Orthopedic Board Review MCQs: Spine, Trauma, Shoulder & Knee | Part 162

Key Takeaway
This page offers Part 162 of an interactive MCQ bank designed for orthopedic surgeons and residents. Featuring 100 high-yield questions modelled on OITE and AAOS exams, it provides comprehensive board review in Study and Exam modes to effectively prepare users for ABOS certification.
About This Board Review Set
This is Part 162 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 162
This module focuses heavily on: Dislocation, Foot, Fracture, Knee, Revision, Scoliosis, Shoulder, Spine, Trauma.
Sample Questions from This Set
Sample Question 1: -A 14-year-old girl has idiopathic scoliosis with a 52-degree right thoracic curve and a 36-degree left lumbar curve. The rotation of the apical vertebra appears greater in the thoracic curve. A sagittal view radiograph shows the spine to b...
Sample Question 2: A 12½-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full...
Sample Question 3: A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?...
Sample Question 4: Figure 2a shows the radiograph of a 48-year-old man who was involved in a motorcycle accident. A CT scan is shown in Figure 2b. The patient underwent pelvic angiography for persistent hypotension despite resuscitation. What vessel is most l...
Sample Question 5: A 17-year-old high school football player sustains a traumatic anterior shoulder dislocation, resulting in a small bony Bankart lesion and small Hill-Sachs lesion. The patient undergoes an arthroscopic Bankart repair with incorporation of t...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
- A 14-year-old girl has idiopathic scoliosis with a 52-degree right thoracic curve and a 36-degree left lumbar curve. The rotation of the apical vertebra appears greater in the thoracic curve. A sagittal view radiograph shows the spine to be virtually straight. The iliac apophyses are Risser 2. Treatment should consist of
Explanation
Question 2
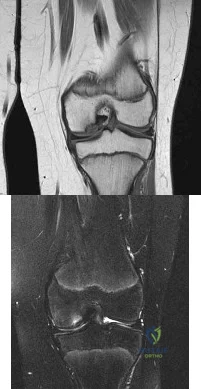
A 12½-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full range of motion without effusion. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI scans are shown in Figures 14a and 14b. Initial treatment should consist of Review Topic
Explanation
Cessation of sport activities for 4 to 6 months may allow healing of the lesion. Surgical treatment of juvenile OCD lesions is reserved for unstable lesions, patients
who have not shown radiographic evidence of healing and are still symptomatic after
6 months of nonsurgical management, or patients who are approaching skeletal maturity. Good results with stable in situ lesions that have failed to respond to nonsurgical management have been reported with both transarticular and retroarticular drilling. Results after excision alone are poor at 5-year follow-up, and it is unclear if microfracture will improve the long-term outcome. Mosaicplasty may be the next best option for patients who remain or become symptomatic after excision of the fragment and microfracture.
Wall et al. reviewed juvenile OCD. They state that JOCD has better potential for healing than adult OCD, but several series have shown up to a 50% failure to heal with nonsurgical techniques. The presence of a loose body is an indication for surgical fixation, drilling or regenerative procedures, depending on the presence/extent of subchondral bone sclerosis and the surgeon's experience.
Figure A and B are coronal MRI images showing a stable appearing JOCD lesion of the medial femoral condyle.
Incorrect
in the first
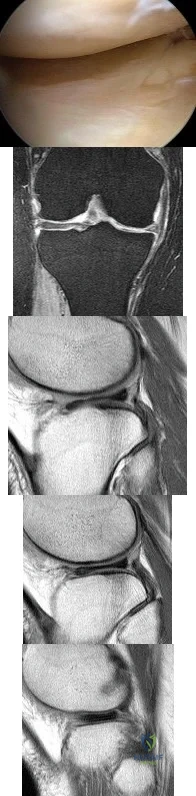
(SBQ13PE.9) A 6-year-old boy complains of a 'clunking' sensation in his left knee. He has no associated pain and denies trauma. He can elicit the sensation when moving his knee from flexion into full extension. He is otherwise healthy, with no birth or developmental issues. On examination, there is a palpable clunk felt over the anterior knee through range of motion. There is no obvious instability or tenderness and he had normal patellar tracking. An AP radiograph of the knee is shown in Figure A. What would be the most likely diagnosis? Review Topic

