Question 1
A pediatric orthopaedic surgeon refers a child to a neurologist. The neurologist's office requests the office records of the pediatric orthopaedic surgeon. To maintain Health Insurance Portability and Accountability Act (HIPAA) compliance, what must the surgeon obtain from the parent(s) prior to sending records?

Explanation
The privacy rules do not require an individual's written authorization for certain permitted or required uses and disclosures of the medical records. Patient or parental authorization is not required for disclosures for certain purposes related to treatment, payment, or health care operations. Specifically, HIPAA does not require a covered entity to obtain patient authorization for many of the health care industry's most fundamental activities such as providing care. Carroll R: Risk Management Handbook for Health Care Organizations, ed 4. Hoboken, NJ, Jossey-Bass, 2003, p 1142.
Question 2
A 13-year-old boy injured his knee playing basketball and is now unable to bear weight. Examination reveals tenderness and swelling at the proximal anterior tibia, with a normal neurologic examination. AP and lateral radiographs are shown in Figures 1a and 1b. Management should consist of



Explanation
1b The patient has a displaced intra-articular tibial tuberosity fracture; therefore, the treatment of choice is open reduction and internal fixation. Periosteum is often interposed between the fracture fragments and prevents satisfactory closed reduction. Fortunately, most patients with this injury are close to skeletal maturity and therefore, growth arrest and recurvatum are unusual. Nondisplaced fractures can be treated with a cast, but displaced fractures are best treated with open reduction and internal fixation. Intra-articular fractures can disrupt the joint surface and are sometimes associated with a meniscal tear; therefore, arthroscopy may be needed at the time of open reduction and internal fixation. McKoy BE, Stanitski CL: Acute tibial tubercle avulsion fractures. Orthop Clin North Am 2003;34:397-403.
Question 3
A 12-year-old boy sustained a grade III open tibial fracture 1 week ago and underwent multiple debridements and fracture fixation. He now has a soft-tissue defect that measures 6 cm x 6 cm, with an area of exposed bone and muscle on the distal medial leg that is a few centimeters proximal to the ankle. Management of the soft-tissue defect should now consist of

Explanation
The soft-tissue defect is in a very difficult position - the distal tibia. The defect is too distal for a gastrocnemius flap, and the exposed bone precludes an immediate skin graft. A free flap and skin graft would be required for closure. VAC is very effective in soft-tissue defects such as this one. Healthy granulation tissues form quickly. VAC can be the definitive treatment, or it can be used before skin grafting. Wet-to-dry dressings could promote granulation, but the process is hastened substantially by VAC. Amputation is not a consideration because there are no signs of infection or fracture healing problems at this time. Mooney JF III, Argenta LC, Marks MW, et al: Treatment of soft tissue defects in pediatric patients using the V.A.C. system. Clin Orthop 2000;376:26-31.
Question 4
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?


Explanation
The tibia has grown into valgus secondary to the proximal fracture. This occurs in about one half of these injuries, and maximal deformity occurs at 18 months postinjury. The deformity gradually improves over several years, with minimal residual deformity. Therefore, treatment at this age is unnecessary as there is a high rate of recurrence and complications regardless of technique. The valgus deformity is not a result of physeal injury or growth arrest. Medial proximal tibial hemiepiphysiodesis is an excellent method of correcting the residual deformity but is best reserved until close to the end of growth. Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482. McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 5
To control most spontaneous bleeding into the knee in children with hemophilia, factor VIII must be replaced to what percentage of normal?

Explanation
The knee is the most common location of spontaneous bleeding in children with hemophilia. Treatment generally requires replacement to 40% to 50% of normal. For surgery, the replacement should be to 100%. The plasma level generally rises 2% for every unit (per kg body weight) of factor VIII administered. Rodriquez-Merchan EC: Management of the orthopaedic complications of hemophilia. J Bone Joint Surg Br 1998;80:191-196.
Question 6
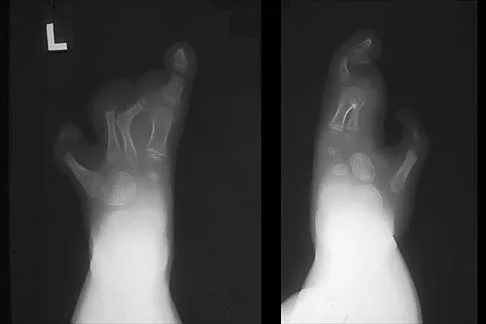
A 6-year-old girl is referred for the elbow injury seen in Figure 2. What is the most appropriate treatment?



