.
Question 54
Which of the following forms of nonsurgical management is considered best for acute low back pain without radiculopathy?
Explanation
Temporary bed rest (less than 4 days) with gradual resumption of activities can be efficacious. Epidural steroid injections may be indicated for acute low back pain with radiculopathy. Acupuncture, facet joint injections, or ligamentous (sclerosant) injections are not indicated. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Question 55
A type 2A hangman's fracture, which has the potential to overdistract with traction, has which of the following hallmark findings?
Explanation
Type 2A hangman's fractures are thought to have a flexion mechanism rather than extension and axial loading. This allows them to rotate around the anterior longitudinal ligament into flexion. Anterior translation of greater than 3 mm and angulation distinguish type 2 fractures from type 1 fractures. Although there is an association between C1 ring fractures and C2 fractures, this does not factor into the classification. If a C2-3 facet dislocation exists in combination with a C2 pars fracture, it is considered a type 3 fracture. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Question 56
Figures 21a and 21b show the radiographs of a 22-year-old man who was shot through the abdomen the previous evening. An exploratory laparotomy performed at the time of admission revealed a colon injury. Current examination reveals no neurologic deficits. Management for the spinal injury should include


Explanation
21b IV broad-spectrum antibiotics should be administered for 7 days. This regimen, when compared to fragment removal or other antibiotic regimens, has been shown to reduce the incidence of spinal infections and reduce the need for metallic fragment removal with perforation of a viscus. Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Question 57
Stability at the atlanto-occipital joint is provided mainly by
Explanation
The atlanto-occipital joint is inherently unstable and would easily dislocate without the supporting ligaments. The apical ligament attaches to the basion and tip of the dens but does not provide adequate stability to the joint. Werne demonstrated that dividing the tectorial membrane and the alar ligaments resulted in gross joint instability. The anterior longitudinal ligament turns into the anterior atlanto-occipital membrane. This is called a membrane rather than a ligament because it is not strong enough to support these two structures. Werne S: Studies in spontaneous atlas dislocation. Acta Orthopaedica Scandinavica 1977;23(supplement).
Question 58
Which of the following are considered characteristic features of degeneration of a disk?
Explanation
Gradual dessication of the disk begins in the third decade as glycosaminoglycan levels within the nucleus begin to decline. The original water content of 88% decreases to 70% in the sixth decade and beyond. As glycosaminoglycan content decreases, there is a corresponding increase in noncollagen glycoprotein. Happey F, Weissman A, Naylor A: Polysaccharide content of the prolapsed nucleus pulposus of the human intervertebral disc. Nature 1961;192:868. Naylor A, Shentall R: Biomechanical aspects of intervertebral discs in aging and disease, in Jayson M (ed): The Lumbar Spine and Back Pain. New York, NY, Grune and Stratton Inc, 1976, pp 317-326.
Question 59
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Explanation
The spinal nerves primarily responsible for bladder function are the S2, S3, and S4 nerve roots. With significant compression of the cauda equina by either disk herniation, tumor, or degenerative stenosis, bladder dysfunction may result. Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Question 60
Figures 22a and 22b show the radiograph and sagittal MRI scan of the upper cervical spine of a 62-year-old woman who has had a long history of rheumatoid arthritis. Following hospitalization and skeletal traction, her symptoms improve significantly, her neurologic examination returns to normal, and repeat radiographs show a normal occiput and C1-C2 relationship. Treatment should now include


Explanation
22b Although opinions differ on whether a decompression is indicated in a patient with symptomatic basilar invagination, it is generally agreed that occipitocervical stabilization is indicated. This has been done with and without concomitant arthrodesis. Crockard HA, Grob D: Rheumatoid arthritis upper cervical involvement, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 701.
Question 61
What is the prognosis for ambulation, from best to worst, for patients with an incomplete spinal cord injury?
Explanation
Of the incomplete spinal cord injuries, Brown-Sequard syndrome has the best prognosis for ambulation. Central cord syndrome has a variable recovery. Anterior cord syndrome has the worst prognosis, with motor recovery rare below the level of the injury. Apple DF: Spinal cord injury rehabilitation, in Herkowitz HN, Garfin SR, Balderston RA, Eismont FJ, Bell GR, Wiesel SW (eds): Rothman-Simeone The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, pp 1130-1131.
Question 62
A skeletally mature 15-year-old girl who was thrown from the car in a rollover accident sustained the injuries shown in Figures 23a through 23d. Examination reveals no neurologic deficit, but the patient has moderate posterior spinal tenderness at the level of the injury. What is the most appropriate treatment?



