Orthopedic Board Exam MCQs: Trauma, Shoulder, Elbow, & Hip | Part 154

Key Takeaway
This page offers Part 154 of a comprehensive OITE & ABOS board review quiz for orthopedic surgeons and residents. It contains 100 verified, high-yield MCQs focusing on Dislocation, Elbow, Fracture, Hip, Shoulder. Designed to simulate board exams, it aids in mastering clinical scenarios for certification preparation.
About This Board Review Set
This is Part 154 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 154
This module focuses heavily on: Dislocation, Elbow, Fracture, Hip, Shoulder.
Sample Questions from This Set
Sample Question 1: A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month followup appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is...
Sample Question 2: A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees great...
Sample Question 3: Figures 1 through 3 demonstrate the MRIs obtained from a 36-year-old man with an injury to the elbow. The expected result of nonsurgical treatment would be weakness of...
Sample Question 4: A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal...
Sample Question 5: During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this ath...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 32-year-old woman sustained an elbow dislocation, and management consisted of early range of motion. Examination at the 3-month followup appointment reveals that she has regained elbow motion but has a weak pinch. A clinical photograph is shown in Figure 21. What is the most likely diagnosis? Review Topic

Explanation
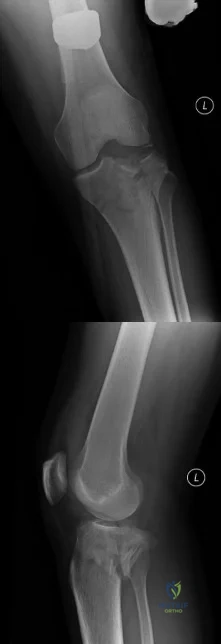
(SBQ12TR.54) A 37-year-old male cashier is shot in the leg. He sustains the injury shown in Figures A and B, and is subsequently taken to the operating room for intramedullary nailing. Figure C shows a radiograph of the nail starting point (*). What complication is most likely to result?

