Question 26
A 67-year-old man is requesting revision surgery because of continued pain in the knee after undergoing a total knee replacement 2 years ago. Examination reveals that the knee is not warm, the incision is well-healed, and the skin has normal coloration and hair formation. No varus or valgus instability is noted, and knee range of motion is 5 degrees to 100 degrees. Laboratory studies show an erythrocyte sedimentation rate of 15 mm/h and a WBC of 5,000/mm3. Aspiration of the knee reveals clear fluid that shows no growth on culture. Radiographs reveal an appropriately positioned cruciate-retaining cemented total knee arthroplasty that is well-fixed. What is the probability that the patient's pain will be improved with revision surgery?

Explanation
The patient has a well-fixed and aligned painful total knee replacement. The success rate of revision knee replacement for pain when no mechanical problem can be identified is approximately 40%. The critical step is to rule out the presence of infection with appropriate laboratory studies and aspiration. If no infection is detected, revision should be avoided. Rand JA: Planning for revision total knee arthroplasty, in Zuckerman JD (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 161-166.
Question 27
For patients undergoing a surgical procedure where the risk of requiring a transfusion is less than 10%, the International Committee of Effective Blood Usage suggests


Explanation
Recent studies have shown a high rate of waste of autologous blood. Therefore, the Committee does not recommend autologous blood donation for procedures that carry a transfusion risk of 10% or less. Toy P, Beattie C, Gould S, et al: Transfusion alert: Use of autologous blood. National Heart, Lung, and Blood Institute Expert Panel on the use of autologous blood. Transfusion 1992;35:703-711.
Question 28
Figure 12 shows the radiograph of a 55-year-old man who has severe, painful osteoarthritis of the left hip and is scheduled to undergo a left total hip arthroplasty. History reveals that he underwent a right total hip arthroplasty 5 years ago that remains pain-free. Based on the preoperative radiograph, the patient is at greatest risk for what complication?






Explanation
The patient is at increased risk for limb-length discrepancy because the radiograph shows that the left leg is already longer than the right leg. To restore the proper biomechanics of the left hip, the left leg may have to be lengthened, further increasing the limb-length discrepancy. Intraoperative fracture, deep vein thrombosis, sciatic nerve palsy, and thigh pain are commonly associated with total hip arthroplasty, but the patient is not at increased risk for these complications.
Question 29
Figures 13a and 13b show the preoperative radiographs of a 60-year-old woman who is scheduled to undergo total knee arthroplasty under epidural anesthesia. Postoperatively she reports a burning sensation on the dorsum of her foot despite the administration of IV analgesics through a patient-controlled analgesia (PCA) pump. Management should now include






Explanation
13b The patient has a significant flexion contracture and valgus deformity; therefore, the risk of peroneal nerve injury is increased. Idusuyi and Morrey noted that epidural anesthesia also increases the risk of peroneal nerve injury. The initial symptom can be a burning sensation on the foot, followed by pain and then motor weakness. Initial management should consist of release of the dressings and knee flexion. Idusuyi OB, Morrey BF: Peroneal nerve palsy after total knee arthroplasty: Assessment of predisposing and prognostic factors. J Bone Joint Surg Am 1996;78:177-184.
Question 30
Figures 14a and 14b show the plain radiographs of an 85-year-old woman who has had severe pain in the right knee for the past 4 months. Management should consist of






Explanation
14b The patient has osteonecrosis of the lateral femoral condyle with collapse of the articular surface. Because there is already collapse of the articular surface, a total knee arthroplasty is the treatment of choice. The results of total knee arthroplasty in these patients are usually excellent. However, knee replacement is only a resurfacing procedure, and some patients with global osteonecrosis of the distal femur may have residual pain after knee replacement. High tibial osteotomy may be indicated in younger patients who have a varus deformity and localized osteonecrosis. Arthroscopic surgery would provide minimal relief for this patient because there is already collapse of the articular surface. A hinged knee brace will not adequately unload the joint. An osteochondral allograft should be considered only for younger patients with localized osteonecrosis. Bergman NR, Rand JA: Total knee arthroplasty in osteonecrosis. Clin Orthop 1991;273:77-82.
Question 31
The failure of the acetabular component shown in Figure 15 is most likely the result of the use of a 32-mm head and








