Orthopedic Board Prep MCQs: Arthroplasty & Trauma | Part 152

Key Takeaway
This page offers Part 152 of a comprehensive orthopedic board review. It features 100 high-yield, verified MCQs tailored for orthopedic surgeons and residents preparing for their OITE, AAOS, and ABOS certification exams. Enhance your knowledge and exam readiness with interactive study and exam modes.
About This Board Review Set
This is Part 152 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 152
This module focuses heavily on: Arthroplasty, Fracture, Hip, Knee, Revision, Shoulder.
Sample Questions from This Set
Sample Question 1: A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patien...
Sample Question 2: Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management?L Intensive phys...
Sample Question 3: A “p value” of 4% (p=0.04) indicates that the...
Sample Question 4: A 20-year-old man has activity-related deep-seated shoulder pain in his dominant right shoulder. He has taken 3 months off training as a college javelin thrower, and management consisting of physical therapy has failed to provide relief. Sh...
Sample Question 5: What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 32-year-old man has a Glasgow Coma Scale score of 8 and an open pelvic fracture. The patient’s family reports that he is a Jehovah’s Witness. Initial hemodynamic instability has resolved. In the operating room during a washout, the patient’s blood pressure becomes unstable. What is the most appropriate action?
Explanation
REFERENCES: Jimenez R, Lewis VO (eds): Culturally Competent Care Guidebook. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007.
Jehovah’s Witnessess Official Web Site: Medical Care and Blood, 2008, http://www.watchtower.org/e/medical_care_and_blood.htm
Question 2
Figure 46 shows the radiograph of a 65-year-old man who reports restricted range of motion and pain with sitting 18 months after undergoing right side revision total hip arthroplasty. What is the most appropriate management? L Intensive physiotherapy
Explanation
REFERENCES: Board TN, Karva A, Board RE, et al: The prophylaxis and treatment of heterotopic ossification following lower limb arthroplasty. J Bone Joint Surg Br 2007;89:434-440.
Harkess JW, Crockarell JR: Arthroplasty of the hip, in Canale ST, Beaty JH (eds): Campbell’s Operative
Orthopaedics, ed 11. Philadelphia, PA, Mosby Elsevier, 2008, vol 1, pp 314-483.
Question 3
A “p value” of 4% (p=0.04) indicates that the
Explanation
The p value is the probability that the chance selection of patients might suggest a difference in treatment that was not real. Only with a small p value are we willing to believe that the observed difference in treatment is very likely real and not simply due to chance.
The confidence interval provides a measure of the magnitude of the possible difference between two groups of patients, regardless of whether or not the p value was small. This makes the confidence interval more informative than the p value when different treatments are compared. This is much beyond the scope of this review.
Question 4
A 20-year-old man has activity-related deep-seated shoulder pain in his dominant right shoulder. He has taken 3 months off training as a college javelin thrower, and management consisting of physical therapy has failed to provide relief. Shoulder arthroscopic views are shown in Figures 16a through 16c. What is the underlying association with this condition? Review Topic
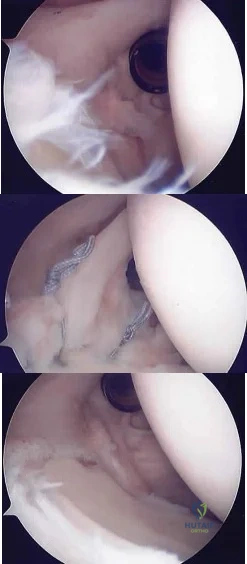
Explanation
Question 5
What postoperative complication occurs at a significantly higher rate in patients undergoing bilateral simultaneous total knee arthroplasty than in patients undergoing unilateral total knee arthroplasty?
Explanation
REFERENCE: Parvizi J, Sullivan TA, Trousdale RT, Lewallen DG: Thirty-day mortality after total knee arthroplasty. J Bone Joint Surg Am 2001;83:1157-1161.
Question 6
A prospective, randomized controlled trial of 150 patients undergoing total hip arthroplasty is performed to test whether repair of the capsule during a posterior approach reduces post-operative dislocations in the first three months. The study found no difference in dislocation rate if the capsule was repaired versus not repaired (p = .34). Subsequently, a multicenter follow-up study of 2000 patients showed that repairing the capsule led to a decreased dislocation rate in the first three months (p = .03). Assuming the second study reflects reality, which of the following errors occurred in the first study?
Explanation
A study can have two types of errors. Type-I errors, or alpha errors, occur when the null hypothesis is rejected when it should have been accepted. The alpha level refers to the probability of a type-I error. By convention, the alpha level of significance is set at 0.05, which means that we accept the finding of a significant association if there is less than a one in twenty chance that the observed association was due to chance alone. Type-II errors, or beta errors, occur when the null hypothesis is accepted when it should be rejected. This often occurs when studies are underpowered. In the example above, the null hypothesis is that repair of the capsule does not reduce dislocations within the first three months. Since the first study did not show a
statistically significant difference, the null hypothesis was accepted. Since a more powered study showed that repair of the capsule does reduce dislocations, the null hypothesis should have been rejected in the initial study (if it was adequately powered).
Fosgate et al. review the importance of sample size calculations when performing research. They state that sample size ensures statistical significance if the subsequent data collection is perfectly consistent with the assumptions made for the sample size calculation (assuming power was set as 50% or greater).
Illustration A shows the difference between type-I and type-II errors. Video V is a lecture discussing statistical definition review of PPV, NPV, sensitivity and specificity.
Incorrect Answers:
Question 7
What proteinaceous compound binds to hyaluronic acid to function as an effective boundary molecular layer in articular cartilage?
Explanation
Question 8
A healthy 64-year-old man just underwent an uncomplicated shoulder arthroplasty for severe glenohumeral osteoarthritis. Intraoperatively, 60 degrees of external rotation was obtained. Postoperatively, he starts on a range-of-motion program. What limitations are recommended? Review Topic
Explanation
surgery. Restriction from external rotation stretching for even 3 weeks would compromise his ultimate functional recovery.
Question 9
- Which of the following types of sarcoma of the bone is most sensitive to external beam radiation?
Explanation
Question 10
Figure 4 shows the AP radiograph of a 28-year-old woman who has had moderate pain in the left hip for the past year. Nonsurgical management has failed to provide relief. She denies any history of hip pain, pathology, or trauma. Management should consist of
Explanation
REFERENCES: Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Pemberton PA: Pericapsular osteotomy of the ilium for the treatment of congenital subluxation and dislocation of the hip. J Bone Joint Surg Am 1965;47:65-86.
Question 11
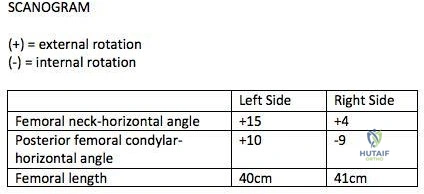
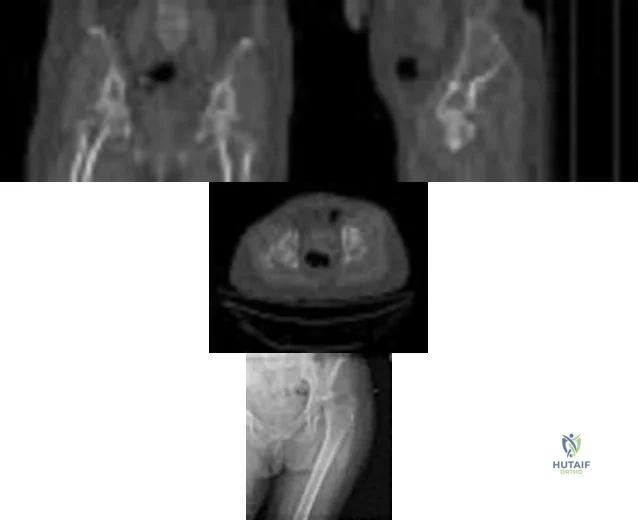
A 26-year-old male underwent statically locked intramedullary nail fixation for a comminuted left femur fracture. An early post-operative computed tomography (CT) scanogram was taken to check rotational alignment, as shown in Figure A. What would be the next best step in the management of this patient?
Explanation
>15 degrees and symptomatic. Therefore, the most appropriate next step would be to continue with postoperative observation and close follow-up.
The primary purpose of CT scanogram is to measure the angle of rotation of the femoral neck relative to the femoral condyle. To do this, the right and left femurs must be scanned together using a 5mm helical slice scanner at the hip and knee. The first slice should reveal the alignment of the femoral neck, so as to allow for measurement of the femoral neck-to-horizontal (FNH) angle. The second slice should reveal the alignment of the posterior femoral condyles. This allows measurement of the posterior condyle-to-horizontal (PCH) angle. Finally, to calculate the rotational alignment (RA), the FNH angle and PCH angles are subtracted (e.g., RA = FNH -PCH). Normal RA is usually +5 to +20 degrees, which is also referred to as 5 to 20 degrees of femoral anteversion.
Lindsey et al. reviewed femoral malrotation following intramedullary nail fixation. They showed the incidence of rotational malalignment was ~28%. Normal femoral neck anteversion (angle of the femoral neck relative to the transverse axis through the femoral condyles) is ~11-13°. However, they noted that some patients have up to 15° difference in rotation in native limbs. Therefore <15 degrees of rotational difference after fixation is considered acceptable.
Gugala et al. examined the long-term functional implications for patients with iatrogenic femoral malrotation following femoral intramedullary nail fixation. They
showed that patients can compensate for even significant femoral malrotation (up to 30 degrees) and tolerate it well. However, external femoral malrotation (more common) appears to be better compensated/tolerated than internal malrotation.
Figure A shows that the left femoral neck is externally rotated (ER) by 15° to the horizontal (ER15). The right femoral neck is externally rotated (ER) by 4° to the horizontal (ER4). The left distal fragment is ER10. The right distal fragment is internally rotated (IR) by 9°. Thus, left femur has a total (ER15)-(ER10)= (+15)-(+10)=(+5), and right femur has (ER4)-(IR9)= (+4)-(-9)=(+13) to the horizontal. Therefore, the difference is 8 degrees.
Incorrect Answers:
>15 degrees and symptomatic.
Question 12
Figures 23a and 23b show the radiographs of a 75-year-old woman who sustained an injury to her nondominant hand. Initial treatment should consist of
Explanation
REFERENCES: Handoll HH, Madhok R: Conservative interventions for treating distal radial fractures in adults. Cochrane Database Syst Rev 2003;2:CD000314.
Young CF, Nanu AM, Checketts RG: Seven-year outcome following Colles’ type distal radial fracture: A comparison of two treatment methods. J Hand Surg Br 2003;28:422-426.
Question 13
A 35-year-old construction worker continues to have weakness with lifting overhead 2 years after he was treated with physical therapy for a "chest muscle" tear. An obvious deformity noted in his axilla worsens with resisted extension and adduction. A clinical photograph and MRI scan are shown in Figures 119a and 119b. What is the most appropriate treatment? Review Topic
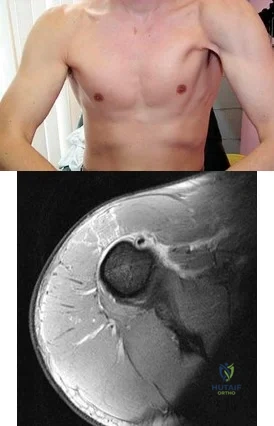
Explanation
Question 14
What is the primary intracellular signaling mediator for bone morphogenetic protein (BMP) activity?
Explanation
REFERENCES: Lieberman J, Daluiski A, Einhorn TA: The role of growth factors in the repair of bone: Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.
Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Zuscik MJ, Drissi MH, Reynolds PR, et al: Molecular and cell biology in orthopaedics, in Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006,
in press.
Question 15
Anabolic steroid use has which of the following effects on serum lipoprotein levels?
Explanation
REFERENCES: Hartgens F, Rietjens G, Keizer HA, et al: Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a). Br J Sports Med 2004;38:253-259.
Blue JG, Lombardo JA: Steroids and steroid-like compounds. Clin Sports Med
1999;18:667-689.
Question 16
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition? Review Topic

