OITE & ABOS Orthopedic Board Exam MCQs: Spine, Lower Extremity, & Shoulder | Part 160

Key Takeaway
This page presents Part 160 of a comprehensive orthopedic board review. It offers 100 verified, high-yield MCQs, meticulously formatted for OITE and AAOS board exams. Designed for orthopedic residents and surgeons, this quiz provides crucial practice and clinical explanations to enhance your board certification preparation across Hip, Knee, Scoliosis, and Shoulder topics.
About This Board Review Set
This is Part 160 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 160
This module focuses heavily on: Hip, Knee, Scoliosis, Shoulder.
Sample Questions from This Set
Sample Question 1: What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?...
Sample Question 2: Figures 54a and 54b show the radiograph and MRI scan of a 7-year-old boy who has a painful right thoracic scoliosis that measures 35°. Neurologic examination is normal. Management should consist of...
Sample Question 3: Figure 46 shows the AP radiograph of a patient with right shoulder pain. What is the most likely diagnosis?...
Sample Question 4: Figures 7a and 7b show the radiographs of a 51-year-old woman who injured her left leg after falling off a stepladder. Surgical reconstruction is performed with a compression screw and side plate; the postoperative radiograph is shown in Fi...
Sample Question 5: A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis....
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
What is the most accurate description of the relationship between gender and knee loading during landing while playing basketball?
Explanation
REFERENCES: Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med 2005;33:492-501.
Ford KR, Meyer GD, Hewett TE: Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exer 2003;35:1745-1750.
Question 2
Figures 54a and 54b show the radiograph and MRI scan of a 7-year-old boy who has a painful right thoracic scoliosis that measures 35°. Neurologic examination is normal. Management should consist of
Explanation
REFERENCES: Zadeh HG, Sakka SA, Powell MP, Mehta MH: Absent superficial abdominal reflexes in children with scoliosis: An early indicator of syringomyelia. J Bone Joint Surg Br 1995;77:762-767.
Schwend RM, Hennrikus W, Hall JE, Emans JB: Childhood scoliosis: Clinical indications for magnetic resonance imaging. J Bone Joint Surg Am 1995;77:46-53.
Farley FA, Song KM, Birch JG, Browne R: Syringomyelia and scoliosis in children. J Pediatr Orthop 1995;15:187-192.
Question 3
Figure 46 shows the AP radiograph of a patient with right shoulder pain. What is the most likely diagnosis?
Explanation
REFERENCE: Cahill BR: Osteolysis of the distal part of the clavicle in male athletes. J Bone Joint Surg Am 1982;64:1053-1058.
Question 4
Figures 7a and 7b show the radiographs of a 51-year-old woman who injured her left leg after falling off a stepladder. Surgical reconstruction is performed with a compression screw and side plate; the postoperative radiograph is shown in Figure 7c. Following gradual progression of weight bearing, she reports that she slipped again and placed full weight on the extremity. She now notes a new onset of increased pain in her left thigh and hip region. Follow-up radiographs are shown in Figures 7d and 7e. Reconstruction should consist of
Explanation
REFERENCES: Bridle SH, Patel AD, Bircher M, Calvert PT: Fixation of intertrochanteric fractures of the femur: A randomized prospective comparison of a gamma nail and dynamic hip screw. J Bone Joint Surg Br 1991;73:330-334.
DeLee JC: Fractures and dislocations of the hip, in Rockwood CA Jr, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 1659-1825.
Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Sanders RW, Regazzoni P: Treatment of subtrochanteric femur fractures using the dynamic condylar screw. J Orthop Trauma 1989;3:206-213.
Question 5
A 50-year-old woman undergoes an L4-S1 laminectomy and noninstrumented fusion for degenerative spondylolisthesis.
Explanation
Complications are numerous in adult spinal deformity surgery. Many complications are related to the patient's sagittal balance following surgery and recognition of the potential to develop sagittal imbalance or flat-back syndrome following spinal fusion. The quality of bone density is important in spinal instrumented fusions, especially among older patients. Patients with osteopenia or osteoporosis have a higher incidence of proximal-level screw cut-out through the vertebral body into the cephalad disk space.
Proximal junctional kyphosis is common in longer instrumented fusions, especially when instrumented to the sacrum/pelvis; when the spine is fixed in a "flat" or hypolordotic position; when the thoracic spine is hyperkyphotic (ie, Scheuermann kyphosis); when the end instrumented vertebrae is kyphotic; or when the sagittal plumb line (measured from C7) is more than 4 cm forward of the posterior corner of the sacrum.
Sagittal imbalance is a common complication when the spine is instrumented in a hypolordotic position. This can occur with degenerative conditions that necessitate multilevel fusions or fusions to sacrum without recognition of the degree of lordosis the patient should have. Pelvic incidence (PI) is a spinopelvic measurement that is a constant that measures an angle from the hips to the midpoint of the sacral end plate. PI correlates to the amount of lumbar lordosis that a patient would typically have in an upright position (+/-10 degrees). If a patient has significant sagittal imbalance, he or she will have a forward lean and lack the ability to extend the spine to stand upright. In an attempt to stand upright, the patient may bend his or her knees or hips in a crouched position. When extending their knees, they again lean forward.
Pseudarthrosis is common with noninstrumented fusions. Deep surgical-site infections are uncommon but can be major complications that are difficult to treat, necessitating formal irrigation and debridement and long-term antibiotics. Patients with diabetes have a higher incidence of infection.
RECOMMENDED READINGS
Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976). 2005 Sep 15;30(18):2024-
Question 6
An ulnar nerve palsy at the level of the wrist is typically associated with deficits in the palmaris brevis, the hypothenar muscles, and what other groups of muscles?
Explanation
median nerve.
REFERENCES: Goldfarb CA, Stern PJ: Low ulnar nerve palsy. JASSH 2003;3:14-26.
Omer G: Ulnar nerve palsy, in Green DP, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, pp 1526-1541.
Question 7
Following resection of malignant tumors, complications related to endoprosthetic reconstruction are most common in what anatomic location?
Explanation
REFERENCE: Horowitz SM, Glasser DB, Lane JM, Healey JH: Prosthetic and extremity survivorship after limb salvage for sarcoma: How long do the reconstructions last? Clin Orthop 1993;293:280-286.
Question 8
What are the five major compartments of the foot?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 262-264.
Shereff MJ: Compartment syndromes of the foot. Instr Course Lect 1990;39:127-132.
Question 9
The best patient-related outcomes, following the surgical treatment of cauda equina syndrome secondary to a large L5-S1 disk herniation, are most closely related to which of the following?
Explanation
REFERENCES: Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522.
Kohles SS, Kohles JD, Karp AP, et al: Time-dependent surgical outcomes following cauda equina syndrome diagnosis: Comments on meta-analysis. Spine 2004;29:1281-1287.
Question 10
Which of the following zones of articular cartilage has the highest concentration of proteoglycans?
Explanation
Question 11
All of the following conditions are associated with the female athlete triad EXCEPT? Review Topic
Explanation
The female athlete triad is an interrelationship of menstrual dysfunction (i.e., amenorrhea or oligomenorrhea), low energy availability (insufficient caloric intake for demand, with or without an eating disorder) and decreased bone mineral density. It is relatively common among young women participating in sports. More recently, it has been suggested that endothelial dysfunction also results, due to an imbalance between vasodilating and vasoconstricting agents triggered from inappropirate levels of nitric oxide on the microscopic level, which predisposes these women to atherosclerotic changes and increases their risk of cardiovascular disease in the future.
Matheson et al. analyzed cases of 320 athletes with bone scan-positive stress fractures (M = 145, F = 175) seen over 3.5 years and assessed the results of conservative management. They found that conservative treatment of stress fractures in athletes is satisfactory in the majority of cases.
Constantini et al. evaluated the prevalence of vitamin D insufficiency and deficiency among young athletes and dancers. They found a higher rate of vitamin D insufficiency among participants who practice indoors, during the winter months, and in the presence of iron depletion.
Nazem et al. reviewed the major components and health consequences of the female athlete triad as well as strategies for diagnosis and treatment of the conditions. They concluded that treatment requires a multidisciplinary approach involving health care professionals as well as coaches and family members.
Yagi et al. followed 230 runners participating in high school running teams for a total of 3 years to report occurrence of medial tibial stress syndrome (MTSS) and stress fracture. Predictors of MTSS and stress fracture were investigated. The authors reported a significant relationship between BMI, internal hip rotation angle and MTSS infemales.
Incorrect Answers:
Question 12
When comparing surgical and nonsurgical extremities in patients who underwent anterior cruciate ligament (ACL) reconstruction using patellar tendon or hamstrings autografts, isokinetic strength measurements obtained 6 months after the surgery would most likely reveal
Explanation
REFERENCES: Carter TR, Edinger S: Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 1999;15:169-172
Howell SM, Taylor MA: Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg Am 1996;78:814-825.
Shelbourne KD, Nitz P: Accelerated rehabilitation after anterior cruciate ligament reconstruction. Am J Sports Med 1990;18:292-299.
Question 13
Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
Explanation
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
Question 14
Osteopenia is defined by the World Health Organization (WHO) as a bone mineral density (BMD) that is
Explanation
The T-score represents a comparison to young normals or optimum peak density. The Z-score represents a comparison of BMD to age-matched normals. Measurements of bone mineral density (BMD) at various skeletal sites help in predicting fracture risk. Hip BMD best predicts fracture of the hip, as well as fractures at other sites.
REFERENCE: Kanis JA, Johnell O, Oden A, et al: Risk of hip fracture according to the World Health Organization criteria for osteopenia and osteoporosis. Bone 2000;27:585-590.
Question 15
Sclerostin and dickkopf-1 (Dkk-1) are direct inhibitors of what pathway related to bone and/or cartilage regulation?
Explanation
Adhesive wear
Abrasive wear
Fatigue wear
Delamination
For each scenario below, please choose the most likely dominant mechanism of wear from the list
above.
Question 16
A 75-year-old woman has a 1-year history of right hip pain and a right total hip arthroplasty (THA) performed in 1999. Her left THA, performed in 2002, is asymptomatic. Plain radiographs show that all of the components appear well fixed and in good position. There is evidence of eccentric polyethylene wear of the right hip with focal osteolysis of the calcar and great trochanter (with none of these findings on the left hip). What is the most likely explanation for her right hip pain?
Explanation
This patient likely has 1 conventional polyethylene hip (1999) and 1 hip with highly cross-linked polyethylene (HXLPE) (2002); most centers transitioned to HXLPE around 2001 to 2002. This explains the clear difference in the clinical and radiographic performance of the 2 hips during the second decade. There is clear evidence of decreased wear and osteolysis and clinical benefits (ie, decreased revision rate) during the second decade following the introduction of HXLPE for THA. Acute infection is unlikely considering the chronicity of symptoms. The radiographs show no obvious evidence of cup loosening. A pseudotumor attributable to trunnionosis, while reported, remains an infrequent clinical issue.
Question 17
Figure 1 is the radiograph of a 21-year-old college lacrosse player who has a 2-year history of progressive left groin pain that is exacerbated by activity. Pain is preventing him from participating with his team. Examination reveals a fit man without tenderness to palpation around the hip. No clicking or popping occurs with hip range of motion. Strength of all muscles about the hip is normal, but there is some mild pain with resisted hip flexion and hip adduction. While lying supine, progressive hip flexion with internal rotation and adduction reproduces his groin pain. The patient participates in physical therapy for 8 weeks with his team's trainer but notes little improvement. What is the most appropriate next diagnostic step to determine the cause of his pain?

