Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
High Yield
The relocation test is most reliable for diagnosing anterior subluxation of the glenohumeral joint when

Detailed Explanation
The relocation test is most accurate when true apprehension is produced with the arm in combined abduction and external rotation and then relieved when posterior pressure is placed on the humeral head. Pain with this test is a less specific response and may occur with other shoulder disorders such as impingement.
Question 2
A 28-year-old man has left knee pain after a snow skiing accident. The MRI scan shown in Figure 47 reveals which of the following?

Explanation
Bone bruises are often noted on MRI after anterior cruciate and medial collateral ligament injuries. The significance of these injuries awaits long-term follow-up studies. The areas of increased signal on T2-weighted images represent areas of acute hemorrhage and are secondary to microfractures of the adjacent medullary trabeculae. Wright RW, Phaneuf MA, Limbird TJ, et al: Clinical outcome of isolated subcortical trabecular fractures (bone bruise) detected on magnetic resonance imaging in knees. Am J Sports Med 2000;28:663-667.
Question 3
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child's back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of


Explanation
Congenital anomalies of the spine, including failure of formation and failure of segmentation, are associated with other anomalies in other organ systems that develop at the same time. These include anomalies in the genitourinary system, cardiac anomalies, Sprengel's deformity, radial hypoplasia, and gastrointestinal anomalies including imperforate anus and trachealesophageal fistula. Spinal dysraphism is the most common associated abnormality. McMaster found an 18% incidence before the common use of MRI. Bradford and associates reported on 16 of 42 patients with congenital spinal anomalies and spinal dysraphism using MRI. Neural axis lesions may be associated with visible midline abnormalities such as a hairy patch or nevus. The child has already had a cardiac and renal work-up, and based on the findings of the hairy patch and congenital vertebral anomalies, MRI of the entire spine is prudent at this time. Spinal fusion is indicated for progressive congenital scoliosis or kyphosis. Physical therapy does not affect the natural history of congenital scoliosis. McMaster MJ: Occult intraspinal anomalies and congenital scoliosis. J Bone Joint Surg Am 1984;66:588-601. Bradford DS, Heithoff KB, Cohen M: Intraspinal abnormalities and congenital spine deformities: A radiographic and MRI study. J Pediatr Orthop 1991;11:36-41.
Question 4
High Yield
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Detailed Explanation
Weil osteotomies are useful in achieving shortening of a lesser metatarsal with preservation of the distal articular surface. The osteotomy is oriented from distal-dorsal to proximal-plantar; therefore, proximal displacement of the distal fragment is associated with plantar (not dorsal) displacement as well. Plantar displacement can result in the intrinsics acting dorsal to the center of the metatarsophalangeal joint and the development of an extended or "floating toe." Nonunion, osteonecrosis, and inadequate shortening are infrequent complications associated with the Weil lesser metatarsal osteotomy. Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Question 5
High Yield
A 40-year-old woman with no history of back problems has a symptomatic L4-5 disk herniation with an L5 radiculopathy that has failed to respond to 12 weeks of nonsurgical management. In the preoperative discussion, the surgeon advises the patient that the chance of recurrence of the herniation after successful diskectomy is what percent?
Explanation
The incidence of recurrent disk herniation after a successful diskectomy is approximately 5% to 10%. Indications for surgical diskectomy for a recurrence are the same as for a primary diskectomy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 685-698.
Question 6
High Yield
A 61-year-old man has a symptomatic bunionette that is refractory to nonsurgical management. A radiograph is shown in Figure 6. What is the optimal surgical correction?

Explanation
The patient has a bunionette with a large 4-5 intermetatarsal angle. This requires not only ostectomy of the lateral prominence but metatarsal osteotomy to decrease the intermetatarsal angle. Excising the head results in a flail joint and creates the possibility of a transfer lesion. Condylectomy can reduce plantar pressures but does not address the bunionette. The joint surface is well maintained, thus there are no indications for resection. Coughlin MJ: Treatment of bunionette deformity with longitudinal diaphyseal osteotomy with distal soft tissue repair. Foot Ankle 1991;11:195-203.
Question 7
High Yield
Which of the following nutraceuticals has been associated with perioperative bleeding?

Explanation
Ginkgo biloba is a popular nutraceutical for patients who have early dementia, intermittent claudication secondary to peripheral vascular disease, vertigo, and tinnitus. It is reported to improve mental alertness and cognitive deficiency. It has antiplatelet properties as a result of one of its components, ginkgolide B, which displaces platelet-activating factor from its receptor binding sight. Rowin and Lewis reported on spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Vale also reported on subarachnoid hemorrhage associated with ginkgo biloba. Bebbington and associates reported on persistent postoperative bleeding after total hip arthroplasty secondary to ginkgo biloba usage. Furthermore, the use of ginkgo biloba with aspirin or other antiplatelet agents or anticoagulants represents a relative contraindication. Physicians should be aware not only of prescribed medications but also alternative nutraceuticals that are used by the patient. Rowin J, Lewis SL: Spontaneous bilateral subdural hematomas associated with chronic ginkgo biloba ingestion. Neurology 1996;46:1775-1776. Vale S: Subarachnoid hemorrhage associated with ginkgo biloba. Lancet 1998;352:36.
Question 8
High Yield
What is the most common site of metastases from a soft-tissue sarcoma?

Explanation
The most common site of metastases from a soft-tissue sarcoma is the lungs and occurs in 40% to 60% of patients. The second most common site of metastases in soft-tissue sarcomas is the lymph nodes. Nodal metastases are seen with regularity in synovial sarcoma, epithelioid sarcoma, and rhabdosarcoma. The liver, brain, bone, and muscle are occasional sites of spread, but the occurrence is very rare. Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Question 9
High Yield
The husband of a 22-year-old woman has hypophosphatemic rickets. The woman has no orthopaedic abnormalities, but she is concerned about her chances of having a child with the same disease. What should they be told regarding this disorder?
Explanation
Hypophosphatemia is a rare genetic disease usually inherited as an X-linked dominant trait. The fact that the woman has no skeletal manifestations would indicate that the husband has the X-linked mutation. The disease is more severe in boys than it is in girls. The husband will not transmit the disease to his sons. However, all of their daughters will be affected either with the disease or as carriers. If the woman has the disease or the trait, there is a 50% chance that her sons will inherit the disease and a 50% chance that her daughters will be carriers or have a milder form of the disease. Parents should be advised to have genetic counseling so they can be informed when deciding whether to have children. Herring JA: Metabolic and endocrine bone diseases, in Tachdjian's Pediatric Orthopaedics, ed 3. New York, NY, WB Saunders, 2002, pp 1685-1743. Sillence DO: Disorders of bone density, volume, and mineralization, in Rimoin DL, Conner JM, Pyerite RE, et al (eds): Principles and Practice of Medical Genetics, ed 4. New York, NY, Churchill Livingstone, 2002.
Question 10
What is the primary limiting membrane and mechanical support for the periphery of the physis?

Explanation
The perichondrial fibrous ring of La Croix acts as a limiting membrane that provides mechanical support for the bone-cartilage junction of the growth plate. It is continuous with the ossification groove of Ranvier, which contributes chondrocytes for the increase in width of the growth plate. The zone of provisional calcification lies at the bottom of the hypertrophic zone and is the site of initial calcification of the matrix. It is quite weak and usually is the cleavage plane for fractures; therefore, it does not qualify as mechanical support. The last intact transverse septum separates the zone of provisional calcification from the primary spongiosa and provides no real support to the physis. The primary spongiosa is the part of the metaphysis nearest the physis. Netter FH: Growth plate, in Woodburne RT, Crelin ES, Kaplan FS, Dingle RV (eds): The Ciba Collection of Medical Illustrations. Summit, NJ, Ciba-Geigy Corporation, 1987, vol 8, pp 166-167.
Question 11
Figures 1a and 1b show the sagittal T2- and T1-weighted MRI scans of a 25-year-old intravenous drug abuser who has low back pain that is increasing in intensity. Laboratory studies show a WBC count of 10,000/mm3 and an erythrocyte sedimentation rate of 80 mm/h. Blood culture is negative. Initial management consist of


Explanation
The MRI scans show vertebral diskitis/osteomyelitis. The treatment of spinal infection in adults should be organism specific; therefore, initial management should consist of CT-guided closed biopsy prior to administration of antibiotic coverage. An open biopsy is indicated for a failed closed biopsy or failure of nonsurgical management. Although Staphylococcus aureus is the most common bacteria, a history of intravenous drug abuse raises suspicion for other organisms, including Pseudomonas. Tay BK, Deckey J, Hu SS: Spinal Infections. J Am Acad Orthop Surg 2002;10:188-197.
Question 12
High Yield
Figures 32a and 32b show the AP and lateral radiographs of an 11-year-old boy who has a severe limp, a fever, and swelling and tenderness of the thigh. Aspiration of the bone reveals purulent material. The patient has most likely been symptomatic for


Explanation
In patients with an osteomyelitic infection, radiographic findings at 1 to 5 days usually show soft-tissue swelling only. Seven to 14 days after symptoms begin, radiographs will most likely show the classic signs of acute osteomyelitis. Reactive bone formation would be expected by 6 months. Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 13
High Yield
A 7-year-old girl reports foot pain and has difficulty ambulating. History reveals that she fell off a scooter 1 week ago, and there is possible exposure to a tick bite. A radiograph is shown in Figure 29. What is the best course of action?

Detailed Explanation
The child has Kohler's disease. This is a self-limiting osteochondritis of the navicular. It is treated symptomatically with initial cast immobilization for 6 to 12 weeks, followed possibly by orthotic management. Findings shown in the radiograph usually will normalize within 1 year, and there are no long-term sequelae. Borges JL, Guille JT, Bowen JR: Kohler's bone disease of the tarsal navicular. J Pediatr Orthop 1995;15:596-598.
Question 14
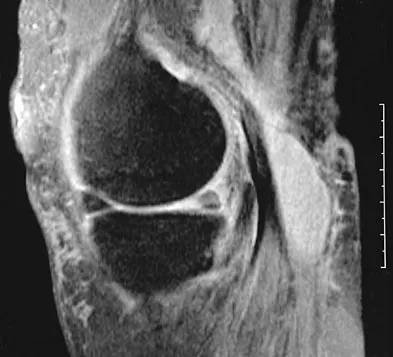
A 28-year-old man reports knee stiffness, swelling, and a constant ache that is worse with activity. Examination reveals an effusion, global tenderness, and warmth to the touch. Flexion is limited to 110 degrees. Figures 48a through 48d show sagittal T1-weighted, sagittal T2-weighted, axial T1-weighted fat-saturated gadolinium, and axial gradient echo MRI scans. Based on these findings, what is the most likely diagnosis?




