Question 1
The transverse diameter of the pedicle is most narrow at which of the following levels?




Explanation
Of the levels given, T5 has the most narrow pedicle in anatomic studies. One study in patients with scoliosis did note that T7 on the concave side was more narrow than T5, but T7 is not listed here as a possible answer. O'Brien MF, Lenke LG, Mardjetko S, et al: Pedicle morphology in thoracic adolescent idiopathic scoliosis: Is pedicle fixation an anatomically viable technique? Spine 2000;25:2285-2293.
Question 2
Subluxation caused by rheumatoid arthritis is most commonly seen at what level of the cervical spine?


Explanation
Approximately 65% of cervical subluxations occur at C1-C2. Of these, 50% are anterior, with the remainder being lateral and posterior. The second most common type is basilar invagination, occurring in 40% of patients. The third most common type is subaxial, occurring in 20% of patients with rheumatoid arthritis. Subluxation at more than one level is common. Boden S, Clark CR: Rheumatoid arthritis of the cervical spine, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 693. Boden SD, Dodge LD, Bohlman HH, Rechtine GR: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Question 3
During a transperitoneal approach to the L5-S1 interspace, care must be taken to protect the superior hypogastric plexus from injury. Which of the following techniques reduces the risk of neurologic injury?


Explanation
Retrograde ejaculation is the sequela of superior hypogastric plexus injury. This structure needs protection, especially during anterior exposure of the L5-S1 disk space. Only blunt dissection should be used, and use of monopolar electrocautery should be avoided. If possible, preserve and retract the middle sacral artery. Once the iliac veins are isolated, blunt dissection is begun along the course of the medial edge of the left iliac vein, reflecting the prevertebral tissues toward the patient's right side. The dissection goes from left to right because the parasympathetic plexus is more adherent on the right side.
Question 4
When treating thoracolumbar spine fractures, which of the following is considered the major advantage of using a thoracolumbosacral orthosis (TLSO) when compared to a three-point fixation brace (Jewett)?

