Question 1
An 8-year-old boy sustains nondisplaced midshaft fractures of the tibia and fibula after being struck by a car while he was riding his bicycle. No other injuries are noted, but the patient reports pain with passive motion of his toes. His neurovascular examination is otherwise normal. What is the best course of action?
Explanation
Pain with passive motion of the toes is a recognized early sign of increased compartment pressures. At a minimum, a baseline evaluation of the leg compartment pressures should be obtained. While it is normal for the patient to have pain related to the associated muscle contusions, any significant concerns should be addressed immediately in light of the severe consequences likely when a compartment syndrome occurs. Mubarak SJ, Owen CA, Hargens AR, et al: Acute compartment syndromes: Diagnosis and treatment with the aid of the wick catheter. J Bone Joint Surg Am 1978;60:1091-1095.
Question 2
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include "onion bulb" formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?




Explanation
The patient has HMSN-III or Dejerine-Sottas syndrome. This form of HMSN progresses very rapidly and frequently results in severe foot deformity in early childhood. The changes are progressive and are the result of muscle imbalance during growth. Balancing of the foot musculature is essential, particularly during the phases of rapid growth of the foot. However, this cannot be accomplished using the anterior tibial muscle because it is already weak and the transfer will further weaken it. Bony procedures also may be required, and tendon transfers cannot be depended on to correct bony deformity. However, these procedures can be deferred until the foot is closer to adult size. Surgeries that lead to joint arthrodesis, such as triple arthrodesis and some midfoot osteotomies, are contraindicated because the feet may lose protective sensation as the disease progresses. Fusions in insensate feet are less successful than realignment procedures that maintain mobility. Wetmore RS, Drennan JC: Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am 1989;71:417-422. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth. J Bone Joint Surg Br 1989;71:17-20.
Question 3
An obese 4-year-old boy has infantile Blount's disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of


Explanation
The deformity is too severe for observation, and at age 4 years, the child is too old for orthotic treatment. To prevent recurrence, surgery should be performed before irreversible changes occur in the medial physis. A proximal tibial osteotomy should overcorrect the mechanical axis to 10 degrees of valgus. Bar resection has not been shown to be as effective in this severe deformity, especially without a concomitant osteotomy. Raney EM, Topoleski TA, Yaghoubian R, Guidera KJ, Marshall JG: Orthotic treatment of infantile tibia vara. J Pediatr Orthop 1998;18:670-674.
Question 4
A 10-year-old boy has activity-related knee pain that is poorly localized. He denies locking, swelling, or giving way. Examination shows mild tenderness at the medial femoral condyle and painless full range of motion without ligamentous instability. Radiographs are shown in Figures 2a through 2c. What is the best course of action?






Explanation
2b 2c The radiographs show an osteochondritis dissecans (OCD) lesion in the medial femoral condyle of a skeletally immature patient. The lesion is not displaced from its bed. Nonsurgical management of a stable OCD lesion in a patient with open physes consists of a period of activity limitation and occasional immobilization. Unstable lesions, loose bodies, and patients with closed physes require more aggressive treatment. Most of the surgical procedures can be done arthroscopically. Because the radiographic appearance is typical, biopsy is unnecessary. The radiographs do not show an osteocartilaginous loose body, and the patient reports no catching or locking; therefore, removal of the loose body is not indicated. Linden B: Osteochondritis dissecans of the femoral condyles: A long term follow-up study. J Bone Joint Surg Am 1977;59:769-776. Cahill BR: Osteochondritis dissecans of the knee: Treatment of juvenile and adult forms. J Am Acad Orthop Surg 1995;3:237-247.
Question 5
Figure 3a shows the preoperative radiograph of a 5-year-old girl who achieved complete correction with valgus osteotomies. Figure 3b shows a radiograph obtained 2 years later. What is the cause of the recurrent deformity on the right side?



