Question 76
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?

Explanation
Patients with a valgus alignment about the knee can have lateral compartment arthritis. Similar to a high tibial osteotomy, a supracondylar femoral osteotomy is indicated in younger patients who have a more active lifestyle and isolated unicompartmental disease. In this young patient who works in a factory and has a valgus knee, a medial closing wedge supracondylar femoral osteotomy is the treatment of choice. The role of arthroplasty is limited in younger patients. Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
Question 77
Figure 46 shows the AP radiograph of an active 80-year-old patient with an acetabular fracture. The fracture was initially managed nonsurgically; however, the patient is now scheduled to undergo total hip arthroplasty. What is the treatment of choice for the contained acetabular bone defect?

Explanation
Acetabular fractures can result in a relative or actual acetabular bone defect. The medial blow-out fracture of the acetabulum has united well in this patient. It is likely that a medial shell of bone will be present during hip arthroplasty. The femoral head may be used as morcellized or structural bone to augment the medial defect and is preferred to structural allograft. Bipolar hip arthroplasty is notorious for medial migration in patients without a medial bone defect; therefore, it will not be a good choice in this patient. Filling the defect with methylmethacrylate cement, though an option, is not the best option in this active patient with an extensive medial defect. A double-bubble acetabular cup is used for patients with deficiency of the bone in the dome region. Mears DC: Surgical treatment of acetabular fractures in elderly patients with osteoporotic bone. J Am Acad Orthop Surg 1999;7:128-141.
Question 78
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?
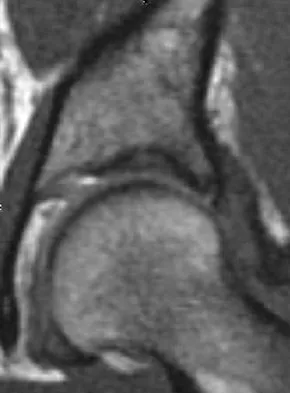
Explanation
The MRI arthrogram reveals dye extravasation into the labrum, consistent with a labral tear. The MRI findings are not typical of osteonecrosis, stress fracture, or transient osteoporosis. There is no increase in bone marrow edema in the neck or femoral head. Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.
Question 79
Figure 48a shows the full-leg standing radiograph of a patient with a prior femoral fracture. Figure 48b shows the lateral view of the same joint. The patient is scheduled to undergo total knee arthroplasty. Because the mechanical axis of the lower extremity in patients with a prior femoral fracture may be disrupted, which of the following should be used during surgery to restore the mechanical axis of the lower extremity in this patient?


Explanation
48b The radiograph shows hardware that was used for fixation of a prior femoral fracture. The mechanical axis of the lower extremity in this patient is nearly normal (3 degrees valgus), and the deformity at the healed fracture site (14 degrees) does not appear to affect the joint alignment and is acceptable. Use of a routine knee prosthesis will be possible in this patient. To avoid hardware removal, extramedullary jigs and/or computerized navigation may be used to measure and restore the long axis of the femur. The use of a hinged prosthesis does not influence the mechanical axis directly. Extra-articular osteotomy is occasionally needed to reverse severe deformities. Papadopoulos EC, Parvizi J, Lai CH, et al: Total knee arthroplasty following distal femoral fractures. Knee 2002;9:267-274.
Question 80
Figure 49 shows a histologic section of the lung in a patient who died during total hip arthroplasty. What unexpected finding is seen in the pulmonary capillaries?
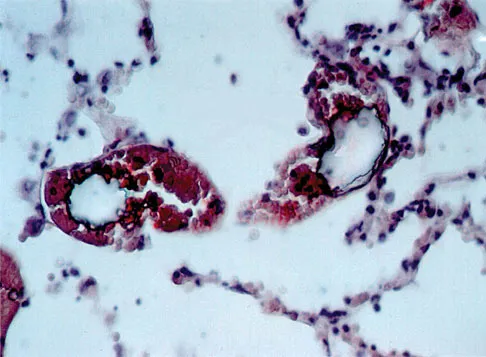
Explanation
Sudden death during total hip arthroplasty has been reported. In a report from the Mayo Clinic, intraoperative death occurred during cemented total hip arthroplasty in 23 patients. Fat and marrow embolization during preparation of the femur or cementing of the femoral component was believed to be responsible for the cardiopulmonary collapse that occurred during arthroplasty. Although fat and marrow emboli were found in the pulmonary capillaries of most of the patients on autopsy, this histologic section shows two particles of cement in the pulmonary capillaries. Parvizi J, Holiday AD, Ereth MH, et al: The Frank Stinchfield Award. Sudden death during primary hip arthroplasty. Clin Orthop 1999;369:39-48.
Question 81
After trial placement of components in a primary total knee arthroplasty, the knee is unable to come to full extension, but the flexion gap is appropriately balanced. After adequate soft-tissue releases have been performed, what is the next most appropriate action to balance the reconstruction?
Explanation
The reconstruction requires additional resection of the distal femur to allow increased extension while maintaining the current flexion gap tension. Resecting more proximal tibia or decreasing the tibial polyethylene thickness will decrease flexion tension as well as extension tension. Adding posterior femoral augments and using a larger femoral component will increase flexion tension. Ayers DC, Dennis DA, Johanson NA, et al: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Question 82
Figure 50 shows the cross table lateral radiograph of a 31-year-old paratrooper who has recalcitrant groin pain. The pain is worse after activities such as standing or sitting (driving). Examination reveals that pain can be reproduced by internal rotation of the leg with the hip and knee in 90 degrees of flexion. Extensive nonsurgical managment has failed to provide relief. What is the treatment of choice?