Explanation
Question 17
What factor is associated with the highest risk for in-hospital complications for patients undergoing a lumbar fusion for degenerative spondylolisthesis? Review Topic
Explanation
Question 18
Which of the following findings is considered the strongest indication for surgical treatment of a mallet fracture of the distal phalanx?
Explanation
REFERENCES: Green DP, Butler TE Jr: Fractures and dislocations in the hand, in Rockwood CA, Green DP, Bucholz RW, Heckman JD (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 621-623.
Light TR (ed): Hand Surgery Update 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 19-28.
Question 19
An 86-year-old woman sustained a fracture of the humerus and underwent surgical fixation 8 weeks ago. There was no radial nerve function below the elbow after surgery. Radiographs are shown in Figures 51a and 51b. What is the most appropriate management at this time?
Explanation
REFERENCES: Shao YC, Harwood P, Grotz MR, et al: Radial nerve palsy associated with fractures of the shaft of the humerus: A systematic review. J Bone Joint Surg Br 2005;87:1647-1652.
Green DP: Radial nerve palsy, in Green DP, Hotchkiss RN, Pederson WC, et al (eds): Green’s Operative Hand Surgery, ed 5. Philadelphia, PA, Elsevier, 2005, p 112.
Question 20
Figure 1 shows a radiograph obtained from an active 30-year-old man who sustained an injury to his ring finger 1 week earlier. The most appropriate treatment is

Explanation

Figure 1 reveals evidence of an intra-articular distal phalanx fracture with a distal interphalangeal (DIP) joint dorsal subluxation. This injury is unstable and requires surgical management for an active individual. Volar distal phalanx fractures are often associated with flexor digitorum profundus avulsion injuries, which are addressed concomitantly. This injury was treated with ORIF of the intra-articular fracture, pinning of the DIP joint, and repair of an avulsed flexor digitorum profundus tendon with a button on the dorsal nail plate, as shown in Figure 2. Splint immobilization would not maintain a reduction of this unstable injury. The terminal tendon is not injured in this patient but is often injured in a dorsal distal phalanx fracture with a volar dislocation. Arthrodesis of the DIP is a salvage procedure and would not be considered acutely.
Question 21
The Coleman block test is used to test for Review Topic
Explanation
Question 22
What malignant disease most commonly develops in conjunction with chronic osteomyelitis?
Explanation
REFERENCES: Dell PC: Hand, in Simon MA, Springfield D (eds): Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, pp 405-420.
McGrory JE, Pritchard DJ, Unni KK, Ilstrup D, Rowland CM: Malignant lesion arising in chronic osteomyelitis. Clin Orthop 1998;362:181-189.
Question 23
-Figures 55a and 55b are the radiograph and CT scan of a 61-year-old woman who has had neck pain after being involved in a high-speed motor vehicle collision. Examination reveals normal strength and sensation in both upper and lower extremities, normal rectal tone, and no other injuries. The C1-C2 lateral mass overhang measures 8.5 mm. What is the most appropriate treatment option?
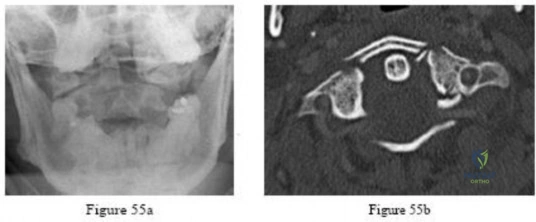
Explanation

Question 24
Figure 1 is the axial cut MRI scan of a 35-year-old woman who has had posteriorly based right hip pain for 3 months. Examination demonstrates full and symmetric range of motion between the right and left hips, negative impingement test, but reproduction of her pain with passive extension of the right hip. Which muscle is indicated by the arrow?