Explanation
3b Although inadequate correction, obesity, patient age of older than 5 years and an increased metaphyseal-diaphyseal angle are all associated with a poorer outcome, the radiographs show a growth arrest of the medial tibial physis. If not recognized and treated with early surgery, progressive genu varum will occur with continued growth of the lateral physis. In addition to repeat osteotomy, options for treating the arrest include physeal bar resection or, as necessary, completion of the growth arrest by epiphyseodesis of the lateral physes, followed by a limb equalization procedure at a later date. Brooks WC, Gross RH: Genu varum in children: Diagnosis and treatment. J Am Acad Orthop Surg 1995;3:326-335. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 840-950.
Question 6
An 8-year-old boy reports ankle pain after striking the ground with the medial aspect of his foot while attempting to kick a soccer ball. Radiographs reveal slight distal tibial physeal widening but no other abnormalities. In treating this injury, which of the following associated conditions is most likely present but may be missed without careful evaluation?

Explanation
Malrotation of the foot is frequently overlooked in this clinical setting. This can be judged by evaluating and comparing the transmalleolar axes of the affected and unaffected legs. The rotation occurs through the physis and frequently is not recognized until the patient has been walking for a few months. The other conditions are not expected to occur in the clinical setting described. Phan VC, Wroten E, Yngve DA: Foot progression angle after distal tibial physeal fractures. J Pediatr Orthop 2002;22:31-35.
Question 7
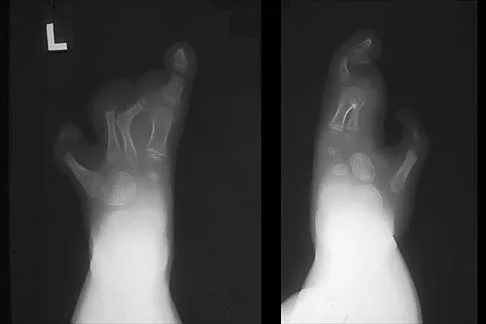
An 11-year-old girl has wrist pain. Figure 4a shows the radiograph, and Figures 4b and 4c show the low- and medium-power photomicrographs of a lesion in the distal radius. What is the most likely diagnosis?




Explanation
4b 4c The radiograph shows an osteolytic eccentric lesion in the metaphyseal-diaphyseal region of the bone, and the photomicrographs show an aneurysmal bone cyst. The low-power photomicrograph shows large empty spaces with fibrous stroma and multinucleated giant cells. The red area in the center is hemorrhage in the stroma. The large empty spaces are cysts, which would be filled with blood in vivo. The medium-power photomicrograph shows a large cyst-like space and hemorrhage in the surrounding stoma. Giant cell tumors have "sheets" of giant cells. A nonossifying fibroma would have spindle cells, and a unicameral bone cyst may have a few giant cells, but blood is rare. Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 540-542.
Question 8
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?


Explanation
In patients with vertebral tuberculosis, involvement of the anterior and posterior elements creates an instability and severe kyphotic collapse can occur. This characteristic has been shown to have a stronger association than level of involvement, age, or pretreatment degree of deformity. In the absence of instability, anterior growth can resume after treatment, leading to a decrease in the deformity. Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br 2001;83:954-962.
Question 9
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include


Explanation
Typically, posterior spinal fusion to the pelvis is recommended for patients with spinal muscular atrophy and advanced scoliosis. Examination for lower extremity muscle contractures is important because the contractures may interfere with good sitting balance. Anterior release and fusion usually are not advised. Diaphragmatic pacing is not indicated because diaphragm function usually is not affected. Patients with spinal muscular atrophy usually are not ambulatory or only marginally ambulatory at the time of scoliosis surgery; therefore, gait analysis usually is not relevant. While a muscle biopsy may have a role in the diagnosis of this disorder, it plays no subsequent role in determining life expectancy or the value of spinal surgery. Daher YH, Lonstein JE, Winter RB, Bradford DS: Spinal surgery in spinal muscular atrophy. J Pediatr Orthop 1985;5:391-395.
Question 10
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of

Explanation
The prognosis for a young patient with a head injury is more favorable compared to that for adults. Full neurologic recovery generally occurs. Spasticity may occur within a few days after injury, which can lead to fracture displacement if immediate spica casting or traction is used. Early surgical stabilization will reduce problems with shortening and malunion and will facilitate transportation of the child for diagnostic tests. Surgery may be performed when it is best for the patient, either on the day of injury or later if time is needed for stabilization. In this patient, the fracture is ideally suited to stabilization using flexible intramedullary nails. Heinrich and associates' report of 78 diaphyseal femur fractures stabilized with flexible intramedullary nails included 14 patients with an associated closed head injury. All fractures healed, and there were no major complications. Tolo VT: Management of the multiply injured child, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 83-95.
Question 11
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of