Explanation
The patient has a displaced lateral condyle fracture; therefore, simple immobilization for 3 to 8 weeks is likely to result in malunion or nonunion. Closed reduction of such injuries is rarely successful. The fracture is unstable, so fixation is required after open reduction. Because the fixation must cross the physis, smooth pins are indicated for the skeletally immature elbow. Open reduction with fixation has been shown to reduce the risk of delayed union and malunion. Beaty JH, Kasser JR: The elbow: Physeal fractures, apophyseal injuries of the distal humerus, avascular necrosis of the trochlea, and T-condylar fractures, in Beaty JH, Kasser JR (eds): Fractures in Children, ed 5. Philadelphia, PA, Lippincott Williams & Wilkins, 2001, pp 625-703. Rutherford A: Fractures of the lateral humeral condyle in children. J Bone Joint Surg Am 1985;67:851-856.
Question 7
A patient who underwent closed reduction of the hips as an infant now reports pain. An abduction internal rotation view shows an incongruous joint. Based on the findings shown in Figure 3, what is the most appropriate type of pelvic osteotomy for the right hip?


Explanation
Pelvic osteotomies that redirect hyaline cartilage over the femoral head offer the potential for long-term preservation of the hip; however, salvage procedures such as the Chiari osteotomy are indicated in patients without a concentrically reducible hip. Ito and associates reported that moderate dysplasia and moderate subluxation without complete obliteration of the joint space and a preoperative center-edge angle of at least minus 10 degrees are desirable selection criteria. Ohashi H, Hirohashi K, Yamano Y: Factors influencing the outcome of Chiari pelvic osteotomy: A long-term follow-up. J Bone Joint Surg Br 2000;82:517-525.
Question 8
An 18-year-old girl with quadriplegic cerebral palsy underwent posterior spinal fusion from T2 to the pelvis 3 weeks ago. She now has a low-grade fever and mild midline erythema in a 1-cm area from which there is slight clear yellowish drainage. What is the next most appropriate step in management?


Explanation
The presence of drainage 3 weeks after surgery is a sign of wound infection. This infection most likely involves deep tissues until proven otherwise. Oral or IV antibiotics, in the absence of debridement, are not sufficient. Removal of the hardware would lead to rapid progression of the scoliosis in a spine that has been surgically destabilized by removal of the facet joints. The appropriate treatment is debridement with wound culture, IV antibiotics, and retention of hardware. The wound should be closed over drains. Theiss SM, Lonstein JE, Winter RB: Wound infections in reconstructive spine surgery. Orthop Clin North Am 1996;27:105-110.
Question 9
A 13-year-old girl is referred for a painful progressive valgus deformity of the right knee. Examination reveals an antalgic gait with an obvious valgus deformity. The right distal femur has a palpable, tender mass with erythema and warmth. Figures 4a and 4b show a clinical photograph and a radiograph. Management should consist of



Explanation
4b The radiograph shows a pathologic fracture through a destructive lesion of the distal femur metaphysis with osteolytic and osteoblastic features. The lateral cortex is destroyed, and there is periosteal new bone formation. These findings are consistent with malignancy, most likely an osteogenic sarcoma. Patients with suspected malignant tumors are best managed by surgeons with specific expertise in orthopaedic oncology. The biopsy of a malignant lesion should be deferred to the surgeon who is capable of definitive management of the patient. Enneking W: Principles of musculoskeletal oncologic surgery, in Evarts C (ed): Surgery of the Musculoskeletal System. New York, NY, Churchill Livingston, 1990.
Question 10
An 18-month-old boy with obstetric brachial plexus palsy is being evaluated for limited right shoulder motion. Physical therapy for the past 6 months has failed to result in improvement of the contracture. Which of the following studies is necessary prior to any shoulder reconstruction?