Explanation

Question 25
What is the most appropriate treatment for a 50-year-old woman who sustains the injury shown in Figures 14a and 14b?
Explanation
REFERENCES: Schemitsch EH, Tencer AF, Henley MB: Biomechanical evaluation of methods of internal fixation of the distal humerus. J Orthop Trauma 1994;8:468-475.
McCarty LP, Ring D, Jupiter JB: Management of distal humerus fractures. Am J Orthop 2005;34:430-438.
Kamineni S, Morrey BF: Distal humeral fractures treated with noncustom total elbow replacement: Surgical technique. J Bone Joint Surg Am 2005;87:41-50.
Question 26
A 10-day-old girl has decreased active motion of the left upper extremity. The mother reports a difficult vaginal delivery with presumed shoulder dystocia. Examination shows full passive range of motion of the shoulder, elbow, and wrist but only active flexion of the fingers and wrist. Factors predictive of a good outcome include which of the following?
Explanation
Question 27
- Which of the following advantages does the use of a vascularized fibula graft have over a nonvascularized fibula graft?
Explanation
And a vascularized graft requires greater technical skills and a larger dissection to isolate the vascular pedicle with associated increased donor site morbidity.
Question 28
Figure 21 shows the radiograph of a 32-year-old patient with right hip pain that has failed to respond to nonsurgical management. What is the most appropriate surgical treatment at this time?
Explanation
REFERENCES: Ganz R, Klaue K, Vinh TS, et al: A new periacetabular osteotomy for the treatment of hip dysplasias: Technique and preliminary results. Clin Orthop 1988;232:26-36.
Trousdale RT, Ekkernkamp A, Ganz R, et al: Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am 1995;77:73-85.
Question 29
A 29-year-old quarterback falls onto his dominant shoulder and sustains the injury shown in Figures 14a and 14b. Management should consist of
Explanation
REFERENCES: Lemos MJ: The evaluation and treatment of the injured acromioclavicular joint in athletes. Am J Sports Med 1998;26:137-144.
Rockwood CA Jr, Green DP, Bucholz RW, et al: Fractures in Adults, ed 5. Philadelphia, PA, Lippincott-Raven, 2001, pp 1209-1240.
Question 30
A 19-year-old male collegiate rower has a 3-month history of right shoulder pain. There was no inciting trauma prior to the onset of his pain. He also complains of weakness, particularly in abduction and overhead activity. Examination reveals no range-of-motion deficits. Strength testing of the right shoulder demonstrates 4/5 motor strength in forward elevation and abduction. His Beighton hypermobility score is 3/9. Figure 1 shows his scapular position during a wall pushup maneuver. An EMG would likely reveal damage to what nerve?

Explanation
Question 31
What is the most important factor in determining recovery after surgical repair of a complete laceration of a nerve at the wrist?
Explanation
REFERENCES: Sunderland S: Nerve Injuries and Their Repair: A Critical Appraisal. New York, NY, Churchill Livingstone, 1991.
Wilgis ES, Brushart TM: Nerve repair and grafting, in Green DP, Hotchkiss RN (eds): Operative Hand Surgery, ed 3. New York, NY, Churchill Livingstone, 1993, p 1325.
Narakas A: The use of fibrin glue in repair of peripheral nerves. Orthop Clin North Am 1988;19:187-199.
Weber RA, Breidenbach WC, Brown RE, et al: A randomized prospective study of
polyglycolic acid conduits for digital nerve reconstruction in humans. Plast Reconstr Surg 2000;106:1036-1045.
Question 32
A collegiate golfer sustains a hook of the hamate fracture. After 12 weeks of splinting and therapy, the hand is still symptomatic. What is the most appropriate management to allow return to competitive activity?
Explanation
REFERENCES: Kulund DN, McCue FC III, Rockwell DA, et al: Tennis injuries: Prevention and treatment: A review. Am J Sports Med 1979;7:249-253.
Morgan WJ, Slowman LS: Acute hand and wrist injuries in athletes: Evaluation and management. J Am Acad Orthop Surg 2001;9:389-400.
Question 33
The most common neurologic injury following an anterior cervical diskectomy and fusion (ACDF) is injury to which of the following structures? Review Topic
Explanation
Question 34
A 59-year-old active woman undergoes elective total hip replacement in which a posterior approach is used. She has minimal pain and is discharged to home 2 days after surgery. Four weeks later, she dislocates her hip while shaving her legs. She undergoes a closed reduction in the emergency department. Postreduction radiographs show a reduced hip with well-fixed components in satisfactory alignment. What is the most appropriate management of this condition from this point forward?
Explanation
First-time early dislocations are often treated successfully without revision surgery, especially when no component malalignment is present. In this clinical scenario, it appears the patient would benefit from better education about dislocation precautions. Hip orthoses are of questionable benefit unless the patient is cognitively impaired. Revision surgery can be successful but is usually reserved for patients with recurrent dislocations.
Question 35
An 18-year-old football player is injured after making a tackle with his left shoulder. He has decreased sensation over the lateral aspect of the left shoulder and radial aspect of the forearm. Motor examination reveals weakness to shoulder abduction and external rotation as well as elbow flexion. He has decreased reflexes of the biceps tendon on the left side but full, nontender range of motion of the cervical spine. What anatomic site has been injured?
Explanation
REFERENCES: Schenck CD: Anatomy of the innervation of the upper extremity, in Torg JS (ed): Athletic Injuries to the Head, Neck, and Face, ed 2. St Louis, MO, Mosby-Year Book, 1991.
Hershman EB: Brachial plexus injuries. Clin Sports Med 1990;9:311-329.
Question 36
In the spine, osteoblastomas usually originate in the
Explanation
REFERENCE: Frassica FJ, Waltrip RL, Sponseller PD, Ma LD, McCarthy EF Jr: Clinicopathologic features and treatment of osteoid osteoma and osteoblastoma in children and adolescents. Orthop Clin North Am 1996;27:559-574.
Question 37
A 27-year-old woman reports the acute atraumatic onset of burning pain in her right shoulder followed a week later by significant weakness and the inability to abduct her shoulder. One week prior to this incident she had recovered from a flu-like syndrome. Examination reveals full passive motion of the shoulder and the inability to actively raise the arm. Sensation in the right upper extremity is normal. Cervical spine examination is normal. Radiographs of the shoulder and cervical spine are normal. What is the most likely diagnosis?
Explanation
REFERENCES: Turner JW, Parsonage MJ: Neuralgic amyotrophy (paralytic brachial neuritis). Lancet 1957;2:209-212.
Omer GE, Spinner M, Van Beek AL (eds): Management of Peripheral Nerve Problems, ed 2. Philadelphia, PA, WB Saunders, 1998, pp 101-104.
Question 38
An acute posterolateral disk herniation at the L4-5 level will most likely affect what nerve root? Review Topic
Explanation
Question 39
Which of the following is considered the most appropriate shoe modification following transmetatarsal amputation?
Explanation
REFERENCES: Philbin TM, Leyes M, Sferra JJ, Donley BG: Orthotic and prosthetic devices in partial foot amputations. Foot Ankle Clin 2001;6:215-228.
Marks RM: Mid-foot/mid-tarsus amputations. Foot Ankle Clin 1999;4:1-16.
Question 40
A 20-year-old man sustains the injury shown in Figures 1a and 1b in a motorcycle accident. In addition to a prompt closed reduction, his outcome might be optimized by
Explanation
REFERENCE: Saltzman C, Marsh JL: Hindfoot dislocations: When are they not benign? J Am Acad Orthop Surg 1997;5:192-198.
Question 41
A study is designed that examines fractures in children with osteogenesis imperfecta after being treated with bisphosphonates compared with a placebo. A difference is found for which the P value is greater than what is considered to be statistically significant. What is the next appropriate statistical analysis?
Explanation
REFERENCES: Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 7.
Kocher MS, Zurakowski D: Clinical epidemiology and biostatistics: A primer for orthopaedic surgeons. J Bone Joint Surg Am 2004;86:607-620.
Question 42
A 21-year-old pitcher reports shoulder pain with hard throwing. He notes that the pain occurs in the early acceleration phase of his throw. Given his history, what structures are at greatest risk for injury?
Explanation
REFERENCES: Paley KJ, Jobe FW, Pink MM, et al: Arthroscopic findings in the overhand throwing athlete: Evidence for posterior internal impingement of the rotator cuff. Arthroscopy 2000;16:35-40.
Jazrawi LM, McCluskey GM III, Andrews JR: Superior labral anterior and posterior lesions and internal impingement in the overhead athlete. Instr Course Lect 2003;52:43-63.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posterosuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg
1992;1:238-245.
Question 43
Figure 43 shows an arthroscopic view of a right shoulder through a lateral portal in the beach chair position. The arrow is pointing to what structure?
Explanation
REFERENCES: Mazzocca AD, Noerdlinger M, Cole B, et al: Arthroscopy of the shoulder: Indications and general principles of techniques, in McGinty JB (ed): Operative Arthroscopy,
ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 412-427.
Burkhart, SS: Arthroscopic management of rotator cuff tears, in McGinty JB (ed): Operative Arthroscopy, ed 3. Philadelphia, PA, Lippincott Williams & Wilkins, 2003, pp 508-546.
Question 44
A 29-year-old female has sustained the acute injury shown in Figure A. Which of the following is an indication for open reduction internal fixation in this patient?