Agenesis of the anterior cruciate ligament
Thickened medial plica
Grade IV chondral flap
Pigmented villonodular synovitis
Abnormal meniscal morphology
This child presents with an asymptomatic click in the knee. It is associated with widening of the lateral joint space of the knee on X-ray. These features are highly suggestive of a discoid lateral meniscus in this age category.
The principal diagnostic feature of a discoid meniscus is the complaint of snapping or clicking in the knee. Children are usually asymptomatic. Although, less frequently, children may present with pain that is largely secondary to an underlying meniscal tear. MRI scans of the knee have show to have the greatest sensitivity for identifying discoid menisci. The presence of a contiguous central meniscus on three consecutive slices is usually indicative of the diagnosis. Treatment is mostly focused on conservative modalities. Surgical intervention is reserved for symptomatic cases with recurrent locking, swelling or persistent pain is present in older children.
Kramer et al. looked at the presentation of pediatric knee pain. They showed that the lateral meniscus is more commonly affected than the medial meniscus. The majority of discoid tears occur in the posterior or middle aspect of the discoid meniscus.
Figure A shows an AP radiograph of a pediatric knee. There is an increased lateral joint space suggestive of a discoid meniscus.
Illustrations A-C show an MRI of the knee with 3 consecutive coronal cuts showing an abnormal appearing discoid meniscus.
Incorrect Answers:
Question 3
A 56-year-old woman sustained the fracture shown in Figures 30a and 30b in a motor vehicle accident. What mechanism is most likely responsible for the injury?
Explanation
REFERENCES: Theiss SM: Thoracolumbar and lumbar spine trauma, in Stannard JP, Schmidt AH, Kregor PJ (eds): Surgical Treatment of Orthopaedic Trauma. New York, NY, Thieme, 2007, pp 179-207.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
Question 4
Figure 2a shows the radiograph of a 48-year-old man who was involved in a motorcycle accident. A CT scan is shown in Figure 2b. The patient underwent pelvic angiography for persistent hypotension despite resuscitation. What vessel is most likely to be injured?
Explanation
REFERENCES: O’Neill PA, Riina J, Sclafani S, et al: Angiographic findings in pelvic fractures. Clin Orthop 1996;329:60-67.
Belley G, Gallix BP, Derossis AM, et al: Profound hypotension in blunt trauma associated with superior gluteal artery rupture without pelvic fracture. J Trauma 1997;43:703-705.
Question 5
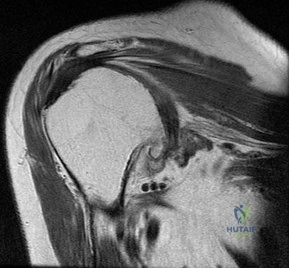
A 17-year-old high school football player sustains a traumatic anterior shoulder dislocation, resulting in a small bony Bankart lesion and small Hill-Sachs lesion. The patient undergoes an arthroscopic Bankart repair with incorporation of the bone fragment and returns to play football the following year. He has a recurrent dislocation at football practice but decides to finish the football season before considering additional treatment. He sustains nine additional dislocations, with the last dislocation occurring while sleeping.What diagnostic test is most appropriate when planning revision surgery?
Explanation
more likely to have pain after surgery. Age and activity level are lesser influences on satisfaction.
Question 6
A 35-year-old laborer who sustained a forefoot injury 10 years ago has returned to work but reports a progressively painful deformity of the hallux and continued midfoot pain that is aggravated by weight-bearing activities. Shoe wear modifications have failed to provide relief. Direct palpation reveals no pain at the first metatarsocuneiform joint. A radiograph is shown in Figure 11. What is the next most appropriate step in management?
Explanation
REFERENCES: Kitaoka HB, Patzer GL: Arthrodesis versus resection arthroplasty for failed hallux valgus operations. Clin Orthop 1998;347:208-214.
McGarvey WC, Braly WG: Bone graft in hindfoot arthrodesis: Allograft vs autograft. Orthopedics 1996;19:389-394.
Ouzounian TJ: Metatarsophalangeal arthrodesis for salvage of failed hallux valgus surgery. Foot Ankle Clin 1997;2:741-752.
Question 7
A 25-year-old man is brought to the emergency department following a motor vehicle accident. Extrication time was 2 hours, and in the field he had a systolic blood pressure by palpation of 90 mm Hg. Intravenous therapy was started, and on arrival in the emergency department he has a systolic blood pressure of 90 mm Hg with a pulse rate of 130. Examination reveals a flail chest and a femoral diaphyseal fracture. Ultrasound of the abdomen is positive. The trauma surgeons take him to the operating room for an exploratory laparotomy. At the conclusion of the procedure, he has a systolic pressure of 100 mm Hg with a pulse rate of 110. Oxygen saturation is 90% on 100% oxygen, and he has a temperature of 95.0° F (35° C). What is the recommended treatment of the femoral fracture at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopaedic surgery. J Trauma 2002;53:452-461.
Bosse M, Kellam JF: Orthopaedic decision making in the multiple trauma patient, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 133-146.
Question 8
Figures 15a through 15d
Explanation
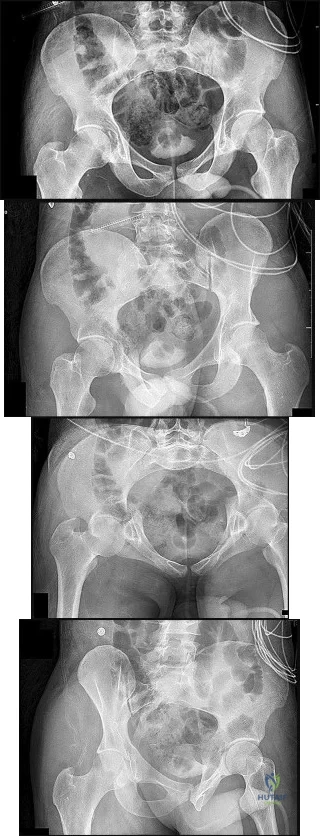
Plain radiographic imaging of a patient with an acetabular injury begins with 5 standard views of the pelvis (anteroposterior [AP], iliac oblique, obturator oblique, inlet, and outlet views). These views will show fractures of the acetabulum and help to evaluate for pelvic fractures and hip joint integrity. The obturator oblique view is taken with the injured side rotated 45 degrees forward with the beam centered on the patient’s affected hip. This shows the anterior column and posterior wall and will reveal if any posterior subluxation of the hip is present. The iliac oblique view is taken with the injured side of the patient rolled 45 degrees forward with the beam centered on the affected hip. This shows the posterior column and the anterior wall. Inlet and outlet pelvic radiographs may depict pelvic injuries such as sacroiliac joint fracture or widening.
Judet and Letournel have a classification system for acetabular fractures. The system consists of 5 elementary fracture patterns: anterior wall, anterior column, posterior wall, and posterior column fractures of the acetabulum and a transverse pattern. There are also 5 associated fracture patterns: posterior column/posterior wall, transverse/posterior wall, T-type, anterior column with hemitransverse fracture of the posterior column, and both-column fractures.
Figure 12b shows a fracture of the posterior column on the Iliac oblique, and Figure 12c shows a fracture of the posterior wall in the obturator oblique.
In Question 13, the figures only reveal a fracture of the posterior wall, and this is best appreciated in Figure 13c, the obturator oblique view.
The T-type fracture is a transverse fracture with a secondary fracture line extending inferiorly. This causes the anterior and posterior columns to be separated. The iliac oblique view, Figure 14b, shows a fracture extending through the posterior column. In the obturator oblique view (Figure 14c), the yellow arrow shows a fracture extending through the anterior column, and the red arrow shows a fracture extending inferiorly through the ischium.
Fractures extending through the anterior and posterior columns are seen, which represent a transverse fracture, but there is no extension inferiorly, which eliminates T-type as a possible correct response. The anterior column fracture is best seen on the inlet view (Figure 15b), but it also can be seen in Figure 15d, the obturator oblique view. Figure 15c shows the fracture through the posterior column. For this patient, a small fracture of the posterior wall is visualized on the AP view (Figure 15a).
RECOMMENDED READINGS
Dickson KF, Dowling RM. Treatment of pelvic and acetabular fractures in elderly patients. Orthopaedic Knowledge Online Journal. Volume 11, Number 8 August 2013.
Tornetta P 3rd. Displaced acetabular fractures: indications for operative and nonoperative management. J Am Acad Orthop Surg. 2001 Jan-Feb;9(1):18-28. Review. PubMed PMID: 11174160. View Abstract at PubMed
Moed BR, Kregor PJ, Reilly MC, Stover MD, Vrahas MS. Current management of posterior wall fractures of the acetabulum. Instr Course Lect. 2015;64:139-59. Review. PubMed PMID: 25745901. View Abstract at PubMed
Question 9
A 58-year-old woman with rheumatoid arthritis has progressive neck pain, upper extremity and lower extremity weakness, and difficulty with fine motor movements. Examination reveals hyperreflexia with mild to moderate objective weakness but the patient has no difficulty with ambulation for short distances. What is the most important preoperative imaging finding that predicts full neurologic recovery with surgical stabilization?
Explanation
REFERENCES: Boden SD, Dodge LD, Bohlman HH, et al: Rheumatoid arthritis of the cervical spine: A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
Boden SD, Clark CR: Rheumatoid arthritis of the cervical spine, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, pp 755-764.
Monsey RD: Rheumatoid arthritis of the cervical spine. J Am Acad Orthop Surg 1997;5:240-248.
Question 10
What is the best initial screening test for a patient with a limb-length discrepancy?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002, pp 1041-1045.
Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1120-1122.
Stanitski DF: Limb-length inequality: Assessment and treatment options. J Am Acad Orthop Surg 1999;7:143-153.
Aaron A, Weinstein D, Thickman D, Eilert R: Comparison of orthoroentgenography and computed tomography in the measurement of limb-length discrepancy. J Bone Joint Surg Am 1992;74:897-902.
Question 11
A 64-year-old woman has left wrist pain and deformity after falling on her hand. Examination shows intact skin and no neurologic or vascular injuries. Radiographs are shown in Figures 43a and 43b. What is the most appropriate management for the injury?
Explanation
REFERENCE: Cohen M, McMurtry RY, Jupiter JB: Fractures and dislocations of the carpus, in Browner BD (ed): Skeletal Trauma, ed 3. Philadelphia, PA, WB Saunders, 2003, pp 1328-1335.
Question 12
Figure 11a shows the AP pelvis radiograph of a 25-year-old man who sustained a spinal cord injury 10 years ago. A bone scan and a CT scan are shown in Figures 11b and 11c. To prevent recurrence after resection, management should consist of
Explanation
REFERENCES: Moore K, Goss K, Anglen J: Indomethacin versus radiation therapy for prophylaxis against heterotopic ossification in acetabular fracture. J Bone Joint Surg Br 1998;80:259.
Stover S, Niemann K, Tullos J: Experience with surgical resection of heterotopic bone in spinal cord injury patients. Clin Orthop 1991;263:71-77.
Question 13
Figure 28 shows an arthroscopic view of a right shoulder in the lateral position through a posterior portal. What is the area between structure B (biceps) and SS (subscapularis tendon)? Review Topic
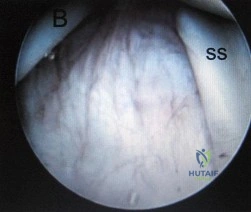
Explanation
Question 14
Figure 18a shows the clinical photograph of a 2-year old boy who has a deformity of the right leg. Examination reveals eight cutaneous markings similar to those shown in Figure 18b. Radiographs are shown in Figure 18c. Management should consist of
Explanation
REFERENCES: Crawford AH Jr, Bagamery N: Osseous manifestations of neurofibromatosis in childhood. J Pediatr Orthop 1986;6:72-88.
Schoenecker PL, Rich MM: The lower extremity, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, vol 2, pp 1059-1104.
Question 15
A 29-year-old quarterback falls onto his dominant shoulder and sustains the injury shown in Figures 14a and 14b. Management should consist of
Explanation
REFERENCES: Lemos MJ: The evaluation and treatment of the injured acromioclavicular joint in athletes. Am J Sports Med 1998;26:137-144.
Rockwood CA Jr, Green DP, Bucholz RW, et al: Fractures in Adults, ed 5. Philadelphia, PA, Lippincott-Raven, 2001, pp 1209-1240.
Question 16
A coronal MRI scan through the shoulder joint is shown in Figure 26. The cyst indicated by the arrow will most likely cause compression of what nerve?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangements of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 306-309.
Iannotti JP, Ramsey ML: Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-745.
Question 17
Plate fixation without bone grafting
Explanation
Which of the following stress fractures most often requires internal fixation:
Question 18
A patient with a documented allergy to nickel requires a total knee arthroplasty. Which of the following prostheses is most likely to provide long-term success in this individual?
Explanation
REFERENCES: Laskin RS: An oxidized Zr ceramic surfaced femoral component for total knee arthroplasty. Clin Orthop 2003;416:191-196.
Nasser S, Campbell PA, Kilgus D, et al: Cementless total joint arthroplasty prostheses with titanium-alloy articular surfaces: A human retrieval analysis. Clin Orthop 1990;261:171-185.
Question 19
In the nonsurgical management of posterior tibial tendon dysfunction with flexible deformity, a common strategy is to prescribe an ankle-foot orthosis or a University of California Biomechanics Laboratory (UCBL) orthosis with medial posting. A high patient satisfaction rating and favorable outcome with this nonsurgical management is most likely in which of the following situations?
Explanation
REFERENCES: Chao W, Wapner KL, Lee TH, et al: Nonoperative management of posterior tibial tendon dysfunction. Foot Ankle Int 1996;17:736-741.
Noll KH: The use of orthotic devices in adult acquired flatfoot deformity. Foot Ankle Clin 2001;6:25-36.
Question 20
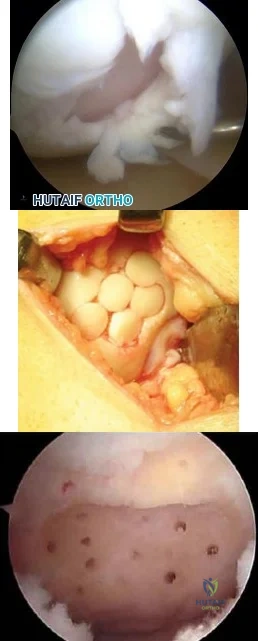
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the most likely cause of this patient's pain?
Explanation
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 21
A 72-year-old female presents to your office with a 24-month old painful nonunion of a 3-part fracture of the proximal humerus. She has been treated conservatively with range of motion exercises but continues to complain of debilitating pain and dysfunction. Operative management should include:

Explanation
The referenced article by Cheung et al reviews treatment options for proximal humeral nonunions and reports successful use of arthroplasty in treating elderly osteoporotic proximal humeral nonunions as a pain relieving procedure.
Dines reported a case series of 20 chronic post-traumatic proximal humerus fractures including nonunions that were treated with shoulder arthroplasty achieving fair to excellent results in 90% at mid-term follow-up
Question 22
Figure 25 shows an arthroscopic thermal capsular shrinkage device being used in the anterior inferior quadrant of a patient with a subluxating shoulder. Which of the following neurologic complications is most frequently reported with this technique?
Explanation
REFERENCES: Fanton GS: Arthroscopic electrothermal surgery of the shoulder. Op Tech Sports Med 1998;6:157-160.
David TS, Drez DJ Jr: Electrothermally-assisted capsular shift. IEEE Eng Med Biol Mag 1998;17:102-104.
Question 23
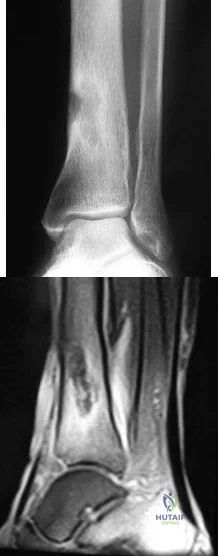
An 11-year-old boy has had a fever and pain and swelling over the lateral aspect of his right ankle for the past 3 days. Examination reveals warmth, swelling, and tenderness over the lateral malleolus, and he has a temperature of 103.2 degrees F (39.5 degrees C). Laboratory studies show a WBC count of 13,200/mm 3 with 61% neutrophils, an erythocyte sedimentation rate of 112 mm/h, and a C-reactive protein of 15.7. Radiographs and a T 2 -weighted MRI scan are shown in Figures 13a through 13c. Aspiration yields 1 mL of purulent fluid. Management should now consist of
Explanation
definitive treatment.
REFERENCES: Scott RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis in children: A review of 116 cases. J Pediatr Orthop 1990;10:649-652.
Vaughan PA, Newman NM, Rosman MA: Acute hematogenous osteomyelitis. J Pediatr Orthop 1987;7:652-655.
Question 24
- A patient has a noncomminuted displaced fracture of the radial head with a distal radioulnar dissociation. What is the most appropriate treatment for the radial head?
Explanation
Question 25
What type of brace is shown in Figures 22a and 22b?
Explanation
REFERENCES: Mehta JA, Brown C, Sargeant N: Charcot restraint orthotic walker. Foot Ankle Int 1998;19:619-623.
Morgan JM, Biehl WC III, Wagner FW Jr: Management of neuropathic arthropathy with the Charcot restraint orthotic walker. Clin Orthop 1993;296:58-63.
Question 26
Which of the following is not a reported mode of failure for a constrained acetabular component?
Explanation
REFERENCES: Lachiewicz PF, Kelley SS: Constrained components in total hip arthroplasty. J Am Acad Orthop Surg 2002;10:233-238.
Anderson MJ, Murray WR, Skinner HB: Constrained acetabular components. J Arthroplasty 1994;9:17-23.
Fisher DA, Kiley K: Constrained acetabular cup disassembly. J Arthroplasty 1994;9:325-329.
Question 27
A 25-year-old male sustains the isolated injury shown in Figure A. Antegrade intramedullary nailing is planned for definite fixation within the next 12 hours. After obtaining lateral radiographs of the injury site, what would be the next best step in management of this patient?

Explanation
Femoral neck fractures are seen less than 10% of the time with femoral shaft fractures, but they are frequently missed on initial evaluation. The neck fracture line is almost vertical and nondisplaced, or minimally displaced. Therefore fine (2-mm) cut CT scan through the femoral neck should be ordered in the preoperative workup of these patients.
Tornetta et al. reported that they reduced the delay in diagnosis of concomitant femoral neck fractures by 91% by instituting a protocol that included: dedicated AP internal rotation plain radiograph, a fine (2-mm) cut CT scan through the femoral neck, an intraoperative fluoroscopic lateral radiograph prior to fixation, as well as postoperative AP and lateral radiographs of the hip in the operating room prior to awakening the patient.
Figure A shows a trauma view lower extremity radiograph with an isolated left midshaft femur fracture.
Incorrect Answers:
setting of fracture. Answer 5: The age, injury and fracture pattern are not consistent with a pathologic femur fracture.
Question 28
A 3-year-old child has refused to walk for the past 2 days. Examination in the emergency department reveals a temperature of 102.2 degrees F (39 degrees C) and limited range of motion of the left hip. An AP pelvic radiograph is normal. Laboratory studies show a WBC count of 9,000/mmP3P, an erythrocyte sedimentation rate (ESR) of 65 mm/h, and a C-reactive protein level of 10.5 mg/L (normal < 0.4). What is the next most appropriate step in management? Review Topic
Explanation
(SBQ13PE.16) A 4-week-old infant who had been born with a dislocated hip has been treated in a Pavlik Harness since 1 week of age. Parents have been compliant with the prescribed bracing protocol, and no complications or neurologic abnormalities have been noted. The hip remains Ortolani positive. Figure A shows the ultrasound image obtained in the office. What is the next best step in management? Review Topic

No further treatment
Continue Pavlik Harness treatment
Convert to semi-rigid abduction brace
Perform a hip arthrogram with closed vs. open reduction under general anesthesia
Perform a pelvic osteotomy
This is a 4 week old infant with DDH who has failed Pavlik harness treatment for 3 weeks. Figure A is an ultrasound image demonstrating a dislocated hip.
Initial treatment for an infant with a dislocated, but reducible ("Ortolani positive") hip is bracing in a Pavlik Harness. The Pavlik harness is a dynamic brace that requires normal muscle function and tone to help keep the hip in a reduced position. If this treatment fails to hold the hip reduced after three weeks of treatment, the harness should be discontinued to prevent "Pavlik Harness Disease" which involves erosion of the posterior acetabulum as the femoral head is inappropriately being held against it.
After failure of Pavlik harness treatment, if the hip remains subluxated, the next step in treatment is to convert to a semi-rigid orthosis of another 2-3 weeks. If the semi-rigid brace likewise fails to keep the hip reduced, then hip arthrogram with closed vs. open reduction and spica-cast placement can be planned.
Swaroop and Mubarak present a study using a protocol of initial pavlik harness treatment with weekly ultrasound assessment for 3 weeks. If the hip remained unstable but reducible, then semi-rigid abduction bracing with continues weekly ultrasounds were done for an additional 2-3 weeks. This treatment protocol had a 93% success rate, which compared favorably to protocols not including the abduction
brace.
Hedequist et al. presented a review of 15 patients treated similarly with intial pavlik harness treatment for 3-4 weeks, and then abduction bracing if the remained unstable but reducible. They found that abduction bracing produced a stable hip within 1-2 months.
Illustration A shows a baby wearing a semi-rigid orthosis. Illustration B is the hip ultrasound image from Figure A with labels added. Illustration C is an ultrasound of a hip that is not dislocated.
Incorrect answers:
Question 29
Figure 1 shows the radiograph of an 11-year-old boy who stubbed his great toe while playing soccer barefoot. He is able to walk home despite a small amount of bleeding at the nail fold. Management should consist of
Explanation
the fracture.
REFERENCES: Noonan KJ, Saltzman CL, Dietz FR: Open physeal fractures of the distal phalanx of the great toe: A case report. J Bone Joint Surg Am 1994;76:122-125.
Banks AS, Cain TD, Ruch JA: Physeal fractures of the distal phalanx of the hallux. J Am Podiatr Med Assoc 1988;78:310-313.
Question 30
A 42-year-old man reports a 3-day history of worsening lower back pain. He denies any history of recent trauma or infections. He also reports difficulty urinating and fecal incontinence in the last 24 hours. Examination reveals generalized lower extremity weakness, diminished sensation in a saddle distribution, and loss of rectal tone. What is the most appropriate management at this time? Review Topic
Explanation
Question 31
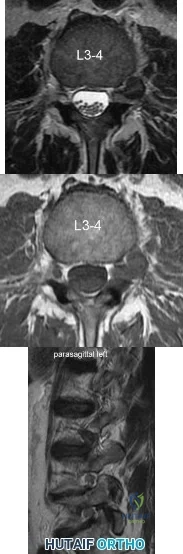
A 39-year-old man presents with back pain radiating to the left lower extremity for the past 6 weeks. Magnetic resonance images of the pathology are
Explanation
Far lateral disc herniations constitute approximately 5-10 percent of disc hernations in the lumbar spine. Given the more vertical anatomy of lumbar nerve roots, at a given disc level, a central or paracentral herniation will affect the traversing nerve root (e.g. nerve root of level below) and a far lateral herniation will affect the exiting nerve root (e.g. nerve root of the level above). Similar to the more common central and paracentral herniations, approximately 90% of patients will improve without surgical intervention. When surgical intervention is needed, the paraspinal approach of Wiltse is utilized.
Marquadt et al. reported long term outcomes of surgical management of far lateral disc herniations. At an average of 146 months follow up, 56.3% of patients had complete relief of symptoms and 27.6% had permanent residual symptoms. Over 75% of patients subjectively rated their outcomes as excellent.
Figure A and B are T2 and T1 axial MRI images, respectively, showing the L3-L4 disc space with a left far lateral disc herniation. Figure C is a left parasagittal T2 MRI image showing impingement on the L3 nerve root. Structures are labeled in illustration A. Illustration B shows the dermatomes of the lower extremity.
Incorrect Answers:
Question 32
A 30-year-old patient has had severe left hip pain and difficulty ambulating, necessitating the use of a cane, for the past 6 months. A photomicrograph of the femoral head sectioned at the time of surgery is shown in Figure 31. What is the most likely diagnosis?
Explanation
REFERENCES: Basset LW, Mirra JM, Cracchiolo A III: Ischemic necrosis of the femoral head: Correlation between magnetic resonance imaging and histologic sections. Clin Orthop 1987;223:181-187.
Sugano N: Osteonecrosis, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopedics. St Louis, MO, Mosby, 2002, pp 878-887.
Question 33
Figures 14a and 14b show the clinical photographs of a patient who was stranded in a subzero region for several days. The photographs were taken the morning after arrival in the hospital. The patient is otherwise healthy and fit, and takes no medication. He has no clinical signs of sepsis. He reports burning pain and tingling in both feet. What is the best treatment?
Explanation
REFERENCES: McAdams TR, Swenson DR, Miller RA: Frostbite: An orthopedic perspective.
Am J Orthop 1999;28:21-26.
Taylor MS: Cold weather injuries during peacetime military training. Milit Med 1992;157:602-604.
Question 34
What is the primary mechanism of degradation of calcium phosphate cement?
Explanation
To treat depressed tibial plateau fractures, surgeons must elevate the depressed segments, which results in a metaphyseal bone void. This void can be filled with multiple materials, including autograft and allograft bone. The addition of BMP-2 or BMP-7 is not recommended to fill contained bone defects. These materials are indicated for application between bone and soft tissue and they do not provide the volume or strength to fill closed defects. Calcium phosphates have been use to fill these voids, demonstrating improved strength and resistance to subsidence when compared to autograft. Although polymethylmethacrylate is commonly used to fill bone voids in patients with cancer, it is not preferred in the setting of acute fracture because of the exothermic reaction that may compromise local bone healing. Although hydroxyapatite may be degraded by macrophage and giant-cell-mediated processes, the calcium phosphate degrades mainly by an osteoclast-mediated method. The calcium phosphate is not soluble in interstitial fluid, so simple dissolution does not occur.
RECOMMENDED READINGS
Bajammal SS, Zlowodzki M, Lelwica A, Tornetta P 3rd, Einhorn TA, Buckley R, Leighton R, Russell TA, Larsson S, Bhandari M. The use of calcium phosphate bone cement in fracture treatment. A meta-analysis of randomized trials. J Bone Joint Surg Am. 2008 Jun;90(6):1186-
Question 35
…The patient underwent an uneventful arthroscopic repair and did well until 1 year later when she crashed during a race. She tore her anterior cruciate ligament (ACL) and underwent reconstruction. Followup after her successful ACL reconstruction reveals complaints of new shoulder pain and posterior instability from using crutches after her ACL surgery. A new MRI scan is shown in Figure 24. What factors are most likely associated with this patient’s recurrence?
Explanation
Question 36
A 55-year-old man sustained an elbow dislocation in a fall. Postreduction radiographs are shown in Figures 40a and 40b. What is the best course of management?
Explanation
REFERENCES: Hildebrand KA, Patterson SD, King GJ: Acute elbow dislocations: Simple and complex. Orthop Clin North Am 1999;30:63-79.
O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. Instr Course Lect
2001;50:89-102.
Question 37
A 75-year-old woman is undergoing a T10-S1 lumbar decompression and fusion for severe degenerative scoliosis. During the deformity corrective maneuver, intraoperative neuromonitoring revealed a sustained 80% decrease in somatosensory-evoked potential (SSEP) amplitudes. Appropriate lead placement and
Explanation
Question 38
-A 37-year-old woman has a 2-month history of weakness in thumb and finger extension, but has normal radial deviation during extension of the wrist. An MRI scan of her forearm shows no abnormality. She does not recall any traumatic event. Needle electromyography findings show fibrillations and reduced
Explanation