Explanation
When treating thoracolumbar spine fractures, the major advantage of using the TLSO is greater rotational control. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 347-349. Krompinger WJ, Fredrickson BE, Mino DE, Yuan HA: Conservative treatment of fractures of the thoracic and lumbar spine. Orthop Clin North Am 1986;17:161-170.
Question 5
Injury to which of the following structures has been reported following iliac crest bone graft harvest?
Explanation
Injury to the lateral femoral cutaneous nerve and the ilioinguinal nerve have both been described with an anterior iliac crest bone graft harvest. The lateral femoral cutaneous nerve may be injured from retraction after elevating the iliacus muscle or from direct injury when the nerve actually courses over the crest. A posterior crest harvest can injure the superior gluteal artery if a surgical instrument violates the sciatic notch. Injury to the inferior gluteal artery has not been described; it leaves the pelvis below the piriformis muscle belly and should not be at risk even with a violation of the sciatic notch. Injury to the ilioinguinal nerve has been reported from vigorous retraction of the iliacus muscle after exposing the inner table of the anterior ilium. Cluneal nerve injury may occur with posterior crest harvest, particularly if the skin incision is horizontal or extends more than 8 cm superolateral from the posterior superior iliac spine. Kurz LT, Garfin SR, Booth RE Jr: Iliac bone grafting: Techniques and complications of harvesting, in Garfin SR (ed): Complications of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1989, pp 323-341.
Question 6
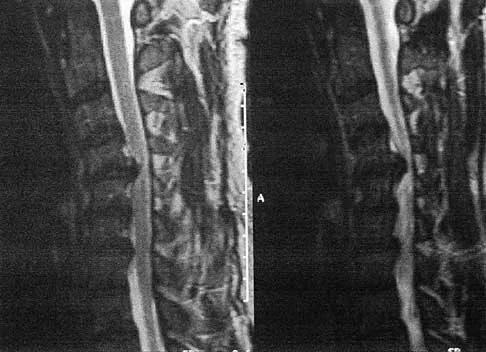
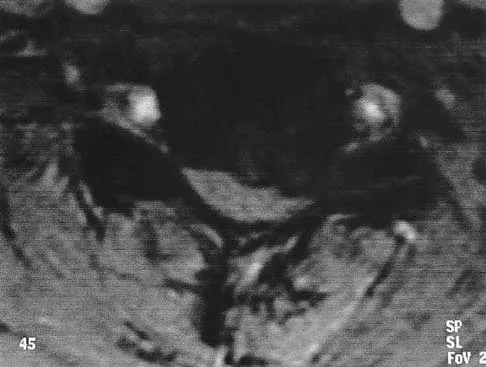
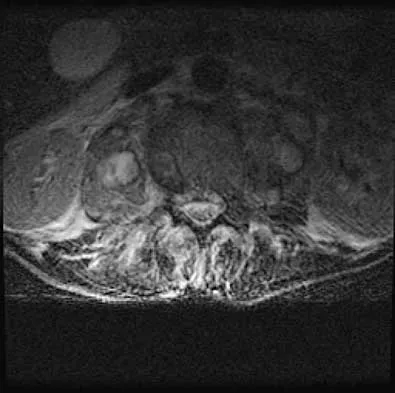
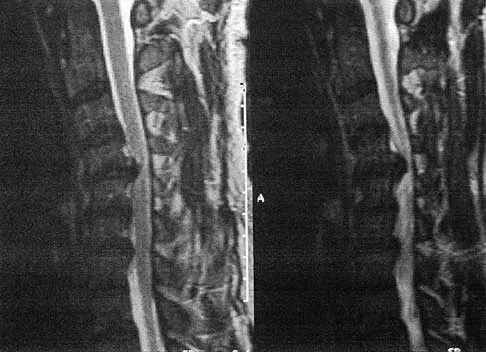
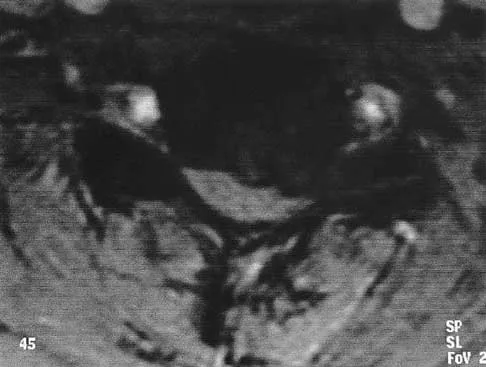
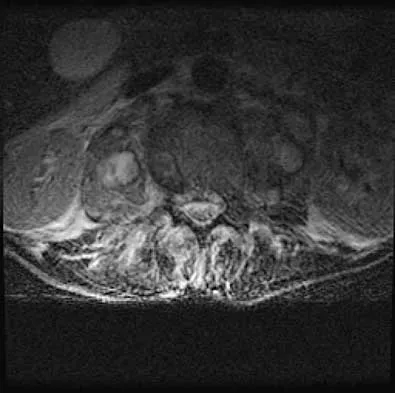
A 44-year-old woman has had lower extremity dysesthesias, urinary incontinence, and has been unable to walk for the past 2 days. She reports no pain or history of trauma. She notes that 3 weeks ago she missed work for 2 days because of back pain, but it resolved with rest. Examination shows decreased or absent sensation below the knees, no motor function below the knees, and decreased rectal tone. Catheterization results in a postvoid residual of 2,000 mL. Plain radiographs and MRI scans without contrast are shown in Figures 1a through 1d. What is the next most appropriate step in management?





Explanation
1b 1c 1d The patient has had a clear and sudden onset of a profound neurologic deficit. The radiographic studies suggest a lesion in the conus medullaris that appears to be intradural and intramedullary. MRI, with and without contrast, will best evaluate this mass further. The addition of gadolinium allows further evaluation of vascularity and the extent of the lesion. Eichler ME, Dacey RG: Intramedullary spinal cord tumors, in Bridwell KH, Dewald RL (eds): The Textbook of Spine Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1997, vol 2, pp 2089-2116.
Question 7
During anterior surgery on the cervical spine, at what level would the lateral dissection of the longus coli muscle most likely cause Horner's syndrome?