Explanation
Astion and associates analyzed 23 acetabular components, out of a total of 173 implanted, that had failed because of either migration or severe osteolysis. The radiographic appearance of osteolysis was positively associated with the duration that the implant had been in situ. The prevalence of osteolysis was also significantly greater in acetabular components with an outer diameter of 55 mm or less (a polyethylene thickness of 8.5 mm or less). Thirteen of the 23 components were revised at a mean of 70 months after the index operation. Examination of the retrieved acetabular components revealed extensive polyethylene damage on the articular and back surfaces of the liners. Cracks in the polyethylene rim of the liner and deformation of the antirotation notch in the polyethylene rim were common findings. The density of the polyethylene was greater than expected, and more particles than anticipated had not fused with the surrounding polyethylene. Factors related to both the design and the material contributed to the failure of these porous-coated anatomic acetabular components.
Question 32
The use of elevated rim acetabular liners and long femoral necks may result in


Explanation
Elevated rim acetabular liners may improve the anteversion of the acetabular component that, in turn, might improve the stability of the hip replacement through a range of motion. Long femoral necks with skirts will increase the abductor tension and may be necessary to equalize limb lengths. However, either of these measures may increase the likelihood of impingement of the femoral component on the acetabular rim and may lead to dislocation. The restricted range of motion secondary to impingement has been shown to lead to further polyethylene wear that may result in osteolysis. Cobb TK, Morrey BF, Ilstrup DM: The elevated rim acetabular liner in total hip arthroplasty: Relationship to postoperative dislocation. J Bone Joint Surg Am 1996;78:80-86.
Question 33
Cementation technique has a definite influence on the long-term survival of cemented femoral components. Both clinical and autopsy studies support the use of a cement mantle with a thickness of how many millimeters?




Explanation
Long-term radiographic analysis of cemented total hips supports the creation of a 2- to 5-mm cement mantle in the proximal medial region. Autopsy studies have shown that the incidence of crack formation was greatest when the cement mantle was less than 2 mm. Ebramzadeh E, Sarmiento A, McKellop HA, Llinas A, Gogan W: The cement mantle in total hip arthroplasty: Analysis of long-term radiographic results. J Bone Joint Surg Am 1994;76:77-87. Jasty M, Maloney WJ, Bragdon CR, O'Connor DO, Haire T, Harris WH: The initiation of failure in cemented femoral components of hip arthroplasty. J Bone Joint Surg Br 1991;73:551-558.
Question 34
A 73-year-old man is scheduled to have mature heterotopic bone resected from around his left total hip arthroplasty. The optimal management for prophylaxis against the return of heterotopic bone postoperatively is radiation therapy that consists of



Explanation
Patients require prophylaxis for heterotopic bone after resection to prevent recurrence. The optimal management has been found to be a dose of 700 cGy in one dose delivered either pre- or postoperatively. A dose of 2,000 to 3,000 cGy is considered excessive. Radiation therapy consisting of 1,000 cGy in five doses is an acceptable prophylaxis; however, it will require an extended hospital stay of 3 to 4 days and is more problematic for the patient who must be transported for radiation therapy for 5 days. A dose of 400 cGy is not as effective in prophylaxis for heterotopic bone formation. Healy WL, Lo TC, DeSimone AA, Rask B, Pfeifer BA: Single-dose irradiation for the prevention of heterotopic ossification after total hip arthroplasty: A comparison of doses of five hundred and fifty and seven hundred centigray. J Bone Joint Surg Am 1995;77:590-595. Pelligrini VD Jr, Gregoritch SJ: Preoperative irradiation for the prevention of heterotopic ossification following total hip arthroplasty. J Bone Joint Surg Am 1996;78:870-881.
Question 35
Which of the following is considered a potential advantage in prophylaxis for the prevention of deep venous thrombosis associated with the use of low-molecular weight heparin (LMWH) as compared with fixed-dose unfractionated heparin?