Explanation
The MRI scans show multiple low-signal intensity lesions scattered throughout the knee, extending posteriorly inferior to the tibial plateau. The low-signal intensity on both the T1- and T2-weighted images, the modest vascularity noted on the gadolinium image, and the "blooming" noted on the gradient echo image (ferrous-laden tissue) are all strongly suggestive of diffuse PVNS. Whereas synovial chondromatosis can present as diffuse masses in the knee, they present as nodule masses that have low T1- and high T2-weighted signal characteristics. Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4241-4252.
Question 15
When the elbow is extended and an axial load is applied, what percent of stress distribution occurs across the ulnohumeral and radiohumeral articular surface, respectively?

Explanation
When load is applied to the wrist, most of the stress is absorbed by the radius. As the load is transferred through the forearm, the interosseous membrane transfers some of the load from the radius to the ulna. The load at the elbow is distributed with 40% at the ulnohumeral articulation and 60% at the radiohumeral articulation. Halls AA, Travill R: Transmission of pressure across the elbow joint. Anat Rec 1964;150:243.
Question 16
A 37-year-old electrician is diagnosed with a frozen shoulder after sustaining an electrical injury at work 2 weeks ago. Examination reveals that he cannot actively or passively externally rotate or abduct the arm. The glenohumeral joint and scapula move in a 1:1 ratio. Radiographs are shown in Figures 15a and 15b. The best course of action should be


Explanation
The patient's history, examination, and radiographs are classic for locked posterior dislocation of the glenohumeral joint. Posterior dislocation of the shoulder remains the most commonly missed dislocation of a major joint. Up to 80% are missed on initial presentation. The primary cause for failure to accurately diagnose this injury is inadequate radiographic evaluation. The typical presentation is a shoulder locked in internal rotation with loss of abduction. An axillary view not only will make the definitive diagnosis but will help assess the size of the articular surface defect and help plan treatment. This view can be done expediently as part of every trauma series. The AP view is suspicious for a posteriorly dislocated humerus with loss of the humeral neck profile, a vacant glenoid sign, and an anterior humeral head compression fracture (reverse Hill-Sachs lesion). Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18. Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosement, IL, American Academy of Orthopaedic Surgeons, 1997, pp 181-189.
Question 17
Which of the following imaging modalities is most accurate in locating a toothpick in the plantar arch of the foot?

Explanation
Ultrasound is best at imaging abrupt changes in the density of adjacent tissue and therefore is best at imaging wood in the soft tissues of the foot. Mizel MS, Steinmetz ND, Trepman E: Detection of wooden foreign bodies in muscle tissue: Experimental comparison of computed tomography, magnetic resonance imaging, and ultrasonography. Foot Ankle Int 1994;15:437-443.
Question 18
High Yield
The MRI findings shown in Figure 51 would most likely create which of the following signs and symptoms?
Explanation
The MRI scan shows a far lateral disk herniation. With the L4-5 disk, a far lateral herniation abuts the left L4 nerve root. The findings would be consistent with those of a left L4 radiculopathy and would include pain or a sensory deficit on the anteromedial aspect of the knee, diminished patellar tendon reflex, and quadriceps weakness, perhaps making it difficult to walk up and down stairs. Fardin DF, Garfin SR (eds): Orthopaedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 329.
Question 19
High Yield
A 42 year-old-woman who underwent surgery for lumbar scoliosis 2 years ago now has fixed sagittal plane imbalance and severe back pain. Which of the following is considered a contraindication to isolated pedicle subtraction osteotomy for the treatment of iatrogenic flatback syndrome in this patient?
Explanation
Pedicle subtraction osteotomy is the preferred osteotomy technique for the treatment of many patients with iatrogenic flatback syndrome. In the presence of an anterior pseudarthrosis, however, it must be done in conjunction with an anterior procedure. Prior laminectomy is not a contraindication. Significant correction, usually averaging about 30 degrees, can be obtained through each osteotomy. Osteotomies should be performed at L2 or below in the presence of kyphosis at the thoracolumbar junction. The pedicle subtraction technique is preferred with vascular calcifications because it does not lengthen the anterior column, which could risk vascular injury. Potter BK, Lenke LG, Kuklo TR: Prevention and management of iatrogenic flatback deformity. J Bone Joint Surg Am 2004;86:1793-1808.
Question 20
High Yield
A 32-year-old man sustained a closed injury after falling 25 feet from a roof. His ankle and foot are severely swollen. Radiographs and CT scans are shown in Figures 29a through 29d. Initial management should consist of


Explanation
The patient has a severe high-energy injury from axial loading to the left ankle and distal tibia. This is a closed injury, but the soft tissues are injured and severely swollen. Initial treatment should focus on skeletal stabilization, and incisions directly over the fracture area should be avoided until soft-tissue stabilization has occurred. Immediate spanning external fixation with plans for a delayed reconstruction as needed for the joint surface is the treatment of choice. Closed reduction and application of a constrictive long leg cast may lead to increased risk of tissue necrosis. Immediate open procedures to internally fix the fracture add the risks of soft-tissue necrosis and are to be avoided. Percutaneous plating may be one of the delayed fixation options but should not be used immediately. Primary ankle arthrodesis is not indicated. Thordarson DB: Complications after treatment of tibial pilon fractures: Prevention and management strategies. J Am Acad Orthop Surg 2000;8:253-265. Marsh JL, Bonar S, Nepola JV, DeCoster TA, Hurwitz SR: Use of an articulated external fixator for fractures of the tibial plafond. J Bone Joint Surg Am 1995;77:1498-1509.
Question 21
High Yield
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a


Detailed Explanation
Meniscal tears have many configurations and locations. The normal medial meniscus has a bow-tie configuration on the two most medial consecutive sagittal views. Toward the center of the joint the anterior and posterior horns have a triangular shape. These images show an abnormal intra-articular low-signal structure located anterior to the intact posterior cruciate ligament. This most likely represents a torn and displaced posterior horn of the medial meniscus, sometimes called "double PCL sign". A popliteal cyst and ligaments of Wrisberg and Humphry are not visible on these figures. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 22
High Yield
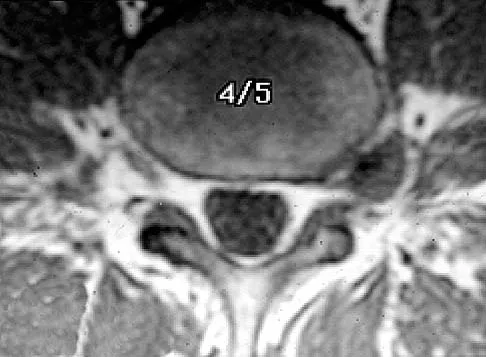
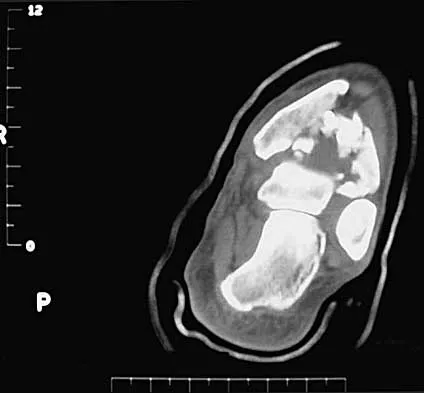
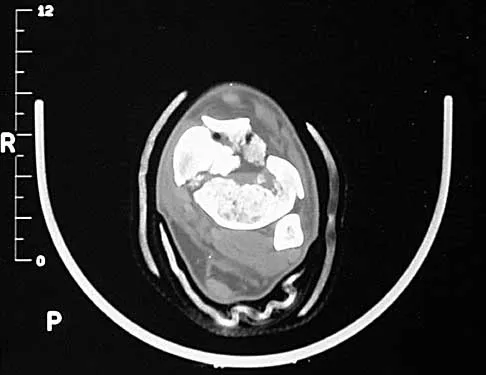
Figure 12 shows the lumbar CT scan of a 24-year-old man who was injured in a snowmobile accident. What is the mechanism of injury?

Explanation
A true compression fracture is a single-column injury that does not create canal compromise. A burst fracture is a two- or three-column injury that disrupts the middle column and thereby narrows the spinal canal. This patient has a burst fracture. The mechanism of injury is usually vertical compression or flexion compression. Garfin SR, Vaccaro AR (eds): Orthopaedic Knowledge Update: Spine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 197-217.
Question 23
High Yield
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured?
Detailed Explanation
The athlete has symptoms referable to the axillary, musculocutaneous, and suprascapular nerves resulting from an injury to the upper trunk of the brachial plexus. This portion of the plexus is formed by contributions of the fourth through sixth cervical nerve roots. This area is often contused or stretched following a tackling maneuver that results in either depression of the shoulder from contact at Erb's point or traction of the upper plexus from forced stretching of the neck to the contralateral side. Schenck CD: Anatomy of the innervation of the upper extremity, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby-Year Book, 1991.
Question 24
High Yield
What type of injury is considered the major mechanism of cervical fracture, dislocation, and quadriplegia in contact sports and diving?

Explanation
A compression or burst injury occurs with vertical loading of the spine, such as from a blow to the vertex with the neck flexed (eg, spear tackling in football). This leads to vertebral end plate fractures before disk injury. At higher forces, the entire vertebra and disk may explode into the spinal canal. Analysis has shown this to be the major mechanism of cervical fracture, dislocation, and quadriplegia. With the normal head-up posture, the cervical spine has a gentle lordotic curve, and forces transmitted to the head are largely dissipated in the cervical muscles. When the neck is flexed, the cervical spine becomes straight, with the vertebral bodies lined up under one another. This allows for minimal dissipation of the impact forces to be absorbed by the neck muscles. Cantu RC: Head and spine injuries in youth sports. Clin Sports Med 1995;14:517-532. Proctor MR, Cantu RC: Head and neck injuries in young athletes. Clin Sports Med 2000;19:693-715.
Question 25
High Yield
What fibers of the anterior cruciate ligament tighten with extension of the knee?
Detailed Explanation
The anterior cruciate ligament consists of two functional bundles: anteromedial and posterolateral. During extension of the knee, the posterolateral bundle becomes taut. In flexion, the anteromedial bundle is tight and the posterolateral bundle relaxes. Traditionally, anterior cruciate ligament reconstruction primarily recreates the anteromedial bundle. Recently, techniques for double bundle reconstruction have been described to recreate the normal anatomic relationship of the two bundles. Girgis FG, Marshall JL, Monajem AS: The cruciate ligaments of the knee joint: Anatomical, functional and experimental analysis. Clin Orthop Relat Res 1975;106:216-231. Cha PS, Brucker PU, West RV, et al: Arthroscopic double-bundle anterior cruciate ligament reconstruction: An anatomic approach. Arthroscopy 2005;21:1275.
Question 26
A 9-year-old child sustains a proximal tibial physeal fracture with a hyperextension mechanism. What structure is at most risk for serious injury?

