Question 1
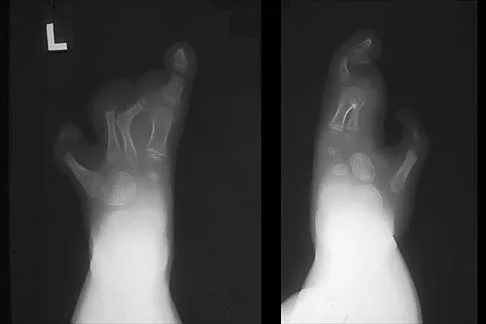
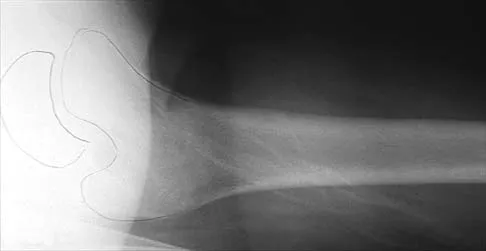
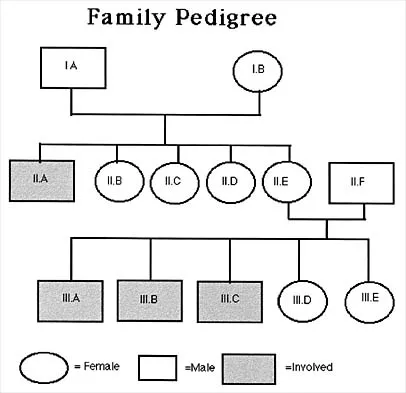
The inheritance of the deformity shown in Figure 1 is most commonly


































Explanation
Cleft hand and cleft foot malformations are commonly inherited as autosomal-dominant traits and are associated with a number of syndromes. An autosomal-recessive and an x-linked inheritance pattern have also been described, but these are much less common and are usually atypical. In the common autosomal-dominant condition, nearly one third of the known carriers of the gene show no hand or foot abnormalities. This is known as reduced penetrance. The disorder may be variably expressed; affected family members often exhibit a range from mild abnormalities in one limb only to severe anomalies in four limbs. Variable expressivity and reduced penetrance can cause difficulty in counseling families regarding future offspring in an affected family. Many patients have a cleft hand that may be caused by the split-hand, split-foot gene (SHFM1) localized on chromosome 7q21.
Question 2
Examination of a 12-year-old girl with bilateral anterior knee pain reveals excessive femoral anteversion and excessive external tibial torsion. The patient has no patellofemoral instability. Nonsurgical management consisting of muscle strengthening and nonsteroidal medication has failed to relieve the patient's pain. Treatment should now consist of





























Explanation
Children with symptomatic severe torsional malalignment of the lower extremity and patellofemoral pathology show excessive femoral anteversion and external tibial torsion on physical examination and analysis of gait. The functional effect of this torsional malalignment is centered about the knee joint. If nonsurgical management fails to alleviate patellofemoral pain, definitive surgical treatment should consist of corrective osteotomies, including internal rotation of the distal part of the tibia or external rotation of the femur, or both. Patients with surgical correction by osteotomy show an improved gait pattern and appearance of the extremity and a marked decrease in knee pain. External rotation of the distal part of the tibia or internal rotation of the distal part of the femur worsens the torsional malalignment. No additional soft-tissue realignment procedures, including retinacular release or patellar realignment, are required.
Question 3
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?

































Explanation
The enthusiasm with which dorsal rhizotomy was received led to the broadening of selection criteria with poorer results. The ideal candidate is an ambulatory 4- to 8-year-old child with spastic diplegia who does not use assistive devices or have joint contractures. The child must be old enough to actively participate in the rigorous postoperative physical therapy program. The use of the procedure in an ambulatory 16-year-old patient is less desirable because joint contractures will most likely have developed to a varying degree. The hemiplegic child is best treated by orthopaedic interventions. Oppenheim WL: Selective posterior rhizotomy for spastic cerebral palsy: A review. Clin Orthop 1990;253:20-29. Renshaw TS, Green NE, Griffin PP, Root L: Cerebral palsy: Orthopaedic management. J Bone Joint Surg Am 1995;77:1590-1606.
Question 4
A 3-year-old boy sustains a complete paralysis following a high thoracic spinal cord injury consistent with a SCIWORA-type injury (spinal cord injury without radiographic abnormality). Subsequent progressive spinal deformity will develop in what percent of patients with this injury?




