Explanation
The child sustained a brachial plexus injury at birth, and internal rotation/adduction contractures frequently develop at the shoulder. Initial treatment should consist of physical therapy to increase the range of motion. If this fails, as in this patient, MRI is used to evaluate the glenohumeral joint. Commonly, there is joint deformity with increased retroversion of the glenoid and even posterior shoulder subluxation. If the deformity is mild, an anterior release, coupled with teres major and latissimus transfers, is very effective. If the deformity is severe and the shoulder is unreconstructable, then humeral derotation osteotomy is the procedure of choice. MRI of the brain, a radiograph of the elbow, and aspiration of the shoulder would not be helpful. Waters PM: Update on management of pediatric brachial plexus palsy. J Pediatr Orthop B 2005;14:233-244. Waters PM, Bae DS: Effect of tendon transfers and extra-articular soft-tissue balancing on glenohumeral development in brachial plexus birth palsy. J Bone Joint Surg Am 2005;87:320-325.
Question 11
Where is the underlying defect in a rhizomelic dwarf with the findings shown in Figure 5?


Explanation
The radiograph shows the typical findings of achondroplasia. The defect is in fibroblast growth factor receptor 3. The pedicles narrow distally in the lumbar spine. The pelvis is low and broad with narrow sciatic notches and ping-pong paddle-shaped iliac wings. This is often called a champagne glass pelvis. Type I collagen abnormalities are typically found in osteogenesis imperfecta, and type II collagen defects are found in spondyloepiphyseal dysplasia and Kneist syndrome. COMP is defective in multiple epiphyseal dysplasia. Sulfate transport defects are seen in diastrophic dysplasia. Johnson TR, Steinbach LS: Essentials of Musculoskeletal Imaging. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 809-812.
Question 12
A 2-year-old boy has complete absence of the sacrum and lower lumbar spine. What is the most likely long-term outcome if no spinal pelvic stabilization is performed?

Explanation
Without stabilization, progressive kyphosis will develop between the spine and pelvis. The kyphosis progresses to the point that the child must use his or her hands to support the trunk, and therefore is unable to use his or her hands for other activities. Neck extension contracture does not usually develop. Neurologic deficit, including sexual dysfunction, is generally present at birth and static. Tachdjian MO: The spine: Congenital absence of the sacrum and lumbosacral vertebrae (lumbosacral agenesis), in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 3, p 2228.
Question 13
Which of the following findings is most prognostic for the ability of a young child with cerebral palsy to walk?

Explanation
Several studies have shown that sitting ability by age 2 years is highly prognostic of walking. Molnar and Gordon reported that children not sitting independently by age 2 years had a poor prognosis for walking. Wu and associates reported that children sitting without support by age 2 years had an odds ratio of 26:1 of walking compared with those unable to sit. This was far higher than the odds ratios for cerebral palsy location, motor dysfunction, crawling, creeping, scooting, or rolling. Molnar GE, Gordon SU: Cerebral palsy: Predictive value of selected clinical signs for early prognostication of motor function. Arch Phys Med Rehabil 1976;57:153-158.
Question 14
A 2-year-old girl has had a 2-day history of fever and refuses to move her left shoulder following varicella. Laboratory studies show an erythrocyte sedimentation rate of 75 mm/h and a peripheral WBC count of 18,000/mm3. What is the most common organism in this scenario?


Explanation
The most common bacterial etiologic agent following varicella is group A beta-hemolytic streptococcus. The other organisms are much less common. Staphylococcus aureus is the most common bone infection organism. Staphylococcus epidermidis is increasingly a bone infection organism. Group B streptococcus occurs more commonly in newborns. Kingella kingae is a common joint pathogen but is not as common following varicella. Schreck P, Schreck P, Bradley J, et al: Musculoskeletal complications of varicella. J Bone Joint Surg Am 1996;78:1713-1719.
Question 15
Which of the following is considered the best method to measure limb-length discrepancy in a patient with a knee flexion contracture?