Explanation
The radiograph reveals the classic "bump" that is seen in patients with femoroacetabular impingement (FAI). Ganz and associates described two types of FAI. This patient has cam impingement, which describes a nonspherical femoral head being forced into the acetabulum during hip motion and resulting in labral and chondral injury. Hip arthroscopy and labral debridement is unlikely to control the symptoms because the underlying anatomic abnormality is often difficult to address with arthroscopy. The treatment involves surgical dislocation of the hip with preservation of the blood supply to the femoral head, removal of the asphericity on the femoral side (femoral osteoplasty), and removal of the acetabular rim (acetabular osteoplasty) if the latter is found to contribute to impingement. Ganz R, Gill TJ, Gautier E, et al: Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br 2001;83:1119-1124. Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: A cause for early osteoarthritis of the hip. Clin Orthop 2003;417:112-120.
Question 83
During total knee arthroplasty, the patella is noted to subluxate laterally despite a lateral retinacular release. Which of the following methods is most likely to improve patellar stability?
Explanation
Slight external rotation of the tibial component will cause a net medialization of the tibial tubercle when the knee is articulated. This will help centralize the extensor mechanism over the trochlear groove and minimize the tendency for lateral subluxation. Internal rotation of the femoral component increases the risk of patellar instability. Anterior translation of the tibial component moves the patellar tendon insertion posteriorly, and may increase force on the patella but should not substantially alter patellar tracking. Clinical studies have shown no patellofemoral benefits to the use of fixed- or mobile-bearing designs. Thicker patellar components will not improve tracking, and may compound the problem. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 207, 323-337 Pagnano MW, Trousdale RT, Stuart MJ, et al: Rotating platform knees did not improve patellar tracking: A prospective, randomized study of 240 primary total knee arthroplasties. Clin Orthop 2004;428:221-227.
Question 84
A 73-year-old man has stiffness after undergoing primary posterior cruciate ligament-retaining total knee arthroplasty 18 months ago. Extensive physiotherapy, dynamic splinting, and manipulations under anesthesia have failed to result in improvement. Examination reveals range of motion from 30 degrees to 60 degrees of flexion. The components are well fixed, and the evaluation for infection is negative. In discussing the possibility of revision arthroplasty, the patient should be advised that
Explanation
Stiffness following primary total knee arthroplasty remains a vexing problem. Treatment options have included extensive physical therapy, dynamic splinting, manipulation under anesthesia, arthroscopic arthrolysis, open arthrolysis with polyethylene exchange, and ultimately revision arthroplasty. Results are not as gratifying as would be expected. Babis and associates performed an open arthrolysis and polyethylene exchange on seven patients who were followed for a mean of 4.2 months. The results were poor. The mean improvement in arc of motion was only 20 degrees. Nicholls and Dorr treated 13 patients for stiffness. Only 40% of those patients obtained good to excellent results. Four patients (30%) required manipulation because of recurrent stiffness postoperatively. They noted they could not predictably improve the arc of motion with a revision operation. Haidukewych and associates reported on 15 patients who underwent revision of well-fixed components after total knee arthroplasty for stiffness. Of the 15 patients, 10 (66%) were satisfied with the outcome revision. Interestingly, they noted that in patients for whom the total arc of motion did not improve but who regained near full extension, there was a greater amount of satisfaction with the procedure than for those who did not regain full extension. Babis GC, Trousdale RT, Pagnano MW, et al: Poor outcomes of isolated tibial insert exchange and arthrolysis for the management of stiffness following total knee arthroplasty. J Bone Joint Surg Am 2001;83:1534-1536. Nicholls DW, Dorr LD: Revision surgery for stiff total knee arthroplasty. J Arthroplasty 1990;5:S73-S77.
Question 85
A 62-year-old patient is seen for routine follow-up after undergoing cementless total hip arthroplasty 2 years ago. The patient reports limited range of motion that severely affects daily activities. A radiograph is shown in Figure 51. Management should now consist of

