Question 51
Flexion and extension of the elbow occur about an axis of rotation that

Explanation
The elbow mimics a true hinge and flexes and extends around an axis that is centered in the centers of the trochlea and capitellum. The medial epicondyle is not perfectly isometrically placed; rather the axis of rotation passes through a point on the anteroinferior aspect of the medial epicondyle. Application of a hinged external fixator is possible because of the fact that there is a single axis of rotation. Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 53-54. London JT: Kinematics of the elbow. J Bone Joint Surg Am 1981;63:529-535.
Question 52
Figure 27 shows the radiograph of a 26-year-old man who sustained a closed head injury and a closed elbow dislocation 6 weeks ago. Examination reveals 65 degrees to 115 degrees of flexion, and intensive physical therapy has resulted in no improvement. A decision regarding the timing of surgical correction of the contracture should be based on


Explanation
The patient has heterotopic ossification, a more common finding in patients who have sustained head injuries. Treatment will require removal of the heterotopic bone and anterior and posterior capsulectomies. The main concern about timing is the possible recurrence of heterotopic bone. While an extended wait was once thought necessary, this is no longer true. The timing is based on the time since injury and evidence of bone maturation on plain radiographs. A sharp marginal demarcation of the new bone and a trabecular pattern within it are usually present 3 to 6 months after onset, indicating that it is safe to proceed with surgical excision. It is not necessary to wait more than 6 months. Bone scan results are not good indicators because they may remain "hot" for long periods of time. The levels of alkaline phosphatase and serum calcium-phosphorus product do not need to be measured.
Question 53
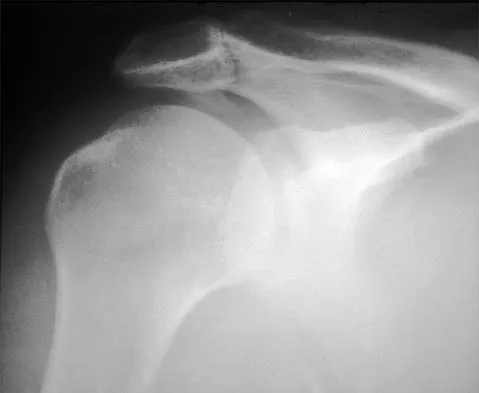
A 70-year-old man who underwent an uncomplicated large rotator cuff repair 6 months ago is now seeking a second opinion regarding persistent pain and weakness in his shoulder. Examination reveals that his incision is well healed and unreactive. The surgical report suggests that the tendons were secured back to bone with sutures through the greater tuberosity. Figure 28 shows a radiograph that was obtained 1 week ago. What is the most likely diagnosis?

Explanation
Symptoms can persist following a rotator cuff repair for a variety of reasons. In the early postoperative period, infection is the primary concern. Stiffness and loss of motion can occur because of postoperative scarring. Complex regional pain syndrome can occur but is rare, and the diagnosis is not made with a plain radiograph. This radiograph shows a superiorly migrated humeral head that articulates with the acromion, indicating that the repair has failed. While large to massive tears may fail more commonly than once thought, the clinical outcome may be satisfactory in many patients. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213.
Question 54
A 29-year-old man who lifts weights states that he injured his left shoulder while performing a bench press 2 days ago. The following morning he noted ecchymosis and swelling in the left chest wall. Examination reveals ecchymosis and tenderness and deformity in the left anterior chest wall and axillary fold that is accentuated with resisted adduction of the arm. Passive range of motion beyond 90 degrees of forward flexion and 45 degrees of external rotation is extremely painful. Glenohumeral stability is difficult to assess because of severe guarding. Figure 29 shows an MRI scan. Management should consist of