Question 39
Figure A is a pelvic radiograph of a healthy 20-month old girl with a limb leg discrepancy. A hip arthrogram under general anesthesia reveals concentric reduction of the left hip ONLY when the hip is positioned in 70 to 80 degrees of abduction. The next best step in treatment would be: Review Topic

Explanation
capsulorrhaphy, +/- femoral osteotomy +/- pelvic osteotomy
In children older than 18 months, open reduction is the preferred treatment for hip dysplasia. Open reduction is also considered when concentric closed reduction cannot be achieved or when excessive abduction (>60 degrees) is required to maintain reduction (due to increasing risk of avascular necrosis). The goal of open reduction is to remove the blocks to reduction and to increase stability by preforming soft-tissue or bone procedures.
Wenger et al. reviewed the surgical treatment of DDH. They say that the impediment to congruent reduction are the iliopsoas muscle, joint capsule, ligamentum teres, pulvinar, labrum, and transverse acetabular ligament. The most commonly used approaches are anterior and medial/anteromedial to the hip.
Gholve et al. reviewed DDH and the factors that contribute to secondary procedures. In their study, neither age nor unilateral vs bilateral dislocation had a direct influence on the outcome or the need for secondary procedures. The variable that significantly influenced the need for a secondary procedure was the concomitant use of a femoral osteotomy during initial surgical treatment. Of the 27 patients who did not have concurrent femoral osteotomy at index surgery, 19/27 (73%) required a secondary procedure (P<0.001).
Figure A shows an AP pelvic radiograph of an infant. Focusing on the left hip, there is lateral and superior subluxation of the femoral head, with the femoral head lateral to Perkin's line. The medial joint space is increased. The acetabular index is increased
>30 degrees. Shenton's line is disrupted. These are all features of DDH.
Incorrect Answers:
Question 40
What is the most common complication associated with scalene regional anesthesia for shoulder procedures?
Explanation
REFERENCES: Weber SC, Jain R: Scalene regional anesthesia for shoulder surgery in a community setting: An assessment of risk. J Bone Joint Surg Am 2002;84:775-779.
Conn RA, Colfield RH, Byer DE, Lindstromberg JW: Interscalene block anesthesia for shoulder surgery. Clin Orthop 1987;216:94-98.
Question 41
The 'Risser sign' is one of the most commonly used markers for skeletal maturation and growth potential in patients with adolescent idiopathic scoliosis. What 'Risser sign' has been shown to correlate with the greatest velocity of skeletal linear growth? Review Topic
Explanation
Risser grades range from 0 to V and are a measure of the progression of ossification in the pelvis. The Risser sign is usually referenced in clinical decision-making regarding adolescent idiopathic scoliosis.
Biondi et al. examined 111 patients to determine the relationship between the accuracy of the Risser sign and bone age determinations. They found that the iliac crest apophysis maturation correlated with skeletal age assessment. They suggest that Risser sign is a reliable method for assessing skeletal bone age.
Illustration A shows an AP pelvis radiograph of a patient that is a Risser II based on the iliac crest apophysis maturation scale. Illustration B shows a chart showing the rate of growth correlated with the Risser staging system. Illustration C shows the Risser staging system from 0 - V.
Risser I: is given when the ilium calcification measures 25%. As this stage the velocity of linear skeletal growth is on a descending slope.
Risser II: the greater trochanteric apophysis unites with the femur and Ilium calcification measures 50%. There is usually 3 cm of sitting growth remaining and no further growth in the lower extremities.
Risser III: Ilium calcification measures 75%. There is usually 2 cm of sitting growth remaining.
Risser IV: Ilium calcification is almost complete. There is usually 1 cm of sitting growth remaining.
Risser V marks complete skeletal maturation.
Incorrect Answers:
Question 42
Figure 11 shows the radiograph of an otherwise healthy 22-year-old man who sustained a midfoot injury in a motor vehicle accident 9 days ago. Treatment should consist of
Explanation
REFERENCES: Teng AL, Pinzur MS, Lomasney L, et al: Functional outcome following anatomic restoration of the tarsal-metatarsal fracture dislocation. Foot Ankle Int
2002;23:922-926.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Question 43
A 29-year-old man sustained an injury when he was playing basketball, landing on his left knee while jumping for a rebound. He had vague pain in the anterior aspect of the knee for several weeks. The initial radiographs were negative with the exception of a large traumatic effusion. Examination reveals no apparent ligament instability but a significant extension lag of 30 degrees. There was a palpable defect above the superior pole of the patella. What is the most appropriate management? Review Topic
Explanation
Question 44
A 32-year-old male sustains an APC-III pelvic ring disruption after a motor vehicle collision. Which of the following imaging techniques best describes the correct utilization of intraoperative flouroscopy for percutaneous iliosacral screw placement across S1?

