Question 1
A patient is scheduled to undergo total knee arthroplasty (TKA) following failure of nonsurgical management. History reveals that she underwent a patellectomy as a teenager as the result of a motor vehicle accident. Examination reveals normal ligamentous stability. For the most predictable outcome, which of the following implants should be used?

Explanation
Paletta and Laskins performed a retrospective study of the results of TKA with cement in 22 patients who had a previous patellectomy. Nine of the patients had insertion of a posterior cruciate ligament-substituting implant. Thirteen patients had insertion of a posterior cruciate ligament-sparing implant. The 5-year postoperative knee scores were 89 for the posterior cruciate ligament-substituting knee versus 67 for the posterior cruciate ligament-sparing knee (P < 0.01). The patella functions to increase the lever arm of the extensor mechanism and to position the quadriceps tendon and the patellar ligament roughly parallel to the anterior cruciate ligament and posterior cruciate ligament, respectively. The patellar ligament thereby provides a strong reinforcing structure that functions to prevent excessive anterior translation of the femur during flexion of the knee. The absence of the patella results in the patellar ligament and the quadriceps tendon being relatively in line with one another. After a patellectomy, the resultant quadriceps force is no longer parallel to the posterior cruciate ligament. This results in loss of the reinforcing function of the patellar ligament. The authors believe this loss of reinforcing function may place increased stresses on the posterior cruciate ligament and posterior aspect of the capsule, which may result in stretching of these structures over time. They found a high rate of anteroposterior instability, a high prevalence of recurvatum, and a high rate of loss of full active extension compared with passive extension in the posterior cruciate ligament-sparing group, which supports their theory. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 559-582.
Question 2
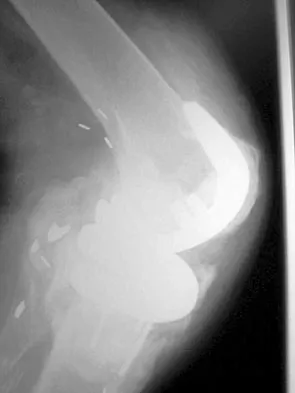
Figure 1 shows the radiograph of a patient who underwent a total knee revision with a posterior stabilized mobile-bearing prosthesis and now has recurrent knee dislocations. What is the most likely cause?


Explanation
The patient has a posterior stabilized total knee revision, and the femoral component has dislocated over the tibial polyethylene cam/post. This usually indicates a loose flexion gap, or "flexion instability." A loose flexion gap can occur due to undersizing of the femoral component, anteriorization of the femoral component, excessive distal augmentation of the distal femur, or collateral ligament insufficiency, especially if combined with posterior capsular insufficiency. Isolated laxity of the extension gap (with a well-balanced flexion gap) causes varus/valgus instability, but it rarely causes the femoral component to "jump" the tibial cam of a posterior stabilized tibial insert. Malrotation of the components may cause patellar instability or a rotational instability of the tibiofemoral joint but should not cause a frank posterior dislocation of the tibia, unless combined with other errors of balancing. Although a mobile-bearing total knee arthroplasty may be more sensitive to errors in balancing than a fixed-bearing total knee arthroplasty, this complication does not reflect a faulty prosthetic design. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 339-365. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 173-186, 227-249.
Question 3
A metal-on-metal bearing used for total hip arthroplasty shows which of the following properties?

Explanation
Activity levels do not affect cobalt and chromium ion levels, which are the bulk of serum ion levels. The majority of ions are produced in the run-in period in the first several years. A gradual reduction in ion levels occurs thereafter. The kidneys are responsible for the bulk of clearance from the serum, and to date there is no relationship of cancer to ion levels in the serum.
Question 4
Which of the following treatment regimens for thromboembolic prophylaxis meets the American College of Chest Physicians Guidelines for 10-day treatment after total hip arthroplasty and total knee arthroplasty?