Explanation
One possible reason for improved efficacy of LMWHs is the relative improved bioavailability compared with that of unfractionated heparin. This is, in part, the result of a more predictable dose response and a longer half-life. There is no alteration of venous flow, and the rate of bleeding complications is the same or slightly higher than that of other prophylactic agents. Colwell CW Jr, Spiro TE, Trowbridge AA: Use of enoxaparin, a low-molecular weight heparin, and unfractionated heparin for the prevention of deep venous thrombosis after elective hip replacement: A clinical trial comparing efficacy and safety. J Bone Joint Surg Am 1994;76:3-14. Bara L, Billaud E, Kher A, Samama M: Increased anti-Xa bioavailability for a low-molecular weight heparin (PK 10169) compared with unfractionated heparin. Semin Thromb and Hemost 1985;11:316-317.
Question 36
Figure 16 shows the radiograph of a 75-year-old man who has progressive groin pain and a limp following total hip replacement. At revision surgery, the anterior and posterior columns of the acetabulum are noted to be intact. The optimal surgical technique for acetabular component reconstruction is a





Explanation
Large cementless acetabular components have been shown to perform well in revision acetabular reconstruction. The use of such components is predicated on the presence of adequate anterior and posterior column bone. If a good press-fit can be achieved between the anterior and posterior columns, typically, the remaining defects can be filled with morcellized bone graft. Protrusio cages are typically used in situations where it is not possible to obtain adequate fixation with a large acetabular component. The use of a high hip center with small sockets is more typical of primary arthroplasty in patients with developmental dysplasia of the hip. Bulk acetabular allografts for large segmental defects might be necessary in certain situations, although the use of bulk allografts has resulted in a high failure rate after 5 years. Early results of the use of protrusio cages and bone grafting for large segmental defects have been favorable. Petrera P, Rubash HE: Revision total hip arthroplasty: The acetabular component. J Am Acad Orthop Surg 1995;3:15-21.
Question 37
Which of the following is a recognized consequence of hip fusion?




Explanation
Low back pain is an expected long-term complication of fusion; ipsilateral knee laxity is frequently encountered, as is degeneration of the contralateral hip. Hip fusion is equally valuable for both men and women, with both genders reporting satisfactory sexual function. Female patients often deliver by elective Cesarean section, although vaginal deliveries are reported. Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Question 38
Treatment of a cruciate-retaining total knee that is unstable in flexion is best accomplished by


Explanation
Pagnano and associates revised 25 painful primary posterior cruciate-retaining total knee arthroplasties for flexion instability. The patients shared typical clinical presentations that included a sense of instability without frank giving way, recurrent knee joint effusion, soft-tissue tenderness involving the pes anserine tendons and the retinacular tissue, posterior instability of 2+ or 3+ with a posterior drawer or a posterior sag sign at 90 degrees of flexion, and above-average motion of the total knee arthroplasty. Twenty-two of the knee replacements were revised to posterior stabilized implants, and three underwent tibial polyethylene liner exchange only. Nineteen of the 22 knee replacements revised to a posterior stabilized implant showed marked improvement after the revision surgery. Only one of the three knee replacements that underwent tibial polyethylene exchange was improved. Flexion instability can be a cause of persistent pain and functional impairment after posterior cruciate-retaining total knee arthroplasty. Revision surgery that focuses on balancing the flexion and extension spaces, in conjunction with a posterior stabilized knee implant, seems to be a reliable treatment for symptomatic flexion instability after posterior cruciate-retaining total knee arthroplasty.
Question 39
The stiffness of a 16-mm femoral stem is mostly influenced by the
Explanation
The stiffness is most influenced by the geometry, in particular the diameter of the stem. The bending rigidity increases to the fourth power of the radius. The elastic modulus of the material increases as a direct linear relationship. The surface coating does not affect the bending rigidity greatly unless it increases the diameter significantly.
Question 40
Figures 17a and 17b show the AP and lateral radiographs of a 75-year-old woman who reports giving way and shifting of the knee, particularly when she is descending stairs or ambulating on level surfaces. History reveals a total knee replacement 5 years ago. Treatment should consist of




