Question 26
Figure 10 shows the MRI scan of a 56-year-old woman with metastatic breast cancer who now reports progressive paraparesis. Her general health remains good. Treatment should consist of


Explanation
If the patient's medical condition and prognosis remain good in the presence of significant and progressive neurologic deficit from cord compression, then the most reliable means of restoring function is via surgical decompression and fusion. Decompression should be directed toward the compressing structure (eg, anteriorly if the compression is from the anterior side). This procedure can be done via a posterolateral technique, such as costotransversectomy in some cases.
Question 27
When 6 weeks of noninvasive nonsurgical management fails to provide relief for a lumbar disk herniation, a trial of epidural steroid injections is likely to yield which of the following results?

Explanation
Lumbar epidural steroid injections appear to play a role in management of a lumbar disk herniation that has failed to respond to at least 6 weeks of nonsurgical treatment. Approximately 42% to 56% of patients report significant pain relief compared with 92% to 98% of those patients treated with diskectomy. Patients with extruded or sequestered herniations report the greatest and most rapid relief. Similarly, those with well-hydrated disk fragments report rapid relief of symptoms. A smaller percentage of patients report symptom relief compared with those having surgery, but the degree of improvement is similar for both groups and the improvement lasts up to 3 years. Butterman GR: Treatment of lumbar disc herniation: Epidural steroid injection compares with discectomy: A prospective, randomized study. J Bone Joint Surg Am 2004;86:670-679.
Question 28
Which of the following anatomic changes is observed as part of the normal aging process of the adult spine?



Explanation
The primary change that takes place in the aging spine is degeneration of the lumbar disks and loss of the overall lumbar lordosis. This also may be associated with osteopenic-related compression fractures. With these changes, the sagittal vertical line moves anteriorly relative to the sacrum; cervical scoliosis is uncommon and not part of the normal aging process. Overall kyphosis in the thoracic spine gradually increases, but the coronal balance remains essentially the same unless scoliosis develops. Gelb DE, Lenke LG, Bridwell KH, et al: An analysis of sagittal spinal alignment in 100 asymptomatic middle and older aged volunteers. Spine 1995;20:1351-1358.
Question 29
A previously healthy 30-year-old woman has neck pain and bilateral hand and lower extremity tingling with weakness after falling down stairs. She is alert and oriented. Examination reveals incomplete quadriplegia at the C6 level that remains unchanged throughout her evaluation and initial treatment. Radiographs show a bilateral facet dislocation of C6 on C7 without fracture. Attempts at reduction with halo cervical traction up to her body weight are unsuccessful. What is the next most appropriate step?


Explanation
A facet dislocation that cannot be reduced in an alert, awake patient with some preservation of cord function requires MRI to evaluate the disk prior to a reduction under anesthesia. The presence or absence of a disk herniation must be assessed, as this factor may influence the method of reduction. Vaccaro AR, Falatyn SP, Flanders AE, et al: Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999;24:1210-1217. Fardon DF, Garfin SR, Abitbol J (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 247-262. Eismont FJ, Arena MJ, Green BA: Extrusion of an intervertebral disc associated with traumatic subluxation or dislocation of cervical facets. J Bone Joint Surg Am 1991;73:1555-1560.
Question 30
Which of the following findings is the best radiographic indicator of segmental instability at L4-L5?