Explanation
In patients who present with no medial widening on standard ankle radiographs and no clinical symptoms of deltoid ligament injury, the integrity of the deltoid ligament remains unknown. The gravity stress radiograph may be used to help identify a deltoid ligament injury in association with an isolated distal fibular fracture. Stage-IV supination-external rotation fractures, which involve the deltoid ligament, are more likely to be treated operatively as they are often considered unstable ankle fractures.
Egol et al. reviewed 101 patients with isolated fibular fracture and an intact mortise. They found that medial tenderness, swelling, and ecchymosis were not sensitive with regard to predicting widening of the medial clear space on stress radiographs. Interestingly, they report that good functional results can be obtained in patients with widening of the medial clear space on a stress radiograph in the absence of medial signs.
Gill et al. compared the effectiveness of gravity stress radiograph as compared to manual stress radiograph for the detection of deltoid ligament injury in isolated fibular fracture. A total of twenty-five patients with SER type-II fracture and SER Type IV-equivalent fractures were enrolled. They found the gravity stress radiograph was equivalent to the manual stress radiograph for determining deltoid ligament injury.
Figure A shows a mortise radiograph displaying a minimally displaced Weber B ankle fracture. Illustration A shows the positioning for a gravity stress radiograph. The patient is in the lateral decubitus position with the injured leg dependent and off the end of the table, a mortise view is taken in 10° of internal rotation of the tibia.
Incorrect Answers:
Question 45
In patients without spondylolisthesis or scoliosis undergoing laminectomy for lumbar spinal stenosis, spinal fusion is generally recommended if
Explanation
REFERENCES: Spivak JM, Connolly PJ (eds): Orthopaedic Knowledge Update: Spine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2006, pp 299-409.
Fischgrund JS, Mackay M, Herkowitz HN, et al: 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 1997;22:2807-2812.
Question 46
A year-old man is about to undergo right total hip arthroplasty. A preoperative AP pelvis radiograph is shown in below. The final acetabular component and polyethylene liner are implanted. With the broach in place, the surgeon trials a standard offset neck and neutral length femoral head. The leg lengths are approximately equal, but the hip is unstable. What is the best next step?
Explanation
The radiograph shows that this patient has a high offset varus femoral morphology of both hips. Preoperative templating would identify this, and the surgeon should choose an implant system that has extended offset options to help match the native anatomy and biomechanics and minimize the risk of instability. Trialing a high offset neck, rather than a standard offset neck, is the next most appropriate step. Depending on the design of the implant system, this step can be accomplished by direct medialization of the femoral head, which would not affect leg length, or by lowering the neck angle, which would affect the leg length and would require a longer femoral head, because the leg lengths had previously been equal. Placement of a longer femoral head would likely improve hip stability but would also make the leg length uneven, which is a common cause of dissatisfaction after total hip arthroplasty. An offset acetabular liner also increases the leg length and does not correct the issue, which is on the femoral side. Trochanteric
advancement is sometimes used as a treatment for instability but would be inappropriate as the next step in this setting.
Question 47
A 46-year-old woman fell from her bicycle and sustained the injury shown in Figure 24. Which of the following ligaments has been disrupted? Review Topic

Explanation
Question 48
Figures 163a through 163c show the radiograph and MRI scans of a 45-year-old woman with severe right arm pain. She has had symptoms for 6 months without resolution despite multiple nonsurgical treatments. Examination reveals weakness in the right triceps and wrist flexors with decreased sensation in the middle finger and a positive Spurling's sign. What is the most appropriate treatment for the patient's symptoms? Review Topic

Explanation
Question 49
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?
Explanation
REFERENCE: Ayers DC, Dennis DA, Johanson NA, Pelligrini VD: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Question 50
A 16-year-old right-hand dominant male pitcher has had increasing pain in his dominant shoulder for the past 6 months without treatment. A coronal T2-weighted MRI scan is shown in Figure 80. What is the most appropriate treatment plan? Review Topic

Explanation
Question 51
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome? Review Topic