Explanation
Spinal cord injury in skeletally immature patients almost always leads to the development of paralytic spinal deformity. The age at injury is the most important factor affecting the development of scoliosis. Spinal cord injury that occurs more than 1 year prior to skeletal maturity is almost always followed by the development of scoliosis. In one study, scoliosis developed in 100% of children who were younger than age 10 years at the time of spinal cord injury. Scoliosis can occur after injury at any level. Spasticity is often a contributing factor. Up to two thirds of patients who have paralytic scoliosis prior to skeletal maturity will eventually require surgery for curve control. Mayfield JK, Erkkila JC, Winter RB: Spine deformity subsequent to acquired childhood spinal cord injury. J Bone Joint Surg Am 1981;63:1401-1411. Lancourt JE, Dickson JH, Carter RE: Paralytic spinal deformity following traumatic spinal cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
Question 5
A 12-year-old girl has progressive development of cavus feet. Examination reveals slightly diminished vibratory sensation on the bottom of the foot. Reflexes are 1+ at the knees and ankles. Motor examination shows that all muscles are 5/5 in the foot, except the peroneal and anterior tibial muscles are rated as 4+/5. Which of the following studies is considered most diagnostic?


































Explanation
The patient most likely has a form of Charcot-Marie-Tooth disease, or hereditary motor sensory neuropathy (HMSN). The most common varieties can now be diagnosed by DNA testing. Mutations have been detected in the peripheral myelin protein-22 (PMP-22) gene in HMSN type IA and in the connexin gene in the x-linked HMSN. Specific DNA diagnosis is useful in genetic counseling. Routine chromosomal testing most likely would not detect these mutations. Nerve conduction velocity study results are normal in some types of HMSN, and delayed nerve conduction, when found, indicates a peripheral neuropathy but does not specify the type or inheritance pattern. Biopsy of the sural nerve or of the quadriceps can be informative in some patients, but is not as specific as DNA testing. These procedures are most often reserved for patients with negative DNA test results. Chance PF: Molecular genetics of hereditary neuropathies. J Child Neurol 1999;14:43-52.
Question 6
A 2-year-old girl was born with the toe deformity shown in Figure 2. She has difficulty wearing shoes despite having adequate room in the toe box. Management at this time should consist of




Explanation
The patient has a congenital curly toe deformity of the third toe, and tenotomy of the toe flexors is highly effective for this problem. Stretching and taping are ineffective for this deformity. The position of the second toe is secondary; therefore, procedures on that toe are unnecessary and ineffective. The flexor to extensor transfer is a more complicated procedure that produces negligible results, or may even worsen the deformity. Resection arthroplasty is contraindicated because it causes abnormal growth of the toes. Hamer AJ, Stanley D, Smith TW: Surgery for curly toe deformity: A double-blind, randomized, prospective trial. J Bone Joint Surg Br 1993;75:662-663. Ross ER, Menelaus MB: Open flexor tenotomy for hammer toes and curly toes in childhood. J Bone Joint Surg Br 1984;66:770-771.
Question 7
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of



Explanation
Asymptomatic spondylolysis in a child or adolescent should be observed for the possible development of spondylolisthesis, but no other active intervention is needed. The initial treatment of choice for symptomatic spondylolysis includes rest and activity modifications, nonsteroidal anti-inflammatory drugs, physical therapy, bracing, and casting. Immobilization with a TLSO or pantaloon spica cast may permit healing of an acute pars fracture. Rarely, surgical treatment may be necessary. Surgical options include posterolateral L5-S1 fusion or direct repair of the pars defect. Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis. J Pediatr Orthop 1989;9:538-540.
Question 8
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20 degrees. Management should consist of







