Question 76
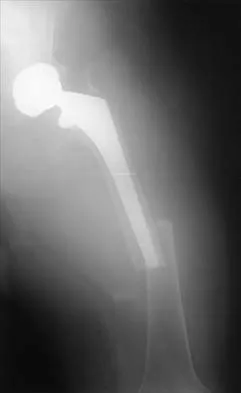
Figure 29 shows the radiograph of a 55-year-old patient who has recurrent total hip dislocation. Dislocation is most likely to occur in this patient when the hip is in which of the following positions?


Explanation
The patient has an acetabular component that is placed in excessive anteversion; this is confirmed by the shoot-through radiograph. The most common reasons for dislocation of a total hip replacement include inappropriate positioning of the components, inadequate abductor tension, or impingement. Implants placed without adequate total anteversion tend to dislocate posteriorly, and implants with excessive anteversion tend to dislocate anteriorly. Superior dislocations can occur if the acetabular component is placed in a severely vertical position with inadequate lateral coverage.
Question 77
Back pain and ipsilateral knee pain are common long-term sequelae of hip arthrodesis. To limit these problems, what position should be avoided during fusion of the hip?
Explanation
The recommended position for a hip fusion is flexion of 20 degrees to 30 degrees, slight adduction (5 degrees) or neutral, and 10 degrees of external rotation. In long-term follow-up, patients who underwent fusion in abduction had more ipsilateral knee and low back pain than patients who were positioned in adduction. Internal rotation should be avoided to prevent interference with the opposite foot during gait. External rotation facilitates the application of shoe wear. Callaghan JJ, Brand RA, Pederson DR: Hip arthrodesis: A long-term follow-up. J Bone Joint Surg Am 1985;67:1328-1335.
Question 78
Which of the following methods most reliably detects mechanical loosening of the hip?
Explanation
Mechanical loosening of the hip is best revealed by serial radiographs of the prosthetic joint. None of the other methods of evaluation is considered reliable in diagnosing mechanical loosening. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 455-492.
Question 79
A 55-year-old man underwent cementless total hip arthroplasty for advanced painful osteoarthritis of the hip 2 years ago. The follow-up radiograph shown in Figure 30 shows


Explanation
The radiograph shows a well-osseointegrated tapered stem with a metaphyseal porous coating, spot welds in the porous region, and calcar rounding. Trochanteric stress shielding and distal cortical hypertrophy are also signs of ingrown stems but are seen more frequently in association with extensively porous-coated stems exhibiting diaphyseal ingrowth. There is no evidence of lucent lines or a pedestal, signs that suggest instability. Femoral stem subsidence can be determined only by a review of sequential radiographs. Engh CA, Massin P, Suthers KE: Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin Orthop 1990;257:107-128.
Question 80
A 52-year-old woman has bicompartmental osteoarthritis following patellectomy. Treatment should consist of
Explanation
The patient has extensive degenerative changes in both the medial and lateral compartments within the knee; therefore, arthroscopic debridement or an osteotomy will not be helpful. A patellar arthroplasty will not address the medial and lateral compartments. Because the extensor mechanism provides a significant amount of anteroposterior stability, a posterior cruciate-substituting total knee arthroplasty is the treatment of choice for this patient. Martin SD, Haas SB, Insall JN: Primary total knee arthroplasty after patellectomy. J Bone Joint Surg Am 1995;77:1323-1330.
Question 81
In hybrid arthroplasty, the use of a polymethylmethacrylate (PMMA) precoated femoral component has been shown to result in
Explanation
Precoating of the femoral stem with PMMA results in increased bonding of the stem to the cement mantle. However, this has not been shown to result in superior survivorship compared with nonprecoated stems of similar design. In one series, the rate of revision of precoated stems was greater than that of nonprecoated cohorts. The wear and infection rates have not been shown to differ between precoated and nonprecoated stems. Sporer SM, Callaghan JJ, Olejniczak JP, Goetz DD, Johnston RC: The effects of surface roughness and polymethylmethacrylate precoating on the radiographic and clinical results of the Iowa hip prosthesis: A study of patients less than fifty years old. J Bone Joint Surg Am 1999;81:481-492.
Question 82
A 72-year-old woman has had progressively increasing pain in the right knee for the past 6 months. She denies any trauma and has no pain in any other joints, but she notes occasional swelling in the knee and a catching sensation. Figures 31a and 31b show the plain radiographs and Figure 31c shows the MRI scan. Treatment should consist of