Varus malunion
Nonunion
Valgus malunion
Malrotation
Superficial peroneal nerve injury
This patient is presenting with a comminuted fracture of the proximal third of the tibia. He is appropriately undergoing intramedullary nail fixation, however, the start point illustrated in Figure C is too medial and often leads to a valgus malunion.
Intramedullary nail fixation is more technically demanding in proximal tibial fractures than diaphyseal fractures. The valgus deformity is due to imbalanced muscle forces on the proximal fragment, which are then accentuated by a start point that is too medial. An apex anterior (procurvatum) deformity can also occur and results from the pull of the patellar tendon or a posteriorly directed nail that deflects off the posterior tibial cortex and rotates the proximal fragment. The ideal starting point for proximal tibial fractures is slightly lateral to the medial aspect of the lateral tibial spine on a true AP x-ray and very proximal and just anterior to the anterior margin of the articular surface.
Nork et al. reported the results of intramedullary nailing of proximal tibial fractures with emphasis on techniques of reduction. Various techniques were found to be successful including attention to the proper starting point, the use of unicortical plates, and the use of a femoral distractor applied to the tibia.
Lowe et al. describe surgical techniques for complex proximal tibial fractures. They describe the extended leg position, use of a femoral distractor, temporary plate fixation, blocking (Poller) screws, and use of percutaneous clamps as means to achieve reduction during fixation.
Figure A and B show an AP and lateral radiograph of a comminuted extra-articular fracture through the proximal third of the tibia. Figure C demonstrates a start point that is too medial (represented by the asterisk) for intramedullary nail fixation. Illustration A and B show the ideal start point for intramedullary nail fixation of the tibia on AP and lateral radiographs.
Incorrect Answers:
Varus malunion is more likely to occur in midshaft tibia fractures with an intact fibula.
Nonunion after a proximal tibial fracture treated with intramedullary nailing is less common than malunion.
Malrotation occurs most commonly after IM nailing of fractures through the distal third of the tibia.
The superficial peroneal nerve is at risk during distal screw fixation using a LISS plating technique for fracture fixation.
Question 2
A 22-year-old wrestler who underwent an open anterior shoulder reconstruction to repair a dislocated shoulder 6 months ago now reports shoulder pain after attempting a takedown. Examination reveals external rotation that is 15 degrees greater than the contralateral side. He has pain associated with abduction and external rotation but no apprehension. Which of the following tests would most likely reveal positive findings?
Explanation
REFERENCES: Gerber C, Krushell RJ: Isolated ruptures of the tendon of the subscapularis muscle: Clinical fractures in 16 cases. J Bone Joint Surg Br 1991;73:389-394.
Hawkins RJ, Bokor DJ: Clinical evaluation of the shoulder, in Rockwood CA, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1990, pp 149-177.
Question 3
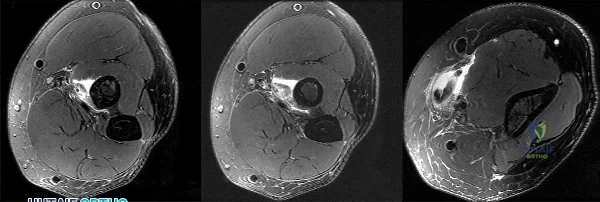
Figures 1 through 3 demonstrate the MRIs obtained from a 36-year-old man with an injury to the elbow. The expected result of nonsurgical treatment would be weakness of
Explanation
The axial T2-weighted MRIs demonstrate a distal biceps rupture. The increased signal is noted superficial to the brachialis muscle and adjacent to the biceps tuberosity. The distal biceps tendon is not seen in the distal cuts and has retracted proximally. The physical examination of patients with these injuries show abnormal contour of the arm and tenderness in the antecubital fossa. The hook test is a provocative maneuver that documents biceps integrity. When performing the maneuver, the examiner attempts to hook a finger around the distal biceps tendon while the patient actively supinates with the elbow held in flexion. Nonsurgical treatment has been documented to result in an average loss of 40% of supination strength and 30% of elbow flexion strength. Repair is optimal within several weeks of injury. The alternative options would not occur with a distal biceps rupture.
Question 4
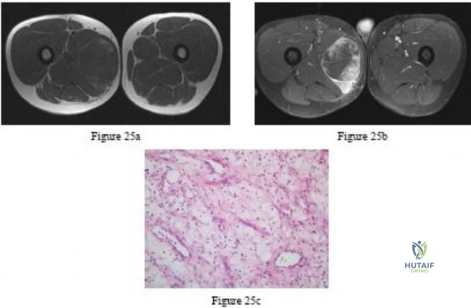
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome?
Explanation
REFERENCES: Lalonde F, Letts M, Yang JP, et al: An analysis of burst fractures of the spine in adolescents. Am J Orthop 2001;30:115-120.
Clark P, Letts M: Trauma to the thoracic and lumbar spine in the adolescent. Can J Surg 2001;44:337-345.
Been HD, Bouma GJ: Comparison of two types of surgery for thoraco-lumbar burst fractures: Combined anterior and posterior stabilization vs posterior instrumentation only. Acta Neurochir (Wien) 1999;141:349-357.
Question 5
During preparation for the NCAA wrestling championships, a participant reports the development of vesicular lesions on his right chest wall that are mildly painful; however, they have not affected his ability to wrestle. How should this athlete be managed? Review Topic
Explanation
Question 6
Figure 7 shows the CT scan of a 25-year-old soccer player who has had posterior ankle pain with plantar flexion for the past 2 years. Immobilization has failed to provide relief. He is ambulatory. Management should consist of
Explanation
REFERENCES: Hedrick MR, McBryde AM: Posterior ankle impingement. Foot Ankle Int 1994;15:2-8.
Abramowitz Y, Wollstein R, Barzilay Y, et al: Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am 2003;85:1051-1057.
Question 7
An osteoprogenitor cell is expected to commit to a bone lineage in the presence of what transcription factor?
Explanation
C/EBPa are transcription factors leading to adipocytes, MyoD promotes myoblasts, and Sox 9 corresponds to chondroblasts.
Question 8
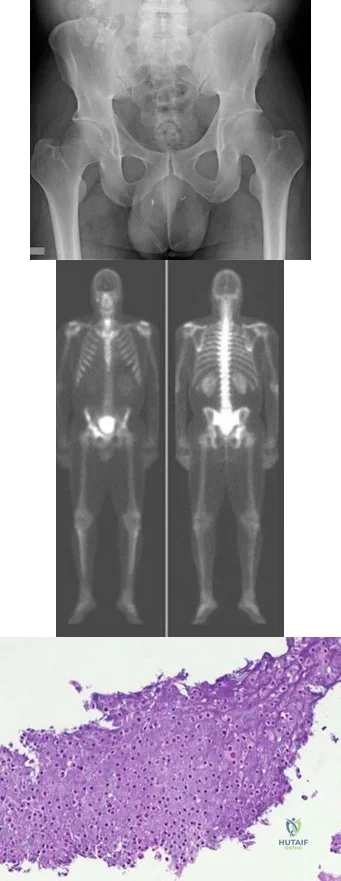
Figures 20a and 20b show the AP and lateral radiographs of a 62-year-old man who has had hip pain for the past 3 weeks. Figure 20c shows a CT scan of the abdomen and pelvis. A needle biopsy specimen is shown in Figure 20d. Preoperative management should include which of the following?
Explanation
REFERENCES: Chatziioannou AN, Johnson ME, Pneumaticos SG, et al: Preoperative embolization of bone metastases from renal cell carcinoma. Eur Radiol 2000;10:593-596.
Sun S, Lang EV: Bone metastases from renal cell carcinoma: Preoperative embolization. J Vasc Interv Radiol 1998;9:263-269.
Question 9
A 47-year-old landscaper presents with worsening left shoulder pain and weakness. Three years ago, he injured the left shoulder in a fall and elected for nonoperative management to minimize time off from work. Physical therapy was effective until 6 months ago when his shoulder function worsened to the point that he is now unable to work. Examination of his active range of motion reveals forward elevation 120° with pain, abduction 100°, IR at neutral to T8 and ER at neutral 5°. He has a positive ER lag sign and Hornblower's sign. Belly press and lift-off tests are normal. A recent radiograph is shown in Figures A. MRI images are shown in Figures B and C. Which of the following is the best treatment option? Review Topic
Explanation
Irreparable rotator cuff tears are marked by: (1) Superior displacement of the humeral head (AHI < 5-7mm), (2) Fatty infiltration of the rotator cuff muscles (Goutallier stage 3-4), (3) Increased duration of the tendon tear and (4) Profound external rotation weakness. These findings are predictive of poor-quality tissue and stiffness of the muscle-tendon unit, not amenable to primary repair. In this setting, a latissimus dorsi
transfer can be utilized to restore shoulder strength, function and improve pain. Relative contraindications include subscapularis deficiency, deltoid deficiency, pseudoparalysis of the shoulder and advanced glenohumeral arthritis.
Gerber et al. performed a case series analysis of 67 patients with irreparable rotator cuff tears managed with latissimus dorsi transfer. Patients with an intact subscapularis demonstrated improvement in pain, range of motion and strength postoperatively, while no improvement was noted in patients with subscapularis deficiency. The authors conclude that latissimus dorsi transfer should not be performed in the setting of poor subscapularis function.
Iannotti et al. found that better clinical results following latissimus dorsi transfer were associated with: preserved active shoulder range of motion and strength (specifically forward elevation > 90° and external rotation > 20°), synchronous firing of the transferred latissimus dorsi muscle and male gender.
Figure A is an AP radiograph of the left shoulder with superior migration of the humeral head (AHI < 5mm) and no evidence of glenohumeral arthritis. Figures B and C show a retracted posterosuperior rotator cuff tear and Goutallier stage 4 atrophy (more fat than muscle) of the supraspinatus, infraspinatus and teres minor, rendering this tear irreparable. Illustration A shows a latissimus dorsi transfer. The latissimus dorsi tendon is positioned over the top of the humeral head, covering most of the rotator cuff defect. The tendon is then secured to the subscapularis tendon edge and lesser tuberosity anteriorly, the remnant supraspinatus and infraspinatus tendons medially, and the greater tuberosity laterally.
Incorrect Answers:
Question 10
What is the most common malignancy involving the hand?
Explanation
REFERENCES: Fink JA, Akelman E: Nonmelanotic malignant skin tumors of the hand. Hand Clin 1995;11:255-264.
Fleegler EJ: Skin tumors, in Green DP, Hotchkiss RN, Pederson WC (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, vol 2, pp 2184-2205.
Question 11
A 47-year-old male tennis player has pain in his nondominant shoulder that has failed to respond to 4 months of nonsurgical management. Examination reveals acromial tenderness and pain at the supraspinatus tendon insertion. He has a positive impingement sign, pain on forward elevation, and minimal cuff weakness. The MRI scans are shown in Figures 30a and 30b. To completely resolve his symptoms, treatment should consist of
Explanation
REFERENCES: Hutchinson MR, Veenstra MA: Arthroscopic decompression of shoulder impingement secondary to os acromiale. Arthroscopy 1993;9:28-32.
Warner JJ, Beim GM, Higgins L: The treatment of symptomatic os acromiale. J Bone Joint Surg Am 1998;80:1320-1326.
Question 12
A 32-year-old woman has an isolated left posterior wall acetabular fracture in which about 25% of the wall surface is involved. Which of the following criteria would indicate the need for surgical reduction and fixation?
Explanation
REFERENCES: Tornetta P III: Non-operative management of acetabular fractures: The use of dynamic stress views. J Bone Joint Surg Br 1999;81:67-70.
Keith JE Jr, Brashear HR Jr, Guilford WB: Stability of posterior fracture-dislocations of the hip: Quantitative assessment using computed tomography. J Bone Joint Surg Am 1988;70:711-714.
Question 13
A 22-year-old woman injures her neck in a motor vehicle accident. Examination reveals no sensory or motor function below T8. Radiographs and an MRI scan show a burst fracture at T7. Forty-eight hours later, the bulbocavernosus reflex is present but there is no evidence of motor or sensory recovery in the lower extremities. What is the most likely diagnosis?
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 179-187.
Herkowitz HN, Garfin SR, Eismont FJ: Rothman-Simone The Spine, ed 5. Philadelphia, PA, Saunders Elsevier, 2006, pp 1132-1133.
Question 14
Which of the following processes does not account for decreased hematopoiesis in patients with metastatic disease?
Explanation
REFERENCE: Frassica FJ, Gitelis S, Sim FH: Metastic bone disease: General principles, pathophysiology, evaluation, and biopsy. Instr Course Lect 1992;41:293-300.
Question 15
A 56-year-old man sustained a nondisplaced extra-articular fracture of the proximal aspect of the third metatarsal after dropping a heavy object on his left foot. Management should consist of
Explanation
REFERENCES: Myerson MS: Foot and Ankle Disorders. Philadelphia, PA, WB Saunders, 2000, pp 1265-1296.
Early JS: Fractures and dislocations of the midfoot and forefoot, in Rockwood and Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001,
pp 2181-2245.
Question 16
A 22-year-old patient underwent successful reduction of a posterolateral elbow dislocation. Management should now consist of
Explanation
REFERENCES: Ross G, McDevitt ER, Chronister R, et al: Treatment of simple elbow dislocation using an immediate motion protocol. Am J Sports Med 1999;27:308-311.
O’Driscoll SW, Jupiter JB, King GJ, et al: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738.
Question 17
Figures 1 through 6 reveal the radiographs and MR images of a 30-year-old man who has a 1-year history of atraumatic medial-sided left knee pain refractory to nonsurgical measures. What is the most appropriate treatment?