Explanation
Indications for surgical treatment of spondylolisthesis include pain and/or progression of deformity. Specifically, surgery is necessary when there is persistent pain or a neurologic deficit that fails to respond to nonsurgical therapy, there is significant slip progression, or the slip is greater than 50%. For patients with mild spondylolisthesis, in situ posterolateral L5-S1 fusion is adequate. In patients with more severe slips (greater than 50%), extension of the fusion to L4 offers better mechanical advantage. Postoperative immobilization may be achieved with instrumentation, casting, or both. In patients with a slip angle of greater than 45 degrees, reduction of the lumbosacral kyphosis with instrumentation or casting is desirable to prevent slip progression. Laminectomy alone is contraindicated in a child. Nerve root decompression is indicated if radiculopathy is present clinically. Seitsalo S, Osterman K, Hyvarinen H, Tallroth K, Schlenzka D, Poussa M: Progression of spondylolisthesis in children and adolescents: A long-term follow-up of 272 patients. Spine 1991;16:417-421.
Question 9
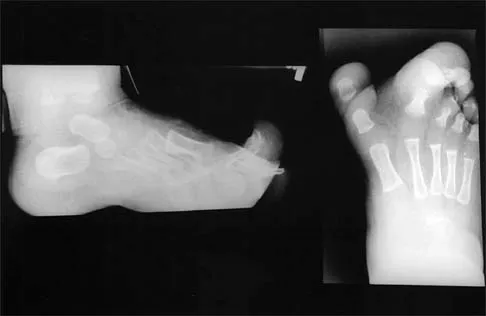
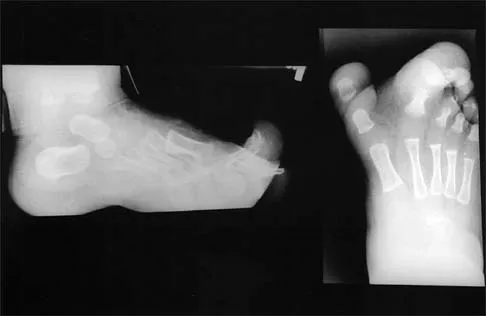
Figures 4a through 4c show the clinical photographs and radiographs of a 12-month-old boy who has progressive difficulty wearing shoes because of the length of the second toe, as well as width of the forefoot. Management should consist of









Explanation
4b 4c The patient has macrodactyly involving the second ray, with significant enlargement of the width and height of the foot. The radiographs show widening of the interval between the first and second metatarsal and between the second and third metatarsal. With this degree of involvement, amputation of the second ray with excision of the overgrowth of affected soft tissue provides the most consistent desired reduction in foot size. A threaded Steinmann pin should be inserted across the remaining metatarsals until healing has occurred. Patients with macrodactyly should be examined to exclude neurofibromatosis type 1 and Klippel-Trenaunay-Weber syndrome.
Question 10
Figures 5a and 5b show the radiographs of an 11-year-old boy who felt a pop and immediate pain in his right knee as he was driving off his right leg to jam a basketball. Examination reveals that the knee is flexed, and the patient is unable to actively extend it or bear weight on that side. There is also a large effusion. Management should include








Explanation
5b Fractures through the cartilage on the inferior pole of the patella, the so-called sleeve fracture, are often difficult to diagnose because of the paucity of ossified bone visible on the radiographs. If the fracture is missed and the fragments are widely displaced, the patella may heal in an elongated configuration that may result in compromise of the extensor mechanism function. The treatment of choice is open reduction and internal fixation using a tension band wire technique to achieve close approximation of the fragments and restore full active knee extension. Heckman JD, Alkire CC: Distal patellar pole fractures: A proposed common mechanism of injury. Am J Sports Med 1984;12:424-428.
Question 11
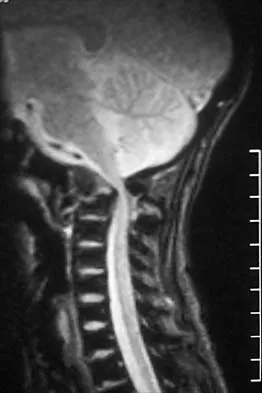
A 2-year-old child has been referred for management of congenital kyphosis. Neurologic examination is normal, and radiographs show a type I congenital kyphosis. Which of the following anomalies is seen in the MRI scan shown in Figure 6?




