Question 26
The parents of a 15-month-old child report that he is not yet walking. Further evaluation, rather than reassurance and observation, should be conducted if the child is not performing what other activity?

Explanation
A child not ambulating at age 15 months is still within normal limits. The child should be able to sit by age 9 months. The remaining milestones listed are reached later in development.
Question 27
Of the following clinical situations, which is most likely to lead to osteonecrosis associated with a slipped capital femoral epiphysis (SCFE)?

Explanation
Osteonecrosis of the femoral head is the most devastating complication of SCFE. There is a 47% incidence of ischemic necrosis associated with an unstable SCFE. By definition, the patient with an unstable SCFE is unable to bear weight even with crutches. Osteonecrosis is most likely associated with the initial femoral head displacement rather than the result of either tamponade from hemarthrosis or from gentle repositioning prior to stabilization. Age, sex, and obesity are not risk factors for osteonecrosis. Loder RT, Richards BS, Shapiro PS, et al: Acute slipped capital femoral epiphysis: The importance of physeal stability. J Bone Joint Surg Am 1993;75:1134-1140.
Question 28
An 8-year-old boy has had pain and swelling around the right knee for the past 4 weeks. He recalls bumping it about 4 weeks ago. He has no pain in other joints, and denies any fevers, chills, or other symptoms. A radiograph is shown in Figure 13. Laboratory studies show a WBC count of 9,700/mm3, an erythrocyte sedimentation rate of 18 mm/h, and a C-reactive protein level of 3.7 mg/L. What is the next most appropriate step in management?



Explanation
The history and laboratory findings are consistent with osteomyelitis of the patella. The radiograph reveals bone destruction in the patella; therefore, the next most appropriate step is open biopsy and debridement of the site. Aspiration of the knee joint may be needed to rule out septic arthritis prior to patellar debridement. With this amount of bone destruction, surgical debridement is helpful to obtain cultures and to remove necrotic material. Administering antibiotics without any prior culture increases the risk of negative cultures later and a potentially incorrect choice of antibiotic. A neoplasm should be included in the differential. It would be inappropriate to initiate chemotherapy and radiation therapy without a biopsy-confirmed diagnosis. A bone scan is likely to demonstrate uptake, but radiographs have already localized the abnormality to the patella. Morrisy RT: Bone and joint sepsis, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 466-470.
Question 29
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal. Radiographs confirm a 2-cm discrepancy in the lengths of the lower extremities. Additional imaging studies should include

Explanation
The patient may have Beckwith-Wiedemann syndrome (BWS), which consists of exophthalmos, macroglossia, gigantism, visceromegaly, abdominal wall defects, and neonatal hypoglycemia. Hemihypertrophy develops in approximately 15% of patients with BWS. Patients with hemihypertrophy that is the result of BWS have a 40% chance of developing malignancies such as Wilms' tumor or hepatoblastoma; therefore, frequent ultrasound screening is recommended until about age 7 years. The absence of nevi and vascular markings helps to rule out other causes of hemihypertrophy, such as neurofibromatosis, Proteus syndrome, and Klippel-Trenaunay syndrome. Bone age estimations are not accurate at this young age but may become more useful later to help predict the timing of epiphysiodesis procedures. DeBaun MR, Tucker MA: Risk of cancer during the first four years of life in children from The Beckwith-Wiedemann Syndrome Registry. J Pediatr 1998;132:398-400. Ballock RT, Wiesner GL, Myers MT, et al: Hemihypertrophy concepts and controversies. J Bone Joint Surg Am 1997;79:1731-1738.
Question 30
A 12 1/2-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full range of motion without effusion. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI scans are shown in Figures 14a and 14b. Initial treatment should consist of



Explanation
14b This skeletally immature patient has a small OCD lesion that appears stable, and he has not undergone any treatment. Therefore, a trial of immobilization until pain resolves is the best initial choice. Thereafter, cessation of sport activities for 4 to 6 months may allow healing of the lesion. Surgical treatment of juvenile OCD lesions is reserved for unstable lesions, patients who have not shown radiographic evidence of healing and are still symptomatic after 6 months of nonsurgical management, or patients who are approaching skeletal maturity. Good results with stable in situ lesions that have failed to respond to nonsurgical management have been reported with both transarticular and retroarticular drilling. Results after excision alone are poor at 5-year follow-up, and it is unclear if microfracture will improve the long-term outcome. Mosaicplasty may be the next best option for patients who remain or become symptomatic after excision of the fragment and microfracture. Wall E, Von Stein D: Juvenile osteochondritis dissecans. Orthop Clin North Am 2003;34:341-353.
Question 31
A 14-year-old boy undergoes application of a circular frame with tibial and fibular osteotomy for gradual limb lengthening. He initiates lengthening 7 days after surgery. During the first week of lengthening, he reports that turning of the distraction devices is becoming increasingly difficult. On the 9th day of lengthening, he is seen in the emergency department after feeling a pop in his leg and noting the acute onset of severe pain. What complication has most likely occurred?