Explanation
The patient has symptomatic postoperative heterotopic ossification after total hip arthroplasty. Postoperative prophylactic treatments include nonsteroidal anti-inflammatory drugs (usually indomethacin) or low-dose irradiation. The heterotopic ossification shown here is quite mature; therefore, nonsurgical management will not be successful. Surgical excision of grade III or IV heterotopic ossification should be followed with postoperative irradiation to minimize the chances of recurrence. Ayers DC, Evarts CM, Parkinson JR: The prevention of heterotopic ossification in high-risk patients by low-dose radiation therapy after total hip arthroplasty. J Bone Joint Surg Am 1986;68:1423-1430.
Question 86
What bilateral surgical intervention is considered inappropriate based on the findings shown in the radiograph in Figure 52?

Explanation
The radiograph reveals osteonecrosis of both femoral heads with reasonably maintained joint surfaces. There may be some slight flattening of the femoral heads. Hip arthrodesis is difficult to perform because of the necrotic bone. Its use in patients with osteonecrotic hips is limited because of the 80% bilaterality; therefore, it is not an acceptable alternative. All the other options are acceptable interventions. Mont MA, Jones LC, Sotereanos DG, et al: Understanding and treating osteonecrosis of the femoral head. Instr Course Lect 2000;49:169-185.
Question 87
Figure 53a shows the AP radiograph of a 70-year-old patient who is scheduled to undergo unicompartmental knee arthroplasty. Figure 53b shows the immediate postoperative radiograph, and the radiograph shown in Figure 53c, obtained 6 months after surgery, shows a medial tibial plateau fracture. The etiology of the fracture is best related to



