Question 51
Figures 29a and 29b show the radiographs of a 13-year-old competitive gymnast who has had elbow pain for the past 2 weeks. The pain is worse with tumbling activities. Examination reveals a mild effusion and slight limitation of extension and forearm rotation with no locking. Initial management should consist of










Explanation
29b The radiographs show a lesion in the capitellum that is consistent with osteochondritis dissecans. There is no evidence of a loose body at this time. Initial management should consist of cessation of gymnastic activities. Nonsteroidal anti-inflammatory drugs and ice may help to alleviate acute symptoms; most symptoms usually resolve in 6 to 12 weeks. The patient may then begin range-of-motion and strengthening exercises, with a slow return to activities once full range of motion and good strength have been achieved. However, the prognosis for a return to high-level competitive gymnastics is guarded. Surgery is indicated for intra-articular loose bodies, a locked elbow, or failure of nonsurgical management. Surgery may be done either open or arthroscopically. Loose bodies should be removed, and cartilage flaps should be debrided. The results of bone grafting and internal fixation generally have been poor. Drilling the base of the defect may stimulate replacement with fibrocartilage, but the benefits of this procedure are not well documented. Maffulli N, Chan D, Aldridge MJ: Derangement of the articular surfaces of the elbow in young gymnasts. J Pediatr Orthop 1992;12:344-350. Bauer M, Jonsson K, Josefsson PO, Linden B: Osteochondritis dissecans of the elbow: A long-term follow-up study. Clin Orthop 1992;284:156-160.
Question 52
A 12-year-old boy who has had a 1-month history of right thigh pain and a limp reports worsening of the pain after a fall, and he can no longer walk or bear weight on the involved extremity. Radiographs of the pelvis reveal a slipped capital femoral epiphysis with moderate to severe displacement. While positioning the patient on the fracture table for screw fixation, partial reduction of the slip is achieved. No further reduction maneuvers are attempted, and the epiphysis is stabilized with a single cannulated screw. What complication is most likely to develop following this procedure?





Explanation
Traditional classification of slipped capital femoral epiphyses is based on the following temporal criteria: acute (symptoms that persist for less than 3 weeks); chronic (symptoms that persist for more than 3 weeks); or acute on chronic (acute exacerbation of long-standing symptoms). A newer classification differentiates between a stable slip where weight bearing is possible, and an unstable slip if it is not. Reduction of an unstable slip often occurs unintentionally with induction of anesthesia and positioning of the patient for surgery. The rate of satisfactory results is lower primarily because of a much higher incidence of osteonecrosis following internal fixation of an unstable slip. Loder RT, Richards BS, Shapiro PS, Reznick LR, Aronson DD: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Question 53
Figure 30 shows the AP radiograph of a 9-month-old girl who has been referred for evaluation of unequal leg lengths. Examination reveals symmetrical abduction of the hips. When the hips are flexed 90 degrees, the right knee height is greater than the left knee. The girth of the right thigh and calf is larger than the contralateral side. There are no cutaneous lesions, and examination of the spine is normal. The infant is moving all extremities equally and spontaneously. Management should consist of



Explanation
Hemihypertrophy or hemihypotrophy is usually idiopathic, and either the leg or the entire side of the body may be involved. In the infant or young child, it is often difficult to determine which side is abnormal if the condition is mild. Because of the association of Wilms' tumor with hemihypertrophy, these patients should undergo a yearly renal ultrasound until at least age 5 years. Other conditions that may exhibit hemihypertrophy include Klippel-Trenaunay-Weber syndrome, Proteus syndrome, and neurofibromatosis. In this patient, the mild hemihypertrophy is idiopathic. Because of the normal spinal examination and absence of neurologic findings, an MRI scan is unnecessary. The absence of clinical and radiographic evidence of hip dysplasia makes both an ultrasound of the hips and application of a Pavlik harness unnecessary. Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont Ill, American Academy of Orthopaedic Surgeons, 1996, pp 185-193. Sponseller PD: Localized disorders of bone and soft tissue, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 305-344.
Question 54
What is the mechanism of action of an intramuscular injection of botulinum type A toxin in reducing spasticitiy?