Explanation
Incomplete corticotomy may result from osteotomy with limited soft-tissue stripping and exposure. When the patient begins distraction, tension develops at all wire/half-pin and bone interfaces, leading to increasing difficulty in distraction and limb pain. Sudden spontaneous completion of the osteotomy with continued tension applied by the fixator results in acute distraction of the osteotomy with severe pain. Premature consolidation is unlikely this early following the initial surgery. Birch JG, Samchukov ML: Use of the Ilizarov method to correct lower limb deformities in children and adolescents. J Am Acad Orthop Surg 2004;12:144-154.
Question 32
What is the most common primary malignant bone or cartilage tumor in children?


Explanation
Osteosarcoma is the most common primary malignant bone tumor (5.6 per 1 million children younger than age 15 years), and Ewing's sarcoma is second (2.1 per 1 million children). Giant cell tumor and chondrosarcoma are rare in children. Osteochondroma is more common than any of the above tumors in children, but it is not malignant. Himelstein BP, Dormans JP: Malignant bone tumors of childhood. Pediatr Clin North Am 1996;43:967-984. Pierz KA, Womer RB, Dormans JP: Pediatric bone tumors: Osteosarcoma, Ewing's sarcoma, and chondrosarcoma associated with multiple hereditary osteochondromatosis. J Pediatr Orthop 2001;21:412-418.
Question 33
What is the peak period of onset in children with pauciarticular juvenile rheumatoid arthritis?

Explanation
Approximately one half of patients with juvenile rheumatoid arthritis (JRA) have the pauciarticular form, which by definition includes only patients with fewer than five joints involved. The peak period of onset is between the ages of 2 and 4 years, with half of the affected children coming to medical attention before age 4 years. The knee is most often affected, with the ankle-subtalar and elbow joints next in frequency. The average duration of the disease is 2 years and 9 months, with half the cases lasting less than 2 years. Arthritis, in Herring JA (ed): Tachdjian's Pediatric Orthopaedics, ed 3. St Louis, MO, WB Saunders, 2002, pp 1811-1839.
Question 34
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of

Explanation
Scoliotic deformities in patients with NF1 are often dysplastic with short, angular curves. Posterior arthrodesis is made more difficult by the presence of kyphosis and of weak posterior elements caused by dural ectasia. Combined anterior and posterior spinal arthrodesis is generally preferred for progressive dysplastic curves to maximize deformity correction and to decrease the risk of pseudarthrosis. Anterior fusion may also prevent crankshaft phenomenon in young children. Brace treatment is not effective for large, rigid, or dysplastic curves. Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Question 35
In obstetrical brachial plexus palsy, which of the following signs is associated with the poorest prognosis for recovery in a 2-month-old infant?


Explanation
Persistent Horner's sign (ptosis, myosis, and anhydrosis) is a sign of proximal injury, usually avulsion of the roots from the cord which disrupts the sympathetic chain. Root rupture or avulsion proximal to the myelin sheath has less chance of healing. Two-month-old infants with persistent weakness in the other areas described may still have a good prognosis for recovery. Concurrent clavicle fracture has been shown to have no prognostic value. Clarke HM, Curtis CG: An approach to obstetrical brachial plexus injuries. Hand Clin 1995;11:563-581.
Question 36
A 6-year-old boy with acute hematogenous osteomyelitis of the distal femur is being treated with intravenous antibiotics. The most expeditious method to determine the early success or failure of treatment is by serial evaluations of which of the following studies?

Explanation
Successful antibiotic treatment of osteomyelitis should lead to a rapid decline in the CRP. The CRP should decline after 48 to 72 hours of appropriate treatment. Imaging studies will take much longer to show resolution of bone infection. Unkila-Kallio L, Kallio MJ, Eskola J, et al: Serum C-reactive protein, erythrocyte sedimentation rate, and white blood cell count in acute hematogenous osteomyelitis of children. Pediatrics 1994;93:59-62.
Question 37
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?