Explanation
Rupture of the pectoralis major tendon most commonly occurs during bench pressing. Wolfe and associates have shown that the most inferiorly located fibers of the sternal head lengthen disproportionately during the final 30 degrees of humeral extension during the bench press. This creates a mechanical disadvantage in the final portion of the eccentric phase of the lift; with forceful flexion of the shoulder these maximally stretched fibers may rupture. In most patients, particularly in young athletes, the treatment of choice is anatomic repair of the ruptured tendon to its insertion in the proximal humerus either with suture anchors or transosseous sutures. Following surgery, most patients experience a near normal return of strength and significant improvement in the cosmetic appearance of the deformity. While more technically challenging, repair of chronic rupture is possible and is indicated in some patients. Wolfe SW, Wickiewicz TL, Cavanaugh JT: Ruptures of the pectoralis major muscle: An anatomic and clinical analysis. Am J Sports Med 1992;20:587-593.
Question 55
What range of motion parameters are required for a patient with posttraumatic elbow stiffness to accomplish all the normal activities of daily living?
Explanation
Activities of daily living such as dressing, eating, and bathing can all be performed with elbow motion through a 100 degrees arc of flexion and extension (30 degrees to 130 degrees) and a 100 degrees arc of forearm rotation (50 degrees pronation, 50 degrees supination). Some patients can accomplish these activities of daily living with 10 degrees less motion at each end point. This is referred to as the functional arc of motion. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 56
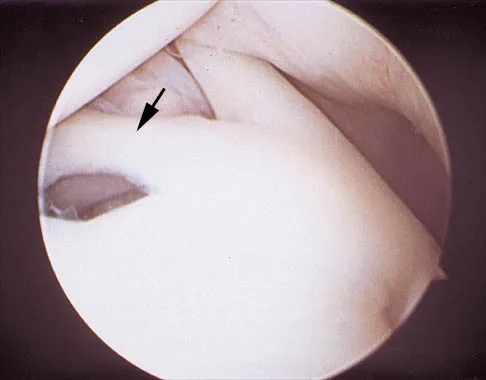
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
Explanation
The photograph shows a normal variant that is a sublabral hole beneath the anterosuperior labrum. In some instances, the labrum will become confluent with the middle glenohumeral ligament as a stout band. Because this variant is not abnormal, no treatment is necessary. Securing this portion of the labrum to the capsule may tighten the middle glenohumeral ligament complex and restrict external rotation of the arm. Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Question 57
The use of a screw between the clavicle and the coracoid process to maintain the clavicle and acromioclavicular (AC) joint in a reduced position is a treatment option for AC joint separations. Screw removal is generally recommended after soft-tissue healing. What effect does this rigid coracoclavicular fixation have on shoulder kinematics?
Explanation
This issue has been debated since Inman published his classic study on clavicular rotation in 1944. Subsequently, it has been shown by several authors that the clinical evaluation of patients with either coracoclavicular screws in place or with arthrodesis of the coracoclavicular reveals little to no loss of shoulder motion. This is most likely the result of synchronous motion of the scapula and clavicle in shoulder movements. Flatow EL: The biomechanics of the acromioclavicular, sternoclavicular, and scapulothoracic joints. Instr Course Lect 1993;42:237-245. Kenedy JC, Cameron H: Complete dislocation of the acromioclavicular joint. J Bone Joint Surg Br 1954;36:202-208. Rockwood CA Jr, Williams GR, Young CD: Disorders of the acromioclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 483-553.
Question 58
Figure 31 shows the AP and lateral radiographs of the elbow of a 56-year-old man with chronic polyarticular rheumatoid arthritis. His function continues to be limited by pain with activities of daily living. Examination shows that his total arc of motion is 110 degrees. Nonsurgical management has failed to provide relief. Treatment should now consist of

Explanation
A semiconstrained prosthesis can provide excellent results in carefully selected patients. Because the radiographs show extensive joint destruction with loss of the capitellum and trochlea, a capitellocondylar total elbow (unconstrained) prosthesis is contraindicated. Elbow fusion is poorly accepted, and the radiographs show too much articular destruction for a radial head excision, synovectomy, or interposition arthroplasty to be effective. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 59
A 12-year-old pitcher has had a 2-month history of pain in his right dominant shoulder after throwing. He reports that the pain has gradually progressed to the point where he cannot throw without pain. He also notes that the pain now awakens him at night if he has been active. Anti-inflammatory drugs have failed to provide relief. Examination reveals no abnormalities except for some localized tenderness over the proximal humerus. Figures 32a and 32b show radiographs of both shoulders. What is the most likely diagnosis?