Explanation
used to diagnose labral pathology. Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result in a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has important functions for hip stability and maintenance of the suction seal of the joint.
Question 18
The parents of a 14-year-old female soccer player are concerned about any future injury. They have been advised that she has the potential to play for the US Olympic team. They are especially concerned about the anterior cruciate ligament (ACL). What should you advise them? Review Topic
Explanation
Question 19
Figures 1 and 2 are radiographs of a 25-year-old man who has had persistent right hip pain for over a year. There was an acute injury and the pain has progressively worsened and is now 9/10 in severity. The pain interferes with activities of daily living and the patient's capacity to participate in sports. The patient has failed nonsurgical treatment in the form of physical therapy and activity modification. On physical examination, forward flexion is limited to 90°, internal rotation is limited to 10°, and flexion adduction internal rotation examination is positive. The hip pain was relieved on physical examination after intra-articular administration of local anesthetic. The patient had an MRI and CT scan. What is the most appropriate surgical option?
Explanation
A. Belly press
B. Hornblower's test
C. External rotation strength
D. Empty can test
A fall on an outstretched upper extremity can commonly result in a traumatic rotator cuff tear. The images require appropriate interpretation of an acute subscapularis tendon rupture with medial subluxation of the biceps tendon. Subscapularis tendon tears result in a positive belly press or lift-off test. Hornblower's tests for external rotation strength with the arm abducted 90° (teres minor weakness). Empty can tests supraspinatus strength. External rotation strength with the arm at the side tests for infraspinatus weakness.
38- Videos 1 and 2 are the coronal plane MRI scan and arthroscopic evaluation of a 48-year-old woman with 2 weeks of posterior knee pain after feeling a “pop” in the knee while climbing stairs. Physical examination reveals passive range of motion of +5° to 120°, with pain limiting her in terminal extension. Failure of surgical repair of the injured structure is most associated with
A. poor vascularity of the injured tissue.
B. BMI >35 kg/m^2.
C. valgus alignment >5°.
D. repair technique. 30
The MRI scan and surgical video are showing an example of a posterior medial meniscal root tear/avulsion. Many studies have shown successful treatment of these tears with repair using various techniques and minimal progression to osteoarthritis (OA). Most studies exclude patients with high BMI. Brophy and associates demonstrated in their series that high BMI was associated with higher rates of clinical OA and need for subsequent surgery.
Multiple studies in the literature demonstrate good results with a variety of techniques. A valgus alignment in this setting would be considered protective, as opposed to a varus alignment >5°, which has also been associated with worse outcomes. The vascularity of the meniscus is consistently poor throughout most of its volume, including the root, and is not considered to be significantly different from person to person and should affect all root repairs equally.
39- A 47-year-old man who is an avid tennis player and laborer has had one year of shoulder pain and weakness. His pain occurs at night and radiates to the deltoid laterally. The patient denies any anterior based pain. He reports no prior surgeries and has been managed with steroid injections and physical therapy. On examination, he has full passive motion with significant weakness with external rotation. His neurologic examination is unremarkable. MRI evaluation reveals a posterior- superior rotator cuff tear with Goutallier grade 4 fatty infiltrate in the supraspinatus and infraspinatus with retraction beyond the glenoid. He is concerned about the lack of rotation of his arm and reports that this disability creates significant disability with his occupation as a mason. What is the best next step?
A. Shoulder arthroscopy and subacromial decompression
B. Tendon transfer
C. Total shoulder arthroplasty
D. Reverse total shoulder arthroplasty
In younger active patients, tendon transfer is considered a preferable treatment option. The patient has failed a course of nonoperative management. Subacromial decompression may offer pain relief but may not be advisable in a patient with rotator cuff deficient shoulder. A total shoulder arthroplasty requires functionality of the supraspinatus and infraspinatus. A reverse total shoulder is an option to alleviate pain and perhaps improve forward flexion height and strength; however, reverse arthroplasty would not improve external rotation in this patient, and there is concern for longevity of the implant in younger patient populations.
40- A multicenter prospective study of 7,500 patients that assesses differences in rerupture rates after anterior cruciate ligament (ACL) reconstruction using hamstring autograft shows a decreased rate of rerupture when the graft diameter is >9.0 mm versus <9.0 mm (p = 0.05). A follow-up study done at a single institution of 200 patients fails to show any difference in rerupture rates based upon graft size. If the multicenter trial is assumed to be accurate, which statistical error occurred in the follow-up study?
A. Type-I error
B. Type-II error
C. Selection bias
D. Alpha error
Type-II errors, or beta errors, occur when the null hypothesis is accepted and should have been rejected. An underpowered study is at risk of this type of error. Power is defined as 1-probability of a type-II (beta error), and this is generally set at a level of 80% for most studies. The type-II error occurs when a study concludes that there is no association between the studied variables when in fact one exists. The type-I error, or alpha error, is defined as rejecting the null hypothesis when it should have been accepted. Alpha errors occur when a study suggests an association does exist when in reality it does not. Selection bias occurs when proper randomization is not achieved and therefore, the study cohort is not representative of the population intended to be analyzed.
41- A 17-year-old male soccer player sustains repeated lateral patellar dislocations refractory to physical therapy, bracing, and taping. After a workup including radiographs and MRI, the orthopaedic surgeon considers an isolated tibial tubercle osteotomy (TTO). A 60-degree anteromedialization is planned to address instability and to unload the patellofemoral joint. What is a relative contraindication to this procedure?
A. Grade III chondrosis of the proximal patella
B. Caton-Deschamps ratio of 1:1
C. Tibial tubercle-trochlear groove (TT-TG) distance of 21 mm
D. Q angle of 17°
TO is a common treatment for patellofemoral instability. The angle of correction must be customized to each patient’s anatomy. For this patient, the orthopaedic surgeon plans an osteotomy that will both anteriorize and
medialize the tubercle. This will consistently result in a change of 32
patellofemoral kinematics and contact pressures. Medialization decreases lateral and increases medial patellofemoral contact pressures, and anteriorization shifts contact pressures from distal to proximal. Significant anteriorization may not be desired in a patient with proximal patellar chondrosis unless a concomitant chondral procedure is performed as well. The patellar height (Caton-Deschamps ratio) is normal, precluding the need for distalization but not medialization. The TT-TG distance, at more than 20 mm, is a strong indication for osteotomy. The Q angle, although a less precise indicator of malalignment, is also elevated and would be considered an indication for osteotomy.
42- During preseason training camp, a 23-year-old football player comes to the sideline complaining of nausea, dizziness and headache after a 2- mile run. Vital signs include blood pressure 110/80, heart rate 115 bpm and core body temperature of 39°C (102°F). He is otherwise alert and oriented. What is the recommended initial treatment?
A. Immediate ice water bath immersion
B. Immediate return to training
C. Rehydration with a carbohydrate- electrolyte beverage
D. Emergent transportation to a local emergency department
The patient has exertional heat exhaustion (EHE). In cases of exertional heat illness with elevated core body temperature, it is critical to differentiate between EHE and exertional heat stroke (EHS). Patients suffering from EHE often complain of dizziness, nausea, cramping and headache. Vital signs can show mild tachycardia and normal to low blood pressure. EHS is defined by elevated core body temperature >40°C (104°F) and organ failure. Rapid cooling is critical in the setting of EHS, but not EHE. In the setting of EHE, the patient should be placed in a cool, shaded area and given fluids. Studies suggest that the presence of carbohydrate (<8%) in combination with electrolytes mildly promotes fluid retention better than drinking water alone.
43- Surgical repair of the injury shown in the MRI scans in Figures 1 through 4 through a single-incision approach has a higher incidence of
Question 20
A 23-year-old college basketball player reports persistent lateral ankle pain after sustaining an inversion injury 6 months ago. Examination reveals pain over the anterolateral ankle, absence of swelling, and no clinical instability. Management consisting of vigorous physical therapy fails to provide relief, and a intra-articular corticosteroid injection provides only temporary relief. Radiographs obtained at the time of injury and subsequent AP and varus stress views are normal. A recent MRI scan fails to show any abnormalities. Management should now include
Explanation
REFERENCES: Ferkel RD, Fasulo GJ: Arthroscopic treatment of ankle injuries. Orthop Clin North Am 1994;25:17-32.
Ferkel RD, Karzel RP, Del Pizzo W, Friedman MJ, Fischer SP: Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440-446.
Question 21
Which specific legislative Act in the United States was created to require reporting of annual monetary gifts or compensation of more than $10 by orthopaedic implant companies to physicians?
Explanation
Under this Act, all manufacturers of drugs and devices covered under Medicare, Medicaid, and SCHIP are obliged to federally report payments beyond $10 annually to physicians and academic centers. The Act was first introduced in 2007, enacted in 2010, and in 2014 the first data (from 2012) was reported publicly online in the Open Payment Program of the Centers for Medicare and Medicaid Services website.
Samuel et al analyze orthopedic surgeons available data from the Sunshine Act regarding industry payments and find over 110 million USD paid to approximately 15,000 orthopedic surgeons over the 5-month study period. No long term data exists to determine if these payments have any affect in healthcare.
Incorrect Answers:
Question 22
A study is conducted to measure the difference in bone mineral density between postmenopausal women taking a drug treatment versus those taking a placebo. What is the most important result to be reported from this study?
Explanation
(ie, the means and standard deviations).
REFERENCE: Ebramzadeh E, McKellop H, Dorey F, et al: Challenging the validity of conclusions based on P-values alone: A critique of contemporary clinical research design and methods. Instr Course Lect 1994;43:587-600.
Question 23
A 72-year-old woman is scheduled to undergo right total hip arthroplasty. Her preoperative radiograph is shown in Figure below. To avoid increasing this patient’s combined offset while maintaining her leg length, what is the most appropriate surgical plan?
Explanation
The management of patients with proximal femoral deformity can be difficult. Appropriate implant selection and preoperative templating are critical. In this patient, it would be difficult to avoid increasing the combined offset by too much, which could contribute to the overtensioning of the soft tissues and trochanteric pain. By medializing the acetabular component (decreasing the combined offset), using a low offset femoral component or a cemented component placed more valgus (decreasing the combined offset), and making a longer neck cut (to avoid shortening of the lower extremity), restoration of the patient’s native offset and leg length can be achieved.
Question 24
03 Which of the following findings is one of the diagnostic criteria for diffuse idiopathic skeletal hyperostosis?
Explanation
Diffuse idiopathic skeletal hyperostosis is a common disease, most prevalent in those over 50 years of age. The usual presentation is a middle-aged or older patient with chronic mild pain in the middle to lower back, spinal stiffness, and typical radiographic changes in the thoracic spine. Diffuse idiopathic skeletal hyperostosis is predominantly a radiographic diagnosis with 3 major diagnostic criteria. 1. Flowing ossification along the anterolateral aspect of at least four contiguous vertebrae. 2. Preservation of disk height in the involved vertebral segment; the relative absence of significant degenterative changes, such as marginal sclerosis in vertebral bodies or vacuum phenomenon. 3.
Absence of facet-joint ankylosis; absence of sacroiliac erosion, sclerosis, or intra-articular osseous fusion. Treatment is typically non-operative, with anti-inflammatories, activity modification and PT.
back to this question next question
Question 25
A 48-year-old male is involved in a motorycycle accident and arrives in the trauma bay in hypovolemic shock. He receives 6 units of packed red blood cells during his resuscitation. Which of the following viral microbes is he most at risk of exposure from the transfusions?

