Question 1
The main advantage of surgical repair of an acute Achilles tendon rupture, when compared with nonsurgical management, is reduced





Explanation
The literature supports similar clinical outcomes after surgical and nonsurgical methods. The chief difference lies in the complications between the groups. Surgical patients experience more wound problems but a significantly lower rerupture rate. Although suturing the tendon allows earlier mobility, the tendon healing time is unchanged. Nonsurgical methods are less expensive to provide. Maffulli N: Rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036. Cetti R, Christensen SE, Ejsted R, Jensen NM, Jorgensen U: Operative versus nonoperative treatment of Achilles tendon rupture: A prospective randomized study and review of the literature. Am J Sports Med 1993;21:791-799.
Question 2
A 25-year-old farm worker sustained a grade III open fracture of the midshaft of the left tibia after falling from a ladder. Which of the following antibiotic regimens is best for this patient?


Explanation
Patients who sustain grade III open fractures that are related to a farm environment require ampicillin or penicillin for Clostridium coverage. Holton PD, Mader J, Nelson CL, Osmon DR, Patzakis MJ: Antibiotics for the practicing orthopaedic surgeon. Instr Course Lect 2000;341:36-42.
Question 3
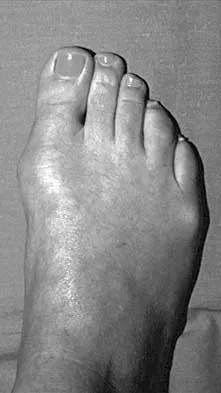
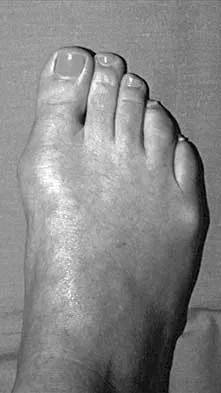
A 60-year-old man reports that he has had shoe pressure pain over his right great toe for several years but has minimal discomfort when barefoot or in sandals. A clinical photograph and radiographs are shown in Figures 1a through 1c. Management should consist of




Explanation
1b 1c Some patients have minimal symptoms associated with hallux rigidus despite significant radiographic evidence of osteoarthritis. This patient's symptoms are primarily related to shoe pressure from the exostosis and can be managed with extra-depth shoe wear. Smith RW, Katchis SD, Ayson LC: Outcomes in hallux rigidus patients treated nonoperatively: A long-term follow-up study. Foot Ankle Int 2000;21:906-913.
Question 4
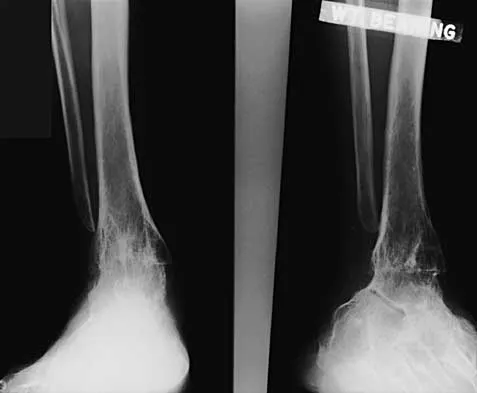
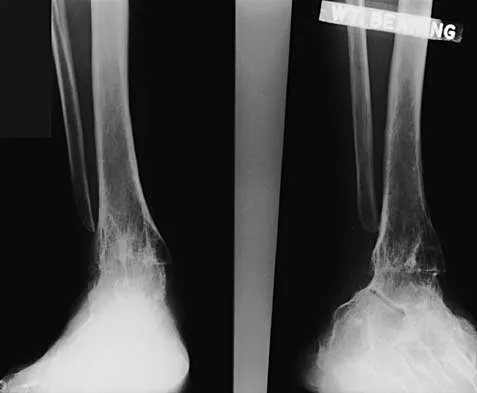
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?