Explanation
32b The history, examination, and radiographs are pathognomonic for Little League shoulder, a stress syndrome of the proximal humeral physis caused by overuse. Complete fracture rarely occurs, and recovery usually occurs with rest. Night pain is always a serious concern and further work-up is needed if the patient does not respond to activity modification. Occult instability is not a real concern in this patient, although it should be included in the differential diagnosis. Albert MJ, Drvaric DM: Little League shoulder: Case report. Orthopedics 1990;13:779-781.
Question 60
Which of the following ligaments is the primary static restraint against inferior translation of the arm when the shoulder is in 0 degrees of abduction?
Explanation
The superior glenohumeral ligament (SGHL) and coracohumeral ligament serve as primary static restraints against inferior translation of the arm when the shoulder is in 0 degrees of abduction. Of these, the coracohumeral ligament has been shown to have a greater cross-sectional area, greater stiffness, and greater ultimate load than the SGHL. The inferior glenohumeral ligament plays a greater stabilizing role with increasing abduction of the arm. The coracoacromial ligament may help provide superior stability, especially when the rotator cuff is deficient. The coracoclavicular ligaments stabilize the acromioclavicular joint. Boardman ND, Debski RE, Warner JJ, et al: Tensile properties of the superior glenohumeral and coracohumeral ligaments. J Shoulder Elbow Surg 1996;5:249-254.
Question 61
A 16-year-old high school student undergoes a routine preparticipation physical examination at the beginning of the school year. Examination reveals marked laxity of both shoulders but only mild generalized laxity in other joints. The load and shift test allows for anterior humeral translation to the glenoid rim and posterior humeral translation beyond the glenoid rim. The sulcus sign is present. What is the next most appropriate step in management?
Explanation
This patient has shoulder laxity without apprehension. Because there is a wide range of normal laxity in asymptomatic shoulders, the physician should inform the student of these findings, recommend shoulder strengthening exercises, and allow unrestricted sports participation unless symptoms develop. Harryman DT, Sidles JA, Harris SL, Matsen FA III: Laxity of the normal glenohumeral joint: A quantitative in vivo assessment. J Shoulder Elbow Surg 1992;1:66-76. Hawkins RJ, Bokor RJ: Clinical evaluation of shoulder problems, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, p 186. McFarland EG, Campbell G, McDowell J: Posterior shoulder laxity in asymptomatic athletes. Am J Sports Med 1996;24:468-471.
Question 62
A 21-year-old professional baseball player has had painful catching and stiffness in his dominant right elbow for the past year. Examination reveals a flexion contracture of 2 degrees and mild pain with full elbow flexion. Radiographs are shown in Figures 33a and 33b. The most effective management should consist of


Explanation
33b The radiographs show osteochondritis dissecans of the capitellum and a loose body in the anterior compartment. Arthroscopic removal is indicated because symptoms referable to the loose body are present. Baumgarten TE: Osteochondritis dissecans of the capitellum. Sports Med Arthroscopy Rev 1995;3:219-223.
Question 63
A 42-year-old patient has had painful inferior subluxation of the glenohumeral joint following a recent cerebrovascular accident (CVA). Figure 34 shows the AP radiograph of the shoulder. Management should consist of

Explanation
Following a CVA and with the resumption of upright posture, downward subluxation of the glenohumeral joint may occur. Although usually painless, some patients may report pain secondary to stretching of the brachial plexus. This is the result of flaccid paralysis of the deltoid muscle, and it will persist until some motor tone or spasticity returns to the shoulder girdle musculature. Early sling support and range-of-motion exercises to prevent contracture will provide the best relief. Surgical procedures are not indicated. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 64
A 50-year-old man who underwent an arthroscopic rotator cuff repair 5 days ago now returns for an early postoperative follow-up because of increasing pain in his shoulder. He reports increasing malaise and has a low-grade fever. Examination reveals no redness or swelling, but he has scant serous drainage from the posterior portal. An emergent Gram stain is positive for gram-positive cocci. The next most appropriate step in management should consist of
Explanation
An infection of the shoulder is considered a surgical emergency unless there are medical reasons that a patient cannot be taken to the operating room. If cultures of wound drainage are in question, then an aspiration should be done emergently, not several days later. The hallmark of infection in any major joint is increasing pain out of proportion to what is expected. Drainage occurring 1 to 2 days after an arthroscopic procedure is not normal, and it should be aggressively treated. Delay in diagnosis can result in sepsis and on a delayed basis, postinfectious arthritis. Both the glenohumeral joint and the subacromial space require debridement and irrigation, followed by antibiotics after both areas are cultured. Mansat P, Cofield RH, Kersten TE, Rowland CM: Complications of rotator cuff repair. Orthop Clin North Am 1997;28:205-213. Settecerri JJ, Pitner MA, Rock MG, Hanssen AD, Cofield RH: Infection after rotator cuff repair. J Shoulder Elbow Surg 1999;8:1-5. Ward WG, Eckardt JJ: Subacromial/subdeltoid bursa abscesses: An overlooked diagnosis. Clin Orthop 1993;288:189-194.
Question 65
A 42-year-old man who is right-hand dominant injured his right shoulder when he fell from a ladder onto his outstretched arm 1 hour ago. Radiographs reveal a two-part greater tuberosity anterior fracture-dislocation. Initial management should consist of
Explanation
Greater tuberosity anterior fractures associated with anterior glenohumeral dislocations respond very well to closed methods in the majority of patients. Closed reduction of the glenohumeral joint often anatomically reduces the greater tuberosity into its cancellous bed, without the need for open fixation or cuff repair. Once closed reduction of the joint is performed, tuberosity displacement and joint articulation should be evaluated radiographically with AP and scapular lateral views as well as an axillary view. The axillary view will not only definitively show the joint articulation but also demonstrate posterior displacement of the greater tuberosity missed on the AP and lateral views. If no or minimal (5 mm) displacement is found, then nonsurgical management consisting of a sling and gentle passive range-of-motion exercises can be instituted. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 66
A 19-year-old man who plays college volleyball undergoes a routine preparticipation physical examination. Figure 35 shows a posterior view of his dominant shoulder. An electromyogram shows that this is a chronic injury, and an MRI scan shows no abnormalities. The best course of action should be

