Question 51
A patient who underwent a high tibial osteotomy (HTO) is now scheduled to undergo total knee arthroplasty (TKA). When compared with a patient undergoing primary TKA without a prior HTO, the patient should be advised to expect a higher incidence of
Explanation
Conversion TKA following a previous HTO can be successful; however, it is associated with poorer clinical results when compared with other primary TKAs. There is an increased likelihood of poor range of motion that is partially affected by patella infera created from the osteotomy. Patella infera also results in difficulty with surgical exposure. There has been no reported increase in the rate of infection, fracture, or loosening.
Question 52
Figures 22a and 22b show the radiographs of a patient who reports stiffness of the hip and associated pain. Management should consist of




Explanation
22b The patient has grade IV heterotopic ossification with the limb in an abnormal nonfunctional position. Treatment should consist of excision of the bone to restore hip motion and prophylaxis to prevent recurrent formation. The best time to excise the bone is controversial, with no conclusive evidence supporting early or late excision. Pellegrini VD Jr, Koniski AA, Gastel JA, Rubin P, Evarts CM: Prevention of heterotopic ossification with irradiation after total hip arthroplasty: Radiation therapy with a single dose of eight hundred centigray administered to a limited field. J Bone Joint Surg Am 1992;74:186-200.
Question 53
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of


Explanation
Because the radiograph shows that the femoral stem is loose within the femoral canal and there is a fracture in the distal cement mantle, the stem should be revised. The Ogden-type plate and the allograft bone plates will reconstruct the femur but will not restore stability to the stem. Similarly, traction may allow the femur to heal but will not restore stability to the femoral stem within the femur. Resection arthroplasty is considered a salvage option following failure of the other procedures. Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Question 54
Compared with wear rates of metal-on-standard polyethylene bearings (75 to 250 um/y), the wear rate of metal-on-metal bearings for hip arthroplasty is approximately how many micrometers per year?
Explanation
Studies on older systems, as well as newer designs, have confirmed that metal-on-metal bearing surfaces undergo linear wear of 2 to 5 um per year. Ceramic bearing surfaces produced with recent technology perform even better, with a wear rate of 0.5 to 2.5 um per year. Clinical wear rates of metal-on-crosslinked polyethylene have not yet been determined. McKellop H, Park SH, Chiesa R, et al: In vivo wear of three types of metal on metal hip prostheses during two decades of use. Clin Orthop 1996;329:S128-S140.
Question 55
A follow-up examination of a patient 6 weeks after knee surgery reveals a range of motion from 5 degrees to 55 degrees of flexion. Which of the following statements best summarizes the role of manipulation under anesthesia for this patient?
Explanation
Esler and associates evaluated the use of manipulation under anesthesia in 47 knees. Manipulation was considered when intensive physical therapy failed to increase flexion to more than 80 degrees. The mean time from arthroplasty to manipulation was 11.3 weeks, and the mean active flexion before manipulation was 62 degrees. One year later, the mean gain was 33 degrees. Definite sustained gains in flexion were achieved even when manipulation was performed 4 or more months after arthroplasty. An additional 21 patients who met the criteria for manipulation declined the procedure, and despite continued physical therapy, they showed no significant increase in knee flexion.
Question 56
The most compelling clinical reason to convert a hip arthrodesis to a total hip arthroplasty is that the latter
Explanation
Studies show that degenerative arthritis of the spine associated with a hip arthrodesis can be decreased with conversion to a total hip arthroplasty. The pain associated with degenerative arthritis of the knee usually persists after arthrodesis take-down procedures, and often requires total knee arthroplasty. Pain in the contralateral hip is not resolved by converting the arthrodesis. Improving range of motion of the hip and correcting a limb-length discrepancy are not good indications for take-down procedures. Strathy GM, Fitzgerald RH Jr: Total hip arthroplasty in the ankylosed hip: A ten-year follow-up. J Bone Joint Surg Am 1988;70:963-966.
Question 57
A 60-year-old woman reports a painful hip arthroplasty after undergoing surgery 18 months ago. Radiographs show stable cementless implants without signs of ingrowth. Laboratory studies show an erythrocyte sedimentation rate of 50 mm/h. Management should now consist of
Explanation
Significant elevation of the erythrocyte sedimentation rate in a patient with a painful hip arthroplasty mandates a complete work-up for infection prior to considering revision surgery. Reproducibility and reliability of ultrasonography as a diagnostic test still needs clarification. Aspiration is the easiest and most cost-effective test and should be performed prior to nuclear imaging. The latter is most valuable if the results are negative, strongly predicting the absence of infection. Barrack RL, Harris WH: The value of aspiration of the hip joint before revision total hip arthroplasty. J Bone Joint Surg Am 1993;75:66-76.
Question 58
Femoral osteotomy for dysplasia of the hip will most likely result in
Explanation
Patients should expect pain relief after femoral osteotomy for hip dysplasia. Patients should not expect improved motion or abduction strength and should be counseled about a postoperative limp and unequal limb lengths. Pellicci PM, Hu S, Garvin KL, Salvati EA, Wilson PD Jr: Varus rotational femoral osteotomies in adults with hip dysplasia. Clin Orthop 1991;272:162-166.
Question 59
Figure 24 shows the radiograph of an otherwise healthy 56-year-old patient who reports hip pain after undergoing a primary cementless hip replacement 4 months ago. The next most appropriate step should consist of