Explanation
Only three thromboembolic treatment protocols have reached Grade 1A status for the American College of Chest Physicians Guidelines for thromboembolic prophylaxis after total hip arthroplasty and total knee arthroplasty. Grade 1A evidence shows a clear benefit/risk improvement with supportive data from randomized clinical trials, which are strongly applicable in most clinical circumstances. Warfarin is recommended but at an INR level of 2 to 3. Low-molecular-weight heparin and fondaparinox are also acceptable treatment options. Aspirin, adjusted dose unfractionated heparin, and elastic compressive stockings are not recommended as stand-alone options. Colwell C: Evidence based guidelines for prevention of venous thromboembolism: Symposia. Proceedings of the 2005 AAOS Annual Meeting. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 15-18.
Question 5
Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include



Explanation
2b The radiographs show massive subsidence of the lateral side of the tibia with severe tibial bone loss and a fractured proximal fibula. Reconstruction should consist of a large metal or bony lateral tibial augmentation, and a stem long enough to bypass the defect is required. The femoral and tibial components are articulating without any remaining polyethylene medially; therefore, the femoral component is damaged and needs revision. The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250. Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Question 6
Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?


Explanation
The radius of curvature of the distal femur is greater over the distal aspect of the lateral femoral condyle than the distal aspect of the medial femoral condyle. As the femur rolls posteriorly during early knee flexion, both condyles undergo similar angular changes equal to the amount of flexion. With a similar amount of angular rotation, the sphere with the larger radius experiences greater net rollback, producing a pivoting motion. Although the anterior cruciate ligament plays a role in producing tibial rotations, the posterior cruciate ligament does not play a significant role in producing such rotations. Similarly, the tibial tubercle does not play a significant role in producing normal rotations of the femur relative to the tibia. The popliteus may also play a role in producing rotational pivots, as might differential laxity of the medial and lateral collateral ligaments in early knee flexion. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.
Question 7
Figure 3 shows the AP radiograph of a patient with diabetes mellitus who has knee pain. A semiconstrained knee prosthesis was used in this patient to prevent which of the following complications?


Explanation
The radiographic appearance of the joint is highly suspicious for neuropathic joint (Charcot's joint). Evidence of bone loss on both the tibial and the femoral sides may necessitate the use of metal and/or bone augments. Patients with a neuropathic joint often have excellent range of motion, and postoperative stiffness is not a problem. The main problem with these patients is instability that occurs secondary to ligamentous laxity. Use of a semiconstrained prosthesis prevents the latter complication. Parvizi J, Marrs J, Morrey BF: Total knee arthroplasty for neuropathic (Charcot) joints. Clin Orthop 2003;416:145-150.
Question 8
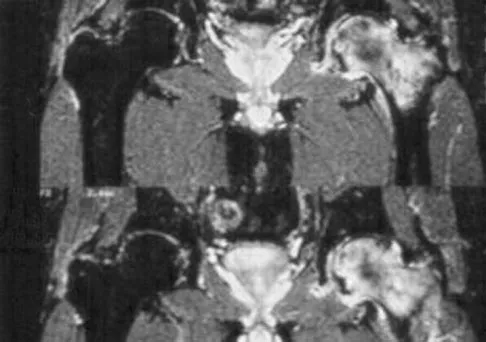
Based on the radiograph shown in Figure 4, the innervation of what muscle is most at risk with total hip arthroplasty?


Explanation
The radiograph reveals a Crowe IV deformity in a patient with developmental dysplasia of the hip. If hip arthroplasty is performed, then some degree of limb lengthening is anticipated. Excessive limb lengthening can result in sciatic nerve palsy in these patients. The peroneal branch of the sciatic nerve is most often affected. Of the muscles listed, only the extensor hallucis longus is innervated by the peroneal branch of the sciatic nerve. Eggli S, Hankemayer S, Muller ME: Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br 1999;81:843-845.
Question 9
A 75-year-old woman who fell on her right knee now reports pain and is unable to bear weight. History reveals that she underwent total knee arthroplasty on the right knee 6 years ago. Radiographs are shown in Figure 5. Management should now consist of



Explanation
The radiographs show a loose femoral component with an associated medial condyle distal femoral fracture. The treatment of choice is open reduction and internal fixation with revision of the femoral component because of the femoral component loosening. Moran MC, Brick GW, Sledge CB, et al: Supracondylar femoral fracture following total knee arthroplasty. Clin Orthop 1996;324:196-209. McLaren AC, DuPont JA, Schroeber DC: Open reduction internal fixation of supracondylar fractures above total knee arthroplasties using the intramedullary supracondylar rod. Clin Orthop 1994;302:194-198.
Question 10
Which of the following nutraceuticals has been associated with perioperative bleeding?