Explanation
view and an inlet pelvis view would best guide anterior-posterior screw orientation.
Routt et al did a review of percutaneous techniques of pelvic surgery. Although anterior pelvic external fixation remains the most common form of percutaneous pelvic fixation, iliosacral screws have the advantage of stabilizing pelvic disruptions directly while diminishing operative blood loss and operative time. They stress importance of a thorough knowledge of pelvic osseous anatomy, injury patterns, deformities, and their fluoroscopic correlations for surgical success.
Routt et al also looked at the complications that can result from percutaneous iliosacral screw placement. Complications ranged from inability for adequate imaging due to patient obesity, L5 nerve root injuries, fixation failure, and sacral nonunions. They support quality triplanar fluoroscopic imaging during iliosacral screw insertions to help accurately reduce injured posterior pelvic rings.
Illustration A shows the radiographic technique used to shoot an outlet pelvis view and illustration of the pelvic view. Illustration B is an example of an outlet view image status post anterior pelvic ring plating and percutaneous iliosacral screw. This outlet view allows superior S1 neural foramen visualization to help guide screw placement and avoid nerve injury.
Question 45
A 5-year-old boy is seen in the emergency department with a 2-day history of refusing to walk. Examination shows that he has a temperature of 102.2 degrees F (39 degrees C) and limited range ot motion of the right hip. The AP pelvic radiograph is normal. The WBC count is normal but the C-reactive protein and erythrocyte sedimentation rate (ESR) are elevated. What is the next step in management?
Explanation
REFERENCES: Herring JA: Tachdjian’s Pediatric Orthopaedics, ed 4. Philadelphia, PA, WB Saunders, 2008, pp 2109-2113.
Abel MF (ed): Orthopaedic Knowlede Update: Pediatrics 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 62-65.
Kocher MS, Mandiga R, Murphy JM, et al: A clinical practice guideline for treatment of septic arthritis
in children: Efficacy in improving process of care and effect on outcome of septic arthritis of the hip. J Bone Joint Surg Am 2003;85:994-999.
Kocher MS, Mandiga R, Zurakowski D, et al: Validation of a clinica l prediction rule for the differentiation between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am 2004;86:1629-1635.
Question 46
Which of the following best describes the recommended treatment for a 13-year-old pitcher with a painful chronic stress injury to the proximal humeral physis as confirmed on an MRI scan? Review Topic
Explanation
Question 47
Figure 1 is the ultrasound of a 23-year-old patient who has had a volar radial 1.5-cm tender and painful wrist mass for 6 months. The additional workup prior to surgery should consist of

Explanation
The ultrasound shows a homogeneous anechoic mass consistent with a ganglion cyst. As a benign lesion, no further workup or biopsy is required prior to a marginal surgical excision other than age-appropriate laboratory studies. An MRI study with contrast would provide no diagnostic benefit.
Question 48
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 49
Figure 38 shows the radiograph of a 16-year-old wrestler who injured his elbow when he was thrown to the mat by his opponent. To minimize additional trauma to the medial soft tissues, the elbow should be reduced in
Explanation
REFERENCES: O’Driscoll SW: Elbow dislocations, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 414.
Norris TR (ed): Orthopaedic Knowledge Update: Shoulder and Elbow. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1997, pp 345-354.
Question 50
A 52-year-old man has had back pain radiating to the left leg for the past 5 weeks. A radiograph, MRI scans, and biopsy specimens are shown in Figures 23a through 23f. What is the most likely diagnosis?
Explanation
REFERENCE: Mirra J: Bone Tumors: Clinical, Radiologic, and Pathologic Correlations. Philadelphia, PA, Lea and Febiger, 1989, vol 1, ch 8.
Question 51
Figures 1 and 2 demonstrate the radiographs obtained from a 35-year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits. Which bearing surface is contraindicated for this patient?
Explanation
THA has proven durable and reliable for pain relief and improving function for patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A metal-on- metal articulation is associated with excellent wear rates in vitro. With its capacity to offer a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis with potential transfer of metal ions across the placental barrier make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child- bearing age. The workup of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including sedimentation rate, CRP, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging including MARS MRI should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so, when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following revision of failed metal-on-metal hip replacements.
Question 52
- The primary effect of deep freezing on musculoskeletal allografts is a reduction of
Explanation
Question 53
Examination of a 30-year-old professional singer who has persistent neck and shoulder pain reveals a positive Hoffman’s sign and clonus because of anterior C2-3 cord compression. The MRI scan shown in Figure 11a and the cervical CT scan shown in Figure 11b reveal focal anterior cord compression at the C2-3 level. Which of the following surgical approaches would least affect her professional career?
Explanation
REFERENCES: McAfee PC, Bohlman HH, Reilly LH Jr, Robinson RA, Southwick WO, Nachlas NE: The anterior retropharyngeal approach to the upper part of the cervical spine. J Bone Joint Surgery Am 1987;69:1371-1383.
Lu J, Ebraheim NA, Nadim Y, Huntoon M: Anterior approach to the cervical spine: Surgical anatomy. Orthopedics 2000;23:841-845.
Question 54
A 23-year-old man cut the dorsal and ulnar aspects of his long finger on a table saw. The dorsal and ulnar skin over the middle phalanx is missing, with a 2-cm x 2-cm area of loss. There is a 50% loss of the extensor tendon (ulnar), and the remaining tendon has no tenosynovium. The physician should recommend irrigation and debridement and
Explanation
The patient has exposed bone and tendon and a partial tendon injury. The remaining radial tendon is satisfactory and no tendon repair is required. The exposed bone and tendon necessitate vascularized tissue coverage. A reversed cross-finger flap from the ring finger is suitable for coverage of the dorsal surface of an adjacent digit.
Question 55
A 20-year-old collegiate pitcher sustains a medial collateral ligament (MCL) rupture of his throwing elbow for which surgical reconstruction is necessary. The goal of surgery is anatomic restoration of the MCL. Which statement best describes the kinematics of the native MCL?
Explanation
full extension and full flexion. True lateral radiographs reveal that the flexion-extension axis, or center of rotation, of the elbow lies in the center of the trochlea and capitellum. The origin of the anterior bundle of the MCL lies slightly posterior to the rotational center of the elbow. The anterior bundle is further divided into an anterior band and a posterior band. The eccentric origin of these anterior bundle components in relation to the rotational center through the trochlea creates a CAM effect during flexion and extension. The anterior band tightens during extension, and the posterior band tightens during flexion. This reciprocal tightening of the two functional components of the anterior bundle allows the ligament to remain taut throughout the full range of flexion. Cadaver dissection studies have identified the origin and insertion of both the medial and lateral stabilizing elbow ligaments. The anterior bundle of the MCL is isometric throughout the flexion/extension arc of motion, making Response C incorrect. The posterior bundle of the MCL elongates with elbow flexion, so Responses B and D are incorrect. The posterior bundle of the MCL also demonstrates the most change in
length from extension to flexion of all the elbow ligaments.
Question 56
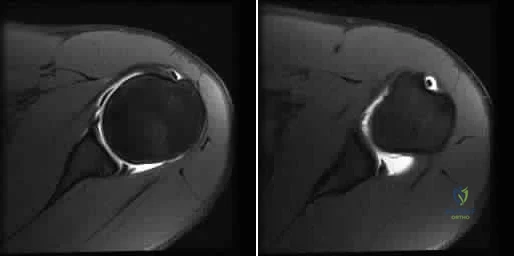
A 21-year-old basketball player reports increased left shoulder pain with all lifting and overhead activities. He denies any history of dislocations. Axial MRI arthrogram images are seen in Figures 34a and 34b. An expected finding on physical examination of the shoulder would be positive findings for which of the following tests? Review Topic
Explanation
then abducted, while maintaining the axial load, and the patient's subjective and objective response is observed. Comparison to the contralateral shoulder is important, especially if painless subluxation is noted, to determine potential evidence of generalized joint laxity.
Question 57
-A 12-year-old boy who plays multiple sports has had insidious-onset heel pain while running for 4 months. On examination, he had ankle dorsiflexion of 5 degrees. The squeeze test result was positive and the Thompson test result was negative. He has no pain with forced ankle plantar flexion. What is the most likely diagnosis?
Explanation
A 15-year-old boy has had shoulder pain for 4 weeks during the middle of baseball season. The patient says his pain is “all over my shoulder.” Examination reveals tenderness to palpation over the anterolateral aspect of the shoulder. Internal and external rotation range of motion is restricted.
Radiographs show metaphyseal sclerosis.
Question 58
A 51-year-old man sustained an open fracture of his tibia in Korea 42 years ago. An infection developed and it was resolved with surgical treatment. For the past 6 months, an ulcer with mild drainage has developed over the medial tibia. The ulcer is small and there is minimal erythema at the ulcer site. A radiograph and MRI scan are shown in Figures 43a and Figure 43b. Initial cultures show Staphylococcus aureus susceptible to the most appropriate antibiotics. Laboratory studies show an erythrocyte sedimentation rate of 70 mm/h. What is the most appropriate surgical treatment at this time? Review Topic
Explanation
Question 59
Figure 80a shows an arthroscopic view from an infralateral portal of a right knee. Figure 80b shows a coronal MRI scan, and Figures 80c through 80e show consecutive sagittal images of the knee. The images show what anatomic finding? Review Topic
Explanation
Question 60
Which of the following infectious organisms may be associated with underlying malignancy?
Explanation
REFERENCES: Schaaf RE, Jacobs N, Kelvin FM, et al: Clostridium septicum infection associated with colonic carcinoma and hematologic abnormality. Radiology 1980;137:625-627.
Katlic MR, Derkac WM, Coleman WS: Clostridium septicum infection and malignancy. Ann Surg 1981;193:361-364.
Question 61
A 21-year-old minor league pitcher reports decreasing velocity and ability to target his pitches over the last 2 months. He notes that his arm will start to feel heavy in the later innings and notes pain in the posterior aspect of his shoulder in the late cocking phase of his motion. He denies any specific event that initiated his symptoms. Examination reveals symmetric rotator cuff strength and no increased anterior or posterior translation of either shoulder. Supine range of motion of the right shoulder in 90 degrees of abduction reveals external rotation to 100 degrees and internal rotation to 25 degrees. The left shoulder has 95 degrees of external rotation and 60 degrees of internal rotation. He has pain with an O'Brien's maneuver and a negative apprehension sign. What is the next most appropriate step in management? Review Topic
Explanation
Question 62
An eversion mechanism of injury is associated with which of the following ankle conditions?
Explanation
REFERENCES: Casillas MM: Ligament injuries of the foot and ankle in the athlete, in DeLee JC, Drez D, Miller MD (eds): Orthopaedic Sports Medicine: Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2323-2357.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 233-245.
Question 63
A 44-year-old man was involved in a low speed rear-end motor vehicle accident 4 weeks ago. He predominantly reports pain in the back of the neck, with occasional radiation into the trapezius region bilaterally. He denies any extremity pain. The pain has not changed in intensity, but is worse with neck range of motion. Cervical spine radiographs were negative for acute osseous trauma or instability. What is the next most appropriate step in management? Review Topic
Explanation
Question 64
A 52-year-old man has shoulder pain and stiffness after undergoing a “mini-lateral” rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/ mm 3 (normal 3,500 to 10,500/ mm 3 ) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
Explanation
REFERENCES: Mirzayan R, Itamura JM, Vangsness CT, et al: Management of chronic deep infection following rotator cuff repair. J Bone Joint Surg Am 2000;82:1115-1121.
Settecerri JJ, Pitnu MA, Rock MG, et al: Infection after rotator cuff repair. J Shoulder Elbow Surg 1994;8:105.
Herrera MF, Bauer G, Reynolds F, et al: Infection after mini-open rotator cuff repair. J Shoulder Elbow Surg 2002;11:605-608.
Question 65
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
Explanation
Complications are numerous in adult spinal deformity surgery. Many complications are related to the patient's sagittal balance following surgery and recognition of the potential to develop sagittal imbalance or flat-back syndrome following spinal fusion. The quality of bone density is important in spinal instrumented fusions, especially among older patients. Patients with osteopenia or osteoporosis have a higher incidence of proximal-level screw cut-out through the vertebral body into the cephalad disk space.
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
Question 66
A 62-year-old man with a long history of right shoulder pain and weakness is scheduled to undergo hemiarthroplasty. Based on the radiographs shown in Figures 6a through 6c, what preoperative factor will most affect postoperative functional outcome?
Explanation
REFERENCES: Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Hettrich CM, Weldon E III, Boorman RS, et al: Preoperative factors associated with improvements in shoulder function after humeral hemiarthroplasty. J Bone Joint Surg Am 2004;86:1446-1451.
Question 67
Figure 10 shows the radiograph of a 9-year-old girl who injured her left lower leg after being thrown from a horse. Examination reveals no other injuries. Which of the following forms of management will provide the lowest rate of complications and the earliest return to function?
Explanation
REFERENCES: Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70:74-77.
Heinrich SD, Drvaric D, Darr K, MacEwen GD: Stabilization of pediatric diaphyseal femoral fractures with flexible intramedullary nails (a technique paper). J Orthop Trauma 1992;6:452-459.
Question 68
Which of the following statements best describes the process of articular cartilage degeneration in osteoarthritis?
Explanation
REFERENCE: Buckwalter JA, Mankin HJ, Grodzinsky AJ: Articular cartilage and osteoarthritis. Instr Course Lect 2005;54:465-480.
Question 69
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
Explanation
REFERENCE: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 70
A 24-year-old dancer sustains the injury shown in Figure 28. Management should consist of
Explanation
REFERENCES: O’Malley MJ, Hamilton WG, Munyak J: Fractures of the distal shaft of the fifth metatarsal: “Dancer’s Fracture.” Am J Sports Med 1996;24:240-243.
DeLee JC: Fractures and dislocations of the foot, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1465-1703.
Hamilton WG: Foot and ankle injuries in dancers, in Yokum L (ed): Sports Clinics of North America. Philadelphia, PA, Williams and Wilkins, 1988.
Question 71
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management?
Explanation
REFERENCES: Miller P, Kendrick D, Bentley E, et al: Cost effectiveness of lumbar spine radiographs in primary care patients with low back pain. Spine 2002;27:2291-2297.
Wong DA, Transfeldt E: Macnab’s Backache, ed 4. Philadelphia, PA, Lippincott Williams and Wilkins 2007, pp 298-338.
Question 72
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient’s symptoms at this time?
Explanation
REFERENCES: Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 73
A 31-year-old male sustains an ipsilateral displaced transverse acetabular fracture, pubic rami fractures, and a sacroiliac joint dislocation. What structure should be reduced and stabilized first?

