OITE & ABOS Orthopedic Board Prep MCQs: Fracture & Shoulder | Part 158

Key Takeaway
This page offers Part 158 of a comprehensive OITE and AAOS Orthopedic Surgery Board Review series. It features 100 verified, high-yield MCQs, mirroring actual exam formats. Designed for orthopedic residents and surgeons, this interactive quiz facilitates rigorous board exam preparation through both Study and Exam Modes, focusing on Fracture and Shoulder topics.
About This Board Review Set
This is Part 158 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 158
This module focuses heavily on: Fracture, Shoulder.
Sample Questions from This Set
Sample Question 1: Examination of a 10-year-old girl with a hypoplastic breast and atrophic pectoralis major may also reveal which of the following findings?...
Sample Question 2: -A patient has a noncomminuted displaced fracture of the radial head with a distal radioulnar dissociation. What is the most appropriate treatment for the radial head?...
Sample Question 3: A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his sho...
Sample Question 4: Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?...
Sample Question 5: An investigation studying whether physical therapy or subacromial injection can be successfully used to treat shoulder pain is conducted. Two groups are identified. One group is prescribed physical therapy, while the other receives a subacr...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Examination of a 10-year-old girl with a hypoplastic breast and atrophic pectoralis major may also reveal which of the following findings?
Explanation
REFERENCES: Wilson MR, Louis DS, Stevenson TR: Poland’s syndrome: Variable expression and associated anomalies. J Hand Surg 1988;13:880-882.
Poland A: Deficiency of the pectoralis muscle. Guys Hosp Rep 1841;6:191.
Question 2
- A patient has a noncomminuted displaced fracture of the radial head with a distal radioulnar dissociation. What is the most appropriate treatment for the radial head?
Explanation
Question 3
A 30-year-old man underwent an open Bankart repair with capsulorrhaphy for recurrent anterior instability 6 months ago. In a recent fall, he described a hyperabduction and external rotation mechanism of injury. He denies dislocating his shoulder. He now has anterior shoulder pain, weakness, and the sensation of instability. Examination reveals tenderness just lateral to the coracoid and bicipital groove. An MRI scan is shown in Figure 31. Management should now consist of
Explanation
REFERENCES: Deutsch A, Altchek DW, Veltri DM, et al: Traumatic tears of the subscapularis tendon: Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med 1997;25:13-22.
Gerber C, et al: Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am 1996;78:1015-1023.
Question 4
Figures 36a and 36b show the MRI scans of a patient who has shoulder weakness. What is the most likely diagnosis?
Explanation
REFERENCES: Resnick D, Kang HS (eds): Internal Derangement of Joints: Emphasis on MR Imaging. Philadelphia, PA, WB Saunders, 1997, pp 308-317.
El-Khoury G: MRI of the Musculoskeletal System. Philadelphia, PA, JB Lippincott, 1998, p 123.
Question 5
An investigation studying whether physical therapy or subacromial injection can be successfully used to treat shoulder pain is conducted. Two groups are identified. One group is prescribed physical therapy, while the other receives a subacromial injection. The groups have similar baseline demographics and shoulder pathologies. Ten patients are randomized in each group and findings show that there is no significant difference in any patient-reported outcome measure. An increase in sample size would reduce the risk of what parameter?
Explanation
Question 6
CLINICAL SITUATION Figures 1 and 2 are the radiographs of a 35-year-old man who is brought into the emergency department after a motor vehicle collision. He is complaining of isolated knee pain. Examination reveals swelling, blood filled blisters, popliteal ecchymosis, joint line pain, and limited knee joint motion. His pulses and sensation are normal. Figures 3 through 8 are the axial and sagittal CT scan sections of the injury. Intra-operative patient positioning for definitive fixation should be

Explanation
femoral condyles remain with the fractured posterior articular pieces while the remainder of the tibia subluxes anteriorly).
Initial management of axially unstable tibial plateau fractures with soft tissue swelling should consist of spanning external fixation and closed manipulative realignment. This allows for soft tissue recovery with the knee joint provisionally stabilized in reduced station. It also provides time for pre-operative planning, which is typically empowered via a CT scan with reconstructions. If the pattern was initially misdiagnosed as a more typically bicondylar tibial plateau fracture, the CT scan will clarify the misconception and allow for better surgical decision making.
Attempting to visualize, reduce, and stabilize a posterior partial articular pattern in the supine position from an anterior approach is fraught with difficulties. Prone positioning is preferred for definitive fixation. Surgical approaches vary, but typically incorporate a posteromedial interval deep to the popliteus and soleus to provide buttress plating to the posterior column of the tibia.
Question 7
A 23-year-old woman has had a 14-month history of ankle pain after surgical treatment of multiple injuries resulting from a motor vehicle accident. Weight bearing began 4 months after surgery. The pain occurs with weight bearing and motion, but there is very little pain at rest. She has no pertinent medical history and does not smoke. Figures 23a and 23b show current radiographs. What is the most appropriate surgical option?

Explanation
Question 8
If the patient had an isolated spine injury without neurologic deficit, the most appropriate next step would be
Explanation
The treatment of thoracolumbar burst fractures has evolved over the years. In the absence of a neurologic deficit or a posterior ligamentous complex injury, nonsurgical treatment is as effective as surgery. The degree of spinal canal compromise is not a risk factor for neurologic symptoms. Similarly, although kyphosis may be a marker of more significant injury, the degree of kyphosis does not correlate with chronic pain. In the setting of a burst fracture, MRI can be used to evaluate the integrity of the posterior ligamentous complex. Polytrauma may be considered a relative indication for surgical intervention in the setting of a stable burst fracture.
RECOMMENDED READINGS
Rechtine GR 2nd. Nonoperative management and treatment of spinal injuries. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S22-7; discussion S36. Review. PubMed PMID: 16685232. View Abstract at PubMed
Shen WJ, Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 1999 Feb 15;24(4):412-5. PubMed PMID: 10065527. View Abstract at PubMed
Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J Bone Joint Surg Am. 2003 May;85-A(5):773-81. Erratum in: J Bone Joint Surg Am. 2004 Jun;86-A(6):1283. Butterman, G [corrected to Buttermann, G]. PubMed PMID: 12728024. View Abstract at PubMed
Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014 Jan;14(1):145-64. doi: 10.1016/j.spinee.2012.10.041. Review. PubMed PMID: 24332321.View Abstract at PubMed
Question 9
The patient experiences little improvement with activity modification and more physical therapy. An intra-articular corticosteroid injection provides excellent relief, but relief only lasts for 1 month. The player requests further treatment for his hip and is counseled regarding surgical intervention. Hip arthroscopy is performed. Intrasurgically, a capsulolabral separation is observed with an underlying pincer lesion. No articular cartilage injury is seen. Which treatment is most appropriate considering these findings?
Explanation

Video 67 for reference
This clinical scenario describes a patient with FAI attributable to pincer (acetabular) deformity. This form of FAI, which involves prominence of the anterosuperior acetabular lip, may be more common among women. Decreased range of motion and pain occur secondary to the abutment of the femoral head against the acetabular labrum and rim. Hip flexion, combined with adduction and internal rotation, recreates this contact and causes pain, but CAM or pincer etiology remains unknown.
The differential diagnosis of hip pain in a young athlete includes femoral neck stress reaction/fracture, sacroiliac arthritis, intra-articular loose body, trochanteric bursitis, osteitis pubis, and hernia. No information presented in this scenario suggests any of these causes. Diagnosis of FAI is best performed via MR imaging, with an arthrogram increasing the sensitivity and specificity for labral pathology. An ultrasound may be useful in the diagnosis of dysplasia or for dynamic assessment of a snapping hip, but ultrasound is not commonly used to diagnose labral pathology.
Although concomitant chondral lesions of the femoral head are uncommon, the forced leverage of the anterosuperior femoral neck upon the anterior acetabulum may result a “contra-coup” chondral injury on the posteroinferior acetabulum. This is the most common location of chondral lesions in this scenario. Without bony resection to prevent further impingement, this patient will continue to experience symptoms. Because there is no evidence of femoral neck prominence (CAM lesion), there is no indication for osteoplasty of the femoral neck; resection of the pincer lesion is necessary. This will often require take-down of the labrum in this location. If possible, iatrogenic or traumatic labral tears should subsequently be repaired after pincer debridement because the labrum has important functions for hip stability and maintenance of the suction seal of the joint.
Question 10
A 25-year-old man is unresponsive at the scene of a high-speed motor vehicle accident and remains obtunded. Initial evaluation in the emergency department reveals a left-sided femoral shaft fracture and a right-sided humeral shaft fracture. The cervical spine remains immobilized in a semi-rigid cervical collar, and the initial AP and lateral radiographs obtained in the emergency department are unremarkable. What is the most appropriate management at this time?
Explanation
REFERENCES: Chiu WC, Haan JM, Cushing BM, et al: Ligamentous injuries of the cervical spine in unreliable blunt trauma patients: Incidence, evaluation, and outcome. J Trauma 2001;50:457-463.
Sanchez B, Waxman K, Jones T, et al: Cervical spine clearance in blunt trauma: Evaluation of a computed tomography-based protocol. J Trauma 2005;59:179-183.
Nunez D Jr: Value of complete cervical helical computed tomographic scanning in identifying cervical spine injury in the unevaluable blunt trauma patient with multiple injuries:
A prospective study. J Trauma 2000;48:988-989.
Question 11
A 36-year-old softball player sustains a shoulder dislocation making a diving catch. The shoulder is successfully reduced in the emergency department. A postreduction MRI is shown in Figure 35. What anatomic lesion is a result of the dislocation? Review Topic