Explanation
Ginkgo biloba is a popular nutraceutical for patients who have early dementia, intermittent claudication secondary to peripheral vascular disease, vertigo, and tinnitus. It is reported to improve mental alertness and cognitive deficiency. It has antiplatelet properties as a result of one of its components, ginkgolide B, which displaces platelet-activating factor from its receptor binding sight. Rowin and Lewis reported on spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Vale also reported on subarachnoid hemorrhage associated with ginkgo biloba. Bebbington and associates reported on persistent postoperative bleeding after total hip arthroplasty secondary to ginkgo biloba usage. Furthermore, the use of ginkgo biloba with aspirin or other antiplatelet agents or anticoagulants represents a relative contraindication. Physicians should be aware not only of prescribed medications but also alternative nutraceuticals that are used by the patient. Rowin J, Lewis SL: Spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Neurology 1996;46:1775-1776. Vale S: Subarachnoid hemorrhage associated with ginkgo biloba. Lancet 1998;352:36.
Question 11
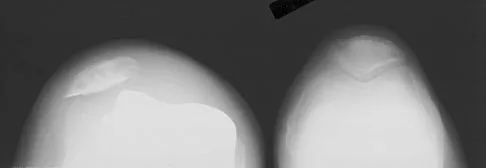
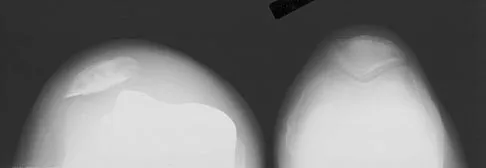
A 64-year-old man undergoes a primary total knee arthroplasty. Three months after surgery he reports persistent pain, weakness, and difficulty ambulating. Postoperative radiographs are shown in Figures 6a through 6c. What is the best course of action at this time?



Explanation
6b 6c The Merchant view reveals subluxation of the patellar component. The etiology of maltracking of the patella includes internal rotation of the femoral component, internal rotation of the tibial component, excessive patellar height, and lateralization of the patella component. The treatment of choice in this patient is revision total knee arthroplasty with external rotation of the femoral component. Preoperatively the patient also may require a lateral release, revision of the tibial component if it is internally rotated, and possibly a soft-tissue realignment. Component malalignment needs to be addressed first. Kelly MA: Extensor mechanism complications in total knee arthroplasty. Instr Course Lect 2004;53:193-199. Malkani AL, Karandikar N: Complications following total knee arthroplasty. Sem Arthroplasty 2003;14:203-214.
Question 12
Compared to metal-on-polyethylene total hip bearing surfaces, the debris particles generated by metal-on-metal articulations are


Explanation
Retrieval studies have shown that the debris particles produced by metal-on-metal articulations in total hip arthroplasty are several orders of magnitude smaller and may be up to 100 times more numerous than those found with metal-on-polyethylene articulations. Davies AP, Willert HG, Campbell PA, et al: An unusual lymphocytic perivascular infiltration in tissues around contemporary metal-on-metal joint replacements. J Bone Joint Surg Am 2005;87:18-27.
Question 13
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?



Explanation
Patella baja is commonly encountered when converting a high tibial osteotomy (HTO) to a TKA. Patella baja most likely occurs because of scarring. Meding and associates' study did not show an increased rate of lateral release when converting a knee that had undergone a previous HTO. Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1265-1271.
Question 14
Antibiotic-loaded bone cement prostheses, such as that shown in Figure 8, are best created by using which of the following methods?


Explanation
In a review of the practical applications of antibiotic-loaded bone cement for the treatment of the infected total joint arthroplasties, Hanssen and Spangehl described commercially available antibiotic-loaded bone cement as low-dose antibiotic cements. These cements generally contained 0.5 g of either tobramycin or gentamicin per 40 g of cement. They are indicated for use in prophylaxis and not for treatment of infected total joint arthroplasties. High-dose antibiotic-loaded bone cements are described as those containing greater than 1.0 g of antibiotic per 40 g of cement. Effective elution levels have been documented with 3.6 g tobramycin and 1.0 g vancomycin per 40 g of bone cement. This was documented by Penner and associates. Furthermore, it was shown that the combination of the two antibiotics in the bone cement improved the elution of both antibiotics. Hanssen AD, Spangehl MJ: Practical applications of antibiotic-loaded bone cement for treatment of infected joint replacements. Clin Orthop 2004;427:79-85.
Question 15
Figures 9a and 9b show the radiographs of a 75-year-old man who underwent a revision total knee arthroplasty with a long-stemmed tibial component. In rehabilitation, he reports fullness and tenderness in the proximal medial leg (at the knee). The strategy that would best limit this postoperative problem is use of