Explanation
Near complete correction and rebalancing of the spine can be achieved by hemivertebral resection that may be done as either a simultaneous or a staged procedure in the young patient. This eliminates the problem of future progression and possible development of compensatory curves. Nonsurgical management is not indicated in congenital scoliosis. Convex hemiepiphyseodesis is best suited for patients younger than age 5 years who have a short curve caused by fully segmented hemivertebrae that correct to less than 40 degrees with the patient supine. Hemiepiphyseodesis and isolated posterior fusion are not indicated. Bradford DS, Boachie-Adjei O: One-stage anterior and posterior hemivertibral resection and arthrodesis for congenital scoliosis. J Bone Joint Surg Am 1990;72:536-540.
Question 12
A newborn with bilateral talipes equinovarus undergoes serial manipulation and casting. What is the primary goal of manipulation?

Explanation
Manipulative treatment and casting of talipes equinovarus has become popular because of disappointing surgical results and enthusiasm for the Ponseti method of manipulation. In this technique, the primary goal is to rotate the foot laterally around a talus that is held fixed by the manipulating surgeon's hands. While the navicular may be rotated anterolaterally with this technique, the primary focus is on the calcaneus. The calcaneus is rotated laterally and superiorly, not translated. Some dorsiflexion of the calcaneus can be obtained by manipulation, but the primary focus is on the rotational relationship of the talus and calcaneus, not the degree of calcaneal dorsiflexion. Ponseti IV: Common errors in the treatment of congenital clubfoot. Int Orthop 1997;21:137-141.
Question 13
Figure 5 shows the radiograph of a 10-year-old girl who reports chronic shoulder pain after her gymnastics classes. Examination reveals pain on internal and external rotation but no instability. What is the most likely diagnosis?




Explanation
The patient has a very wide humeral growth plate, indicating the presence of a proximal humeral stress fracture, an uncommon diagnosis in gymnasts. Gymnasts are prone to stress fractures of the scaphoid, distal radius, elbow, and clavicle. Proximal humeral stress fractures are more commonly seen in those participating in racket or throwing sports. Stress fractures can lead to growth arrest or inhibition, particularly in the distal radius. The radiograph shows normal findings for the acromion, acromioclavicular joint, scapula, and triceps origin. Fallon KE, Fricker PA: Stress fracture of the clavicle in a young female gymnast. Br J Sports Med 2001;35:448-449. Sinha AK, Kaeding CC, Wadley GM: Upper extremity stress fractures in athletes: Clinical features of 44 cases. Clin J Sports Med 1999;9:199-202. Caine D, Howe W, Ross W, Bergman G: Does repetitive physical loading inhibit radial growth in female gymnasts? Clin J Sports Med 1997;7:302-308.
Question 14
Figure 6 shows the clinical photographs of a newborn who underwent a colostomy for an imperforate anus. Examination shows extended knees, flexed hips, and equinovarus feet. Dimpling is noted over the buttocks. Patients with these findings differ from patients with myelodysplasia in that they


Explanation
The patient has sacral agenesis. Clinical signs include the classic dimpling over the buttocks and the characteristic lower extremity deformities. Imperforate anus is often associated with this disorder. Although motor function correlates with the level of vertebral defect, sensation is usually intact. This is important therapeutically, because patients are not as prone to pressure sores as are those with myelodysplasia. Kyphosis may develop in many patients with lumbosacral agenesis, but lordosis is unusual. Latex allergy and progressive neural deterioration may occur in patients with either myelodysplasia or sacral agenesis but is more common in the former.
Question 15
Which of the following patients is considered the most appropriate candidate for selective dorsal rhizotomy?