Explanation
Question 26
A 15-year-old girl reports a 6-month history of activity-related knee pain and swelling. A radiograph, MRI scan, and biopsy specimen are shown in Figures 21a through 21c. What is the most likely diagnosis?
Explanation
REFERENCES: Huvos AG: Bone Tumors: Diagnosis, Treatment, and Prognosis. Philadelphia, PA, WB Saunders, 1991, pp 295-313.
Lin PP, Thenappan A, Deavers MT, et al: Treatment and prognosis of chondroblastoma. Clin Orthop Relat Res 2005;438:103-109.
Question 27
A 45-year-old right-hand dominant woman falls onto an outstretched left hand. Imaging shows a complex elbow dislocation. The postreduction CT scan demonstrates a reduced joint, comminuted radial head fracture, and type I coronoid fracture. Surgical intervention is recommended to address the involved structures. Which component of the intervention adds the most rotational stability?
Explanation
A. Improved longevity in comparison to the linked prosthesis
B. A significantly larger flexion-extension arc
C. A higher incidence of postsurgical instability
D. Lower frequency of ulnar nerve dysfunction
TEA is a popular option for treatment of end-stage elbow arthritis for elderly, lower-demand patients with rheumatoid arthritis. Good success rates have been published by several authors. The clear benefit of the current nonconstrained prosthesis has yet to be proven. Plaschke and associates investigated the Danish National Patient Registry to compare the longevity of the 2 types of implants. These authors found similar survival rates associated with both linked and unlinked implants at 10 years (88% and 77%, respectively). However, studies have documented an approximate 20% incidence of postsurgical instability with nonconstrained implants.
Question 28
A 65-year-old woman with rheumatoid arthritis is undergoing revision total knee arthroplasty (TKA) during which the medial collateral ligament (MCL) is damaged. Suture anchors are used to attempt primary repair, and a varus-valgus constrained insert also is used. Postsurgically she experiences instability that does not respond to bracing with a 3+ opening to valgus stress (Figure 120). What is the most appropriate surgical option?
Explanation
MCL repair or reconstruction may be considered in younger, more active patients, but this intervention is technically demanding and produces variable results. Rotating-hinge TKA is associated with good results in a number of small series that include cases performed with MCL insufficiency or absence. A rotating hinge is preferable over a fixed hinge because of decreased stresses on implants imposed by fixed-hinge devices.
Question 29
What is the most common site of metastases from a soft-tissue sarcoma?
Explanation
REFERENCES: Simon SR (ed): Orthopaedic Basic Science. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 219-276.
Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 255-259.
Question 30
A 12-year-old child with L4 myelomeningocele who is schedules for foot surgery has a functioning ventriculoperitoneal shunt and has no history of allergies. Management should include
Explanation
Question 31
Which of the following pharmacologic agents is most likely to adversely affect the success rate of bony union after lumbar arthrodesis?
Explanation
REFERENCES: Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Dimar JR II, Ante WA, Zhang YP, et al: The effects of nonsteroidal anti-inflammatory drugs on posterior spinal fusions in the rat. Spine 1996;21:1870-1876.
Question 32
Figure 52 shows the MRI scan of a 28-year-old baseball pitcher. Examination will most likely reveal which of the following findings?
Explanation
REFERENCES: Piatt BE, Hawkins RJ, Fritz RC, et al: Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-604.
Inokuchi W, Ogawa K, Horiuchi V: Magnetic resonance imaging of suprascapular nerve palsy.
J Shoulder Elbow Surg 1998;7:223-227.
Question 33
In infantile idiopathic scoliosis, which of the following factors suggests progression?
Explanation
REFERENCES: Mehta MH: The rib-vertebra angle in the early diagnosis between resolving and progressive infantile scoliosis. J Bone Joint Surg Br 1972;54:230-243.
Fischgrund JS (ed): Orthopedic Knowledge Update 9. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2008, p 697.
Question 34
A 12-year-old girl with juvenile rheumatoid arthritis (JRA) has had chronic pain and synovitis about the knee that is now well-controlled medically. Examination reveals 20° of valgus at the knee. Knee range of motion shows 10° to 90° of flexion. Treatment should consist of
Explanation
REFERENCE: Rydholm U, Brattstrom H, Bylander B, Lidgren L: Stapling of the knee in juvenile chronic arthritis. J Pediatr Orthop 1987;7:63-68.
Question 35
Figures A and B show routine postoperative radiographs obtained 2 weeks after anterior cruciate ligament (ACL) reconstruction with autologous patellar tendon graft. Based on these findings, what is the next most appropriate action? Review Topic