Explanation
The referenced article by Matta reviewed 259 patients with acetabular fractures treated within 21 days of injury and found that the hip joint can be preserved and post-traumatic osteoarthrosis can be avoided if an anatomical reduction is achieved.
Question 74
A patient has a C6 spinal cord injury. Following stabilization of the spine, the patient should be advised that their expected maximum level of function
Explanation
Question 75
A 22-year-old professional baseball pitcher has had pain in the axillary region of his dominant shoulder for the past several weeks. While throwing a pitch during a game, he notes a sharp pulling sensation with a “pop” in his shoulder. Examination the following day reveals tenderness along the posterior axillary fold and pain and weakness with resisted extension of the shoulder. What is the most likely cause of his symptoms?
Explanation
REFERENCES: Schickendantz MS, Ho CP, Keppler L, et al: MR imaging of the thrower’s shoulder: Internal impingement, latissimus dorsi/subscapularis strains and related injuries.
Magn Reson Imaging Clin N Am 1999;7:39-49.
Livesey JP, Brownson P, Wallace WA: Traumatic latissimus dorsi: Tendon rupture. J Shoulder Elbow Surg 2002;11:642-644.
Question 76
A 78-year-old woman underwent total hip arthroplasty 15 years ago. She reports a recent history of increasing thigh pain prior to a fall and is now unable to ambulate. Radiographs are shown in Figures 87a and 87b. What is the best treatment for this condition?
Explanation
REFERENCES: Barrack RL, Booth RE Jr, Lonner JH, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 475503.
Kwong LM, Miller AJ, Lubinus P: A modular distal fixation option for proximal bone loss in revision total hip
arthroplasty: A 2- to 6-year follow-up study. J Arthroplasty 2003;18:94-97.
Question 77
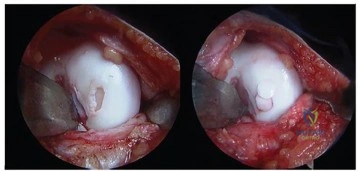
A 35-year-old man presents with mechanical knee pain after a fall. An arthroscopic picture taken during diagnostic arthroscopy is shown in Figure A. His surgeon considers treatment with Technique B and Technique C, which are shown in Figures B and C, respectively. Which of the following statement is true with respect to Technique B and C? Review Topic
Explanation
The initial treatment for small articular cartilage defects is rest, NSAIDS and bracing. For larger defects (<2-4cm2), options include marrow stimulation procedures (abrasion chondroplasty, microfracture, osteochondral drilling) and autograft procedures (Mosaicplasty, a technique of osteochondral autograft transfer (OAT).
Alford et al. reviewed cartilage restoration. They defined a spectrum of treatment option ranging from (1) palliative (debridement/lavage), intended to reduce irritation
and inflammation, (2) reparative (marrow stimulation techniques), intended to recruit stem cells to proliferate fibrocartilage repair tissue, to (3) restorative (osteochondral grafting), designed to replace articular cartilage and subchondral bone as a single unit.
Magnussen et al. reviewed the treatment of cartilage defects in the knee. They compared autologous chondrocyte implantation (ACI), OATs, matrix-induced ACI, and microfracture. No one technique was superior to the rest. Outcomes for microfracture tended to be worse in larger lesions.
Figures A is an arthroscopic picture showing a grade IV chondral defect. Figure B shows microfracture. Figure C shows the multiple cylindrical plugs of mosaicplasty, a technique of osteochondral autograft transfer (OAT). Illustration A shows donor and recipient sites in mosaicplasty. Illustration B shows the spectrum of treatment options defined by Alford et al (MST = marrow stimulation; ACI = autologous chondrocyte implantation; OCG = osteochondral grafting with autograft/allograft).
Incorrect Answers:
Question 78
A 25-year-old patient undergoes the procedure seen in Figure A. Which of the following statements best describes the incorporation of the graft and biopsy results of the graft at one year? Review Topic
Explanation
Articular cartilage defects can be treated by a variety of methods including debridement, fixation of unstable osteochondral fragments, marrow stimulation techniques (microfracture, abrasion chondroplasty), cartilage replacement techniques (osteochondral autograft and allograft) and cellular techniques (autologous chondrocyte implantation). Osteochondral autograft transfer is performed by harvesting normal articular cartilage with underlying bone from lesser weightbearing areas (e.g. intercondylar notch) and transferring the graft to a recipient socket at the site of the chondral defect. Graft incorporation occurs by integration of the bony graft into the subchondral bone and healing of the overlying cartilage layer.
Hangody et al. reviewed the outcomes of autologous osteochondral mosaicplasty in professional athletes. They found successful outcomes similar to that of less athletic patients, despite a higher rate of preoperative osteoarthritic changes in the athletic population. The authors noted that histological evaluation revealed good graft incorporation in all 11 cases.
Alford et al. authored a two part Current Concepts article on cartilage restoration. They constructed an algorithm (Illustration A) highlighting many factors that impact treatment choice, including patient activity level and defect characteristics such as location and size. This algorithm also illustrates comorbidities (malalignment, ligament insufficiency) that warrant correction prior to addressing the chondral defect.
Figure A shows a full-thickness chondral defect (left) and subsequent osteochondral autograft transfer (right). Illustration A is a treatment algorithm for the management of chondral defects, as discussed above. Illustration B shows a microfracture procedure, a marrow stimulation technique resulting in fibrocartilage filling of the chondral defect. Illustration C shows an osteochondral allograft transplant, a cartilage replacement technique useful for large defects in which donor graft is obtained from a cadaver hemicondyle and transferred to a recipient socket at the site of the chondral defect. Illustration D shows the autologous chondrocyte implantation technique, a two-stage procedure consisting of 1. Cartilage biopsy for growth of autologous
chondrocytes, and 2. Subsequent injection of autologous chondrocytes beneath a periosteal patch.
Incorrect
Question 79
A 23-year-old right-hand dominant professional baseball pitcher has right shoulder pain when releasing the ball. He has noticed his velocity has decreased over the past 2 months. Examination reveals supine abducted external rotation of 110 degrees compared to 100 degrees on the left side. His internal rotation is 30 degrees on the right compared to 70 degrees on the left side. Rotator cuff strength is normal. All other clinical tests are normal. MRI with contrast reveals no intra-articular lesions. What is the best course of treatment? Review Topic
Explanation
should then be followed by appropriate rotator cuff and scapular stabilization exercises. Only if this management fails to relieve the patient's symptoms should surgery be considered. This patient clearly does not need external rotation stretching given the fact that he has normal external rotation.
Question 80
The essential lesion in recurrent or posterior instability following simple dislocation of the elbow typically involves which of the following structures?
Explanation
Question 81
A patient has a large T11-T12 disk herniation that is causing substantial compression of the spinal cord. The patient reports walking imbalance over the past few weeks. Examination of the patient's reflexes is likely to show Review Topic
Explanation
Question 82
A 15-year-old boy has had pain in the right shoulder for the past 3 months. He denies any history of trauma and has no constitutional symptoms. Examination reveals a large firm mass in the proximal arm. A radiograph and MRI scan are shown in Figures 27a and 27b. Biopsy specimens are shown in Figures 27c and 27d. Management should consist of
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 232-233.
Simon M, et al: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-196.
Question 83
A 25-year-old woman has had pain and stiffness in her knee following a motor vehicle accident 9 months ago. The radiograph, CT scan, MRI scan, and biopsy specimen are shown in Figures 53a through 53d. What is the most likely diagnosis?
Explanation
REFERENCES: Horne LT, Blue BA: Intra-articular heterotopic ossification in the knee following intramedullary nailing of the fractured femur using a retrograde method. J Orthop Trauma 1999;13:385-388.
Stannard JP, Wilson TC, Sheils TM, McGwin G Jr, Volgas DA, Alonso JE: Heterotopic ossification associated with knee dislocation. Arthroscopy 2002;18:835-839.
Mills WJ, Tejwani N: Heterotopic ossification after knee dislocation: The predictive value of the injury severity score. J Orthop Trauma 2003;17:338-345.
Question 84
Which sterilization method is expected to produce the most degradation of an allograft used for anterior cruciate ligament reconstruction?
Explanation
A biomechanical study compared unprocessed, irradiated (2.0 Mrad-2.8 Mrad), and supercritical CO2-treated soft-tissue allografts and demonstrated a 27% to 36% decrease in stiffness of the supercritical CO2-treated grafts. No significant difference was found between the irradiated and untreated soft-tissue allografts. Low-dose (1.0 Mrad-1.2 Mrad) gamma irradiation of bone-patellar-tendon-allograft has been shown to produce a 20% decrease in graft stiffness. Deep freezing or cleansing with 4% chlorhexidine gluconate does not appear to adversely affect the biomechanical properties of the allograft tissue.

