Question 1
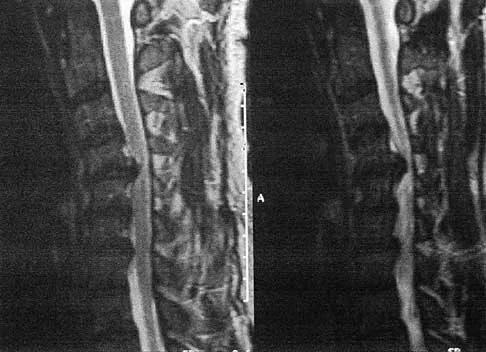
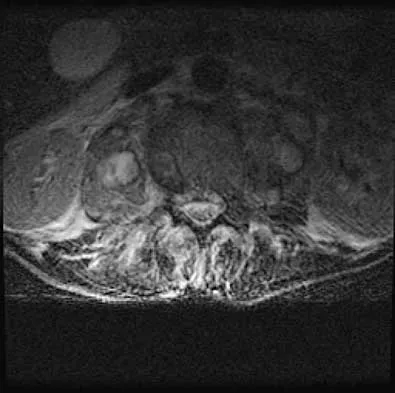
Figures 1a and 1b show the sagittal T2- and T1-weighted MRI scans of a 25-year-old intravenous drug abuser who has low back pain that is increasing in intensity. Laboratory studies show a WBC count of 10,000/mm3 and an erythrocyte sedimentation rate of 80 mm/h. Blood culture is negative. Initial management consist of


Explanation
1b The MRI scans show vertebral diskitis/osteomyelitis. The treatment of spinal infection in adults should be organism specific; therefore, initial management should consist of CT-guided closed biopsy prior to administration of antibiotic coverage. An open biopsy is indicated for a failed closed biopsy or failure of nonsurgical management. Although Staphylococcus aureus is the most common bacteria, a history of intravenous drug abuse raises suspicion for other organisms, including Pseudomonas. Tay BK, Deckey J, Hu SS: Spinal Infections. J Am Acad Orthop Surg 2002;10:188-197.
Question 2
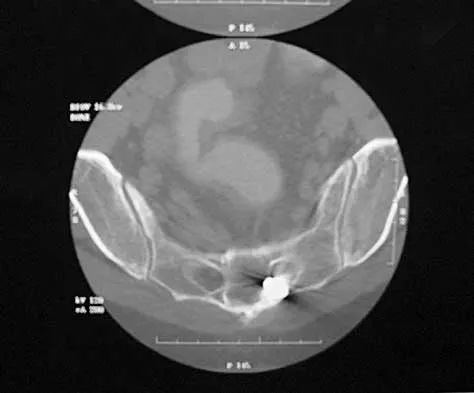
A 27-year-old man sustained a gunshot wound to the lumbar spine and undergoes an exploratory laparotomy. An injury to the cecum is identified and treated. Management should now include

Explanation
Gunshot wounds to the spine present relatively little risk of infection in most cases. When there has been an injury to the colon, the risk of infection can be minimized with a 7-day course of broad-spectrum antibiotics. Fragment removal is not indicated. Roffi RP, Waters RL, Adkins RH: Gunshot wounds to the spine associated with a perforated viscus. Spine 1989;14:808-811.
Question 3
A 68-year-old man reports a 1-year history of debilitating neck pain without neurologic symptoms. History reveals a C5-6 anterior diskectomy and bone grafting 10 years ago that provided good relief of arm and neck pain. Radiographs show evidence of fibrous union at C5-6, spondylotic disk narrowing at C4-5 and C6-7, and a fixed 2-mm subluxation at C3-4. Examination reveals cervical stiffness and discomfort at the extremes of movement. His neurologic examination is normal. Treatment should now consist of


Explanation
Axial pain can be difficult to manage. Pain management is not always successful, and surgical approaches may provide disappointing results unless there is discrete pathology. Whereas planning of a surgical approach should consider prior approaches and preexisting laryngeal dysfunction, no compelling case for surgical intervention can be made for this patient. Therefore, management should consist of patient education, exercise, and nonnarcotic medication. Ahn NU, Ahn UM, Andersson GB, et al: Operative treatment of the patient with neck pain. Phys Med Rehabil Clin N Am 2003;14:675-692. Algers G, Pettersson K, Hildingsson C, et al: Surgery for chronic symptoms after whiplash injury: Follow-up of 20 cases. Acta Orthop Scand 1993;64:654-656.
Question 4
Which of the following is considered the lowest level that a standard thoracolumbosacral orthosis (TLSO) can immobilize?