Explanation
The most effective way to measure a limb-length discrepancy in a patient with a knee flexion contracture is a lateral CT scanogram. All the other methods listed provide inaccurate results with a knee flexion contracture because the measurements are made in the coronal plane. Aaron A, Weinstein D, Thickman D, et al: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Question 16
A 5-year-old boy sustained an elbow injury. Examination in the emergency department reveals that he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. The radial pulse is palpable at the wrist, and sensation is normal throughout the hand. Radiographs are shown in Figures 6a and 6b. In addition to reduction and pinning of the fracture, initial treatment should include



Explanation
6b The findings are consistent with a neurapraxia of the anterior interosseous branch of the median nerve. This is the most common nerve palsy seen with supracondylar humerus fractures, followed closely by radial nerve palsy. Nearly all cases of neurapraxia following supracondylar humerus fractures resolve spontaneously, and therefore, further diagnostic studies and surgery are not indicated. Cramer KE, Green NE, Devito DP: Incidence of anterior interosseous nerve palsy in supracondylar humerus fractures in children. J Pediatr Orthop 1993;13:502-505.
Question 17
An 11-year-old basketball player reports that he felt a painful pop in the left knee when he stumbled while running. He is unable to bear weight on the extremity and cannot actively extend the knee against gravity. Examination reveals a large knee effusion. A lateral radiograph is shown in Figure 7. Management should consist of


Explanation
The radiograph shows an avulsion fracture, or "sleeve fracture," of the distal pole of the patella. The distal fragment is much larger than it appears on the radiograph because it largely consists of cartilage; therefore, excision of the fragment is contraindicated. The treatment of choice is open reduction and tension band fixation to correct patella alta and restore the extensor mechanism. Maguire JK, Canale ST: Fractures of the patella in children and adolescents. J Pediatr Orthop 1993;13:567-571.
Question 18
Figures 8a and 8b show the clinical photograph and radiograph of a 4-month-old infant who has a left foot deformity. Examination reveals that the foot deformity is an isolated entity, and the infant has no known neuromuscular conditions or genetic syndromes. Which of the following studies will best confirm the diagnosis?



Explanation
8b The clinical photograph shows a rocker-bottom deformity, and the lateral radiograph suggests a congenital vertical talus deformity. A lateral radiograph of the foot in maximum plantar flexion is needed to demonstrate the fixed position of the deformity with malalignment of the talar-metatarsal axis. A fixed dislocation of the navicular on the talus differentiates a congenital vertical talus from the oblique talus with talonavicular subluxation. Kumar SJ, Cowell HR, Ramsey PL: Vertical and oblique talus. Instr Course Lect 1982;31:235-251. Kodros SA, Dias LS: Single-stage correction of congenital vertical talus. J Pediatr Orthop 1999;19:42-48.
Question 19
An 8-year-old girl was treated for a Salter-Harris type I fracture of the right distal femur 2 years ago. Examination reveals symmetric knee flexion, extension, and frontal alignment compared to the contralateral knee. She has 1-cm of shortening of the right femur. History reveals that she has always been in the 50th percentile for height, and her skeletal age matches her chronologic age. Radiographs are shown in Figure 9. What is the expected consequence at maturity?



Explanation
The child has a near complete central physeal arrest of the distal femur and worsening limb-length discrepancy will develop. She is growing at the average rate for the population. The distal femoral physis grows at a rate of roughly 9 mm per year. Girls finish their growth at approximately age 14 years. Thus, at maturity the left leg will be 6.4 cm longer than the right. An angular deformity has not developed at this point and her arrest is central; therefore, angular deformity is unlikely to develop in any plane. Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphysiodesis. J Pediatr Orthop 1996;16:173-179.
Question 20
Examination of an obese 3-year-old girl reveals 30 degrees of unilateral genu varum. A radiograph of the involved leg with the patella forward is shown in Figure 10. Management should consist of


Explanation
The clinical scenario describes infantile tibia vara (Blount's disease). The radiograph shows severe deformity with the characteristic Langenskiold stage 3 changes of the medial proximal tibial metaphysis that distinguish it from physiologic bowing. The preferred treatment is proximal tibiofibular osteotomy with acute correction into slight valgus to unload the damaged area of the physis. This method provides the best results in patients younger than age 4 years. Continued observation would result in progressive deformity. Bracing is most effective in younger children with less severe deformity. Lateral proximal tibial hemiepiphysiodesis relies on growth of the injured medial physis for correction and would result in severe tibial shortening in this young child. Complete epiphysiodesis also produces severe shortening and requires multiple lengthening procedures. Johnston CE II: Infantile tibia vara. Clin Orthop 1990;255:13-23.
Question 21
What is the most important consideration in the preoperative evaluation of a child with polyarticular or systemic juvenile rheumatoid arthritis (JRA)?