CLINICAL SITUATION FOR QUESTIONS 43 THROUGH 46
Figures 43a and 43b are the MR arthrogram images of a 16-year-old, right-hand-dominant baseball player who injured his left shoulder 4 weeks ago during a game. He now has pain, weakness, and the inability to swing a bat and can no longer do push-ups. He denies prior injury to his left shoulder. Radiographs are unremarkable.
Question 85
Figure 28 is the radiograph of a 25-year-old soccer player who twisted her left ankle 1 week ago. She has pain and swelling over the anterolateral ankle and there is ecchymosis over the lateral ankle. She has these muscle group findings: anterior tibial tendon-right 5/5, left 5/5; posterior tibial tendon-right 5/5, left 5/5; peroneals-right 5/5, left 4/5; Achilles-right 5/5, left 5/5. What is the best next diagnostic or treatment step?

Explanation
Thousands of ankle sprains occur in the United States every day. Most affected patients do not have serious sequelae associated with their injury. In this case, a young athlete sprained her ankle. Her only area of tenderness is isolated to the anterior talofibular ligament. She also has associated weakness. The radiograph shows an os subfibulare; this is an entity that she likely was born with. There is no indication of bony pain, and it is too soon to test for instability; consequently, no further imaging is required. Considering the nature of the sprain and her weakness, physical therapy with proprioceptive training and peroneal strengthening would be most beneficial.
RECOMMENDED READINGS
Lephart SM, Pincivero DM, Giraldo JL, Fu FH. The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med. 1997 Jan-Feb;25(1):130-7. PubMed PMID: 9006708. View Abstract at PubMed
McGuine TA, Keene JS. The effect of a balance training program on the risk of ankle sprains in high school athletes. Am J Sports Med. 2006 Jul;34(7):1103-11. Epub 2006 Feb 13. PubMed PMID: 16476915. View Abstract at PubMed
Chun TH, Park YS, Sung KS. The effect of ossicle resection in the lateral ligament repair for treatment of chronic lateral ankle instability. Foot Ankle Int. 2013 Aug;34(8):1128-33. doi: 10.1177/1071100713481457. Epub 2013 Mar 7. PubMed PMID: 23471672.View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 29 THROUGH 33
Figures 29a and 29b are the weight-bearing radiographs of a 49-year-old woman who has had several months of increasing pain and deformity in her left foot. She points to her plantar medial arch as her area of greatest pain; however, she also has pain just distal to the tip of the distal fibula. Her pain worsens with walking or navigating stairs. Upon examination she has a flexible unilateral pes planus deformity with increased heel valgus and forefoot abduction. She is unable to perform a single heel raise.

29A

B
Question 86
When compared to traditional open repair through a posterior incision, percutaneous Achilles tendon repair clearly results in a reduction of what complication?
Explanation
REFERENCES: Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures:
A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am 2002;84:161-170.
Calder JD, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: A prospective study. Br J Sports Med 2005;39:857-859.
Cretnik A, Kosanovic M, Smrkolj V: Percutaneus versus open repair of the ruptured Achilles tendon: A comparative study. Am J Sports Med 2005;33:1369-1379.
Question 87
An axial T 1 -weighted MRI scan of the pelvis is shown in Figure 13. The arrow is pointing to what muscle?
Explanation
REFERENCES: Higuchi T: Normal anatomy and magnetic resonance appearance of the pelvis, in Takahashi HE, Morita T, Hotta T, Ogose A (eds): Operative Treatment of Pelvic Tumors. Tokyo, Japan, Springer-Verlag, 2003, pp 4-21.
Berquist TH: Pelvis, hips and thigh, in Berquist TH (ed): MRI of the Musculoskeletal System,
ed 4. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 210-238.
Question 88
A 22-year-old swimmer underwent thermal capsulorrhaphy treatment for recurrent anterior subluxation. Following 3 weeks in a sling, an accelerated rehabilitation program allowed him to return to swimming in 3 1/2 months. While practicing the butterfly stroke, he sustained an anterior dislocation. He now continues to have symptoms of anterior instability and has elected to have further surgery. Surgical findings may include a
Explanation
REFERENCES: Abrams JS: Thermal capsulorrhaphy for instability of the shoulder: Concerns and applications of the heat probe. Instr Course Lect 2001;50:29-36.
Hecht P, Hayashi K, Lu Y, et al: Monopolar radiofrequency energy effects on joint capsular tissue: Potential treatment for joint instability. An in vivo mechanical, morphological, and biochemical study using an ovine model. Am J Sports Med 1999;27:761-771.
Question 89
.A patient is unable to actively externally rotate the shoulder when the arm is placed into 90 degrees of abduction and neutral rotation. This finding is most consistent with a tear of the
Explanation
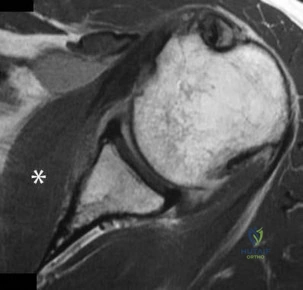
Question 90
Figure 72 is the MRI scan of a 61-year-old man who had left shoulder pain with a massive rotator cuff tear. Active forward elevation was 120 degrees. Arthroscopic examination revealed that the rotator cuff tear was irreparable. The articular surfaces of the glenohumeral joint have a normal appearance without significant degenerative changes. What is the most appropriate treatment option? Review Topic
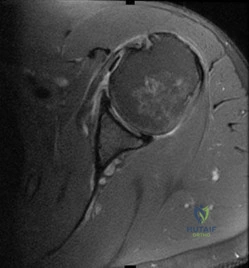
Explanation
Question 91
Patients with rheumatoid arthritis may exhibit an increase in viral load for which of the following viruses?
Explanation
REFERENCES: Callan MF: Epstein-Barr virus, arthritis, and the development of lymphoma in arthritis patients. Curr Opin Rheumatol 2004;16:399-405.
Baecklund E, Sundstrom C, Ekbom A, et al: Lymphoma subtypes in patients with rheumatoid arthritis: Increased proportion of diffuse large B cell lymphoma. Arthritis Rheum
2003;48:1543-1550.
Question 92
A 12-year-old girl has the painful foot deformity seen in Figure 79. You advise her that she has juvenile bunions. How do they differ from adult bunions?