Explanation
Without more distal immobilization such as a thigh extension, the lower two lumbar segments generally show the same or even increased mobility with a TLSO. White AA, Panjabi MM: Clinical Biomechanics of the Spine, ed 2. Philadelphia, PA, JB Lippincott, 1990, pp 475-509.
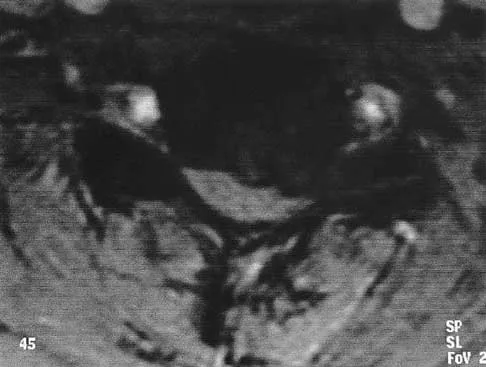
Question 5
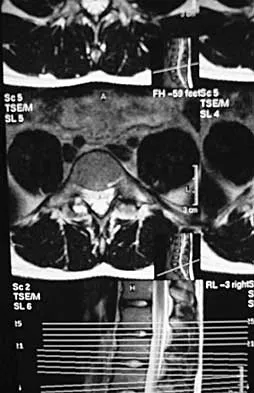
A 65-year-old man with ankylosing spondylitis has neck pain after falling back over his lawnmower, striking his thoracic spine, and forcing his neck into extension. Examination reveals subtle weakness of the intrinsics and finger flexors at approximately 4+/5. Initial management consists of immobilization in a rigid collar, and placing his head in the anatomic position. Radiographs reveal a subtle extension fracture of the lower cervical spine. Approximately 6 hours after the injury, he reports increasing paresthesias in his upper and lower extremities, and examination now shows his intrinsics are 2/5, finger flexors are 3/5, and his triceps are now weak at 4/5 on manual motor testing. In addition, his lower extremities now show weakness in both dorsal and plantar flexion of the ankle in the range of 4/5. Repeat radiographs appear unchanged. An MRI scan is shown in Figure 2. Management should now consist of

Explanation
It is not uncommon for patients with ankylosing spondylitis to sustain extension-type fractures, most typically of the cervicothoracic junction. These fractures can appear nondisplaced or minimally displaced initially, making them difficult to diagnose. Because there is no mobility between vertebrae, fractures tend to occur more like those of a transverse fracture of a long bone. In addition, the vertebral bodies are vascular and their canals are relatively enclosed, making them vulnerable to epidural bleeding. The MRI scan reveals an epidural hematoma located posteriorly on the cord; therefore, the treatment of choice is surgical evacuation and a posterior laminectomy. Because of the intrinsic instability of such fractures at the time of the laminectomy, internal fixation and stabilization with a posterior fusion is warranted. A simple laminectomy will only increase instability, and control is unlikely with halo vest immobilization. An anterior procedure will not effectively treat the problem given the location of the hematoma. Consideration can be given to methylprednisolone and observation; however, this will not eradicate the problem. Bohlman HH: Acute fractures and dislocations of the cervical spine. J Bone Joint Surg Am 1979;61:1119-1142.
Question 6
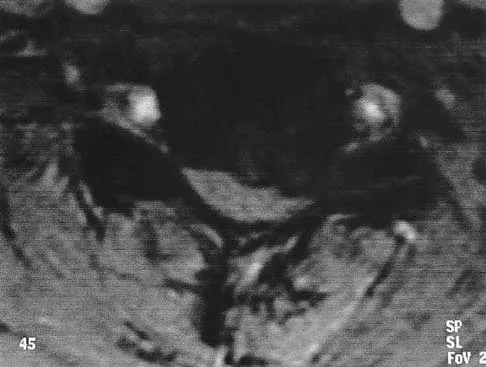
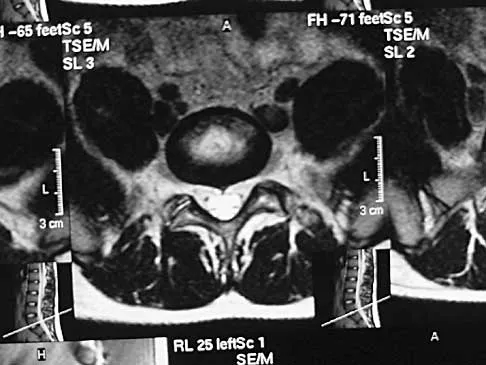
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?