Explanation
The sympathetic chain approaches the lateral border of the longus coli muscle at C6 and is more vulnerable to injury at this level. Injury to the chain will cause Horner's syndrome, usually seen as unilateral ptosis.
Question 8
When compared with cobalt-chromium and stainless steel implants, a titanium implant has what biomechanical properties?

Explanation
Titanium implants are commonly used in spinal surgery, especially when MRI may be needed after implantation. Titanium implants have a lower modulus of elasticity when compared with cobalt-chromium and stainless steel implants. This is felt to allow less stress shielding for these types of implants. The other properties do not apply to titanium implants.
Question 9
A 22-year-old college basketball player who was hit from behind while going up for a rebound is rendered immediately quadraparetic for approximately 10 minutes, followed by complete resolution of motor loss and return of full sensation. The radiograph and MRI scan of the cervical spine shown in Figures 2a and 2b reveal a canal diameter of 13 mm, loss of cerebrospinal fluid space about the spinal cord, and no signal change within the cord. What is the best course of action?


Explanation
2b The correct decision on return to sports participation after episodes of transient quadraparesis is controversial. Cantu and Mueller feel strongly that the loss of cerebrospinal fluid space about the spinal cord signifies an unacceptable risk for future spinal cord injury if the athlete returns to sports. However, Watkins and Torg and Lasgow have reported no evidence of increased spinal cord injury in athletes with narrow spinal canals, even in football. These authors suggest judgment be used in advising return to contact or high-energy sports and that the physician's responsibility is to give accurate and relevant information, allowing the athlete to make his or her own choice regarding return to sports participation. Cantu R, Mueller FO: Catastrophic spine injuries in football (1977-1989). J Spinal Disord 1990;3:227-231. Watkins RG: Neck injuries in football players. Clin Sports Med 1986;5:215-246. Torg JS, Lasgow SG: Criteria for return to contact activities following cervical spine injury. Clin Sports Med 1991;1:12-26.