Explanation
The use of intramuscular botulinum type A toxin has been shown to be a useful adjuvant in the management of dynamic deformity in patients with cerebral palsy. Botulinum type A toxin is a neurotoxin produced by Clostridium botulinum that works by interfering with presynaptic acetylcholine release at cholinergic nerve terminals. At the cellular level, the mechanism involves endocytosis of the intact botulinum toxin molecule by cells in the end plate, followed by disulfide cleavage and translocation of the light chain into the cytosol where it disrupts the normal binding of the synaptosomal vesicles to the axon terminal membrane. Neither the nerve terminal nor the neuromuscular junction is damaged. The muscle paralysis is reversible and dose-dependent. Baclofen is a neuropharmacologic agent that functions as a GABA agonist. Dorsal rhizotomy is a neurosurgical procedure that reduces spasticity by dividing afferent (excitatory) fibers in the posterior rootlet of the spinal nerves. Koman LA, Mooney JF III, Smith B, Goodman A, Mulvaney T: Management of cerebral palsy with botulinum-A toxin: Preliminary investigation. J Pediatr Orthop 1993;13:489-495.
Question 55
A 5-year-old boy has had right hip pain and a limp for the past 3 months. Examination of the right hip reveals irritability and restricted abduction and internal rotation. AP and lateral radiographs of the hips are shown in Figures 31a and 31b. Initial management should consist of








Explanation
31b A favorable prognosis can be expected in up to 70% of children with Legg-Calve-Perthes disease who are younger than age 6 years. Containment treatment has not been shown to alter the outcome in this age group. The goals of treatment in this patient are to reduce pain (synovitis), restore motion, and improve function. Symptomatic treatment modalities include bed rest, traction, crutches, activity modification, and nonsteroidal anti-inflammatory drugs. Herring JA: The treatment of Legg-Calve-Perthes disease: A critical review of the literature. J Bone Joint Surg Am 1994;76:448-458.
Question 56
Hamstring lengthening and posterior transfer of the rectus femoris will be most successful in a patient with cerebral palsy who has which of the following gait abnormalities?


Explanation
Children with cerebral palsy typically ambulate with a crouched gait characterized by excessive flexion of the hips and knees during stance. Many patients exhibit co-contracture of the quadriceps and hamstrings, causing a stiff-knee gait. Normally, the rectus femoris fires at the initiation of swing and in terminal swing through initial contact. Prolonged activity of the rectus femoris throughout the swing phase interferes with normal knee flexion. This contributes to a stiff knee during swing phase and prevents clearance of the foot. Lengthening of the hamstrings alone will not improve foot clearance. Hamstring lengthening is contraindicated when there is hyperextension during stance. Transfer of the rectus femoris to one of the knee flexors has been shown to improve knee flexion during swing by an average of 15 degrees. This allows improved foot clearance. Gage JR, Perry J, Hicks RR, Koop S, Werntz JR: Rectus femoris transfer to improve knee function of children with cerebral palsy. Dev Med Child Neurol 1987;29:159-166.
Question 57
Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reveals a normal neurologic examination, and the patient reports no discomfort with the cast and crutches. Management should now include