Explanation
The most serious injury associated with proximal tibial physeal fracture is vascular trauma. The popliteal artery is tethered by its major branches near the posterior surface of the proximal tibial epiphysis. During tibial physeal displacement, the popliteal artery is susceptible to injury. Injuries to the other structures are less common.
Question 27
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management?
Explanation
Examination reveals an irritable hip, creating a differential diagnosis of transient synovitis versus pyogenic hip arthritis. Kocher and associates described four criteria to help predict the presence of infection: inability to bear weight, fever, ESR of more than 40 mm/h, and a peripheral WBC count of more than 12,000/mm3. This patient meets three of the four criteria, with a positive predictive value of 73% to 93% for joint infection. Therefore, aspiration of the hip is warranted, with a high likelihood that emergent hip arthrotomy will be indicated. Ideally, intravenous antibiotics should be administered after culture material has been obtained from needle aspiration of the hip. An urgent bone scan is better indicated as a screening test for sacroiliitis or diskitis. If the arthrocentesis proves negative, CT or MRI of the pelvis may be indicated to rule out a pelvic or psoas abscess. Del Beccaro MA, Champoux AN, Bockers T, et al: Septic arthritis versus transient synovitis of the hip: The value of screening laboratory tests. Ann Emerg Med 1992;21:1418-1422. Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinical prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 28
An otherwise healthy 16-year-old boy who has had thoracolumbar pain with an increasingly worse deformity for the past 2 years now reports that the pain is worse at night. He responded well to nonsteroidal anti-inflammatory drugs initially, but they have become less effective. He denies any neurologic or constitutional symptoms. Examination is consistent with a mild thoracolumbar scoliosis and is otherwise normal. Laboratory studies show a normal CBC, erythrocyte sedimentation rate, and C-reactive protein. Standing radiographs show a 20 degree left thoracolumbar scoliosis, and he has a Risser stage of 4. A bone scan shows increased uptake at L2; a CT scan through this level is shown in Figure 18. Management should now consist of

Explanation
The findings and radiographic appearance are most consistent with osteoid osteoma involving the medial pedicle. Scoliosis is commonly seen with this lesion and usually does not need surgical intervention. Excellent results have been reported with surgical excision as well as with percutaneous thermocoagulation. Nonsurgical treatment also has been described in peripheral osteoid osteoma but is not well described for lesions within the spine. Cove JA, Taminiau AH, Obermann WR, Vanderschueren GM: Osteoid osteoma of the spine treated with percutaneous computed tomography-guided thermocoagulation. Spine 2000;25:1283-1286. Kneisl JS, Simon MA: Medical management compared with operative treatment for osteoid-osteoma. J Bone Joint Surg Am 1992;74:179-185.
Question 29
High Yield
Which of the following mechanisms is considered the most common cause of failure of osteoarticular allografts used for articular reconstruction?

Explanation
Mechanical loosening and infection can occur as complications after surgery, but the most common cause of osteoarticular allograft failure is graft collapse during revascularization. Clinical rejection because of an immune response is an unusual means of failure. Meyers MH, Akeson W, Convery FR: Resurfacing of the knee with fresh osteochondral allograft. J Bone Joint Surg Am 1989;71:704-713.
Question 30
High Yield
A 24-year-old athlete has a painful right shoulder. Figure 30 shows an intra-articular photograph that was obtained through a posterior portal during arthroscopy; the labrum is indicated by the arrow. Based on these findings, management should consist of
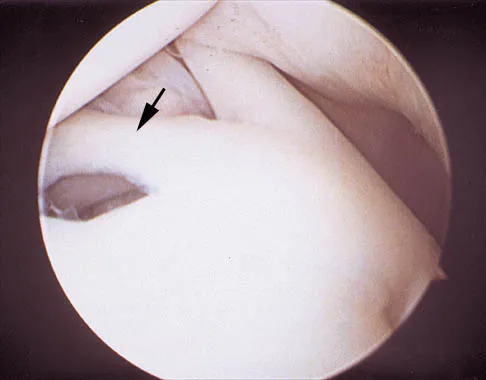
Explanation
The photograph shows a normal variant that is a sublabral hole beneath the anterosuperior labrum. In some instances, the labrum will become confluent with the middle glenohumeral ligament as a stout band. Because this variant is not abnormal, no treatment is necessary. Securing this portion of the labrum to the capsule may tighten the middle glenohumeral ligament complex and restrict external rotation of the arm. Andrews JR, Guerra JJ, Fox GM: Normal and pathologic arthroscopic anatomy of the shoulder, in Andrews JR, Timmerman LA (eds): Diagnostic and Operative Arthroscopy, ed 1. Philadelphia, PA, WB Saunders, 1997, pp 60-76.
Question 31
A 65-year-old man has chronic Achilles insertional tendinitis that is refractory to nonsurgical management. A radiograph is shown in Figure 9. Preoperative counseling should include a discussion of the realistic duration of postoperative recovery. You should inform the patient that his expected recovery will last

Explanation
An older patient with calcaneal enthesopathy may take a year or more to recover after tendon debridement and calcaneal ostectomy. Young patients, and those with purely tendon pathology, may recover more quickly. McGarvey WC, Palumbo RC, Baxter DE, et al: Insertional Achilles tendinitis: Surgical treatment through a central tendon splitting approach. Foot Ankle Int 2002;23:19-25.
Question 32
A 58-year-old reports pain and stiffness in his left shoulder following a seizure episode. Diagnosis at the time of the seizure is a frozen shoulder, and management consists of an aggressive physical therapy program of stretching exercises. Four months later he continues to have shoulder pain and has not gained any additional range of motion. A CT scan is shown in Figure 50. Management should now consist of

Explanation
Humeral arthroplasty is indicated for chronic posterior dislocations when the impression defect in the humeral head is greater than 45% to 50%. If the condition remains undiagnosed for more than 9 to 12 months, secondary degenerative changes on the glenoid may occur, necessitating total shoulder arthroplasty. Open reduction and transfer of the subscapularis and lesser tuberosity are used for impression defects that consist of 20% to 40% of the humeral articular surface. Closed reduction and immobilization with the arm in slight extension and external rotation is useful when the posterior dislocation is diagnosed within the first 6 weeks and the articular defect is less than 20%. Hawkins RJ, Neer CS II, Pianta RM, Mendoza FX: Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 1987;69:9-18.
Question 33
Figure 39 shows the radiograph of a 4-month old infant who has been undergoing weekly casting since birth for a congenital equinovarus deformity. Management should now consist of

Explanation
The radiograph shows the development of a rocker-bottom foot deformity. A rocker-bottom foot occurs in the treatment of clubfoot when casting is continued in the presence of a very tight gastrocnemius-soleus complex and an uncorrected hindfoot. While there are some preliminary reports on using Botox injection and continued casting for the equinus deformity, most authors recommend posterior or posterior medial release. Percutaneous tenotomy has been recently recommended with the resurgence of the Ponsetti technique. Lehman WB, Atar D: Complications in the management of talipes equinovarus, in Drennan JC (ed): The Child's Foot and Ankle. New York, NY, Raven Press, 1992, pp 135-136. Herring JA: Tachdjian's Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 927-935.
Question 34
Vertebral fractures are common in the thoracolumbar spine. What is the most important factor that determines the strength of the cancellous bone in the vertebral body?
Explanation
Cancellous bone strength and stiffness are determined primarily by the apparent density (the amount of bone per unit volume). Strength varies approximately as the square of the density, and stiffness as the cube of the density; therefore, these are very strong relationships. Cancellous bone strength also depends on the mineral content, the rate of loading (it is viscoelastic), the anatomic level, and the trabecular number (an histomorphometry term), but all to a markedly lesser extent than density. Carter DR, Hayes WC: The compressive behavior of bone as a two-phase porous structure. J Bone Joint Surg Am 1977;59:954-962.
Question 35
High Yield
A patient with diabetic peripheral neuropathy undergoes a partial first ray amputation for a chronic ulcer beneath the first metatarsal head. The insertion of the anterior tibialis is preserved. The patient has 10 degrees of passive dorsiflexion at the ankle and no other foot deformities or ulcers. Which of the following is considered appropriate shoe wear for this patient?
Explanation
The steel shank is a flat 1-inch steel strip placed between layers of the shoe to extend the foot lever and prevent deformity at the toe break seen following a partial first ray amputation. A rocker sole may be added as well to facilitate transition from foot flat to the toe-off phase of gait. Proper shoe fit is important, but "snug" fitting shoes in a patient with peripheral neuropathy and likely fluctuations in volume from intermittent swelling are to be avoided. A custom shoe is an unnecessary expense. The patient has at least 10 degrees of dorsiflexion at the ankle with an intact anterior tibialis muscle; therefore, catching the sole on carpeting should not be a problem. Philbin TM, Leyes M, Sferra JJ, et al: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Question 36
High Yield
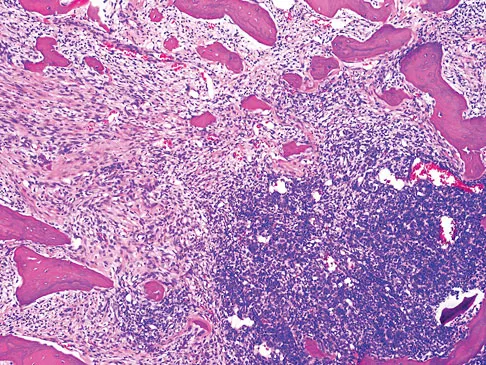
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?