Explanation
Question 18
An 18-year-old man has acute respiratory distress after sustaining injuries in a motorcycle accident. He has a blood pressure of 80/60 mm Hg and a pulse rate of 110/min. Examination reveals chest tympany to percussion, distended neck veins, and deviation of the trachea away from his right hemithorax where the breath sounds are diminished. Heart sounds are regular and normal on auscultation. Initial management should consist of
Explanation
REFERENCE: Mattox KL, Feliciano DV, Moore EE (eds): Management of Shock, ed 4. New York, NY, McGraw Hill, 2000, p 215.
Question 19
When converting the knee shown in Figure 20 to a total knee arthroplasty, satisfactory outcome can be expected in what percent of patients?
Explanation
REFERENCE: Naranja RJ Jr, Lotke PA, Pagnano MW, Hanssen AD: Total knee arthroplasty in a previously ankylosed or arthrodesed knee. Clin Orthop 1996;331:234-237.
Question 20
Figures 4a and 4b show the radiographs of a 32-year-old man who has right groin pain with activity or prolonged standing. Which of the following factors would not prohibit consideration of acetabular liner exchange and grafting of the defects?
Explanation
REFERENCES: Maloney WJ, Herzwurm P, Paprosky W, Rubash HE, Engh CA: Treatment of pelvic osteolysis associated with a stable acetabular component inserted without cement as part of a total hip replacement. J Bone Joint Surg Am 1997;79:1628-1634.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 417-451.
Question 21
Which of the following conditions routinely requires early surgical intervention in patients with Marfan syndrome? Review Topic
Explanation
Question 22
A middle-aged man sustains traumatic loss of the second, third, and fourth toes in a lawnmower accident. The wound is grossly contaminated with soil. Penicillin is added to his antibiotic regimen for coverage of what bacteria? Review Topic
Explanation
Question 23
A 65-year-old woman with rheumatoid arthritis is unable to actively extend her index, middle, ring, and little fingers secondary to tendon rupture. In performing a flexor digitorum sublimis (FDS) of the middle/ring finger to extensor digitorum communis (EDC) transfer to restore active metacarpophalangeal (MCP) joint extension, the FDS should be passed
Explanation
Question 24
A 35-year-old recreational basketball player reports shoulder pain following a sprawl for a rebound. While examination reveals that he can actively elevate the arm with pain, a subacromial injection fails to provide relief. An MRI scan reveals medial subluxation of the long head of the biceps. Which of the following structures most likely has also been injured?
Explanation
REFERENCES: Petersson CJ: Spontaneous medial dislocation of the tendon of the long biceps brachii. Clin Orthop 1986;211:224-227.
Gerber C, Sebesta A: Impingement of the deep surface of the subscapularis tendon and the reflection pulley on the anterosuperior glenoid rim: A preliminary report. J Shoulder Elbow Surg 2000;9:483-490.
Question 25
- Figure 24 shows the AP radiograph of a 22-year-old woman who has pain with activity and crepitus at he second metatarsophalangeal joint. Despite nonsurgical treatment, the pain has become progressively worse over the past year. Treatment should include

Explanation
Question 26
Chronic traumatic encephalopathy (CTE) is a neurodegenerative disease that is characterized by
Explanation
Question 27
At the level of tibial bone resection in total knee arthroplasty, where does the common peroneal nerve lie?
Explanation
REFERENCES: Clarke HD, Schwartz JB, Math KR, et al: Anatomic risk of peroneal nerve injury with the “pie crust” technique for valgus release in total knee arthroplasty. J Arthroplasty 2004;19:40-44.
Anderson JE: Grant’s Atlas of Anatomy, ed 7. Baltimore, MD, Lippincott Williams & Wilkins, 1978, pp 4-52, 4-53.
Question 28
A baseball pitcher has intractable posterior and superior shoulder pain. The arthroscopic view seen in Figure 25 shows no Bankart or Hill-Sachs lesion and a negative drive-through sign. There are no signs of ligamentous laxity, but active compression and anterior slide tests are positive. Treatment should consist of
Explanation
REFERENCES: Morgan CD, Burkhart SS, Palmeri M, et al: Type II SLAP lesions: Three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998;14:553-565.
Mileski RA, Snyder RJ: Superior labral lesions in the shoulder: Pathoanatomy and surgical management. J Am Acad Orthop Surg 1998;6:121-131.
Levitz CL, Dugas J, Andrews JR: The use of arthroscopic thermal capsulorrhaphy to treat internal impingement in baseball players. Arthroscopy 2001;17:573-577.
Question 29
A 35-year-old patient sustained a bimalleolar ankle fracture. What is the most reliable method of predicting a tear of the interosseous membrane?
Explanation
REFERENCE: Nielson JH, Sallis JG, Potter HG, et al: Correlation of interosseous membrane tears to the level of the fibular fracture. J Orthop Trauma 2004;18:68-74.
Question 30
Which of the following pharmacologic agents is most likely to adversely affect the success rate of bony union after lumbar arthrodesis?
Explanation
REFERENCES: Glassman SD, Rose SM, Dimar JR, et al: The effect of postoperative nonsteroidal anti-inflammatory drug administration on spinal fusion. Spine 1998;23:834-838.
Dimar JR II, Ante WA, Zhang YP, et al: The effects of nonsteroidal anti-inflammatory drugs on posterior spinal fusions in the rat. Spine 1996;21:1870-1876.
Question 31
Figure 11 shows the radiograph of a 3-year-old girl who sustained a proximal radius injury. Appropriate initial management should include
Explanation
REFERENCES: Leung AG, Peterson HA: Fractures of the proximal radial head and neck in children with emphasis on those that involve the articular cartilage. J Pediatr Orthop
2000;20:7-14.
Radomisli TE, Rosen AL: Controversies regarding radial neck fractures in children. Clin Orthop 1998;353:30-39.
Skaggs DL, Mirzayan R: The posterior fat pad sign in association with occult fracture of the elbow in children. J Bone Joint Surg Am 1999;81:1429-1433.
Gonzalez-Herranz P, Alvarez-Romera A, Burgos J, et al: Displaced radial neck fractures in children treated by closed intramedullary pinning (Metaizeau technique). J Pediatr Orthop 1997;17:325-331.
Question 32
Figures 44a and 44b show the radiographs of a 28-year-old woman who has had progressive hip pain for the past 3 months. What is the most likely diagnosis?
Explanation
REFERENCES: Scarborough M, Moreau G: Benign cartilage tumors. Orthop Clin North Am 1996;27:583-589.
Garrison R, Unni K, McLeod RA, Pritchard DJ, Dahlin DC: Chondrosarcoma arising in osteochondroma. Cancer 1982;49:1890-1897.
Question 33
Figures A and B show radiographs of a 24-year-old female with a soccer injury. A physical examination reveals an isolated, closed injury with no clinical features of neurovascular injury or compartment syndrome. She has been consented to be treated with intramedullary nail fixation. A pre-operative note by the anaesthesiology team makes reference to the patients fair skin and natural red-hair color. How will this information affect the post-operative management of this patient?