Explanation
53b 53c While all of the above may contribute to the etiology of a tibial plateau fracture following unicompartmental knee arthroplasty, the recent literature has clearly noted that pin placement for fixation of tibial resection guides is the most critical factor associated with a tibial plateau fracture following unicompartmental knee arthroplasty. Vince and Cyran suggest that fractures associated with unicompartmental knee arthroplasty might be avoidable by limiting the number and paying attention to the location of the pin holes that are created to secure the tibial resection guides. Brumby and associates suggest avoiding multiple guide pin holes in the proximal tibia for unicompartmental knee arthroplasty. They currently recommend the use of one centrally placed pin and an ankle clamp to stabilize the resection guide. Yang and associates note that a medial tibial plateau fracture in association with minimally invasive unicompartmental knee arthroplasty can be eliminated by avoiding fixation pins close to the medial tibial cortex. Brumby SA, Carrington R, Zayontz S, et al: Tibial plateau stress fracture: A complication of unicompartmental knee arthroplasty using 4 guide pinholes. J Arthroplasty 2003;18:809-812. Yang KY, Yeo SJ, Lo NN: Stress fracture of the medial tibial plateau after minimally invasive unicompartmental knee arthroplasty: A report of 2 cases. J Arthroplasty 2003;18:801-803.
Question 88
During impaction of a cementless acetabular component, the posterior column was fractured and found to be displaced. Which of the following is considered the most appropriate surgical option?
Explanation
Acetabular bone loss presents a challenge during reconstruction. A cementless hemispherical cup can be used in most patients provided that the acetabular rim, particularly the posterior column, is intact. When the posterior column is disrupted, fixation with a reconstruction plate and/or the use of an antiprotrusio cage is recommended. The latter is particularly important when the posterior column is fractured and displaced, such as in this patient. Under these circumstances, reduction of the fracture and application of an antiprotrusio cage is recommended. In this particular type of case, some surgeons may elect to retain the hemispherical cup and apply an antiprotrusio cage over the cup ("cage over cup" technique). Berry DJ: Antiprotrusio cages for acetabular revision. Clin Orthop 2004;420:106-112.
Question 89
Which of the following factors increases the risk of sciatic nerve injury in primary total hip arthroplasty (THA)?
Explanation
Injury to the sciatic nerve is a relatively rare but serious complication of THA. Dissection of the sciatic nerve is not typically done during primary THA, although the nerve can be identified during the surgical approach. An anterolateral approach to THA would not necessarily be associated with any greater incidence of sciatic nerve injury than other approaches. Screw fixation for the acetabular component is often a matter of surgeon preference. Provided that the anatomic safe zones for screw fixation (posterior inferior and posterior superior) are recognized, injury to the sciatic nerve from acetabular screws can be minimized. Restoration of anatomic length is important in primary THA. Overlengthening can result in sciatic nerve palsy. Developmental dysplasia of the hip can lead to a congenitally shortened extremity with concomitant congenital shortening of the associated neurovascular structures. Overlengthening of the extremity during THA for developmental dysplasia of the hip can lead to sciatic palsy. Osteonecrosis is not an associated risk factor for sciatic nerve palsy. DeHart MM, Riley LH Jr: Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg 1999;7:101-111.
Question 90
A 68-year-old woman who underwent a right total hip arthroplasty 1 year ago has dislocated her hip five times since surgery. Radiographs show a retroverted acetabular component. What is the best treatment for this patient?
Explanation
The most common cause of recurrent dislocation following total hip arthroplasty continues to be component malposition. Component malposition should be addressed prior to any other treatment options, such as increasing soft-tissue tension with increased femoral offset or greater trochanteric advancement. A larger femoral head size may help, but correcting the component malposition should give more predictable results. A retroverted acetabular component should be revised to 15 degrees to 20 degrees of anteversion, matching the patient's anatomy with an abduction angle close to 45 degrees. Daly PJ, Morrey BF: Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am 1992;74:1334-1343. Jolles BM, Zangger P, Leyvraz PF: Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J Arthroplasty 2002;17-282-288.
Question 91
Figure 54 shows the preoperative radiograph of a 45-year-old woman who is considering total hip arthroplasty with her orthopaedic surgeon. What femoral characteristic is a typical concern in this patient?

Explanation
Developmental dysplasia of the hip (DDH) leads to early arthritis of the hip as seen in this patient. Although DDH is believed to mostly affect the acetabulum, most patients with DDH also have anatomic aberrations of the femur. Using three-dimensional computer models generated by reconstruction of CT scans, dysplastic femurs were shown to have shorter necks and smaller, straighter canals than the controls. The shape of the canal became more abnormal with increasing subluxation. The studies also have shown that the primary deformity of the dysplastic femur is rotational, with an increase in anteversion of 5 degrees to 16 degrees, depending on the degree of subluxation of the hip. The rotational deformity of the dysplastic femur arises within the diaphysis between the lesser trochanter and the isthmus and is not attributable to a torsional deformity of the metaphysis. Osteopenia is not a concern in a patient with an excellent cortical index (thick cortices and narrow canal). Femoral varus or bowing of the femur is not a typical finding in patients with DDH. Noble PC, Kamaric E, Sugano N, et al: Three-dimensional shape of the dysplastic femur: Implications for THR. Clin Orthop 2003;417:27-40.
Question 92
A 68-year-old man with no significant medical history underwent a total knee arthroplasty 4 years ago. A radiograph is shown in Figure 55. He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm3. Management should consist of