Explanation
angle is less than the adult bunion. Bursal thickenings and prominence of the medial eminence are less in a juvenile bunion.
Question 93
When harvesting an iliac crest bone graft from the posterior approach, what anatomic structure is at greatest risk for injury if a Cobb elevator is directed too caudal?
Explanation
REFERENCES: Banwart JC, Asher MA, Hassanein RS: Iliac crest bone graft harvest donor site morbidity: A statistical evaluation. Spine 1995;20:1055-1060.
Shin AY, Moran ME, Wenger DR: Superior gluteal artery injury secondary to posterior iliac crest bone graft harvesting: A surgical technique to control hemorrhage. Spine 1996;21:1371-1374.
Question 94
Figures 25a and 25b are the radiographs of a 63-year-old man who had right total hip arthroplasty (THA) 4 months ago. Progressive stiffness began 2 months after surgery, and he now reports pain only after prolonged physical activity. His examination reveals normal gait and painless range of motion with flexion of 70 degrees, extension of 0 degrees, internal rotation of 20 degrees, external rotation of 20 degrees, abduction of 10 degrees, and adduction of 10 degrees. His erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels are within defined limits. Physical therapy has produced no benefit. What is the most appropriate next step?
Explanation
This patient presents with HO 4 months after undergoing THA. Symptomatic HO may complicate nearly 7% of primary THA cases. Improvement in pain is expected within 6 months, and most patients will not need surgical treatment. Surgical excision may be warranted for symptomatic patients after full maturation of the HO, usually 6 to 18 months after the surgery. Patients can be followed with repeated serum alkaline phosphatase levels, which are elevated initially and should return to normal upon maturation of HO. Alternatively, a bone scan can show decreased activity once the HO has matured. Twenty-five milligrams of indomethacin 3 times daily for 6 weeks or 1 dose of irradiation at 700 to 800 Gy is effective in the prevention of HO, not for the treatment of established HO.
RESPONSES FOR QUESTIONS 26 THROUGH 29
Minimum inhibitory concentration (MIC)
Minimum bactericidal concentration (MBC)
Antiobiotic susceptibility
Antibiograms
Antimicrobial resistance
Spectrum of coverage
Match the description below with the appropriate response above.
Question 95
A 17-year-old pitcher reports pain over the medial aspect of the elbow that occurs during the acceleration phase of throwing, and it prevents him from throwing at the velocity needed to be competitive. What structure is most likely injured in this patient?
Explanation
REFERENCES: Azar FM, Andrews JR, Wilk KE, et al: Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med 2000;28:16-23.
Cain EL, Dugas JR, Wolf RS, et al: Elbow injuries in throwing athletes: A current concepts review. Am J Sports Med 2003;31:621-635.
Rettig AC, Sherrill C, Snead DS, et al: Nonoperative treatment of ulnar collateral ligament injuries in
throwing athletes. Am J Sports Med 2001 ;29:15-17.
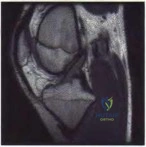
/
Figure 55a Question 55
A 22-year-old male basketball player has had knee pain for the past 3 months. He denies any history of trauma. He has symptoms of catching but no locking. He has rested for 2 weeks but symptoms returned when he resumed sporting activities. Tr and T2-weighted MRI scans are shown in Figures 55a and 55b. What is the most likely diagnosis?
Locked lateral meniscus tear
Anterior cruciate ligament tear
Ganglion cyst of the anterior cruciate ligament
Synovial osteochondromatosis
Pigmented villonodular synovitis PREFERRED RESPONSE: 3
DISCUSSION: The MRI scans show a cystic structure within the anterior cruciate ligament. It is fluid filled as seen on the T2 sequence. Ganglion cysts of the cruciate ligaments are rare. The most common presentation is pain with occasional loss of motion. Instability is not a chief complaint and often there is no evidence of laxity on examination. If nonsurgical management fails, arthroscopic debridement of the cyst is the accepted method of treatment.
REFERENCES: Liu SH, Osti L, Mirzayan R: Ganglion cysts of the anterior cruciate ligament: A case report and review of the literature. Arthroscopy 1994; 10:110-112.
Parish EN, Dixon P, Cross MJ: Ganglion cysts of the anterior cruciate ligament: A series of 15 cases. Arthroscopy 2005;21:445-447.

Question 96
Which lower extremity muscle is first weakened in Charcot-Marie-Tooth (CMT) disease?
Explanation
Although many of the lower extremity muscles may be affected in CMT, those innervated by the longest axons have been shown to be affected first. In the lower extremity the muscles innervated by the longest axons are the intrinsic foot muscles. The tibialis anterior and the peroneus brevis may be severely affected but not before the foot intrinsics. The peroneus longus typically is spared, resulting in the cavus.
RECOMMENDED READINGS
Pareyson D, Marchesi C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol. 2009 Jul;8(7):654-67. Review. PubMed PMID: 19539237. View Abstract at PubMed
Wenz W, Dreher T. Charcot-Marie-Tooth disease and the cavovarus foot. In: Pinzur MS, ed. Orthopaedic Knowledge Update: Foot and Ankle 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:291-306.
CLINICAL SITUATION FOR QUESTIONS 60 THROUGH 63
Figure 60 is the standing radiograph of a 27-year-old man who played football throughout his teen years. During those years, he noted that he had less mobility of his left foot and ankle. He twisted his left foot and ankle 8 months ago and has tried over-the-counter nonsteroidal anti-inflammatory drugs and a brace. He now has pain and edema in the left sinus tarsi area. Upon examination the following arcs of motion are identified: ankle dorsiflexion-right, 5 degrees/left, 5 degrees; ankle plantar flexion-right, 30 degrees/left 30 degrees; foot inversion-right, 10 degrees/left, 5 degrees; foot eversion-right, 10 degrees/left 5 degrees.

Question 97
A favorable outcome following nonsurgical management of a partial tear of the posterior cruciate ligament (PCL) is best associated with
Explanation
REFERENCES: Parolie JM, Bergfeld JA: Long-term results of nonoperative treatment of isolated posterior cruciate ligament injuries in the athlete. Am J Sports Med 1986;14:35-38.
Griffin JR, Annunziata CC, Harner CD: Posterior cruciate ligament injuries in the adult, in Drez D, DeLee JD, Miller MD (eds): Orthopaedic Sports Medicine Principles and Practice, ed 2. Philadelphia, PA, WB Saunders, 2003, pp 2083-2106.
Question 98
A 5-year-old boy has a deformity of his right arm after falling from a jungle gym. A radiograph is shown in Figure 37. Management should consist of
Explanation
REFERENCES: Wilkins KE: Changes in the management of Monteggia fractures. J Pediatr Orthop 2002;22:548-554.
Kay RM, Skaggs DL: The pediatric Monteggia fracture. Am J Orthop 1998;27:606-609.
Ring D, Jupiter JB, Waters PM: Monteggia fractures in children and adults. J Am Acad Orthop Surg 1998;6:215-224.
Question 99
A 33-year-old man had his foot run over by a forklift 1 hour ago. Examination reveals that the head of the fifth metatarsal is extruded through the plantar aspect of the foot. The foot is severely swollen and pale, there is no sensation in the toes, and the pulses are not palpable. Radiographs are shown in Figures 42a and 42b. Emergent management should consist of
Explanation
REFERENCES: Fakhouri AJ, Manoli A II: Acute foot compartment syndromes. J Orthop Trauma 1992;6:223-228.
Myerson MS: Management of compartment syndromes of the foot. Clin Orthop 1991;271:239-248.
Ziv I, Mosheiff R, Zeligowski A, Liebergal M, Lowe J, Segal D: Crush injuries of the foot with compartment syndrome: Immediate one-stage management. Foot Ankle 1989;9:185-189.
Question 100
Reconstruction of the injured structure is performed. After surgery, the patient initially notes limitation in motion, and later develops recurrent instability of the knee. Which factor most likely contributed to the development of instability?
Explanation
The anteromedial bundle originates on the anterior and proximal aspect of the lateral femoral condyle and inserts on the anteromedial aspect of the anterior cruciate ligament (ACL) footprint on the proximal tibia. The posterolateral bundle originates posterior and distal to 63 the anteromedial bundle and inserts on the posterolateral aspect of the tibial footprint. The fibers are parallel when the knee is in an extended position. As the knee moves into flexion,
the fibers of the anteromedial bundle rotate externally with respect to the posterolateral bundle. The anteromedial bundle is tensioned in both flexion and extension. The posteromedial bundle is tensioned in extension, but relaxes as the knee moves into flexion.
The lateral meniscus is more commonly injured with an acute injury to the ACL. The medial meniscus is injured more commonly when the ACL is chronically unstable.
The ACL is an intra-articular and intrasynovial structure. It is innervated by posterior articular branches from the tibial nerve. Innervation of the ACL involves several types of mechanoreceptors (Ruffini, Pacini, Golgi tendon, and free-nerve endings) that may contribute to proprioceptive function of the knee and modulation of quadriceps function.
Injury to the ACL is predominantly associated with instability to anterior translation of the tibia in extension. The ACL plays a secondary role to limit internal rotation of the tibia, and a loss of ACL stability is confirmed by the reduction of the tibia from a position of anterior translation and internal rotation (pivot shift). The radiographs demonstrate anterior placement of the femoral tunnel. The convex shape of the lateral femoral condyle can make it more difficult to visualize the anatomic femoral origin of the ACL. Failure to identify the
anatomic footprint can result in anterior placement of the femoral tunnel. Anterior ACL graft placement can result in its impingement against the posterior cruciate ligament and early limitation of knee flexion. Over time, impingement on the graft may result in stretching of the graft and recurrent knee instability symptoms.
RECOMMENDED READINGS
Duthon VB, Barea C, Abrassart S, Fasel JH, Fritschy D, Ménétrey J. Anatomy of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):204-13. Epub 2005 Oct 19. Review. PubMed PMID: 16235056. View Abstract at PubMed
Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament anatomy and function relating to anatomical reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006 Oct;14(10):982-92. Epub 2006 Aug 5. Review. PubMed PMID: 16897068. View Abstract at PubMed