Explanation
31b 31c The plain radiographs show a defect in the lateral femoral condyle and narrowing of the lateral joint space. The MRI scan shows a lesion consistent with osteonecrosis of the lateral femoral condyle. The treatment alternatives for this condition are an osteotomy or a total knee replacement, but a total knee replacement is the treatment of choice for a 72-year-old patient. Arthroscopy or an osteochondral bone graft will not address her symptoms. A valgus osteotomy will exacerbate the problem by overloading the lateral joint, which is already diseased. Lotke PA, Ecker ML: Osteonecrosis of the knee. J Bone Joint Surg Am 1988;70:470-473.
Question 83
Which of the following is considered the most appropriate indication for conversion of a hip fusion to total hip arthroplasty?
Explanation
Hip fusion provides successful long-term results (20 to 30 years). The usual mode of failure is symptomatic arthrosis of the lower back, contralateral hip, or the ipsilateral knee. Disabling low back pain is the best indication for conversion and responds well to the procedure. Degenerative changes in the other joints do not respond as well and frequently require replacement arthroplasty. Restoration of limb length is not predictable after conversion to hip replacement. Santore RF: Hip reconstruction: Nonarthroplasty, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 109-115.
Question 84
Which of the following methods is effective in correcting recurrent dislocation following total hip arthroplasty?
Explanation
Recurrent dislocation following total hip arthroplasty is a difficult problem to correct. Studies conducted by the Mayo Clinic show a failure rate of close to 40% with surgical treatment. A variety of methods have been successful, but no specific approach has been reported to be the most predictably successful. To select and institute the proper treatment option, the cause of the dislocation must be identified. Surgical options fall into several broad categories that include increasing soft-tissue tension (trochanteric advancement or longer neck lengths) or more stable articulation (larger diameter head component, bipolar prosthesis, or a constrained component). In a series of total hip arthroplasties done with a constrained cup, the loosening rates of the cup and the stem were reported to be 6% each, comparable to a reported series of complex revision total hip arthroplasties at a similar follow-up interval. Woo RY, Morrey BF: Dislocations after total hip arthroplasty. J Bone Joint Surg Am 1982;64:1295-1306.
Question 85
A 58-year-old woman who underwent a successful total hip replacement for degenerative arthritis 8 years ago reports groin pain for the past 6 months. A radiograph of the hip is shown in Figure 32. At revision, severe deficiency of the posterior column is noted. What reconstructive option would be most appropriate for the acetabulum?


Explanation
The radiograph shows medial migration of the cementless acetabular component, strongly suggesting acetabular discontinuity with a combined segmental and cavitary medial deficiency. The treatment of choice is a morcellized or structural graft, supported with a reconstructive cage bridging the pelvic discontinuity, and a cemented cup. Whiteside LA: Selection of acetabular component, in Steinberg ME, Garino JP (eds): Revision Total Hip Arthroplasty. Philadelphia, PA, Lippincott Williams and Wilkins, 1999, pp 209-220.
Question 86
A patient with a previously pain-free knee replacement now reports a sudden inability to ambulate. Radiographs of the knee are shown in Figures 33a and 33b. Management should consist of




Explanation
33b The radiographs show a patellar tendon rupture following a total knee replacement. This infrequent, but serious, complication is reported to occur in 0.17% to 1.4% of patients after total knee arthroplasty. Although the radiographs show concerning features such as incomplete tibial and femoral periprosthetic lucencies, it is most important for the surgeon to recognize extensor mechanism disruption. Insall J, Salvati E: Patella position in the normal knee joint. Radiology 1971;101:101-104. Lynch AF, Rorabeck CH, Bourne RB: Extensor mechanism complications following total knee arthroplasty. J Arthroplasty 1987;2:135-140.
Question 87
Which of the following factors will adversely affect bone ingrowth in a revision porous-coated stem?
Explanation
The optimal conditions for bony ingrowth include a pore size of 100 to 400 um, interface micromotion of 50 um or less, intimate contact between the bone and the implant, circumferential porous coating of the implant, and use of a biocompatible material. Stem designs with patch coatings have a poor record of bony ingrowth, especially in the revision setting. Failure of ingrowth in the previous stem would be the result of its own mechanical milieu and would not necessarily predict results for the new stem. Berry DJ, Harmsen WS, Ilstrup D, Lewallen DG, Cabanela ME: Survivorship of uncemented proximally porous-coated femoral components. Clin Orthop 1995;319:168-177. Cook SD, Thomas KA, Haddad RJ Jr: Histologic analysis of retrieved human porous-coated total joint components. Clin Orthop 1988;234:90-101.
Question 88
In the preoperative planning of revision acetabular reconstruction, the surgeon should identify significant posterior column deficiency by noting which of the following radiographic features?
Explanation
Proximal and medial migration of the femoral head usually indicates deficiencies of the dome or anterior column. Wear of the polyethylene may result in osteolysis and impingement, which are not indicative of any major bone deficiency. A significant osteolytic lesion in the ischium may represent a major posterior column deficiency that can create a technical challenge during the reconstruction. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 89
An 82-year-old woman reports right buttock pain after a car trip. Laboratory studies show an erythrocyte sedimentation rate of 30 mm/h and WBC of 4,600/mm3. Figure 34a shows a plain AP radiograph of the pelvis, and Figure 34b shows a delayed technetium Tc 99m bone scan. Management should consist of