Explanation
Isolated palsy of the infraspinatus portion of the suprascapular nerve is common in volleyball players and is seen frequently in the throwing arm of baseball players. The exact cause is not known, but it may be the result of either tethering or traction on the nerve at the spinoglenoid notch. Synovial cysts in the spinoglenoid notch also can be a cause, but the patient's negative MRI findings rule out that entity. Because many isolated nerve palsies of the infraspinatus branch are asymptomatic, initial management should always be nonsurgical. Surprisingly, many athletes with this injury can participate fully in sports. Surgical treatment with decompression at the notch is unpredictable and generally is indicated only if nonsurgical management fails. Ferretti A, Cerullo G, Russo G: Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am 1987;69:260-263.
Question 67
A 59-year-old construction worker who is right-hand dominant has had right shoulder pain for the past 9 months with no history of injury. Nonsurgical management consisting of two cortisone injections, physical therapy for 3 months, and nonsteroidal anti-inflammatory drugs has failed to provide lasting relief. Examination reveals tenderness over the acromioclavicular (AC) joint and over the subacromial bursa. He has positive Neer and Hawkins impingement signs and AC joint pain with adduction of the shoulder. Radiographs are shown in Figures 36a and 36b. An MRI scan reveals an intact rotator cuff. Management should now consist of

Explanation
36b Because the patient has clinical and radiographic signs of AC arthritis and subacromial impingement, the treatment of choice is anterior acromioplasty and distal clavicle excision. Arthroscopic acromioplasty alone would not address the AC arthritis. The rotator cuff is intact; therefore, rotator cuff repair is not indicated. An open Mumford procedure would address the AC arthritis only and not the impingement symptoms. Immobilization might lead to stiffness of the shoulder and is not recommended for treating impingement.
Question 68
What three structures are considered the primary constraints necessary for elbow stability?
Explanation
The three primary constraints necessary for elbow stability in all directions are the ulnar part of the lateral collateral ligament (also called the lateral ulnar collateral ligament), the anterior band of the medial collateral ligament, and the coronoid. The radial head and capsule are secondary constraints to elbow instability. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 69
A 68-year-old woman has been progressing slowly after undergoing humeral head replacement for a four-part fracture 3 months ago. She has not regained active elevation, she feels an audible clunk on attempting elevation, and she reports pain and weakness. She used a sling for 2 weeks in the immediate postoperative period. Radiographs are shown in Figure 37a through 37c. Management should consist of


Explanation
37b 37c Immediate repair of the tuberosity and rotator cuff is recommended on identifying the avulsion or nonunion. Revising the humeral component to increase tension and length will overtighten the cuff and increase the chance of tuberosity pull-off. The glenoid is uninvolved and should not be replaced. Attempts to strengthen the rotator cuff will be unsuccessful because the insertions are no longer attached to the humerus when the tuberosities avulse. Brown TD, Bigliani LU: Complications with humeral head replacement. Orthop Clin North Am 2000;31:77-90.
Question 70
What is the most important feature in choosing an outcome instrument to assess shoulder disorders?
Explanation
There has been a recent increase in the use of outcome instruments to document and measure effects of treatment of medical conditions, including shoulder disorders. The most important feature of an instrument is whether it actually measures what it purports to measure; this is defined as its validity. Leggin BG, Iannotti JP: Shoulder outcome measurement, in Iannotti JP, Williams GR (eds): Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, p 1027.
Question 71
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in