Explanation
Motion segments that demonstrate more than 4 mm of translation or 10 degrees of angulation compared with adjacent motion segments on flexion-extension radiographs have excessive motion and instability. Anterior marginal osteophytes form at the insertion of the annulus from increased forces but do not indicate increased motion. A spondylolisthesis or lateral listhesis is often static without increased motion. More than 3.5 mm of translation or 11 degrees of angulation is considered instability criteria for the cervical spine. Internal disk disruption does not denote instability. Boden SD, Wiesel SW: Lumbosacral segmental motion in normal individuals. Have we been measuring instability properly? Spine 1990;15:571-576.
Question 31
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
Although pseudarthrosis can be found anywhere within the spine that has been fused using long multisegmental fixation to the sacrum, it most commonly occurs at the lumbosacral junction. The thoracolumbar junction is another common site of potential pseudarthrosis. In this location, the anatomy changes from lumbar transverse processes to thoracic through the transition zone, and overlying instrumentation often makes it difficult to obtain enough sound bone on decorticated bone to achieve a successful fusion. Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653. Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine 1983;8:489-500.
Question 32
The afferent pain innervation of the L3-L4 facet joint arises from the medial branch nerve of
Explanation
Afferent pain fibers to the lumbar facet joints arise from the medial branch nerves originating from the next two cephalad levels. Therefore, innervation of the L3-L4 facet joint arises from the L2 and L3 medial branch nerves. This effect should be taken into account when considering a medial branch block or facet denervation. The medial branch nerve arises from the dorsal ramus of the exiting nerve root. Nade SL, Bell E, Wyke BD: The innervation of the lumbar spinal joint and its significance. J Bone Joint Surg Br 1980;62:255-261
Question 33
When posterior fusion with instrumentation to the sacrum is used to treat adult scoliosis, what instrumentation technique best increases the chance of a successful lumbosacral fusion?
Explanation
As the chance of success of lumbosacral fusion increases with the stiffness and rigidity of the construct, fixation and stiffness improve with fixation into both the upper sacrum and the ilium. In a review of individuals treated with long constructs to the pelvis for adult scoliosis, Islam and associates reported that the rate of pseudarthrosis was significantly lower with sacral and iliac fixation compared with sacral fixation alone or iliac fixation alone. Iliac screws provide significant fixation anterior to the instantaneous axis of rotation for flexion and extension, as well as provides resistance to lateral bending and rotational forces. Numerous biomechanical studies support the concept of increasing biomechanical stabilization with increased fixation from the sacrum to the ilium. Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173. O'Brien N, et al: Sacral pelvic fixation and spinal deformity, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 601-614.
Question 34
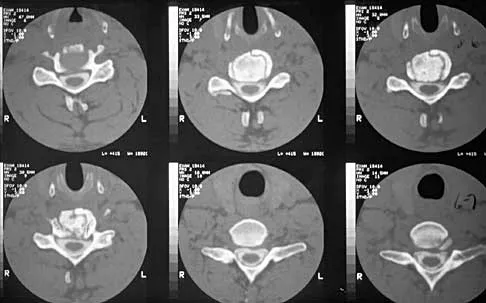
Which of the following structures runs through the site indicated by the arrow in Figure 11?

Explanation
The vertebral artery traverses through the arcuate foramen after exiting the lateral aspect of C1 and before entering the skull. The foramen usually is not fully formed, but a complete foramen such as this one has been reported in up to 18% of patients. Stubbs DM: The arcuate foramen: Variability in distribution related to race and sex. Spine 1992;17:1502-1504.
Question 35
A 42-year-old man has had left lower extremity pain in an L5 radicular pattern for the past 6 weeks. He denies significant axial low back pain. History reveals that he underwent an L4-5 diskectomy with successful relief of similar pain 5 years ago. Which of the following imaging studies would offer the greatest amount of information?
Explanation
MRI with gadolinium will best identify recurrent herniated nucleus pulposus or other root compression and distinguish scar from recurrent disk. CT is unable to distinguish scar from recurrent disk density, and the addition of myelogram dye can reveal compromise of the thecal sac but cannot distinguish the scar from recurrent disk as the source of compression. Although lateral flexion-extension radiographs may be important to rule out any instability, much of that information can be inferred from the associated disk and adjacent bony changes on MRI. Bone scan techniques may identify subtle stress fractures resulting from previous aggressive facet resection, but low back pain also would be expected. Mirowitz SA, Shady KL: Gadopentetate dimeglumine-enhanced MR imaging of the postoperative lumbar spine: Comparison of fat-suppressed and conventional T1-weighted images. Am J Roentgenol 1992;159:385-389.
Question 36
Figure 12 shows the radiograph of an 80-year-old woman who has had an 8-month history of back pain after a fall. What is the most likely diagnosis based on the radiographic findings at the fractured vertebrae?