Explanation
Question 12
A collegiate football player who sustained a blow to the head during the first quarter of a game is confused for several minutes after the hit but does not lose consciousness. He had two similar episodes in games earlier in the season. When should he be allowed to return to play?
Explanation
REFERENCES: Guskiewwicz KM, Barth JT: Head injuries, in Schenk RC Jr (ed): Athletic Training and Sports Medicine. Rosemont, IL, American Academy of Orthopedic Surgeons, 1999, pp 143-167.
Kelly JP, Rosenberg JH: Diagnosis and management of concussion in sports. Neurology 1997;48:575-580.
Question 13
A 35-year-old man reports the development of a painful 2-cm nodule on his dorsal wrist over the past 3 years. A surgeon excised the lesion with a presumptive diagnosis of a ganglion cyst. Histology sections from the excision are shown in Figures 11a and 11b. What is the most likely diagnosis?
Explanation
REFERENCES: Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St Louis, MO, Mosby, 1995, p 913.
Lucas DR, Nascimento AG, Sim FH: Clear cell sarcoma of soft tissues: Mayo Clinic experience with 35 cases. Am J Surg Pathol 1992;16:1197-1204.
Question 14
A 53-year-old man with insulin-dependent diabetes has the ulcer on his heel shown in Figure 9. Radiographs and an MRI scan are consistent with osteomyelitis of the calcaeus, contiguous with the ulcer itself. Arterial flow to the foot is adequate. Management should consist of

Explanation
Question 15
-A 45-year-old woman sustained a fall from height and has the injury shown in Figures 135a and 135b.A 3-dimensional reconstruction CT scan is shown in Figure 135c. Joint-spanning external fixation is applied on the day of injury. Ten days later, her skin is acceptable for definitive fixation. What is the most appropriate type of fixation for her fracture?
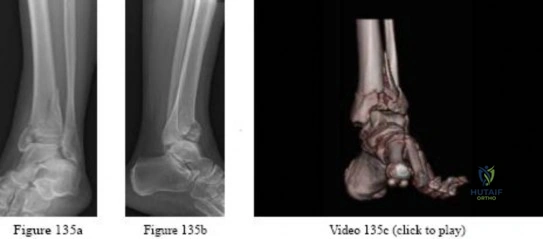
Explanation

Question 16
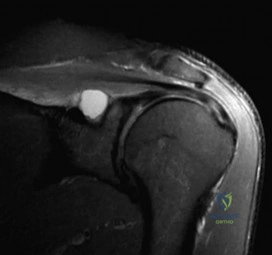
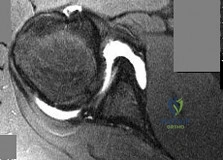
A 24-year-old avid volleyball player has noted gradual onset of shoulder fatigue and weakness limiting his game. Radiographs done by his primary care physician were normal and he has failed to improve with 6 weeks of physical therapy. Given the MRI image shown in Figure A, this patients physical exam may reveal weakness with which of the following actions? Review Topic
Explanation
Extrinsic compression or traction on the suprascapular nerve can result in suprascapular neuropathy. Compression of the nerve may occur at two distinct locations: the suprascapular notch and the spinoglenoid notch. Extrinsic compression of the suprascapular nerve by ganglion cysts can occur at the spinoglenoid notch or, less commonly, at the suprascapular notch. These cysts may originate from the transverse scapular ligament, the fibrous tissue of the scapula, or the glenohumeral joint.
Mittal et al. reviewed the literature and found that the formation of ganglionic cysts in the spinoglenoid fossa occurs with cumulative trauma and leads to entrapment neuropathy of the suprascapular nerve and denervation of the infraspinatus muscle.
Romeo et al. reported on various etiologies of suprascapular neuropathy including traction injury at the level of the transverse scapular ligament or the spinoglenoid ligament and direct trauma to the nerve. They noted that sports involving overhead motion, such as tennis, swimming, and weight lifting, may result in traction injury to the suprascapular nerve, leading to dysfunction. They also reported that the onset of weakness can be subtle and must be differentiated from cervical radiculopathy and degenerative disease of the shoulder.
Figure A depicts a T2 coronal MRI of the shoulder with a cyst easily visualized occupying the suprascapular notch. Illustration A is an algorithm for the management of suprascapular neuropathy. Illustration B is a sagittal MRI from the same patient depicting the ganglion cyst within the suprascapular notch once again leading to atrophy of both the supraspinatus and infraspinatus (asterisks).
Incorrect Answers:
Question 17
Figure below shows the standing AP radiograph obtained from a 55-year-old man who has a 5-year history of daily left knee medial joint line pain with weight-bearing activities. He denies night pain or symptoms of instability. On examination, his range of motion is 0° to 140°. He has a mild, fully correctable varus deformity and a negative Lachman test result. Nonsurgical treatment has failed. What is the UKA survivorship for a 55-year-old patient, compared with the survivorship for total knee arthroplasty?
Explanation
A patient with medial compartment arthritis and a correctable varus deformity with no clinical or examination findings of knee instability most likely has an intact anterior cruciate ligament (ACL). The pattern of medial compartment osteoarthritis most commonly associated with an intact ACL is that of anteromedial osteoarthritis. An incompetent ACL is commonly associated with a fixed varus deformity and radiographic signs of posteromedial wear. An incompetent ACL is a relative contraindication to a mobile-bearing UKA. When evaluating patients for a mobile-bearing UKA, a stress radiograph aids the orthopaedic surgeon in determining the correction of the varus deformity and assessing the lateral compartment. An inability to fully correct the deformity or narrowing of the lateral compartment with valgus stress should influence the surgeon against UKA. Joint registries across the world have shown decreased survivorship associated with TKA and UKA in men compared with other age groups, but survivorship is lower for UKA than for TKA. No studies to date have shown any differences in survivorship between fixed-bearing and mobile-bearing UKAs. The complication that is unique to mobile-bearing UKA is bearing spinout, which occurs in less than 1% of mobile-bearing UKA procedures. In vivo and in vitro polyethylene wear in mobile-bearing UKA are low. Arthritis may progress faster in patients with mobile-bearing UKAs than in those with fixed-bearing UKAs.
Question 18
Figure 1 is the T2 axial MRI scan of a 21-year-old man who was injured while playing for his college football team. His pain was aggravated with blocking maneuvers and alleviated with rest, and he had to stop playing because of the pain. What examination maneuver most likely will reproduce his pain?
Explanation
Question 19
A 70-year-old former baseball catcher reports long-standing pain in the ring and little fingers. A gradient-echo MRI scan is shown in Figure 26. What is the most likely diagnosis?
Explanation
as indicated by the arrow. This technique suppresses the signal of the surrounding fat
and causes the stationary surrounding tissues to become intermediate in signal intensity.
The flowing blood is then easily identified with a bright signal because it does not absorb the radiofrequency pulse. Based on the findings, the diagnosis is an ulnar artery aneurysm, most likely caused by years of repetitive trauma as the result of catching baseballs. Neurolemmoma and giant cell tumor of the tendon sheath would be intermediately enhanced on this image sequence, and the continuity with the ulnar artery, demonstrated here, would not be expected. Lipomas are not enhanced using the gradient-echo technique. The chronic nature of the patient’s symptoms is not indicative of a hematoma, and the hematoma would be dark on this imaging sequence since it is stationary tissue.
REFERENCES: Koman LA, Ruch DS, Patterson Smith B, et al: Vascular disorders, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, vol 2, pp 2254-2302.
Holder LE, Merine DS, Yang A: Nuclear medicine, contrast angiography, and magnetic resonance imaging for evaluating vascular problems in the Hand: Vasospastic disorders. Hand Clin 1993;9:95-113.
Question 20
A 10-year-old soccer player has bilateral heel pain and reports that the pain is worse during and immediately after sports. Examination reveals that the calcaneal tuberosities are painful to palpation bilaterally. What is the most likely diagnosis?
Explanation
REFERENCES: Micheli LJ, Ireland ML: Prevention and management of calcaneal apophysitis in children: An overuse syndrome. J Pediatr Orthop 1987;7:34-38. 500.
FOR ALL MCQS CLICK THE LINK ORTHO MCQ BANK
Question 21
Following a vertebroplasty of L2, cement is noted to protrude directly anterior to the L2 vertebral body. The cement is closest to which of the following structures?
Explanation
and duodenum are anterior to the aorta. The aorta lies in the midline just in front of the
vertebral body.
REFERENCES: Clement CD: Anatomy: A Regional Atlas of Human Anatomy, ed 3.
Baltimore, MD, Munich, Germany, Urban and Schwarzberg, 1987, Figure 331.
Netter FH: Atlas of Human Anatomy. Summit, NJ, Ciba-Geigy, 1989, plate 328.
Question 22
Based on the findings seen in the radiograph in Figure 26, emergent management should consist of
Explanation
REFERENCES: Isenberg J, Prokop A, Schellhammer F, et al: Palmar lunate dislocation. Unfallchirurg 2002;105:1133-1138.
Ruby LK: Fractures and dislocations of the carpus, in Browner BD, Jupiter JB (eds): Skeletal Trauma, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 1367-1372.
Question 23
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Explanation
REFERENCES: Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Salvati EA, Pelligrini VD Jr, Sharrock NE, et al: Recent advances in venous thromboembolic prophylaxis during and after total hip replacement. J Bone Joint Surg Am 2000;82:252-270.
Question 24
Which of the following factors increase the risk of nonunion in midshaft clavicle fractures when treated nonoperatively?