Explanation
34b The radiograph shows bilateral cemented total hip arthroplasties. The acetabular components are loose bilaterally, but there has been no acute change. Therefore, it is unlikely that the acetabular loosening is contributing to the patient's pain. The bone scan is consistent with a sacral insufficiency fracture. This is best treated with bed rest and pain medication. Activity can be increased as the pain allows. Revision will not address the pain. Newhouse KE, el-Khoury GY, Buckwalter JA: Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am 1992;74:1472-1477.
Question 90
Figures 35a and 35b show the radiographs of a patient who underwent debridement of a chronically infected, fully constrained knee prosthesis and now reports pain and instability despite bracing. History reveals that the patient has had no drainage since undergoing the last debridement 6 months ago. A C-reactive protein level and aspiration are negative for infection. Treatment should now consist of




Explanation
35b The radiographs show a significant loss of the proximal anterior tibial cortex, consistent with an extensively damaged or deficient extensor mechanism. Such a deficit precludes insertion of another knee arthroplasty. Arthrodesis is the treatment of choice for this patient and is indicated for loss of the extensor mechanism and knee instability. A recent report on arthrodesis following removal of an infected prosthesis showed a union rate of 91% using a short intramedullary nail. Insertion of an antibiotic-impregnated PMMA spacer is not indicated because the rationale for using a spacer is to maintain a space for reinsertion of another prosthesis. Reconstruction of the extensor mechanism would not address the loss of the joint. Amputation is the final treatment option if the arthrodesis fails. Rand JA: Alternatives to reimplantation for salvage of the total knee arthroplasty complicated by infection. J Bone Joint Surg Am 1993;75:282-289. Lai KA, Shen WJ, Yang CY: Arthrodesis with a short Huckstep nail as a salvage procedure for failed total knee arthroplasty. J Bone Joint Surg Am 1998;80:380-388.
Question 91
Which of the following is considered an advantage of metal femoral heads compared with ceramic heads?
Explanation
Ceramic-on-ceramic bearing surfaces have superior tribological properties and show lower linear wear than metal-on-metal implants. However, because of their lower strength and vulnerability to fracture, design considerations constrain the neck-length options available to ensure optimal taper fit.
Question 92
What is the most common result if the acetabulum is rotated too far anteriorly during a periacetabular osteotomy?
Explanation
In patients with hip dysplasia who undergo a periacetabular osteotomy, the authors note that the freed acetabular segment can be overcorrected for the deformity. If it is placed too anteriorly, then hip flexion is limited. Posterior dislocation is a rare complication. The other complications should not occur as a result of this procedure. Hussell JG, Rodriguez JA, Ganz R: Technical complications of the Bernese periacetabular osteotomy. Clin Orthop 1999;363:81-92.
Question 93
Which of the following radiographic views best assesses anterior coverage of the dysplastic hip?
Explanation
Anterior coverage of the hip may be best estimated by the anterior center edge angle of Lequesne and de Seze (analogous to Wiberg's angle), which is measured on the well-defined faux profil view. Evaluation with CT scans also has been described. Klaue K, Wallin A, Ganz R: CT evaluation of coverage and congruency of the hip prior to osteotomy. Clin Orthop 1988;232:15-25.
Question 94
Figure 36a shows the current radiograph of a 65-year-old woman who slipped and fell. History reveals that prior to the fall she was actively functioning without pain. Figure 36b shows a radiograph obtained 1 year ago. Based on the fracture pattern, the failure is most likely related to



