Question 1
Which of the following statements best describes why the ulnar nerve is most prone to neuropathy at the elbow?

Explanation
The ulnar nerve is more prone to neuropathy than the radial or median nerves for many reasons. It has the greatest longitudinal excursion required to accommodate elbow range of motion, subjecting it to potential traction forces. The dimensions of the entrance of the cubital tunnel change with elbow motion, potentially causing compression in flexion. For these two reasons, the ulnar nerve is subjected to both compression and traction during elbow motion. Although it passes between two muscle heads as it enters the forearm, so do the median and radial nerves. Finally, the vascular supply is adequate because of the anastamoses between the superior ulnar collateral artery, the posterior ulnar recurrent artery, and the inferior ulnar collateral artery. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 369-378. Prevel CD, Matloub HS, Ye Z, Sanger JR, Yousif NJ: The extrinsic blood supply of the ulnar nerve at the elbow: An anatomic study. J Hand Surg Am 1993;18:433-438.
Question 2
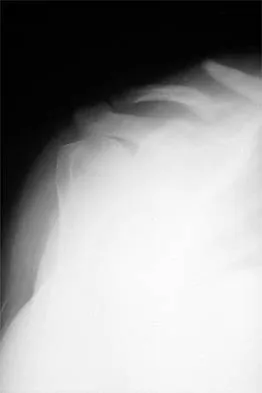
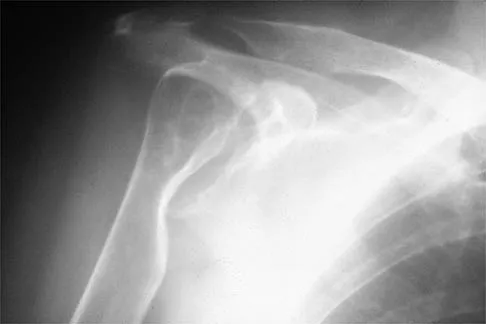
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include

Explanation
Given the size of the rotator cuff tear, it is likely to be repaired; therefore, the treatment of choice is a total shoulder replacement with rotator cuff repair. Severe rotator cuff insufficiency can lead to early glenoid failure because of superior instability, and glenoid resurfacing should be avoided in those instances. Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Question 3
Which of the following is considered the cause of Milwaukee shoulder, a joint disease similar to rotator cuff arthropathy?

Explanation
Neer and associates focused on mechanical and nutritional factors as the etiology of rotator cuff arthropathy. McCarty and associates, in describing a similar syndrome known as Milwaukee shoulder, focused on an inflammatory cause in proposing the pathogenic role of hydroxyapatite, a basic calcium phosphate. Neer CS II, Craig EV, Fukuda H: Cuff-tear arthropathy. J Bone Joint Surg Am 1983;65:1232-1244.
Question 4
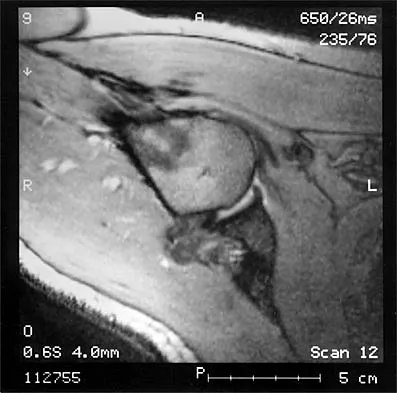
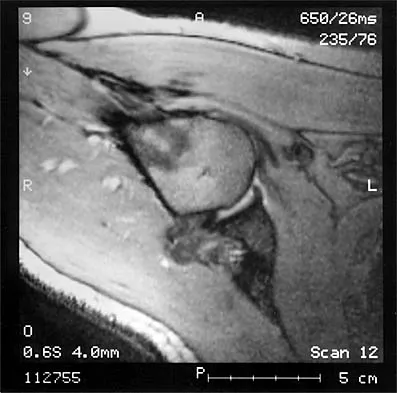
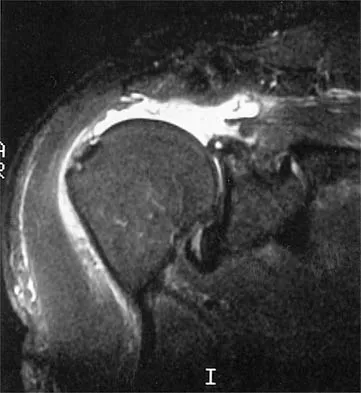
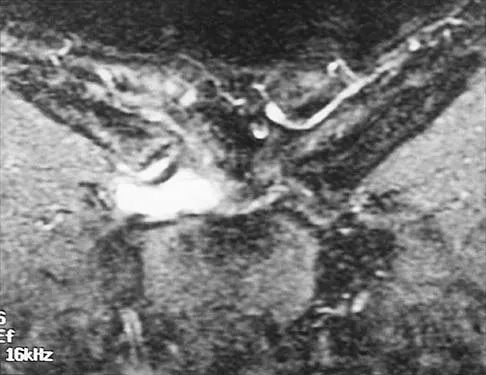
The MRI scan of the shoulder shown in Figure 2 was performed with the arm in abduction and external rotation. The image reveals what condition?