Explanation
3b Muliple neurofibromas result in marked foraminal enlargement as seen on the sagittal MRI scan. Collagen disorders leading to dural ectasia may show similar enlargement, but none of these is listed as a possible answer. Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 7
A Trendelenburg gait is most likely to be seen in association with

Explanation
A Trendelenburg gait results from weakness of the gluteus medius, which is innervated by the L5 nerve root. A paracentral disk herniation at L4-L5 most commonly results in an L5 radiculopathy and thus weakness of the gluteus medius. A paracentral herniation at L5-S1 most commonly affects the S1 nerve root. A paracentral herniation at L3-L4, a central herniation at L3-L4, and a far lateral herniation at L4-L5 all affect the L4 root. Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Question 8
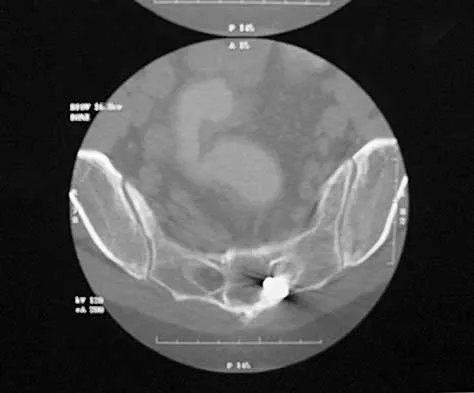
An otherwise healthy 70-year-old man has back and bilateral leg pain in an L5 distribution that is aggravated by standing more than 10 minutes or walking more than 100 feet. He has to sit to get relief. Neurologic and pulse examinations are normal. A radiograph and MRI scan are shown in Figures 4a and 4b. Treatment should consist of



Explanation
4b The patient has a degenerative spondylolisthesis at L4-5 with associated spinal stenosis. His symptoms are consistent with neurogenic claudication. Based on these findings, the surgical treatment of choice is decompression and posterolateral fusion. Use of instrumentation is controversial. Laminectomy alone is reserved for the patient who is frail medically. There is no role for an anterior approach or for fusion alone without decompression. Fischgrund JS, Mackay M, Herkowitz HN, et al: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 9
Figures 5a and 5b show the radiograph and MRI scan of a patient who has severe mechanical neck pain but no neurologic problems. Biopsy and work-up show the lesion to be a solitary plasmacytoma. Treatment should consist of



Explanation
5b Plasmacytoma is very sensitive to radiation therapy and given the complexity of the resection and complications of surgery in the given location, radiation therapy is preferred. However, the patient has clear loss of bony structural integrity, and resultant instability would persist even with tumor irradiation; therefore, posterior stabilization is warranted. Chemotherapy and bone marrow transplant are reserved for systemic disease with multiple myeloma. Corwin J, Lindberg RD: Solitary plasmacytoma of bone vs. extramedullary plasmacytoma and their relationship to multiple myeloma. Cancer 1979;43:1007-1013.
Question 10
A 71-year-old woman undergoes a posterior lumbar decompression and fusion from L4-S1. Thirty-six hours after the procedure, she reports severe right-sided chest pain and shortness of breath. Doppler ultrasound reveals a clot proximal to the knee within the femoral vein. A large pulmonary embolus is confirmed by CT angiography. The next most appropriate step in management should consist of