Explanation
2b An increased density of the talar body compared to the distal tibia following fracture of the talar neck is highly suggestive of vascular compromise of the talar body. Subchondral osteopenia of the talus at 6 to 8 weeks (Hawkins sign) is a favorable sign but does not eliminate the possibility of osteonecrosis. Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Question 5
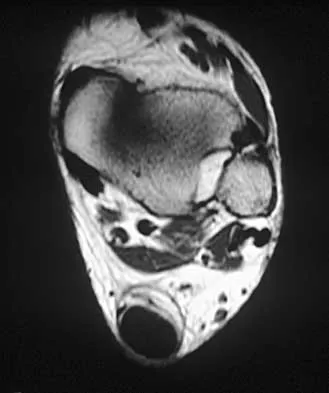
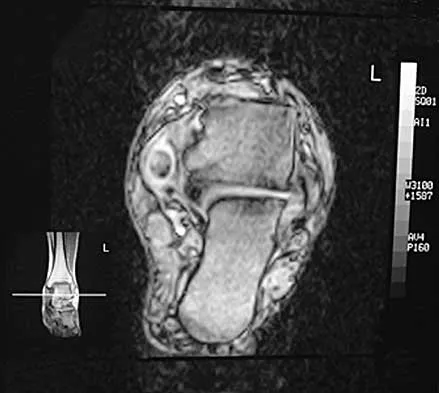
A 28-year-old woman who is training for the New York Marathon reports pain in the posteromedial aspect of her right ankle. Examination reveals tenderness just posterior to the medial malleolus. Radiographs are normal. An MRI scan is shown in Figure 3. What is the most likely diagnosis?



Explanation
Any of the above conditions is credible with a limited history. The MRI scan unequivocally shows the stress fracture in the distal tibia. Most tibial stress fractures can be managed with rest and immobilization. Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Question 6
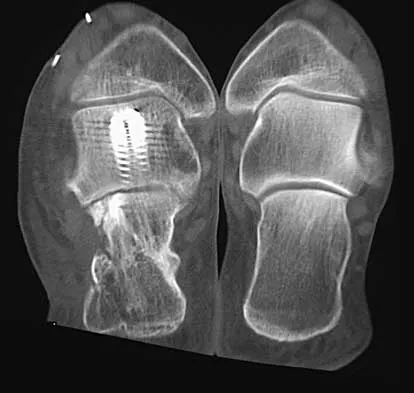
A 50-year-old laborer sustained an isolated closed injury to his heel after falling 11 feet off a wall. A radiograph and a CT scan are shown in Figures 4a and 4b. To minimize the patient's temporary disability and allow him to return to work most rapidly, management should consist of



Explanation
4b With a severe articular injury to the calcaneus, the ability to achieve satisfactory results with open reduction and internal fixation diminishes. An arthrodesis is often needed to allow a person who works as a laborer to return to work. Recent literature suggests that this can be successfully performed primarily, improving the odds of an earlier return to the labor force at 1 year. Huefner T, Thermann H, Geerling J, Pape HC, Pohlemann T: Primary subtalar arthrodesis of calcaneal fractures. Foot Ankle Int 2001;22:9-14. Coughlin MJ: Calcaneal fractures in the industrial patient. Foot Ankle Int 2000;21:896-905.
Question 7
Figures 5a and 5b show the clinical photograph and radiograph of a patient who has difficulty wearing shoes and has persistent symptoms medially and laterally at the first and fifth metatarsophalangeal joints. Because shoe modifications have failed to provide relief, management should now consist of



Explanation
5b A significant bunionette deformity that fails to respond to conservative management is best addressed surgically, in this case with the bunion deformity. The radiograph reveals a prominent lateral condyle at the fifth metatarsal head without a significant increase in the intermetatarsal angle. Simple exostectomy is preferred with less risk of complications. Complete excision would risk transfer lesions to the medial metatarsals. Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 415-435.
Question 8
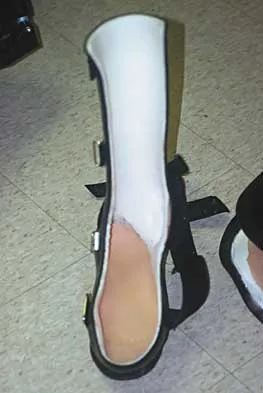
What is the most appropriate orthotic management for the lesion shown in Figure 6?


Explanation
The figure shows an intractable plantar keratosis (IPK). The keratoma usually forms beneath a bony prominence. This can occur under the sesamoids, most commonly the tibial sesamoid, or under the fibular condyle of a prominent metatarsal head. The initial treatment of an IPK consists of paring down the callused lesion and placing a metatarsal pad proximal to the lesion to provide posting to unload the bony prominence.
Question 9
Examination of a 45-year-old man with Charcot-Marie-Tooth disease reveals a cavus foot, a tight Achilles tendon, and forefoot callus formation. Radiographs reveal advanced degenerative changes in the hindfoot. Shoe wear modifications have failed to provide relief. Treatment should now consist of

Explanation
The patient has the typical end stage residuals from long-standing Charcot-Marie-Tooth disease. Initial management consisting of shoe wear modifications and orthotic devices is preferred, but these are not successful when the disease process has progressed. Surgical correction with calcaneal osteotomy or Achilles tendon lengthening and Steindler stripping is not indicated in the presence of significant hindfoot arthritis. Because this patient has findings consistent with hindfoot arthritis, a triple arthrodesis with correction of the cavus deformity is the preferred treatment. Roper BA, Tibrewal SB: Soft tissue surgery in Charcot-Marie-Tooth disease. J Bone Joint Surg Br 1989;71:17-20.
Question 10
A Canale view best visualizes which of the following structures?