Explanation
Internal impingement of the shoulder is now a well-recognized cause of shoulder pain in the throwing athlete. First described by Walch and associates, it involves contact of the rotator cuff and labrum in the maximally externally rotated and abducted shoulder, such as in the late cocking phase of the throwing motion. Schickendantz and associates have shown this contact to be physiologic in most patients and becoming pathologic with repetitive overhead activity. Schickendantz MS, Ho CP, Keppler L, Shaw BD: MR imaging of the thrower's shoulder: Internal impingement, latissimus dorsi/subscapularis strains, and related injuries. Magn Reson Imaging Clin N Am 1999;7:39-49. Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 5
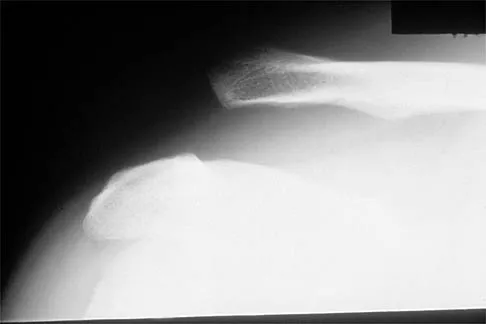
Figure 3 shows the radiographs of a 32-year-old man who fell 12 feet onto his outstretched arm and sustained a fracture-dislocation of the elbow. Initial management consisted of closed reduction of the dislocation. Surgical treatment should now include repair or reduction and fixation of the



Explanation
The radiographs show fractures of the coronoid and radial head. The medial collateral ligament has been avulsed from the ulnar insertion, and there is a valgus opening on the medial side. The lateral collateral ligament is always disrupted in elbow dislocations and fracture-dislocations that occur secondary to falls. This is known as the terrible triad injury (dislocation and fractures of the coronoid and radial head); it has a very poor prognosis because of its propensity for recurrent or persistent instability and late arthritis. The principle in treating this injury is to repair all of the injured parts or protect them with a hinged external fixator until they heal. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294.
Question 6
It is important to avoid which of the following exercises in the immediate postoperative period after humeral head replacement for an acute four-part fracture?


Explanation
It is critical to withhold active range of motion of the shoulder within the first 6 weeks after arthroplasty for acute fracture to prevent tuberosity avulsion. When radiographic and clinical findings show that the tuberosities are healed, active motion may be instituted, usually at 6 to 8 weeks. Immediate passive range-of-motion exercises, including external rotation with a stick, pendulum, and passive elevation, should begin within the limits of the repair on the day of surgery to prevent stiffness. Hartstock LA, Estes WJ, Murray CA, et al: Shoulder hemiarthroplasty for proximal humerus fractures. Orthop Clin North Am 1998;29:467-475.
Question 7
A 38-year-old man has winging of the ipsilateral scapula after undergoing a transaxillary resection of the first rib 3 weeks ago. What is the most likely cause of this finding?