Explanation
An intravertebral vacuum cleft suggests nonunion of the vertebral fracture with osteonecrosis and is not seen in routine healing fractures. MRI characteristically shows a high T2 signal in the cleft. The cleft is not indicative of an infectious or neoplastic lesion. A vacuum disk phenomenon is associated with end-stage degenerative disk disease, but those findings are not found in the vertebral body. Murakami H, Kawahara N, Gabata T, et al: Vertebral body osteonecrosis without vertebral collapse. Spine 2003;28:E323-E328.
Question 37
Which of the following complications is uniquely associated with an anterior approach to the lumbosacral junction?
Explanation
Retrograde ejaculation is a sequela of injury to the superior hypogastric plexus. The structure needs protection, especially during anterior exposure of the lumbosacral junction. The use of monopolar electrocautery should be avoided in this region. The ideal exposure starts with blunt dissection just to the medial aspect of the left common iliac vein, sweeping the prevertebral tissues toward the patient's right side. Although erectile dysfunction can be seen after spinal surgery, it is not typically related to the surgical exposure because erectile function is regulated by parasympathetic fibers derived from the second, third, and fourth sacral segments that are deep in the pelvis and are not at risk with the anterior approach. The other choices are complications of spinal surgery but are not uniquely associated with an anterior L5-S1 exposure. Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492. Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107.
Question 38
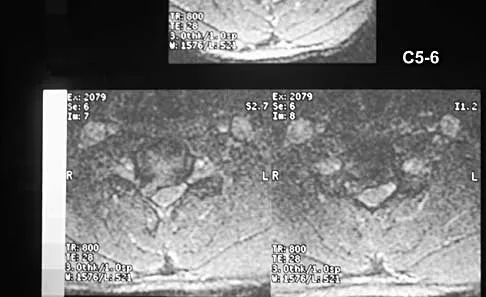
A 68-year-old woman with a history of rheumatoid arthritis has had neck pain and weakness in all four extremities that has become worse in the past 6 months. She has gone from a community to a household ambulator and uses a wheelchair outside of the home. Examination of the extremities reveals poor coordination, diffuse weakness, hyperactive reflexes, and bilateral sustained clonus. She has a broad-based and unsteady gait. The posterior atlanto-dens interval is 12 mm. Based on these findings and the radiograph and MRI scan shown in Figures 13a and 13b, the treatment of choice is surgical decompression and stabilization. However, the patient inquires about the prognosis with surgery compared to nonsurgical management. Assuming there are no complications from surgery, the patient should be informed that, with surgery, she will most likely


Explanation
13b The patient has a cervical myelopathy with more than 10 mm of space available for the cord; therefore, she has a reasonable chance of improved neurologic function following surgery. If not treated with surgery, however, her neurologic condition likely will worsen and she will die earlier than if she had surgery. Matsunaga S, Sakou T, Onishi T, et al: Prognosis of patients with upper cervical lesions caused by rheumatoid arthritis: Comparison of occipitocervical fusion between C1 laminectomy and nonsurgical management. Spine 2003;28:1581-1587.
Question 39
Five weeks after undergoing a successful L4-L5 diskectomy, with complete relief of his preoperative sciatica, a 36-year-old man has severe, relentless back and buttock pain. Examination and laboratory studies are unremarkable with the exception of an erythrocyte sedimentation rate (ESR) of 90 mm/h. What is the next most appropriate step in management?
Explanation
The patient's history, including the timing and type of symptoms, is typical for postoperative diskitis. The elevated ESR, 5 weeks after surgery, is also consistent with infection; a normal WBC count is not unusual. Management should consist of MRI with gadolinium; if positive, this should be followed by percutaneous biopsy to confirm the organism. Open biopsy may be considered if the percutaneous biopsy is unsuccessful. Anterior debridement and interbody fusion is reserved for the occasional patient that fails to respond to intravenous antibiotics, bed rest, and immobilization. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 257-271.
Question 40
An 18-year-old man sustained a knife injury to his midback, with the entry wound 2 cm to the left of the midline. He has been diagnosed with a hemicord transection. Neurologic examination will most likely reveal left-sided loss of
Explanation
Brown-Sequard syndrome results from an injury to one half of the spinal cord and is characteristically seen in penetrating injuries. The spinothalamic fibers cross the midline below the level of the lesion, resulting in contralateral loss of pain and temperature sensation. The posterior columns and corticospinal tracts carry vibratory, position, and light touch sensation, as well as motor function from the ipsilateral side of the body. This results in the characteristic neurologic findings seen with Brown-Sequard syndrome. Northrup BE, Evaluation and early treatment of acute injuries to the spine and spinal cord, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 541-549.
Question 41
When using surgery extending to the pelvis to treat long spinal deformity in adults, the addition of anterior interbody structural support at the lumbosacral junction serves what biomechanical function?
Explanation
Shufflebarger and others have reported that the placement of anterior interbody structural support at the lumbosacral junction increases the overall construct stiffness and reduces the strain on posterior instrumentation, thereby reducing the risk of screw pull-out or fracture. The stiffness of the posterior instrumentation actually increases, whereas the actual strength of the instrumentation remains the same. Actual strain measured at an adjacent intervertebral disk to a fusion construct is expected to increase. Shufflebarger HL: Moss-Miami spinal instrumentation system: Methods of fixation of the spondylopelvic junction, in Margulies JI, Floman Y, Farcy JPC, et al (eds): Lumbosacral and Spinal Pelvic Fixation. Philadelphia, PA, Lippincott-Raven, 1996, pp 381-393. Cunningham BW: A biomechanical approach to posterior spinal instrumentation: principles and applications, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 588-600.
Question 42
A 40-year-old woman has had sciatic pain on the left side for the past 8 weeks. She reports that the pain radiates to her posterior thigh, lateral calf, and into the dorsum of her left foot. Neurologic examination shows weakness of the left extensor hallucis longus. Axial T2-weighted MRI scans through L4-L5 are shown in Figure 14. Management should consist of