Question 10
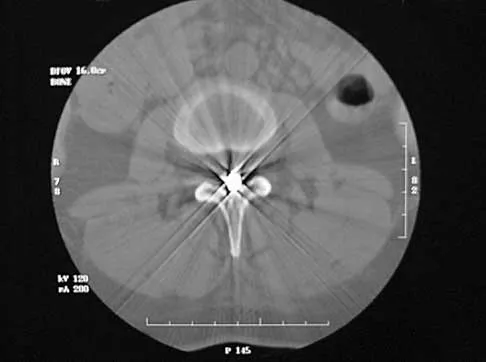
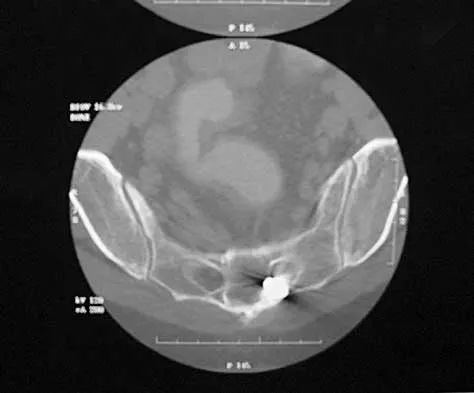
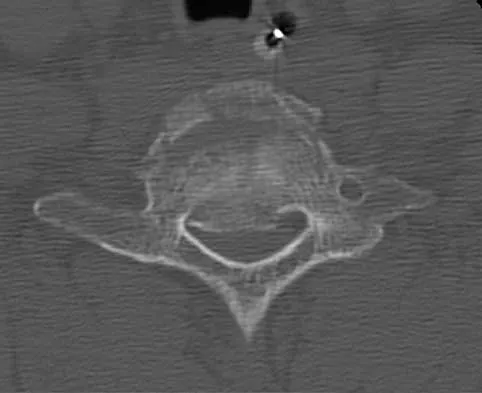
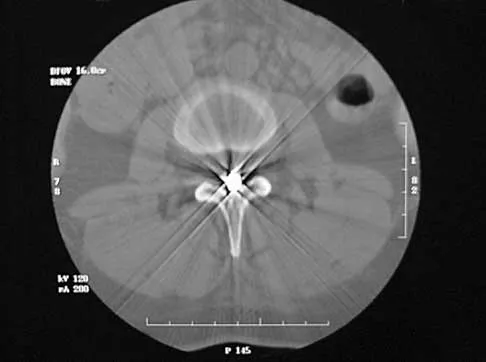
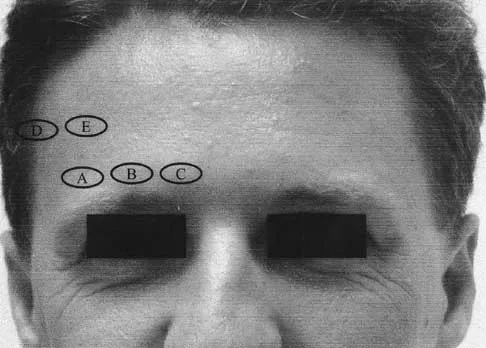
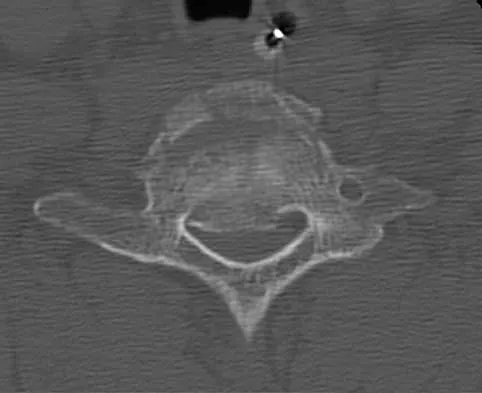
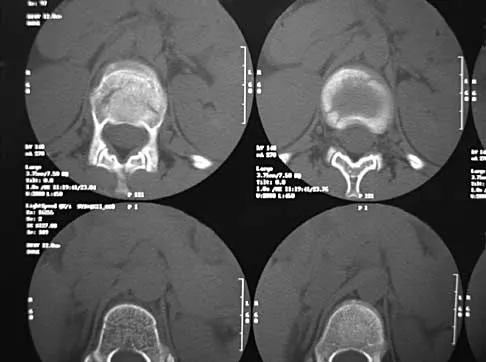
A 40-year-old woman has local back pain and intense burning pain in her perianal region after being shot twice in the back. Motor and sensory examination of her lower extremities reveals no apparent deficit. She has present but decreased sensation in her perianal region, an intact anal wink, good rectal tone, and an intact bulbocavernosus reflex. Radiographs and CT scans are shown in Figures 3a through 3d. What is the next most appropriate step in management?



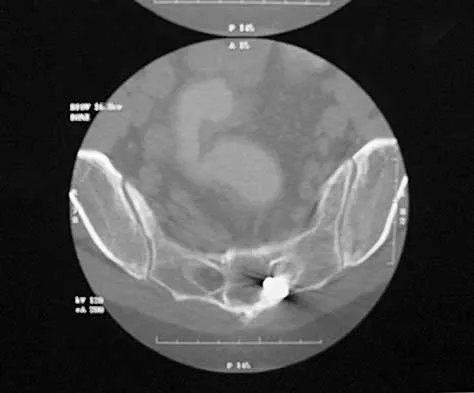
Explanation
3b 3c 3d Because the patient has an apparent compressive neuropathy secondary to the metallic fragments, removal of the fragments in this incomplete lesion at the cauda equina level can be expected to improve her sensory dysesthesias and pain. Steroids are not indicated in a root lesion secondary to a penetrating injury. MRI will have significant artifact effect and will not provide much additional information. The posterior bony elements are not significantly injured; therefore, stabilization is not indicated. Bracken MB, Shepard MJ, Holford TR: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. JAMA 1997;277:1597-1604. Waters RL, Adkins RH: The effects of removal of bullet fragments retained in the spinal canal: A collaborative study by the National Spinal Cord Injury Model Systems. Spine 1991;16:934-939.
Question 11
A patient who sustained injuries in a motorcycle accident 30 minutes ago has significant motor and sensory deficits corresponding to a C6 level of injury. A lateral radiograph obtained during the initial on-scene evaluation reveals bilateral jumped facets at C5-C6; this appears to be an isolated injury. The patient is awake and alert. The next step in management of the dislocation should consist of