Explanation
23b 23c 23d The majority of patients with thoracolumbar burst fractures without neurologic deficit can be effectively treated with a TLSO or a hyperextension body cast. Indications for surgery are neurologic deficit and/or significant deformity (greater than 50% loss of anterior vertebral body height or marked kyphosis). Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Question 63
The MRI scan shown in Figure 24 reveals a right-sided herniated nucleus pulposus at L4-5 in a patient with pain in the right leg. Administration of a caudal epidural steroid injection provides immediate relief. Over the next week he notes generalized weakness of the lower extremities and has one episode of urinary incontinence. What is the next most appropriate step in management?

Explanation
Whenever a patient's condition changes following a test or a procedure, the physician must determine the cause. A steroid flare reaction will not cause incontinence or weakness of the lower extremities. An L4-5 diskectomy may alleviate the problem if the right-sided L4-5 disk herniation is the etiology of the symptoms. However, it is unlikely that a right-sided disk herniation alone will cause a cauda equina syndrome. Possible etiologies include a further extrusion of a disk fragment at L4-5 that now obliterates the spinal canal, a disk herniation at another level, or an epidural abscess following injection of corticosteroids through a caudal approach. In the presence of a possible infection, myelography should not be performed from a lumbar puncture. The fastest and least invasive way to make an appropriate diagnosis is to obtain an MRI of the lumbar spine. In this patient, the MRI revealed an epidural abscess that was compressing the cauda equina. Because of the large dose of steroids that were injected, the patient did not manifest symptoms such as fevers and chills until late in the course. Knight JW, Cordingley JJ, Palazzo MG: Epidural abscess following epidural steroid and local anaesthetic injection. Anaesthesia 1997;52:576-578.
Question 64
At the L4-5 level, what is the location of the S2-5 nerve roots in relationship to the L5 and S1 nerve roots?
Explanation
The nerve roots of S2-5 are positioned dorsally and in the midline relative to the L5 and S1 nerve roots. The L5 nerve root is located lateral to S1 as it prepares to exit under the L5 pedicle. The S1 nerve root is located lateral and ventral to the S2-5 nerve roots. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 3-17.
Question 65
A comparison of dural tears repaired with suture alone and those treated by suture with fibrin glue supplementation will reveal which of the following findings?
Explanation
Animal studies assessing the influence of fibrin glue supplementation have detected a markedly greater inflammatory response at the site of application. An increased incidence of infection and delays in healing were not noted. Cain JE Jr, Rosenthal HG, Broom MJ, Jauch EC, Borek DA, Jacobs RR: Quantification of leakage pressures after durotomy repairs in the canine. Spine 1990;15:969-970.
Question 66
A 19-year-old woman reports lower back pain following a motor vehicle accident. Radiographs obtained immediately after the accident and a bone scan obtained 4 weeks later are shown in Figures 25a through 25c. The patient asks questions regarding the cause, genetics, and natural history of her condition. She should be informed that the condition was