Explanation
While other surgical and nonsurgical options exist for management of spasticity, the criteria originally laid out by Peacock and associates describe the most appropriate candidate for rhizotomy as a patient with spastic diplegia who is between the ages of 4 to 8 years and has a stable gait pattern that is limited by lower extremity spasticity. Rhizotomy is not recommended in patients with athetosis because of unpredictable results. In addition, rhizotomy should be avoided in nonambulatory patients with spastic quadriplegia because it is associated with significant spinal deformities. Peacock WJ, Arens LJ, Berman B: Cerebral palsy spasticity: Selective posterior rhizotomy. Pediatr Neurosci 1987;13:61-66. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29.
Question 16
A 2-day-old infant has the hyperextended knee deformity shown in Figure 7. No other deformities are found on examination. A radiograph shows that the ossified portion of the proximal tibia is slightly anterior to that of the distal femur. Management should consist of


Explanation
Congenital dislocation of the knee is an uncommon deformity that varies in presentation from simple hyperextension to complete anterior dislocation of the tibia on the femur. Treatment varies with the age at presentation and the severity of the deformity. Most authors recommend early nonsurgical management. A recent study of 24 congenital knee dislocations in 17 patients found that satisfactory results were obtained in most instances using closed treatment. Based on their findings, the authors concluded that immediate reduction or serial casting should be performed when the patient is seen early after birth. If the patient is seen late and correction cannot be achieved by serial casting, traction followed by closed or open reduction may be necessary. Early percutaneous quadriceps recession has been described for complex congenital knee dislocations associated with underlying disorders, such as arthrogryposis and Ehlers-Danlos syndrome. Ko JY, Shih CH, Wenger DR: Congenital dislocation of the knee. J Pediatr Orthop 1999;19:252-259. Johnson E, Audell R, Oppenheim WL: Congenital dislocation of the knee. J Pediatr Orthop 1987;7:194-200.
Question 17
Figures 8a and 8b show the current radiographs of a 10-year-old boy with a hip disorder who was treated with an abduction orthosis 3 years ago. If no further remodeling occurs, what is the most likely prognosis?



Explanation
8b The radiographs show a child with Legg-Calve-Perthes disease (LCPD) that has healed. Deformity (asphericity) of the femoral head is evident, but the femoral head and acetabulum are congruous. Stulberg and associates found that hips with aspherical congruity at skeletal maturity functioned well until the fifth or sixth decade of life. Similarly, another study found that degenerative arthritis caused deteriorating hip function after age 40 years in patients with this degree of residual deformity. Repeated episodes of ischemic necrosis are unlikely. Although some studies suggested coagulation abnormalities such as protein C and S deficiencies in children with LCPD, other studies failed to show any evidence of inherited thrombophila in most children with this disorder. There are no studies to suggest growth acceleration occurs following LCPD. Stulberg SD, Cooperman DR, Wallenstein R: The natural history of Legg-Calve-Perthes disease. J Bone Joint Surg Am 1984;66:479-489.
Question 18
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?



Explanation
PHV generally occurs while girls are still Risser 0; menarche typically occurs before Risser 1, which has a wide variation in its timing. The curve magnitude at the PHV is the best prognostic indicator available. Most untreated patients with curves greater than 30 degrees at PHV require surgery, while patients with smaller curves at that stage typically do not require surgery. Little DG, Song KM, Katz D, Herring JA: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Question 19
Examination of a 6-year-old boy who sustained a displaced Salter-Harris type II fracture of the distal radius reveals 35 degrees of volar angulation. A satisfactory reduction is obtained with the aid of a hematoma block. At the 10-day follow-up examination, radiographs show loss of reduction and 35 degrees of volar angulation. Management should now consist of

Explanation
In a 6-year-old child with a physeal fracture, the healing response 10 days after injury is so advanced that manipulation would have to be very forceful to be successful. A forceful manipulation in a patient this age increases the risk of early growth arrest and a significant disability because 80% of the growth of the radius comes from the distal physis. Because of the large contribution of growth from the distal radial physis and the angulation being in the plane of wrist motion, the potential for remodeling of this fracture is great. It is highly probable that this fracture will completely remodel in 1 to 2 years of growth. In this patient, even a "gentle" open reduction would probably require enough force that the physis would be damaged. Dimeglio A: Growth in pediatric orthopaedics, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 33-62.
Question 20
Figures 9a and 9b show the radiographs of a 12-year-old girl who has had right hip pain for the past 4 months. She reports that the pain is so severe that she is unable to walk and is now using a wheelchair. Examination reveals pain with any attempted range of motion. Management should include