Explanation
During transaxillary resection of the first rib, the long thoracic nerve is at risk as it passes either through or posterior to the middle scalene muscle. Injury to this nerve may occur as the result of overly aggressive retraction of the middle scalene during the procedure. Leffert RD: Thoracic outlet syndrome. J Am Acad Orthop Surg 1994;2:317-325.
Question 8
A 73-year-old man who underwent repair of the left rotator cuff 6 years ago reports good pain relief but notes residual weakness of the left shoulder, especially with overhead tasks. He denies having pain at night and has minimal discomfort with activities of daily living but is dissatisfied with his shoulder strength. Radiographs show an acromiohumeral interval of 2 mm. Appropriate management should consist of
Explanation
An exercise program to strengthen the deltoid and remaining rotator cuff will most likely offer the best results. Revision rotator cuff surgery yields better results in decreasing pain than improving strength and function, and this patient has only minimal pain. Tendon transfers, involving the use of the latissimus dorsi or teres major, have been used when the rotator cuff is deemed irreparable but are not indicated in elderly patients with minimal symptoms. Bigliani LU, Cordasco FA, McIlveen SJ, Musso ES: Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 1992;74:1505-1515. DeOrio JK, Cofield RH: Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am 1984;66:563-567.
Question 9
A 45-year-old woman has had progressive right shoulder pain for the past 6 months. She notes that the pain disrupts her sleep, she has pain at rest that requires the use of narcotic analgesics, and she has limited use of her left shoulder for most activities of daily living. History reveals the use of corticosteroids for systemic lupus erythematosus. Examination shows diminished range of motion. Radiographs of the right shoulder are shown in Figures 4a and 4b. Treatment should consist of




Explanation
4b Humeral arthroplasty provides excellent pain relief and function for stage IV osteonecrosis with humeral collapse. In late disease with glenoid involvement (stage V), total shoulder arthroplasty is preferred. Some authors have reported satisfactory results with core decompression of the humeral head for early stages of osteonecrosis, but results for stage IV osteonecrosis are less satisfactory when compared with those for humeral arthroplasty. Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317. LePorte DM, Mont MA, Mohan V, Pierre-Jacques H, Jones LC, Hungerford DS: Osteonecrosis of the humeral head treated by core decompression. Clin Orthop 1998;355:254-260.
Question 10
The relocation test is most reliable for diagnosing anterior subluxation of the glenohumeral joint when
Explanation
The relocation test is most accurate when true apprehension is produced with the arm in combined abduction and external rotation and then relieved when posterior pressure is placed on the humeral head. Pain with this test is a less specific response and may occur with other shoulder disorders such as impingement.
Question 11
A 16-year-old high school pitcher notes acute pain on the medial side of his elbow during a pitch. Examination that day reveals medial elbow tenderness, pain with valgus stress, mild swelling, and loss of extension. Plain radiographs show closed physes and no fracture. Which of the following diagnostic studies will best reveal his injury?


Explanation
The history and findings are consistent with a diagnosis of a sprain of the medial collateral ligament (MCL) of the elbow; therefore, contrast-enhanced MRI is considered the most sensitive and specific study for accurately showing this injury. Arthroscopic visualization of the MCL is limited to the most anterior portion of the anterior bundle only; complete inspection of the MCL using the arthroscope is not possible. CT without the addition of contrast is of no value in this situation. Use of a technetium Tc 99m bone scan is limited to aiding in the diagnosis of occult fracture, a highly unlikely injury in this patient. There are no clinical indications for electromyography. Timmerman LA, Andrews JR: Undersurface tear of the ulnar collateral ligament in baseball players: A newly recognized lesion. Am J Sports Med 1994;22:33-36. Timmerman LA, Schwartz ML, Andrews JR: Preoperative evaluation of the ulnar collateral ligament by magnetic resonance imaging and computed tomography arthrography: Evaluation of 25 baseball players with surgical confirmation. Am J Sports Med 1994;22:26-32.
Question 12
Figures 5a and 5b show the radiographs of a 45-year-old patient. What is the most likely diagnosis?