Explanation
25b 25c The radiographs show L5 spondylolysis without spondylolisthesis (slip). The bone scan is normal, indicating that the pars interarticularis fractures are not acute. The incidence of spondylolysis is approximately 5% in the general population. The lesion generally develops in children age 5 to 6 years, and there is a second peak in the adolescent population. There is a familial predisposition, with reported rates of 27% to 69% in close relatives. A recent long-term follow-up study found that 90% of the spondylolisthesis had occurred before the patient's first visit to the physician. Spondylolisthesis tends to progress during the initial growth spurt and is similar in some respects to idiopathic scoliosis. Progression of a lytic spondylolysis to spondylolisthesis in adulthood has been reported; however, this is exceedingly rare. Lauerman WC, Cain JE: Isthmic spondylolisthesis in the adult. J Am Acad Orthop Surg 1996;4:201-208. Hensinger RN: Spondylolysis and spondylolisthesis in children and adolescents. J Bone Joint Surg Am 1989;71:1098-1107. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Question 67
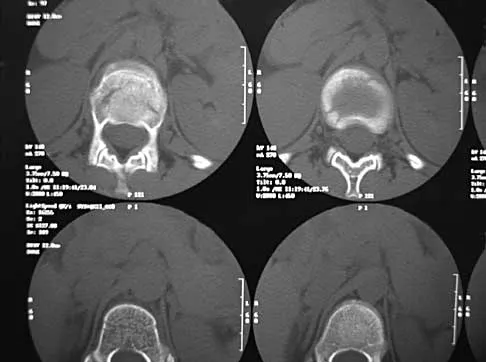
A patient underwent an anterior cervical diskectomy and interbody fusion for a C5-6 herniated nucleus pulposus and left C6 radiculopathy 8 months ago. He now reports new onset of severe neck pain and left C6 radicular pain, with wrist extension weakness. The radiograph and CT scan shown in Figures 26a and 26b reveal pseudarthrosis at C5-6. The next step in management should consist of

Explanation
26b Brodsky and associates reviewed 34 cases of cervical pseudarthrosis after anterior fusion. Seventeen were treated with revision anterior fusion and 17 with posterior foraminotomy and fusion. Good results were seen in 75% of patients who underwent revision anterior surgery, but better results (94%) were seen with posterior surgery, including foraminotomy and stabilization. Tribus and associates reported treatment of 16 patients with pseudarthrosis using revision anterior debridement of the fibrous tissue and fusion with autograft and plates. There was improvement of the neck in 75% of the patients, nonunion in 19%, continued weakness in 28%, and dysphagia in 5%. Farey and associates reported on 19 patients treated with posterior foraminotomy, stabilization, and fusion with a fusion rate of 100%, resolution of arm pain in 94%, resolution of weakness in 100%, and resolution of neck pain in 75%. It would appear that posterior foraminotomy is more effective for relieving arm pain and neurologic deficits associated with pseudarthrosis. Posterior fusion has the most reliable rate of arthrodesis in this setting. Dysphagia is reported in some patients undergoing more extensive anterior dissections required for applying plates. A neck brace is unlikely to aid in healing of pseudarthrosis in a patient who underwent surgery 8 months ago. A neck brace would be most effective within the first 3 months if a delayed union is identified. Brodsky AE, Khalil MA, Sassard WR, Neuman BP: Repair of symptomatic pseudarthrosis of anterior cervical fusion: Posterior versus anterior repair. Spine 1992;17:1137-1143. Tribus CB, Corteen DP, Zdeblick TA: The efficacy of anterior cervical plating in the management of symptomatic pseudarthrosis of the cervical spine. Spine 1999;24:860-864.
Question 68
A 44-year-old farmer involved in a rollover accident on his tractor sustained an L1 burst fracture with a 20% loss of anterior vertebral body height, 30% canal compromise, and 15 degrees of kyphosis. He remains neurologically intact. The preferred initial course of action should consist of
Explanation
Surgical decompression is unnecessary in a patient with no neurologic deficit and canal compromise of less than 50%. A compression deformity of less than 50% and kyphosis of less than 30 degrees may be successfully treated with a TLSO extension brace. Deformity in this range will reliably heal with minimal risk for late deformity or residual pain. Although some studies suggest 6 weeks of bed rest as treatment, early mobilization and bracing is preferred. Hartman MB, Chrin AM, Rechtine GR: Nonoperative treatment of thoracolumbar fractures. Paraplegia 1995;33:73-76. Chow GH, Nelson BJ, Gebhard JS, Brugman JL, Brown CW, Donaldson DH: Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine 1996;21:2170-2175.
Question 69
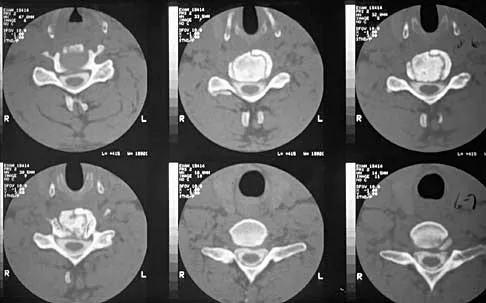
A 40-year-old carpenter has a 3-month history of right arm pain and neck pain that now leaves him unable to work. Examination reveals a positive Spurling test, weakness of the biceps, and a mildly positive Hoffman's sign on the right side. Electromyography and nerve conduction velocity studies show a right C6 deficit. Figures 27a through 27c show MRI scans that reveal two-level spondylotic disease at C5-6 and C6-7, a large herniated nucleus pulposus at C5-6, and a prominent ridge and hard disk at C6-7. Nonsurgical management fails to provide relief, so the patient elects surgical intervention. Which of the following surgical options would give the best long-term results?