Explanation
9b The problem with this reconstruction is the medial protrusion of the base plate. The use of a base plate with an offset stem can prevent the protrusion and thus the impingement and pain. Allograft bone or smoothing the outline with cement would be just as prominent and likely to cause pain. An ingrowth surface may improve soft-tissue attachment but would still leave the implant protruding medially and likely to cause pain. A nonstemmed tibial base plate would lead to less medial protrusion but at the expense of a smaller area for load carriage on the proximal tibia.
Question 16
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?


Explanation
The patient has a periprosthetic fracture around a loose cemented femoral component. The proximal bone stock is poor; therefore, this fracture may be categorized as Vancouver 3-B. Hip arthrodesis and resection arthroplasty provide suboptimal results, particularly for ambulatory patients. Although impaction allografting may be an option to restore the bone stock in a younger patient, the latter procedure will be very difficult to perform when the proximal bone is poor in quality and fractured. Cementing another component into this wide femur is not an option. The best option for revision of the femoral component in this elderly patient is proximal femoral replacement arthroplasty. Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Question 17
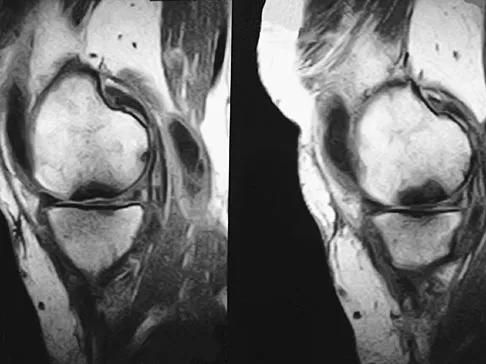
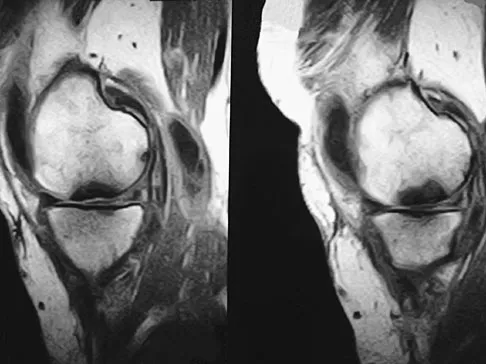
A 74-year-old woman has had acute medial right knee pain for the past 3 months. She denies any history of trauma or previous problems. Coronal and sagittal MRI scans are shown in Figures 11a and 11b. What is the most likely diagnosis?


Explanation
11b Spontaneous osteonecrosis of the medial femoral condyle is seen in the MRI scans, and is most common in women older than age 60 years. Although usually present in the weight-bearing portion of the medial femoral condyle, spontaneous osteonecrosis has also been described involving the lateral femoral condyle and patella. Most patients are seen postcollapse, and the treatment of choice is arthroplasty. Optimal treatment in precollapse stages is controversial. Kidwai AS, Hemphill SD, Griffiths HJ: Spontaneous osteonecrosis of the knee reclassified as insufficiency fracture. Orthopedics 2005;28:236,333-336. Soucacos PN, Xenakis TH, Beris AE, et al: Idiopathic osteonecrosis of the medial femoral condyle: Classification and treatment. Clin Orthop 1997;341:82-89.
Question 18
Patients with patellar clunk syndrome are best managed by which of the following methods?