Explanation
Question 52
The patient returns 4 days after surgery and says he has noticed a red, swollen knee since yesterday. He reports a fever of 38.0°C since last evening and denies traumatic injury. He has an erythematous knee with a large, tense effusion; his range of motion is limited; and the surgical incisions are not draining. Radiographs taken in the office show no change from the immediate postsurgical images. Aspiration in the office returns 50 cc of cloudy, blood-tinged synovial fluid, and analysis of the fluid reveals a white blood cell count of 92000 (reference range 4500-11000 /µL). Which bacteria is most commonly responsible for this clinical scenario?
Explanation
This patient has a history of failed primary and revision ACL reconstructions, both times with medial meniscus repairs. The clinical scenario suggests a recurrent ACL injury with a recurrent medial meniscus tear that is now locked. The most critical risk factor for ACL reconstruction is age younger than 20 years. The meniscal repair success rate using an all-inside device is between 80% and 90%. Traditionally, it was believed that healing rates were
higher in ACL reconstruction, but current literature demonstrates a similar rate of healing associated with ACL reconstruction and no reconstruction of stable knees.
The images show a vertical femoral tunnel resulting from this patient’s prior reconstruction and revision. The MR images reveal a locked bucket-handle tear of the medial meniscus, and the examination shows a positive Lachman test finding attributable to ACL graft failure. In the setting of a young individual who has failed 2 meniscal repairs, a third repair is not indicated. In addition to a revision ACL reconstruction to stabilize the knee, a partial medial meniscectomy is indicated. An attempt at revision medial meniscus repair would be indicated if the technique were poor in the first attempt, but a failed repair otherwise should indicate the need for partial meniscectomy. The postsurgical images reveal a much more anatomic position of the femoral tunnel that should provide better rotational control of the knee, thereby improving the pivot shift (compared to the vertical femoral tunnel).
This patient has an obvious postsurgical infection based on the timing, examination, and results of the aspiration. In multiple studies of septic arthritis following ACL reconstruction, the most common pathogen was coagulase-negative staph (Staphylococcus epidermidis), followed by S. aureus. If S. aureus is the causative pathogen, the rate of necessary graft removal is higher because of the aggressive nature of this specific bacteria.
Question 53
A 47-year-old woman with no history of trauma has had a painful, stiff shoulder for the past 3 months. Treatment consisting of subacromial injection and nonsteroidal anti-inflammatory drugs has been ineffective. Her active range of motion is painful and is limited to 90 degrees of abduction, 60 degrees of elevation, 30 degrees of external rotation, and internal rotation to the posterior superior iliac spine. Plain radiographs of the cervical spine and shoulder are normal. Management at this time should consist of
Explanation
Question 54
Figures 43a and 43b show the clinical photographs of a 4-month-old child with bilateral popliteal pterygium. The fixed knee contractures measure 100 degrees bilaterally. What future treatment is most likely to successfully correct this deformity?
Explanation
40 degrees. Moderate contractures of up to 60 degrees usually require Z-plasties in the popliteal fossa and postoperative serial casting to avoid undue tension on neurovascular structures. Contractures of more than 60 degrees require a femoral shortening osteotomy or gradual correction with an external fixator. However, rapid recurrence following fixator removal is common if formal soft-tissue procedures and postoperative splinting are not performed.
REFERENCES: Parikh SN, Crawford AH, Do TT, et al: Popliteal pterygium syndrome: Implications for orthopaedic management. J Pediatr Orthop B 2004;13:197-201.
Brunner R, Hefti F, Tgetgel JD: Arthrogrypotic joint contracture at the knee and foot: Correction with a circular frame. J Pediatr Orthop B 1997;6:192-197.
Question 55
Figure 22 shows the radiographs of a 16-year-old boy who injured his elbow in a fall 1 year ago. Although he has no pain, he reports restricted forearm rotation and elbow flexion. What is the most likely diagnosis?
Explanation
REFERENCES: Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, p 196.
Bell SN, Morrey BF, Bianco AJ Jr: Chronic posterior subluxation and dislocation of the radial head. J Bone Joint Surg Am 1991;73:392-396.
Question 56
Figures 122a and 122b are the radiographs of a 79-year-old woman with a 2-year history of progressively worsening right hip pain. She had a right total hip arthroplasty 7 years prior. An infection workup is negative. She opts for revision surgery; the most appropriate surgical plan to address her femoral component is
Explanation
The patient’s radiographs show loosening of the cemented femoral stem and varus remodeling of the femur. An extended trochanteric osteotomy is necessary because attempting to extract the existing prosthesis and implant another prosthesis without an osteotomy is likely to cause a proximal femoral fracture. Also, an osteotomy would facilitate atraumatic removal of the stem and cement. Cementless fixation is likely to produce a more predictable long-term outcome than cemented fixation for the revision implant.
Question 57
Figures 6a through 6d show the radiographs and biopsy specimens of an 8-year-old girl with leg pain. Management of the lesion should consist of
Explanation
REFERENCES: Wilson AJ, Kyriakos M, Ackerman LV: Chondromyxoid fibroma: Radiographic appearance in 38 cases and in a review of the literature. Radiology 1991;179:513-518.
Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 167-189.
Question 58
Figure 35 shows the lateral radiograph of a 15-year-old basketball player who felt a dramatic pop in his knee when landing after a lay-up. The patient reports that he cannot bear weight on the injured extremity. Management should consist of
Explanation
REFERENCES: Ogden JA, Tross RB, Murphy MJ: Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am 1980;62:205-215.
Pape JM, Goulet JA, Hensinger RN: Compartment syndrome complicating tibial tubercle avulsion. Clin Orthop 1993;295:201-204.
Question 59
-Which gene correlates with severity of disease in spinal muscular atrophy (SMA)?
Explanation
The other choices are not associated with spinal muscular atrophy.Defects in PMP22 are the cause of 70% to 80% of cases of Charcot-Marie-Tooth disease. Mutations in the dystrophin gene cause Duchenne muscular dystrophy.
Question 60
Ulnar collateral ligament (UCL) reconstruction using a modified Jobe technique
Explanation
Certain complications are more strongly associated with the approach and surgical procedure for elbow pathology. With a 2-incision distal biceps repair, heterotopic ossification
with a radial-ulnar synostosis is a concern. This complication can be minimized through irrigation of bone debris and care to avoid dissection between the radius and ulna. With a single-incision distal biceps repair, the lateral antebrachial cutaneous nerve is retracted during the procedure. Numbness on the lateral side of the forearm is common, although often temporary. During arthroscopic debridement for lateral epicondylitis, injury to the radial UCL can occur, leading to posterolateral rotatory instability of the elbow. The modified Jobe technique for UCL reconstruction typically involves an ulnar nerve transposition during the procedure. Numbness and tingling in the fourth and fifth digits are concerns when this procedure is performed.
Question 61
A year-old patient fell 3 weeks after undergoing a total hip arthroplasty using cementless fixation of the femoral component. She sustained a comminuted Vancouver type B-2 fracture with displacement of the calcar fragment. What is the best treatment option?
Explanation
The patient has an acute postoperative fracture of the proximal femur with subsidence. It is also common that the stem retroverts relative to the femur. It is most often seen in proximally porous coated stems within 90 days of surgery, one paper found it to occur 0.7% of the time in modern implants. There is always a debate whether this is a missed intraoperative fracture, or a new fracture that has resulted from an event of increased hoop stresses. Removal of the primary stem, placement of a diaphyseal engaging
stem (most frequently a tapered-fluted stem), and cabling of the fracture is the most successful treatment.
Question 62
What is the most appropriate next step in the work-up of a patient with the asymptomatic lesion shown in Figure 23?
Explanation
REFERENCES: Marks KE, Bauer TW: Fibrous tumors of bone. Orthop Clin North Am 1989;20:377-393.
Bullough PG, Walley J: Fibrous cortical defect and non-ossifying fibroma. Postgrad Med J 1965;41:672-676.
Skrede O: Non-osteogenic fibroma of bone. Acta Orthop Scand 1970;41:362-380.
Question 63
Figure 92 is the radiograph of a 45-year-old man who was thrown from his horse and now reports groin pain. Which of the following is the most common long-term sequelae of this injury?