Explanation
The Canadian Orthopaedic Trauma Society in a randomized, prospective study showed that for midshaft fracture in adults with 100% displacement, ORIF results in improved DASH and Constant scores (p = 0.001 and p < 0.01, respectively), lower nonunion (2 vs. 7, p=0.042) & lower malunion (0 vs. 9, p=0.001). Surgery resulted in quicker radiographic union (16.4 weeks vs. 28.4 weeks, p=0.001). However, 15% had hardware and wound complications. At one year, the operative group was more likely to be satisfied with the shoulder in general (p=0.002) and the appearance of the shoulder in particular (p=0.001) in comparison to the nonoperative group.
Prior studies have shown that greater than 2cm of shortening treated non-operatively results in increased fatigueability and poor outcome, but not necessarily nonunion. The Lazarides article concluded that “Final clavicular shortening of more than 18 mm in male patients and of more than 14 mm in female patients was significantly associated with an unsatisfactory result.”
Studies have shown no difference in outcome when treated with a Figure-of-8 harness compared to a simple sling
Question 25
Which of the following provocative tests would most likely be positive in a patient with medial epicondylitis? Review Topic
Explanation
Medial epicondylitis is an overuse syndrome of the flexor-pronator mass. The pronator teres (PT) and flexor carpi radialis (FCR) are thought to be most affected with this condition. It is most common in the dominant arm and occurs with activities that require repetitive wrist flexion/forearm pronation. Patients are most tender over the origin of PT and FCR at the medial epicondyle. Resisting a patient with their fist clenched, wrist flexed and pronated can cause worsening of their pain. This maneuver can be used as a provocative test for this condition.
Cain et al. reviewed elbow injuries in throwing athletes. They comment that the common flexor-pronator muscle origin provides dynamic support to valgus stress in the throwing elbow, especially during early arm acceleration and help produce wrist flexion during ball release.
Amin et al. reviewed the evaluation and management of medial epicondylitis. They report that medial epicondylitis typically occurs in the fourth through sixth decades of life, the peak working years, and equally affects men and women. Physical therapy and rehabilitation is the main aspect of recovery from medial epicondylitis, once acute symptoms have been alleviated.
Illustration A shows a video of this provocative test for medial epicondylitis. Incorrect Answers:
Question 26
What is the most appropriate treatment at this time?
Explanation
Prompt diagnosis and treatment of patients with spinal epidural abscess is crucial to maintain and/or improve neurologic function. This clinical scenario stresses the importance of advanced imaging studies. It is also important to recognize the imaging features of spinal epidural abscess. T1-weighted gadolinium-enhanced images show ring enhancement with a central nonenhancing, low-signal area. In such a case, urgent decompression is indicated. Because of the location of the abscess, which is anterior to the spinal cord, an anterior decompression and reconstruction (ie, fusion) is probably the best treatment plan. Steroids are contraindicated in the presence of an epidural abscess. IV antibiotics alone will not adequately treat a patient with a neurological deficit. A posterior laminectomy and fusion will not safely allow access to the abscess.
RECOMMENDED READINGS
Bluman EM, Palumbo MA, Lucas PR. Spinal epidural abscess in adults. J Am Acad Orthop Surg. 2004 May-Jun;12(3):155-63. Review. PubMed PMID: 15161168. View Abstract at PubMed Ghobrial GM, Beygi S, Viereck MJ, Maulucci CM, Sharan A, Heller J, Jallo J, Prasad S, Harrop JS. Timing in the surgical evacuation of spinal epidural abscesses. Neurosurg Focus. 2014 Aug;37(2):E1. doi: 10.3171/2014.6.FOCUS14120. PubMed PMID: 25081958. View Abstract
at PubMed
This is the last question of the exam.




Question 27
Figures 1 through 3 show the radiograph and MR arthrograms obtained from a 25-year-old woman who has had right groin pain since joining the military 4 years ago. She has undergone treatment with NSAIDs, physical therapy, and activity modification. Examination reveals positive flexion abduction and external rotation, a positive external log roll, and increased range of motion. What is the most appropriate treatment?

Explanation
This patient has symptomatic hip dysplasia that has been recalcitrant to nonsurgical management. Radiographs reveal an upsloping sourcil (acetabular index of 18) and a lateral center edge angle of 14, with posterior uncovering. The MR arthrogram shows no definitive evidence of a labral tear. Appropriate surgical management would include periacetabular osteotomy. Viscosupplementation in the hip is controversial in the treatment of osteoarthritis and plays no role in the treatment of dysplasia. Hip arthroscopy with labral repair is controversial in mild hip dysplasia, with studies demonstrating between 60% and 77% good and excellent results, inferior to the results for hip arthroscopy in a femoroacetabular impingement cohort. In moderate to severe dysplasia, hip arthroscopy is not recommended. Because the acetabular cartilage is well maintained, total hip arthroplasty would not be recommended in this young and active patient.
Question 28
An 18-year-old boy has had pain in the right knee for the past 6 months. Examination reveals some fullness behind the knee but no significant palpable soft-tissue mass. There is no effusion, and he has full knee range of motion. The remainder of the examination is unremarkable. A radiograph and MRI scans are shown in Figures 33a through 33c, and biopsy specimens are shown in Figures 33d and 33e. What is the most likely diagnosis?
Explanation
REFERENCES: Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990, pp 20-21.
Unni KK, Dahlin DC, Beabout JW, Ivins JC: Parosteal osteogenic sarcoma. Cancer 1976;37:2466-2475.
Question 29
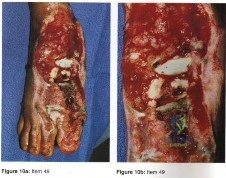
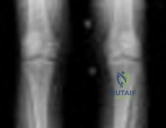
- The radiograph shown in Figure 50a and the CT scan shown in Figure 50b reveal a lesion in the left femoral neck of a 12-year-old boy who has pain in the left hip. The most likely cause of the osteopenia of the left proximal femur is
Explanation
Question 30
A right-handed 20-year-old college baseball pitcher has had a 6-month history of vague right elbow pain while pitching. Examination reveals full flexion of the elbow and a loss of only a few degrees of full extension. The elbow is stable, but palpation reveals tenderness over the olecranon. Plain radiographs are inconclusive. MRI and CT scans are shown in Figures 20a and 20b. Management should consist of
Explanation
REFERENCES: Azar FM, Wilk KE: Nonoperative treatment of the elbow in throwers. Oper Tech Sports Med 1996;4:91-99.
Griffin LY (ed): Orthopaedic Knowledge Uupdate: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 191-203.
Question 31
When comparing mobile-bearing total knee arthroplasty (TKA) to fixed-bearing total condylar arthroplasty, the mobile-bearing procedure provides
Explanation
REFERENCES: Aglietti P, Baldini A, Buzzi R, et al: Comparison of mobile-bearing and fixed-bearing total knee arthroplasty: A prospective randomized study. J Arthroplasty 2005;20:145-153.
Sorrells RB: The rotating platform mobile bearing TKA. Orthopedics 1996;19:793-796.
Dennis DA, Komistek RD: Kinematics of mobile-bearing total knee arthroplasty. Instr Course Lect 2005;54:207-220.
Question 32
A 17-year-old presents with persistent left knee pain after a twisting injury during a soccer match 24 hours ago. On physical exam he has a mild effusion. He has tenderness to palpation on the medial joint line. Lachman test, anterior drawer test and posterior drawer test are attempted but limited secondary to pain. Dial test reveals a side-to-side external rotation difference of roughly 5 degrees. His MRI images are seen in Figures A-D. These findings would be most consistent with: Review Topic

Explanation
Many provocative tests have been described to aid in the diagnosis of meniscus tears.
The Apley test is performed with the patient prone, by axially loading the tibiofemoral joint at 90° of knee flexion. Pain with compression and external rotation (medial meniscus) or internal rotation (lateral meniscus) is considered positive.
The Ege's test is performed by having the patient squat with their knees maximally externally rotated or internally rotated. The test is positive when pain and/or a click is felt by the patient.
The McMurray test is performed by passively moving the knee from flexion to extension while externally or internally rotating the leg. A palpable click at the joint line with external rotation (medial meniscus) or internal rotation (lateral meniscus) is considered positive.
The Thessaly test is performed by supporting the patient as they internally or externally rotate their knee and body while keeping the foot planted, with the knee in 5° of flexion and then 20° of flexion. The test is positive when joint line pain and/or sense of locking/catching is experienced by the patient.
Ryzewicz et al. performed a systematic review of prospective cohort studies comparing magnetic resonance imaging (MRI) and clinical examination to arthroscopy in the diagnosis of meniscus tears. The Apley test, Ege's test, McMurray test and Thessaly test at 5° were shown have high specificity but low sensitivity. Joint line tenderness has a higher sensitivity, but lower specificity. The Thessaly test at 20° demonstrated the highest sensitivity and specificity, although there was only one available study evaluating this test.
Abdon et al. performed a prospective study looking at 68 clinical parameters to
determine which combinations of symptoms and signs indicated the presence of a meniscus tear. They found that joint-line tenderness and mechanical locking were predictive of a meniscus tear, while the McMurray sign did not prove valuable. Pain at rest, sick leave and medial patellar tenderness all negated the presence of a meniscus tear. The clinical accuracy in diagnosing meniscal tears was 61% in this study.
Figures A and B are T1 sagittal MR images demonstrating an intact anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL), respectively. Figures C and D are T2 coronal and sagittal MR images showing a complex tear of the posterior horn of the medial meniscus. Illustration A demonstrates the Ege's test. Illustration B shows the Thessaly test at 5° of flexion.
Incorrect
Question 33
A college basketball player is struck in the eye by a player’s hand while driving to the basket. Fluorescein evaluation reveals the injury shown in Figure 18. Management should consist of
Explanation
REFERENCES: Brucker AJ, Kozart DM, Nichols CW, et al: Diagnosis and management of injuries to the eye and orbit, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face. St Louis, MO, Mosby-Year Book, 1991, pp 650-670.
Zagelbaum BM: Treating corneal abrasions and lacerations. Phys Sports Med 1997;25:38-44.
Question 34
What is the treatment of choice for the injury shown in Figures 20a through 20c?
Explanation
REFERENCES: Prokuski LJ, Eglseder WA Jr: Concurrent dorsal dislocations and fracture-dislocations of the index, long, ring, and small (second to fifth) carpometacarpal joints. J Orthop Trauma 2001;15:549-554.
Lawlis JF III, Gunther SF: Carpometacarpal dislocations: Long-term follow-up. J Bone Joint Surg Am 1991;73:52-59.
Question 35
Figure 1 is the MR image of a 14-year-old football player who injured his right knee during a game. He describes feeling a "pop" and then needing help walking off the field. His knee is visibly swollen. The patient undergoes surgery to repair/reconstruct the damaged structure and has no postsurgical complications and begins physical therapy rehabilitation. The boy and his parents stress they want to “get the therapy over with as fast as possible" to expedite his return to sports, and the surgeon and rehabilitation team consider their request. Compared with nonaccelerated rehabilitation, patients who follow an early accelerated rehabilitation protocol experience