Explanation
15b The patient has an abnormal neurologic exam as shown by the abnormal abdominal reflexes. Furthermore, she has a significant curve and is younger than age 10 years. These findings are not consistent with idiopathic scoliosis. MRI will best rule out syringomyelia or an intraspinal tumor. Bracing and surgery are not indicated for this small curvature prior to obtaining an MRI scan. Ginsburg GM, Bassett GS: Back pain in children and adolescents: Evaluation and differential diagnosis. J Am Acad Orthop Surg 1997;5:67-78.
Question 38
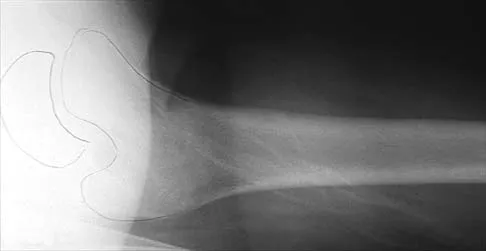
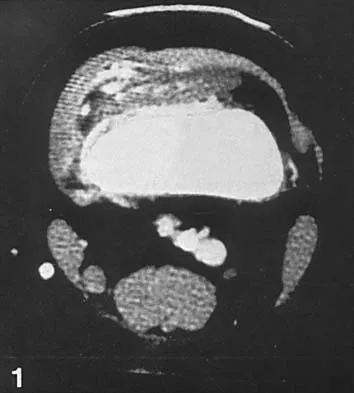
Figure 16 shows the radiograph of a 7-year-old boy who sustained a pathologic fracture of the left humerus 1 day ago. Initial management should consist of

Explanation
The radiograph shows a pathologic fracture through a unicameral (simple) bone cyst (UBC). This is the most common location and presentation of a UBC. Less than 10% of UBCs heal spontaneously following a fracture. Urgent biopsy is not indicated because the lesion appears benign and the histology of fracture callus may be misinterpreted as osteosarcoma. After the fracture heals with the use of a sling and swathe, the UBC may be treated with a minimally invasive procedure such as injection of bone marrow and/or demineralized bone matrix. The chance for success is relatively low in an active cyst located adjacent to the physis. More invasive procedures, such as curettage, Rush rod fixation, or cannulated screw decompression, have been described but are rarely necessary for treatment of upper extremity cysts. Rougraff BT, Kling TJ: Treatment of active unicameral bone cysts with percutaneous injection of demineralized bone matrix and autogenous bone marrow. J Bone Joint Surg Am 2002;84:921-929. Robosch A, Saraph V, Linhart WE: Flexible intramedullary nailing for the treatment of unicameral bone cysts in long bones. J Bone Joint Surg Am 2000;82:1447-1453.
Question 39
Figure 17 shows the AP radiograph of a 5-year old child who has mild short stature and a painless bilateral gluteus medius lurch. Initial work-up should include


Explanation
Bilateral flattening of the femoral heads suggests multiple epiphyseal dysplasia; therefore, a skeletal survey is indicated to look for involvement of other epiphyses. Unilateral flattening of the femoral head would suggest Legg-Perthes disease. Sponseller PD: Skeletal dysplasias, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 269-270.
Question 40
A 7-year-old girl with spinal muscular atrophy (SMA) type II has popping of the left hip. Examination reveals painless subluxation of the joint in adduction with palpable reduction in abduction. Radiographs show coxa valga, subluxation of the left hip, and pelvic obliquity with elevation of the left hemipelvis. Treatment should consist of

Explanation
Observation is the treatment of choice. Hip subluxation and dislocation are not uncommon in patients with SMA type II who are unlikely to be ambulatory. Scoliosis occurs in these patients 100% of the time and frequently creates pelvic obliquity. However, in long-term follow-up, patients with SMA type II and hip dislocations had little associated pain or functional limitations because of hip instability. In addition, recurrent hip subluxation after surgical treatment has been documented. Given the rarity of symptoms from hip instability in long-term follow-up, and the possibility of recurrent dislocation, surgical intervention for hip instability may expose SMA type II patients to undue surgical risk for minimal if any functional gain. Sporer SM, Smith BG: Hip dislocation in patients with spinal muscular atrophy. J Pediatr Orthop 2003;23:10-14.
Question 41
A newborn with myelomeningocele has no movement below the waist and has bilateral hips that dislocate with provocative flexion and adduction. What is the best treatment option for the hip instability?