Explanation
Question 36
A 36-year-old woman with familial neurofibromatosis has an enlarging mass in the posterior thigh. The lesion has slowly increased in size and is now constantly painful. Pressure on the mass causes dysesthesias in the foot. Figures 44a through 44c show T 1 -weighted, STIR, and T 1 -weighted fat-saturated gadolinium scans, respectively. Figure 44d shows a PET scan. What does this lesion most likely represent?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 225-230.
Resnick D (ed): Diagnosis of Bone and Joint Disorders. Philadelphia, PA, WB Saunders, 2002, pp 4218-4235.
Question 37
A 35-year-old man sustained an injury to his lower extremity after falling 10 feet from a ladder; initial management was nonsurgical. He now reports chronic hindfoot and anterior ankle pain. Radiographs are shown in Figures 22a and 22b. Surgical reconstruction of this painful process should consist of
Explanation
REFERENCES: Carr JB, Hansen ST , Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Juliano TJ, Myerson MS: Fractures of the hindfoot, in Myerson MS (ed): Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1297-1340.
Romash MM: Reconstructive osteotomy of the calcaneus with subtalar arthrodesis for malunited calcaneal fractures. Clin Orthop 1993;290:157-167.
Question 38
A 50-year-old man undergoes revision total knee arthroplasty (TKA). The tibial component shown in Figure 153 was retrieved at the time of revision. The wear damage demonstrated on the backside of the tibial component is most likely related to which wear mechanism(s)?
Explanation
Pitting and delamination seen in tibial component retrievals on the bearing surface of a TKA is related to fatigue wear. Backside wear is shown in the photograph; this is where the lot numbers usually are present, but now they are not distinguishable because of backside wear. This wear mechanism is attributable to adhesive and abrasive wear. The nanometer-size particles created by this wear mechanism account for the higher prevalence of osteolysis associated with modular tibial components.
CLINICAL SITUATION FOR QUESTIONS 154 AND 155
Five weeks ago, an 82-year-old man underwent revision total knee arthroplasty (TKA). Three weeks after surgery he had a dental cleaning. The patient now reports 2 days of worsening pain following a long physical therapy session. His C-reactive protein (CRP) level is 15.0 mg/L (reference range, 0.08-3.1 mg/L). Upon examination, there is no drainage and slight effusion, and he has a passive range of motion to 110 degrees. Radiographs are unremarkable.
Question 39
A year-old woman underwent an uncemented medial/lateral tapered femoral placement during a total hip arthroplasty. The orthopaedic surgeon noticed a nondisplaced vertical fracture in the calcar region of the femoral neck during final implant insertion. What is the most appropriate treatment?
Explanation
The recognized treatment for a proximal periprosthetic fracture is to first identify the extent and then optimize the correction of the fracture. Several studies indicate that proximal cerclage wiring is adequate to create "barrel hoop" stability of the proximal femur. Braided cables offer superior stability compared with twisted wires or Luque wires. Finally, the appropriate postoperative treatment is protected
weight bearing for 6 weeks, with periodic radiographs taken at 2-week intervals. Other options such as
cementing the femoral stem and using a revision arthroplasty device are indicated for unstable fractures.
Question 40
What is the most appropriate way to communicate instructions to a family when there is a language barrier?
Explanation
Ideally, professional medical interpreters should be used in situations involving language difficulties. Printed instructions are helpful, but, if there is a language barrier, these instructions cannot substitute for conversing and answering questions. Asking the child to translate (no matter how fluent he or she may be) is suboptimal. Nonmedical staff may not be fluent enough to adequately translate medical terms.

RESPONSES FOR QUESTIONS 14 THROUGH 16
Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
Aspiration, cultures, Lyme serology, and oral amoxicillin
Biopsy, culture, curettage, bone graft, and possible internal fixation
Physical therapy, ibuprofen, and an antinuclear antibody test
Select the most appropriate treatment above to address each clinical scenario below.
Question 41
Which of the following is a contraindication to laminoplasty in a patient with cervical spondylotic myelopathy?
Explanation
REFERENCES: Emery SE: Cervical spondylotic myelopathy: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:376-388.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 235-247.
Question 42
Figure 26 shows the MRI scan of a 60-year-old man who has had groin pain for the past 2 months. The patient reports pain with ambulation, and examination reveals an antalgic gait. He denies any history of steroid or alcohol abuse. Plain radiographs are normal. Management should include
Explanation
REFERENCE: Guerra JJ, Steinberg ME: Distinguishing transient osteoporosis from avascular necrosis of the hip. J Bone Joint Surg Am 1995;77:616-624.
Question 43
Figure 35 is the radiograph of a 37-year-old woman who began having right forefoot pain about 4 weeks ago after increasing her daily running mileage. She denies any specific injury. Upon examination she has tenderness over the medial forefoot with mild swelling. In addition to her activity level, what is the primary etiology of the radiograph finding?