Explanation
Question 36
Which of the following types of ultra-high molecular weight polyethylene has been associated with the poorest clinical performance?
Explanation
REFERENCES: Wright TM, Rimnac CM, Stulberg SD, et al: Wear of polyethylene in total joint replacements: Observations from retrieved PCA knee implants. Clin Orthop 1992;276:126-134.
Landy MM, Walker PS: Wear of ultra-high molecular-weight polyethylene components of 90 retrieved knee prostheses. J Arthroplasty 1988;3:S73-S85.
Skyrme AD, Mencia MM, Skinner PW: Early failure of the porous-coated anatomic cemented unicompartmental knee arthroplasty: . A 5- to 9-year follow-up study. J Arthroplasty 2002;17:201-205.
Question 37
A 15-year-old boy who participates in track reports acute pain along the left iliac crest during a sprint. Examination reveals that the anterior superior iliac spine is nontender. The most likely diagnosis is an injury to the
Explanation
REFERENCES: Clancy WG Jr, Foltz AS: Iliac apophysitis and stress fractures in adolescent runners. Am J Sports Med 1976;4:214-218.
Waters PM, Millis MB: Hip and pelvic injuries in the young athlete, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 279-293.
Lombardo SJ, Retting AC, Kerlan RK: Radiographic abnormalities of the iliac apophysis in adolescent athletes. J Bone Joint Surg Am 1983;65:444-446.
Paletta GA Jr, Andrish JT: Injuries about the hip and pelvis in the young athlete. Clin Sports Med 1995;14:591-628.
Question 38
03 Figure 9 shows the radiograph of a patient who has anterior knee pain and range of motion from 0-of the tibial tubercle. Treatment should consist of

Explanation
The picture shows a laterally subluxed and a relatively-externally rotated patella on a femoral component. The question tells us that the femoral component is internally rotated and the tibial component is perfectly placed. If we know that the femoral component should be externally
rotated about 3 degrees, we know that in this patient, that’s where the problem is. So, we don’t have to do anything to the quads, tubercle or tibial component. We need to revise the femur. Besides, a lateral retinacular release may damage the lateral geniculates; since this patient most likely had a medial arthrotomy, this may devascularize the patella and lead to patellar AVN. A lateral retinacular release will not address the malpositioned components )
back to this question next question
Question 39
The acceleration of an object under the influence of a force depends directly on the mass of the object. The angular acceleration of an object under the influence of a moment depends directly on the
Explanation
REFERENCES: Andriacchi T, Natarajan RN, Hurwitz DE: Musculoskeletal dynamics, locomotion, and clinical applications, in Mow VC, Hayes WC (eds): Basic Orthopaedic Biomechanics, ed 2. New York, NY, Lippincott-Raven, 1997, pp 43-47.
Burstein AH, Wright TM: Fundamentals of Orthopaedic Biomechanics. Baltimore, MD, Williams and Wilkins, 1994, pp 3-7.
Question 40
A 25-year-old woman returns for her first postoperative visit after arthroscopic thermal capsulorrhaphy for recurrent multidirectional instability. Examination reveals that the portals are healed, there is no swelling; and passive range of motion is within the normal range. However, she is unable to actively raise her arm. Shoulder radiographs are normal. What is the most likely cause of these findings? Review Topic
Explanation
Question 41
Figure 88 is the radiograph of a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?
Explanation
Based on the fact that the fracture is occurring around the stem (type B) and the stem is clearly loose (type B2), the appropriate treatment is removal of the in situ stem (which is loose), ORIF of the femur (cerclage wires, cables, or a plate would be acceptable), and insertion of a longer revision stem (a tapered fluted modular titanium or fully porous coated cylindrical stem) to bypass the fracture. All other responses are incorrect because they provide inappropriate treatment options for a Vancouver B2 fracture.
Question 42
A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis? Review Topic

Explanation
Question 43
A 4-year-old boy who was struck by a motor vehicle has a right pneumothorax requiring placement of a chest tube, an open (Gustilo) grade IIIA midshaft fracture of the left femur, and a closed displaced subtrochanteric fracture of the right femur. He also sustained a subdural hematoma that requires neurosurgical intervention. In addition to irrigation and debridement of the left femur, treatment should include
Explanation
Question 44
A B Figures 90a and 90b are MR images of a 34-year-old man who is referred to your office by his primary care physician after failing 4 months of nonsurgical treatment that included epidural steroids for severe right arm pain occurring in a C6 distribution. He also has associated paresthesias in this region. The patient is weak in elbow flexion and wrist extension. What are his likely outcomes if he is treated with a posterior foraminotomy instead of anterior cervical diskectomy and fusion (ACDF)?

Explanation
This patient has a right-sided C5-C6 disk herniation causing C6 radicular symptoms in the right upper extremity. Studies have shown that both ACDF and posterior foraminotomy confer similar results in terms of pain relief and functional outcome. Patients treated with posterior foraminotomy are at higher risk for neck pain and recurrence of radiculopathy at the same level. Those who receive ACDF are at higher risk for occurrence of radiculopathy at an adjacent level.
RECOMMENDED READINGS
Rao RD, Currier BL, Albert TJ, Bono CM, Marawar SV, Poelstra KA, Eck JC. Degenerative cervical spondylosis: clinical syndromes, pathogenesis, and management. J Bone Joint Surg Am. 2007 Jun;89(6):1360-78. Review. PubMed PMID: 17575617. View Abstract at PubMed Bolesta MJ, Gill K. Acute neck pain and cervical disk herniation. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:227-234.
Question 45
A 45-year-old woman with grade II adult-acquired flatfoot deformity has pain on the lateral side of her foot just distal to the tip of the fibula. Which component of a comprehensive flatfoot reconstruction most likely will address the deformity responsible for this pain?
Explanation
Patients develop lateral ankle pain with progression of adult-acquired flatfoot deformity. This is associated with increased hindfoot valgus deformity. Calcaneal fibular impingement has been considered the primary cause of this pain. Studies demonstrate that arthrosis of the posterior facet of the subtalar joint strongly correlates with lateral pain in adult-acquired flatfoot deformity. Both conditions are related to hindfoot valgus deformity. Although lateral column lengthening is a powerful tool for correction of flatfoot deformity, its effect on hindfoot deformity is less defined. Lateral column lengthening provides better correction of the longitudinal arch of the midfoot and realignment of the medial column than other osteotomies. A medializing calcaneal osteotomy has a significant linear effect on hindfoot valgus alignment. Spring ligament reconstruction and medial cuneiform opening-wedge osteotomies have less effect on hindfoot alignment than the medial calcaneal slide.
RECOMMENDED READINGS
Ellis SJ, Deyer T, Williams BR, Yu JC, Lehto S, Maderazo A, Pavlov H, Deland JT. Assessment of lateral hindfoot pain in acquired flatfoot deformity using weightbearing multiplanar imaging. Foot Ankle Int. 2010 May;31(5):361-71. doi: 10.3113/FAI.2010.0361. PubMed PMID:
Question 46
Which of the following factors will adversely affect bone ingrowth in a revision porous-coated stem?
Explanation
REFERENCES: Berry DJ, Harmsen WS, Ilstrup D, Lewallen DG, Cabanela ME: Survivorship of uncemented proximally porous-coated femoral components. Clin Orthop 1995;319:168-177.
Cook SD, Thomas KA, Haddad RJ Jr: Histologic analysis of retrieved human porous-coated total joint components. Clin Orthop 1988;234:90-101.
Spector M: Historical review of porous-coated implants. J Arthroplasty 1987;2:163-177.
Question 47
A 45-year-old man with a painful varus knee is being considered for an upper tibial osteotomy. Which of the following factors is considered the most compelling argument against this procedure?
Explanation
REFERENCE: Kelly MA: Nonprosthetic management of the arthritic knee, in Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 245-249.
Question 48
-Figures 14a through 14d are the radiographs and sagittal T1- and T2-weighted MRI scans of an otherwise healthy 10-year-old girl who has experienced 3 weeks of worsening pain with weight bearing and is now refusing to bear weight to either of her lower extremities. She denies any history of injury or trauma.She has not had any fevers or recent illnesses. She denies any numbness or parasthesias. She has had no bowel or bladder incontinence. In the emergency department she is afebrile and tender to palpation over the midlumbar spine. She has pain with hyperextension and flexion of her back. Her white blood cell count is 11.4 (reference range, 4.5-11.0 x109/L), erythrocyte sedimentation rate is 40 mm/h (reference range, 0-20 mm/h), and C-reactive protein is 2.6 mg/L (reference range, 0.08-3.1 mg/L). What is the most appropriate course of action at this time?