Explanation
The status of the hips (located or dislocated) in children with thoracic-level myelomeningocele has no effect on the functional outcome of these patients. Management of unstable hips in this population should be limited to treatment of the contractures that may lead to poor limb positioning in either braces or a wheelchair. The use of the Pavlik harness and/or spica cast is contraindicated because they would promote flexion and abduction contractures. In the past, open reduction either through an anterior or medial approach had been performed with a high incidence of redislocation and other complications, with little functional gain for the child. Gabriel KG: Natural history of hip deformity in spina bifida, in Sarwark JR, Lubicky JP (eds): Caring for the Child With Spina Bifida. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2001, pp 89-103.
Question 42
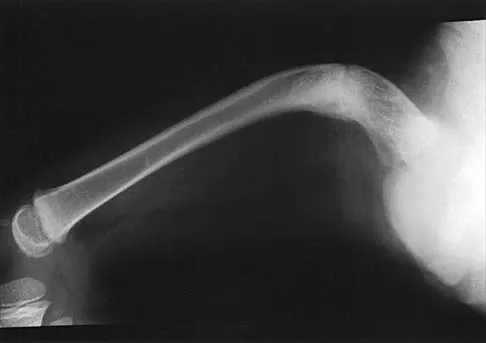
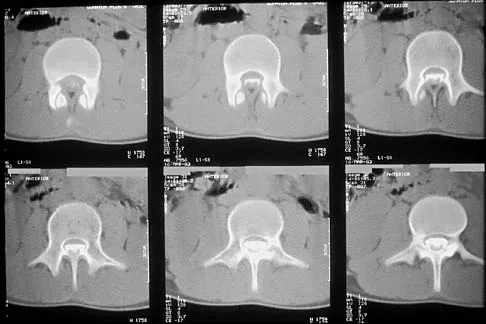
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition?



Explanation
The patient has a grade 4 spondylolisthesis. Optimal surgical management is posterior spinal fusion from L4 to the sacrum. The use of instrumentation is controversial. Vertebrectomy is typically reserved for spondylo-optosis (grade 5) cases. Spinal fusion from L5 to S1 usually is not successful for a slip that is greater than 50%. Isolated anterior spinal fusion has not been successful, and direct repair of the pars defect is only useful for spondylolysis without spondylolisthesis. Lenke LG, Bridwell KH: Evaluation and surgical treatment of high-grade isthmic dysplastic spondylolisthesis. Instr Course Lect 2003;52:525-532.
Question 43
Duchenne's muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?


Explanation
Patients with Duchenne's muscular dystrophy show progressive muscular weakness because of the absence of dystrophin and have the clinical picture of progressive muscle weakness. The condition is an X-linked genetic disease. Fitzgerald RH, Kaufer H, Malkani AL: Orthopaedics. St Louis, MO, Mosby Year Book, 2002, pp 1573-1583.
Question 44
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child's back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of


Explanation
19b Congenital anomalies of the spine, including failure of formation and failure of segmentation, are associated with other anomalies in other organ systems that develop at the same time. These include anomalies in the genitourinary system, cardiac anomalies, Sprengel's deformity, radial hypoplasia, and gastrointestinal anomalies including imperforate anus and trachealesophageal fistula. Spinal dysraphism is the most common associated abnormality. McMaster found an 18% incidence before the common use of MRI. Bradford and associates reported on 16 of 42 patients with congenital spinal anomalies and spinal dysraphism using MRI. Neural axis lesions may be associated with visible midline abnormalities such as a hairy patch or nevus. The child has already had a cardiac and renal work-up, and based on the findings of the hairy patch and congenital vertebral anomalies, MRI of the entire spine is prudent at this time. Spinal fusion is indicated for progressive congenital scoliosis or kyphosis. Physical therapy does not affect the natural history of congenital scoliosis. McMaster MJ: Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am 1984;66:588-601. Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 45
A 12-year-old boy reports limping and chronic knee pain that is now inhibiting his ability to participate in sports. Clinical examination and radiographs of the knee are normal. Additional evaluation should include
Explanation
While all of the answers may be appropriate, radiating pain from hip pathology must be excluded. At this age, a slipped capital femoral epiphysis is likely. Therefore, the hip must be examined. Kocher MS, Bishop JA, Weed B, et al: Delay in diagnosis of slipped capital femoral epiphysis. Pediatrics 2004;113:322-325.
Question 46
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Explanation
Histologic studies have shown that increased bone turnover is the rule in OI. Pamidronate (and all bisphosphonates) reduce osteoclast-mediated bone resorption. Osteoblastic new bone formation on the periosteal surface of long bones is minimally impaired. With inhibition of osteoclastic bone resorption on the endosteal surface, the cortex of the bone can begin to thicken as it does with normal growth in individuals unaffected by OI. Mineralization and collagen matrix organization are not directly affected by pamidronate. Zeitlin L, Fassier F, Glorieux FH: Modern approach to children with osteogenesis imperfecta. J Pediatr Orthop B 2003;12:77-87. Falk MJ, Heeger S, Lynch KA, et al: Intravenous bisphosphonate therapy in children with osteogenesis imperfecta. Pediatrics 2003;111:573-578.
Question 47
Split posterior tibial tendon transfer is used in the treatment of children with cerebral palsy. Which of the following patients is considered the most appropriate candidate for this procedure?
Explanation
Split posterior tibial tendon transfers are best performed in patients with spastic cerebral palsy who are between the ages of 4 and 7 years and have flexible equinovarus deformities. Rigid deformities typically require bony reconstruction procedures. Tendon transfers in patients with athetosis are unpredictable. Green NE, Griffin PP, Shiavi R: Split posterior tibial-tendon transfer in spastic cerebral palsy. J Bone Joint Surg Am 1983;65:748-754.
Question 48
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Cubitus varus, elbow hyperextension, and internal rotation are all typical components of the gunstock deformity. This deformity results from malunion of a supracondylar fracture of the humerus. All of the problems listed above have been reported as sequelae of a gunstock deformity, although the malunion usually causes no functional limitations. Unacceptable appearance is the most common reason why patients or parents request corrective osteotomy. O'Driscoll SW, Spinner RJ, McKee MD, et al: Tardy posterolateral rotatory instability of the elbow due to cubitus varus. J Bone Joint Surg Am 2001;83:1358-1369. Gurkan I, Bayrakci K, Tasbas B, et al: Posterior instability of the shoulder after supracondylar fractures recovered with cubitus varus deformity. J Pediatr Orthop 2002;22:198-202.
Question 49
An 11-year-old boy sustained an ankle injury while playing football. Figure 20 shows an AP radiograph obtained the day of injury. Treatment should consist of