Explanation
32b Stable fractures and minimally displaced fractures in children can and should be treated by closed methods. Because loss of reduction is common, alignment of tibia fractures must be monitored closely for the first 3 weeks after cast application. This is most easily handled in a cooperative patient by cast wedging. Some children require application of a second cast under general anesthesia 2 to 3 weeks after injury, particularly if the subsidence of swelling has caused the cast to loosen. Surgical indications include the presence of soft-tissue injuries, unstable fracture patterns, fractures associated with compartment syndrome, and the child with multiple injuries. Surgical options in children include percutaneous pins, external fixation, plates and screws, and intramedullary nails. Heinrich SD: Fractures of the shaft of the tibia and fibula, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1340-1346.
Question 58
A 14-year-old patient with an L3 myelomeningocele underwent anterior and posterior spinal fusion for a curve of 50 degrees. Follow-up examination 1 week after the procedure now reveals persistent drainage from the posterior wound. Results of laboratory cultures show Streptococcus viridans, Staphylococcus aureus, and Enterococcus. In addition to IV antibiotics, surgical irrigation, and debridement, management should include
Explanation
The rate of wound infections has dramatically decreased with the routine use of prophylactic antibiotics. Factors known to increase the risk of infection include instrumentation, prolonged surgical time, excessive blood loss, poor perioperative nutritional status, a history of surgery, and a history of infection. The use of allograft does not result in an increased rate of infection. Adequate treatment requires early diagnosis and intervention. Temperature elevation and persistent wound drainage are highly suspicious for infection. An erythrocyte sedimentation rate and a WBC are not useful in diagnosis unless serial examinations show rising levels. Patients should be taken to the operating room where the entire wound can be reopened, irrigated, and debrided. Bone graft can be washed and replaced. Hardware should not be removed. The wound should be closed over suction drains. IV antibiotics should be given for a period of at least 10 days, followed by 6 weeks orally. Leaving the wound open to granulate with dressing changes results in prolonged hospitalization, inadequate treatment of the infection, and a poor cosmetic result. Lonstein JE: Complications of treatment, in Bradford DS, Lonstein JE, Moe JH, et al (eds): Moe's Textbook of Scoliosis and Other Spinal Deformities, ed 2. Philadelphia, Pa, WB Saunders, 1987, p 476.
Question 59
What is the primary mechanism of injury for the fracture shown in Figures 33a and 33b?




Explanation
33b The radiographs show a triplane fracture of the ankle. In adolescence, closure of the distal tibial physis starts peripherally at the anteromedial aspect of the medial malleolus and extends posteriorly and laterally. The anterolateral quadrant of the physis is the last to close, making this region the most susceptible to separation. When the foot is twisted into external rotation, the anterolateral portion of the epiphysis is avulsed by the pull of the anterior tibiofibular ligament. When this fragment alone is avulsed, the result is a juvenile Tillaux fracture. When the fracture extends to involve the remainder of the physis and posterior metaphysis, as in this patient, the result is a triplane fracture. Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 267-272. Dias LS, Giegerich CR: Fractures of the distal tibial epiphysis in adolescence. J Bone Joint Surg Am 1983;65:438-444.
Question 60
Figure 34 shows the standing AP radiograph of a 2-year-old girl who has a left bowleg deformity. Her mother states that she first noticed the problem when the child began walking at age 10 months, and the deformity has worsened over the past 6 months. Examination reveals a definite lateral thrust of the knee during the stance phase of gait. Management should consist of


Explanation
Infantile tibia vara is a developmental condition characterized by a varus angulation of the proximal end of the tibia that is caused by a growth disturbance of the proximal medial physis. In a study of 42 affected extremities in 24 children younger than age 3 years, it was found that daytime ambulatory brace treatment favorably altered the natural history of tibia vara. Another study of 27 patients with stage II Langenskiöld disease found a success rate of 70% (improved alignment without the need for osteotomy) using brace treatment. These authors also noted that children with unilateral disease were more likely to obtain correction of the deformity compared with those with bilateral disease. In this patient, observation is not warranted because untreated tibia vara has a significant risk for progressive worsening. Osteotomy is best reserved for those patients who, despite bracing, do not show satisfactory clinical and radiographic improvement by age 4 years. Elevation of the medial tibial plateau is a treatment option for older patients who have more advanced disease. An MRI scan would not provide any useful clinical information at this time. Zionts LE, Shean CJ: Brace treatment of early infantile tibia vara. J Pediatr Orthop 1998;18:102-109. Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount's disease. J Pediatr Orthop 1998;18:374-380.
Question 61
Figures 35a and 35b show the radiographs of a 7-year-old patient who has progressive deformity of the right thigh accompanied by a dull persistent pain radiating to the knee. Examination reveals an obvious bulge in the right thigh, with flexion of the hip beyond 50 degrees only if the hip is allowed to externally rotate. Management should consist of