Explanation
17b The radiographs show well-fixed components of a posterior cruciate-retaining total knee replacement. The relative position of the femoral component is anteriorly subluxated relative to the tibial component. The AP radiograph shows that the articular space is markedly asymmetric, indicating either failure or fracture of the polyethylene or subluxation of the femur relative to the tibia. The patient's symptoms suggest a failure of the posterior cruciate ligament that is consistent with the radiographic findings; therefore, the treatment of choice is revision to a posterior cruciate-substituting implant.
Question 41
Factors contributing to an increased risk of hip fracture include reduced bone mineral density of the femoral neck, cognitive status of the individual, and
Explanation
The etiology of hip fractures in the elderly is multifactorial, and intervention and prevention can occur at multiple points. Events leading to hip fracture from a fall include fall initiation (during which the individual's neuromuscular status, cognitive status, and vision come into play along with environmental hazards); fall descent (fall direction toward the side being the most influential, energy content of the fall, and fall height, along with muscle activity of the muscles of the thigh); impact (impact location, soft-tissue attenuation such as from trochanteric padding or from overlying fat, impact surface, and muscle activity); and the structural capacity of the femur (bone mineral density, bone geometry, and bone architecture). Hayes and Myers noted that striking the ground in a stiff state with the trunk muscles contracted actually increased the peak impact force, whereas falling in a relaxed state actually reduced peak impact force. Flexion of the trunk at impact had no bearing on the impact force. Direction of the fall was important; falls to the side, not forward, were associated with an increased risk of hip fracture. Increased muscle activity about the hip is thought to be associated with spontaneous fractures of the hip and may actually account for up to 25% of hip fractures; however, it is not related to fractures resulting from a fall.
Question 42
A healthy 70-year-old man has a swollen knee after undergoing a knee replacement 10 years ago. Aspiration of the knee reveals cloudy, viscous synovial fluid. Laboratory studies show an erythrocyte sedimentation rate of 10 mm/h and a C-reactive protein level of less than 0.5. What is the most likely diagnosis?
Explanation
Polyethylene wear debris can result in significant synovitis and subsequent cloudy appearing synovial fluid. Typically, laboratory studies show a WBC of less than 30,000/mm3 no left shift. Cytologic examination can reveal intra-articular polyethylene particles. Infected total knee arthroplasty is extremely uncommon in a healthy, immune-competent patient who has a normal preoperative erythrocyte sedimentation rate and C-reactive protein level.
Question 43
The insurance carrier of a patient who underwent total knee arthroplasty 4 days ago is now demanding that the patient be discharged from the hospital. However, examination reveals that the patient has a range of motion of only 10 degrees to 55 degrees, and the patient is concerned whether she will ever move her knee normally. The insurance company representative should be advised that
Explanation
Examination findings that show flexion of only 55 degrees at discharge should alert the surgeon that the patient will require close scrutiny and follow-up. Mauerhan and associates examined the records of 745 patients who had a primary total knee arthroplasty from 1993 to 1996. At their institution, development and implementation of clinical pathways resulted in a significant decrease in the average length of stay, beginning in 1993 with 6.4 days +/- 1.8 days and progressively decreasing to 4.4 days +/- 1.0 days in 1996. The rate of manipulation (patients manipulated at 6 weeks/total number of patients receiving total knee arthroplasty) was 6.0% in 1993, 11.3% in 1994, 13.5% in 1995, and 12.0% in 1996. In the period of 1993 to 1996, patients requiring manipulation consistently had a lower range of motion of 69.0 degrees +/- 10 degrees at the time of discharge compared with patients not requiring manipulation who had a range of motion of 80.7 degrees +/- 10.6 degrees. In this era of outpatient services, however, another solution would be to arrange for outpatient physical therapy on a more frequent basis and to see the patient more frequently in the office until an acceptable range of motion is established.
Question 44
Figure 18 shows the radiograph of a patient with a total hip arthroplasty dislocation. During revision, increasing the diameter of the femoral head while maintaining the ratio of head-to-neck diameter constant has the effect of