Explanation
The Canale view, which visualizes the talar neck, is taken with the ankle in maximum plantar flexion and the foot pronated 15 degrees. The radiograph is directed at a 75 degree angle from the horizontal plane in the anteroposterior plane. The Broden view, which is different from the Canale view, is best for imaging the posterior facet of the subtalar joint. Canale ST, Kelly FB Jr: Fractures of the neck of the talus: Long-term evaluation of seventy-one cases. J Bone Joint Surg Am 1978;60:143-156.
Question 11
A 45-year-old woman with a long-standing history of diabetes mellitus has a large draining plantar ulcer of the right foot. Examination reveals some local cellulitis and erythema surrounding the ulcer. A clinical photograph is shown in Figure 7. Based on these findings, what is the most appropriate antibiotic?


Explanation
Combination drugs with activity against both aerobic and anaerobic organisms have been determined to be the best approach. The first-generation cephalosporins do not provide adequate coverage for gram-negative and anaerobic organisms. Gentamicin alone would not provide adequate activity against anaerobes, and there is the risk of renal and auditory toxicity. Pinzur MS, Slovenkai MD, Trepman E: Guidelines for diabetic foot care. Foot Ankle Int 1999;20:695-702.
Question 12
A 35-year-old man reports forefoot pain with weight-bearing activities. He reports that he has had high arches since adolescence but has never been treated. Examination reveals stiff cavus feet. He has no plantar callus or hammer toe formation. The ankle can be passively dorsiflexed 10 degrees. Initial management should consist of

Explanation
The patient has cavus feet with minimal clinical symptoms. At this stage, conservative management is preferred. The use of a molded orthosis will allow better support of the midfoot and provide cushioning of the forefoot. This will most likely result in long-term relief. In more advanced cases with forefoot callus formation, Achilles tendon lengthening or calcaneal osteotomy and Steindler stripping are effective in correcting the cavus deformity. In the presence of arthritic changes in the hindfoot, a triple arthrodesis with corrective bone resection may be necessary. Janisse DJ: Indications and prescriptions for orthoses in sports. Orthop Clin North Am 1994;25:95-107.
Question 13
A 70-year-old woman had poliomyelitis as a young child, and the residual weakness she has as an adult principally involves the lower extremities. She now notes progressive weakness in both legs and she tires easily. What is the best course of action?

Explanation
The most likely diagnosis is postpolio syndrome, which is characterized by increasing weakness in both the paretic and previously normal muscles. Fatigability, joint pain, muscle atrophy, respiratory insufficiency, dysphagia, and sleep apnea are also seen. Gentle exercise and modification in lifestyle demands are generally recommended. Vigorous rehabilitation is likely to be detrimental in this condition. Further diagnostic work-up is not indicated at this time. Dalakas MC, Elder G, Hallett M, et al: A long-term follow-up study of patients with post-poliomyelitis neuromuscular symptoms. N Eng J Med 1986;314:959-963.
Question 14
A patient with Charcot-Marie-Tooth disease has a progressively rigid cavovarus foot deformity. The patient states that the pain is restricted to the forefoot, where rigid claw toe deformities have developed. Which of the following structures is primarily involved in creation of a claw toe deformity?

Explanation
Diseases such as Charcot-Marie-Tooth result in spasticity to the extrinsic flexor tendons. This results in hyperflexion of the proximal and distal interphalangeal joints of the involved toe, as well as hyperextension at the metatarsophalangeal joint. The tendon often becomes contracted with progressive equinus of the ankle. Correction of ankle equinus exaggerates the claw toe deformity. The interosseous tendon plays no role in the etiology of a claw toe but may become contracted in later stages of the disease. Laxity of the volar plate may precipitate a claw toe deformity in a nonspastic situation. In patients with a head injury, claw toe deformities are generally the result of overactivity of the extensor tendons. Keenan MA, Gorai AP, Smith CW, Garland DE: Intrinsic toe flexion deformity following correction of spastic equinovarus deformity in adults. Foot Ankle 1987;7:333-337. Pichney GA, Derner R, Lauf E: Digital "V" arthrodesis. J Foot Ankle Surg 1993;32:473-479.
Question 15
A 45-year-old man who underwent an ankle arthrodesis reports that for the first 6 years he had significant pain relief after the fusion healed. However, he now has increasing pain in the sinus tarsi. AP and lateral radiographs are shown in Figures 8a and 8b. What is the most likely cause of the patient's symptoms?