Explanation
The MRI scans show hypertrophy of the left L4-L5 facet joint and ligamentum flavum, with a synovial cyst. Appropriate surgical management consists of a hemilaminectomy and direct decompression of the neural elements. Fusion, in addition to the decompression, may be considered, particularly in patients with an associated spondylolisthesis. Epstein NE: Lumbar laminectomy for the resection of synovial cysts and coexisting lumbar spinal stenosis or degenerative spondylolisthesis: An outcome study. Spine 2004;29:1049-1055.
Question 43
During C1-C2 transarticular screw fixation, screw misplacement is most likely to result in injury to the
Explanation
With C1-C2 transarticular screw fixation, the following structures are potentially at risk: vertebral artery, spinal cord, occiput-C1 joint, and hypoglossal nerve. The vertebral artery is most vulnerable to injury with drill misdirection or anatomic variations in the vertebral foramen. The hypoglossal nerve may be injured if the drill, tap, or screw passes too far anterior to the lateral mass of C1. This complication is extremely rare. The occiput-C1 joint may be injured if the screw trajectory is too cephalad or cranially directed; however,this scenario is very unlikely because the exposure tends to direct the screw into a caudally inclined direction. This caudal orientation has the potential to cause vertebral artery injury, especially in patients who have a large vertebral foramen in the lateral mass of C2 because of erosions (rheumatoid arthritis) or anatomic variation. CT of the vertebral foramen is recommended when C1-C2 transarticular fixation is being considered. Spinal cord injury is extremely unlikely because of the very large size of the spinal canal in the upper cervical spine; the spinal cord lies far away from the lateral masses of C1 and C2. Mueller ME, Allgower M, et al: Manual of Internal Fixation, ed 3. New York, NY, Springer-Verlag, 1991, pp 634-636.
Question 44
A 27-year-old professional soccer player sustained an injury to his cervical spine in a collision with another player. Initially he was diagnosed with a right C6 radiculopathy that resolved with rest, anti-inflammatory medications, and physical therapy. Following a fall in a game, he noted a recurrence of neck pain without radicular signs or symptoms. Additional nonsurgical management over the past few months has failed to provide relief. A cervical MRI scan shows a right-sided C5-6 herniation without any evidence of disk disease at other cervical levels. The patient desires to continue his career as a professional soccer player. What treatment offers the best long-term option for return to play?
Explanation
The patient has chronic neck pain that is affecting his career as a professional soccer player. Although he had signs and symptoms of a right C6 radiculopathy, neck pain is his only current symptom. Therefore, procedures to address the relief of radiculopathy (keyhole foraminotomy and transforaminal epidural steroid injection) are likely to be ineffective. Although Watkins and others have described continuing nonsurgical management for symptomatic herniated disks and return to play only when asymptomatic, the patient has not found relief with these modalities. A single-level cervical fusion (either postoperative or congenital) generally is not considered a contraindication for return to play in collision or contact sports. Therefore, anterior cervical fusion at C5-6 offers the best long-term option for return to play. Watkins RG: Cervical spine injuries in athletes, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 373-386. Watkins RG: Neck injuries in football players. Clin Sports Med 1986;5:215-246. Morganti C, Sweeney CA, Albanese SA, et al: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Question 45
A collegiate football player who sustained an injury to his neck has significant neck pain and weakness in his extremities. Following immobilization, which of the following steps should be taken prior to transport?
Explanation
Prior to transport, the face mask should be removed so that the airway can be easily accessible. If serious injury is suspected, the helmet and shoulder pads should be left in place until he is assessed at the hospital and radiographs are obtained. Leaving the helmet and shoulder pads in place helps to keep the spine in the most neutral alignment. Removal of the helmet will result in extension of the neck, whereas removal of the shoulder pads will most likely result in flexion of the neck. Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 376. Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347. Waninger KN, Richards JG, Pan WT, et al: An evaluation of head movement in backboard-immobilized helmeted football, lacrosse, and ice hockey players. Clin J Sport Med 2001;11:82-86. Donaldson WF III, Lauerman WC, Heil B, et al: Helmet and shoulder pad removal from a player with suspected cervical spine injury: A cadaveric model. Spine 1998;23:1729-1732.
Question 46
What is the most common complication following total disk arthroplasty in the lumbar spine?
Explanation
In a midterm (7 to 11 years) follow-up study of lumbar total disk arthroplasty, 5 of 55 patients had transient radicular leg pain without evidence of nerve root compression. Implant migration is rare. Deep venous thrombosis, incisional hernia, and retrograde ejaculation are less common complications of disk arthroplasty.
Question 47
A 42-year-old woman has cervical stenosis and radicular deficits at the C5-6 and C6-7 levels. History reveals that she has smoked one pack of cigarettes a day for 25 years. Because nonsurgical management has failed to provide relief, she is now seeking surgical treatment. After preoperative counseling, it becomes clear that she is not likely to stop smoking. Which of the following surgical procedures should be used?
Explanation
In a review of 190 anterior cervical fusions, Hilibrand and associates reported that only 20 of 40 patients who smoked had solid fusion at all levels, whereas 64 of 91 nonsmokers had solid fusions at all levels when treated with multilevel interbody technique (Smith-Robinson). When fused with strut grafts, 14 of 15 smokers and 41 of 44 nonsmokers had solid fusions with a fusion rate of 93% in the same series. Multilevel allografts have a lower fusion rate than autografts, and diskectomy without fusion has an increased rate of residual neck pain. Hilibrand AS, Fye MA, Emery SE, et al: Impact of smoking on the outcome of anterior cervical arthrodesis with interbody or strut-grafting. J Bone Joint Surg Am 2001;83:668-673.
Question 48
An otherwise healthy 54-year-old man who underwent a successful multilevel lumbar decompression and fusion 4 years ago now reports increasingly severe bilateral thigh claudication with paresthesia and severe back pain for the past 12 months. Physical therapy, bracing, and epidural steroids have failed to provide relief. A radiograph and MRI scans are shown in Figures 15a through 15c. He is afebrile, and laboratory studies show an erythrocyte sedimentation rate of 5 mm/h and a normal WBC count. What is the best course of action?