Explanation
The child has an injury involving both the growth plate and the articular surface of the ankle. Because of the significant displacement, open reduction and internal fixation is indicated to realign the physis and joint surface. The best method of fixation to avoid growth arrest is one that does not cross the physis. This is usually achieved by a transverse epiphyseal screw parallel to the physis. If the metaphyseal fragment was large enough, a transverse metaphyseal screw could be used instead. The incidence of growth arrest following physeal ankle injuries is as high as 50%, and long-term follow-up is indicated. Cass JR, Peterson HA: Salter-Harris Type-IV injuries of the distal tibial epiphyseal growth plate, with emphasis on those involving the medial malleolus. J Bone Joint Surg Am 1983;65:1059-1070.
Question 50
A 3-year-old child has bilateral genu varum and short stature. Radiographs show physeal widening and generalized osteopenia. The femora and tibiae show anterolateral bowing. Laboratory studies show low normal serum calcium values, significantly decreased serum phosphate levels, and normal parathyroid hormone (PTH), alkaline phosphatase, and vitamin-D levels. These findings are consistent with
Explanation
Children with vitamin D-resistant rickets are short in stature and have genu varum, physeal widening, and generalized osteopenia. The abnormality in inherited vitamin D-resistant rickets is the renal tubule's inability to resorb phosphate leading to hypophosphatemia. Laboratory findings in the condition are normal or near normal serum calcium values, significantly decreased serum phosphate levels, elevated alkaline phosphatase levels, and normal PTH and vitamin-D levels. The most common form is inherited as an X-linked dominant trait. Nutritional rickets has a normal or low serum phosphate levels, normal or low serum calcium values, and decreased levels of 25(OH) vitamin D and 1,25-dihydroxyvitamin D. Hypophosphatasia is a rare condition characterized by a deficiency of alkaline phosphatase in the serum and tissues, leading to generalized abnormal mineralization of bone. Primary hyperparathyroidism usually is caused by a parathyroid adenoma, and the child generally has abdominal problems and hypercalcemic crisis. Laboratory findings include elevated serum calcium values, alkaline phosphatase levels, and PTH levels, and decreased serum phosphate levels. Children with renal osteodystrophy tend to have genu valgum, and laboratory findings include elevated serum phosphate, alkaline phosphatase, and PTH levels, and low serum calcium values. Findings of renal disease include elevated BUN and creatinine. Herring JA: Metabolic and endocrine bone diseases, in Herring JA (ed): Tachdjian's Pediatric Orthopaedics, ed 3. Philadelphia, PA, WB Saunders, 2002, pp 1686-1710.
Finish Exam?
You cannot change answers after submitting.