Explanation
Patellar clunk syndrome is usually the result of a fibrous nodule that forms on the undersurface of the distal quadriceps tendon. It may get entrapped in the intercondylar notch of the femoral component during flexion, and lead to a sudden snap as the nodule is pulled out of the notch during active extension. Nonsurgical management is rarely successful. Surgical debridement is usually curative, with only rare recurrence. More aggressive procedures such as realignment, revision, or patellectomy are usually not necessary, and are reserved for cases resistant to soft-tissue debridement. Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 329. Diduch DR, Scuderi GR, Scott WN, et al: The efficacy of arthroscopy following total knee replacement. Arthroscopy 1997;13:166-171.
Question 19
Increasing articular conformity of the tibial polyethylene insert of a fixed-bearing total knee arthroplasty (TKA) prosthesis will have which of the following biomechanical effects?

Explanation
Increasing articular conformity increases the surface area for contact between the polyethylene and the femoral component. Advantages of this include lower peak contact stress within the polyethylene and less risk of polyethylene fatigue failure. Patellofemoral tracking is unchanged by increasing conformity unless gross component apposition is present. A potential disadvantage of increasing conformity includes some restriction in tibial rollback. Modest changes in conformity have not been shown to alter the rate of mechanical loosening. If conformity was increased to the extent of significant constraint, a potential increased risk of loosening would be expected, not a decrease. Design of modern TKAs includes a compromise in achieving enough constraint to lower polyethylene stress, without providing so much constraint as to limit kinematics and stress the fixation interfaces. D'Lima DD, Chen PC, Colwell CW Jr: Polyethylene contact stresses, articular congruity, and knee alignment. Clin Orthop 2001;392:232-238.
Question 20
A 63-year-old woman reports giving way of the knee and pain after undergoing primary total knee arthroplasty (TKA) 1 year ago. Examination reveals that the knee is stable in full extension but has gross anteroposterior instability at 90 degrees of flexion. The patient can fully extend her knee with normal quadriceps strength. Studies for infection are negative. AP and lateral radiographs are shown in Figures 12a and 12b, respectively. What is the appropriate management?


Explanation
12b The radiographs show posterior flexion instability that is the result of a flexion-extension gap imbalance and posterior cruciate ligament incompetence after a posterior cruciate ligament-retaining TKA. The femur is anteriorly displaced on the tibia, with lift-off of the femoral component from the tibial polyethylene. Revision to a larger femoral component will address the larger flexion gap relative to the extension gap, and a posterior stabilized implant will address the posterior cruciate ligament insufficiency. Pagnano and associates, reporting on a series of painful TKAs previously diagnosed as pain of unknown etiology, showed that the pain was secondary to flexion instability. Pain relief was achieved by revision to a posterior stabilized implant. Pagnano MW, Hanssen AD, Lewallen DG, et al: Flexion instability after primary posterior cruciate retaining total knee arthroplasty. Clin Orthop 1998;356:39-46. Fehring TK, Valadie AL: Knee instability after total knee arthroplasty. Clin Orthop 1994;299:157-162.
Question 21
A 72-year-old woman who underwent right total hip arthroplasty 7 years ago now reports right hip pain and limb shortening. Studies for infection are negative. AP and lateral radiographs are shown in Figures 13a and 13b. What is the most appropriate management?



Explanation
13b Current literature supports the use of reinforcement cages for the reconstruction of failed, loosened acetabular components associated with major bone loss as seen in this patient. Although results of revision using the so-called jumbo cup with screws generally have been good, the amount of bone loss and medial wall penetration shown here and the likelihood of pelvic discontinuity precludes the use of that technique. With either technique, bone grafting of remaining defects is recommended. Sporer SM, O'Rourke M, Paprosky WG: The treatment of pelvic discontinuity during acetablular revision. J Arthroplasty 2005;20:79-84.
Question 22
What is the most prevalent adverse event associated with allogeneic blood transfusion?


Explanation
Clerical error leading to acute hemolysis and even death occurs in 1:12,000 to 1:50,000 transfusions. Bacterial contamination leading to sepsis/shock occurs in 1:1 million transfusions. HIV transmission is approximately 1:500,000 transfusions and hepatitis C is 1:103,000 transfusions. Anaphylactic reactions occur in 1:150,000 transfusions. Aubuchon JP, Birkmeyer JD, Busch MP: Safety of the blood supply in the United States: Opportunities and controversies. Ann Intern Med 1997;127:904-909.
Question 23
At the time of the revision surgery shown in Figure 14, the acetabular component was found to be stable. Polyethylene exchange with a standard ultra-high molecular weight polyethylene liner and grafting was performed. The patient is at significantly increased risk for