Explanation
Surgical open reduction may increase the neurologic deficit if a disk herniation exists. Evidence from animal studies suggests that rapid decompression of the spinal cord may improve recovery. Serially increasing traction weight to reduce the dislocation has been shown to be safe when used in patients who are awake. Indications for MRI include patients who are unable to cooperate with serial examinations, the need for open reduction, and progression of deficit during awake reduction. Delamarter RB, Sherman J, Carr JB: Pathophysiology of spinal cord injury: Recovery after immediate and delayed decompression. J Bone Joint Surg Am 1995;77:1042-1049. Star AM, Jones AA, Cotler JM, Balderston RA, Sinha R: Immediate closed reduction of cervical spine dislocations using traction. Spine 1990;15:1068-1072.
Question 12
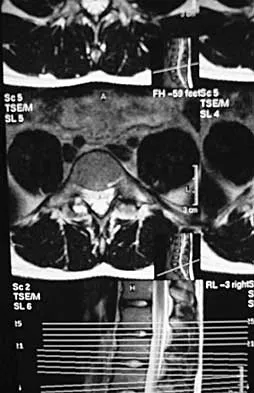
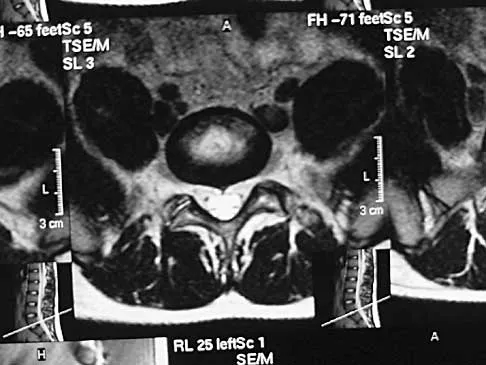
Figure 4 shows the MRI scan of a patient who has had bilateral leg pain, weakness, diffuse numbness, and urinary retention for the past week. Examination reveals that motor strength is diffusely decreased, although it may be secondary to pain. The patient is numb throughout both legs, and reflexes in the lower extremities are absent. Rectal examination shows decreased tone, but voluntary tightening is present. Management should consist of


Explanation
The patient has a cauda equina syndrome. The fact that he has decreased rectal tone and urinary retention suggests the need for urgent surgery. Patients who are left untreated will have a poor prognosis for return of function. Although most patients who have insidious onset of symptoms with urinary retention will regain normal motor function following decompression, nearly one third will continue to have abnormal voiding patterns or sexual dysfunction of varying degrees. Kostuik JP, Harrington I, Alexander D, Rand W, Evans D: Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am 1986;68:386-391.
Question 13
A 62-year-old man has cervical myelopathy with no evidence of cervical radiculopathy. MRI reveals stenosis at C4-5 and C5-6 with severe cord compression. Examination will most likely reveal which of the following findings?