Explanation
The treatment of choice for a late hematogenous infection is two-stage resection arthroplasty and reimplantation, with parenteral antibiotics prior to reimplantation. This is particularly true when septic loosening has occurred as in this patient. Open irrigation and debridement with polyethylene exchange has been used successfully when the duration of symptoms is 3 weeks or less. Long-term suppressive antibiotics are most commonly used when the patient's medical condition precludes further surgery. Delayed reimplantation has been shown to be superior to immediate reimplantation in multiple studies. Little data support the use of arthroscopic irrigation and debridement. Swanson KC, Windsor RE: Diagnosis of infection after total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1485-1491.
Question 93
Which of the following substances makes up the majority by weight of the extracellular matrix for articular cartilage?
Explanation
The extracellular matrix consists of water, proteoglycans, and collagen. Water makes up the majority (approximately 65% to 80%) of wet weight; 95% of the collage is type II with much smaller amounts of other collagens, including types IV, VI, IX, X, and XI. The exact functions of these other collagens are unknown, but they are believed to be important in matrix attachment and stabilization of the diameter of collagen fibrils. Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 444-445.
Question 94
A 58-year-old woman is seen in the emergency department after falling at home. History reveals that she underwent right total knee arthroplasty 2 years ago. Radiographs are shown in Figures 56a and 56b. What is the most appropriate treatment?


Explanation
56b The radiographs show an oblique periprosthetic distal femoral fracture. Of the options listed, open reduction and internal fixation is the most appropriate surgical option because a well-fixed, posterior stabilized closed box femoral component is present. Nonsurgical methods are not favored because of the highly displaced, unstable fracture pattern and prolonged immobility. Revision with a stemmed component is an option but would sacrifice more bone stock in this younger patient. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. Raab GE, Davis CM III: Early healing with locked condylar plating of periprosthetic fractures around the knee. J Arthroplasty 2005;20:984-989.
Question 95
A patient with a valgus knee and lateral compartment bone loss undergoes a total knee arthroplasty using posterior condylar referencing instrumentation. Six months after surgery, the patient reports significant anterior knee pain, and radiographs reveal severe lateral patellar tilt. Management should consist of
Explanation
Severe valgus deformity is frequently accompanied by hypoplasia of the lateral femoral condyle. Posterior referencing instrumentation can substantially internally rotate the femoral component with respect to the transepicondylar axis and Whiteside's line. The femoral component malrotation must be corrected to properly address this problem. Berger RA, Della Valle CJ, Rubash HE: Patellofemoral problems in total knee arthroplasty, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1245-1258.
Question 96
Figures 57a through 57c show the radiographs of a patient who has pain, discomfort, and a popping sensation localized to the posterior aspect of the knee after undergoing primary left total knee arthroplasty 6 months ago. Examination reveals that the patient is able to ambulate without a limp. There is no significant swelling, erythema, or effusion. Range of motion is 0 degrees to 115 degrees, and a palpable crepitation or snapping is detected at the posterior lateral joint line. What is the most likely diagnosis?