Explanation
There is a high incidence of intraspinal anomalies in patients with congenital scoliosis and kyphosis. Bradford and associates reported an incidence rate of 38% in 42 patients. The MRI scan shows that the filum terminale is thickened and adherent distally in the spinal canal. Although the conus is at L1, which may be normal, neurologic dysfunction may occur with further growth. There are no signals of high intensity within the cord that would suggest a syrinx. A Chiari II malformation would be found in the upper cervical region, not shown in this MRI scan. Meningocele and diastematomyelia are not present. Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 12
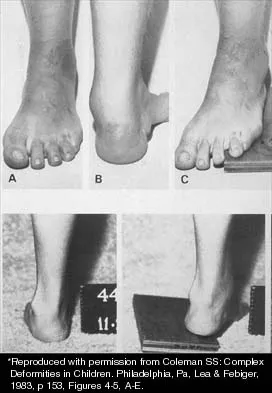
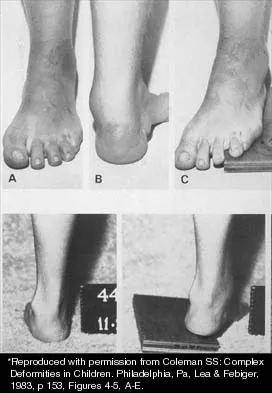
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of






Explanation
The clinical photographs show a patient with a type I hereditary sensory motor neuropathy who has cavus feet with a flexible hindfoot. The Coleman block test shows that the hindfoot corrects into valgus. To prevent progressive cavus, patients with this condition may benefit from soft-tissue releases at a younger age while the foot is flexible. Once there is fixed deformity, combined soft-tissue and bone procedures usually are necessary. Metatarsal osteotomies will correct the cavus, but will do nothing for the drop foot. Transfer of the extensor hallucis longus to the neck of the first metatarsal and modified transfer of the extensor digitorum longus to the dorsum of the foot will prevent further claw toes and improve foot dorsiflexion. Anterior transfer of the posterior tibialis tendon will also aid in dorsiflexion. Calcaneal osteotomy should be reserved for fixed hindfoot varus that does not correct with block testing, and triple arthrodesis should be avoided as long as possible because the long-term outcome is poor. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245. Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Question 13
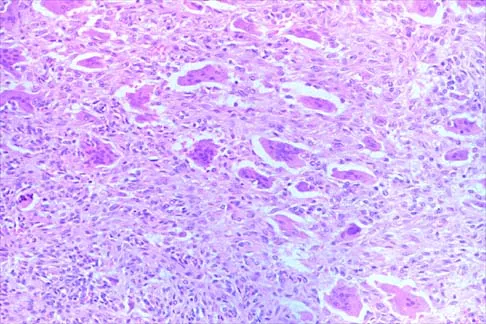
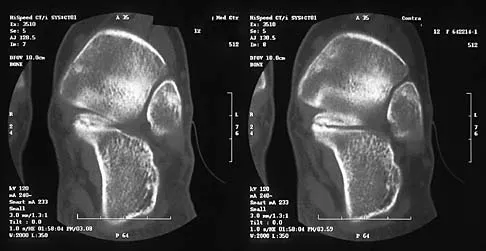
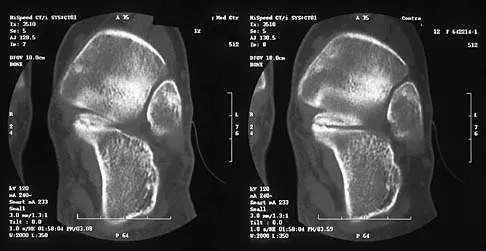
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of