Explanation

Question 49
Figure 35 is the sagittal MR image of a 56-year-old woman who has a 3-year history of severe back pain. Her pain is worse with flexion at the lumbosacral junction and is relieved with extension. She denies any pain in her lower extremities and has no symptoms of neurogenic claudication. Which mediators play roles in the pathogenesis of this condition?

Explanation
The patient has degenerative disk disease with diskogenic back pain. Several studies in both humans and animals have implicated TNF-a, IL-1, and MMP in extracellular matrix degeneration and disk degradation. TGF-ß, BMP-2, latent membrane protein 1, and growth and development factor-5 are all postulated to play anabolic roles in the intervertebral disk. Biglycan is a small leucine-rich proteoglycan that regulates extracellular matrix assembly within the disk. Noggin and gremlin are biochemical factors not involved in disk degradation.
RECOMMENDED READINGS
Kim HT, Yoon ST, Jarrett C. Articular cartilage and intervertebral disk. In: Fischgrund JS, ed. Orthopaedic Knowledge Update 9. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2008:23-33.
Hoyland JA, Le Maitre C, Freemont AJ. Investigation of the role of IL-1 and TNF in matrix degradation in the intervertebral disc. Rheumatology (Oxford). 2008 Jun;47(6):809-14. doi: 10.1093/rheumatology/ken056. Epub 2008 Apr 8. PubMed PMID: 18397957. View Abstract at PubMed
Gruber HE, Ingram JA, Hanley EN Jr. Immunolocalization of MMP-19 in the human intervertebral disc: implications for disc aging and degeneration. Biotech Histochem. 2005 May-Aug;80(3-4):157-62. PubMed PMID: 16298901. View Abstract at PubMed
Question 50
An otherwise healthy 30-year-old man undergoes right shoulder arthroscopic Bankart repair under regional anesthesia using an interscalene brachial plexus block. In the recovery room, he reports mild difficulty breathing and his chest radiograph shows a high riding diaphragm on the right side. His peripheral oxygenation is 97% on 2 liters of oxygen by nasal cannula. What is the most appropriate management?
Explanation
Question 51
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of
Explanation
REFERENCES: Pizzutillo PD, Hummer CD III: Nonoperative treatment for painful adolescent spondylolysis or spondylolisthesis. J Pediatr Orthop 1989;9:538-540.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1996, pp 129-137.
Question 52
While performing long fusion with osteotomies for a patient with adult scoliosis and sagittal plane deformity, the neurophysiologist reports a change in motor-evoked potentials in the lower extremities. What is the most appropriate next step?
Explanation
The use of intraoperative neuromonitoring is expanding, especially in the setting of deformity surgery. Changes in monitoring are concerning for the possibility of a neurologic injury; however, several other factors can alter signals. These include hypotension, changes in anesthesia depth and medications, the use of paralytic agents, and technical issues such as leads falling out or becoming disconnected. If a change in neuromonitoring signals is noted, these factors should be checked first to rule out false-positive findings. If this does not correct the problem, the wound should be explored to ensure there is no compression on the neural elements. Finally, if the deformity has been corrected, some of the correction can be released in an attempt to improve the signals. A wake-up test is difficult to perform and does not provide specific information regarding the location of the problem or how to correct it. Steroids may be used depending on surgeon preference, but should not be used until neurologic injury is ruled out. Any neuromonitoring changes always necessitate immediate investigation.
RECOMMENDED READINGS
Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091. View Abstract at PubMed
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
Review. PubMed PMID: 21102290. View Abstract at PubMed
Question 53
There is increasing concern about the ethical relationship of orthopaedists to the orthopaedic equipment industry. Which of the following describes the most appropriate relationship?
Explanation
REFERENCE: Opinions on ethics and professionalism, in Guide to The Ethical Practice of Orthopaedic Surgery, ed 6. American Academy of Orthopaedic Surgeons, Rosemont, IL, 2006, pp 38-42.
Question 54
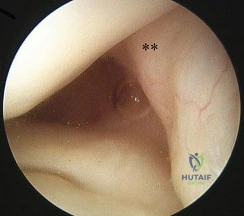
Figure 62 is an arthroscopic view of the intercondylar notch of a right knee from an anterolateral portal. What is the main function of the structure delineated by the black asterisks? Review Topic
Explanation
Question 55
An awake and alert patient with neck pain arrives at the emergency department after an automobile crash. Upon examination he is weak in the left deltoid and biceps muscles (3/5 strength). CT scans performed 2 hours after admission are shown in Figures 70a and 70b. His weakness deteriorates to 1/5 strength in the upper and lower extremities. What is the most appropriate treatment? A B
Explanation
Facet subluxation reduction may be performed in awake patients. Posterior spinal laminectomy and fusion can result in worsening neurologic status and is not recommended in this setting. Generally, corpectomy in the setting of facet subluxation is not recommended because it does not facilitate reduction or fully alleviate spinal cord compression. High-dose steroid use is not supported by current literature.
RECOMMENDED READINGS
Fehlings MG, Perrin RG. The timing of surgical intervention in the treatment of spinal cord injury: a systematic review of recent clinical evidence. Spine (Phila Pa 1976). 2006 May 15;31(11 Suppl):S28-35; discussion S36. Review. PubMed PMID: 16685233. View Abstract at PubMed
Lee AS, MacLean JC, Newton DA. Rapid traction for reduction of cervical spine dislocations. J Bone Joint Surg Br. 1994 May;76(3):352-6. PubMed PMID: 8175833.View Abstract at PubMed
Question 56
A 32-year-old male hockey player who is right-hand dominant was checked from behind and landed with full force into the boards. In the emergency department he reports shortness of breath. Figure 113 shows a 2-D CT scan. What is the best initial treatment for this injury?
Explanation
Question 57
Figures 4a and 4b show the radiographs of a 32-year-old man who has right groin pain with activity or prolonged standing. Which of the following factors would not prohibit consideration of acetabular liner exchange and grafting of the defects?
Explanation
REFERENCES: Maloney WJ, Herzwurm P, Paprosky W, Rubash HE, Engh CA: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 58
A 45-year-old man who is a smoker has a significant hemothorax and bilateral closed femoral fractures. On insertion of a chest tube, 1,100 mL of blood was returned. He has had 75 mL of chest tube output over the last 2 hours while being resuscitated in the ICU. His base deficit is now 2 and his urine output has been 3 mL/kg over the last hour. What is the next most appropriate step in management?
Explanation
REFERENCES: Nork SE, Agel J, Russell GV, et al: Mortality after reamed intramedullary nailing of bilateral femur fractures. Clin Orthop Relat Res 2003;415:272-278.
Pape HC, Zelle BA, Hildebrand F, et al: Reamed femoral nailing in sheep: Does irrigation and aspiration of intramedullary contents alter the systemic response? J Bone Joint Surg Am 2005;87:2515-2522.
Question 59
Figures 21a and 21b show a transverse MRI scan at L4/5 and a lateral radiograph of a 75-year-old man with a 2-year history of worsening low back and bilateral leg pain that occurs with ambulation beyond approximately a half a block. Management consisting of physical therapy, anti-inflammatory medications, and muscle relaxants has failed to successfully resolve his symptoms. He has minimal medical comorbidities. What is the best treatment approach for this patient? Review Topic

Explanation
Question 60
Figures 26a and 26b show the radiograph and MRI scan of an 18-year-old man who fell from a trampoline. Examination reveals exquisite local tenderness at the thoracolumbar junction, but he is neurologically intact. Management should consist of
Explanation
REFERENCES: Carl AL: Adult spine trauma, in DeWald RL (ed): Spinal Deformities: A Comprehensive Text. New York, NY, Thieme, 2003, pp 406-423.
Lewandrowski KU, McLain RF: Thoracolumbar fractures: Evaluation, classification, and treatment, in Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine. Philadelphia, PA, Lippincott Williams and Wilkins, 2004, pp 817-843.
Question 61
-An athletic 30-year-old sustained multiple injuries in a high-speed motor vehicle collision that resulted in a loss of approximately 30% of blood volume. On arrival to the emergency department, the heart rate is100 and blood pressure is 104/62. The best means with which to evaluate true hemodynamic status is
Explanation
Question 62
During placement of an external fixator for a distal radius fracture, the most commonly injured nerve is a branch of which of the following nerves? Review Topic
Explanation
(SBQ12TR.106) A 67-year-old female sustains the injury shown in Figure A after a trip and fall. When discussing the outcomes of surgery with the patient, which of the following statements is true?