Explanation
5b Glenoid dysplasia is an uncommon anomaly that usually has a benign course but may result in shoulder pain, arthritis, or multidirectional instability. Shoulder pain and instability often improve with shoulder strengthening exercises. Wirth MA, Lyons FR, Rockwood CA Jr: Hypoplasia of the glenoid: A review of sixteen patients. J Bone Joint Surg Am 1993;75:1175-1184.
Question 13
A 14-year-old boy sustains a twisting injury to his right shoulder and recalls feeling a snap during a wrestling match. Examination shows hesitancy to raise the arm away from the side, diffuse tenderness and swelling of the upper arm, and no evidence of neurovascular compromise. Figures 6a and 6b show an AP radiograph and MRI scan. What is the most likely diagnosis?



Explanation
6b While difficult to appreciate on the AP radiograph of the shoulder, the increased physeal signal demonstrated on the axial MRI scan is consistent with a nondisplaced growth plate fracture. A comparison radiograph of the left shoulder also could be considered and the injured shoulder evaluated for physeal widening. Proximal humeral fractures in children are somewhat unusual, representing less than 1% of all fractures seen in children and only 3% to 6% of all epiphyseal fractures. Physeal injuries are classified according to the Salter-Harris classification scheme. Salter-Harris type I fractures represent approximately 25% of physeal injuries to the proximal humerus in adolescents. The proximal humeral physis is responsible for 80% of the longitudinal growth of the humerus; therefore, there is tremendous potential for remodeling of fractures in this region. Management for nondisplaced Salter-Harris type I fractures is limited to a short period of immobilization followed by a gradual return to activities as clinical symptoms resolve. Curtis RJ, Rockwood CA Jr: Fractures and dislocations of the shoulder in children, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 991-1007.
Question 14
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of


Explanation
The radiograph shows a displaced type II distal clavicle fracture with nonunion. Because the patient's symptoms are minimal, the injury can be treated like a grade III acromioclavicular separation. Present management should consist of ice, anti-inflammatory drugs, activity modification, and perhaps physical therapy. If nonsurgical management fails to provide relief, the surgical options are varied with no uniformity in the literature regarding surgical treatment of this injury. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Question 15
Figure 8 shows the AP radiograph of a 33-year-old woman who sustained a midshaft clavicle fracture from a motorcycle accident 15 months ago. She continues to have significant pain with activities of daily living. Management should consist of



Explanation
The patient has a symptomatic painful atrophic midclavicular nonunion, and the treatment of choice is rigid internal fixation with a dynamic compression plate and autogenous bone grafting. A tension band effect is desired and achieved by placing the plate superiorly. Excellent success rates of 90% to 100% have been reported using this technique. Intramedullary screw fixation without bone grafting has a decreased success rate. Partial claviculectomy is not a preferred option. Jupiter JB, Leffert RD: Non-union of the clavicle: Associated complications and surgical management. J Bone Joint Surg Am 1987;69:753-760.
Question 16
A 62-year-old patient with rheumatoid arthritis has had pain and instability of the elbow following total elbow replacement 2 years ago. A complete work-up, including aspiration and cultures, is negative. Figures 9a and 9b show the AP and lateral radiographs. Treatment should consist of