Explanation
Question 64
Which of the following statements is most accurate regarding undetected intraoperative surgical glove perforation?
Explanation
REFERENCES: Al-Habdan I, Sadat-Ali M: Glove perforation in pediatric orthopaedic practice. J Pediatr Orthop 2003;23:791-793.
Sadat-Ali M, Al-Othman A: Glove perforations in orthopaedic practice. Saudi Med J 1996;17:811-813.
Question 65
Among patients with adolescent idiopathic scoliosis, a thoracolumbosacral orthosis is most effective for which type of curve?
Explanation
A thoracolumbosacral orthosis is most effective for bracing of curves when the apex is at T7 or below. Bracing is used for patients who are skeletally immature (Risser stage 0, 1, or 2), and it is recommended that the brace be worn 16 to 23 hours per day and continued until skeletal maturity or until the curve progresses to beyond 45 degrees, at which point bracing is no longer considered effective.
RECOMMENDED READINGS
Luhmann SJ, Skaggs DL: Pediatric spine conditions, in Lieberman JR (ed): AAOS Comprehensive Orthopaedic Review. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2009, pp 245-265.
Shaughnessy WJ. Advances in scoliosis brace treatment for adolescent idiopathic scoliosis. Orthop Clin North Am. 2007 Oct;38(4):469-75, v. Review. PubMed PMID: 17945126. View Abstract at PubMed
Question 66
A 21-year-old woman is struck by a car and sustains a Gustillo IIIB fracture of the tibia. The wound was debrided and immobilized with an external fixator. Radiographs are shown in Figure A. The soft tissue defect was covered with a free flap. Her recovery was complicated by wound infection with Klebsiella pneumoniae and Escherichia coli. One month after her injury, she underwent intramedullary nailing and placement of an antibiotic spacer measuring 15cm in length. Radiographs are shown in Figure B. At the next stage of surgery 6 weeks later, the surgeon should plan to do all of the following:

Explanation
The Masquelet staged technique of induced membranes is an option for filling large bone defects up to 25cm in length. This technique protects against autograft resorption, stimulates mesenchymal cell-to-osteoblast differentiation, maintains graft position, and prevents soft tissue interposition. Cement impregnation achieves high local antibiotic concentration without risk of systemic toxicity.
Ashman et al. discussed the techniques of addressing bone defects. Options include:
(1) acute limb shortening (up to 4cm in the tibia and humerus, and 7cm in the femur);
(2) distraction osteogenesis for defects up to 10cm long (at 1mm/day with consolidation period of 5days per mm, or total treatment time of up to 60days/cm), (3) autograft (up to 25cm of vascularized fibula, or 3cm of nonvascularized iliac crest),
and (4) Masquelet technique.
Taylor et al. reviewed the induced membranes technique. They found that the membrane is well vascularized and composed of type I collagen with fibroblasts with an inner epithelial cell layer. There is a high concentration of VEGF, RUNX2 (CBFA1), TGFß1, and BMP2. The membrane is sutured over bone graft to create a closed pouch. When a nail is present, they note a second internal membrane around the nail, potentially increasing local vascularity and osteoinductive factor concentration.
Figure A shows a Gustillo IIIB tibia fracture with a large bone defect held in a temporizing external fixator. Figure B shows the same defect following intramedullary nailing and with a cement spacer placed circumferentially around the nail in the defect.
Incorrect Answers
Question 67
Figure A shows immediate post-operative radiographs of a 75-year-old patient with primary osteoarthritis. She presents 3 years later with increasing pain and weakness in the shoulder despite home physical therapy. Examination reveals limited active range of motion, with forward elevation of 80 degrees and external rotation of 50 degrees. Her deltoid function is intact. Repeat radiographs are seen in Figure B.

Explanation
RTSA is considered a viable treatment option for patients with failed shoulder arthroplasty. It allows for improved arm elevation and abduction in the setting of nonfunctional rotator cuff muscles, as seen in this example. Despite the expanding indications for rTSA, there are high complication rates in the revision setting. Complication rates for rTSA after failed shoulder arthroplasty have been reported to be between 11-36%. This procedure should, therefore, be performed by surgeons with extensive training in reconstructive shoulder arthroplasty.
Patel et al. retrospectively reviewed 31 patients (mean age, 68.7 years) who underwent rTSA for treatment of a failed shoulder arthroplasty. They found the greatest improvement with active forward elevation from 44° preoperatively to 108° postoperatively (P < .001). Complications occurred in 3 patients with periprosthetic fracture.
Hattrup et al. reviewed a series of 19 patients that underwent open rotator cuff repair after shoulder arthroplasty. Out of the 19 patients only 4 shoulders were successfully repaired. They concluded that successful rotator cuff repair after shoulder arthroplasty is possible but failure is more common.
Figure A shows a left total shoulder arthroplasty that is well reduced in the glenoid. Figure B shows antero-superior escape of the prosthesis, indicative of a massive rotator cuff tear.
Incorrect Answers:
Question 68
A 55-year-old woman with polyarticular rheumatoid arthritis has had progressively increasing left shoulder pain for the past 2 years despite nonsurgical management. No focal weakness is noted during examination of the shoulder. AP and axillary radiographs are shown in Figures 47a and 47b. Treatment should consist of
Explanation
REFERENCES: Boyd AD Jr, Thomas WH, Scott RD, Sledge CB, Thornhill TS: Total shoulder arthroplasty versus hemiarthroplasty: Indications for glenoid resurfacing. J Arthroplasty 1990;5:329-336.
Kelly IG, Foster RS, Fisher WD: Neer total shoulder replacement in rheumatoid arthritis. J Bone Joint Surg Br 1987;69:723-726.
Question 69
Figure 10 is an anteroposterior pelvis radiograph of an 82-year-old man who had right hip pain that began 2 weeks ago but has since resolved with use of over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs). Currently he has no pain. Examination of his hip shows decreased internal rotation and minimal pain at the extremes of motion. What is the most appropriate treatment at this point?

Explanation
The radiograph shown is consistent with Paget disease of the bone. It demonstrates classic findings of widened lamellae and disorganized sclerotic and lytic areas. The cause is not clearly defined, but may be linked to a viral infection and subsequent alterations of osteoblastic and osteoclastic activity. Most patients are asymptomatic, and Paget disease is often found incidentally on radiographs. In this case, the patient’s symptoms likely were caused by hip arthritis, but Paget disease can cause diffuse bone pain in some cases. Considering the patient’s mild and short-term symptoms, observation and NSAID use is most appropriate. An MRI scan or biopsy is indicated if sarcomatous transformation is suspected, but this condition is rare and is associated with a substantial, unrelenting increase in pain. SPEP and UPEP are tests for multiple myeloma, of which the radiographs show no signs.
RECOMMENDED READINGS
Ralston SH. Pathogenesis of Paget's disease of bone. Bone. 2008 Nov;43(5):819-25. doi: 10.1016/j.bone.2008.06.015. Epub 2008 Jul 11. Review. PubMed PMID: 18672105.View Abstract at PubMed
Bonenberger E, Einhorn T. Metabolic bone diseases. In: Callaghan JJ, Rosenberg
AG, Rubash HE, eds. The Adult Hip. 2nd ed. Philadelphia, PA: Lippincott Williams 14
& Wilkins; 2007:514-533.
Question 70
Based on the Young and Burgess classification of pelvic ring injuries, an anterior-posterior compression type II injury does not result in disruption of which of the following?