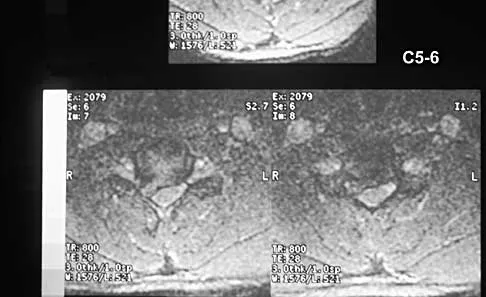
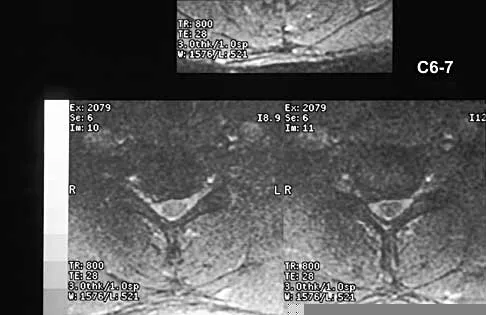

Explanation
27b 27c The patient has a single-level deficit by clinical examination but an adjacent level that may be pathologic. Hilibrand and associates, in a review of 374 patients with myeloradiculopathy treated with single-level or multilevel anterior cervical diskectomy and fusion, showed that 25% of patients had an occurrence of new radiculopathy or myelopathy at an adjacent level within 10 years after surgery. Reoperation rates were highest in those patients where the adjacent nonfused segment was C5-6 or C6-7. Those patients who had multilevel fusions had a lower incidence of adjacent segment disease. The authors recommended incorporating an adjacent level in the initial procedure in patients with myelopathy or radiculopathy when significant disease was noted. Posterior keyhole foraminotomy is an excellent procedure for single-level radiculopathy but is not effective in relieving myelopathy. Anterior cervical diskectomy without fusion has an increased incidence of hypermobility and neck pain on long-term follow-up. In a later review, these authors reported improved fusion rates and better clinical outcomes with the use of strut fusions instead of multilevel interbody grafts. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH: Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 1999;81:519-528. Henderson CM, Hennessy RG, Shuey HM Jr, Shackelford EG: Posterior-lateral foraminotomy as an exclusive operative technique for cervical radiculopathy: A review of 846 consecutively operated cases. Neurosurgery 1983;13:504-512.
Question 70
A patient with rheumatoid arthritis has an unstable pseudarthrosis after undergoing C1-2 posterior fusion. No neurologic deficits are noted, and repair with posterior transarticular fixation screws and a posterior wiring technique at C1-2 is planned. Which of the following preoperative studies offers the best visualization?
Explanation
Dickman and associates reported a greater than 10% incidence of vertebral artery anomalies at the C1-2 junction that would preclude the use of either unilateral or bilateral transarticular screw placement. They noted that 13 of 105 patients had a high-riding transverse foramen that precluded bilateral screw placement. In another series, 17 of 94 patients had unilateral high-riding transverse foramina and three had bilateral anomalies. Thin-cut CT with sagittal reconstructions offers the best visualization of the anomalous position of the vertebral artery. They noted that single screw placement in combination with posterior C1-2 fusion was an effective means to secure C1-2 stability. MRI gives excellent visualization of soft tissues and spinal cord compression but is not as clear as thin-cut CT for visualization of the vertebral artery foramina. Vertebral artery angiography is an invasive study with an inherent potential for complications. Electromyography does not correlate with vertebral artery anatomy. Paramore CG, Dickman CA, Sonntag VK: The anatomic suitability of the C1-2 complex for transarticular screw fixation. J Neurosurg 1996;85:221-224. Dickman CA, Sonntag VK: Posterior C1-C2 transarticular screw fixation for atlantoaxial arthrodesis. Neurosurgery 1998;43:275-280.
Question 71
An elderly patient falls and sustains an extension injury to the neck that results in upper extremity weakness, spared perianal sensation, and lower extremity spasticity. These findings best describe what syndrome?
Explanation