Explanation
In a review of 13,000 spinal procedures, nine patients were treated with heparin following development of pulmonary emboli. Of these patients, six had serious complications ranging from wound drainage to paralysis. Heparin therapy instituted within 10 days of the surgical procedure resulted in a 100% complication rate. Vena cava filter placement has a complication rate of 0.12% to 10.1%. Removable filters are currently in clinical trials. Cain JE Jr, Major MR, Lauerman WC, et al: The morbidity of heparin therapy after development of pulmonary embolus in patients undergoing thoracolumbar or lumbar spinal fusion. Spine 1995;20:1600-1603. Roberts AC: Venous imaging and inferior vena cava filters. Curr Opin Radiol 1992;4:88-96.
Question 11
Figure 6 shows the lateral radiograph of a 22-year-old woman who has painful Scheuermanns's kyphosis in the middle and lower thoracic spine. When planning surgical correction using instrumentation, the distal aspect of the instrumentation should ideally extend to the


Explanation
Posterior constructs for Scheuermann's kyphosis ideally should extend from the most superior to the most inferior aspect of the Cobb angulation. However, the most distal fusion level must be in a stable or lordotic position to avoid the development of junctional kyphosis. Lowe reported that failure to incorporate the first lordotic segment of the lumbar spine is associated with a higher risk of junctional kyphosis. The first lordotic segment of the lumbar spine is typically at least one level below the distal aspect of the curve as measured by the Cobb technique and most commonly is in the upper part of the lumbar spine. Lowe TG: Scheuermann's disease. Orthop Clin North Am 1999;30:475-487.
Question 12
Figure 7 shows the radiograph of a 64-year-old man who has neck pain and weakness of the upper and lower extremities following a motor vehicle accident. Examination reveals 3/5 quadriceps and 4/5 hip flexors but no ankle dorsiflexion or plantar flexion. His intrinsics are 1/5, with finger flexors of 3/5. He is awake, alert, and cooperative. Management should consist of

Explanation
In patients with facet dislocations and an incomplete neurologic deficit, early decompression of the canal via reduction of the dislocation generally is considered safe if the patient is alert and can cooperate. However, patients who cannot cooperate with serial neurologic examinations during the reduction are at risk for increased deficit secondary to herniated nucleus pulposus, and MRI should be performed prior to either closed or open reduction. Star AM, Jones AA, Cotler JM, et al: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Question 13
What is the recommended insertion torque for halo pins in adults?


Explanation
Garfin and associates have shown that halo pins inserted with 8 in-lb of insertion torque results in significantly less loosening with cyclical loading than pins inserted with 6 in-lb of torque. Moreover, Botte and associates reported that 8 in-lb of torque is clinically safe and effective in lowering the incidence of pin loosening and infection. Botte MJ, Byrne TP, Garfin SR: Application of the halo device for immobilization of the cervical spine utilizing an increased torque pressure. J Bone Joint Surg Am 1987;69:750-752. Garfin SR, Lee TO, Roux RD, et al: Structural behavior of the halo orthosis pin-bone interface: Biomechanical evaluation of standard and newly designed stainless steel halo fixation pins. Spine 1986;11:977-981.
Question 14
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45-degree lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
There are several indications for extending adult scoliosis fusions to the sacrum, rather than stopping in the lower lumbar spine. These indications include posterior column deficiencies at L5-S1, such as spondylolysis and laminectomy, and deformities extending to the sacrum, such as fixed tilt of L5-S1 or sagittal imbalance. MRI signal changes in the L5-S1 disk do not preclude stopping the fusion at L5. Some surgeons use diskography or diagnostic facet blocks to evaluate the integrity of the L5-S1 level prior to stopping the fusion at L5. Long scoliosis fusions stopping at L5 have a significant risk of failure, highlighting the importance of careful selection of fusion levels. Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629. Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Question 15
Which of the following findings is considered a contraindication for posterior decompression (with or without fusion) for myelopathy?