Explanation
Melanocortin-1-receptor (MC1R) is one of the key proteins involved in hair color and skin tone. Mutations of the MC1R alleles can render this protein non-functional, which results in a phenotype of red-hair and fair skin. Mutations of the MC1R have shown to modulate the pain response and opioid efficacy in these patients. Women are
more commonly affected and often require more anaesthetic and higher dosages of opioid to achieve comparable MAC level and pain-relief, respectively, as women with other hair types.
Liem et al. showed that a greater concentration of induction and maintenance agents (sevoflurane and desflurane, respectively) were required to sustain comparable MAC levels in red-haired patients as dark haired patients.
Fillingim et al. reviewed the affect of gender, sex and pain. They concluded there is a biopsychosocial element of pain that is perceived differently by men and women. In terms of postoperative and procedural pain, the outcome might be more severe in women than men.
Delaney et al. looked at the involvement of the melanocortin-1 receptor in acute pain in mice. They found that while the MC1R is better known as a gene involved in mammalian hair colour, it was shown to be involved in the pain pathway of inflammatory but not neuropathic origin. Mutations of MC1R showed increased tolerance to noxious pain stimulus in mice.
Figures A and B are AP and lateral radiographs of a left tibia. There is a low energy, distal third shaft fracture with no cortical apposition on the AP view.
Incorrect Answers:
Question 34
Which of the following is a long-term complication of ankle arthrodesis for posttraumatic arthritis?
Explanation
REFERENCES: Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Mazur JM, Schwartz E, Simon SR: Ankle arthrodesis: Long-term follow-up with gait analysis. J Bone Joint Surg Am 1979;61:964-975.
Question 35
A 12-year-old boy reports the acute onset of pain and a pop over the right side of his pelvis while swinging a baseball bat during a Little League game. Radiographs reveal an avulsion of the anterior superior iliac spine with 2 cm of displacement. Management should consist of
Explanation
REFERENCES: Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 139-153.
White KK, Williams SK, Mubarack SJ: Definition of two types of anterior superior iliac spine avulsion fractures. J Pediatr Orthop 2002;22:578-582.
Question 36
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Explanation
REFERENCES: Staheli LT, Chew DE, Elliot JS, Mosca VS: Management of hip dislocations in children with arthrogryposis. J Pediatr Orthop 1987;7:681-685.
Szoke G, Staheli LT, Jaffe K, Hall JG: Medial-approach open reduction of hip dislocation in amyoplasia-type arthrogryposis. J Pediatr Orthop 1996;16:127-130.
Richards BS (ed): Orthopaedic Knowledge Update: Pediatrics. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1996.
Question 37
When harvesting iliac crest bone graft during a posterior spinal decompression and fusion, injury to what structure can result in painful neuromas or numbness over the skin of the buttocks?
Explanation
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins 1998, pp 770-773.
Kurz LT, Garfin SR, Booth RE Jr: Harvesting autogenous iliac bone grafts: A review of complications and techniques. Spine 1989;14:1324-1331.
Mrazik J, Amato C, Leban S, et al: The ilium as a source of autogenous bone grafting: Clinical considerations. J Oral Surg 1980;38:29-32.
Question 38
An 11-year-old girl has had pain in the medial arch of her foot for the past 3 months. She reports that pain is present even with daily activities such as walking to class at school, and ibuprofen provides some relief. She denies any history of trauma. Examination reveals a flexible pes planus with focal tenderness over a prominent tarsal navicular tuberosity. Radiographs show a prominent accessory navicular. Management should consist of
Explanation
REFERENCE: Bordelon RL: Flatfoot in children and young adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 717-756.
Question 39
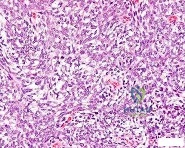
A 13-year-old girl has had right groin pain for the past 3 weeks. She denies any history of trauma. Examination of the hip reveals no palpable soft-tissue mass or lymphadenopathy, and there is full range of motion. A plain radiograph and MRI scan are shown in Figures 15a and 15b. Biopsy specimens are shown in Figures 15c and 15d. What is the most likely diagnosis?
Explanation
REFERENCES: Enneking WF, Gearen PF: Fibrous dysplasia of the femoral neck: Treatment by cortical bone grafting. J Bone Joint Surg Am 1986;68:1415-1422.
Simon MA, Springfield DS, et al: Common Benign Bone Tumors: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, pp 194-200.
Question 40
50%
Explanation
Enneking et al. conducted both radiographic and histologic studies of sixteen massive retrieved human allografts four to sixty-five months after implantation. Analysis of the articular cartilage revealed no evidence that any chondrocytes had survived, even when the graft had been cryoprotected before it was preserved by freezing.
A 64-year-old woman with a longstanding history of rheumatoid arthritis complains of finger dysfunction for the past 6 months. Figure A displays her hand during active extension of all fingers. Figure B displays her hand maintaining her fingers extended following passive extension. What is the next most appropriate treatment for the ring finger?
Spiral oblique retinacular ligament reconstruction
Sagittal band reconstruction
Lateral band reconstruction
Central slip reconstruction
Triangular ligament and transverse retinacular ligament reconstruction
Sagittal band disruption is often associated with rheumatoid arthritis. When this patient attempts to actively extend the affected digit, the extensor tendon
subluxates ulnarly as a result of the sagittal band rupture, and is left with an extensor lag. If one passively extends the finger fully, the patient is able to maintain this position, as the tendon is intact.
Sagittal band reconstruction can be performed with Watson's technique of creating a distally based tendon graft harvested from the central third of the extensor tendon, passed deep to the intermetacarpal ligament and sutured back to itself. Illustration A depicts an intraoperative view of the tendon before reconstruction and Illustration B displays tendon following sagittal band reconstruction. Illustration C displays all of the anatomic locations
of the options listed above.
A splenectomy is performed in a 7-year-old boy following a motor vehicle accident. All of the following are recommended for long-term management EXCEPT:
Pneumococcal vaccination
Haemophilus influenza type B vaccination
Meningococcal group C vaccination
Lifelong prophylactic antibiotics
Hepatitis A vaccination
All of the responses are correct except the need for Hepatitis A vaccine. Hepatitis A is a virus with tropism for hepatocytes which causes infection from fecal-oral contaminated food/water, and shows no increased rate of either infectivity or morbidity in patients with hyposplenism.
Basic recommendations for splenectomized patients include:
All splenectomized patients and those with functional hyposplenism should receive pneumococcal immunization.
Patients not previously immunized should receive haemophilus influenza type B vaccine.
Patients not previously immunized should receive meningococcal group C conjugate vaccine.
Influenza immunization should be given.
Lifelong prophylactic antibiotics are still recommended (oral phenoxymethylpenicillin or erythromycin). This is seemingly despite lack of good data demonstrating a role for lifelong chemoprophylaxis and the acknowledgement that long-term compliance may be problematic.
Davies et al review the current level of evidence supporting these guidelines
for infection prevention in patients with hyposplenism. New to these guidelines are issues regarding occupational exposure and the use of the meningococcal group C and the seven-valent pneumococcal vaccine in non-immunized hyposplenic patients.
Gandhi et al evaluated their nonoperative management of blunt splenic injury in pediatric trauma care. They found compared to historical controls, children with blunt splenic injuries who were hemodynamically stable could be safely monitored with a protocol which required 4 days of inpatient care, 3 weeks of quiet home activities, and 3 months of light activity. This protocol seems to allow for safe return to unrestricted activity.
Incorrect Answer:
Ligaments attach to bone by both direct insertion and indirect insertion. Which of the following most accurately describes the order of the four transition zones of direct insertion?
Ligament > fibrocartilage > mineralized fibrocartilage > bone
Ligament > mineralized fibrocartilage > fibrocartilage > bone
Ligament > mineralized fibrocartilage > periosteum > bone
Ligament > Sharpey's fiber > periosteum > bone
Ligament > periosteum > fibrocartilage > bone
There are two types of tendon/ligament insertion into bone: direct and indirect insertion. The more common, indirect insertion, occurs when the superficial ligament fibers insert into the periosteum. Direct insertion of tendon/ligaments
into bone occurs through a transition of 4 distinct phases: 1) ligament, 2) fibrocartilage, 3) mineralized fibrocartilage, and 4) bone.
While flexing the elbow to perform a biceps curl, what type of muscle contraction is occuring?
Isometric
Isokinetic
Plyometric
Eccentric
Concentric
Concentric muscle contractions occur when a muscle shortens during contraction, as in the upward motion when performing a biceps curl. An eccentric contraction occurs when a muscle lengthens with contraction, as in the "negative" or lowering motion of a biceps curl. An example of an isometric (muscle contracts while maintaining constant length) contraction would be pushing against an immovable object. An example of an isokinetic (muscle has constant speed of contraction) occurs with specialized equipment like Cybex machines. Plyometric contractions occur when a muscle rapidly lengthens just prior to contraction - like during repetitive box jumping.
Woo and Buckwalter describe the mechanisms, barriers, and molecular processes involved in ligament and tendon injury and repair.
A 34-year-old laborer has her left foot crushed in a piece of farming equipment as shown in Figure A. All of the following are reasons for a poor outcome following a crush injury to the foot EXCEPT:
Workers compensation injury
Development of reflex sympathetic dystrophy (complex regional pain syndrome)
Delayed soft-tissue coverage in mangled extremities
Immediate skeletal stabilization
Ongoing litigation
This patient has a mangled extremity. Rigid skeletal stabilization is recommended to enhance soft-tissue healing.
Level 4 evidence from Myerson et al found that delayed soft-tissue coverage in mangled extremities correlated with poor outcome. Poor results also occurred
if treatment was not immediately initiated (immediate debridement shown in Illustration A), if patients subsequently had neuritis or reflex sympathetic dystrophy, or if patients were involved in ongoing workers' compensation and litigation. Neuroischemia following substantial soft-tissue injury likely plays a role in the development of chronic pain after crush injuries to the foot, either through direct trauma to the peripheral nerves or by intraneural or extraneural fibrosis. This trauma to the nerve may cause chronic neuritis, which then triggers a sympathetically mediated reflex sympathetic dystrophy (complex regional pain syndrome).
A 65-year-old man undergoes total knee replacement and is found to have deep vein thrombosis two days later. What molecule is
thought to be involved in this process when it is released during surgical dissection?
Prothrombin
RANKL
IL-1b
Thromboplastin
Factor XI Corrent answer: 4
Thromboplastin is also known more commonly as Tissue Factor (TF), which is involved in the Extrinsic Pathology of the coagulation cascade.
During surgical dissection, insults occur to the endothelial walls of blood vessels. There are three ways in which the body reacts to form a clot so that the patient does not bleed excessively. One is via vessel contraction, another is by collagen release, and a third is by tissue thromboplastin release. Thromboplastin release is part of the extrinsic coagulation pathway (see
Illustration A). Thromboplastin release activates Factor VII which activates Factor X which converts prothrombin to thrombin. Thrombin is the catalyst for converting fibrinogen to fibrin which induces clot formation. While this is useful for decreasing bleeding, it is the same mechanism by which a deep venous thrombosis (DVT) develops.
Which of the following materials has a Young's modulus of elasticity that is most similar to cortical bone
Titanium
Zirconia
Stainless steel
Ceramic (Al2O3)
Alloy (Co-Cr-Mo)
Of the materials listed Titanium has an elastic moduli closest to cortical bone. Titanium is extra-ordinarily light, strong, highly ductile, and corrosion resistant. Titanium is however very notch sensitive and has poor wear resistance.
Young Modulus of Elasticity is defined as the stiffness (ability to maintain
shape under external loading) of a material. On the stress vs. strain curve it is defined as the slope of the line in the elastic zone (see Illustration A). Young’s modulus is constant and different for each material. The relevant moduli (unit GPa) are approximated below:
Question 41
What percentage of bone weight is collagen?
Explanation
Question 42
- A 19-year-old man sustains a complete spinal cord injury at the C7 level as a result of diving into a lake. He has a blood pressure of 90/50 mm Hg, a pulse of 60/min, and respirations of 20/min. These values most likely signify
Explanation
Question 43
A 35-year-old construction worker has developed isolated lateral compartment arthritis. He has lost 50 pounds, now has a body mass index of 30, and still has pain that limits his activities of daily living and work despite receiving a 4-month course of nonsteroidal anti-inflammatory medications and 2 intra-articular cortisone injections. His range of motion is 5 to 110 degrees, and his mechanical axis is 18 degrees of valgus. What is the most appropriate surgical treatment for this patient?
Explanation
Knee arthritis in a young laborer is challenging to address. A surgeon could perform an arthroplasty, but there is concern for early failure and the subsequent need for multiple revisions during this patient’s lifespan. Indications for distal femoral varus osteotomy include at least a 12- to 15-degree valgus mechanical axis and range of motion of at least 15 to 90 degrees. Contraindications for this procedure include inflammatory arthritis and restricted knee motion.
RESPONSES FOR QUESTIONS 138 THROUGH 141
Acute periprosthetic infection
Chronic periprosthetic infection
Joint dislocation
Periprosthetic fracture
Pseudotumor
Femoral nerve palsy
Sciatic nerve palsy
Aseptic prosthetic loosening
Select the total hip arthroplasty (THA) complication listed above that most commonly is associated with the clinical scenario described below.
Question 44
A 62-year-old active man returns for routine follow-up 16 years after hip replacement. He has no hip pain. Radiographs reveal a well-circumscribed osteolytic lesion around a single acetabular screw. All hip components are perfectly positioned. Comparison radiographs obtained 6 months later show an increase in the size of the osteolytic lesion. CT depicts a well-described lesion that is 3 cm at its largest diameter and is localized around one screw hole with an eccentric femoral head. What treatment is appropriate, assuming that well-fixed cementless total hip components are in place?
Explanation
Given a well-fixed acetabular metal shell and a localized osteolytic lesion, good outcomes can be expected from liner revision in this clinical scenario with retention of the metal socket, assuming no damage to the components or other unexpected findings arise during revision surgery. Here, complete cup revision is not warranted, considering the appropriate implant position. Beaulé and associates reviewed 83 consecutive patients (90 hips) in whom a well-fixed acetabular component was retained in a clinical scenario such as the one described. No hip showed recurrence or expansion of periacetabular osteolytic lesions. If the metal cup is unstable, acetabular component revision may be indicated.
Question 45
Which soft-tissue sarcoma is most likely to develop lymphatic metastasis?
Explanation
Question 46
Figure 90 is the radiograph of this patient 5 months later when he returned for his preseason football physical. He is asymptomatic. What is the best next step?
Explanation
This patient has a closed midshaft clavicle fracture with significant displacement that has healed and remodeled nicely with nonsurgical treatment. Functional disability or nonunion after nonsurgical treatment of clavicle fractures in adolescents is rare. Schulz and associates showed no differences in pain, strength, range of motion, or subjective outcome scores between injured and uninjured limbs treated nonsurgically to address displaced, shortened midshaft clavicle fractures in adolescents. Bae and associates demonstrated that clavicle fracture malunions in adolescents do not cause loss of motion or strength.