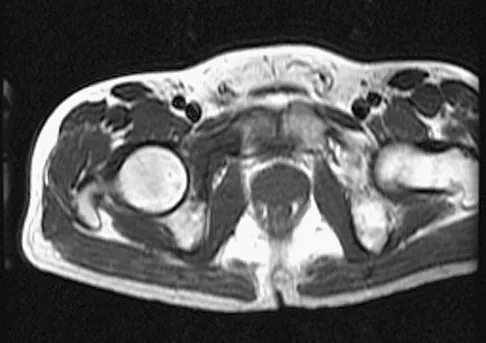

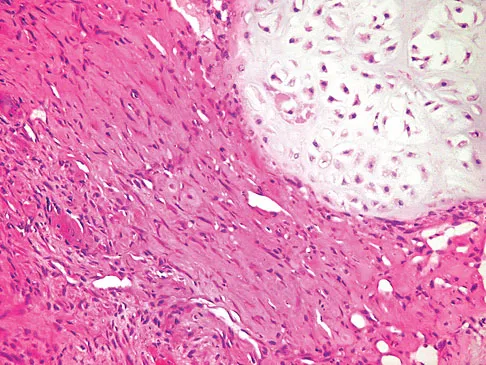
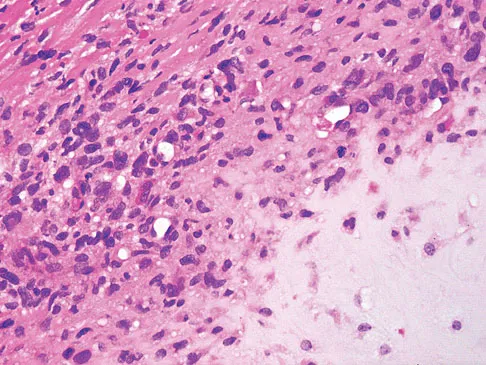
Explanation
The definitive surgery would be removal of the entire resection bed, and in this case of dedifferentiated chondrosarcoma, a hemipelvectomy was performed. The MRI and CT scans show an aggressive cartilage lesion. The histology, representative of a dedifferentiated chondrosarcoma, shows a bimorphic low-grade cartilage lesion with high-grade spindle cell sarcoma. The cartilage lesion is usually an enchondroma or low-grade chondrosarcoma. The dedifferentiated portion is typically a malignant fibrous histocytoma, osteosarcoma, or fibrosarcoma. Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Question 37
Figure 25 shows the radiograph of an 84-year-old woman who has pain and is unable to extend her knee. History reveals that she underwent total knee arthroplasty 8 years ago. Aspiration and studies for infection are negative. During revision surgery, management of the tibial bone loss should consist of

Explanation
Massive bone loss encountered in revision total knee arthroplasty remains a significant challenge. Recent reports have shown high success rates using structural allograft to reconstruct large structural bone defects. A hinged prosthesis is not required in this setting. In this patient, a large amount of posterior cortex has been lost, making the area too large to fill with cement or iliac crest bone graft. Because of her age, the treatment of choice is a revision tibial implant and metal augments. Structural allograft would be suitable in a younger patient. Mow CS, Wiedel JD: Structural allografting in revision total knee arthroplasty. J Arthroplasty 1996;11:235-241. Engh GA, Herzwurm PJ, Parks NL: Treatment of major defects of bone with bulk allografts and stemmed components during total knee arthroplasty. J Bone Joint Surg Am 1997;79:1030-1039.
Question 38
A 64-year-old man with a history of diabetes mellitus underwent open reduction and internal fixation of a displaced ankle fracture 8 weeks ago. Examination now reveals recent onset erythema, warmth, and swelling of the midfoot. Radiographs are shown in Figures 23a through 23d. What is the most likely reason for the swelling of the foot?




Explanation
A Charcot flare in adjacent joints is not uncommon in patients with neuropathy who undergo surgery or other trauma. Venous thrombosis would present with swelling of the entire leg, while infection would present earlier in the postoperative period. The radiographs are pathognomonic of Charcot arthropathy, not an unrecognized fracture or gout. A compartment syndrome this late after injury is extremely rare, and there would be no bony distraction associated with compartment syndrome.
Question 39
Figure 63 shows the radiographs of a 23-year-old man who sustained a twisting injury at work. Swelling, tenderness, and ecchymosis are noted about the entire midfoot. What associated injury is most likely to be problematic?

Explanation
This cuboid compression fracture ("nutcracker" injury) is associated with subtle injury to the Lisfranc complex. This diagnosis must be made to ensure proper treatment.
Question 40
Figures 21a through 21c show the radiographs of a 70-year-old woman who has persistent pain with activity after undergoing hip revision 6 months ago. Treatment should now consist of



Explanation
The radiographs show disruption of the posterior column of the acetabulum with radiolucencies about the component. Because the patient requires a stable construct to allow the bone to heal, the treatment of choice is an antiprotrusio cage and a graft. Gill TJ, Sledge JB, Muller ME: The Burch-Schneider anti-protrusio cage in revision total hip arthroplasty: Indications, principles, and long-term results. J Bone Joint Surg Br 1998;80:946-953.
Question 41
A 42-year-old man has had left lower extremity pain in an L5 radicular pattern for the past 6 weeks. He denies significant axial low back pain. History reveals that he underwent an L4-5 diskectomy with successful relief of similar pain 5 years ago. Which of the following imaging studies would offer the greatest amount of information?
Explanation
MRI with gadolinium will best identify recurrent herniated nucleus pulposus or other root compression and distinguish scar from recurrent disk. CT is unable to distinguish scar from recurrent disk density, and the addition of myelogram dye can reveal compromise of the thecal sac but cannot distinguish the scar from recurrent disk as the source of compression. Although lateral flexion-extension radiographs may be important to rule out any instability, much of that information can be inferred from the associated disk and adjacent bony changes on MRI. Bone scan techniques may identify subtle stress fractures resulting from previous aggressive facet resection, but low back pain also would be expected. Mirowitz SA, Shady KL: Gadopentetate dimeglumine-enhanced MR imaging of the postoperative lumbar spine: Comparison of fat-suppressed and conventional T1-weighted images. Am J Roentgenol 1992;159:385-389.
Question 42
High Yield
Which of the following statements best describes synovial fluid?
Detailed Explanation
Synovial tissue is composed of vascularized connective tissue that lacks a basement membrane. Two cell types (type A and type B) are present: type B cells produce synovial fluid. Synovial fluid is made of hyaluronic acid and lubricin, proteinases,and collagenases. It is an ultrafiltrate of blood plasma added to fluid produced by the synovial membrane. It does not contain erythrocytes, clotting factors, or hemoglobin. It lubricates articular cartilage and provides nourishment via diffusion. Synovial fluid exhibits non-Newtonian flow characteristics. The viscosity coefficient is not a constant, the fluid is not linearly viscous, and its viscosity increases as the shear rate decreases.
Question 43
High Yield
A 42-year-old man sustained a fracture of the distal radius with subsequent stiffness in the ipsilateral shoulder. Despite a 6-month program of range-of-motion exercises, external rotation at the side is limited to 10 degrees. Attempts at closed manipulation are unsuccessful. Treatment should now consist of

Detailed Explanation
When external rotation at the side is limited, the most likely diagnosis is contracture of the rotator cuff interval, including the superior glenohumeral and coracohumeral ligaments. Therefore, the treatment of choice is arthroscopic release of the rotator cuff interval.
Question 44
High Yield
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of


Explanation
The patient has a displaced femoral neck fracture. Although the treatment remains controversial, most clinicians advocate either a closed or open reduction in younger active patients. Achieving an anatomic reduction is necessary to avoid loss of reduction, nonunion, or osteonecrosis. An acceptable reduction may have up to 15 degrees of valgus angulation and 10 degrees of posterior angulation. Parallel multiple screws or pins are the most common method of internal fixation. Prosthetic replacement is generally reserved for older and less active individuals. Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Question 45
Examination of a 41-year-old man who was thrown from a motorcycle reveals that both legs appear externally rotated and there is bruising in the perineal area. He has a blood pressure of 80/40 mm Hg, a pulse rate of 140/min, a respiratory rate of 25/min, and he appears confused. Following administration of 4 L of saline solution and 2 units of packed red blood cells, he has a blood pressure of 80/40 mm Hg, a pulse rate of 160/min, and a respiratory rate of 25/min. The abdominal assessment for intraperitoneal blood is negative. An AP radiograph shows an anteroposterior compression injury with 7 cm of symphysis diastasis but no posterior displacement in the sacroiliac joints. What is the next most appropriate step in management?
Explanation
Because the patient has sustained a major high-energy injury to the pelvic ring, it can be assumed that there is serious bleeding or hemodynamic instability related to a pelvic vascular injury. The goal of intervention at this time is to assist in the resuscitative effort and to stop the bleeding. All attempts at providing fluid and blood are important, but without cessation of the bleeding continued loss occurs and significant problems can ensue such as coagulopathy and multiple organ failure. Noninvasive methods of stabilizating the pelvic ring should be used to stop the bleeding. These methods include wrapping a sheet around the pelvis or using commercially available belts, vacuum beanbags, or pneumatic shock garments. This will provide time to prepare for arteriography and/or external fixation. The next step is debatable but in view of negative findings for intra-abdominal blood, arteriography performed with the pelvis reduced using noninvasive methods would be ideal. Bassam D, Cephas GA, Ferguson KA, Beard LN, Young JS: A protocol for the initial management for unstable pelvic fractures. Am Surg 1998;64:862-867. Levine AM (ed): Orthopaedic Knowledge Update: Trauma. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996, pp 217-226.
Question 46
High Yield
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?


Explanation
The floating elbow is best managed with early open reduction and internal fixation of the humeral and forearm fractures, followed by early range of motion. These fractures predispose the elbow to stiffness, and early range of motion is recommended. Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Question 47
High Yield
Which of the following factors is most closely associated with early postoperative migration of "stand-alone" lumbar interbody fusion cages?