Explanation
The cervical spine may be involved in a child with polyarticular or systemic JRA; fusion or instability can occur. Radiographic assessment of the cervical spine should include lateral flexion-extension views. The potential exists for spinal cord injury during intubation or positioning in the presence of an unstable cervical spine. Limitations of the TMJ and micrognathia may affect ease of intubation and administration of anesthesia via a mask. If the TMJ and jaw are involved, some patients may have dental findings such as dental caries and even abscesses which can affect surgery. Some children, particularly those with systemic arthritis, may be taking corticosteroids long-term and may need stress dosing with complex surgeries. Although it is important to routinely check for uveitis and iritis in children with JRA, this usually is not needed preoperatively. Uveitis and iritis are less likely in a child with systemic JRA. Cassity JT, Petty RE (eds): Textbook of Pediatric Rheumatology, ed 5. Philadelphia, PA, WB Saunders, 2005. Ilowite N: Current treatment of juvenile rheumatoid arthritis. Pediatrics 2002;109:109-115. Ruddy S, Harris ED, Sledge CB (eds): Kelley's Textbook of Rheumatology, ed 6. Philadelphia, PA, WB Saunders, 2001.
Question 22
A 15-year-old boy has a mass at the knee. Radiographs show an aggressive tumor involving the proximal tibia, and biopsy findings reveal a high-grade osteosarcoma. Staging studies show that the tumor impinges on the neurovascular bundle. The tumor enlarges during preoperative chemotherapy. Management should now consist of

Explanation
Limb salvage procedures have become the usual treatment for even high-grade osteosarcomas. However, tumors associated with pathologic fracture, tumors encasing the neurovascular bundle, and tumors that enlarged during preoperative therapy and are adjacent to the neurovascular bundle require amputation.
Question 23
Figure 11 shows the radiograph of a 2-year-old child with marked genu varum and tibial bowing. Based on these findings, what is the best initial course of action?


Explanation
The radiograph shows multiple wide physes, consistent with a diagnosis of rickets. A low serum phosphorous level and an elevated alkaline phosphatase level are the hallmarks in diagnosing familial hypophosphatemic Vitamin D-resistant rickets. Serum calcium is usually normal or low normal. This disease is inherited as an X-linked dominant trait and usually presents at age 18 to 24 months. The disease results from a poorly defined problem with renal phosphate transport in which normal dietary intake of vitamin D is insufficient to achieve normal bone mineralization. Renal tubular dysfunction is associated with urinary phosphate wasting. Treatment involves oral phosphate supplementation, which can cause hypocalcemia and secondary hyperparathyroidism. To prevent associated problems, high doses of Vitamin D are administered. While obtaining a scanogram may be clinically indicated in an associated limb-length discrepancy, and subsequent corrective surgery may be indicated, either of these choices would not be the first course of action. An orthosis may slow the progression of genu varum in this disorder but is less important than establishing the correct diagnosis to begin pharmacologic treatment. This amount of varum and tibial bowing far exceeds the normal limits of physiologic genu varum. Skeletal dysplasias usually are not associated with abnormal laboratory values. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743.
Question 24
Figure 12 shows the radiograph of a 15-year-old boy with cerebral palsy who has pain at the first metatarsophalangeal joints. He is a community ambulator. Management consisting of accommodative shoes has failed to provide relief. What is the treatment of choice?


Explanation
While other surgeries have provided some success, first metatarsophalangeal joint arthrodesis has the highest overall success rate compared to other surgeries in ambulatory and nonambulatory children with cerebral palsy. The recurrence rate is unacceptably high with the other procedures listed above. In contrast, neurologically normal children are amenable to osteotomies and soft-tissue procedures. Davids JR, Mason TA, Danko A, et al: Surgical management of hallux valgus deformity in children with cerebral palsy. J Pediatr Orthop 2001;21:89-94.
Question 25
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery?



Explanation
The magnitude of the curve at the time of the peak height velocity is the most prognostic sign in relationship to surgery. More than 70% of curves that measure more than 30 degrees at this time are likely to reach surgical range. Little DG, Song KM, Katz D, et al: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Finish Exam?
You cannot change answers after submitting.