Explanation
Cervical myelopathy involves compression of the spinal cord and presents as an upper motor neuron disorder. Patients commonly have extremity spasticity and problems with ambulation and balance. Hoffman's sign is often present and is elicited by suddenly extending the distal interphalangeal joint of the middle finger; reflexive finger flexion represents a positive finding. The extremities are usually hyperreflexic with myelopathy. With cervical radiculopathy (lower motor neuron disorder), reflexes are hyporeflexic, and patients report pain along a dermatomal distribution. A hyperactive jaw jerk reflex indicates pathology above the foramen magnum or in some cases, systemic disease. Flaccid paraparesis suggests a lower motor neuron problem. Sachs BL: Differential diagnosis of neck pain, arm pain and myelopathy, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 741-742.
Question 14
A patient who has had neck pain radiating down the arm for the past 4 weeks reports that the pain was excruciating during the first week. Management consisting of anti-inflammatory drugs and physical therapy has decreased the neck and arm symptoms from 10/10 to 3/10. He remains neurologically intact. MRI and CT scans are shown in Figures 5a and 5b. The best course of action should be





Explanation
5b Although the patient has a large herniated nucleus pulposus, the pain has decreased from 10/10 to 3/10 over a 4-week period and the patient is now free of any neurologic symptoms. It is quite likely that further nonsurgical management will continue to resolve his symptoms. In the absence of any neurologic deficits, there is no evidence that the patient is at significant risk for paralysis. Saal JS, Saal JA, Yurth EF: Nonoperative management of herniated cervical intervertebral disc with radiculopathy. Spine 1996;21:1877-1883.
Question 15
Examination of a supine patient in which the hip is abducted, externally rotated, and flexed is referred to as
Explanation
During Patrick's test, also known as the FABER test, the flexed, abducted, and externally rotated hip is positioned to isolate sacroiliac pathology. Back pain with this test is not considered diagnostic. With Kernig's sign, the spinal cord is placed on stretch, eliciting root or meningeal irritation by forcibly flexing the patient's head and neck with his or her hands clasped behind the head. For Lasegue's sign, the patient performs a straight leg raise with the immobile hip already held in flexion. The femoral stretch test can be performed in the prone position or side lying, but the hip is held in extension while the knee is flexed, testing for femoral neuritis. Watkins RG: History, physical examination, and diagnostic tests for back and lower extremity problems, in Watkins RG (ed): The Spine in Sports. St Louis, MO, Mosby, 1996, Chapter 7.
Question 16
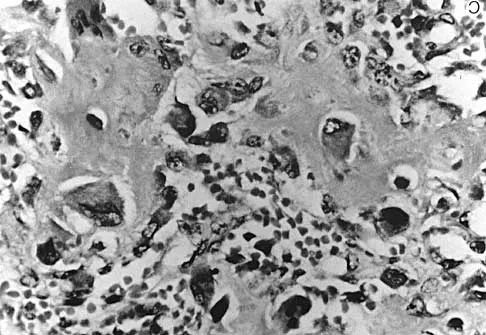
During the evaluation of a patient suspected of having a lumbar disk herniation, T1- and T2-weighted MRI scans reveal a hyperintence lobular, well-defined lesion in the L2 vertebral body. What is the most likely diagnosis?

Explanation
The findings are characteristic of hemangioma. When the hemangioma is large enough, vertical striations may be visible on plain radiographs. Axial CT scans commonly reveal a speckled appearance. Metastatic lesions are typically hypointense on T1-weighted images because they replace the fatty marrow. Bony islands, like cortical bone, are dark on T1- and T2-weighted images. Intravertebral disk herniation would have characteristics similar to the disk and be in continuity with the disk. Osteoporosis is more diffuse. Ross JS, Masaryk TJ, Modic MT, Carter JR, Mapstone T, Dengel FH: Vertebral hemangiomas: MR imaging. Radiology 1987;165:165-169.
Question 17
A 32-year-old man notes increasing back pain and progressive paraparesis over the past few weeks. He is febrile, and laboratory studies show a WBC of 12,500/mm3. MRI scans are shown in Figures 6a and 6b. Management should consist of