Detailed Explanation
Postoperative migration of lumbar interbody fusion cages is a rare complication. It is most commonly seen after placement of the cages through a posterior approach, with instability of the final construct. It is not associated with the design of the cage, the type of graft used, or a resultant pseudarthrosis. McAfee PC: Interbody fusion cages in reconstructive operations on the spine. J Bone Joint Surg Am 1999;81:859-880.
Question 48
High Yield
Figure 6 shows the radiograph of a 14-year-old baseball player who felt a pop and had an immediate onset of pain in his elbow after a hard throw from the outfield. The best course of action should be to

Explanation
The valgus stress at the elbow caused by throwing strains the medial collateral ligament. The medial epicondyle, on which the ligament inserts, is the last ossification center to fuse to the distal humerus, and acute avulsion of the medial epicondyle can occur in adolescents. If the elbow is allowed to heal in a displaced position, valgus instability and loss of elbow extension may result. Valgus instability is especially problematic for the throwing athlete. Surgical treatment with rigid internal fixation is the treatment of choice for displaced medial epicondyle avulsion fractures. Valgus instability is prevented, and the rigid fixation allows for early range of motion. Case SL, Hennrikus WL: Surgical treatment of displaced medial epicondyle fractures in adolescent athletes. Am J Sports Med 1997;25:682-686.
Question 49
High Yield
Figure 32 shows the radiograph of a laborer who jammed his thumb in a fall. Examination reveals pain at the base of the thumb and proximal thenar eminence region. Management should consist of

Explanation
The radiographs are classic for a Bennett's fracture, which involves a fracture of the palmar ulnar aspect of the proximal phalanx. This fracture fragment is still attached to the anterior oblique ligament. The deforming forces that cause subluxation of the base of the proximal phalanx include the pull of the abductor pollicis longus as well as the adductor pollicis. Adequate reduction can be achieved by closed reduction, percutaneous pin fixation, and casting. The fragment is too small for secure internal fixation. Stern PJ: Fractures of the metacarpals and phalanges, in Green DP, Hotchkiss RN, Pederson WC (eds): Green's Operative Hand Surgery, ed 4. Philadelphia, PA, 1999, pp 711-771.
Question 50
High Yield
Degenerative spondylolisthesis of the cervical spine is most commonly seen at which of the following levels?
Explanation
Degenerative spondylolisthesis of the cervical spine is seen almost exclusively at C3-4 and C4-5; this is in contrast to degenerative changes, which are most commonly seen at C5-6 and C6-7. Tani T, Kawasaki M, Taniguchi S, et al: Functional importance of degenerative spondylolisthesis in cervical spondylotic myelopathy in the elderly. Spine 2003;28:1128-1134.
Question 51
The first branch of the lateral plantar nerve innervates the
Explanation
The first branch of the lateral plantar nerve innervates the abductor digiti quinti, and more distal branches of the lateral plantar nerve supply the quadratus plantae and the interossei. The medial plantar nerve supplies the abductor hallucis brevis and the flexor digitorum brevis. Pansky B, House EH: Review of Gross Anatomy, ed 3. New York, NY, Macmillan, 1975, pp 464-476.
Question 52
Figure 7 shows the MRI scan of a 23-year-old competitive rugby player who has anterior ankle pain and swelling. He states that he has been playing for many years and has sprained his ankle several times. Examination will reveal what specific hallmark feature?

Explanation
The history and MRI findings indicate the presence of anterior tibiotalar osteophytes. This is frequently observed in soccer, rugby, and football athletes who play on grass or turf surfaces and repetitively push off and change directions. Examination may reveal an effusion but no loss of subtalar motion. A positive external rotation (Klieger) test is described as pain at the distal ankle with external rotation of the foot and is observed in patients with syndesmosis sprains. This patient may have an increased anterior drawer because of a history of sprains; however, this finding is not specific for anterior impingement of tibiotalar osteophytes. The most specific finding on physical examination is pain with forced dorsiflexion. Ogilvie-Harris DJ, Mahomed N, Demaziere A: Anterior impingement of the ankle of the ankle treated by arthroscopic removal of bony spurs. J Bone Joint Surg Br 1993;75:437-440.
Question 53
Figure 23 shows the radiograph of a 7 year-old girl with a low thoracic-level myelomeningocele. She has a history of skin ulcers over the apex of the deformity, but her current skin condition is good. Management of the spinal deformity should consist of

Explanation
This form of severe kyphosis results in intractable difficulties with sitting position, compression of internal organs, and chronic skin breakdown. Kyphectomy and posterior fusion with instrumentation, while associated with a high rate of complications, provides one of the best solutions to this clinical dilemma. The other choices are either completely ineffective or inadequate in managing this degree of deformity. Lindseth RE: Spine deformity in myelomeningocele. Instr Course Lect 1991;40:273-279.
Question 54
High Yield
What is the maximum acceptable amount of divergence of the interference screw in the femoral tunnel from the bone plug of a bone-patellar tendon-bone graft in anterior cruciate ligament (ACL) reconstruction before pull-out strength is statistically decreased?

Detailed Explanation
In the early 1990s, a transition was made from a two-incision ACL reconstruction to a single-incision ACL reconstruction, and there was concern over divergence of the femoral screws. It was shown radiographically that approximately 5% of the time, divergence of the screw was greater than 15 degrees from the bone plug. In a bovine model, there was significant loss of pull-out strength with an increase in divergence from 15 degrees to 30 degrees. Therefore, attempts should be made to minimize divergence to 15 degrees or less. Lemos MJ, Jackson DW, Lee TO, et al: Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy 1995;11:37-41.
Question 55
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mm3 and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of
Explanation
The patient has diskitis. Administration of IV antibiotics speeds resolution and minimizes recurrence. Bed rest and cast immobilization have been successfully used to treat this disorder but can be associated with prolonged recovery and frequent recurrence, even when oral antibiotics are administered. A perivertebral abscess seen in association with this condition usually resolves without surgery. Ring D, Johnston CE II, Wenger DR: Pyogenic infectious spondylitis in children: The convergence of discitis and vertebral osteomyelitis. J Pediatr Orthop 1995;15:652-660.
Question 56
In the first dorsal compartment of the wrist, what tendon most frequently contains multiple slips?
Explanation
The first extensor compartment of the wrist typically contains a single extensor pollicis brevis tendon and the abductor pollicis longus tendon that nearly always has multiple tendon slips. The extensor pollicis brevis tendon is frequently found to be separated from the slips of the abductor pollicis longus tendon by an intracompartmental septum. During surgery, this septum must be divided to complete the release of the compartment. Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM: Anatomical variations in the first extensor compartment of the wrist: A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-926.
Question 57
Which of the following best describes the course of the ulnar nerve in the midforearm?

Explanation
In the midforearm, the ulnar nerve travels deep to the flexor carpi ulnaris muscle and ulnar to the ulnar artery as it lies on the flexor digitorum profundus muscle. In this region, the ulnar nerve and artery lie side-by-side, whereas more proximal in the forearm, the ulnar artery originates from the brachial artery in the antecubital fossa, and the ulnar nerve lies within the cubital tunnel. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Question 58
High Yield
Which of the following actions best enhances performance when an athlete is participating in a 10K race?
Explanation
Proper hydration prior to an athletic event is the most important determinant of performance. It is virtually impossible to keep pace with fluid loss during an athletic competition. When a net loss of fluid occurs and the athlete is properly prehydrated, this fluid loss will not adversely affect performance. It is not necessary to load up on carbohydrates prior to a 10K race, or to replace calories burned during the race. Hyponatremia can develop in ultra-endurance athletes, especially marathoners, if they hydrate without replacing electrolytes lost through sweating; however, this is highly unlikely for a 10K race. Newmark SR, Toppo FR, Adams G: Fluid and electrolyte replacement in the ultramarathon runner. Am J Sports Med 1991;19:389-391.
Question 59
A 48-year-old man has recurrent right knee pain. Figure 52a shows the sagittal proton density T2-weighted MRI scan, and Figure 52b shows the sagittal T2-weighted MRI scan at the same level. The arrow is pointing to a


Explanation
Meniscal tears have many configurations and locations. The normal medial meniscus has a bow-tie configuration on the two most medial consecutive sagittal views. Toward the center of the joint the anterior and posterior horns have a triangular shape. These images show an abnormal intra-articular low-signal structure located anterior to the intact posterior cruciate ligament. This most likely represents a torn and displaced posterior horn of the medial meniscus, sometimes called "double PCL sign". A popliteal cyst and ligaments of Wrisberg and Humphry are not visible on these figures. Helms CA: MR image of the knee, in Fundamentals of Skeletal Radiology, ed 2. Philadelphia, PA, WB Saunders, 1995, pp 172-191.
Question 60
High Yield
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of

Explanation
The patient has a stable bony fracture that will heal with immobilization in a rigid collar. Flexion-extension radiographs may be obtained at 6 weeks to verify that there is no instability; mobilization may then be begun.
Question 61
A 16-year-old girl injured her hip in a fall. Radiographs are shown in Figures 14a and 14b. She denies any history of pain prior to the fall and is currently asymptomatic. A bone scan, MRI scan, and biopsy specimens are shown in Figures 14c through 14f. What is the most likely diagnosis?






Explanation
Although the classic radiographic appearance of fibrous dysplasia is one of a central metaphyseal lesion with ground glass matrix, it is not unusual to see either a more radiodense-appearing lesion or a more peripheral location. The histologic finding of spicules of woven bone without osteoblastic rimming in a bland fibrous background is diagnostic of fibrous dysplasia. The imaging studies could be consistent with low-grade osteosarcoma, osteoblastoma, or osteomyelitis, but all have a very different histologic picture. Observation is indicated in the absence of symptoms, impending fracture, or deformity. Fibrous dysplasia most commonly occurs in the proximal femur. Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 30-43.
Question 62
High Yield
A 61-year-old woman has increasing pain in her left great toe. She states that she has had discomfort for years but now has pain with all shoe wear. A radiograph is shown in Figure 35. To provide the most predictable pain-free result, treatment should consist of

Explanation
Because the patient has a hallux valgus with increased intermetatarsal and hallux valgus angles and advanced degenerative arthritis of the joint, arthrodesis of the first metatarsophalangeal joint will provide the most predictable pain-free result. An attempt to correct the bunion with a bunionectomy or osteotomy would most likely fail. The hallux valgus and advanced degenerative changes put the foot beyond the indications for a cheilectomy. Long-term results with silicone arthroplasty have been disappointing. Mann RA: Disorders of the first metatarsophalangeal joint. J Am Acad Orthop Surg 1995;3:34-43.
Question 63
A 50-year-old competitive tennis player sustained a shoulder dislocation after falling on his outstretched arm 3 weeks ago. He now reports that he has regained motion but continues to have painful elevation and weakness in external rotation. A subacromial cortisone injection provided 3 weeks of relief, but the pain has returned. Which of the following studies will best aid in diagnosis?