Explanation
8b 8c 8d Tarsal coalitions commonly present in the preadolescent age group as a rigid, planovalgus foot. Small coalitions of the calcaneonavicular joint or the middle facet of the talocalcaneal joint can be excised with interposition of fat or muscle tissue. Isolated calcaneocuboid joint coalitions are very rare. This patient has an associated large talocalcaneal coalition; therefore, resection is contraindicated. Surgery is warranted after failure of nonsurgical management, and because of the involvement of two joints, the only viable option for the severely symptomatic foot is triple arthrodesis. Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Question 14
Figures 9a and 9b show the spinal radiographs of a 3-year-old child with short limb dwarfism. The lateral radiograph is obtained with maximal lumbar extension. Management should consist of





Explanation
9b The patient has kyphosis in association with achondroplasia. The AP radiograph shows decreased interpedicular distance at the lower lumbar vertebrae, a feature considered to be a distinctive sign of achondroplasia. Most patients with achondroplasia have kyphosis, and this usually resolves spontaneously. When the fixed component is greater than 30 degrees, however, brace treatment is recommended. Spinal fusion is seldom required.
Question 15
A 10-year-old boy with severe hemophilia A (factor VIII) sustained an injury to his right forearm 2 hours ago when a classmate fell on his arm during a scuffle. Examination reveals moderate swelling in the forearm, decreased sensation in the distribution of the median and ulnar nerves, and pain on passive extension of the fingers. What is the most appropriate sequence of treatment?






Explanation
The patient has severe hemophilia with a volar forearm hemorrhage and an emerging compartment syndrome. Therefore, it is critical to normalize the clotting deficiency as the first step in treatment. In a patient who has a factor VIII level of less than 1% and no inhibitors to factor VIII, transfusion with 4 unit/kg will typically raise the factor VIII level to 100%. Continuous transfusion can then be used to maintain this level. Compartment pressures can be safely measured after infusion of factor VIII. Because the hemorrhage is of limited duration and any surgery is considered serious in a patient with hemophilia, the compartment pressure should be measured before making a decision regarding a fasciotomy. However, it is important to note that the use of factor VIII concentrates allows both emergency and elective surgery provided that adequate hematology backup is available. Splinting the elbow and wrist in flexion reduces the pressure in the volar compartments, protects the forearm from further trauma, and makes the patient more comfortable. Greene WB: Diseases related to the hematopoietic system, in Morrissy RT, Weinstein SL (eds): Lovell & Winter's Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 345-391. Greene WB, McMillan CW: Nonsurgical management of hemophilic arthropathy, in Barr JS (ed): Instructional Course Lectures 38. Park Ridge, Ill, American Academy of Orthopaedic Surgeons, 1989, pp 367-381.
Question 16
Figures 10a and 10b show the radiographs of an athletic 9-year-old boy who has activity-related anterior knee pain with intact active knee extension. Examination reveals tenderness to palpation over the inferior pole of the patella. There is no effusion or ligamentous instability. Initial management should consist of








Explanation
10b The radiographs show fragmentation of the inferior pole of the patella. This finding, along with the clinical presentation, is most consistent with Sindig-Larsen-Johansson disease. This is an overuse syndrome commonly seen in boys ages 9 to 11 years. The differential diagnosis includes bipartite patella and patellar sleeve fracture. Like most overuse syndromes, Sindig-Larsen-Johansson disease responds to activity modification and nonsteroidal anti-inflammatory drugs. While symptoms usually resolve with short periods of activity restriction, radiographic findings may persist. Stanitski CL: Anterior knee pain syndromes in the adolescent. J Bone Joint Surg Am 1993;75:1407-1416.
Question 17
A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh. Passive movement of the hip appears to elicit tenderness and very limited hip motion. A radiograph of the pelvis shows mild subluxation of the left hip. The next step in evaluation should consist of


Explanation
The diagnosis of bone and joint sepsis in a newborn is difficult because of the relative lack of obvious signs and symptoms. Fever is usually absent. A study of 34 newborns with osteomyelitis identified prematurity and delivery by cesarean section as predisposing factors. In that study, the most common clinical findings were pseudoparalysis, local swelling, and pain on passive movement. Because early diagnosis is so important, any infant who exhibits these findings should be suspected as having bone or joint sepsis. Once the area of involvement is identified, aspiration is mandatory. In newborns who have an infection about the hip, radiographs may reveal subluxation. In this patient, septic arthritis must be ruled out by aspiration of the hip. Developmental dysplasia of the hip is not painful and is not accompanied by localized swelling. If no purulent material is obtained at the time of hip aspiration, an arthrogram should be obtained to rule out epiphysiolysis of the proximal femur. Because the area of involvement has been identified by clinical examination, a gallium scan or MRI scan of the spine is not indicated. Knudsen CJ, Hoffman EB: Neonatal osteomyelitis. J Bone Joint Surg Br 1990;72:846-851.
Question 18
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of