Explanation
8b The patient has a solid ankle fusion radiographically. With a tibiotalar arthrodesis, the adjacent joints (subtalar and transverse tarsal) take additional stress. Over time, progressive degenerative arthritis will occur in these adjacent joints, often necessitating further surgery. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631.
Question 16
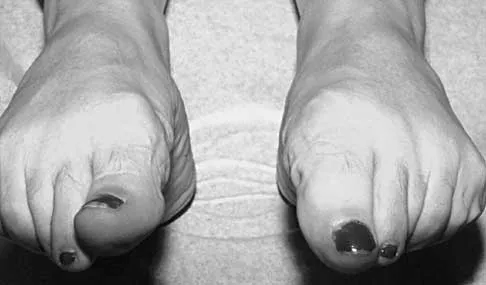
What is the most common surgical cause of the foot deformity shown in Figure 9?

Explanation
The radiograph shows a hallux varus deformity. Iatrogenically acquired hallux varus is most often the result of excessive lateral soft-tissue release, sesamoidectomy, or both. It also can be caused by a medial tibial sesamoid subluxation in conjunction with excessive postoperative dressing application, overcorrection of the intermetatarsal angle, or excessive medial eminence resection. Donley BG: Acquired hallux varus. Foot Ankle Int 1997;18:586-592.
Question 17
What is the reported failure rate for surgical treatment of a Morton's neuroma?

Explanation
The reported failure rate is in the range of 15%, which may be the result of incorrect diagnosis, improper web space selection, or formation of a stump neuroma. Therefore, the procedure should be approached with caution, measures should be taken to ensure that the diagnosis is accurate, and nonsurgical options should be exhausted. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111. Beskin JL: Nerve entrapment syndromes of the foot and ankle. J Am Acad Orthop Surg 1997;5:261-269.
Question 18
A 35-year-old woman who runs long distance has had posterior calf tenderness for the past 3 months. A clinical photograph is shown in Figure 10a, and MRI scans are shown in Figures 10b and 10c. Management at this point should consist of



Explanation
10b 10c The initial treatment for peritendinitis should consist of calf stretching in an eccentric mode and physical therapy. In a recent study, this treatment has been found superior to surgical debridement in nonextensive peritendinitis and pantendinitis. A non-weight-bearing cast, while useful in reducing inflammation, will result in calf atrophy and poorly organized collagen repair. Cortisone is contraindicated because of the danger of tendon damage. Tendon debridement at this stage is not indicated. Alfredson H, Pietila T, Jansson P, Lorentzon R: Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med 1998;26:360-366.
Question 19
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?



Explanation
The patient has nonunions of the metatarsal fractures and a hallux valgus deformity with arthritic changes. To address all of the findings, management should consist of open treatment of the metatarsal nonunions and hallux metatarsophalangeal arthrodesis. Cast immobilization and a bone stimulator are unlikely to be beneficial at this time. Isolated correction of the hallux valgus deformity will not address the metatarsal nonunions or the arthritis at the hallux metatarsophalangeal joint. Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214. McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Question 20
The use of posting (a wedge added to the medial or lateral side of an insole) is useful to balance forefoot or hindfoot malalignment. Assuming normal subtalar joint pronation, what is the maximum amount of recommended hindfoot posting?


Explanation
Generally, patients cannot tolerate more than 5 degrees of hindfoot posting. Donatelli RA, Hurlbert C, Conaway D, et al: Biomechanics foot orthotics: A retrospective study. J Orthop Sports Phys Ther 1988;10:205-212. Michaud TM: Foot Orthoses and Other Forms of Conservative Foot Care. Baltimore, MD, Williams & Wilkins, 1993, pp 61-65, 186.
Question 21
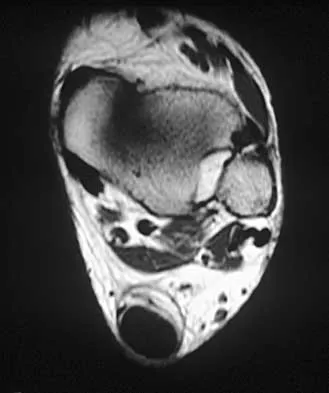
A 40-year-old woman has a symptomatic mass on the anterior aspect of the ankle. She reports no constitutional symptoms. An MRI scan is shown in Figure 12. What is the most likely diagnosis?