Explanation
Based on these findings, the most likely diagnosis is a rotator cuff injury and probable tear; therefore, MRI is the study of choice. CT is preferred for articular fractures. A bone scan is nonspecific and can identify inflammation or occult fracture. Joint aspiration is not likely to identify an effusion. Physical therapy and a functional capacity examination are used to identify weakness during recovery prior to a return to work or sports. Hawkins RJ, Bell RH, Hawkins RH, Koppert GJ: Anterior dislocation of the shoulder in the older patient. Clin Orthop 1986;206:192-195.
Question 64
A patient with refractory long head biceps pain in the shoulder undergoes biceps tenotomy. The patient is concerned about possible postoperative deformity and loss of supination strength. Which of the following techniques provides the strongest initial fixation to prevent distal migration?
Explanation
Recent articles have looked at the cyclic load failure and ultimate load failure of biceps tenodesis techniques. The interference screw has proved superior to bone tunnel, suture anchor, and soft-tissue tenodesis techniques in laboratory cadaveric testing. Whether this is clinically relevant or not is still unknown. Ozalay M, Akpinar S, Karaeminogullari O, et al: Mechanical strength of four different biceps tenodesis techniques. Arthroscopy 2005;21:992-998.
Question 65
High Yield
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
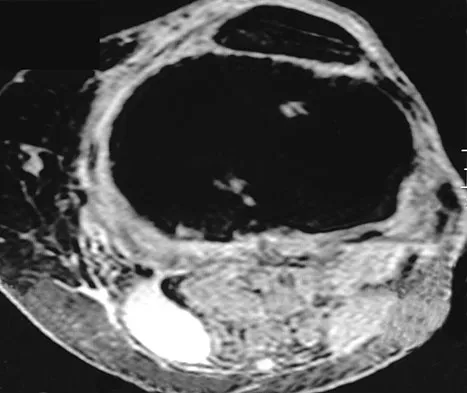
Explanation
The MRI scans show a popliteal cyst (Baker's cyst) in its most common location. The cyst emerges from the knee joint between the medial head of the gastrocnemius muscle and the tendon of the semimembranosus muscle. These images are diagnostic; therefore, no further work-up is indicated. Since the patient is asymptomatic, no treatment is necessary. Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Question 66
Following application of a short leg cast, a patient reports a complete foot drop. A compression injury of the peroneal nerve at the fibular neck is confirmed by electrical studies. Which of the following muscles is expected to be the last to recover function during the ensuing months?
Explanation
The recovery process from peroneal nerve palsy may take many months as axonal regrowth occurs. Of the muscles listed, the extensor hallucis is innervated most distally by the peroneal nerve. The flexor digitorum longus is innervated by the tibial nerve.
Question 67
A 3-year-old patient with L3 myelomeningocele has bilateral dislocated hips. Management should consist of

Explanation
In patients with myelomeningocele, the presence of bilateral hip dislocation does not affect ambulation, bracing requirements, sitting ability, degree of scoliosis, or level of comfort. There is little evidence to support active treatment of bilateral hip dislocations in patients with myelomeningocele proximal to L4. Fraser RK, Hoffman EB, Sparks LT, et al: The unstable hip and mid-lumbar myelomeningocele. J Bone Joint Surg Br 1992;74:143-146.
Question 68
High Yield
A 60-year-old patient had the procedure shown in Figure 7 performed 5 years ago. When converting this patient to a total knee arthroplasty (TKA), what patellar problem is commonly encountered intraoperatively?

Explanation
Patella baja is commonly encountered when converting a high tibial osteotomy (HTO) to a TKA. Patella baja most likely occurs because of scarring. Meding and associates' study did not show an increased rate of lateral release when converting a knee that had undergone a previous HTO. Yoshino N, Shinro T: Total knee arthroplasty after failed high tibial osteotomy, in Callaghan JJ, Rosenberg AG, Rubash HE, et al (eds): The Adult Knee. Philadelphia, PA, JB Lippincott, 2003, vol 2, pp 1265-1271.
Question 69
A 12-year-old girl sustains an acute injury to the right elbow in a fall. An AP radiograph is shown in Figure 5. Nonsurgical management will most likely result in

Explanation
The patient has a significantly displaced medial epicondyle fracture. The only absolute indication for surgical treatment is irreducible incarceration in the joint. Nonsurgical management usually results in a painless nonunion with good elbow function and little elbow instability. Prolonged immobilization should be avoided to prevent stiffness. Tardy ulnar nerve palsy and cubitus varus are not complications of medial epicondyle fractures. Chamber HG, Wilkins KE: Part IV: Apophyseal injuries of the distal humerus, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 801-812.
Question 70
Figures 2a and 2b show the radiographs of a 72-year-old man with aseptic loosening of the tibial component of his total knee arthroplasty. Optimal management should include


Explanation
The radiographs show massive subsidence of the lateral side of the tibia with severe tibial bone loss and a fractured proximal fibula. Reconstruction should consist of a large metal or bony lateral tibial augmentation, and a stem long enough to bypass the defect is required. The femoral and tibial components are articulating without any remaining polyethylene medially; therefore, the femoral component is damaged and needs revision. The insertions of the lateral ligaments are absent, thereby rendering the lateral side of the knee predictably unstable. Also, the large valgus deformity compromises the medial collateral ligament. The posterior cruciate ligament is also likely to be deficient with this much tibial bone destruction. The patient requires a posterior stabilized femoral component at the minimum, and possibly a constrained femoral component. Retention of the femoral component, even though it may be well-fixed, jeopardizes the outcome. Lotke PA, Garino JP: Revision Total Knee Arthroplasty. New York, NY, Lippincott-Raven, 1999, pp 137-250. Insall JN, Windsor RE, Scott WN, et al: (eds): Surgery of the Knee, ed 2. New York, NY, Churchill Livingstone, 1993, pp 935-957.
Question 71
High Yield
An eversion mechanism of injury is associated with which of the following ankle conditions?
Detailed Explanation
An inversion ankle injury typically involves ligamentous damage to the lateral ligaments of the ankle to include the anterior talofibular ligament and calcaneofibular ligament. Acute and particularly chronic ankle sprains also can have associated injuries. The inversion mechanism has been implicated in osteochondral and transchondral talar dome lesions, producing splits in the peroneus tendons, and in the development of meniscoid and soft-tissue impingement lesions in the anterolateral ankle. An inversion mechanism can also stretch the superficial peroneal nerve, leading to pain and paresthesias along its distribution. A fracture of the anterior colliculus is typically the result of an eversion mechanism resulting in a bony avulsion of the deltoid ligament from the anterior colliculus of the medial malleolus. Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Question 72
What neurovascular structure is in closest proximity to the probe in the arthroscopic view of the elbow shown in Figure 50?

Explanation
The image shows a view of the radiocapitellar joint from an anterior medial portal. The radial nerve lies on the elbow capsule at the midportion of the capitellum. It is at risk for injury when capsular excision is performed in this region. Field LD, Altchek DW, Warren RF, et al: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 73
A patient sustained a sharp laceration to the base of his left, nondominant thumb 4 months ago. Examination reveals no active flexion but full passive motion of the interphalangeal joint. What is the best treatment option?

Explanation
The patient has a chronic flexor tendon laceration. There are options to restore motion and strength; therefore, fusion is not necessary. Full range of motion is present so the soft tissues are suitable for a tendon transfer. A transfer of the flexor digitorum superficialis of the ring finger to the insertion of the flexor pollicis longus on the distal phalanx provides good results with a one-stage operation. Schneider LH, Wiltshire D: Restoration of flexor pollicis longus function by flexor digitorum superficialis transfer. J Hand Surg Am 1983;8:98-101.
Question 74
The spread of malignant cells to the vertebrae is often through
Explanation
In 1940, Batson described a valveless plexus of veins that extend from the dural venous sinuses of the skull to the sacrum. This system permits retrograde blood flow and enables tumor cells to enter vertebral bodies at multiple levels. Increased intra-abdominal pressure will enhance this retrograde blood flow.
Question 75
High Yield
Iliosacral screws placed for stabilization of posterior pelvic ring injuries (eg, sacroiliac dislocation) that exit the sacrum anteriorly are most likely to injure which of the following structures?
Explanation
Iliosacral screws have gained popularity for posterior stabilization of pelvic ring disruptions, but complications attributed to incorrect placement are a clinical problem. The L5 nerve root is at greatest risk and is in closest proximity to a malpositioned screw (exiting the sacrum). The L4 root is more anterior at this level. The S1 root is still intraosseous at this level and is at risk but not from the screw exiting anteriorly at this level. The arteries are at risk but are more anterior and are at less risk than the L5 nerve root.
Question 76
High Yield
A 35-year-old female runner reports progressive vague aching pain involving her midfoot. Her pain is most notable when running. She denies specific injury. Examination reveals minimal swelling and localized tenderness over the dorsal medial midfoot and navicular. Radiographs and an MRI scan are shown in Figures 37a through 37c. What is the most appropriate management?



Detailed Explanation
A high index of suspicion is required to identify a possible navicular stress fracture, especially in runners. High pain tolerance in the competitive athlete and often minimal swelling contribute to frequent delays in diagnosis. Localized tenderness over the dorsal navicular (so-called "N spot") in a running athlete should alert the treating physician. In this patient, the radiographs are negative and the MRI scan shows marrow edema within the navicular. This could represent a stress reaction, stress fracture, or osteonecrosis. Appropriate management should include non-weight-bearing immobilization and obtaining a CT scan to determine if a fracture is present. Early surgical treatment may be considered but only if a fracture is identified. Lee A, Anderson R: Stress fractures of the tarsal navicular. Foot Ankle Clin 2004;9:85-104.
Question 77
High Yield
An otherwise healthy 33-year-old man who works in construction reports a 3-month history of knee pain. Radiographs are shown in Figures 9a and 9b. An axial T1-weighted MRI scan with contrast, an angiogram, and histologies are shown in Figures 9c through 9f. What is the most likely diagnosis?