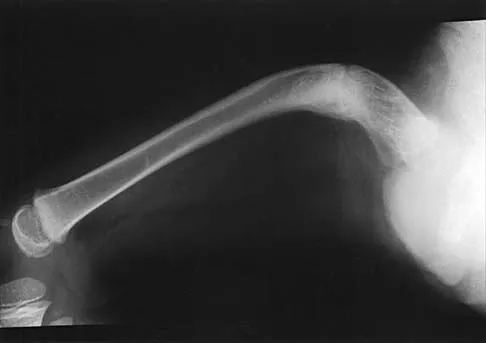

Explanation
35b The patient has radiographic signs of osteogenesis imperfecta, including osteopenia, mild acetabular protrusio, cortical thinning, and bowing associated with anterior stress fracturing. The treatment of choice is correction of the bow with osteotomies, followed by intramedullary fixation to prevent further deformity. Biphosphonates, such as pamidronate, may be useful in increasing bone density and preventing fractures. Large multicenter studies on biphosphonate efficacy are currently in progress. Zionts LE, Ebramzadeh E, Stott NS: Complications in the use of the Bailey-Dubow extensible nail. Clin Orthop 1998;348:186-195. Luhmann SJ, Sheridan JJ, Capelli AM, Schoenecker PL: Management of lower-extremity deformities in osteogenesis imperfecta with extensible intramedullary rod technique: A 20-year experience. J Pediatr Orthop 1998;18:88-94.
Question 62
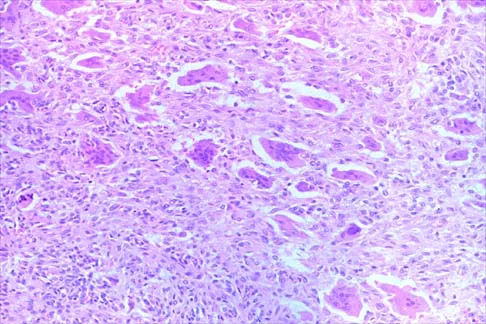
Figures 36a and 36b show the MRI scans of a 15-year-old girl who has had pain and recurrent hemarthrosis in the knee for the past year. Plain radiographs are normal. What is the most likely diagnosis?
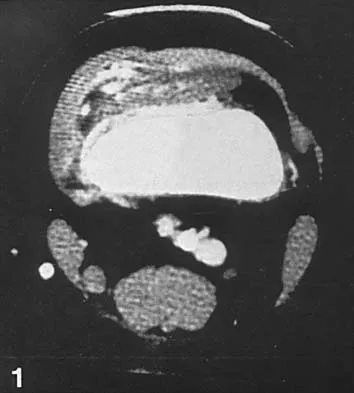



Explanation
36b In pediatric patients who have pain and recurrent hemarthrosis in the knee, hemangioma is often seen as an internal derangement of the knee, and long delays in diagnosis are common. An MRI scan is noninvasive and will best aid in diagnosis. In this patient, the MRI scan shows a hemangioma with no evidence of meniscal injury or discoid meniscus. Hemophilia is unlikely because the patient is female. The presence of hemarthrosis makes JRA an unlikely diagnosis.
Question 63
A 2-year-old child has marked hypotonia and depressed reflexes. History reveals that the child was normal at birth and developed normally for the first year. The child also began to ambulate, but lost this ability during the next 6 months. Laboratory studies show a creatine phosphokinase level that is within the normal range. DNA testing confirms a deletion in the survival motor neuron (SMN) gene. What is the most likely diagnosis?
Explanation
The patient has spinal muscular atrophy, type 2. This type is intermediate in severity between the Werdnig-Hoffmann type (type 1) and the Kugelberg-Welander type (type 3). It normally manifests itself between the ages of 3 and 15 months. Survival until adolescence is common. All three types of spinal muscular atrophy have been linked to the SMN gene at the 5q12.2-13.3 locus. DNA testing is available and is preferred to muscle biopsy because it is less invasive and more definitive. Biros I, Forrest S: Spinal muscular atrophy: Untangling the knot? J Med Genet 1999;36:1-8.
Question 64
A 13-year-old boy sustains a valgus stress injury to the knee while playing football, and he is unable to bear weight after the injury. Examination reveals tenderness medially superior to the joint line. The knee is held in flexion, and he has a large effusion and localized medial swelling. Plain radiographs show no obvious fracture. What is the next diagnostic step?
Explanation
In the skeletally mature individual, this mechanism of injury will often result in a sprain of the medial collateral ligament. In skeletally immature patients, the same mechanism can cause a fracture of the distal femoral physis. If the fracture is nondisplaced, the plain radiographs may show only soft-tissue swelling or effusion. While the MRI scan may show edema in the soft tissues on the medial side of the knee and even an abnormality of the physis, stress radiographs provide a quicker and less expensive means of making the diagnosis. Arthroscopy and arthrography would not be helpful in making the diagnosis. Arthroscopy may result in further displacement of the injury. Smith L: Concealed injury to the knee. J Bone Joint Surg Am 1962;44:1659-1660.
Question 65
Figure 37 shows the clinical photograph of a 1-day-old infant who weighed 10.25 lb at birth. Examination reveals an absent right Moro reflex and limited active motion of the right shoulder, elbow, and wrist, but flexion of the fingers. Passive range of motion of the shoulder and elbow is normal. What is the most likely diagnosis?