Explanation
Although cervical instability is a contraindication to posterior decompression alone, segmental instability in the myelopathic cervical spine can be addressed with concomitant posterior fusion with instrumentation. Cervical lordosis represents the ideal scenario for posterior decompressive procedures for myelopathy (laminectomy and laminoplasty) because compression from anterior osteophytes, if present, is relieved as the spinal cord migrates posteriorly. The anteroposterior diameter of the spinal canal does not have an impact on the selection of surgical approach. Posterior unroofing-type procedures in kyphotic cervical spines, however, are ineffective because anterior impingement on the spinal cord will remain; therefore, kyphosis of more than 10 degrees is considered a contraindication for posterior decompression. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 16
A patient reports progessive bilateral hand clumsiness and ataxia. Examination reveals a positive Hoffmann's sign and intrinsic atrophy. MRI reveals multilevel cervical spondylosis, and lateral flexion and extension radiographs show cervical kyphosis in the neutral position, with restoration of lordosis on extension. Which of the following procedures is most likely to result in poor long-term results?
Explanation
Adequate decompression of the cervical cord can be achieved in a variety of ways depending on the pathoanatomy of the compression, but kyphosis is a relative contraindication to laminectomy alone. For laminectomy to be effective, the lordosis must be maintained so the cord can displace posteriorly away from the anterior structures. In addition, removing the posterior tension band increases the probability that the kyphosis will progress, therefore increasing the force against the front of the cord as it tents across the kyphosis. Albert TJ, Vaccaro A: Postlaminectomy kyphosis. Spine 1998;23:2738-2745. Truumees E, Herkowitz HN: Cervical spondylotic myelopathy and radiculopthy. Instr Course Lect 2000;49:339-360.
Question 17
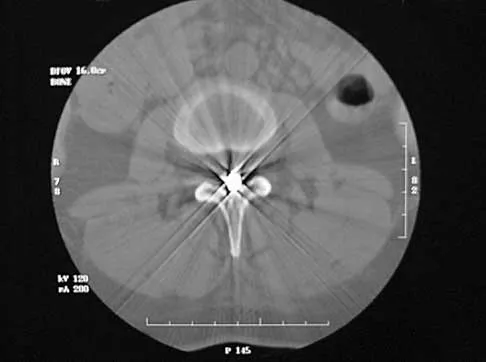
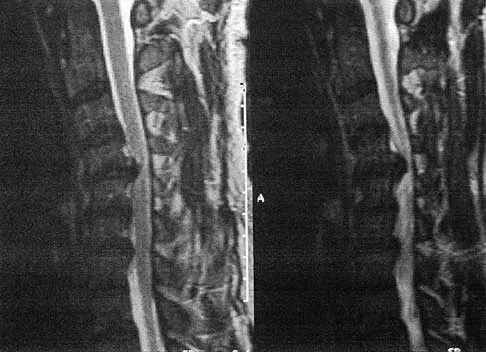
A 45-year-old man seen in the emergency department reports a 1-week history of worsening low back pain and a progressive neurologic deficit in the S1 distribution. Examination reveals 2/5 strength in the gastrocnemius. Laboratory studies show a WBC count of 13,500/mm3 and an erythrocyte sedimentation rate of 74 mm/h. Radiographs of the lumbosacral spine show narrowing of the L5-S1 disk space, with irregularity of the end plates. A sagittal T2-weighted MRI scan is shown in Figure 8. Definitive management should consist of

Explanation
The history, physical examination, laboratory, and radiographic findings are most consistent with an infectious process. When there are signs of neurologic compromise, surgery is generally recommended. This is an anterior process, and anterior column debridement is necessary, followed by stabilization. Anterior or posterior stabilization is a reasonable option, but posterior decompression alone is unlikely to adequately reverse the process and may lead to segmental kyphosis. Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott Williams and Wilkins, 2003, pp 165-189.
Question 18
In a retroperitoneal approach to the lumbar spine, what structure runs along the medial aspect of the psoas and along the lateral border of the spine?

Explanation
The sympathetic trunk runs longitudinally along the medial border of the psoas. The ilioinguinal nerve emerges along the upper lateral border of the psoas and travels to the quadratus lumborium, and the genitofemoral nerve lies more laterally on the psoas. The ureter is adherent to the posterior peritoneum and falls away from the psoas and the spine in the dissection, as does the aorta. Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983, p 107.
Question 19
What is the most likely primary cause of decreased success rates of bony fusion in smokers undergoing lumbar arthrodesis?



Explanation
A number of studies have shown a lower success rate of arthrodesis in smokers. Animal models also have shown that administration of nicotine can markedly decrease the rate of arthrodesis. Although it may not be possible to completely eliminate some of the other associated factors that contribute to the failure of arthrodesis, it does appear that nicotine is the primary factor. Andersen T, Christensen FB, Laursen M, et al: Smoking as a predictor of negative outcome in lumbar spinal fusion. Spine 2001;26:2623-2628.
Question 20
Flexion-distraction injuries of the thoracolumbar spine are most frequently associated with injury to what organ system?