Explanation
9b The patient has aseptic loosening of the original semiconstrained prosthesis and significant proximal ulnar bone destruction; therefore, the treatment of choice is revision arthroplasty using a semiconstrained design. Although orthotic stabilization could be used, it will not provide long-term pain relief. Resection arthroplasty after removal of the components may lead to painful instability. Elbow arthrodesis would be difficult with the bone stock loss and is not considered the best option. Two main contraindications to the use of an unconstrained prosthesis are significant bone loss and previous use of a hinged or semiconstrained prosthesis. An ulnar allograft could be combined with the use of a semiconstrained long-stemmed ulnar prosthesis as a treatment modification. Ewald FC, Simmons ED Jr, Sullivan JA, et al: Capitellocondylar total elbow replacement in rheumatoid arthritis: Long-term results. J Bone Joint Surg Am 1993;75:498-507.
Question 17
A 21-year-old football player reports increasing pain and a deformity involving his chest after colliding with another player during a scrimmage. Imaging studies confirm an anterior sternoclavicular dislocation. Management should consist of
Explanation
For the patient with an anterior sternoclavicular dislocation, the most appropriate initial treatment should be symptomatic. Surgical options are usually contraindicated because the incidence of intraoperative and postoperative complications is high. A deformity from an anterior sternoclavicular dislocation is usually well tolerated. Return to play is allowed when symptoms resolve. Rockwood CA Jr: Disorders of the sternoclavicular joint, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 477-525.
Question 18
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should


Explanation
The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results. Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346. Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Question 19
What is the most common contracture deformity of the spastic shoulder secondary to a cerebrovascular accident?


Explanation
The resultant spasticity and weakness (paresis) following a cerebrovascular accident leads to muscle imbalance that commonly results in contracture of the shoulder in adduction, internal rotation, and varying degrees of forward flexion. In addition, the elbow is usually flexed and the forearm pronated. Braun RM, Botte MJ: Treatment of shoulder deformity in acquired spasticity. Clin Orthop 1999;368:54-65.
Question 20
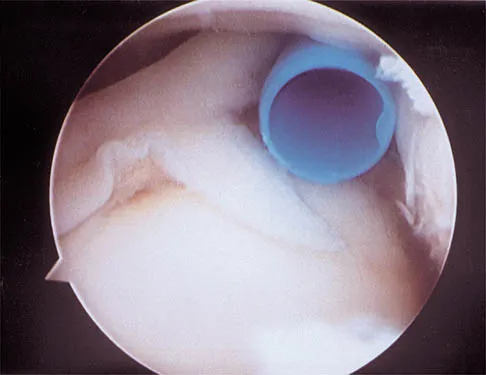
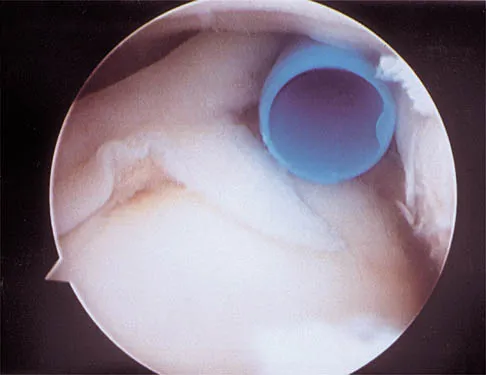
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic


Explanation
The lesion is a variation of a type I superior labrum anterior and posterior lesion; therefore, appropriate treatment is simple debridement. Biceps tenodesis or release is not indicated because the biceps tendon and anchor are intact. There is no indication for labral repair or capsulorraphy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Question 21
After humeral head replacement for four-part fractures, what is the most commonly reported difficulty?