Explanation
The patient's right upper extremity is held in the "head waiter's" posture with the shoulder internally rotated, the elbow extended, and the wrist in flexion. The Erb type of obstetrical brachial plexus palsy involves the C5 and C6 nerve root, and occasionally, as in this child, the C7 nerve root. Obstetrical palsy is a traction injury, and is associated with a high birth weight, shoulder dystocia, cephalopelvic disproportion, or the use of forceps. Erb palsy is four times more common than injury to the entire plexus or injury to the C8 and T1 nerve roots. It results from the shoulder being depressed while the head and neck are laterally rotated, extended, and tilted in the opposite direction. Most patients recover wrist extension and elbow flexion. Patients with residual weakness of shoulder external rotation and abduction will benefit from release of the pectoralis major, latissimus dorsi, and teres major, with transfer of the latissimus dorsi and the teres major to the posterosuperior aspect of the rotator cuff. Recent studies using arthrograms and CT scans have shown a higher incidence of posterior glenoid deficiency and posterior subluxation than that observed with plain radiographs. The posterior subluxation or dislocation can be effectively reduced by tendon release and transfer procedures. Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:997-1001. Pearl ML, Edgerton BW: Glenoid deformity secondary to brachial plexus birth palsy. J Bone Joint Surg Am 1998;80:659-667.
Question 66
Figure 38 shows the radiograph of a 5-year-old child who sustained a type III supracondylar fracture. Examination reveals the absence of a radial pulse, but an otherwise well-perfused hand. Following closed reduction and percutaneous pinning, the radial pulse remains absent; however, the hand is pink and well perfused. Management should now include


Explanation
In a study of over 400 patients with displaced supracondylar fractures, 3.2% of the fractures were associated with the absence of the radial pulse with an otherwise well-perfused hand. Based on this study, a period of close observation with frequent neurovascular checks should be completed before attempting invasive correction of the problem. Because of the satisfactory results with expectant management, angiography, exploration, removal of fixation and exploration, and thrombectomy are contraindicated.
Question 67
Figures 39a and 39b show the radiographs of an otherwise healthy 10-year-old boy who has had thigh pain and a limp for the past 9 months. Examination reveals that the left lower extremity is 1 cm shorter, with reduced flexion, abduction, and internal rotation on the left side. The patient is at the 50th percentile for height and the 90th percentile for weight. Serum studies will most likely show




Explanation
39b The patient has a slipped capital femoral epiphysis (SCFE) at a younger than average age (average age 13.5 years for boys and 12.0 years for girls); therefore, an etiology that is not idiopathic must be considered. Hypothyroidism can result in a SCFE, but these children typically fall into the category of less than the 10th percentile for height. SCFE may develop in children with a growth hormone deficiency who have undergone hormonal replacement. Osteodystrophy caused by chronic renal failure may result in a SCFE, but the bone quality is markedly osteopenic on radiographs and the children are chronically ill with both low height and weight percentiles. An elevated estrogen level results in physeal closure and is protective to physeal slippage. Therefore, this child will most likely have normal laboratory values. Loder RT, Hensinger RN: Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop 1997;17:205-211.
Question 68
A 7-year-old patient has had a painless limp for several months. Examination reveals pain and spasm with internal rotation, and abduction is limited to 10 degrees on the involved side. Management consists of 1 week of bed rest and traction, followed by an arthrogram. A maximum abduction/internal rotation view is shown in Figure 40a, and abduction and adduction views are shown in Figures 40b and 40c. The studies are most consistent with