Explanation
Stress fractures are the result of physiological bone response to increased stress. Increased stress on bone triggers an increase in remodeling, which begins with resorption of bone at the site of stress. Ongoing stress can overwhelm bone strength, resulting in a fracture. In the foot this most commonly is seen in the second metatarsal at the junction of the middle and distal thirds. Contributing factors to increased loading of the second metatarsal include hallux valgus (decreased hallux loading transfers to the second metatarsal head), hallux rigidus (offloading of the hallux attributable to pain increases second metatarsal loading), and a long second metatarsal (increased duration of contact during push-off in the stance phase).
RECOMMENDED READINGS
Shindle MK, Endo Y, Warren RF, Lane JM, Helfet DL, Schwartz EN, Ellis SJ.
Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg. 2012 Mar;20(3):167-
Question 44
The decision to perform fasciotomy of the fingers for a hand compartment syndrome is most appropriately made using
Explanation
Compartment syndrome of the hand can result from a variety of factors, including a traumatic event such as crush injury, fracture, vascular insult, a high-pressure injection injury, or an insect or spider bite. The treatment involves decompressive fasciotomy of the involved compartments. The diagnosis of hand compartment syndrome is determined by history, examination, and objective testing. Patients experience pain out of proportion to the injury, along with swelling and tense skin. Pain may occur with passive motion of the metacarpophalangeal joints as the intrinsic muscles are stretched. Invasive intracompartmental pressures can be measured in the compartments of the hand but not in the fingers. Arterial Doppler studies assess arterial blood flow, and an abnormality would be a late finding. MRI would show edema of the hand and fingers, but the decision to perform surgical release is less likely made from the findings. The most appropriate method of determining the need for finger fasciotomy is the history and physical examination.
Question 45
A 24-year-old professional football player underwent surgery for a symptomatic cervical disk herniation with radiculopathy 9 months ago. A current radiograph is shown in Figure 17. He has normal neurologic findings, no pain, and full range of motion. A CT scan shows a solid fusion. When can he expect to return to play?
Explanation
REFERENCES: Thomas B, McCullen GM, Yuan HA: Cervical spine injuries in football players. J Am Acad Orthop Surg 1999;7:338-347.
Torg JS, Ramsey-Emrhein JA: Management guidelines for participation in collision activities with congenital, developmental, or post-injury lesions involving the cervical spine. Clin Sports Med 1997;16:501-530.
Question 46
Figure 59 shows properties of a material being tested for use as an implant. What is represented by the portion of the stress-strain curve from point A to point B?
Explanation
REFERENCES: Vaccaro AR (ed): Orthopaedic Knowledge Update 8. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2005, pp 45-46.
El-Ghannam A, Ducheyne P: Biomaterials, in Mow VC, Huiskes R (eds): Basic Orthopaedic Biomechanics and Mechano-Biology, ed 3. Philadelphia, PA, Lippincott-Raven, 2005, pp 501-503.
Question 47
- Figures 38a & 38b show radiographs of a 40 year old man who underwent a Putti-Platt repair for recurrent dislocations at age 22. He reports increasing pain in the shoulder and limited motion for five years. Examination reveals 130 degrees of elevation and 15 degrees of external rotation. Non-surgical treatment has failed. Treatment should now consist of what?
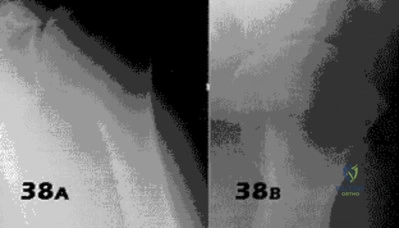
Explanation
Late onset of pain (average 13 years) was noted following this procedure in a small number of patients. The pain is attributed to excessive G-H compressive forces due to limited external rotation. NSAIDS and PT are first line treatments. If these fail, the authors demonstrated good results with release of the anterior structures. Choices 3 & 4 would probably be reserved for patients older than 50 with more advanced signs of degenerative disease.
Question 48
What is the most appropriate initial diagnostic imaging study for a patient with presumed diskogenic low-back pain?
Explanation
Radiography is the best initial study. Vacuum phenomenon may be found within the disk space. Other possible sources for back pain such as osteoporotic collapse, osteolytic collapse, and deformity also can be evaluated. The other tests may be beneficial and are more appropriate as later imaging options.
RECOMMENDED READINGS
Yu WD, Williams SL. Spinal imaging: Radiographs, computed tomography, and magnetic resonance imaging. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine
Question 49
A Trendelenburg gait is most likely to be seen in association with
Explanation
REFERENCES: Fardon DF, Garfin SR, Abitbol J, et al (eds): Orthopedic Knowledge Update: Spine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 323-332.
Andersson GB, Deyo RA: History and physical examination in patients with herniated lumbar discs. Spine 1996;21:10S-18S.
Question 50
Figure 1 shows the radiograph and Figure 2 shows the MRI scan obtained from a 37-year-old woman with a month history of left hip pain. Which combination of a single symptom and examination finding is most likely in this scenario?
Explanation
Question 51
A 22-year-old college basketball player who was hit from behind while going up for a rebound is rendered immediately quadraparetic for approximately 10 minutes, followed by complete resolution of motor loss and return of full sensation. The radiograph and MRI scan of the cervical spine shown in Figures 2a and 2b reveal a canal diameter of 13 mm, loss of cerebrospinal fluid space about the spinal cord, and no signal change within the cord. What is the best course of action?
Explanation
REFERENCES: Cantu R, Mueller FO: Catastrophic spine injuries in football (1977-1989).
J Spinal Disord 1990;3:227-231.
Watkins RG: Neck injuries in football players. Clin Sports Med 1986;5:215-246.
Torg JS, Lasgow SG: Criteria for return to contact activities following cervical spine injury. Clin Sports Med 1991;1:12-26.
Morganti C, Sweeney CA, Albanese SA, Burak C, Hosea T, Connolly PJ: Return to play after cervical spine injury. Spine 2001;26:1131-1136.
Question 52
A 47-year-old man has an acute swollen, red, painful first metatarsophalangeal joint. He denies any history of similar symptoms. What is the first step in evaluation?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 172-173.
Jahss MH: Disorders of the Foot and Ankle, ed 2. Philadelphia, PA, WB Saunders, 1991,
pp 1712-1718.
Question 53
What procedure can eliminate a sulcus sign?
Explanation
REFERENCES: Field LD, Warren RF, O’Brien SJ, et al: Isolated closure of rotator interval defects for shoulder instability. Am J Sports Med 1995;23:557-563.
Cole BJ, Rodeo SA, O’Brien SJ, et al: The anatomy and histology of the rotator interval capsule of the shoulder. Clin Orthop 2001;390:129-137.
Question 54
A year-old woman had a primary total hip arthroplasty 7 years ago that included a proximally coated titanium stem, a cobalt alloy femoral head, a titanium hemispherical acetabular component, and a polyethylene liner. She did well for 4 years but has now had two dislocations and reports pain and weakness around the left hip. She denies any fevers, chills, or constitutional symptoms. On examination, the patient walks well without any signs of an antalgic or Trendelenburg gait. Her abductor mechanism demonstrates good strength. Her erythrocyte sedimentation rate and C-reactive protein level are normal. On radiographs, all components appear well fixed and in good alignment. What is the most appropriate treatment at this time?
Explanation
Trunnionosis is a recently recognized complication following total hip arthroplasty and can occur when a cobalt alloy femoral head is used on a titanium alloy or cobalt alloy femoral stem. Patients often present with pain or swelling around the hip but at times can present with instability. Certain femoral stem designs have been associated with increased reports of trunnionosis. In a patient with a cobalt alloy femoral head who presents with instability, swelling, and weakness around the hip, the potential for trunnionosis and
an adverse local tissue reaction should be considered.
Question 55
Which of the following is a function of siRNA (small interfering RNA)?
Explanation
siRNA are short (usually 20 to 24-bp) double-stranded RNA (dsRNA) sequences with phosphorylated 5' ends and hydroxylated 3' ends. Because of their ability to block a gene of interest, they have been generating interest in the treatment of disease processes that involve gene expression.
Noh et al. study the affects of PD98059, an extracellular signal-regulated kinase 1/2 (ERK1/2) inhibitor, on osteosarcoma. They found that blocking the ERK1/2 pathway with PD98059 induces osteosarcoma cell death by inhibiting a potential drug-resistance mechanism.
Illustration A shows how siRNA works to block translation of mRNA. Incorrect Answers:
Question 56
Figures 55a through 55c are the clinical photograph and radiographs of a 5-year-old boy who fell and injured his right elbow. His radial pulse is thready. Which neurologic deficit most commonly is associated with this injury?
Explanation
This injury is a type III supracondylar humerus fracture with posterolateral displacement. The area of ecchymosis is anteromedial, corresponding to the proximal spike of the humeral metaphysis. The brachial artery is likely tented over this spike, leading to diminished perfusion. The median nerve also resides in this area, and any neurological deficit is likely in its most vulnerable fibers, those of the anterior interosseous nerve (AIN). The AIN contains no sensory fibers, and its motor function involves flexion of both the thumb IP joint and the index distal IP joint.
First dorsal web space anesthesia and an inability to extend the fingers would indicate radial nerve neuropraxia, which would be more likely with posteromedially displaced fractures and lead to anterolateral ecchymosis. Finger abduction is controlled by the ulnar nerve, which most often is injured in flexion injuries and iatrogenically by medially placed pins.

Question 57
Figures 61a and 61b show the CT and MRI scans of a 40-year-old man who has hip pain. He undergoes total hip arthroplasty and curettage and cementation of the lesion as shown in Figure 61c. Histopathologic photomicrographs of the curettage specimen are shown in Figures 61d and 61e. What is the best course of treatment?
Explanation
REFERENCES: Weber KL, Pring ME, Sim FH: Treatment and outcome of recurrent pelvic chondrosarcoma. Clin Orthop Relat Res 2002;397:19-28.
Pring ME, Weber KL, Unni KK, et al: Chondrosarcoma of the pelvis: A review of sixty-four cases. J Bone Joint Surg Am 2001;83:1630-1642
Question 58
-A likely candidate for treatment with a thoracic lumbosacral orthosis scoliosis brace is seen in
Explanation