Explanation
The prognosis for most patients with Osgood-Schlatter disease is good. When the secondary ossification center unites with the main body of the tibial tubercle, the patellar tendon has a more rigid anchor, and heterotopic ossification and its associated reaction often become quiescent. However, even after closure of the growth plates, some patients have persistent symptoms. Excision of the ossicle and prominence of the tibial tuberosity decompresses the patellar tendon and allows most patients to resume sports activities. Nonsurgical modalities are ineffective. Better results have been reported after excision than after drilling of the tubercle. Excision of the ossicle is not indicated prior to skeletal maturity because symptoms will resolve in most patients when the secondary ossification center unites. Flowers MJ, Bhadreshwar DR: Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J Pediatr Orthop 1995;15:292-297.
Question 19
A 10-lb, 2-oz infant who was born via a difficult breech delivery 12 hours ago is now being evaluated for hip pain. Although the infant is resting comfortably, examination reveals that the patient is not moving the right lower extremity and manipulation of the right hip causes the infant to cry. The Galeazzi sign is positive. An AP radiograph of the pelvis shows proximal and superior migration of the right proximal femoral metaphysis. What is the most likely diagnosis?






Explanation
Transphyseal fractures of the proximal femur at birth are more likely to occur in large newborns after a difficult delivery. At rest, the patients are comfortable and show a pseudoparalysis; however, passive motion of the lower extremity results in discomfort. Teratologic hip dislocations will have a positive Galeazzi sign, but are not painful. Development of a septic hip would be unlikely within 12 hours postpartum. Congenital coxa vara is typically painless. Postpartum ligamentous laxity might account for a positive Ortolani sign, but is painless. Weinstein JN, Kuo KN, Millar EA: Congenital coxa vara: A retrospective review. J Pediatr Orthop 1984;4:70-77.
Question 20
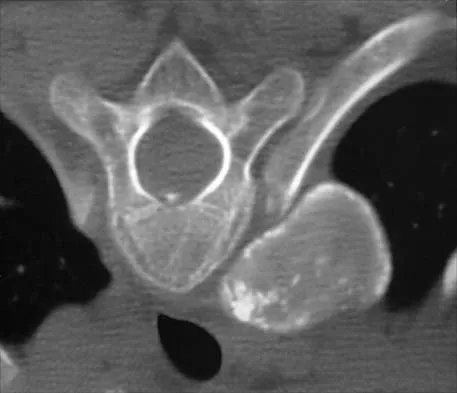
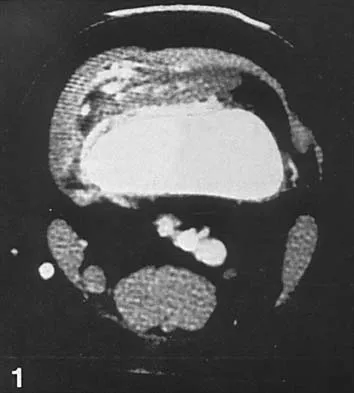
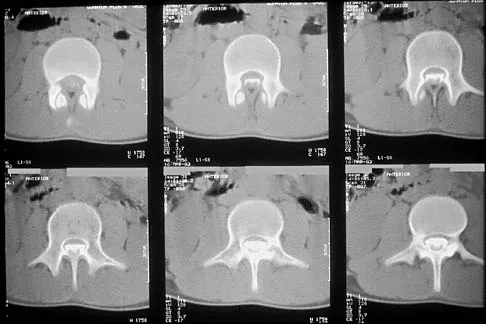
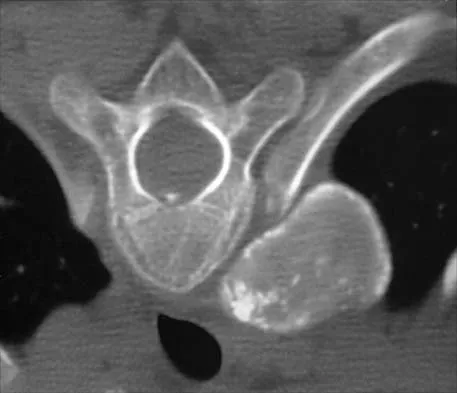
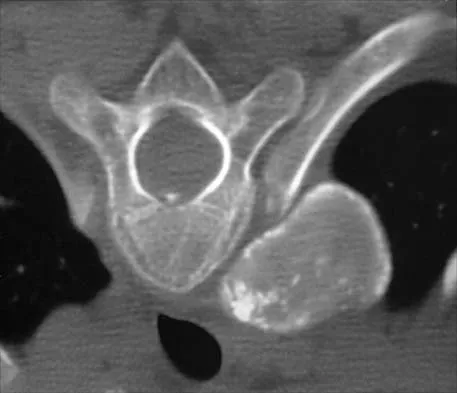
A 10-year-old girl has been referred for evaluation of a prominence at the lower cervical spine. The patient is asymptomatic, and the examination reveals no evidence of neurologic abnormality. A radiograph and CT scans are shown in Figures 12a through 12c. What is the most likely diagnosis?