Explanation
40b 40c The radiographs show classic hinge abduction. The diagnostic feature is the failure of the lateral epiphysis to slide under the acetabular edge with abduction, and the abduction view shows medial dye pooling because of distraction of the hip joint. Persistent hinge abduction has been shown to prevent femoral head remodeling by the acetabulum. Radiographic changes are characteristic of severe involvement with Legg-Calve-Perthes disease.The Catterall classification cannot be well applied without a lateral radiograph, but this degree of involvement would likely be considered a grade III or IV. Because the lateral pillar is involved, this condition would be classified as type C using the Herring lateral pillar classification scheme.
Question 69
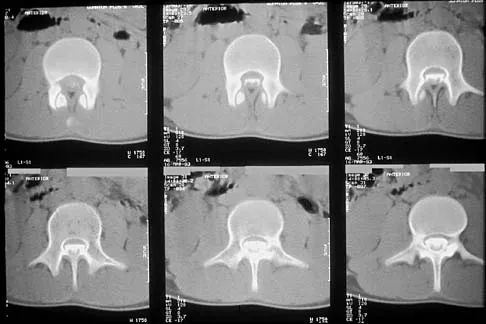
A 14-year-old football player has had thigh pain and weakness following a full-contact scrimmage 24 hours ago. He recalls that he felt a sharp pain in his back after colliding with a much heavier player. Examination reveals that the spine is minimally tender to palpation in the upper lumbar region. Motor testing reveals quadriceps weakness bilaterally, and a reverse straight leg raising test is positive. Plain radiographs of the thoracolumbar spine are normal. A myelogram, a CT scan with contrast, and an MRI scan are shown in Figures 41a through 41c. What is the most likely diagnosis?





Explanation
41b 41c Fracture of the vertebral end plate is a relatively uncommon injury that is most often seen in adolescent boys. The injury is characterized by traumatic displacement of the vertebral ring-apophysis into the spinal canal and associated disk herniation. Over one third of these injuries are seen in children with lumbar Scheuermann disease. The injury most frequently involves the midlumbar vertebra, and symptoms are often indistinguishable from those associated with a herniated disk. The injury is usually not visible on plain radiographs. The diagnosis is typically made after obtaining MRI or contrast CT scans. Treatment consists of laminotomy and excision of the osteochondral fragments. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 635-651.
Question 70
Figure 42 shows the radiograph of a 12-year-old boy who has a limp and pain in the left hip with athletic activity. Examination reveals decreased abduction and internal rotation of the left hip, with pain at the extremes of motion and a 1-cm limb-length discrepancy. Management should consist of


Explanation
The radiograph shows changes that are most consistent with Legg-Calve Perthes disease. Valgus extension osteotomy is the salvage procedure of choice in patients with late symptomatic Perthes disease with severe joint incongruity. Prerequisites for valgus extension osteotomy include an adequate range of hip adduction and proof of improved congruity in the new position. Total hip arthroplasty is not a good alternative in the young patient. Varus osteotomy would further shorten the extremity and place a flattened portion of the femoral head in the acetabulum. A prerequisite of the innominate osteotomy is a congruent reduction. Skaggs DL, Tolo VT: Legg-Calve-Perthes disease. J Am Acad Orthop Surg 1996;4:9-16.
Question 71
The mother of a 5-year-old child reports that he has had a fever of 103 degrees F (39.4 degrees C), leg swelling, and has been unwilling to bear weight on his right lower leg for the past 7 days. Examination reveals point tenderness at the distal femur. Aspiration at the metaphysis yields 10 mL of purulent fluid, and a Gram stain reveals gram-positive cocci. In addition to hospital admission, management should include
Explanation
The patient has a subperiosteal abscess. Because aspiration revealed 10 mL of purulent fluid, the treatment of choice is surgical incision and drainage of the abscess, followed by immobilization to reduce the risk of pathologic fracture. With an adequate response to IV antibiotics and a susceptible bacteria, the patient may then be switched to oral antibiotics.
Question 72
Figure 43 shows the lateral radiograph of a 12-year-old boy with mild osteogenesis imperfecta who injured his left elbow after pushing his brother. Treatment should consist of