Explanation
well as sacrotuberous and sacrospinous ligaments. An APC III also involves disrupted posterior SI ligaments, causing complete SI joint disruption with potential translational and rotational displacement.
The reference by Young et al is a classic article that describes the Young and Burgess classification of pelvic ring injuries. They retrospectively analyzed pelvic ring radiographs and discussed four patterns of injury: anteroposterior compression, lateral compression, vertical shear, and a complex/combined pattern.
The reference by Burgess et al is a validation of the aforementioned classification and study, as they reviewed 210 consecutive patients who sustained a pelvic ring injury. They validated the classification scheme and found that overall blood replacement averaged: lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units. Overall mortality was: lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear, 0%; combined mechanical, 18.0%.
Incorrect answers:
1,2,4,5: An APC - 2 pelvic ring injury involves injury to all of these structures.
Question 71
All of the following conditions are associated with the female athlete triad EXCEPT? Review Topic
Explanation
The female athlete triad is an interrelationship of menstrual dysfunction (i.e., amenorrhea or oligomenorrhea), low energy availability (insufficient caloric intake for demand, with or without an eating disorder) and decreased bone mineral density. It is relatively common among young women participating in sports. More recently, it has been suggested that endothelial dysfunction also results, due to an imbalance between vasodilating and vasoconstricting agents triggered from inappropirate levels of nitric oxide on the microscopic level, which predisposes these women to atherosclerotic changes and increases their risk of cardiovascular disease in the future.
Matheson et al. analyzed cases of 320 athletes with bone scan-positive stress fractures (M = 145, F = 175) seen over 3.5 years and assessed the results of conservative management. They found that conservative treatment of stress fractures in athletes is satisfactory in the majority of cases.
Constantini et al. evaluated the prevalence of vitamin D insufficiency and deficiency among young athletes and dancers. They found a higher rate of vitamin D insufficiency among participants who practice indoors, during the winter months, and in the presence of iron depletion.
Nazem et al. reviewed the major components and health consequences of the female athlete triad as well as strategies for diagnosis and treatment of the conditions. They concluded that treatment requires a multidisciplinary approach involving health care professionals as well as coaches and family members.
Yagi et al. followed 230 runners participating in high school running teams for a total of 3 years to report occurrence of medial tibial stress syndrome (MTSS) and stress fracture. Predictors of MTSS and stress fracture were investigated. The authors reported a significant relationship between BMI, internal hip rotation angle and MTSS infemales.
Incorrect Answers:
Question 72
A 64-year-old man who underwent total shoulder arthroplasty 4 weeks ago is making satisfactory progress in physical therapy, but his therapist notes limitations in external rotation to neutral. A stretching program is started, and the patient suddenly gains 90 degrees of external rotation but now reports increased pain and weakness. What is the best course of action?
Explanation
REFERENCES: Wirth MA, Rockwood CA Jr: Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am 1996;78:603-616.
Miuer SL, Hazrati Y, Klepps S, et al: Loss of subscapularis function after shoulder replacement: A seldom recognized problem. J Shoulder Elbow Surg 2003;12:29-34.
Question 73
A 59-year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Figure 1. Postreduction CT is shown in Figures 2 through 4. What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
Question 74
Examination of an obese 3-year-old girl reveals 30 degrees of unilateral genu varum. A radiograph of the involved leg with the patella forward is shown in Figure 10. Management should consist of
Explanation
REFERENCES: Johnston CE II: Infantile tibia vara. Clin Orthop 1990;255:13-23.
Richards BS, Katz DE, Sims JB: Effectiveness of brace treatment in early infantile Blount’s disease. J Pediatr Orthop 1998;18:374-380.
Question 75
A 24-year-old man has right forearm pain after sliding head first into home plate. Examination reveals that the arm is swollen, but there are no neurovascular deficits or skin lacerations. Radiographs reveal a both-bone forearm fracture. The ulna has an oblique fracture with a 30% butterfly fragment, and the radius is comminuted over 75% of its circumference. In addition to reduction and plate fixation of both bones, management should consist of
Explanation
REFERENCES: Anderson LD, Sisk TD, Tooms RE, Park WI III: Compression-plate fixation in acute diaphyseal fractures of the radius and ulna. J Bone Joint Surg Am 1975;57:287-297.
Chapman MW, Gordon JE, Zissimos AG: Compression-plate fixation of acute fractures of the diaphyses of the radius and ulna. J Bone Joint Surg Am 1989;71:159-169.
Wright RR, Schmeling GJ, Schwab JP: The necessity of acute bone grafting in diaphyseal forearm fractures: A retrospective review. J Orthop Trauma 1997;11:288-294.
Wei SY, Born CT, Abene A, Ong A, Hayda R, Delong WG Jr: Diaphyseal forearm fractures treated with and without bone graft. J Trauma 1999;46:1045-1048.
Question 76
...Figure 74 is the radiograph of an 11-year-old boy with pain in his left arm. Prognosis is most influenced by
Explanation