Explanation
Although there is strong clinical and laboratory evidence that suggests smaller head size is linked with lower rates of polyethylene wear, moving to the use of 22-mm heads from larger sizes would tend to increase the dislocation rate. The key premise to this argument is that the absolute size of the femoral neck remains unchanged. While neck diameters were appropriate for the early monoblock femoral components, the use of modular femoral stems allows the surgeon to place 22-mm heads onto the same neck and trunion as used by larger heads. This has the effect of lessening the head-to-neck diameter ratio, which then accentuates the rate of impingement and dislocation. Reducing the neck diameter in proportion to the head diameter would eliminate the range-of-motion penalty accompanying head size reduction. Scifert and associates used a three-dimensional finite element model to study various combinations of femoral head size and neck ratios. They found that increasing the diameter of the femoral head while maintaining a constant head-to-neck diameter had the effect of significantly increasing the resisting moment necessary to induce a dislocation. The higher the head-to-neck ratio, the greater the range of motion until impingement and the greater the range of motion to dislocation.
Question 45
During primary total knee arthroplasty with trial implants in place, the surgeon notes technically satisfactory patellar resurfacing and restoration of a physiologic mechanical axis but excessively lateral patellar tracking. Treatment should now include
Explanation
The most common causes of patellar instability after total knee arthroplasty are valgus malalignment, internal rotation of the femoral or tibial component, medialization of the femoral component, errors in patellar preparation and resurfacing, and failure to perform a lateral release. These factors should be addressed before considering capsular closure. Distal extensor mechanism realignment should be avoided because of the complication rate. The proximal extensor mechanism would not adequately compensate for implant malrotation. Barnes CL, Scott RD: Patellofemoral complications of total knee replacement, in Heckman JD (ed): Instructional Course Lectures 42. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993, pp 309-314.
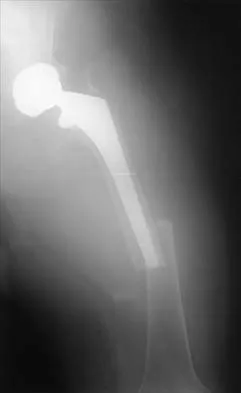
Question 46
Figure 19 shows the current radiograph of a 48-year-old man who reports hip pain and marked difficulty walking after undergoing revision of a failed total hip replacement 2 years ago. What is the mechanism of failure?


Explanation
Fatigue from repetitive loading of the stem with the distal aspect well-fixed resulted in stem failure. If the stem had loosened, it would not have broken. Crevice corrosion occurs at a taper interface; galvanic corrosion occurs at the junction of two metals of differing electrochemical potentials, not along a uniform portion of the implant. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 449-486.
Question 47
Torsional moments about the longitudinal axis of a total hip arthroplasty show what change during stair climbing compared with walking?
Explanation
The magnitudes of out-of-plane loads on a total hip replacement during activities of daily living can be substantial. Bergmann and associates studied these forces about two instrumented hip prostheses. They noted that the torsional moment about the hip during stair climbing is twice as high as during slow walking and that similar moments are generated during slow jogging. Higher loads were noted when the patients stumbled without falling. They also noted that the torsional moments observed in vivo were close to or even exceeded the experimentally determined limits of the torsional strength of implant fixations. Hurwitz DE, Andriacchi TP: Biomechanics of the hip, in Callaghan JJ, Rosenberg AG, Rubash HE (eds): The Adult Hip. Philadelphia, PA, Lippincott Raven, 1998, pp 75-85.
Question 48
When converting the knee shown in Figure 20 to a total knee arthroplasty, satisfactory outcome can be expected in what percent of patients?