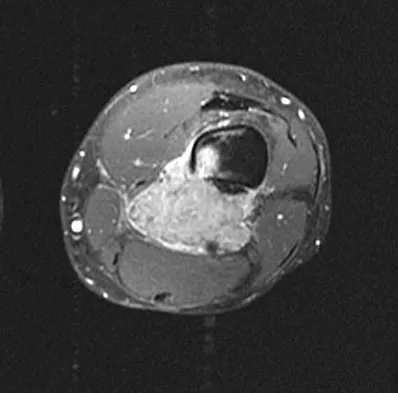
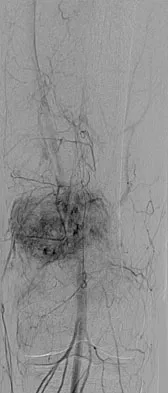
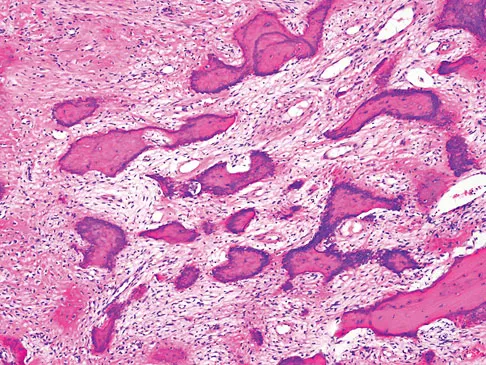
Explanation
Dedifferentiated parosteal osteosarcoma designates high-grade transformation of conventional low-grade parosteal osteosarcoma. Unlike conventional parosteal osteosarcoma, where wide surgical excision alone is considered adequate treatment, patients with dedifferentiated osteosarcoma are treated with neoadjuvant chemotherapy and wide local resection. Recognition of dedifferentiated areas with angiography can localize the area that should be biopsied and thus render an accurate diagnosis. Percutaneous biopsy of hypervascular areas should prompt the administration of chemotherapy and wide local excision to optimize patient outcome. Sheth DS, Yasko AW, Raymond AK, et al: Conventional and dedifferentiated parosteal osteosarcoma: Diagnosis, treatment, and outcome. Cancer 1996;78:2136-2145.
Question 78
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
If a Cobb elevator is directed caudally while stripping the periosteum over the iliac wing, it will encounter the sciatic notch. Although this puts the sciatic nerve at risk, the first structure encountered is the superior gluteal artery. Because it is tethered at the superior edge of the notch, it is very vulnerable to injury and can then retract inside the pelvis, making it difficult to obtain hemostasis. The inferior gluteal artery exits the sciatic notch below the piriformis and is more protected. The cluneal nerves are at risk only if the incision extends too anteriorly, and the sacroiliac joint can be entered while harvesting the graft. Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Question 79
A 22-year-old man who sustained a Gustilo-Anderson grade IIIC open fracture of the right tibia and fibula was treated with an immediate open transtibial amputation. After two serial debridements, he underwent wound closure with a posterior myocutaneous soft-tissue flap. What is the preferred method of early rehabilitation?

Explanation
There is no evidence that early weight bearing enhances ultimate rehabilitation. At the other extreme, weight bearing should not be delayed for a prolonged period of time. In a young, healthy individual, the rigid plaster dressing appears to be the safest method of protecting the wound during the early postoperative period. If the wound appears to be secure, early partial weight bearing can be safely initiated. Burgess EM, Romano RL, Zettl JH: The Management of Lower Extremity Amputations. Washington, DC, US Government Printing Office, 1969, also at: www.prs-research.org.
Question 80
High Yield
What risk factor is most associated with progression of idiopathic scoliosis to a curve requiring surgery?

Explanation
The magnitude of the curve at the time of the peak height velocity is the most prognostic sign in relationship to surgery. More than 70% of curves that measure more than 30 degrees at this time are likely to reach surgical range. Little DG, Song KM, Katz D, et al: Relationship of peak height velocity to other maturity indicators in idiopathic scoliosis in girls. J Bone Joint Surg Am 2000;82:685-693.
Question 81
What is the recommended insertion torque for halo pins in adults?

Explanation
Garfin and associates have shown that halo pins inserted with 8 in-lb of insertion torque results in significantly less loosening with cyclical loading than pins inserted with 6 in-lb of torque. Moreover, Botte and associates reported that 8 in-lb of torque is clinically safe and effective in lowering the incidence of pin loosening and infection. Botte MJ, Byrne TP, Garfin SR: Application of the halo device for immobilization of the cervical spine utilizing an increased torque pressure. J Bone Joint Surg Am 1987;69:750-752. Garfin SR, Lee TO, Roux RD, et al: Structural behavior of the halo orthosis pin-bone interface: Biomechanical evaluation of standard and newly designed stainless steel halo fixation pins. Spine 1986;11:977-981.
Question 82
A 7-year-old boy sustained a head contusion and small bowel injuries in a motor vehicle accident in which he was wearing a lap belt. He subsequently required a bowel resection. Six weeks after the accident, his parents note a painful mass in his lower back. His neurologic examination is normal. A radiograph and CT scans are shown in Figures 47a through 47c. Definitive management should now consist of



Explanation
The posttraumatic lumbar kyphotic deformity will not remodel and is likely to worsen with time because the central line of gravity lies anterior to the deformity and the ligamentous disruption will not heal. The worsening deformity also puts the patient at some risk for future neurologic damage. Ebraheim NA, Savolain ER, Southworth SR, et al: Pediatric lumbar seat belt injuries. Orthopedics 1991;14:1010-1013.
Question 83
A 67-year-old man is requesting revision surgery because of continued pain in the knee after undergoing a total knee replacement 2 years ago. Examination reveals that the knee is not warm, the incision is well-healed, and the skin has normal coloration and hair formation. No varus or valgus instability is noted, and knee range of motion is 5 degrees to 100 degrees. Laboratory studies show an erythrocyte sedimentation rate of 15 mm/h and a WBC of 5,000/mm3. Aspiration of the knee reveals clear fluid that shows no growth on culture. Radiographs reveal an appropriately positioned cruciate-retaining cemented total knee arthroplasty that is well-fixed. What is the probability that the patient's pain will be improved with revision surgery?

Explanation
The patient has a well-fixed and aligned painful total knee replacement. The success rate of revision knee replacement for pain when no mechanical problem can be identified is approximately 40%. The critical step is to rule out the presence of infection with appropriate laboratory studies and aspiration. If no infection is detected, revision should be avoided. Rand JA: Planning for revision total knee arthroplasty, in Zuckerman JD (ed): Instructional Course Lectures 48. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 161-166.
Question 84
A 20-year-old man with fascioscapulohumeral dystrophy has severe scapular winging of both shoulders. He can no longer abduct above 80 degrees, and it affects his activities of daily living. A clinical photograph is shown in Figure 26. Definitive management should consist of

Explanation
The patient's history is typical of patients with severe fascioscapulohumeral dystrophy. The scapular winging can be so pronounced that there is significant loss of function of the upper extremity. The surgical options include transfer of the pectoralis major muscle with a tendon graft or scapulothoracic fusion. The latter is a technically demanding procedure but can provide a very stable platform for the upper extremity. Most patients will see increased elevation of the extremity once the scapula is stabilized. Pectoralis minor transfer has not been described and would not be effective. Shapiro F, Specht L: The diagnosis and orthopaedic treatment of inherited muscular diseases of childhood. J Bone Joint Surg Am 1993;75:439-454.
Question 85
A 30-year-old woman sustained a nondisplaced unilateral facet fracture of C5 in a motor vehicle accident. She is neurologically intact and has no other injuries. Management should consist of

Explanation
The patient has a stable bony fracture that will heal with immobilization in a rigid collar. Flexion-extension radiographs may be obtained at 6 weeks to verify that there is no instability; mobilization may then be begun.
Question 86
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of

Explanation
In a subgroup of patients with monoarticular JRA and a limb-length discrepancy that developed before the age of 9 years, Simon and associates showed that a subsequent growth deceleration on the affected side may correct a large part of the difference in length. This possibility would make surgery unnecessary and should prompt further observation. Simon S, Whiffen J, Shapiro F: Leg-length discrepancies in monoarticular and pauciarticular juvenile rheumatoid arthritis. J Bone Joint Surg Am 1981;63:209-215.
Question 87
High Yield
A patient who underwent open reduction and internal fixation of an olecranon fracture 2 months ago now reports painless limitation of motion. Examination reveals a well-healed incision and a flexion-extension arc from 40 degrees to 80 degrees. The patient has been performing home exercises. Radiographs are shown in Figures 26a and 26b. What is the most appropriate treatment?


Explanation
The radiographs do not show an articular malunion. Treatment is directed at the soft-tissue contracture and should begin with formal physical therapy and static progressive splinting. Radiation therapy is effective in the perioperative period and is indicated when ectopic bone formation is a concern. Morrey BF: The posttraumatic stiff elbow. Clin Orthop Relat Res 2005;431:26-35.
Question 88
A 22-year-old woman injures her neck in a motor vehicle accident. Examination reveals no sensory or motor function below T8. Radiographs and an MRI scan show a burst fracture at T7. Forty-eight hours later, the bulbocavernosus reflex is present but there is no evidence of motor or sensory recovery in the lower extremities. What is the most likely diagnosis?

Explanation
Spinal shock typically ends after 48 hours with the return of reflexes, including the bulbocavernosus reflex. Lack of motor or sensory recovery in the lower extremities with the return of reflexes generally indicates a complete cord syndrome. Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Question 89
A 20-year-old college pitcher reports medial elbow pain after 3 innings of hard throwing. He recalls no injury and reports no pain with light throwing. The examination shown in the clinical photograph in Figure 48 reproduces the elbow pain. What is the most likely diagnosis?