Explanation
Results show that patients who underwent humeral head replacement for fracture almost routinely report pain relief, but functional reports vary. The most commonly reported difficulty is the use of weight in the overhead position with wide variation in active elevation. Factors found to affect active elevation include age, humeral offset, greater tuberosity positioning, and four-part (as compared with three-part) fractures. Goldman RT, Koval KJ, Cuomo F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and fourth-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4:81-86.
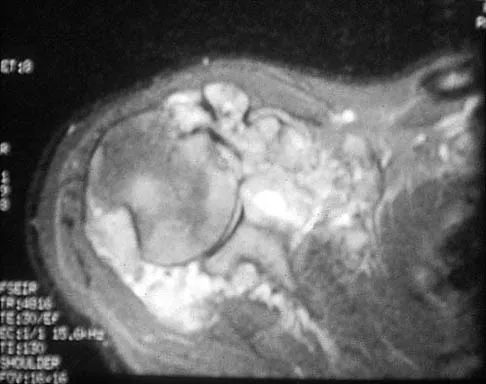
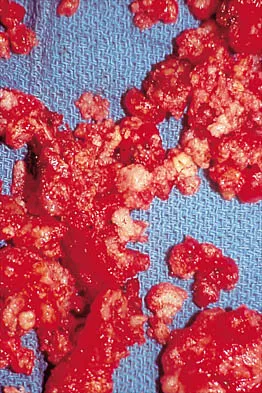
Question 22
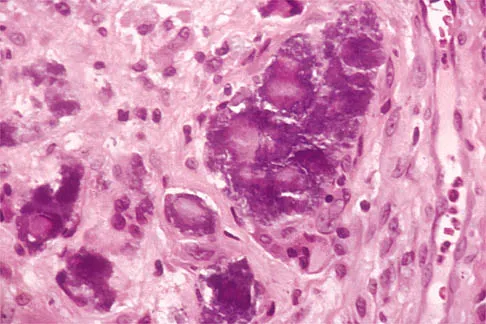
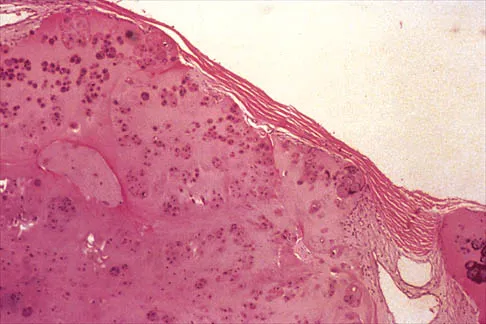
Figures 11a and 11b show the AP and lateral radiographs of a 32-year-old patient on hemodialysis who has increasing elbow pain and a visibly growing mass over the extensor surface. Figure 11c shows the photomicrograph of the biopsy specimen. What is the most likely diagnosis?


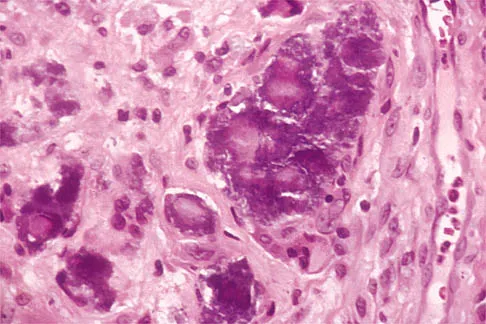

Explanation
11b 11c The radiographic findings are classic for tumoral calcinosis; they are not consistent with myositis ossificans, fungal granuloma, or hemochromatosis. The condition typically appears as large aggregations of dense calcified lobules confined to the surrounding soft tissues. Hyperphosphatemia is a fundamental factor in many patients with this condition. Tumoral calcinosis also occurs in the setting of chronic renal failure when mineral homeostasis is not controlled. The histologic appearance is essentially a foreign body granuloma reaction. Multilocular cysts with purplish amorphous material are surrounded by thick connective tissue capsules. The fibrous walls contain numerous foreign body giant cells. Surgical excision is indicated if the tumor causes discomfort or interferes with function. Sisson HA, Murray RO, Kemp HBS (eds): Orthopaedic Diagnosis: Clinical, Radiological and Pathological Coordinates. New York, NY, Springer-Verlag, 1984.
Question 23
A 52-year-old man who was a former high school pitcher now reports loss of elbow flexion and extension with pain at the extremes of motion. Nonsurgical management has failed to provide relief. Examination reveals movement from 50 degrees to 110 degrees and is painful only at the limits of motion. A radiograph is shown in Figure 12. Treatment should consist of