Explanation
In patients with flexion-distraction injuries of the thoracolumbar spine, 50% have associated, potentially life-threatening, visceral injuries that occasionally are diagnosed hours or even days after admission. Based on these findings, consultation with a general surgeon is recommended. Blunt and penetrating injuries to the cardiopulmonary system or aorta sometimes can be seen with this type of injury, but they are no more common than with other types of thoracolumbar fractures because of the relatively mild bony injury anteriorly. Neurologic trauma with this type of fracture is also somewhat rare. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 351-360.
Question 21
What is the most common adverse postoperative complication of laminoplasty for multilevel cervical spondylotic myelopathy?
Explanation
A 30% to 50% loss of cervical range of motion is reported postoperatively in most patients following cervical laminoplasty. Inadvertent closure of the laminoplasty does occur but is rare. Laminoplasty is advocated in lieu of laminectomy to prevent progressive kyphosis and can effectively decompress the spinal cord. C5 nerve root palsies are a poorly understood but rare complication of surgical decompression for cervical spondylotic myelopathy. Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Question 22
The thickest bone in the occiput is located

Explanation
Anatomic studies have shown that the thickest bone of the occiput is at the level of the external occipital protuberance. It ranges from 11.5 mm to 15.1 mm in men and from 9.7 mm to 12 mm in women. In general, the bone thins as it extends distally from the external occipital protuberance and it also moves laterally from the midline. The structures at risk during screw placement include the venous sinuses. Nadim Y, Lu J, Sabry FF, et al: Occipital screws in occipitocervical fusion and their relation to the venous sinuses: An anatomic and radiographic study. Orthopedics 2000;23:717-719.
Question 23
A patient who underwent an L5-S1 diskectomy 18 months ago has persistent pain in the left leg. Figures 9a and 9b show postoperative axial T1-weighted MRI scans at the L5-S1 level without and with gadolinium. What is the most likely diagnosis?




Explanation
9b Persistent or recurrent symptoms after lumbar diskectomy are troublesome and can be difficult to assess. Gadolinium-enhanced MRI scans may be helpful. The images show enhancement about the left S1 root, a finding that is most consistent with perineural (epidural) fibrosis. The root itself does not enhance. Root enhancement has been associated with compressive radicular symptoms. A disk herniation does not enhance with gadolinium. A neurilemmoma enhances with gadolinium, but the involved root would be enlarged. There is no evidence of a fluid collection which would be consistent with an epidural abscess. Babar S, Saifuddin A: MRI of the post-discectomy lumbar spine. Clin Radiol 2002;57:969-981. Kikkawa I, Sugimoto H, Saita K, et al: The role of Gd-enhanced three-dimensional MRI fast low-angle shot (FLASH) in the evaluation of symptomatic lumbosacral nerve roots. J Orthop Sci 2001;6:101-109.
Question 24
Which of the following factors is most closely associated with early postoperative migration of "stand-alone" lumbar interbody fusion cages?
Explanation
Postoperative migration of lumbar interbody fusion cages is a rare complication. It is most commonly seen after placement of the cages through a posterior approach, with instability of the final construct. It is not associated with the design of the cage, the type of graft used, or a resultant pseudarthrosis. McAfee PC: Interbody fusion cages in reconstructive operations on the spine. J Bone Joint Surg Am 1999;81:859-880.
Question 25
If a laminectomy for spinal stenosis is performed, which of the following is an indication for concomitant arthrodesis at that level?
Explanation
A prospective randomized study of patients with degenerative spondylolisthesis and spinal stenosis by Herkowitz and Kurz showed significantly improved clinical outcomes in patients who also received a lumbar arthrodesis. Patients with a laminectomy at an adjacent level do not have improved outcomes with an arthrodesis. Minimal lumbar scoliosis does not require arthrodesis. Arthrodesis is indicated in cases where there is removal of more than 50% of the facets bilaterally but not with an associated foraminal stenosis. Herkowitz HN, Kurz LT: Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 1991;73:802-807.
Finish Exam?
You cannot change answers after submitting.