Explanation
57b 57c Popliteal snapping syndrome represents the most likely diagnosis. Barnes and Scott noted that the popliteus tendon can be a potential source of internal derangement after total knee arthroplasty. They noted that it can be subluxated anteriorly and posteriorly over a retained lateral femoral condyle osteophyte. Allardyce and associates described the condition as a popliteus condition, snapping as it rolls over a retained lateral femoral condylar osteophyte. Patellar clunk syndrome is a distinct syndrome associated with the patella and has been reported in posterior stabilized knees. In addition to crepitation with range of motion, the patella literally snaps or jumps as the knee is taken from flexion to extension. Beight JL, Yao B, Hozack WJ, et al: The patellar "clunk" syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142. Barnes CL, Scott RD: Popliteus tendon dysfunction following total knee arthroplasty. J Arthroplasty 1995;10:543-545.
Question 97
Which of the following is the primary mechanism of polyethylene wear in the hip?
Explanation
Although previous theories on acetabular wear implicated fatigue cracking and delamination as primary wear mechanisms, these have actually manifested as major modes of polyethylene wear in knees. The primary mechanism of wear in polyethylene acetabular components appears to be adhesion and abrasion. In an analysis of 128 components retrieved at autopsy or revision surgery, wear appeared to occur mostly at the surface of the components and was the result of large strain plastic deformation and orientation of the surface layers into fibrils that subsequently ruptured during multidirectional motion. It was also shown conclusively that 32-mm heads displayed significantly more wear (volumetric wear) than either 22-mm or 26-/28-mm heads (1-mm increase in size increased volumetric wear by 10%). The wear at the articulating surface was characterized by highly worn polished areas superiorly and less worn areas inferiorly separated by a ridge. Abrasion was very common, occurring after adhesion and plastic deformation of polyethylene fibrils, and abrasion secondary to third-body wear. Wear rates decreased with longer survival of components, indicating a "bedding in" phenomenon, arguing against oxidative and fatigue wear. Crevice corrosion occurs in fatigue cracks with low oxygen tension (under screw heads, etc). Oscillatory fretting consists of cyclical abrading of the outer surface from small movements. Fatigue and delamination is predominant in total knee arthroplasty where stresses are maximum just below the surface of the polyethylene component, causing fatigue over time with subsequent delamination. In contrast, hip wear occurs primarily at the surface of the polyethylene component. Jasty M, Goetz DD, Bragdon CR, et al: Wear of polyethylene acetabular components in total hip arthroplasty: An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg Am 1997;79:349-358. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 47-53. Bell CJ, Walker PS, Abeysundera MR, et al: Effect of oxidation on delamination of ultrahigh-molecular-weight polyethylene tibial components. J Arthroplasty 1998;13:280-290.
Question 98
Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?
Explanation
Advocates of resurfacing hip arthroplasty cite preservation of the proximal femoral bone stock as the main advantage of this procedure over total hip arthroplasty. Fracture of the retained femoral neck has been reported following resurfacing arthroplasty. The exact etiology of the latter is unknown. Technical errors, such as notching of the femoral neck or possibly disruption of the blood supply to the femoral head during extensive soft-tissue exposure, may result in femoral neck fracture. Gabriel JL, Trousdale RT: Stem fracture after hemiresurfacing for femoral head osteonecrosis. J Arthroplasty 2003;18:96-99.
Question 99
Which of the following statements best describes results that have been reported with roentgen stereophotogrammetric analysis (RSA)?
Explanation
Migration of total hip femoral components has been measured by RSA, a technique that affords accuracy of 2 degrees and 0.5 mm. Several published studies on total hip arthroplasty femoral components have established the importance of this technique. Both cemented and cementless components migrate, with the rate of migration suggesting the adequacy of fixation of a component. Migration of 1 mm to 2 mm (occurring in either the varus-coronal plane and retroversion-transverse plane, or both) has been associated with a higher risk of loosening of the component.
Question 100
Osteonecrosis of the large joints may develop in patients with which of the following conditions?
Explanation
Osteonecrosis of major joints can occur in patients exposed to corticosteroids, alcohol, and antiseizure medications, as well as patients with hemaglobulinopathy, such as sickle cell anemia. In addition, patients with primary APS who had not taken corticosteroids were also found to be at high risk for osteonecrosis of the hip. In one study of 30 patients with primary APS, asymptomatic osteonecrosis was evident in 20%. A recent article has also found a high association between idiopathic osteonecrosis of the hip and collagen II mutation. None of the other conditions has been shown to be associated with a higher risk of osteonecrosis. Tektonidou MG, Malagari K, Vlachoyiannopoulos PG, et al: Asymptomatic avascular necrosis in patients with primary antiphospholipid syndrome in the absence of corticosteroid use: A prospective study by magnetic resonance imaging. Arthritis Rheum 2003;48:732-736.
Finish Exam?
You cannot change answers after submitting.