These finding indicate central cord syndrome, and injury that is more common in the older population who have some degree of spondylosis. The physiologic insult can be a central spinal hematoma with resultant hematomyelia. Bowel and bladder functional return has a good prognosis, unlike the upper extremity motor loss. Cauda equina syndrome generally involves injury at the lumbar levels, with some degree of lower extremity motor loss. Posterior cord syndrome is characterized by preservation of motor function below the level of injury and position/vibratory sensory loss. Brown-Sequard syndrome, which is often produced by a penetrating injury, results in contralateral hypalgesia and ipsilateral weakness. Anterior cord syndrome has a poor prognosis for functional return; lower extremity findings include loss of light touch, sharp/dull, and temperature sensations below the level of injury, as well as motor function. Apple DF Jr: Spinal cord injury rehabilitation, in Rothman RH, Simeone FA (eds): The Spine, ed 3. Philadelphia, PA, WB Saunders, 1992, Chapter 31.
Question 72
In the treatment of thoracic disk herniations, what approach is associated with the highest risk of iatrogenic paraplegia?
Explanation
Laminectomy is associated with the highest risk of iatrogenic paraplegia because retraction on the cord is necessary for visualization, but retraction is difficult because of tethering of the intradural dentate ligaments. All of the other approaches allow for access to the disk herniation through an angle that avoids the cord itself, although other limitations may exist. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 87-96.
Question 73
Which of the following factors is the strongest predictor of vertebral fracture in postmenopausal women?
Explanation
If a woman has two or more osteoporotic compression fractures, her risk of another is increased 12 fold. A decrease of two standard deviations in bone mineral density increases the risk four to six fold, a positive family history 2.7 fold, premature menopause 1.6 fold, and smoking 1.2 fold. It should be noted that these studies were carried out in Caucasian and Asian women. Melton LJ III: Epidemiology of spinal osteoporosis. Spine 1997;22:2S-11S.
Question 74
A 23-year-old man sustains a unilateral jumped facet with an isolated cervical root injury in a motor vehicle accident. Acute reduction results in some initial improvement of his motor weakness. Over the next 48 hours, examination reveals ipsilateral loss of pain and temperature sensation in his face, limbs, and trunk, as well as nystagmus, tinnitus, and diplopia. What is the most likely etiology for these changes?
Explanation
The patient is showing signs of vertebral artery stroke. The signs of Wallenberg syndrome include those listed above, as well as contralateral loss of pain and temperature sensation throughout the body, an ipsilateral Horner's syndrome, dysphagia, and ataxia. Vertebral artery injuries are not unusual in significant cervical facet injuries. A lesion in the cervical spinal cord is not associated with these symptoms, and an intracranial hemorrhage from trauma is unlikely to present in this manner. Young PA, Young PH: Basic Clinical Neuroanatomy. Baltimore, MD, Williams and Wilkins, 1997, pp 242-243. Hauop JS, et al: The cause of neurologic deterioration after acute cervical spinal cord injury. Spine 2001;26:340-346.
Question 75
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?
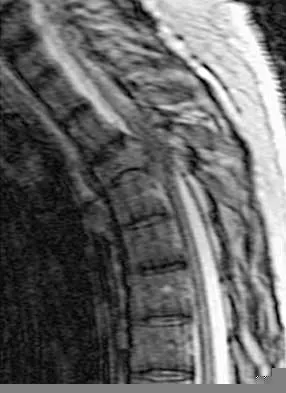

Explanation
Surgical decompression and stabilization have been shown to be the most effective means of improving neurologic function. Decompression is most reliably done from the side of the compression, which is anterior in this patient. Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Finish Exam?
You cannot change answers after submitting.