Explanation
12b 12c Tuberculosis is uncommon in the cervical spine but has a relatively greater incidence in young children. In a review of 40 patients with lower cervical spine involvement (C2 to C7), 24 were younger than age 10 years at presentation. In children, the disease is characterized by more extensive involvement with the formation of large abscesses. In older patients with lower cervical tuberculosis, the disease is more localized but is more likely to cause paraplegia. Four-drug antituberculosis therapy should be used. For patients with pain or neurologic dysfunction, anterior excision of diseased bone and grafting are indicated. Whether vertebral body excision and grafting should be done in an asymptomatic 10-year-old child is debatable. The CT scan shows a large "cold" abscess that is partially calcified. Hsu LC, Leong JC: Tuberculosis of the lower cervical spine (C2 to C7): A report on 40 cases. J Bone Joint Surg Br 1984;66:1-5.
Question 21
Which of the following types of iliac osteotomy provides the greatest potential for increased coverage?




Explanation
The degree of acetabular dysplasia and the age of the child are important considerations when choosing what type of osteotomy to perform. The ability to obtain concentric reduction is a prerequisite of all osteotomies that redirect the acetabulum. Procedures that cut all three pelvic bones allow more displacement and, therefore, correction of acetabular dysplasia. The closer the osteotomy is to the acetabulum, the greater the coverage of the femoral head. Compared with the other acetabular osteotomies, the Ganz periacetabular osteotomy provides the greatest potential for correcting acetabular deficiency because there are no bone or ligamentous restraints to limit correction, but it has the disadvantage of being a technically demanding procedure. The amount of coverage provided by the Salter osteotomy is limited. Millis MB, Poss R, Murphy SB: Osteotomies of the hip in the prevention and treatment of osteoarthritis, in Eilert RE (ed): Instructional Course Lectures XLI. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1992, pp 145-154.
Question 22
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4 degrees F (37.4 degrees C), and examination reveals that abduction of the left hip is limited to 30 degrees. Laboratory studies show a WBC of 11,000/mm3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of