Explanation
Maloney and associates reported a 35% increased risk of pelvic osteolysis after total hip arthroplasty with a porous-coated acetabular component without cement. All components were stable at the time of revision. Only liners were exchanged and debridement of the granuloma with or without bone graft was performed. No defects progressed and one third of the lesions were no longer visible on radiographs, regardless of bone grafting. Unfortunately, despite the technical ease of many of these types of revisions, the dislocation rate for these cases is significant. Precautions should be taken postoperatively, and patients should be educated about this risk preoperatively. Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 411-424. Boucher HR, Lynch C, Young AM, et al: Dislocation after polyethylene liner exchange in total hip arthroplasty. J Arthroplasty 2003;18:654-657.
Question 24
What is the most frequent complication of both lateral closing wedge high tibial osteotomy and medial opening wedge osteotomy?

Explanation
Scuderi and associates reported on patellar height after a high tibial osteotomy. Eighty-nine percent of the patellae, as measured by the Insall-Salvati index, and 76.3 percent, as measured by the Blackburne-Peel index, were observed to be lowered. More recently, Wright and associates reported a 64% incidence of patella baja in patients undergoing a medial opening wedge osteotomy. The incidence of intra-articular fracture during medial opening wedge osteotomy has been reported to be as high as 11% by Hernigou and associates, whereas the incidence of intra-articular fracture during lateral closing wedge high tibial osteotomy has been reported to be 10% to 20% by Matthews and associates. The incidence of peroneal nerve palsy with a lateral closing wedge high tibial osteotomy ranges from 0% to 20%, according to Marti and associates, whereas the incidence of peroneal palsy following a medial opening wedge osteotomy has been reported to be 15.7% by Flierl and associates. The exact incidence of compartment syndrome after a high tibial osteotomy is not known; however, it does not reach the level of patella baja. The incidence of deep infection after a lateral closing wedge high tibial osteotomy ranges from 0% to 4% according to Billings and associates. Scuderi GR, Windsor RE, Insall JN: Observations on patellar height after proximal tibial osteotomy. J Bone Joint Surg Am 1989;71:245-248. Wright JM, Crockett HC, Slawski DP, et al: High tibial osteotomy. J Am Acad Orthop Surg 2005;13:279-289. Hernigou P, Medevielle D, Debeyre J, et al: Proximal tibial osteotomy for osteoarthritis with varus deformity: A ten to thirteen-year follow-up study. J Bone Joint Surg Am 1987;69:332-354. Matthews LS, Goldstein SA, Malvitz TA, et al: Proximal tibial osteotomy: Factors that influence the duration of satisfactory function. Clin Orthop 1988;229:193-200. Marti CB, Gautier E, Wachtl SW, et al: Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 2004;20:366-372. Marti RK, Verhigan RA, Kerkhoffs GM, et al: Proximal tibial varus osteotomy: Indications, technique, and five to twenty-one-year results. J Bone Joint Surg Am 2001;83:164-170. Flierl S, Sabo D, Hornig K, et al: Open wedge high tibial osteotomy using fractioned drill osteotomy: A surgical modification that lowers the complication rate. Knee Surg Sports Traumatol Arthrosc 1996;4:149-153.
Question 25
Stiffness can occur following total knee arthroplasty. What is the most appropriate management for a patient who has deteriorating arc of motion after undergoing a revision knee arthroplasty 9 months ago?

Explanation
Stiffness following total knee arthroplasty can be a disabling condition. There are many reasons for loss of knee motion following total knee arthroplasty. Technical errors, such as overstuffing of the patella, malpositioning of the components, and ligamentous imbalance, are all known to result in stiffness following total knee arthroplasty. In some patients with a possible genetic predisposition, aggressive arthrofibrosis may develop and result in loss of knee motion. In any patient who has deteriorating knee motion, particularly after revision arthroplasty, deep infection should be ruled out. Although on occasion surgical intervention may be required to address knee stiffness, the outcome of revision surgery is poor if no reason for stiffness can be determined. Kim J, Nelson CL, Lotke PA: Stiffness after total knee arthroplasty: Prevalence of the complication and outcomes of revision. J Bone Joint Surg Am 2004;86:1479-1484.
Finish Exam?
You cannot change answers after submitting.