Explanation
The milking test, as seen in the photograph, elicits pain when a tear is present in the medial collateral ligament. Complete rupture is possible but unlikely when there is no history of trauma and the patient is able to throw pain-free for several innings. Subluxation of the ulnar nerve and triceps tendon subluxation present as a painful snapping over the medial aspect of the elbow. Williams RJ III, Urquhart ER, Altchek DW: Medial collateral ligament tears in the throwing athlete. Instr Course Lect 2004;53:579-586.
Question 90
Figures 26a through 26c show the MRI scans of a 47-year-old man who underwent arthroscopic shoulder surgery 6 months ago and continues to have pain despite a prolonged course of rehabilitation. Management should now consist of



Explanation
The MRI scans show an os acromiale of the mesoacromion type. This represents an unfused acromial apophysis. Pain is thought to be caused by either motion at the site or downward displacement of the anterior aspect of the acromion onto the rotator cuff, causing impingement. Most patients can be treated nonsurgically as they are usually asymptomatic. In those patients with persistent symptoms of pain and tenderness over the acromion, surgery consisting of rigid internal fixation and bone grafting has yielded satisfactory results. Excision may be a viable treatment option for the preacromion type. Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20. Warner JP, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 91
High Yield
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include

Detailed Explanation
The patient has a displaced radial neck fracture. Displaced radial neck fractures with angulation of more than 30 to 45 degrees require reduction. Methods of attempted closed reduction include wrapping the arm with an Esmarch's bandage and applying direct pressure over the maximum deformity of the radial head. More aggressive methods include a Kirschner wire used as a joystick or intramedullary reduction as described by the Metaizeau technique. Open reduction should be avoided because of complications such as stiffness or osteonecrosis. Indications for open reduction are irreducible displacement of more than 45 degrees with severe restriction of forearm rotation. Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop 2000;20:7-14. Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39. Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Question 92
Figures 34a and 34b show the clinical photograph and a weight-bearing radiograph of a patient with diabetes mellitus who has had recurrent ulcers under the head of the talus that have previously resolved with a series of non-weight-bearing total contact casts. The deformity does not correct passively. Dorsalis pedis and posterior tibial pulses are palpable. The patient is insensate to the Semmes-Weinstein 5.07 (10 gm) monofilament. The ulcer is currently healed. What is the best option to prevent recurrent ulceration and infection?


Explanation
This is a nonplantigrade deformity in a patient with a Charcot foot deformity. Longitudinal studies have shown that recurrent ulceration/infection is likely unless the deformity is corrected. Achilles tendon lengthening is advised for simple forefoot ulcers. The current approach to this problem is best managed with surgical correction of the deformity, Achilles tendon lengthening, and therapeutic footwear. Bevan WP, Tomlinson MP: Radiographic measures as a predictor of ulcer formation in diabetic charcot midfoot. Foot Ank Int 2008;29:568-573. Simon SR, Tejwani SG, Wilson DL, et al: Arthrodesis as an early alternative to nonoperative management of Charcot arthropathy of the diabetic foot. J Bone Joint Surg Am 2000;82:939-950.
Question 93
High Yield
After making a tackle, a football player is found prone and unconscious without spontaneous respirations. Initial management should consist of

Explanation
The on-field evaluation and management of a seriously injured athlete requires that health care teams have a game plan in place and proper equipment that is readily available. The initial step, which consists of stabilizing the head and neck by manually holding them in a neutral position, is then followed by assessment of breathing, pulses, and level of consciousness. If the athlete is breathing, management should consist of mouth guard removal and airway maintenance. If the athlete is not breathing, the face mask should be removed, with the chin strap left in place. The airway must be established, followed by initiation of assisted breathing. CPR is instituted only when breathing and circulation are compromised. In the unconscious athlete or if a cervical spine injury is suspected, the helmet must not be removed until the athlete has been transported to an appropriate facility and the cervical spine has been completely evaluated. McSwain NE, Garnelli, RL: Helmet removal from injured patients. Bull of Am Coll Surg 1997;82:42-44.
Question 94
High Yield
A 35-year-old man is seen for evaluation of his left ankle following multiple previous ankle sprains and frequent episodes of the ankle giving way. Examination reveals marked laxity about the lateral ankle with associated tenderness along the peroneal tendons. Physical therapy, anti-inflammatory drugs, and supportive bracing have failed to provide relief. An MRI scan shows peroneal tenosynovitis and a possible tear. He elects to undergo a peroneal tendon repair and lateral ligament reconstruction. Which of the following best describes the structure labeled "A" in Figure 45?
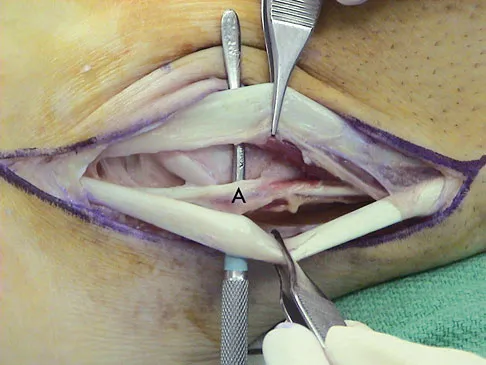
Explanation
The structure labeled "A" is a peroneus quartus, a supernumary muscle arising most commonly from the peroneus brevis. The presence of peroneus quartus is not uncommon, with an incidence of up to 21%, and is associated with lateral ankle pain and peroneal tendon symptoms, theoretically as a result of mass effect within the peroneal tendon sheath. Zammit J, Singh D: The peroneus quartus muscle: Anatomy and clinical relevance. J Bone Joint Surg Br 2003;85:1134-1137.
Question 95
A 78-year-old woman falls onto her nondominant left elbow and sustains the injury shown in Figure 5. What treatment option allows her the shortest recovery time and highest likelihood of good function and range of motion?

Explanation
Total elbow arthroplasty has become the treatment of choice for complex, comminuted distal humeral fractures in patients older than age 70 years. It yields a faster recovery with more predictable functional outcomes, although limitations of lifting weight of more than 5 pounds must be followed to avoid loosening. Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement. J Bone Joint Surg Am 2004;86:940-947.
Question 96
What fibers of the anterior cruciate ligament tighten with extension of the knee?
Explanation
The anterior cruciate ligament consists of two functional bundles: anteromedial and posterolateral. During extension of the knee, the posterolateral bundle becomes taut. In flexion, the anteromedial bundle is tight and the posterolateral bundle relaxes. Traditionally, anterior cruciate ligament reconstruction primarily recreates the anteromedial bundle. Recently, techniques for double bundle reconstruction have been described to recreate the normal anatomic relationship of the two bundles. Girgis FG, Marshall JL, Monajem AS: The cruciate ligaments of the knee joint: Anatomical, functional and experimental analysis. Clin Orthop Relat Res 1975;106:216-231. Cha PS, Brucker PU, West RV, et al: Arthroscopic double-bundle anterior cruciate ligament reconstruction: An anatomic approach. Arthroscopy 2005;21:1275.
Question 97
High Yield
Which of the following benign bone lesions can develop lung metastases?
Explanation
Although considered benign bone lesions, lung metastases can develop in giant cell tumors and chondroblastomas. These often can be treated with multiple thoracotomies, resulting in long-term survival. Roberts PF, Taylor JG: Multifocal benign chondroblastomas: Report of a case. Hum Pathol 1980;11:296-298.
Question 98
A 51-year-old woman is seen for evaluation of chronic supraspinatus and infraspinatus tendon tears. Three years ago, in an attempted repair the surgeon was unable to repair the supraspinatus and infraspinatus tendon tears. Currently she has a marked amount of pain, reduced range of motion, and weakness. Examination reveals anterosuperior escape. Radiographs show no signs of arthritic changes. You are considering a latissimus dorsi tendon transfer. During the discussion, you mention that
Explanation
Latissimus dorsi tendon transfer is considered a surgical option for treatment in patients with chronic supraspinatus and infraspinatus tendon tears. Preoperative subscapularis function is necessary for good clinical results. Additionally, men with active elevation to shoulder level and active external rotation to 20 degrees have predictably good results. Women with active shoulder elevation limited to below chest level have poor results from this procedure and should not be considered candidates. Postoperatively they lack pain control, active elevation, and active external rotation. Muscular atrophy in the latissimus dorsi does not occur, and glenohumeral arthritic changes frequently develop postoperatively. Gerber C, Maquieira G, Espinosa N: Latissimus dorsi transfer for the treatment of irreparable rotator cuff tears: Factors affecting outcome. J Bone Joint Surg Am 2006;88:113-120.
Question 99
High Yield
A 20-year-old soccer player who collapsed after a goal kick reports weakness and nausea. He appears slightly confused. Examination reveals that he is not sweating. His skin is warm and dry. The outdoor temperature is 80 degrees F (26.6 degrees C) with a relative humidity of 80%. Management should consist of
Explanation
There is a spectrum of heat-related conditions. Heat cramps are the mildest form of heat illness. In heat exhaustion, cramps are associated with headache and weakness, and the skin is pale and moist. Treatment of heat cramps or heat exhaustion consists of removing and loosening excess clothing, applying ice to the axilla and groin, ingestion of cool water, and cool water sprays. This patient demonstrates symptoms of heat stroke which is a medical emergency. The core body temperature may be as high as 106 to 110 degrees F (41.1 to 43.3 degrees C). In heat stroke, the patient may no longer be sweating, and the skin may be hot and red. The athlete is usually confused, weak, nauseated, and may have seizure activity. Central nervous system depression has been called the most important marker of heat stroke, and progresses from confusion and bizarre behavior to collapse, delirium, and coma. Bizarre behavior is often the first sign of heat stroke. The patient needs to be treated and moved to a medical facility rapidly. During transfer, IV fluids and cooling of the athlete should be initiated. The best treatment of heat-related illness appears to be prevention with adequate hydration and monitoring of conditions (temperature and humidity), with cancellation of competition when conditions do not comply with guidelines. Griffin LY: Emergency preparedness: Things to consider before the game starts. J Bone Joint Surg Am 2005;87:894-902. Barker TA, Motz HA, Gersoff WK: Environmental factors in athletic performance, in Fu FH, Stone DA (eds): Sports Injuries, ed 2. Philadelphia, PA, Lippincott, 2001, pp 67-68.
Question 100
Figure 28 shows the radiograph of a 6-year-old girl who has a right thoracic scoliosis that measures 60 degrees. Examination shows multiple cafe-au-lait spots, and family history reveals that the child's mother has the same disorder. The gene responsible for this disorder codes for

Explanation
The patient has the dystrophic type of scoliosis seen in patients with neurofibromatosis type I (NF-1). The NF-1 gene is located on chromosome 17 and codes for neurofibromin, believed to be a tumor-suppresser gene. Abnormalities in the dystrophin gene are seen in Duchenne muscular dystrophy and Becker muscular dystrophy. A mutation in the frataxin gene is responsible for Friedreich ataxia. The most common type of hereditary motor and sensory neuropathy (Charcot-Marie-Tooth), HMSN type IA is caused by a complete duplication of the peripheral myelin protein gene. A defect in the cellular sulfate transport protein results in undersulfation of proteoglycans seen in diastrophic dysplasia.