Explanation
Periosteal new bone formation is a warning sign of prosthetic infection. Indomethacin may prevent heterotopic ossification if given early enough; however, it is irrelevant in this patient. A C-reactive protein and a sed rate are useful screening studies that add to the predictive value of the radiographs and may be performed routinely if sepsis is suspected. A bone scan obtained 4 months after surgery would show increased uptake in all cases. If results of a sed rate and C-reactive protein are normal, then a biopsy should be considered to rule out a neoplasm.
Question 60
Which of the following is considered a physiologic effect of anemia?
Explanation
The expected physiologic effects of anemia include an increased heart rate and increased cardiac output. The coronary blood flow requirement increases. There is a decrease in peripheral resistance and blood viscosity.
Question 61
A patient with severe rheumatoid arthritis reports progressive hip pain. Serial hip radiographs will most likely show which of the following findings?
Explanation
Radiographic findings in patients with rheumatoid arthritis include symmetric joint space narrowing, periacetabular and femoral head erosions, and diffuse periarticular osteopenia. In advanced stages, protrusio acetabuli is a common finding. Ranawat and associates have shown a rate of superior femoral head migration of 4.5 mm per year and medial (axial) migration of 2.5 mm per year. Asymmetric joint space narrowing is a classic radiographic finding of degenerative arthrosis. Sacroiliac joint ankylosis commonly occurs in ankylosing spondylitis. Hip synovitis is a pathologic diagnosis, not a radiographic finding. Lachiewicz PF: Rheumatoid arthritis of the hip. J Am Acad Orthop Surg 1997;5:332-338.
Question 62
A 70-year-old woman reports anterior knee pain after undergoing an uncomplicated total knee arthroplasty 6 months ago. Examination reveals prepatellar tenderness, with no extensor lag. The radiographs shown in Figures 25a through 25c reveal a well-fixed patellar component. Management should consist of






Explanation
25b 25c Patellar fractures that occur after a total knee arthroplasty are usually stress fractures. Integrity of the extensor mechanism precludes the need for surgical repair or internal fixation, while stability and fixation of the patellar component determine whether revision is indicated. A cylindrical cast and full weight bearing for 6 weeks is recommended for transverse fractures with an intact extensor mechanism and a stable component. A similar fracture, if vertical, may be treated with earlier motion. Rorabeck CH, Angliss RD, Lewis PL: Fractures of the femur, tibia, and patella after total knee arthroplasty: Decision making and principles of management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 449-458. Hozack WJ, Goll SR, Lotke PA, Rothman RH, Booth RE Jr: The treatment of patellar fractures after total knee arthroplasty. Clin Orthop 1988;236:123-127.
Question 63
Figure 26 shows the MRI scan of a 60-year-old man who has had groin pain for the past 2 months. The patient reports pain with ambulation, and examination reveals an antalgic gait. He denies any history of steroid or alcohol abuse. Plain radiographs are normal. Management should include
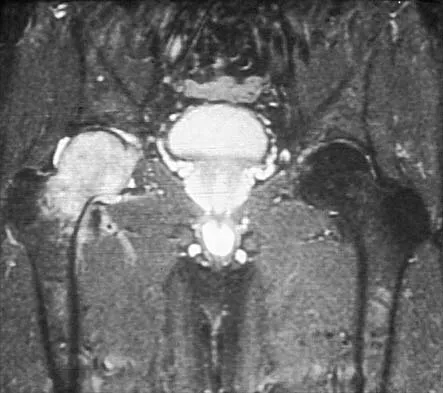