Explanation
The patient has a displaced fracture of the apophysis of the olecranon for which most authorities recommend surgical treatment. In older children, stability of the reduction may be achieved by the use of two parallel medullary Kirschner wires and a figure-of-8 tension band loop of either stainless steel wire or absorbable suture. The use of an absorbable suture does not require removal of the implant. Absorbable suture alone is best used in very young patients who have this type of injury. An intramedullary screw would pose an unnecessary risk of future growth disturbance. A displaced, isolated fracture of the apophysis of the olecranon is an unusual injury in a child. It has been suggested by several authors that children who have osteogenesis imperfecta may be especially prone to this injury. One study reported seven of these fractures occurring in five children who had the mild form of osteogenesis imperfecta (Sillence type IA). The authors of this study suggest that the diagnosis of osteogenesis imperfecta be considered in any child who has a displaced fracture of the apophysis of the olecranon, especially when the injury is associated with relatively minor trauma. Stott NS, Zionts LE: Displaced fractures of the apophysis of the olecranon in children who have osteogenesis imperfecta. J Bone Joint Surg Am 1993;75:1026-1033. Gaddy BC, Strecker WB, Schoenecker PL: Surgical treatment of displaced olecranon fractures in children. J Pediatr Orthop 1997;17:321-324.
Question 73
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include


Explanation
The patient has severe acetabular protrusio, a condition that is frequently associated with Marfan syndrome. An echocardiogram is necessary to rule out the most serious consequence of this syndrome, aortic root widening, which can lead to aortic valve dysfunction or fatal aortic rupture. An electromyogram may be indicated for Charcot-Marie-Tooth disease, which is associated with acetabular dysplasia, but not protrusio. The renal ultrasound, the MRI scan, and the biopsy would be of no value in this patient. Protrusio can also be seen in patients with osteogenesis imperfecta and juvenile rheumatoid arthritis. Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Question 74
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of


Explanation
In a retrospective review of 10 patients treated with hemivertebra excision for hemivertebra in the levels of T12 to L3, the procedure was found to be safe and effective. The procedure provided an average curve correction of 67 degrees and was greatest in patients who were younger than age 4 years at the time of surgery. Long anterior and posterior fusion with instrumentation is not the treatment of choice at this age. Either anterior hemiepiphyseodesis or posterior hemiarthrodesis in this isolated hemivertebra setting would be inadequate. Brace treatment is ineffective in management of the primary curvature.
Question 75
A 10-year-old girl with a history of an obstetrical brachial plexus palsy has been referred for evaluation. Examination reveals a severe adduction internal rotation contracture of the shoulder and a mild flexion contracture of the elbow. Hand function is normal. Radiographs show mild glenohumeral joint incongruity. To achieve the best functional outcome, management should consist of
Explanation
The patient has an upper plexus palsy (Erb palsy) with severe shoulder contracture. While physical therapy for stretching is the treatment of choice to prevent contracture in the newborn, it is unlikely to be of benefit in the older child with an established contracture. Contracture release alone or in combination with muscle transfers can improve the cosmetic appearance, and in the case of a mild deformity, may also improve function. These procedures are less likely to help when there is deformity of the shoulder joint or when arthritic changes are present. The procedure of choice for an older child with joint deformity is rotational osteotomy of the proximal humerus because it can improve cosmesis and function, even in the face of joint deformity. Jahnke AH Jr, Bovill DF, McCarroll HR Jr, James P, Ashley RK: Persistent brachial plexus birth palsies. J Pediatr Orthop 1991;11:533-537. Strecker WB, McAllister JW, Manske PR, Schoenecker PL, Dailey LA: Sever-L'Episcopo transfers in obstetrical palsy: A retrospective review of 20 cases. J Pediatr Orthop 1990;10:442-444.
Finish Exam?
You cannot change answers after submitting.