Explanation
The MRI scan reveals a lobular mass that is below the vitamin E tablet marker taped to the skin. This is juxtaposed to the tibialis anterior tendon. It is slightly more enhanced than the surrounding subcutaneous fat and is consistent with a ganglion. Osteosarcoma, aneurysmal bone cyst, or unicameral bone cyst all would demonstrate enhancement or pathology in the bone. This is clearly a well-defined soft-tissue mass. Gouty tophi show low to intermediate signal on T1- and T2-weighted images. Kransdorf MJ, Jelinek JS, Moser RP Jr, et al: Soft tissue masses: Diagnosis using MR imaging. Am J Roentgenol 1989;153:541-547. Wetzel LH, Levine E: Soft-tissue tumors of the foot: Value of MR imaging for specific diagnosis. Am J Roentgenol 1990;155:1025-1030.
Question 22
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?

Explanation
The most likely diagnosis is a stress fracture of the calcaneus and is supported by the history of running, female gender, and amenorrhea. Reproducing pain with medial and lateral compression of the heel also supports the diagnosis. A bone scan or MRI would most likely confirm the diagnosis. Plantar fasciitis would result in pain on the bottom of the heel with point tenderness. The lack of other areas of involvement or other symptoms does not support a seronegative inflammatory arthritis. Tarsal tunnel syndrome and peripheral neuropathy are unlikely because of the normal neurologic examination. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Question 23
A 28-year-old woman has a moderate hallux valgus deformity and a prominence of the medial eminence. She can participate in all activities and reports that she could wear 3-inch heels in the past, but she now notes medial eminence pain even while wearing a soft leather flat shoe with a cushioned sole. She requests recommendations regarding surgical correction. Examination reveals a 1-2 intermetatarsal angle of 10 degrees. A clinical photograph and radiograph are shown in Figures 13a and 13b. What is the best course of action?


Explanation
13b Based on her symptoms and prior shoe wear modifications, the treatment of choice is surgical correction of the hallux valgus with a chevron osteotomy. There are no data to support the use of a custom orthosis to delay the progression of a hallux valgus deformity. Steroid injection would only risk infection, as well as joint and capsule damage. Extra-depth shoes are an option; however, the patient is interested in surgical options. Chou LB, Mann RA, Casillas MM: Biplanar chevron osteotomy. Foot Ankle Int 1998;19:579-584. Coughlin MJ: Roger A. Mann Award: Juvenile hallux valgus. Etiology and treatment. Foot Ankle Int 1995;16:682-697.
Question 24
A 20-year-old woman has lateral foot and ankle pain after sustaining an inversion injury of the ankle while playing soccer 3 months ago. Activity modifications and physical therapy have failed to provide relief. She describes burning pain that extends from the anterior aspect of the ankle to the foot and lateral two toes. The pain is often worse at night. Plain radiographs, a bone scan, and an MRI scan are normal. Stress examination reveals no instability. What is the most likely diagnosis?

Explanation
Persistent pain following an ankle sprain can present a diagnostic dilemma. All of the injuries listed should be considered in the differential diagnosis. The superficial peroneal nerve courses in the lateral compartment and exits the crural fascia 12 to 15 cm above the level of the ankle. Muscle herniation through the fascial defect has been reported to be associated with entrapment of this nerve. The fascial hiatus also may serve as a potential tether in cases of inversion injuries causing injury to the superficial peroneal nerve. Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Question 25
A 35-year-old runner has pain beneath the second metatarsophalangeal joint. He reports that he has significantly decreased his running distance since the onset of the pain. He denies any history of trauma or injury to the foot. A radiograph is shown in Figure 14. Initial management should consist of


Explanation
The presence of the relatively long second metatarsal, along with the close approximation of the second and third metatarsal heads, are consistent with second metatarsophalangeal tenosynovitis. The hallmark of initial management is conservative. Modalities include taping, nonsteroidal anti-inflammatory drugs, metatarsal pads, and cortisone injections. Trepman and Yeo combined the use of a cortisone injection with a rocker bottom sole. Mizel and Michelson reported their results using an extended rigid steel shank shoe along with a cortisone injection. Trepman E, Yeo SJ: Nonoperative treatment of metatarsophalangeal joint synovitis. Foot Ankle Int 1995;16:771-777.
Finish Exam?
You cannot change answers after submitting.