RESPONSES FOR QUESTIONS 91 THROUGH 96
Chromosome 17 mutation
MYH3 mutation
Embryonic vascular interruption
Infantile vascular interruption
Chromosome 11 mutation
Sporadic inheritance
Select the appropriate etiology listed above for each pictured syndrome.
Question 47
An otherwise healthy 26-year-old woman is involved in a high speed motor vehicle accident and sustains the injury shown in Figure 54 to her dominant right arm. Appropriate treatment of this injury complex includes
Explanation
REFERENCE: Rettig ME, Raskin KB: Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg Am 2001;26:228-235.
Question 48
A 17-year-old girl has multidirectional instability of the shoulder. What is the most appropriate initial management?
Explanation
REFERENCES: Neer CS II, Foster CR: Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder: A preliminary report. J Bone Joint Surg Am 1980;62:897-908.
D’Alessandro DF, Bradley JP, Fleischli JE, et al: Prospective evaluation of thermal capsulorrhaphy for shoulder instability: Indications and results, two- to five-year follow-up.
Am J Sports Med 2004;32:21-33.
Levine WN, Clark AM Jr, D’Alessandro DF, et al: Chondrolysis following arthroscopic thermal capsulorrhaphy to treat shoulder instability: A report of two cases. J Bone Joint Surg Am 2005;87:616-621.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 278-279.
Question 49
Osteoporotic vertebral compression fractures are associated with Review Topic
Explanation
Question 50
Exostoses in which of the following anatomic locations is the most likely to undergo malignant transformation in a patient with multiple hereditary exostosis (MHE)?
Explanation
REFERENCES: Peterson HA: Multiple hereditary osteochondromata. Clin Orthop 1989;239:222.
McCornack EB: The surgical management of hereditary multiple exostosis. Orthop Rev 1981;10:57.
Question 51
- The Magnetic resonance imaging signal characteristics of a high-grade soft-tissue sarcoma are best described as
Explanation
other characteristics, such as size, pattern of growth, integrity of natural boundaries, and homogeneity.
Intravenous contrast agents are not necessary to evaluate neurovascular structures. Both the T1 & T2 weighted images are essential to detect and characterize soft tissue lesions.
Most Tumors have long T1 and T2 relaxation times, therefore, in most instances signal intensity alone is of limited benefit. Exceptions are lipoma, hematoma, intra-lesional hemorrhage.
Hemorrhage may occur in some soft tissue lesions, especially sarcomas, leading to the low T1 and high T2 intensity sound on MR. Miller, indicates that Water, CSF, acute hemorrhage and soft tissue tumors appear dark on T1 and light on T2.
Question 52
A 79-year-old woman with a massive rotator cuff tear presents to the emergency department with pain and difficulty moving her arm 7 weeks after undergoing reverse TSA for a displaced 4-part proximal humerus fracture.
Explanation
The complication rate is high after surgical treatment of proximal humerus fractures, particularly in elderly patients with osteoporotic bone. In patients treated with ORIF, common complications include varus malunion (16%), avascular necrosis (10%), screw penetration (8%), and infection (4%). In cases involving a dislocation of the humeral head, avascular necrosis is more common. In patients treated with hemiarthroplasty or TSA, complications include component loosening, infection, and dislocation. TSA is associated with
glenoid loosening in patients with rotator cuff incompetence and should be avoided in these patients. Reverse TSA is a potential solution for this population. Dislocation and postoperative infection are potential complications after reverse TSA.
RECOMMENDED READINGS
Krappinger D, Bizzotto N, Riedmann S, Kammerlander C, Hengg C, Kralinger FS. Predicting failure after surgical fixation of proximal humerus fractures. Injury. 2011 Nov;42(11):1283-
Question 53
Which of the following studies has the highest sensitivity and specificity in diagnosis of osteonecrosis of the femoral head?
Explanation
REFERENCES: Steinberg ME: Early diagnosis, evaluation, and staging of osteonecrosis, in Jackson DW (ed): Instructional Course Lectures 43. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 513-518.
Glickstein MF, Burk DL Jr, Schiebler ML, et al: Avascular necrosis versus other diseases of the hip: Sensitivity of MR imaging. Radiology 1988;169:213-215.
Question 54
.What is the most common detrimental impact of an unplanned excision of a high-grade soft-tissue sarcoma?
Explanation
Figures 64a through 64c are the radiograph, MRI scan, and histology of a 53-year-old man with medial knee pain and swelling below the knee.