Post-surgical mortality rates are significantly lower after total hip arthroplasty compared to hemiarthroplasty
Internal fixation shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to arthroplasty
Bipolar hemiarthroplasty shows better outcomes (reoperation rate, functional status, and/or complication rates) compared to unipolar hemiarthroplasty
A delay in surgery greater than 48 hours is recommended if the patient has multiple medical comorbiditiesm which are not fully optimized
Dislocation rates are equivalent between total hip arthroplasty and hemiarthroplasty
Moderate evidence supports that hip fracture surgery within 48 hours of admission is associated with better outcomes. However, patients with significant medical comorbidity should be fully optimized before surgery.
Although several studies have shown a benefit to surgery within 48 hours, no definitive time frame has been elucidated. The majority of literature has shown improved outcomes in regards to pain, complications, and length of stay with early surgery. Patients with significant medical comorbidities have been shown to have the highest mortality rates.
Moran et al. aimed to determine whether a delay in surgery for hip fractures had an affect on postoperative mortality among elderly patients. In an observational study of 2660 patients, they showed that mortality following hip fracture surgery was 9% at 30-days, 19% at 90-days, and 30% at 12-months. Patients with medical comorbidities had 2.5 times the risk of death within 30-days of surgery. In addition, individuals who had surgery delayed beyond 4 days had increased mortality at 90-days and 12-months.
Papakostidis et al. examined the timing of internal fixation of intracapsular fractures of the neck of femur on the development of late complications, particularly osteonecrosis of femoral head (ONFH) and non-union. They showed no benefit of
early surgery on incidence of AVN. However, delay of internal fixation of more than
24 hours showed increased rates of non-union.
Figure A shows a displaced right femoral neck fracture. Incorrect Answers:
Question 63
A 78-year-old man with ankylosing spondylitis sustains a minor fall. Shortly afterward he experiences sudden worsening of his chronic back pain and is brought to the emergency department by his caregiver. Radiographs and a CT scan of the spine do not show a clear fracture. What is the most appropriate next step?
Explanation
Patients with ankylosing spondylitis are at high risk for occult fractures after low-energy injuries. Although radiographs and a CT scan do not demonstrate a spinal fracture in this patient, high risk for an unstable occult fracture necessitates further imaging with MRI to ensure that no fractures are missed. Although a CT scan is typically the primary imaging modality for workup of spine injuries in similar patients, CT and MRI complement each other and each detects fractures that are missed using the other modality. A CT myelogram might detect cord or root compression but would not aid in the diagnosis of an occult fracture. Nonsteroidal anti-inflammatory drugs are first-line treatment for idiopathic low-back pain. In a patient with ankylosing spondylitis at high risk for fracture, further workup is needed to rule out an occult fracture. Flexion and extension radiographs of the spine are inferior to MRI for evaluating occult fractures and ligamentous injuries. The primary concern for this patient remains an unstable spinal fracture, which necessitates an MRI of the spine before initiating a workup for other possible causes of his back pain.
RECOMMENDED READINGS
Duane TM, Cross J, Scarcella N, Wolfe LG, Mayglothling J, Aboutanos MB, Whelan JF, Malhotra AK, Ivatury RR. Flexion-extension cervical spine plain films compared with MRI in the diagnosis of ligamentous injury. Am Surg. 2010 Jun;76(6):595-8. PubMed PMID: 20583514. View Abstract at PubMed
Hitchon PW, From AM, Brenton MD, Glaser JA, Torner JC. Fractures of the thoracolumbar spine complicating ankylosing spondylitis. J Neurosurg. 2002 Sep;97(2 Suppl):218-22. PubMed PMID: 12296682. View Abstract at PubMed
Koivikko MP, Koskinen SK. MRI of cervical spine injuries complicating ankylosing spondylitis. Skeletal Radiol. 2008 Sep;37(9):813-9. doi: 10.1007/s00256-008-0484-x. Epub 2008 Apr
Question 64
Which of the following is considered a potential advantage of arthroscopic repair for anterior instability of the shoulder? Review Topic
Explanation
Question 65
A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month follow-up appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is shown in Figure 21. What is the most likely diagnosis?
Explanation
REFERENCES: Schantz K, Reigels-Nielsen P: The anterior interosseous nerve syndrome.
J Hand Surg Br 1992;17:510-512.
Seror P: Anterior interosseous nerve lesions: Clinical and electrophysiological features. J Bone Joint Surg Br 1996;78:238-241.
Question 66
What is the most common cause for poor outcomes in patients who undergo total shoulder arthroplasty?
Explanation
REFERENCES: Chin PY, Sperling JW, Cofield RH, et al: Complications of total shoulder arthroplasty: Are they fewer or different? J Shoulder Elbow Surg 2006;15:19-22.
Hasan SS, Leith JM, Campbell B, et al: Characteristics of unsatisfactory shoulder arthroplasties. J Shoulder Elbow Surg 2002;11:431-441.
Question 67
A 24-year-old male presents following a motorcycle crash with an isolated injury to his right lower extremity. He has a 3x2cm wound over the fracture site, and he immediately receives Gram positive and Gram negative coverage along with a tetanus booster. The patient is splinted, optimized, and brought to the operating room where the wound is debrided and classified as a Type IIIB fracture. Deemed stable, the plastic surgery team arrives and acutely performs a free flap for coverage, following definitive fixation with an intramedullary nail. All of the following are factors that have been shown to increase infection risk EXCEPT: Review Topic

Explanation
When concerning management of open fractures, the most important factor is a thorough debridement. However, the quality of debridement is often not able to be quantified and thus, often not mentioned in studies. While early clinical and animal studies have shown that initial debridement should occur within 6 hours of injury, more recent clinical trials have not found a significant correlation within that urgent time frame, but rather recommend initial debridement as soon as possible within 24 hours. Time to antibiotic administration has been found to have a significant impact in lowering infection risk. Immediate administration in the emergency room is recommended. The ability to cover and/or close an open wound also has a significant impact on infection. Recent studies have recommended placing hardware after fasciotomy closure and have also demonstrated lower infection rates when flaps are placed within 72 hours of injury.
Pape and Webb concisely review the evolution of open fractures and wound management. The authors describe the early days where amputation was favored, to wet-to-dry dressings, to the advent of negative pressure wound therapy. Throughout, however, the authors emphasize the importance of soft tissue coverage. They also stress the importance of a technically thorough debridement, the most important factor of any wound management.
Scheneker et al. performed a systematic review and meta-analysis of 16 studies to determine if time to the operating room for debridement was an independent, modifiable risk factor in regards to subsequent infection following open tibia fracture. At the time of the study, the gold standard (based on a previous rat model), had recommended initial debridement within 6 hours of injury. The results of this meta-analysis, however, could not find conclusive evidence to suggest that late debridement alone placed the patient at a significantly higher risk for infection. The authors provided a moderate recommendation that initial debridement should occur as soon as possible within 24 hours, although more data is required in order to find a definitive time.
The SPRINT investigators report a landmark study that randomized over 1200 patients to either reamed or unreamed tibial IMN with the primary outcome analyzed as return to the operating room for either non-union treatment or deep infection. A notable difference between the two cohorts was a significantly higher primary event rate in the unreamed group.
Figure A exhibits a distal third open tibia fracture.
Incorrect answers:
Question 68
03 Fig 51c. What laboratory finding is most likely associated with this disease entity?
Explanation
Gibbs CP, Weber K, Scarborough MT: Malignant bone tumors. Inst Course Lect 2002;51:413-428
back to this question next question
Question 69
What are the proposed biomechanical advantages of the Grammont reverse total shoulder arthroplasty when compared to a standard shoulder arthroplasty? Review Topic
Explanation
Question 70
The bending stiffness of a slotted stainless steel intramedullary nail will be increased most by
Explanation
Question 71
Fixed hyperextension of the metatarsophalangeal joint is associated with
Explanation
REFERENCES: Marks RM: Anatomy and pathophysiology of lesser toe deformities. Foot Ankle Clin 1998;3:199-213.
Myerson MS, Shereff MJ: The pathological anatomy of claw and hammer toes. J Bone Joint Surg Am 1989;71:45-49.
Question 72
A 65-year-old woman who works as a florist has had pain in her right elbow for the past 6 months after lifting a flowerpot. MRI scans are shown in Figures 55a and 55b. The area of increased signal intensity seen in Figure 55b most likely represents which of the following findings?
Explanation
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 492-504.
Morrey B: Distal biceps tendon rupture, in Master Techniques in Orthopedic Surgery:
The Elbow, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2002, pp 173-192.
Question 73
Figures 1 and 2 are the CT and MRI scans of a patient with shoulder instability. Contrasting these two imaging techniques for decision making in shoulder instability would suggest
Explanation
A. Inability to flex the distal interphalangeal joint of the index finger
B. Positive Froment’s sign
C. Weakness with wrist extension
D. Decreased capillary refill
Question 74
A patient is treated with volar plating for a distal radius fracture. The CT scan shown in Figure 15 is obtained after union of the fracture because the patient reports ongoing symptoms. The prominent hardware is most likely injuring what tendon?
Explanation
REFERENCES: Benson EC, Decarvalho A, Mikola EA, et al: Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res 2006;451:218-222.
Cooney WP, Linscheid RL, Dobyns JH (eds): The Wrist: Diagnosis and Operative Treatment. Philadelphia, PA, Mosby-Year Book, 1998.
Question 75
When performing a long fusion to the sacrum in an osteopenic patient in whom optimal sagittal balance is restored, which of the following is a benefit of extending the distal fixation to the pelvis, rather than the sacrum alone? Review Topic
Explanation
Question 76
A 42-year-old man sustained the periprosthetic fracture shown in Figures 19a and 19b. The femoral component is well fixed. What is the next most appropriate step in management?
Explanation
REFERENCES: Duncan CP, Masri BA: Fractures of the femur after hip replacement. Instr Course Lect 1995;44:293-304.
Bono JV, McCarthy JC, Thornhill TS, Bierbaum BE, Turner RH (eds): Revision Total Hip Arthroplasty. New York, NY, Springer Verlag, 1999, pp 530-592.
Question 77
They found statistically significant decreases in need for secondary intervention, hardware failure, and infection as well as faster wound healing and faster time to fracture union.
Explanation
A 76-year old patient underwent partial foot amputation through the talonavicular and calcaneocuboid joints. Besides Achilles tendon lengthening, what additional procedure(s) may be required to prevent the most common post-operative deformity?
Posterior capsule release
Anterior tibialis transfer to the talar neck
Anterior tibialis transfer to cuboid
Flexor hallucis longus transfer to calcaneus
Peroneus brevis transfer to calcaneus Corrent answer: 2
Achilles tendon lengthening AND anterior tibialis transfer to the talar neck would be required to prevent equinovarus deformity.
Partial foot amputation through the talonavicular and calcaneocuboid joints is also known as the Chopart amputation. Chopart amputation alone is known to result in significant equinovarus deformity. This deformity results in excessive pressure on the anterior wound during gait, causing pain and wound complications. Transfer of the tibialis anterior tendon to talar neck will provide force, and muscle tone, that promotes ankle dorsiflexion. Lengthening of the Achilles tendon will also reduce the equinus moment force across the ankle joint.
Dillion et al. examined the gait patterns of partial foot amputees. They found that amputations proximal to the metatarsal heads compromised the normal propulsive function of the foot and ankle. The ideal level of amputation to maintain normal propulsive function was distal to the metatarsal heads (i.e., disarticulating the metatarsophalangeal (MTP) joint).
Illustration A is a lateral radiograph showing a Chopart amputation. Incorrect Answers:
prevent the equinovarus deformity.