Explanation
The patient has transient osteoporosis of the hip. Transient osteoporosis is usually a self-limited condition that is most frequently seen in women in the third trimester of pregnancy and in men in the sixth decade of life. Transient osteoporosis is best treated with protected weight bearing.
Question 64
Which of the following is considered the most common complication of the impaction grafting technique for femoral revision surgery?
Explanation
Impaction grafting technique for femoral revision surgery has become increasingly popular over the past decade. This technique is designed to address cavitary deficiencies of the femur. The femoral stem is inserted with cement fixation. Its clinical efficacy has not been shown to be superior to extensively porous-coated stems. Early subsidence of the stem has been reported in more than 50% of the patients. However, loss of fixation has occurred infrequently (5%) in reported series conducted by experienced surgeons. It has not been shown to have a higher infection rate. Gie GA, Linder L, Ling RS, Simon JP, Slooff TH, Timperley AJ: Impacted cancellous allografts and cement for revision total hip arthroplasty. J Bone Joint Surg Br 1993;75:14-21.
Question 65
What is the most likely late complication associated with cementless total knee replacement?
Explanation
In cementless total knee replacement, the risk of osteolysis is 30% if both components are placed without cement and screws are used for tibial fixation. The risk is 10% when a cemented tibial component is used, and the risk is 0% when both components are cemented. Loss of motion, patellofemoral pain, heterotopic bone formation, and patellar clunk are complications that can occur after cemented or cementless components are placed.
Question 66
Figure 27 shows the radiograph of a 68-year-old woman with a history of rheumatoid arthritis who was injured in a fall. History reveals that she has been asymptomatic since undergoing a left total knee arthroplasty 9 years ago. Management should consist of


Explanation
A supracondylar fracture of the femur that occurs after total knee replacement can be treated effectively by a number of methods. For this fracture, the use of a retrograde supracondylar nail has been found to be effective in several series. The treatment of these complex injuries needs to be individualized based on the stability of the implant, the quality of the bone, and the extent of comminution of the fracture. Revision with the use of an unstemmed implant will not result in effective stabilization of the knee or the fracture.
Question 67
Design factors that enhance the long-term survival of proximally coated cementless hip implants include both initial stability and
Explanation
Proximally coated femoral components were conceived in response to the proximal stress shielding seen with extensively coated total hip stems, but initial patient studies showed problems with osteolysis, thigh pain, and stability. However, Mont and Hungerford now report that second-generation devices that have been in use more than 5 years clinically have shown very low aseptic loosening rates (1% to 3%), and patients report less thigh pain (less than 5% in most studies). These results can be attributed to improved geometry, instruments, and technique, which ensure initial implant stability. The authors suggest that proximal coating must be circumferential to seal the diaphysis from wear debris, and they note that the concept of proximal coating for cementless femoral stems seems viable as long as the twin requirements of circumferential coating and rigid initial stability are realized. Mont MA, Hungerford DS: Proximally coated ingrowth prostheses: A review. Clin Orthop 1997;344:139-149. Engh CA, Hooten JP Jr, Zettl-Schaffer KF, Ghaffarpour M, McGovern TF, Bobyn JD: Evaluation of bone ingrowth in proximally and extensively porous-coated anatomic medullary locking prostheses retrieved at autopsy. J Bone Joint Surg Am 1995;77:903-910.
Question 68
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
Proximal tibial osteotomy is appropriate for the younger and/or athletic patient who has mild to moderate medial compartment osteoarthritis. Relative contraindications include limited range of motion (eg, flexion contracture of 15 degrees), anatomic varus of greater than 10 degrees, advanced patellofemoral arthritis, and tibial subluxation. Inflammatory arthritides involve all the compartments and are a contraindication to osteotomies around the knee.
Question 69
An obese patient undergoing total knee arthroplasty is at increased risk for which of the following complications?
Explanation
The rate of wound complications is significantly increased after total knee arthroplasty in obese patients. Knee scores and the rate of aseptic loosening or patellar subluxation do not appear to be significantly altered. Winiarsky R, Barth P, Lotke P: Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am 1998;80:1770-1774. Stern SH, Insall JN: Total knee arthroplasty in obese patients. J Bone Joint Surg Am 1990;72:1400-1404.
Question 70
Figures 28a and 28b show the radiographs of a 79-year-old man who has constant knee pain. Prior to performing elective knee replacement surgery, management should include