Question 55
Nerve conduction velocity is slowed by
Explanation
A number of factors affect nerve conduction velocity; for example, increased body temperature increases nerve conduction velocity. Nerve conduction velocity is slowed by advancing age, compression, decreased blood flow, and fibrosis (from large imprecise sutures used for nerve repair). There is no association between hand dominance and nerve conduction velocity.
Question 56
Which of the following changes is seen with age and degeneration in the intervertebral disk? Review Topic
Explanation
Question 57
An inverted radial reflex is associated with
Explanation
REFERENCES: Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 1998, p 762.
Vaccaro AR, Betz RR, Zeidman SM (eds): Principles and Practice of Spine Surgery. St Louis, MO, Mosby, 2002, p 323.
Question 58
A 17-year-old boy underwent open reduction and internal fixation of a navicular fracture 5 days ago. A follow-up examination now reveals a tensely swollen foot with erythema and multiple skin bullae. The patient is febrile and has marked pain with palpation of the entire forefoot and hindfoot. What is the next step in management?
Explanation
REFERENCES: Ault MJ, Geiderman J, Sokolov R: Rapid identification of group A streptococcus as the cause of necrotizing fasciitis. Ann Emerg Med 1996;28:227-230.
McHenry CR, Piotrowski JJ, Pentrinic D, Malangoni MA: Determinants of mortality for necrotizing soft-tissue infections. Ann Surg 1995;221:558-563.
Question 59
- Which of the following injuries is most commonly associated with a fracture of the scapular body?
Explanation
Question 60
A 37-year-old recreational athlete has osteoarthritis of the glenohumeral joint. He has failed nonsurgical measures and is interested in surgical intervention but would like to avoid arthroplasty. When performing shoulder arthroscopy for glenohumeral arthritis, which radiographic parameter is most predictive of clinical failure?
Explanation
22% conversion to total shoulder arthroplasty at 10.1 months.
Question 61
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of
Explanation
REFERENCES: Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Pemberton PA: Pericapsular osteotomy of the ilium for the treatment of congenital subluxation and dislocation of the hip. J Bone Joint Surg Am 1965;47:65-86.
Question 62
Figures 21a and 21b show the clinical photograph and radiograph of a 15-year-old girl who has a deformity of her feet. Her parents are concerned because there is a family history of Charcot-Marie-Tooth disease. The patient reports some mild instability of the ankle and has noticed mild early callosities; however, she is not having any significant pain. Coleman block testing reveals a forefoot valgus and supple hindfoot. She has weakness to eversion and dorsiflexion. Initial management should consist of
Explanation
REFERENCES: Pinzur MS: Charcot’s foot. Foot Ankle Clin 2000;5:897-912.
Holmes JR, Hansen ST Jr: Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486.
Thometz JG, Gould JS: Cavus deformity, in The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 343-353.
Question 63
A 14-year-old boy sustained a femoral neck fracture in a fall from a tree and underwent open reduction and internal fixation 6 months ago. Follow-up examination now reveals an antalgic Trendelenburg gait and painful range of motion. A radiograph is shown in Figure 23, and a CT scan shows a nonunion. Treatment should consist of
Explanation
REFERENCES: Lam SF: Fractures of the neck of the femur in children. J Bone Joint Surg Am 1971;53:1165-1179.
Canale ST, Beaty JH: Pelvic and hip fractures, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1109-1193.
Question 64
Figure 55 shows the radiograph of a 30-year-old man who sustained a closed comminuted fracture of the right clavicle. Examination reveals decreased sensation in the radial nerve distribution. Weakness is noted with shoulder abduction, internal rotation, and wrist extension. A displaced bone fragment is most likely pressing on what portion of the brachial plexus? Review Topic

Explanation
Question 65
A 7-year-old boy sustained a head contusion and small bowel injuries in a motor vehicle accident in which he was wearing a lap belt. He subsequently required a bowel resection. Six weeks after the accident, his parents note a painful mass in his lower back. His neurologic examination is normal. A radiograph and CT scans are shown in Figures 47a through 47c. Definitive management should now consist of
Explanation
REFERENCES: Ebraheim NA, Savolain ER, Southworth SR, et al: Pediatric lumbar seat belt injuries. Orthopedics 1991;14:1010-1013.
Taylor JA, Eggli KD: Lap belt inhuries of the lumbar spine in children: A pitfall in CT diagnosis. Am J Rad 1988;150:1355-1358.
Question 66
Which of the follow scenarios is most likely to be amenable to a complete repair of a massive rotator cuff tear? Review Topic
Explanation
Question 67
An 18-month-old boy with obstetric brachial plexus palsy is being evaluated for limited right shoulder motion. Physical therapy for the past 6 months has failed to result in improvement of the contracture. Which of the following studies is necessary prior to any shoulder reconstruction?
Explanation
REFERENCES: Waters PM: Update on management of pediatric brachial plexus palsy.
J Pediatr Orthop B 2005;14:233-244.
Waters PM, Bae DS: Effect of tendon transfers and extra-articular soft-tissue balancing on glenohumeral development in brachial plexus birth palsy. J Bone Joint Surg Am
2005;87:320-325.
Moukoko D, Ezaki M, Wilkes D, et al: Posterior shoulder dislocation in infants with neonatal brachial plexus palsy. J Bone Joint Surg Am 2004;86:787-793.
Question 68
Figures 6a and 6b are the radiographs of a thin 23-year-old man who sustained a closed injury to his left arm in a fall. He has no other injuries and his

Explanation
Question 69
Which of the following best describes the relative content of the components of articular cartilage in decreasing order?
Explanation
REFERENCE: Schiller AL: Pathology of osteoarthritis, in Kuettner KE, Goldberg VM: Osteoarthritic Disorders. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995,
pp 95-101.
Question 70
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?
Explanation
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Yokoyama K, Itoman M, Kobayashi A, et al: Functional outcomes of “floating elbow” injuries in adult patients. J Orthop Trauma 1998;12:284-290.
Question 71
An 18-year-old football player reports acute pain and swelling after a direct injury to his plantar flexed foot. Examination reveals midfoot swelling and tenderness. Nonstanding radiographs are normal. What is the next most appropriate step in management?
Explanation
to activity.
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 39-54.
Chiodo CP, Myerson MS: Developments and advances in the diagnosis and treatment of injuries with the transmetatarsal joint. Orthop Clin North Am 2001;32:11-20.
Question 72
A 13-year-old boy has pain and a firm mass in his left knee. A radiograph and MRI scan are shown in Figures 2a and 2b, and a biopsy specimen is shown in Figure 2c. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 267.
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990,
pp 14-15.
Question 73
A 7-year-old boy sustained an acute puncture wound of the foot after stepping barefoot on a piece of glass 1 day ago. His mother states that she is not sure if she got the piece of glass out; however, she reports that his immunizations are up-to-date. Examination reveals that the wound is slightly erythematous, less than 1 mm in length on the heel, and is not currently draining. What is the next most appropriate step im management?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 199-205.
DeCoster TA, Miller RA: Management of traumatic foot wounds. J Am Acad Orthop Surg 1994;2:226-230.
Question 74
Which of the following increases radiation exposure to patients and personnel during surgery?
Explanation
REFERENCE: Wagner L, Archer B: Minimizing Risks from Fluoroscopic X-rays: A Credentialing Program for Anesthesiologists, Cardiologists, Surgeons, Radiologists, and Urologists, ed 3. The Woodlands, TX, Partners in Radiation Management, 2000.
Question 75
.Figures 75a through 75d are the radiograph, CT scan, bone scan, and biopsy of a 45-year-old man who has had a several-month history of progressive pain in his right hip and groin region. Based on these images and histology, what is the most appropriate treatment?
Explanation

Question 76
A 57-year-old man involved in a motor vehicle accident sustains an injury to his right shoulder. A spot AP radiograph is shown in Figure 34. What is the next most appropriate step in the orthopaedic management of this patient?
Explanation
REFERENCE: Simon JA, Puopolo SM, Capla EL, et al: Accuracy of the axillary projection to determine fracture angulation of the proximal humerus. Orthopedics 2004;27:205-207.
Question 77
Figures 1 and 2 are the radiograph and MRI scan of a 16-year-old boy who injured his right knee by a lateral side impact while playing football. The MRI indicates what structure was most likely injured?