Explanation
Naranja and associates reviewed 37 knees (35 patients, with 28 women and 7 men) without any motion that were converted to total knee arthroplasties. After an average follow-up of 90 months, the patients lacked an average of 7 degrees of extension and had 62 degrees of flexion. Results showed a short-term complication rate of 24% (stiffness requiring manipulation, delayed wound healing, and recurrent hemarthrosis), a major complication rate of 35% (patellar tendon or tibial tubercle avulsion, persistent pain requiring arthrodesis, loosening, and joint stiffness requiring arthrotomy for excision of scar tissue), and an infection rate of 14%. The total complication rate was 57%. A satisfactory outcome (no pain and an unlimited ambulation distance) was obtained in only 10 patients (29%). There was no relationship between results and the angle at which the knee was ankylosed preoperatively. This study revealed that although success in reconstructing a previously ankylosed or arthrodesed knee is possible, the lack of consistent adequate motion and the complication rate may suggest that the surgeon reconsider the risks and benefits of this difficult procedure.
Question 49
The specificity of intraoperative frozen sections obtained for the evaluation of infected total hip arthroplasty may be improved by
Explanation
Lonner and associates conducted a prospective study to determine the reliability of analysis of intraoperative frozen sections for the identification of infection during 175 consecutive revision total joint arthroplasties (142 hips and 33 knees). The mean interval between the primary arthroplasty and the revision arthroplasty was 7.3 years (range, 3 months to 23 years). Of the 175 patients, 23 had at least 5 polymorphonuclear leukocytes per high-powered field on analysis of the frozen sections and were considered to have an infection. Of these 23 patients, five had 5 to 9 polymorphonuclear leukocytes per high-powered field and 18 had at least 10 polymorphonuclear leukocytes per high-powered field. The frozen sections for the remaining 152 patients were considered negative. On the basis of cultures of specimens obtained at the time of the revision surgery, 19 of the 175 patients were considered to have an infection. Of the 152 patients who had negative frozen sections, three were considered to have an infection on the basis of the results of the final cultures. Of the 23 patients who had positive frozen sections, 16 were considered to have an infection on the basis of the results of the final cultures; all 16 had frozen sections that showed at least 10 polymorphonuclear leukocytes per high-powered field. The sensitivity and specificity of the frozen sections were similar regardless of whether an index of 5 or 10 polymorphonuclear leukocytes per high-powered field was used. Analysis of the frozen sections had a sensitivity of 84% for both indices, whereas the specificity was 96% when the index was 5 polymorphonuclear leukocytes and 99% when it was 10 polymorphonuclear leukocytes. However, the positive predictive value of the frozen sections increased significantly (P < 0.05), from 70% to 89%, when the index increased from 5 to 10 polymorphonuclear leukocytes per high-powered field. The negative predictive value of the frozen sections was 98% for both indices. At least 10 polymorphonuclear leukocytes per high-powered field was predictive of infection, while 5 to 9 polymorphonuclear leukocytes per high-powered field was not necessarily consistent with infection. Less than 5 polymorphonuclear leukocytes per high-powered field reliably indicated the absence of infection. Feldman DS, Lonner JH, Desai P, Zuckerman JD: The role of intraoperative frozen sections in revision total joint arthroplasty. J Bone Joint Surg Am 1995;77:1807-1813. Lonner JH, Desai P, Dicesare PE, Steiner G, Zuckerman JD: The reliability of analysis of intraoperative frozen sections for identifying active infection during revision hip or knee arthroplasty. J Bone Joint Surg Am 1996;78:1553-1558. Spangehl MJ, Younger AS, Masri BA, Duncan CP: Diagnosis of infection following total hip arthroplasty, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 285-295.
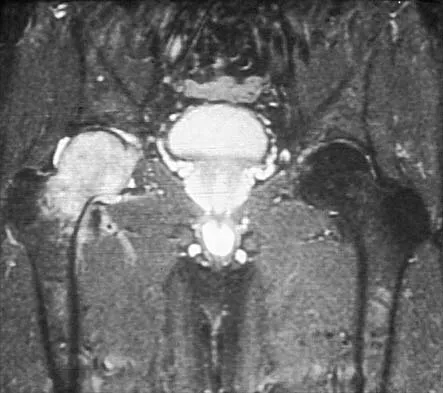
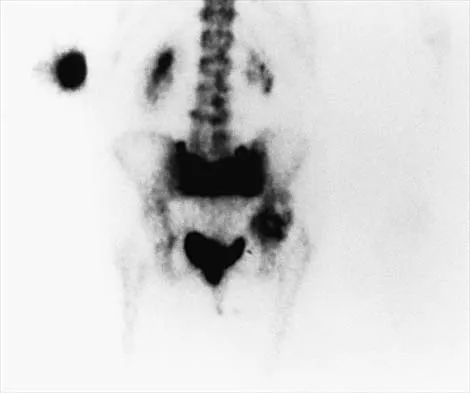
Question 50
Figures 21a through 21c show the radiographs of a 70-year-old woman who has persistent pain with activity after undergoing hip revision 6 months ago. Treatment should now consist of






Explanation
21b 21c The radiographs show disruption of the posterior column of the acetabulum with radiolucencies about the component. Because the patient requires a stable construct to allow the bone to heal, the treatment of choice is an antiprotrusio cage and a graft. Gill TJ, Sledge JB, Muller ME: The Burch-Schneider anti-protrusio cage in revision total hip arthroplasty: Indications, principles, and long-term results. J Bone Joint Surg Br 1998;80:946-953.
Finish Exam?
You cannot change answers after submitting.