Explanation
6b Indications for surgery in spinal infections include progressive destruction despite antibiotic treatment, an abscess requiring drainage, neurologic deficit, need for diagnosis, and/or instability. This patient has a progressive neurologic deficit. Debridement performed at the site of the abscess should effect canal decompression. Once the debridement is complete back to viable bone, the defect can be reconstructed with a strut graft. Additional posterior stabilization is used as deemed necessary by the degree of anterior destruction. CT-guided needle aspiration, while occasionally useful in the earliest phases of an infection, produces frequent false-negative results and would provide little useful information in the management of this patient. Emery SE, Chan DP, Woodward HR: Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine 1989;14:284-291. Lifeso RM: Pyogenic spinal sepsis in adults. Spine 1990;15:1265-1271.
Question 18
A 21-year-old woman with Marfan syndrome is seeking evaluation of her scoliosis. She reports no back or leg pain, and the neurologic examination is normal. Lateral and bending radiographs are shown in Figures 7a through 7e. Management should consist of






Explanation
7b 7c 7d 7e Because the patient's thoracolumbar scoliosis is of a large enough magnitude, observation or bracing is not recommended. The thoracolumbar curve is flexible enough and L4 corrects well enough to the pelvis to consider anterior spinal fusion from T10 to L4. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 161-171. Turi M, Johnston CE II, Richards BS: Anterior correction of idiopathic scoliosis using TSRH instrumentation. Spine 1993;18:417-422.
Question 19
Which of the following substances is least likely to affect the success of bone union after lumbar arthrodesis?

Explanation
Much attention has been given to the use of supplemental postoperative analgesia with nonsteroidal anti-inflammatory drugs (NSAIDs), and a significant reduction in narcotic use has been recorded. However, a high failure rate of arthrodesis has been associated with the use of postoperative NSAIDs. Glassman and associates reported 29 cases of pseudarthrosis in 167 patients when ketorolac was used as a postoperative analgesic, whereas only five fusion failures were noted in 121 patients not using ketorolac. Indomethacin and ibuprofen have been shown to adversely affect bone formation in clinical and animal trials. Nicotine has also been shown in a number of studies to decrease the fusion rate. Oxycodone hydrochloride is a synthetic morphine and does not affect the fusion process. Glassman SD, Rose SM, Dimar JR, Puno RM, Campbell MJ, Johnson JR: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838. Deguchi M, Rapoff AJ, Zdeblick TA: Posterolateral fusion for isthmic spondylolisthesis in adults: Analysis of fusion rate and clinical results. J Spinal Disord 1998;11:459-464.
Question 20
A 33-year-old woman sustains a C6 burst fracture diving into a swimming pool, resulting in a complete spinal cord injury. The canal compromise is shown in Figures 8a and 8b. Functional recovery would be maximized with



Explanation
8b Although the patient has sustained a complete spinal cord injury, an anterior decompression, even performed late, can gain an additional level of root function. In the quadriplegic patient, this can mean the difference between dependent and independent function. Posterior procedures do not afford adequate access to the retropulsed bony fragments compromising the canal. Bohlman HH, Anderson PA: Anterior decompression and arthrodesis of the cervical spine: Long-term motor improvement. Part I: Improvement in incomplete traumatic quadriparesis. J Bone Joint Surg Am 1992;74:671-682.
Question 21
In the upright standing position, approximately what percent of the vertical load is borne by the lumbar spine facet joints?


Explanation
Direct measurement and finite element modeling results show that approximately 20% of the vertical load is borne by the posterior structures of the lumbar spine in the upright position. Adams MA, Hutton WC: The effect of posture on the role of the apophyseal joints in resisting intervertebral compressive forces. J Bone Joint Surg Br 1980;62:358-362.
Question 22
A 40-year-old patient who has a type II odontoid fracture is placed in a halo vest for 12 weeks; however, current radiographs show no evidence of healing. The next most appropriate step in management should consist of


Explanation
Because nonsurgical managment has failed and a significant number of type II odontoid fractures will go on to a nonunion, the salvage treatment of choice is posterior fusion at C1-2. Odontoid screws are contraindicated in patients with a chronic nonunion, which this patient has at the end of 3 months. Montesano PX: Anterior and posterior screw and plate techniques used in the cervical spine, in Bridwell KH, DeWald RL (eds): The Textbook of Spinal Surgery, ed 2. Philadelphia, PA, Lippincott-Raven, 1996, vol 2, pp 1743-1761. Bohler J: Anterior stabilization for acute fractures and non-unions of the dens. J Bone Joint Surg Am 1982;64:18-27.
Question 23
In the initial evaluation of acute low back pain (duration of less than 4 weeks), plain radiographs are recommended in which of the following situations?