Explanation
Question 78
A 20-year-old soccer player who collapsed after a goal kick reports weakness and nausea. He appears slightly confused. Examination reveals that he is not sweating. His skin is warm and dry. The outdoor temperature is 80 degrees F (26.6 degrees C) with a relative humidity of 80%. Management should consist of
Explanation
REFERENCES: Griffin LY: Emergency preparedness: Things to consider before the game starts. J Bone Joint Surg Am 2005;87:894-902.
Barker TA, Motz HA, Gersoff WK: Environmental factors in athletic performance, in Fu FH, Stone DA (eds): Sports Injuries, ed 2. Philadelphia, PA, Lippincott, 2001, pp 67-68.
Roberts WO: Environmental concerns, in Kibler WB (ed): ACSM’s Handbook for the Team Physician. Baltimore, MD, Williams & Wilkins, 1996, p 172.
Question 79
-Figure 39 is the anteroposterior radiograph of a marathon runner who has left groin pain that prevents her from running. She recently got back into her usual running routine after an ankle injury preventedbher from running for several months. She now has pain with any weight bearing. What is the most appropriate treatment option?
Explanation

Question 80
A 41-year-old right-hand-dominant man has been treated nonsurgically for right elbow arthritis. His radiographs reveal end-stage ulnohumeral arthritis with complete loss of the joint space. He reports pain during the mid-arc of elbow flexion and extension. During the last 8 years, he has attempted activity modification, medication, physical therapy, and multiple cortisone injections. His symptoms have progressed, resulting in constant pain, loss of a functional range of motion, and an inability to perform many activities of daily living. Secondary to his age and activity demands, he undergoes a soft-tissue interposition arthroplasty of his elbow with an Achilles allograft. Which presurgical finding correlates with elevated risk for postsurgical complications?
Explanation
restrictions for patients after surgery and remains a reasonable salvage procedure. Larson and Morrey published their findings on 38 patients with a mean age of 39 years following soft-tissue interposition arthroplasty for posttraumatic and inflammatory end-stage elbow arthritis. These investigators reported a significant improvement in Mayo Elbow Performance Score in addition to improvement in the flexion- extension arc from 51° to 97° after surgery. They reported worse results and elevated incidence of complications for patients with presurgical elbow instability upon examination; retained hardware from prior
surgery was not deemed a contraindication.
Question 81
Which muscles are responsible for the displacement of the proximal fragment of the fracture shown in Figure 75?

Explanation
(SBQ12TR.39) A 36-year-old male falls from a 10-ft scaffold and suffers the injuries shown in Figures A and B. The patient is placed in a spanning external fixator and brought back to the operating room once his soft tissues are amenable. Planning to use a dual-incision approach, what is the correct interval to use when approaching the medial side?
Popliteus and pes anserine
Lateral head of the gastrocnemius and pes anserine
Politeus and lateral head of the gastrocnemius
Iliotibial band and medial head of the gastrocnemius
Pes anserine and medial head of the gastrocnemius
The posteromedial approach to the tibial plateau is between the the pes anserine tendons and the medial head of the gastrocnemius.
A dual-incision approach is often utilized to optimally place definitive fixation for bicondylar tibial plateau fractures. For fractures that require posterior or posteromedial fixation, the correct interval is between the pes anserine and the medial head of the gastrocnemius.
Higgins et al. in a large cohort morphological review, noted a high incidence of a posteromedial fragment in bicondylar fractures. Occurring at a high frequency, the
authors recommended direct visualization and reduction via a dual approach rather than using indirect reduction techniques.
Falker et al. describes a step-by-step approach to utilizing the posteromedial approach for the tibial plateau and placing an anti-glide plate.
Figure A and B exhibit a bicondylar tibial plateau fracture with a posteromedial fragment noted on the lateral x-ray. Illustration A exhibits the surrounding anatomy and interval in between the medial head of the gastrocnemius and the pes anserine.
Incorrect answers:
Question 82
A 53-year-old man complains of recurrent lateral elbow pain. He was surgically treated approximately one year ago with some improvement in his direct lateral elbow pain. He now reports new-onset discomfort at the posterolateral elbow, as well as difficulty when pushing himself up from a chair. On examination, he has a well-healed 6-cm incision over the lateral epicondyle with full active and passive range of motion. He has pain with palpation along the posterior lateral elbow and a positive posterior drawer test. Radiographs are unremarkable. What is the best next step?
Explanation
instability of the elbow, for which the recommended treatment is lateral collateral ligament reconstruction.
Question 83
An increase in advanced glycation end-products (AGEs) is characteristic of which of the following clinical conditions and results in which pathologic process?
Explanation
AGEs are produced from spontaneous nonenzymatic glycation of proteins when sugars (glucose, fructose, ribose) react with lysine or arginine residues. Because of the low turnover, cartilage is susceptible to AGEs accumulation. The accumulation of AGEs has been thought to play a role in the development of OA of the knee and ankle.
Li et al. reviewed age-related changes in cartilage. They state that with aging, there is excessive collagen cross-linking increases cartilage stiffness, while shortening/degradation of aggrecan leads to loss of sugar side chains and water-binding ability, while increased levels of AGEs are associated with a decline in anabolic activity. There is also increased chondrocyte death and/or apoptosis.
Anderson et al. reviewed the relationship between osteoarthritis and aging. They state that knee cartilage thins with aging (especially on the femoral and patellar sides, suggesting a gradual loss of cartilage matrix. AGEs formation leads to modification of type II collagen by cross-linking of collagen molecules, increasing stiffness and brittleness and increasing susceptibility to fatigue failure.
Incorrect Answers:
Question 84
- Which of the following nerves supply the muscles on each side of internervous plane identified when performing the anterior (Smith-Petersen) approach to the hip?
Explanation
Question 85
Which of the following hip fracture patterns is at increased risk of proximal fragment flexion malreduction with dynamic hip screw fixation?

Explanation
Mohan et al conducted a study to assess the effect of clockwise rotational torque onto the fracture configuration in unstable and stable intertrochanteric fractures fixed with a dynamic hip screw construct. They found that 11 out of 30 unstable fractures showed an anterior spike (flexion malreduction) in left-sided fixations due to clockwise torque. This malreduction was not present in right-sided or stable fractures.
Question 86
A 35-year-old woman reports worsening pain after undergoing a neurectomy in the third interspace for a Morton’s neuroma 12 months ago. She states that the pain is sharp and electrical, worse than before her surgery, and prevents her from participating in her usual work and exercise activities. Use of wider shoes and pads used before her surgery have failed to provide relief. Examination does not reveal any deformity or inflammation. Tenderness along with neuritic pain occurs with compression of the plantar aspect of the foot between the third and fourth metatarsal head area. To most reliably alleviate her pain, management should consist of
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 101-111.
Johnson JE, Johnson KA, Unni KK: Persistent pain after excision of an interdigital neuroma: Results of reoperation. J Bone Joint Surg Am 1988;70:651-657.
Beskin JL, Baxter DE: Recurrent pain following interdigital neurectomy: A plantar approach. Foot Ankle 1988;9:34-39.
Amis JA, Siverhus SW, Liwnicz BH: An anatomic basis for recurrence after Morton’s neuroma excision. Foot Ankle 1992;13:153-156.
Question 87
What is the most appropriate plating technique utilized for the medial malleolus fracture typically seen in a displaced supination-adduction ankle fracture?

Explanation
According to the referenced article by Toolan et al, placement of two horizontal (perpendicular to the fracture line) lag screws from medial to lateral are biomechanically the most important aspect of the construct whether a plate is used or not.
Question 88
Figure 91 is the radiograph of a 20-year-old man who kicked a door while intoxicated. At the emergency department, his leg is placed into a long-leg cast. After 2 hours, he reports increasing pain, numbness, and tingling in his toes. What is the most appropriate initial treatment?