Question 59
Familial (Leiden) thrombophilia is of importance in joint arthroplasty because of an abnormality in the clotting cascade. Which of the following statements best describes the condition?
Explanation
Question 60
A 25-year old right-hand dominant professional baseball pitcher complains of posteromedial right elbow pain that is worsened by throwing. He also reports occasional paresthesias in his small and ring finger after lengthy bullpen sessions. On examination, he is tender along the medial olecranon and complains of pain when extending the elbow >- 20° of extension. He has negative valgus stress, moving valgus stress, and milking maneuver tests. He is stable to varus stress, chair rise, and lateral pivot shift tests. Radiographs reveal a small osteophyte along the posteromedial border of the olecranon. What is the most likely diagnosis?
Explanation
A. Lateral head of triceps (radial nerve) and brachialis (musculocutaneous nerve)
B. Lateral head of the triceps (radial nerve) and biceps brachii (musculocutaneous nerve)
C. Lateral brachialis (radial nerve) and medial brachialis (musculocutaneous nerve)
D. Brachialis (musculocutaneous nerve) and coracobrachialis (musculocutaneous nerve)
Question 61
Which of the following mechanisms is considered the most common cause of failure of osteoarticular allografts used for articular reconstruction?
Explanation
REFERENCES: Meyers MH, Akeson W, Convery FR: Resurfacing of the knee with fresh osteochondral allograft. J Bone Joint Surg Am 1989;71:704-713.
Beaver RJ, Mahomed M, Backstein D, Davis A, Zukor DJ, Gross AE: Fresh osteochondral allografts for posttraumatic defects in the knee: A survivorship analysis. J Bone Joint Surg Br 1992;74:105-110.
Question 62
A 19-year-old man sustains a low-velocity gunshot wound to the forearm. What factor most strongly correlates with the development of compartment syndrome after this injury?
Explanation
REFERENCES: Moed BR, Fakhouri AJ: Compartment syndrome after low-velocity gunshot wounds to the forearm. J Orthop Trauma 1991;5:134-137.
Hahn M, Strauss E, Yang EC: Gunshot wounds to the forearm. Orthop Clin North Am 1995;26:85-93.
Question 63
Video 1 shows a 20-year-old right-hand dominant man with a 6-month history of left wrist pain and popping that has failed nonsurgical measures. No other positive findings upon examination are noted. What is the most appropriate course of treatment?
Explanation
A. Abductor pollicis longus reconstruction with palmaris autograft
B. Extensor pollicis brevis repair
C. Extensor pollicis longus (EPL) repair
D. Extensor indicis proprius (EIP) to extensor pollicis longus tendon transfer
The EPL is the only tendon that will lift a thumb off of a table as described. It is the most frequently ruptured tendon associated with distal radius fractures. Rupture is more common with nondisplaced fractures. Rupture after a nondisplaced or minimally displaced fracture suggests an ischemic etiology. The patient will not be able to lift her thumb off of a table with her hand lying flat, palm-down. Direct repair is often difficult because of retraction of tendon ends, atrophy, and fraying. The EIP has a similar amplitude and direction of pull. Prerequisites for the use of the EIP to EPL tendon transfer include independent extension of the index finger.
15- Figure 1 is the clinical photograph of a very functional 17-year-old boy with cerebral palsy and quadriplegia. He has no active supination but has full passive supination. His ability to determine position and sensibility without visual input are good. Radiographs show no osseous malalignment. Which treatment can best improve this patient's function?
A. Physical therapy for supination strengthening
1- Figures 1 through 3 are the radiographs of a 40-year-old woman who sustained a minor injury to her left ring finger. Prior to this injury she was asymptomatic, but she now notes pain and swelling. What is the best course of treatment?
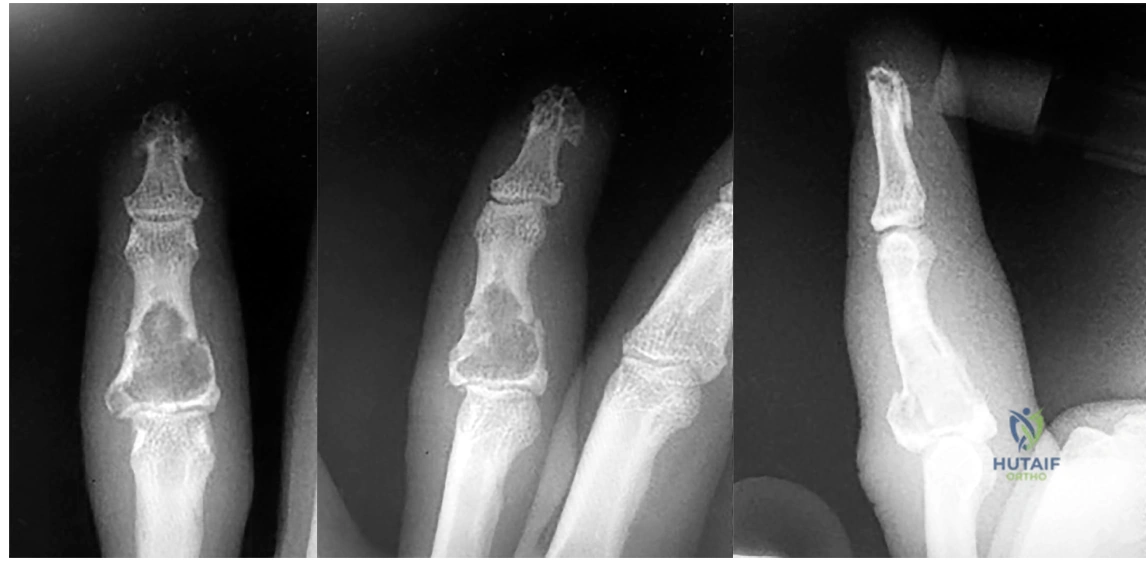
A. Observation only
B. Fluoroscopic-guided intralesional steroid injection followed by serial radiographs
C. Immediate curettage without bone grafting
D. Splint immobilization with curettage and possible grafting after the fracture has healed
This patient has a fracture of the middle phalanx attributable to the presence of an enchondroma. Enchondromas are the most common benign bone tumor affecting the hand. This particular enchondroma has thinned the cortices extensively so that even minor trauma can cause a pathologic fracture. Observation is not the best treatment because a fracture is present, and, at a minimum, the digit should be immobilized.
Question 64
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Explanation
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 65
In the anterior approach (Smith-Petersen) to the hip, dissection is carried out between muscles innervated by the
Explanation
REFERENCES: Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 82-85.
Williams PL, Warwick R, Dyson M, Bannister LH: Myology, in Gray’s Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 638-639.
Question 66
Which clinical sign is the most sensitive for the diagnosis of compartment syndrome in a child with a supracondylar humerus fracture?

Explanation
Bae et al reviewed thirty-six cases of compartment syndrome in 33 pediatric patients. Approximately 75% of these patients developed compartment syndrome in the setting of fracture. "They found pain, pallor, paresthesia, paralysis, and pulselessness were relatively unreliable signs and symptoms of compartment syndrome in these children. An increasing analgesia requirement in combination with other clinical signs, was a more sensitive indicator of compartment syndrome."
Whitesides et al summarizes the diagnosis and treatment of acute compartment syndrome. They emphasize the need for early diagnosis, as "muscles tolerate 4 hours of ischemia well, but by 6 hours the result is uncertain; after 8 hours, the damage is irreversible." They recommend fasciotomy be performed when tissue pressure rises past 20 mm Hg below diastolic pressure.
Question 67
A 30-year-old patient reports chronic medial knee pain and swelling. Figure 9a shows an articular cartilage lesion observed during arthroscopy. The surgeon decides to treat the lesion with the microfracture technique seen in Figure 9b. A biopsy of the repaired tissue 1 year after treatment is likely to show which of the following findings?
Explanation
REFERENCES: Buckwalter JA, Mankin HJ: Articular cartilage: Degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect 1998;47:487-504.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 471-488.
Question 68
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty? Review Topic
Explanation
Question 69
A 47-year-old woman with no history of trauma has had a painful, stiff shoulder for the past 3 months. Treatment consisting of subacromial injection and nonsteroidal anti-inflammatory drugs has been ineffective. Her active range of motion is painful and is limited to 90 degrees of abduction, 60 degrees of elevation, 30 degrees of external rotation, and internal rotation to the posterior superior iliac spine. Plain radiographs of the cervical spine and shoulder are normal. Management at this time should consist of
Explanation
Question 70
Figure 1 shows a radiograph obtained from an active 30-year-old man who sustained an injury to his ring finger 1 week earlier. The most appropriate treatment is