Explanation
28b The radiographs show established Paget's disease. Bony expansion is evident, with thickened trabeculae consistent with the disordered bone remodeling process. A reduction of the serum alkaline phosphatase level to 50% of the pretreatment level may reduce pain from Paget's disease, and it is recommended prior to consideration of joint replacement. In elective cases, treatment of Paget's disease should begin at least 6 weeks prior to surgery. The other modalities are not related to the treatment of Paget's disease. Kaplan FS, Singer FS: Paget's disease of bone: Pathophysiology, diagnosis, and management. J Am Acad Orthop Surg 1995;3:336-344. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 129-184.
Question 71
What is the most common complication of using structural bulk allograft to reconstruct segmental defects of the acetabulum?
Explanation
Both autograft and allograft have been used for complex acetabular reconstructions. They have been shown to be successful in the short term. However, graft resorption with collapse and subsequent cup loosening have occurred at high rates for both types of grafts, especially if reinforcement rings or cages are not used. Jasty M, Harris WH: Salvage total hip reconstruction in patients with major acetabular bone deficiency using structural femoral head allografts. J Bone Joint Surg Br 1990;72:63-67. Paprosky WG, Magnus RE: Principles of bone grafting in revision total hip arthroplasty: Acetabular technique. Clin Orthop 1994;298:147-155.
Question 72
Radiographs of a 12-year-old boy who has knee pain show a 2-cm osteochondral lesion of the lateral aspect of the medial femoral condyle. The fragments are not detached from the femur. Initial management should consist of
Explanation
For a pediatric patient without mechanical symptoms, initial management of an osteochondral defect lesion that is not detached should consist of casting in flexion. Failure to respond to several weeks or months of nonsurgical management may warrant surgical treatment.
Question 73
Which of the following drawbacks is associated with the Ganz periacetabular osteotomy?
Explanation
Although technically challenging, the Ganz periacetabular osteotomy offers advantages over other rotational pelvic osteotomies. Posterior column integrity is maintained, as is the acetabular vascular supply. Free mobility of the fragment makes large corrections in the center edge angle possible. Because of the asymmetric cuts and the need to restore anterior coverage, there is a tendency to anterior displacement of the joint while flexing the acetabulum. The procedure is commonly performed through a Smith-Petersen incision. Trousdale RT, Ganz R: Periacetabular osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, Pa, Lippincott-Raven, 1998, pp 789-802. Ganz R, Klaue K, Vinh TS, Mast JW: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Question 74
Which of the following lesions is best suited for autologous chondrocyte implantation?
Explanation
Articular chondrocyte implantation is best performed for focal chondral defects of one area of the joint. It is not indicated for osteoarthritis. Mandelbaum BR, Brown JE, Fu F, et al: Articular cartilage lesions of the knee. Am J Sports Med 1998;26:853-861. Minas T, Nehrer S: Current concepts in the treatment of articular cartilage defects. Orthopedics 1997;20:525-538.
Question 75
The additional risk of complications in organ transplant patients receiving a total joint arthroplasty is attributed to
Explanation
Tannenbaum and associates found that patients who had a joint replacement after an organ transplantation had a rate of infection of 19% (five of 27 joint replacements in 16 patients). They retrospectively reviewed the results of 35 joint (hip or knee) replacements in 19 patients who had an organ transplant. The patients received a standard immunosuppressive induction regimen at the time of the transplantation and were maintained on a combination of prednisone, azathioprine, and cyclosporin A. All patients received antibiotics perioperatively, but antibiotic-impregnated bone cement was not used for any procedure. Six joint replacements in three patients (median patient age of 48.2 years at the time of the arthroplasty) were performed before a renal transplantation. Twenty-four joint replacements in 14 patients (average patient age of 40.9 years at the time of the arthroplasty) were performed after an organ transplantation. Two patients, with an average age of 53.8 years at the time of the arthroplasty, each had a joint replacement both before and after a liver transplantation (a total of five joint replacements). The average duration of follow-up after the first joint replacement was 8.8 years (range, 1 to 23 years). An infection developed around the implant in five patients who had undergone the joint replacement after a transplantation. The average interval from implantation of the prosthesis until detection of the infection was 3.4 years (range, 1 to 6 years). Of two patients who underwent a liver transplant, one had Pseudomonas aeruginosa infection and the other Escherichia coli infection. Of three patients who underwent a renal transplantation, one was infected with Staphylococcus epidermidis, one with Enterococcus, and one with Serratia marcescens.
Finish Exam?
You cannot change answers after submitting.