Explanation
36b The radiograph shows a fracture distal to the prosthesis in a stable, apparently well-fixed prosthetic stem. The well-fixed prosthesis-bone composite is stiff, creating a modulus mismatch between the proximal and distal femur. Therefore, the risk of fracture, particularly in osteoporotic bone, is increased at this level. Revision of the stem to a longer construct is unnecessary, and standard plate and screw fixation has been shown to yield union rates of greater than 90%. Nonsurgical treatment of fractures distal to the tip of the prosthesis results in high nonunion rates, reported to be from 25% to 42%. Johansson JE, McBroom R, Barrington TW, Hunter GA: Fracture of the ipsilateral femur in patients with total hip replacement. J Bone Joint Surg Am 1981;63:1435-1442. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 95
A 70-year-old man has worn through his metal-backed patellar component and sustained damage to the femoral component. Following removal of the components and debridement of the metal-stained synovium, the surgeon finds that the thickness of the remaining patella is 10 mm. Treatment should now include
Explanation
Revision of a failed patellar component can be difficult because of bone loss and damage to the extensor mechanism. Several authors have advised against reinsertion of a patellar component if the residual patellar thickness is 10 mm or less. Leaving an unresurfaced bony remnant in place at the time of revision or reimplantation surgery has been shown to be a reasonable option; however, the results are of a lower quality when compared with revision surgery where the patellar component can be retained or revised. The other treatment options have not been shown to be effective approaches to this problem. Rand JA: The patellofemoral joint in total knee arthroplasty. J Bone Joint Surg Am 1994;76:612-620. Pagnano MW, Scuderi GR, Insall JN: Patellar component resection in revision and reimplantation total knee arthroplasty. Clin Orthop 1998;356:134-138.
Question 96
A 65-year-old man has a painful and often audible crepitus after undergoing a total knee arthroplasty 8 months ago. His symptoms are reproduced with active extension of about 30 degrees. Examination reveals no effusion or localized tenderness, a stable knee, and a range of motion of 5 degrees to 120 degrees. Radiographs are shown in Figures 37a and 37b. Management should consist of




Explanation
37b This is a typical presentation of the patellar clunk syndrome. The syndrome usually follows implantation of a posterior stabilized prosthesis. It is thought to be the result of femoral component design and altered extensor mechanics. The condition usually resolves with arthroscopic debridement of the suprapatellar fibrous nodule. Arthrotomy or revision is seldom warranted. Beight JL, Yao B, Hozack WJ, Hearn SL, Booth RE Jr: The patellar "clunk" syndrome after posterior stabilized total knee arthroplasty. Clin Orthop 1994;299:139-142.
Question 97
What clinical parameter will most likely decrease the need for blood transfusion after total joint arthroplasty?
Explanation
Bilateral joint replacement, chronic disease, and preoperative autologous donation all increase the risk of needing blood. Young patients and a high hemoglobin level (greater than 15 g/dL) are considered clinical parameters that decrease the risk for requiring allogenic blood. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB: An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10.
Question 98
Figure 38 shows the radiograph of a 40-year-old woman who reports severe groin pain and lack of motion of the right hip. History reveals that the patient underwent a femoral osteotomy for hip dysplasia approximately 30 years ago. Treatment should include


Explanation
Although the patient is young, a total hip arthroplasty will provide pain relief and improve her range of motion. The arthritis is too advanced for the patient to benefit from an osteotomy. In addition, periacetabular osteotomy and hip arthrodesis do not improve range of motion of the hip. It has not been established that patients with severe osteoarthritis will benefit from arthroscopic debridement of the hip.
Question 99
What is the primary concern for arthrodesis of a failed infected total knee arthroplasty using internal fixation?
Explanation
Arthrodesis of the failed infected total knee arthroplasty may be accomplished by external fixation, intramedullary rod fixation, and dual plates and screws. External fixation runs the risk of pin tract infection, although after its removal, there are no metal surfaces left in place. Intramedullary rods have been used successfully in the treatment of infected total knees, although they also leave metal within the region of the infection. The dual plate technique of knee fusion is useful in patients with rheumatoid arthritis who require fusion in the absence of infection because it provides good initial stability and avoids the use of external pins. However, in the face of infection, the large surface area of the screws and plates may serve as a site for bacteria to hide within a glycocalyx and make eradication of the infection almost impossible.
Question 100
Oxidation of polyethylene after sterilization occurs most rapidly when the implant undergoes
Explanation
The use of gamma radiation to sterilize polyethylene will result in the formation of free radicals in the material that increase the susceptibility of the material to oxidation and wear. The packaging can also have an impact. If the polyethylene is packaged in air, the oxygen in the packaging can significantly oxidize the material on the shelf prior to clinical use. Gas plasma and ethylene oxide sterilization do not appear to increase oxidation of polyethylene. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486. Wright TM: Ultra-high molecular weight polyethylene, in Morrey BF (ed): Joint Replacement Arthroplasty. New York, NY, Churchill Livingstone, 1991, pp 37-46.
Finish Exam?
You cannot change answers after submitting.