Explanation

Figure 1 reveals evidence of an intra-articular distal phalanx fracture with a distal interphalangeal (DIP) joint dorsal subluxation. This injury is unstable and requires surgical management for an active individual. Volar distal phalanx fractures are often associated with flexor digitorum profundus avulsion injuries, which are addressed concomitantly. This injury was treated with ORIF of the intra-articular fracture, pinning of the DIP joint, and repair of an avulsed flexor digitorum profundus tendon with a button on the dorsal nail plate, as shown in Figure 2. Splint immobilization would not maintain a reduction of this unstable injury. The terminal tendon is not injured in this patient but is often injured in a dorsal distal phalanx fracture with a volar dislocation. Arthrodesis of the DIP is a salvage procedure and would not be considered acutely.
Question 71
A 63-year-old woman has a femoral neck fracture. A biopsy specimen obtained from the fracture site at the time of her hemiarthroplasty reveals metastatic carcinoma. Seven days after surgery, she becomes confused and lethargic. Which of the following laboratory values is most likely implicated in the patient’s symptoms at this time?
Explanation
REFERENCES: Clohishy D: Management of skeletal metastasis in clinical orthopaedics, in Craig E (ed): Operative Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 994-997.
Mundy GR: Hypercalcemia of malignancy revisited. J Clin Invest 1988;82:1-6.
Question 72
Figure 2 shows the radiograph of a 26-year-old auto mechanic who injured his right dominant elbow in a fall during a motocross race. Examination reveals pain and catching that limits his range of motion to 45 degrees of supination and 20 degrees of pronation. The interosseous space and distal radioulnar joint are stable. Management should consist of
Explanation
REFERENCES: Hotchkiss RN: Displaced fractures of the radial head: Internal fixation or excision? J Am Acad Orthop Surg 1997;5:1-10.
Esser RD, Davis S, Taavao T: Fractures of the radial head treated by internal fixation: Late results in 26 cases. J Orthop Trauma 1995;9:318-323.
Question 73
All of the following are true statements regarding compartment syndrome in the pediatric patient EXCEPT:

Explanation
Level 4 evidence by Bae et al reviewed 33 children with compartment syndrome. They found that all 10 compartment syndrome patients that had access to nurse or patient controlled analgesia (PCAs), during their initial evaluation, demonstrated an increasing requirement for pain medication.
Matsen et al reviewed 24 children with compartment syndrome with the most common causes being fracture, vascular injury, and tibial osteotomy. The study concluded that is imperative that a compartment syndrome be identified and treated as promptly as possible.
Question 74
What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?
Explanation
REFERENCE: Parvizi J, Sullivan TA, Trousdale RT, Lewallen DG: Thirty-day mortality after total knee arthroplasty. J Bone Joint Surg Am 2001;83:1157-1161.
Question 75
The AP radiograph of a 5-year-old boy shows a 20-degree left thoracic scoliosis. He was noted by his pediatrician to have asymmetry on a forward bend test. On examination he is neurologically intact except for decreased sensation on the lateral aspect of both flanks and to pinprick in both hands. He has no pain. What is the best initial step in treatment at this time? Review Topic
Explanation
Question 76
Figure 39 shows the radiograph of a 4-month old infant who has been undergoing weekly casting since birth for a congenital equinovarus deformity. Management should now consist of
Explanation
REFERENCES: Lehman WB, Atar D: Complications in the management of talipes equinovarus, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992,
pp 135-136.
Herring JA: Tachdjian’s Pediatric Orthopedics, ed 4. Philadelphia, PA, WB Saunders, 2002,
pp 927-935.
Tachdjian MO: Pediatric Orthopedics, ed 2. Philadelphia, PA, WB Saunders, 1990,
pp 2461-2564.
Question 77
An obese (BMI = 35) 72-year-old woman with diabetes mellitus, hyptertension and a 22-pack-year smoking history is scheduled to undergo posterior spinal fusion from T10 to S1 with a pedicle subtraction osteotomy at L3 for the spinal deformity seen in Figure 1. Which of the following risk factors is most predictive of major complication following surgery Review Topic
Explanation
The surgical treatment of adult spinal deformity often requires multilevel arthrodesis with complex osteotomies including three column osteotomies such as pedicle
subtraction (PSO) and vertebral column resection (VCR). They can involve both anterior and posterior surgical approaches. Surgical time, blood loss, length of hospital stay, and length of recovery can be greater than it is for the more common degenerative conditions.
Auerbach et al. characterized the risk factors for the development of major complications in patients undergoing 3-column osteotomies for adult spinal deformity correction. They also aimed to determine whether the presence of complications affected the ultimate clinical outcome. They found age > 60 years, > or = 3 comorbid conditions and preoperative sagittal imbalance of = 40mm was associated with a major complication. However, the presence of a major complication did not affect the ultimate clinical outcomes at 2 years or more.
Daubs et al. conducted a retrospective analysis of forty-six patients = 60 years of age who underwent major spinal deformity surgery requiring a minimum 5-level arthrodesis procedure to determine the rate of complication and outcomes. The overall complication rate was 37% and the major complication rate was 20%. Increasing age was a significant factor (p<0.05) in predicting the presence of a complication, while presence of comorbidities was found to have no association.
Figure A is a standing preoperative lateral radiograph of the spine demonstrating a thoracic kyphosis of ~25° and thoracolumbar kyphosis of ~25°. Illustration A demonstrates proper sagittal balance after spinal fusion from T10 to S1 and L3 PSO.
Incorrect Answers:
Question 78
Surgical treatment of an adult cavovarus foot with fixed forefoot valgus that does not correct on Coleman block testing should consist of Review Topic
Explanation
Question 79
Which of the following enzymes is used to resorb bone by mature osteoclasts?
Explanation
Question 80
An 8-year-old boy sustains a 100% displaced extension-type supracondylar humerus fracture. Examination reveals no sensory deficit. Capillary refill is approximately 1 second. The patient is unable to flex the index distal interphalangeal joint and the thumb interphalangeal joint. The remainder of the motor examination is normal. Which of the following best explains these physical findings? Review Topic
Explanation
Question 81
An active 47-year-old woman with rheumatoid arthritis reports forefoot pain and deformity and has difficulty with shoe wear. Examination reveals hallux valgus and claw toes. A radiograph is shown in Figure 10. What is the most appropriate surgical treatment?
Explanation
REFERENCES: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 572.
Abdo RV, Iorio LJ: Rheumatoid arthritis of the foot and ankle. J Am Acad Orthop Surg 1994;2:326-332.
Question 82
During reconstruction of insertional gaps of a chronic Achilles tendon rupture, what tendon provides the most direct route of transfer?
Explanation
REFERENCES: Wilcox DK, Bohay DR, Anderson JG: Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot Ankle Int 2000;21:1004-1010.
Wapner K, Pavlock GS, Hecht PJ, Naselli F, Walther R: Repair of chronic Achilles tendon rupture with flexor hallucis longus tendon transfer. Foot Ankle Int 1993;14:443-449.
Question 83
The mother of a 5-year-old child reports that he has had a fever of 103°F (39.4°C), leg swelling, and has been unwilling to bear weight on his right lower leg for the past 7 days. Examination reveals point tenderness at the distal femur. Aspiration at the metaphysis yields 10 mL of purulent fluid, and a Gram stain reveals gram-positive cocci. In addition to hospital admission, management should include
Explanation
REFERENCE: Kasser JR (ed): Orthopaedic Knowledge Update 5. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 149-161.
Question 84
What factor is considered one of the early changes in osteoarthritic cartilage?
Explanation
The normal regulation of a cartilage surface is a delicate balance of degradation and synthesis. When this normal regulation of the cartilage is disturbed, a proinflammatory state tips the cellular pathway in the direction of degradation. The proinflammatory state upregulates the production of cytokines and proteolytic enzymes, specifically matrix metalloproteinases. These enzymes attack the proteoglycan content of the cartilage, leading to an overall reduction in the proteoglycan content. This reduction in content leads to increased permeability of the cartilage substrate. With increased permeability, water is able to move into the cartilage itself, thereby increasing the overall water content within the cartilage in an arthritic state. Finally, because of the increased permeability and increased water content, the overall load or pressure placed on the underlying solid matrix is increased. Increased water content, decreased proteoglycan content, and an increased load on the solid matrix are typical of an osteoarthritic process within normal cartilage. Therefore, the only correct option is that the cartilage has an increased amount of permeability in osteoarthritis.
Question 85
A patient reports hyperesthesia over the base of the thenar eminence following volar locked plating of a distal radius fracture. A standard volar approach of Henry was used. What is the most likely cause of the hyperesthesia?
Explanation
REFERENCES: Jupiter JB, Fernandez DL, Toh CL, et al: Operative treatment of volar intra-articular fractures of the distal end of the radius. J Bone Joint Surg Am 1996;78:1817-1828.
Hoppenfield S, deBoer P (eds): Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia, PA, JB Lippincott, 1994, pp 156-176.
Question 86
An 80-year-old woman notes a painless mass posterior to her left knee. MRI scans are shown in Figures 31a and 31b. What is the best course of action?
Explanation
REFERENCES: Dlabach JA: Nontraumatic soft tissue disorders, in Canale ST (ed): Campbell’s Operative Orthopaedics, ed 10. Philidelphia, PA, Mosby, 2003, vol 1, pp 885-969.
Fritschy D, Fasel J, Imbert JC, et al: The popliteal cyst. Knee Surg Sports Traumatol Arthrosc 2006;14:623-628.
Question 87
Which of the following findings is a prerequisite for a high tibial valgus osteotomy for medial compartment gonarthrosis?
Explanation
REFERENCES: Naudie D, Bourne RB, Rorabeck CH, Bourne TT: The Insall Award: Survivorship of the high tibial valgus osteotomy. A 10- to 22-year followup study. Clin Orthop 1999;367:18-27.
Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 255-264.
Question 88
Which of the following medications has been shown to improve skeletal muscle regeneration and decrease fibrosis following muscle injury in an animal model? Review Topic
Explanation
Skeletal muscle undergoes a natural process of healing and regeneration after injury. The formation of fibrous tissue in place of normal muscle is also part of this process. However, fibrous tissue in place of muscle can predispose the area to re-injury and impaired function. Administration of angiotensin II receptor blockade medications (e.g. losartan) after skeletal muscle injury has been shown to decrease the apoptotic cascade response and the formation of fibrous tissue. The mechanism of benefit is thought to be associated with blockade of insulin-like growth factor.
Terada et al. looked at the affect of platelet-rich plasma (PRP) and losartan on muscle healing after contusion injuries. They showed that PRP plus losartan combination
therapy improved overall skeletal muscle healing by enhancing angiogenesis and follistatin expression as well as reducing the expression of phosphorylated Smad2/3 and the development of fibrosis.
Bedair et al. used a rat model to investigate the effect of angiotensin receptor blockade on muscle fibrosis after injury. They found that angiotensin receptor blockade therapy significantly reduced fibrosis and led to an increase in the number of regenerating myofibers in acutely injured skeletal muscle.
Incorrect
Question 89
An adult patient has an 8- x 4- x 10-cm soft-tissue mass located within the adductor compartment of the thigh. Staging studies should consist of
Explanation
REFERENCES: Demetri GD, Pollock R, Baker L, et al: NCCN sarcoma practice guidelines: National Comprehensive Cancer Network. Oncology (Huntingt) 1998;12:183-218.
Pollock R, Brennan M, Lawrence W Jr: Society of Surgical Oncology practice guidelines: Soft-tissue sarcoma surgical practice guidelines. Oncology (Huntingt) 1997;11:1327-1332.
Question 90
Figure 125 is the anteroposterior knee radiograph of a 65-year-old man who has been treated for knee pain for 6 years. His pain is constant and is worse when walking up and down stairs and when sitting for a prolonged period. He has medial joint line tenderness and a positive patellofemoral grind test finding. His knee is stable to varus and valgus stress. A Lachman test result is 2+. He had a trial of nonsteroidal anti-inflammatory medications with good relief until 4 months ago. Physical therapy has provided minimal relief, and he has undergone a series of intra-articular injections with corticosteroids. The last 2 injections each provided 1 week of pain relief. What is the most appropriate next treatment option?
Explanation
Osteoarthritis is a complex disease. Multiple studies have demonstrated a genetic predisposition and critical role of proinflammatory cytokines in the disease process. Osteoarthritis of the knee has a multifactorial pathogenesis. It is age related and affects women more commonly than men. It is also influenced by such factors as obesity, trauma, repetitive use, muscle weakness, and joint laxity. The treatment of osteoarthritis is multimodal.
Nonsurgical treatments include nonsteroidal anti-inflammatory medications, intra-articular injections, weight loss, and physical therapy. Surgical treatments include osteotomy and unicompartmental and TKA.
Question 91
Local administration of recombinant bone morphogenetic protein-2 (rhBMP-2) to patients with type III-A and III-B open tibial shaft fractures at the time of initial surgery has shown all of the following when compared to standard treatment EXCEPT:

Explanation
Question 92
Spontaneous rupture of the extensor pollicis longus tendon is most frequently associated with which of the following scenarios?

Explanation
clinically satisfactory.
The referenced article by Gelb is a review of the etiology and treatment of this injury. He reviews the above discussion and findings.
Question 93
Figures 18a through 18c show the clinical photograph, radiograph, and CT scan of a 21-year-old man who reports persistent pain after injuring his right shoulder 4 months ago. What is the most likely factor associated with this patient’s diagnosis?
Explanation
REFERENCES: Lazarus MD, Seon C: Fractures of the clavicle, in Bucholz RW, Heckman JD, Court-Brown C (eds): Fractures in Adults. Philadelphia, PA, Lippincott Williams and Wilkins, 2006, vol 2, pp 1241-1242.
White RR, Anson PS, Kristiansen T, et al: Adult clavicle fractures: Relationship between mechanism of injury and healing. Orthop Trans 1989;13:514-515.
Question 94
Which of the following is considered the appropriate initial management protocol for an unconscious football player without spontaneous respirations?
Explanation
REFERENCES: McSwain NE, Garnelli RL: Helmet removal from injured patients. Bull Am Coll Surg 1997;82:42-44.
Vegso JJ, Lehman RC: Field evaluation and management of head and neck injuries. Clin Sports Med 1987;6:1-15.
Arndt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-101.
Question 95
When a structure like a long bone is under a bending load, its maximum stress is most dependent on what factor?
Explanation
REFERENCES: Hayes WC, Bouxsein ML: Biomechanics of cortical and trabecular bone: Implications for assessment of fracture risk, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 76-82.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 161-167.
Question 96
Which ligament attaches to the bony fragment identified by the CT image arrows in Figures 42a and 42b?
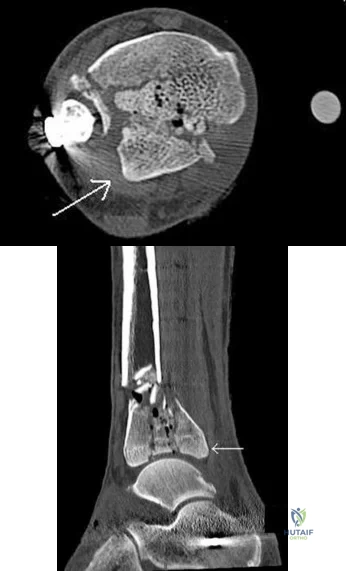
Explanation
The distal tibiofibular syndesmosis is a ligamentous complex that consists of the AITFL, PITFL, intertransverse ligament (ITL), and IOL. The PITFL originates on the posterior inferior aspect of the tibia (Volkmann tubercle) and inserts on the lateral malleolus. The AITFL originates on the anterolateral aspect of the tibia (Chaput tubercle) and inserts on the distal anterior aspect of the fibula (Wagstaffe tubercle). The ITL is a group of fibers running transversely just inferior to the PITFL. As a group, these structures maintain the appropriate tibial plafond and talus relationship throughout physiologic range of motion.
RECOMMENDED READINGS
Carr JB. Malleolar fractures and soft tissue injuries of the ankle. In: Browner BD, Alen LM, Peter TG, Jupiter JB, et al. Skeletal Trauma. 3rd ed. Philadelphia, PA: Saunders; 2003:2309. Zalavras C, Thordarson D. Ankle syndesmotic injury. J Am Acad Orthop Surg.2007 Jun;15(6):330-9. Review. PubMed PMID: 17548882.View Abstract at PubMed
CLINICAL SITUATION FOR QUESTIONS 43 THROUGH 46


A 46-year-old healthy right-hand-dominant man falls and sustains the injury shown in Figures 43a and 43b.
Question 97
Which of the following is considered a disadvantage of knee disarticulation when compared with transfemoral amputation?
Explanation
disarticulation versus transfemoral amputation is the degree of trauma involving the soft tissue around the knee, as increased tissue trauma may lead to painful residual limbs and eventually the need for revision amputation at a higher level. If the residual limb of the knee disarticulation is unable to accommodate the distal-end weight bearing of the socket, then patients with a knee disarticulation may experience decreased levels of function compared with patients undergoing transfemoral amputation.
Question 98
Figure 4 shows the MRI scan of a patient who has had bilateral leg pain, weakness, diffuse numbness, and urinary retention for the past week. Examination reveals that motor strength is diffusely decreased, although it may be secondary to pain. The patient is numb throughout both legs, and reflexes in the lower extremities are absent. Rectal examination shows decreased tone, but voluntary tightening is present. Management should consist of
Explanation
REFERENCES: Kostuik JP, Harrington I, Alexander D, Rand W, Evans D: Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am 1986;68:386-391.
Wisneski RJ, Garfin SR, Rothman RH, Lutz GE: Lumbar disk disease, in Herkowitz HN, Garfin SR, Balderston RA, et al (eds): The Spine, ed 4. Philadelphia, PA,WB Saunders, 1992, vol 1,
pp 613-679.
Question 99
What factor is associated with a high risk of developing pseudotumors after metal-on-metal hip resurfacing?
Explanation
Question 100
- While under a physician’s care, a 45-year-old man verbally abuses the staff and nurses who are attempting to carry out orders. A decision to discharge the patient is best carried out by
Explanation