Explanation
Based on the history, examination, and radiograph, the patient has typical degenerative arthritis of the elbow. This condition is found almost exclusively in men, and there is almost universally a history of repetitive heavy use or overuse of the elbow. Patients report pain at terminal extension and usually have a flexion contracture. Radiographs reveal osteophytes on the coronoid and olecranon and in the coronoid and olecranon fossae. The osteophytes are often associated with loose bodies that sometimes are attached to the soft tissues. Treatment should consist of removal of all loose bodies and impinging osteophytes using open technique or by arthroscopy. The capsular contractures should be released at the same time. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 283-294. Morrey BF: Primary degenerative arthritis of the elbow: Treatment by ulnohumeral arthroplasty. J Bone Joint Surg Br 1992;74:409-413. Redden JF, Stanley D: Arthroscopic fenestration of the olecranon fossa in the treatment of osteoarthritis of the elbow. Arthroscopy 1993;9:14-16.
Question 24
A 79-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing right shoulder pain for the past year, and nonsurgical management has failed to provide relief. Her neurologic examination is entirely normal, but she is unable to elevate her arm against gravity. An AP radiograph is shown in Figure 13. Treatment should consist of

Explanation
Because the patient has end-stage rheumatoid arthritis with glenoid and rotator cuff deficiency, humeral arthroplasty is the treatment of choice. When a patient has an intact rotator cuff and there is sufficient glenoid bone stock to implant a glenoid component, total shoulder arthroplasty is the preferred method because it appears to provide more predictable pain relief. Glenohumeral arthrodesis is generally avoided when there is a functional deltoid or rotator cuff. Open synovectomy is appropriate in early rheumatoid disease before articular changes are present. Anterior acromioplasty with coracoacromial ligament resection is avoided in patients with rheumatoid arthritis because this procedure compromises the coracoacromial arch and may result in anterosuperior instability. Neer CS II, Watson KC, Stanton FJ: Recent experience in total shoulder replacement. J Bone Joint Surg Am 1982;64:319-337. Neer CS II: Glenohumeral arthroplasty, in Neer CS II (ed): Shoulder Reconstruction. Philadelphia, PA, WB Saunders, 1990, pp 143-271. Pollock RG, Deliz ED, McIlveen ST, et al: Prosthetic replacement in rotator cuff deficient shoulders. J Shoulder Elbow Surg 1992;1:173-186.
Question 25
A 22-year-old woman has had progressive upper extremity weakness for the past several years. History reveals no pain in her neck or shoulders. Examination reveals scapular winging of both shoulders and weakness in external rotation. She can abduct to only 120 degrees bilaterally, and there is mild supraspinatus weakness. She is otherwise neurologically intact with normal sensation and reflexes; however, she has difficulty whistling. A clinical photograph is shown in Figure 14. What is the most likely diagnosis?



Explanation
Progressive weakness is a common sign with a large differential diagnosis. Nerve, muscle, and joint problems should be excluded when a patient has diffuse weakness and atrophy. Fascioscapulohumeral dystrophy is a rare disease characterized by facial muscle weakness and proximal shoulder muscle weakness. The weakness is usually bilateral, and scapular winging is common. If the scapular winging becomes pronounced, elevation of the shoulder can be affected. In severe cases, scapulothoracic fusion or pectoralis muscle transfer to the scapula may be indicated. Duchenne muscular dystrophy is typically severe and progressive. The other diagnoses are not compatible with the history or the physical findings. Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Finish Exam?
You cannot change answers after submitting.