Explanation
Prolonged use of steroids is associated with compression fractures with minimal trauma. Indications for radiography with acute low back pain include possible tumor, fracture, infection, or cauda equina syndrome. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, Appendix A15.
Question 24
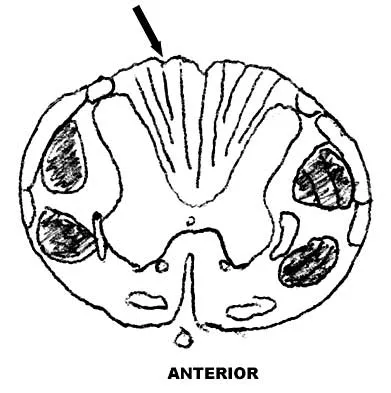
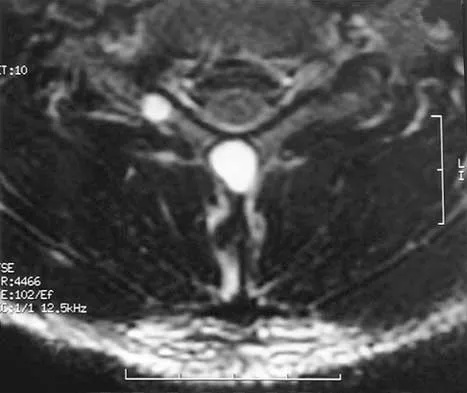
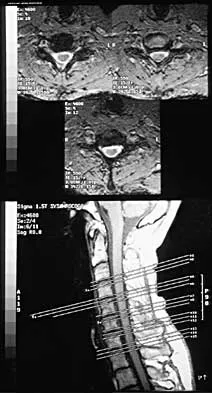
Figure 9 shows a cross-sectional view of the spinal cord at the lower cervical level. Injury to the structure indicated by the black arrow will lead to what neurologic deficit?

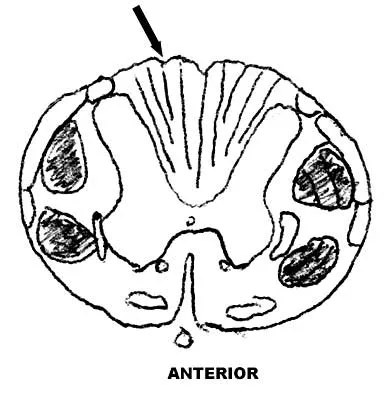
Explanation
The arrow is pointing to the posterior columns of the spinal cord that transmit position sense, vibratory sense, and proprioception. There are no motor tracts in the posterior columns. Bohlman H, Ducker T, Levine A: Spine trauma in adults, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 911.
Question 25
A 26-year-old woman who noted right-sided lumbosacral pain 10 days ago while vacuuming now reports that the pain has intensified. She denies any history of back problems. No radicular component is present, and her neurologic examination is normal. The next most appropriate step in management should consist of



Explanation
The initial management of a lumbar strain should consist of 2 to 3 days of bed rest when symptoms are severe, activity restrictions, and nonsteroidal anti-inflammatory drugs. It has been estimated that 60% to 80% of the adult population experiences back pain, with 2% to 5% affected yearly. Spontaneous improvement generally will occur within 4 weeks. Further study is indicated by the presence of radiculopathy, weakness, trauma, or suspicion of malignancy. Bigos S, Boyer O, Braen GR, et al: Acute low back pain in adults: Clinical practice guideline No. 14. AHCPR Publication No. 95-0642. Rockville, MD, Agency for Health Care Policy and Research, Public Health Service, US Department of Health and Human Services, December, 1994.
Finish Exam?
You cannot change answers after submitting.