Explanation
15b 15c The patient has degeneration of an adjacent segment with resultant kyphosis and stenosis. Because he is healthy, has responded well to previous surgery, and has a potentially correctable lesion, he is not a good candidate for an end-stage failed back procedure such as a morphine pump. The stenosis is exacerbated by the deformity; therefore, a simple decompression will contribute to instability. Because of the kyphosis and the patient's relatively young age, the treatment of choice is restoration of sagittal alignment and posterior decompression.
Question 49
Which of the following is considered a risk factor for the development of low back pain?
Explanation
Risk factors associated with low back pain include poor physical fitness, smoking, a history of repetitive bending or stooping on the job, or whole body vibration exposure. Some radiographic factors such as stenosis, spondyloarthropathy, severe deformity, or instability are also associated with low back pain. Gender, weight, transitional anatomy, or facet trophism are not associated with low back pain.
Question 50
A corset-type brace may help reduce symptoms during an episode of acute low back pain as the result of
Explanation
Although there is no significant alteration in motion with a corset, studies have shown a decrease in intradiskal pressure. Nachemson A, Morris JM: In vivo measurements of intradiscal pressure: Discometry, a method for determination of pressure in the low lumbar disc. J Bone Joint Surg Am 1964;46:1077-1092.
Finish Exam?
You cannot change answers after submitting.