Explanation
The elbow dislocates by a three-dimensional movement of supination and valgus during flexion. Additional trauma during reduction is minimized by recreating the deformity and reducing the elbow in supination. The actual maneuver includes full supination (actually hypersupination) of the elbow in a valgus position. This is followed by pushing the olecranon distally in line with the long axis of the ulna while swinging the elbow into varus, and then relaxing the supination torque. Postreduction stability is enhanced in pronation, except when the soft-tissue disruption is extensive. O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 414.
Question 72
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
In the study done by Pevny and associates, 35% of patients older than age 40 years sustained rotator cuff tears and 8% had axillary nerve palsies. All of the patients with axillary nerve palsy also had rotator cuff tears. Imaging of the rotator cuff is indicated in this age group. The incidence of recurrent instability in patients older than age 40 years is 10% to 15%. Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294. Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Question 73
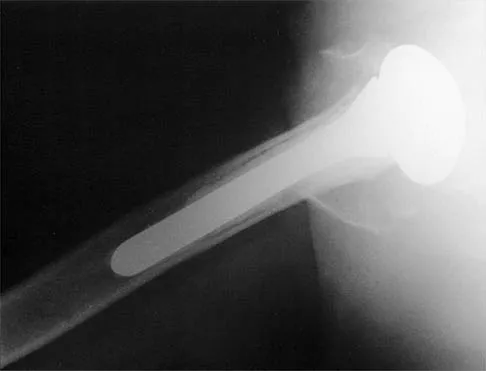
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and

Explanation
An unconstrained prosthesis dislocation is a disconcerting problem that is not easily resolved; however, revision to a semiconstrained prosthesis would best achieve both pain relief and stability. Removal of the components and distraction arthroplasty or conversion to a resection arthroplasty are options, but the results would be unpredictable with regards to pain relief, postoperative motion, or elbow stability. Arthrodesis is poorly tolerated. With revision to another unconstrained prosthesis, there is the risk of continued redislocation because of chronic ligamentous insufficiency. Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Question 74
A 67-year-old woman undergoes a revision total shoulder arthroplasty for replacement of a loose glenoid component. Examination in the recovery room reveals absent voluntary deltoid and triceps contraction, weakness of wrist and thumb extension, and absent sensation in the palmar aspect of all fingertips and the radial forearm. The next most appropriate step in management should consist of
Explanation
Neurologic injury after shoulder replacement is relatively uncommon, occurring in 4% of shoulders in one large series. The importance of identifying and protecting the musculocutaneous and axillary nerves cannot be overemphasized; it is especially critical during revision arthroplasty when the normal anatomic relationships have been distorted. The long deltopectoral approach leaving the deltoid attached to the clavicle was found to be significant in the development of postoperative neurologic complications. A correlation was found between surgical time and postoperative neurologic complications, with long surgical times being associated with more neurologic complications. The presumed mechanism of injury is traction on the plexus that occurs during the surgery. A neurologic injury after total shoulder arthroplasty usually does not interfere with the long-term outcome of the arthroplasty itself; it is best managed by protective measures with passive range of motion of the involved extremity. Wirth MA, Rockwood CA Jr: Complications of shoulder arthroplasty. Clin Orthop 1994;307:47-69.
Question 75
Figure 40 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. Closed reduction is readily accomplished, and the elbow seems stable. Management should now consist of application of a splint for

Explanation
Flexion contractures are the most common complication of elbow dislocations. About 15% of patients lose more than 30 degrees of flexion. The risk of contracture is proportional to the duration of immobilization. Elbows should be moved within the first few days after reduction. The splinting is for comfort and protection only while the pain subsides. Mehlhoff TL, Noble PC, Bennett JB, Tullos HS: Simple dislocation of the elbow in the adult: Results after closed treatment. J Bone Joint Surg Am 1988;70:244-249. Linscheid RL, O'Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 441-452. O'Driscoll SW, Jupiter JB, King GJ, Hotchkiss RN, Morrey BF: The unstable elbow. Instr Course Lect 2001;50:89-102.
Finish Exam?
You cannot change answers after submitting.