Explanation
9b In addition to mild hip dysplasia, the radiograph shows an osteoblastic lesion of the right ilium. The patient's symptoms are much more severe than is typical for late hip dysplasia. MRI can determine the extent of the lesion in the bone and soft tissues. Following work-up and biopsy, the patient was diagnosed with Ewing's sarcoma. Springfield DS, Gebhardt MC: Bone and soft tissue tumors, in Morrissy RT, Weinstein SL (eds): Lovell and Winter's Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 507-518, 542-544.
Question 21
An 18-month-old boy has 45 degrees of kyphosis in the thoracolumbar spine secondary to type I congenital kyphosis. Examination reveals that he is neurologically intact, and an MRI scan shows no evidence of intraspinal pathology. Management should consist of

Explanation
Surgery is indicated for congenital kyphosis once the deformity reaches a certain size or if significant progression is documented. In a young patient with a relatively small deformity, the treatment of choice is isolated in situ posterior fusion and postoperative immobilization. If an adequate posterior fusion can be obtained, an epiphyseodesis effect can be generated, allowing the remaining anterior growth to cause some correction. Because there is no evidence of neurologic compression and the deformity is less than 50 degrees, anterior surgery is not indicated. There is no role for bracing in the management of congenital kyphosis. Winter RB: Congenital Deformities of the Spine. New York, NY, Thieme-Stratton, 1983, pp 229-261.
Question 22
Following an acute dislocation of the patella, the risk of a recurrent dislocation is greater if the patient has which of the following findings?

Explanation
Recurrent dislocations may follow an earlier dislocation. One study found that in patients who had a patellar dislocation between the ages of 11 to 14 years, 60% had a recurrent dislocation. The incidence of recurrent dislocation dropped to 33% in patients who had a patellar dislocation between the ages of 15 to 18 years. The authors also found that the incidence of recurrence was greater in patients who demonstrated a predisposition to dislocation as determined by evaluation of the unaffected knee. Predisposing signs included passive lateral hypermobility of the patella, a dysplastic distal third of the vastus medialis obliquis muscle, and a high and/or lateral position of the patella. A second study found that the risk of redislocation was considerably higher in patients who were in their teens at the first episode of dislocation compared to older patients. There are no studies linking either a patella baja or a bipartite patella to an increased risk of redislocation. Cash JD, Hughston JC: Treatment of acute patellar dislocation. Am J Sports Med 1988;16:244-249.
Question 23
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?

Explanation
Unopposed action of the tibialis anterior with weakness of the peroneus longus will lead to a dorsal bunion and supination deformity. Overpull of the gastrocnemius-soleus complex and posterior tibialis with weakness of the peroneus brevis will cause equinovarus deformity. A strong posterior tibialis with weakness of the peroneals will cause varus of the hindfoot. Unopposed peroneus brevis and incompetence of the posterior tibialis will lead to a flatfoot deformity. The etiology of a cavus foot is complex, but findings usually include a contracted plantar fascia and weakness of the tibialis anterior. Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 289-302.
Question 24
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?


Explanation
C-reactive protein declines rapidly as the clinical picture improves. Failure of the C-reactive protein to decline after 48 to 72 hours of treatment should indicate that treatment may need to be altered. Blood culture is positive only 50% of the time and will be negative soon after antibiotics are administered, even if treatment is not progressing satisfactorily. WBC count is highly variable and poorly correlated with treatment. The ESR rises rapidly but declines too slowly to guide treatment. Radiographic findings may not change but can take up to 2 weeks to show changes.
Question 25
Figure 10 shows the radiograph of a 7-year-old patient who has a bilateral Trendelenburg limp and limited range of hip motion but no pain. His work-up should include


Explanation
The radiograph shows bilateral flattening of the femoral heads with mottling and "fragmentation" suggestive of Legg-Calve-Perthes disease. However, when these changes occur bilaterally and are symmetric, multiple epiphyseal dysplasia or spondyloepiphyseal dysplasia should be suspected. Skeletal survey will show irregularity of the secondary ossification centers. With these conditions, there is no true osteonecrosis and no evidence that orthotic or surgical "containment" will alter the outcome of progressive degenerative arthritis. Cardiac anomalies and coagulopathies are not associated with the epiphyseal dysplasias. Crossan JF, Wynne-Davies R, Fulford GE: Bilateral failure of the capital femoral epiphysis: Bilateral Perthes disease, multiple epiphyseal dysplasia, pseudoachondroplasia, and spondyloepiphyseal dysplasia congenita and tarda. J Pediatr Orthop 1983;3:297-301.
Finish Exam?
You cannot change answers after submitting.