Explanation
(SBQ12TR.88) When evaluating a fracture dislocation of the elbow, a varus and posteromedial rotation mechanism of injury typically results in what injury pattern?
A fracture of the radial head requiring ORIF
A highly comminuted radial head fracture requiring radial head arthroplasty or resection
An MCL injury requiring repair
A type I avulsion fracture of the coronoid
An anteromedial coronoid fracture
A varus and posteromedial rotation mechanism of injury typically results in a fracture of the anteromedial facet of the coronoid which frequently requires reduction and fixation to restore stability.
A varus and posteromedial mechanism of injury about the elbow presents with an injury pattern distinctly different from other injury patterns. A key part of treating this injury pattern is recognizing a fracture of the anteromedial facet of the coronoid, which often requires reduction and fixation to restore stability about the elbow. It is important to recognize this during preoperative planning since this injury typically requires a medial approach.
Steinman presents a review article describing coronoid fracture patterns and their mechanisms of injury.
Doornberg and Ring present a level 4 review showing that coronoid fracture patterns and their required treatments are predictable based on mechanism of injury. Varus and posteromedial mechanisms were found to reliably create a fracture of the anteromedial facet of the coronoid, and were associated with sparing of the MCL and radial head.
Doornberg and Ring also presented a Level 3 review of anteromedial facet cornoid fractures. They found that they could not be adequately visualized and treated from a lateral approach, and that they typically required reduction and fixation to restore adequate stability to the elbow. This stresses the importance of recognizing this injury pattern during preoperative planning.
Illustrations A and B are AP and lateral radiographs of an elbow following a varus/posteromedial injury with an anteromedial coronoid facet fracture. Illustration C is a diagram demonstrating fracture lines that create an anteromedial facet fracture fragment. This fracture can be subclassified into three subtypes [anteromedial rim (a), rim plus tip (b), and rim and tip plus the sublime tubercle (c)]
Incorrect answers:
(SBQ12TR.78) A 67-year-old female patient presents with increasing right hip/thigh pain over the past three months, which is now recalcitrant to anti-inflammatories. There is no history of trauma or constitutional symptoms. Her past medical history consists of hypertension, coronary artery disease, osteoporosis and gastric reflux. Physical examination reveals mild pain at the extremes of range of motion of the hip and a painful right sided limp. A radiograph of the right hip is seen in Figure A. What would be the most appropriate treatment for this patient at this time? Review Topic

Observation only
Referral to physiotherapy
MRI spine and hip
Total hip arthroplasty
Intramedullary femoral nail
This osteoporotic female patient is presenting with subtrochanteric lateral cortical thickening and hip pain. This is consistent with an insufficiency fracture of the femur secondary to use of bisphosphonate medication for treatment of osteoporosis. The most appropriate treatment would be intramedullary femoral nail fixation.
Bisphosphonate medications have been shown to be associated with atypical (subtrochanteric) femur fractures. These patients often have prodromal hip pain and lateral cortical thickening on radiographs prior to fracture. In addition, there has shown to be a significantly increased risk of fracture in the presence of the “dreaded black line” that occurs at the site of thickening.
Lenart et al. examined a case series of patients using bisphosphonates for the treatment of osteoporosis. They identified 15 postmenopausal women who had been receiving alendronate for a mean (±SD) of 5.4±2.7 years and who presented with atypical low-energy fractures. Cortical thickening was present in the contralateral femur in all the patients with this pattern.
Goh et al. retrospectively reviewed patients who had presented with a low-energy subtrochanteric fractures. They identified 13 women of whom nine were on long-term alendronate therapy. Five of these nine patients had prodromal pain in the affected hip in the months preceding the fall, and three demonstrated a stress reaction in the cortex in the contralateral femur.
Figure A shows a right hip radiograph with subtrochanteric lateral cortical thickening. There is mild arthritic changes in the hip. Illustration A shows a bone scan and radiographs of subtrochanteric lateral cortical thickening that resulted in fracture.
Incorrect Answers
Question 89
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?

Explanation
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal. The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
Question 90
Figure 88 is the radiograph of a 68-year-old man who fell 3 weeks after undergoing a successful left primary total hip arthroplasty. He is experiencing a substantial increase in pain and an inability to bear weight. What is an appropriate treatment plan?
Explanation
Based on the fact that the fracture is occurring around the stem (type B) and the stem is clearly loose (type B2), the appropriate treatment is removal of the in situ stem (which is loose), ORIF of the femur (cerclage wires, cables, or a plate would be acceptable), and insertion of a longer revision stem (a tapered fluted modular titanium or fully porous coated cylindrical stem) to bypass the fracture. All other responses are incorrect because they provide inappropriate treatment options for a Vancouver B2 fracture.
Question 91
Following resection of malignant tumors, complications related to endoprosthetic reconstruction are most common in what anatomic location?
Explanation
REFERENCE: Horowitz SM, Glasser DB, Lane JM, Healey JH: Prosthetic and extremity survivorship after limb salvage for sarcoma: How long do the reconstructions last? Clin Orthop 1993;293:280-286.
Question 92
Hamstring lengthening and posterior transfer of the rectus femoris will be most successful in a patient with cerebral palsy who has which of the following gait abnormalities?
Explanation
REFERENCES: Gage JR, Perry J, Hicks RR, Koop S, Werntz JR: Rectus femoris transfer to improve knee function of children with cerebral palsy. Dev Med Child Neurol 1987;29:159-166.
Sutherland DH, Santi M, Abel MF: Treatment of stiff-knee gait in cerebral palsy: A comparison by gait analysis of distal rectus femoris transfer versus proximal rectus release. J Pediatr Orthop 1990;10:433-441.
Question 93
A 38-year-old woman has persistent elbow pain but is unable to recall a specific traumatic event. Examination reveals that the patient exhibits apprehension when the elbow is placed in valgus with forearm supination and axial loading. Because of chronicity and failure to respond to nonsurgical management, what is the most appropriate treatment? Review Topic
Explanation
Question 94
Type I collagen fibers in peripheral nerves are primarily responsible for which of the following?
Explanation
The COL1A1 gene produces a component of type I collagen, called the pro-alpha1(I) chain. This chain combines with another pro-alpha1(I) chain and also with a pro-alpha2(I) chain (produced by the COL1A2 gene) to make a molecule of type I procollagen. These triple-stranded, rope-like procollagen molecules must be processed by enzymes outside the cell. Once these molecules are processed, they arrange themselves into long, thin fibrils that cross-link to one another in the spaces around cells. The cross-links result in the formation of very strong mature type I collagen fibers.
Wong et al. provide a review of the basic science behind nerve healing and the recovery after nerve repair. They note the importance of minimizing additional surgical insult and careful handling of nerve tissue during repair to optimize outcomes.
Pertici et al. noted that autologous nerve implantation to bridge a long nerve gap presents the greatest regenerative performance in spite of substantial drawbacks. They were able to show improved nerve guided regrowth with a type I collagen matrix conduit as compared to a conduit made of a mix of type I and type III collagen.
Illustration A shows a diagram of type I collagen, showing the rope-like characteristics behind the tensile strength.
Incorrect Answers:
Question 95
An 83-year-old man has a painful mass of the great toe. Radiographs and a biopsy specimen are seen in Figures 22a and 22b. What is the most likely diagnosis?
Explanation
REFERENCES: Hamilton W, Breedman KB, Haupt HM, Lackman R: Knee pain in a 40-year-old man. Clin Orthop 2001;383:282-285,290-292.
Mizel M, Miller R, Scioli M (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 301-302.
Question 96
The radiographic finding in Figure 58 is indicative of what type of acetabular fracture?

Explanation
(SBQ12TR.58) A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries? Review Topic

Bilateral open reduction and internal fixation
Open reduction internal fixation on the right, reamed intramedullary nailing on the left
Temporizing external fixation on the right, open reduction and internal fixation on the left
Bilateral reamed intramedullary nailing
Bilateral temporizing external fixation
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
Question 97
A patient with a transverse femur fracture undergoes statically locked antegrade intramedullary nailing. Postoperatively, the patient appears to have a
Explanation
Question 98
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of
Explanation
REFERENCES: Vincent KA: Tarsal coalition and painful flatfoot. J Am Acad Orthop Surg 1998;6:274-281.
Olney BW: Tarsal coalition, in Drennan JC (ed): The Child’s Foot and Ankle. New York, NY, Raven Press, 1992, pp 169-181.
Question 99
An infant is born with a mass that involves both the volar and dorsal compartments of the left arm. A clinical photograph and biopsy specimen are shown in Figures 41a and 41b. What is the best initial course of action?
Explanation
REFERENCE: Kurkchubasche AG, Halvorson EG, Forman EN, Terek RM, Ferguson WS: The role of preoperative chemotherapy in the treatment of infantile fibrosarcoma. J Pediatr Surgery 2000;35:880-883.
Question 100
A 32-year-old motorcycle rider is involved in a motor vehicle accident and radiographs show a burst fracture at L2 with 20 degrees of kyphosis. The neurologic examination is consistent with unilateral motor and sensory involvement of the L5, S1, S2, S3, and S4 nerve roots. He has no other injuries. CT demonstrates 20% anterior canal compromise with displaced laminar fractures at the level of injury. What is the best option for management of this patient?
Explanation
REFERENCES: Cammisa FP Jr, Eismont FJ, Green BA: Dural laceration occurring with burst fractures and associated laminar fractures. J Bone Joint Surg Am 1989;71:1044-1052.
Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 201-216.