Explanation
The most likely diagnosis is transient synovitis. Initial management should consist of bed rest and serial observation to rule out atypical septic arthritis of the hip. In an unreliable family situation, hospitalization for bed rest and observation may be indicated. Other disorders such as proximal femoral osteomyelitis, leukemia, juvenile rheumatoid arthritis, pelvic osteomyelitis, diskitis, and arthralgia secondary to other inflammatory disorders should be considered. However, these disorders are unlikely because of the paucity of abnormal clinical signs exhibited by the patient. On the other hand, transient synovitis of the hip in children is a diagnosis of exclusion; other possibilities should be explored if the patient's symptoms do not follow a typical course and resolve in 4 to 21 days.
Question 23
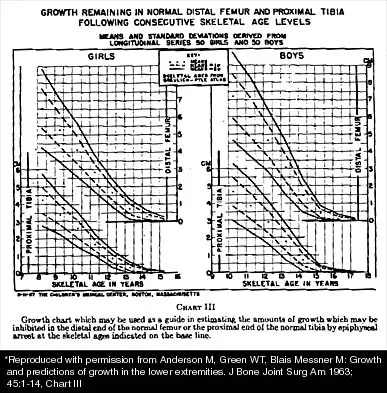
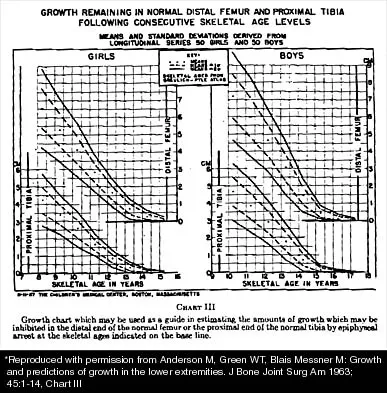
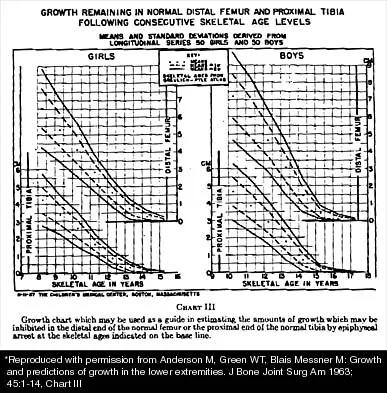
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of



Explanation
In a subgroup of patients with monoarticular JRA and a limb-length discrepancy that developed before the age of 9 years, Simon and associates showed that a subsequent growth deceleration on the affected side may correct a large part of the difference in length. This possibility would make surgery unnecessary and should prompt further observation. Simon S, Whiffen J, Shapiro F: Leg-length discrepancies in monoarticular and pauciarticular juvenile rheumatoid arthritis. J Bone Joint Surg Am 1981;63:209-215.
Question 24
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of








Explanation
15b 15c The plain radiograph and tomogram show an abnormality of the upper cervical spine, with erosion of the dens. The MRI scan shows evidence of cord impingement. The cervical spine is frequently involved in polyarticular JRA. Stiffness and autofusion are commonly seen, but C1-2 instability can also occur secondary to synovitis and bony erosion. Basilar invagination is rare in JRA. There is no consensus regarding fusion in the asymptomatic patient. In patients with symptoms and neurologic signs, C1-2 posterior fusion is indicated. Fried JA, Athreya B, Gregg JR, Das M, Doughty R: The cervical spine in juvenile rheumatoid arthritis. Clin Orthop 1983;179:102-106.
Question 25
Figures 16a and 16b show the radiographs of an otherwise healthy 3 1/2-year-old boy who has an isolated deformity of the left leg. Definitive primary treatment of this condition should consist of








Explanation
16b Treatment of congenital pseudarthrosis of the tibia is problematic. To achieve union, a resection of the pseudarthrosis, stabilization, and bone grafting must be performed. Simple cast immobilization does not yield union. There are various options for the resection, immobilization, and grafting. On the first surgical attempt, retrograde intramedullary nailing offers the best chance for success by transfixing the ankle and subtalar joints with abundant autogenous bone grafting. Distraction osteogenesis and vascularized free fibular graft are reserved as salvage procedures. Gilbert A, Brockman R: Congenital pseudarthrosis of the tibia: Long-term follow-up of 29 cases treated by microvascular bone transfer. Clin Orthop 1995;314:37-44. Boero S, Catagni M, Donzelli O, Facchini R, Frediani PV: Congenital pseudarthrosis of the tibia associated with neurofibromatosis - 1: Treatment with Ilizarov's device. J Pediatr Orthop 1997;17:675-684.
Finish Exam?
You cannot change answers after submitting.