OrthoCash 2020
A 32-year-old male is involved in a motor vehicle collision and sustains the injury seen in Figure A. What is the most common urological injury associated with this injury pattern?

Testicular torsion
Posterior urethral tear
Bladder denervation
Testicular rupture
Renal hematoma
The figure shows an anteroposterior pelvic ring injury. The most common urological injury with pelvic ring injuries remains the posterior urethral tear, followed by bladder rupture.
Watnik et al notes lower urinary tract (bladder to end of urethra) injuries in up to 25% of patients with this injury. He reports that when contaminated urine communicates with the anterior arch, the possibility of infection exists, and early repair of bladder disruptions with simultaneous anterior arch plating minimizes this risk.
Routt et al notes that even with simultaneous treatment of these injuries, complications are common (late stricture in 44%, impotence in 16%, delayed incontinence in 20% of females, anterior deep pelvic infection in 4%). Despite this, they report that early urological repairs are easily performed at the time of anterior pelvic open reduction and internal fixation.
OrthoCash 2020
A 26-year-old women, 31-weeks pregnant, presents to the emergency department with the injury shown in Figure A. She states the injury occurred while lifting a heavy vacuum five days ago. She suffers from chronic headaches and sleep disturbances. On inspection, there are multiple dorsal and volar bruising over her wrist and upper arm. She is neurologically intact. After closed reduction and immobilizing the arm, what would be the next best step in management of this patient?

Diagnostic wrist arthroscopy
Urgent MRI wrist
Skeletal survey radiographs
Request a consultation with social worker in the hospital
Urgent open reduction internal fixation Corrent answer: 4
This patient presents with classic features of domestic violence. The most appropriate next step would be consultation with a social worker at the hospital, assess for child and patient safety, and encouraging the patient to seek self-protection.
Factors suggestive of domestic violence in the patient include pregnancy, delayed presentation after injury, inconsistent history, multiple bruises and complaints of chronic headache/sleep disturbances. Victims frequently miss days of work and as a result are at risk for losing their jobs. Victims are also more likely to engage in high-risk behavior with sex, drugs, alcohol, smoking, and eating.
The AAOS published a document outlining the Orthopaedic Surgeon’s responsibilities in domestic and family violence. Musculoskeletal injuries that should raise a suspicion of a problem include (1) Multiple injuries/fractures; (2) Unusual patterns of injury/fracture; (3) Injuries/fractures of varying ages; (4)
Injuries/fractures inconsistent with or disproportional to the history; (5) Multiple injuries treated in different hospital emergency departments or by different providers.
Incorrect Answers:
OrthoCash 2020
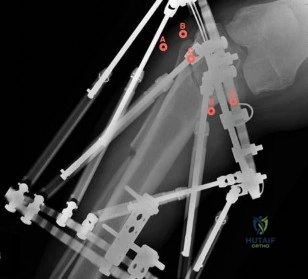
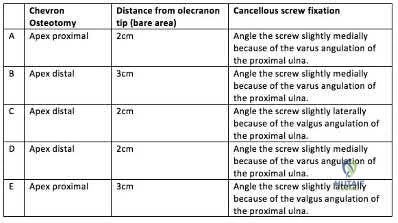
A 45-year-old man undergoes open reduction and internal fixation for a comminuted intra-articular humerus fracture . An olecranon osteotomy is performed and subsequently fixed with an intramedullary cancellous screw. Which of the following options in the table shown in Figure A best describes the characteristics of this osteotomy?
Question 78
An active 65-year-old man has pain in the left shoulder 5 years after undergoing a hemiarthroplasty. He has a remote history of two previous instability operations. Examination reveals that forward elevation is 140 degrees and external rotation is 40 degrees. Serologic studies for infection are negative. AP and axillary radiographs are shown in Figures 7a and 7b. What surgical procedure will provide the most predictable pain relief and function? Review Topic

Explanation
Question 79
A 19-year-old collegiate offensive lineman injures his left elbow in a scrimmage. He reports reaching out with his left arm to prevent the defensive player from getting around him, and, as he grabbed the player, his elbow was forced into extension. He had immediate pain and weakness and heard a “pop.” He has mild swelling in the antecubital fossa and a prominent-appearing biceps muscle belly. His hook test result is abnormal at the elbow. Which type of contraction of the involved muscle most likely resulted in this lineman's injury?
Explanation
followed by the ECU, EDQ, and, finally, the EIP.
Question 80
Figure 83 is the CT scan of a 36-year-old man who fell from a roof. Eight hours later at the emergency department he describes low-back pain with numbness and weakness in his bilateral lower extremity. A neurologic examination reveals 2/5 strength in his quadriceps and iliopsoas bilaterally, 2/5 strength in his right anterior tibialis and gastrocsoleus, and 1/5 strength in his left anterior tibialis and gastrocsoleus. Two hours later, strength in his lower extremities has diminished markedly. What is the best next step?

Explanation
Any progressive neurologic deficit requires emergent surgical intervention. Lumbar injuries cannot be reliably reduced with traction. Although IV steroids and management of mean arterial blood pressure are appropriate interventions for injuries in the region of the conus medullaris, steroids are only indicated when given within 8 hours of injury and are not appropriate as a sole means of management for progressive neurologic deficit.
RECOMMENDED READINGS
Bono CM, Rinaldi MD. Thoracolumbar trauma. In: Spivak JM, Connolly PJ, eds. Orthopaedic Knowledge Update: Spine 3. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2006:201-216.
Mikles MR, Stchur RP, Graziano GP. Posterior instrumentation for thoracolumbar fractures. J Am Acad Orthop Surg. 2004 Nov-Dec;12(6):424-35. Review. PubMed PMID: 15615508. View Abstract at PubMed
Question 81
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms? Review Topic

Explanation
Question 82
A 54-year-old man with metastatic renal cell carcinoma has had increasing pain in the left hip for the past 6 weeks. A radiograph is shown in Figure 36. Prophylactic stabilization will most likely result in
Explanation
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Harrington KD: Impending pathologic fractures from metastatic malignancy: Evaluation and management. Instr Course Lect 1986;35:357-381.
Question 83
An anatomic reduction is obtained at the femoral neck. The most likely reason for development of avascular necrosis (AVN) in this scenario would be
Explanation
A damage-control approach is indicated for this patient. Debridement of the open fracture wound and rapid stabilization without an extensive surgical
approach are indicated. Rapid percutaneous fixation of the femoral neck would compromise long-term outcomes for this displaced fracture because obtaining a quality reduction and fixation construct is critical for the long-term outcome. This patient likely would not tolerate cephalomedullary nailing or open approaches very well at this time.
A vertically oriented (Pauwels 3) femoral neck fracture is more common in younger patients who sustain high-energy injuries. Because of the mechanism of injury, many of these patients have associated injuries. This is a biomechanically challenging fracture because the fracture is subject to shear forces rather than compression, making it inherently unstable. This type of fracture often necessitates different fixation strategies to counter shearing forces, such as use of a transversely oriented (Pauwels) screw to compress the fracture or a fixed-angle device.
The femoral neck fracture should be prioritized in this scenario. This does not necessarily mean that the femoral neck should be repaired first, but the strategy should emphasize optimal fixation of the femoral neck. It has been demonstrated that this is less successful when using a single implant to repair both fractures. It is possible to place femoral neck fixation around an antegrade femoral nail; however, it is much more likely that optimal fixation will be achieved with shaft fixation that does not obstruct placement of fixation for the femoral neck.
AVN is more common among physiologically young patients after femoral neck fractures. The higher energy of injury is a likely contributor. Closed reduction has not been shown to increase the risk for AVN when an anatomic reduction is obtained. A surgical delay of 24 hours does not cause AVN. Patients with associated femoral shaft fractures are not at increased risk for AVN; in fact, some studies have shown a relatively lower rate of AVN when a femoral neck fracture is associated with a femoral shaft fracture.
RECOMMENDED READINGS
Liporace F, Gaines R, Collinge C, Haidukewych GJ. Results of internal fixation of Pauwels type-
3 vertical femoral neck fractures. J Bone Joint Surg Am. 2008 Aug;90(8):1654-9. doi: 10.2106/JBJS.G.01353. PubMed PMID: 18676894. View Abstract at PubMed
Bedi A, Karunakar MA, Caron T, Sanders RW, Haidukewych GJ. Accuracy of reduction of ipsilateral femoral neck and shaft fractures--an analysis of various internal fixation strategies. J Orthop Trauma. 2009 Apr;23(4):249-53. doi: 10.1097/BOT.0b013e3181a03675. PubMed PMID: 19318867. View Abstract at PubMed
Haidukewych GJ, Rothwell WS, Jacofsky DJ, Torchia ME, Berry DJ. Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J Bone Joint Surg Am. 2004 Aug;86-A(8):1711-6. PubMed PMID: 15292419. View Abstract at PubMed Peljovich AE, Patterson BM. Ipsilateral femoral neck and shaft fractures. J Am Acad Orthop Surg. 1998 Mar-Apr;6(2):106-13. PubMed PMID: 9682073. View Abstract at PubMed
Upadhyay A, Jain P, Mishra P, Maini L, Gautum VK, Dhaon BK. Delayed internal fixation of fractures of the neck of the femur in young adults. A prospective, randomised study comparing closed and open reduction. J Bone Joint Surg Br. 2004 Sep;86(7):1035-40. PubMed PMID: 15446534. View Abstract at PubMed
RESPONSES FOR QUESTIONS 96 THROUGH 99
- Warfarin (Coumadin)
- Dabigatran (Pradaxa)
- Rivaroxaban (Xarelto)
- Apixaban (Eliquis)
Match the appropriate oral anticoagulant listed with the description.
This medication is a vitamin K antagonist and can be reversed.
- Warfarin (Coumadin)
- Dabigatran (Pradaxa)
- Rivaroxaban (Xarelto)
- Apixaban (Eliquis)
Question 84
A 21-year-old woman is struck by a car and sustains a Gustillo IIIB fracture of the tibia. The wound was debrided and immobilized with an external fixator. Radiographs are shown in Figure A. The soft tissue defect was covered with a free flap. Her recovery was complicated by wound infection with Klebsiella pneumoniae and Escherichia coli. One month after her injury, she underwent intramedullary nailing and placement of an antibiotic spacer measuring 15cm in length. Radiographs are shown in Figure B. At the next stage of surgery 6 weeks later, the surgeon should plan to do all of the following:

Explanation
The Masquelet staged technique of induced membranes is an option for filling large bone defects up to 25cm in length. This technique protects against autograft resorption, stimulates mesenchymal cell-to-osteoblast differentiation, maintains graft position, and prevents soft tissue interposition. Cement impregnation achieves high local antibiotic concentration without risk of systemic toxicity.
Ashman et al. discussed the techniques of addressing bone defects. Options include:
(1) acute limb shortening (up to 4cm in the tibia and humerus, and 7cm in the femur);
(2) distraction osteogenesis for defects up to 10cm long (at 1mm/day with consolidation period of 5days per mm, or total treatment time of up to 60days/cm), (3) autograft (up to 25cm of vascularized fibula, or 3cm of nonvascularized iliac crest),
and (4) Masquelet technique.
Taylor et al. reviewed the induced membranes technique. They found that the membrane is well vascularized and composed of type I collagen with fibroblasts with an inner epithelial cell layer. There is a high concentration of VEGF, RUNX2 (CBFA1), TGFß1, and BMP2. The membrane is sutured over bone graft to create a closed pouch. When a nail is present, they note a second internal membrane around the nail, potentially increasing local vascularity and osteoinductive factor concentration.
Figure A shows a Gustillo IIIB tibia fracture with a large bone defect held in a temporizing external fixator. Figure B shows the same defect following intramedullary nailing and with a cement spacer placed circumferentially around the nail in the defect.
Incorrect Answers
Question 85
Figure 1 shows the radiograph of a 71-year-old man who has had increasing pain and weakness in his shoulder for the past 3 years. Nonsurgical management has failed to provide relief. Examination shows 130 degrees of active forward flexion and intact external rotation strength. During surgery, a 1- x 1-cm rotator cuff tear involving the supraspinatus is encountered. Treatment should include
Explanation
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Arntz CT, Jackins S, Matsen FA III: Prosthetic replacement of the shoulder for treatment of defects in the rotator cuff and surface of the glenohumeral joint. J Bone Joint Surg Am 1993;75:485-491.
Question 86
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?
Explanation
REFERENCES: Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461.
Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416.
Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Renaldo N, Egol K: Damage-control orthopaedics: Evolution and practical applications.
Am J Orthop 2006;35:285-291.
Question 87
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?
Explanation
REFERENCES: Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647.
Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Mills JD, Moore GE, Thompson PD: The athlete’s heart. Clin Sports Med 1997;16:725-737.
Question 88
What is the greatest benefit of external fixation for treatment of displaced and unstable pelvic ring injuries with hemodynamic instability? Review Topic
Explanation
Question 89
A 38-year-old man sustains a complete avulsion with retraction of the ischial attachment of the hamstring muscles in a fall while water skiing. He indicates that he is an aggressive athlete who participates regularly in multiple running and cutting-type sports, and he strongly desires to continue his athletic competition. Management should consist of
Explanation
REFERENCES: Orava S, Kujala UM: Rupture of the ischial origin of the hamstring muscles. Am J Sports Med 1995;23:702-705.
Clanton TO, Coupe KJ: Hamstring strains in the athlete: Diagnosis and treatment. J Am Acad Orthop Surg 1998;6:237-248.
Question 90
Passive glycation of articular cartilage results in
Explanation
REFERENCES: DeGroot J, Verzijl N, Wenting-van Wijk MJ, et al: Accumulation of advanced glycation end products as a molecular mechanism for aging as a risk factor in osteoarthritis. Arthritis Rheum 2004;50:1207-1215.
Chen AC, Temple MM, Ng DM, et al: Induction of advanced glycation end products and alterations of the tensile properties of articular cartilage. Arthritis Rheum 2002;46:3212-3217.
Question 91
In patients older than age 40 years who sustain a first-time anterior dislocation of the shoulder, prolonged morbidity is most commonly associated with
Explanation
REFERENCES: Pevny T, Hunter RE, Freeman JR: Primary traumatic anterior shoulder dislocation in patients 40 years of age and older. Arthroscopy 1998;14:289-294.
Sonnabend DH: Treatment of primary anterior shoulder dislocation in patients older than 40 years of age: Conservative versus operative. Clin Orthop 1994;304:74-77.
Hawkins RJ, Mohtadi NG: Controversy in anterior shoulder instability. Clin Orthop 1991;272:152-161.
Question 92
The mother of an otherwise healthy 1-month-old infant reports that he is not moving his left leg after falling from his high chair 2 days ago. He has a temperature of 99.5°F (37.5°C). Examination reveals that the left thigh is moderately tender to palpation. Because the infant is apprehensive, range of motion is difficult to quantify, but appears to be normal at the hips and ankles. Range of motion of the left knee is approximately 25° to 90°. A radiograph of the leg is shown in Figure 27. Management should consist of
Explanation
REFERENCES: Akbarnia BA: The role of the orthopaedic surgeon in child abuse, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1315-1334.
Black GB: Child abuse fractures, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994, pp 931-944.
Question 93
Tension band wire fixation is best indicated for which of the following types of olecranon fractures?
Explanation
Question 94
In a patient who has rheumatoid arthritis with acetabular protrusion, what is the best biomechanical position for the cup with respect to the preoperative center of rotation?
Explanation
REFERENCES: Crowninshield RD, Brand RA, Pedersen DR: A stress analysis of acetabular reconstruction in protrusio acetabuli. J Bone Joint Surg Am 1983;65:495-499.
Ranawat CS, Dorr LD, Inglis AE: Total hip arthroplasty in protrusio acetabuli of rheumatoid arthritis. J Bone Joint Surg Am 1980;62:1059-1065.
Question 95
Figure 10 shows the radiograph of an active 75-year-old woman who reports severe leg pain after a fall. Management should consist of
Explanation
REFERENCES: Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242.
Montijo H, Ebert FR, Lennox DA: Treatment of proximal femur fractures associated with total hip arthroplasty. J Arthroplasty 1989;4:115-123.
Question 96
Results of a study demonstrating no difference between treatments when a difference truly exists is an example of which of the following?
Explanation
fragile p-values is that small sample sizes may result in wide variability of p-values with only one change in a data point for a given group. This singular change could be a chance occurrence, but it still can affect the statisticalsignificance of the outcomes analysis. Fragility of p-values is limited by increasing sample sizes. Negative predictive value is the proportion of patients with negative test results who are correctly diagnosed.
Question 97
A 69-year-old woman has just undergone an uncomplicated total shoulder arthroplasty for glenohumeral osteoarthritis. A press-fit humeral stem and a cemented all-polyethylene glenoid component were placed. At this point, what is the postoperative rehabilitation plan?
Explanation
at 3 weeks risks tearing the subscapularis tendon repair. Active strengthening should not begin for 6 weeks postoperatively to allow the subscapularis tendon repair time to heal.
REFERENCES: Boardman ND III, Cofield RH, Bengston KA, et al: Rehabilitation after total shoulder arthroplasty. J Arthroplasty 2001;16:483-486.
Matsen FA III, Lippitt SB, Sidles JA, et al: Practical Evaluation and Management of the Shoulder. Philadelphia, PA, WB Saunders, 1994, pp 215-218.
Question 98
At what age does the lateral epicondyle normally ossify in males?
Explanation
Question 99
Which modality has the broadest application for reduction of postsurgical transfusion?
Explanation
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
Question 100
Changes to the properties of ultra-high molecular weight polyethylene with increasing irradiation dose include improved
Explanation
Irradiation leads to the production of free radicals, requiring a step in the manufacturing process (melting, annealing, vitamin E doping) to stabilize the free radicals and reduce the potential for oxidation. Wear resistance is improved with irradiation; however, there is minimal benefit with doses of greater than 10 Mrads.
REFERENCES: Collier JP, Currier BH, Kennedy FE, et al: Comparison of cross-linked polyethylene materials for orthopaedic applications. Clin Orthop Relat Res 2003;414:289-304.
Gordan AC, D’Lima DD, Colwell CW Jr: Highly cross-linked polyethylene in total hip arthroplasty. J Am Acad
Orthop Surg 2006;14:511-523.
Jacobs CA, Christian CP, Greenwald AS, et al: Clinical performance of highly cross-linked polyethylenes in total hip arthroplasty. J Bone Joint Surg Am 2007;89:2779-2786.