Question 77
A 66-year-old woman who previously underwent hemiarthroplasty 2 years ago for a fracture continues to have severe pain and loss of motion despite undergoing physical therapy. A radiograph is shown in Figure 2. What is the most likely reason that this patient has failed to improve her motion?
Explanation
REFERENCES: Bigliani LU, Flatow EL, McCluskey G, et al: Failed prosthetic replacement for displaced proximal humeral fractures. Orthop Trans 1991;15:747-748.
Boileau P, Krishnan SG, Tinsi L, et al: Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002;11:401-412.
Tanner MW, Cofield RH: Prosthetic arthroplasty for fractures and fracture-dislocations of the proximal humerus. Clin Orthop Relat Res 1983;179:116-128.
Question 78
A 26-year-old ballet dancer reports posterolateral ankle pain, especially with maximal plantar flexion. Examination reveals maximal tenderness just posterior to the lateral malleolus, and symptoms are heightened with forced passive plantar flexion. Radiographs are shown in Figures 42a and 42b. What is the most likely cause of the patient’s symptoms?
Explanation
REFERENCES: Marotta JJ, Micheli LJ: Os trigonum impingement in dancers. Am J Sports Med 1992;20:533-536.
Hamilton WG: Foot and ankle injuries in dancers, in Mann RA, Coughlin MJ (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, CV Mosby, 1993, pp 1241-1276.
Question 79
Figure 25 shows the clinical photograph of a 48-year-old man who has had a forefoot ulcer for the past 4 months. History reveals that he has had type II diabetes mellitus for the past 10 years. Examination reveals sensory and motor neuropathy, with weak ankle dorsiflexion. The ankle cannot be passively dorsiflexed past a neutral position. Initial management should consist of
Explanation
REFERENCES: Lin SS, Lee TH, Wapner KL: Plantar forefoot ulceration with equinus deformity of the ankle in diabetic patients: The effect of tendo-Achilles lengthening and total contact casting. Orthopedics 1996;19:465-475.
Armstrong DG, Stacpoole-Shea S, Nguyen H, Harkless LB: Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot. J Bone Joint Surg Am 1999;81:535-538.
Question 80
A 36-year-old woman was injured in a train derailment. She has a significant open depressed skull fracture with active bleeding, a hemopneumothorax, and blood in the left upper quadrant and colic gutter by Focused Assessment with Sonography for Trauma (FAST) examination. Additionally, she has the pelvic injury seen on the CT scans in Figures 18a and 18b. The mortality rate for this patient approaches
Explanation
REFERENCES: Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: Classification by mechanism is key to pattern of organ injury, resuscitative requirements and outcome. J Trauma 1989;29:981-1000.
Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center. J Trauma 1997;42:695-700.
Gilliland MD, Ward RE, Barton RM, et al: Factors affecting mortality in pelvic fractures.
J Trauma 1982;22:691-693.
Question 81
A 24-year-old man was thrown from a car and is seen in the emergency department with a Glasgow Coma Scale (GCS) score of 8. A CT scan of the head shows no significant bleeding. The patient is hemodynamically stable. The left femur has the closed injury shown on the radiographs in Figures 53a and 53b. What is the best treatment for this patient?
Explanation
REFERENCES: Starr AJ, Hunt JL, Chason DP, et al: Treatment of femur fracture with associated head injury. J Orthop Trauma 1998;12:38-45.
Nau T, Kutscha-Lissberg F, Muellner T, et al: Effects of a femoral shaft fracture on multiply injured patients with a head injury. World J Surg 2003;27:365-369.
McKee MD, Schemitsch EH, Vincent LO, et al: The effect of a femoral fracture on concomitant closed head injury in patients with multiple injuries. J Trauma 1997;42:1041-1045.
Brundage SI, McGhan R, Jurkovich GJ, et al: Timing of femur fracture fixation: Effect on outcome in patients with thoracic and head injuries. J Trauma 2002;52:299-307.
Question 82
The newborn foot deformity seen in Figures 64a and 64b should initially treated with
Explanation
REFERENCES: Abel MF (ed): Orthopaedic Knowledge Update: Pediatrics 3. Rosemont, IL, American AcademAyL-oMfadOenrathCooppayedic Surgeons, 2006, pp 240-241.
Farsetti P, Weinstein SL, Ponseti IV: The Long-term functional and radiographic outcomes of untreated
and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265. Question 65
A 4-year-old girl has been limping for the past 2 months. There is no history of trauma, previous injury, fever, or other systemic complaints. Examination reveals a moderate right knee effusio n with a 10-degree knee flexion contracture. What is the next most appropriate step in evaluation?
Arthroscopy
Antinuclear antibody
MRI
Bone scan
HLA-B27
DISCUSSION: The patient presents with juvenile idiopathic arthritis manifestations. The American College of Rheumatology defines this as one or more joints involved with swelling of 6 weeks or longer. A positive antinuclear antibody test would be diagnostic. Consideration should be made to have the patient see an ophthalmologist for evaluation of possible uveitis. Although the patient could have Lyme disease, that choice is not an option. The presence of an elevated antinuclear antibody by itself should not necessarily be used for diagnosing arthritis; however, the test does have clinical utility as a screening test. The frequency of a positive antinuclear antibody test is greatest in younger girls with oligoarticular disease and carries an increased risk for anterior uveitis. Arthroscopy might be indicated if this patient was presenting with a discoid meniscus, but there is no history of clicking, which is often one of the classic signs of discoid meniscus. MRI would not be used to diagnose juvenile idiopathic arthritis, but
MRI would be useful to help diagnose discoid meniscus. A bone scan would show increased uptake in the patient’s knee but again, this would not help diagnose her condition. HLA-B27 has no role in diagnosing juvenile idiopathic arthritis, especially in females.
REFERENCES: Iesaka K, Kubiak EN, Bong LR, et al: Orthopaedic surgical management of hip and knee involvement in patients with juvenile rheumatoid arthritis. Am J Orthop 2006;35:67-73.
Wright DA: Juvenile idiopathic arthritis, in Morrissey RT, Weinstein SL (eds): Love l and Winter’s Pediatric Orthopaedics, ed 6. Philadelphia PA, Lippincott Williams and Wilkins, 2006, pp 405-438. Question 66
An 18-month-old girl is brought in by her parents because of concerns about intoeing, bowlegs, and tripping and fa ling. Prenatal and birth history are otherwise unremarkable. The child’s growth and
development appear to be normal and she has a normal neurologic exam, a straight spine with no defects, and the hips are stable. Examination reveals hip internal rotation of 40 degrees and hip external rotation of 60 degrees. The thigh-foot angle is internal 30 degrees. Feet are straight and supple. Gait is characterized by intoeing with occasional tripping and falling. Based on these findings, what is the most appropriate action?
No treatment because internal tibial torsion slowly resolves on its own
Immediate treatment with a Denis-Browne bar
Distal tibial osteotomies
Proximal femoral derotational osteotomies
Treatment with twister cables PREFERRED RESPONSE: 1
DISCUSSION: The child has classic internal tibial torsion that is very commonly seen in younger children who are just beginning to walk. The normal outcome is for slow resolution of this problem and it seldom requires any treatment. Treatment with a Denis-Browne bar or with twister cables has not been proven to be effective. Surgical treatment at this point is premature and clearly not indicated.
REFERENCES: Lincoln TL, Suen PW: Common rotational variations in children. J Am Acad Orthop Surg 2003;11:312-320.
Staheli LT, Corbett M, Wyss C, et al: Lower-extremity rotational problems in children: Normal values to guide management. J Bone Joint Surg Am 1985;67:39-47.

Question 83
A 22-year-old professional baseball catcher has posterior shoulder pain and severe external rotation weakness with the arm in adduction. Radiographs are normal. MRI scans are shown in Figures 15a through 15c. Management should consist of
Explanation
REFERENCES: Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment.
J Bone Joint Surg Am 2000;82:415-424.
Martin SD, Warren RF, Martin TL, et al: Suprascapular neuropathy: Results of non-operative treatment. J Bone Joint Surg Am 1997;79:1159-1165.
Question 84
A 75-year-old man presents with a displaced femoral neck fracture. During your surgical exposure for a hemiarthroplasty, the femoral neck has fractured through a pathologic lesion which is diagnosed as a lymphoma on frozen section. The lesion is located in the center of the femoral neck and the calcar femorale is not involved. Your treatment should include:
Explanation
The clinical and radiographic features specific to lymphoma of bone are outlined by Dürr but on the whole are not diagnostic.
Vose describes the current treatment protocols for patients with non-Hodgkin's lymphoma including patients with impending/sustained pathologic fractures.
Question 85
A 47-year-old man has acute right shoulder pain after falling off a ladder. The MRI scan shown in Figure 9 reveals
Explanation
REFERENCES: Herzog RJ: Magnetic resonance imaging of the shoulder. Instr Course Lect 1998;47:3-20.
Iannotti JP, Zlatkin MB, Esterhai JL, et al: Magnetic resonance imaging of the shoulder: Sensitivity, specificity, and predictive value. J Bone Joint Surg Am 1991;73:17-29.
Question 86
A 46-year-old man reports occasional squeaking of his hip 2 years after undergoing an uneventful total hip arthroplasty. History reveals no pain, physical examination cannot reproduce audible squeaking, and radiographs show appropriate implant position. What is the most appropriate management?
Explanation
Hopefully, with a better understanding of acoustic phenomena following ceramic total hip arthroplasty, this complication can be minimized.
REFERENCES: Yang CC, Kim RH, Dennis DA: The squeaking hip: A cause for concem-disagrees. Orthopedics
2007;30:739-742.
Walter WL, O’Toole GC, Walter WK, et al: Squeaking in ceramic-on-ceramic hips: The importance of acetabular component orientation. J Arthroplasty 2007;22:496-503.

Figure 80a Figure 80b
Question 87
Within the menisci, the majority of the large collagen fiber bundles are oriented in what configuration?
Explanation
REFERENCES: Mow VC, et al: Structure and function relationships of the menisci of the knee, in Mow VC, Arnoczky SP, Jackson DW (eds): Knee Meniscus: Basic and Clinical Foundations. New York, NY, Raven Press, 1992, pp 37-57.
DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Question 88
Which of the following is considered the appropriate initial management protocol for an unconscious football player without spontaneous respirations?
Explanation
REFERENCES: McSwain NE, Garnelli RL: Helmet removal from injured patients. Bull Am Coll Surg 1997;82:42-44.
Vegso JJ, Lehman RC: Field evaluation and management of head and neck injuries. Clin Sports Med 1987;6:1-15.
Arndt EA (ed): Orthopaedic Knowledge Update: Sports Medicine 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 93-101.
Question 89
- A patient undergoes an acute repair of a laceration of the median nerve in the antecubital fossa. A lack of functional recovery 6 months later is most likely due to
Explanation
Functional recovery is generally complete after a crush injury because the basement membrane and endoneurium are left intact, and the damaged axons can regenerate within their original endoneurial tubes and reinnervate their original target organ. After a complete lesion to the nerve, however, functional recovery of movement is often quite poor. The loss of functional recovery probably is related to the failure of the axons to regenerate and the misdirection of regenerating axons, which leads to inappropriate innervation of denervated muscles. Inappropriate innervation is thought to result in a loss in the ability to accurately recruit individual muscles and motor units within a muscle, resulting in the loss of motor control.
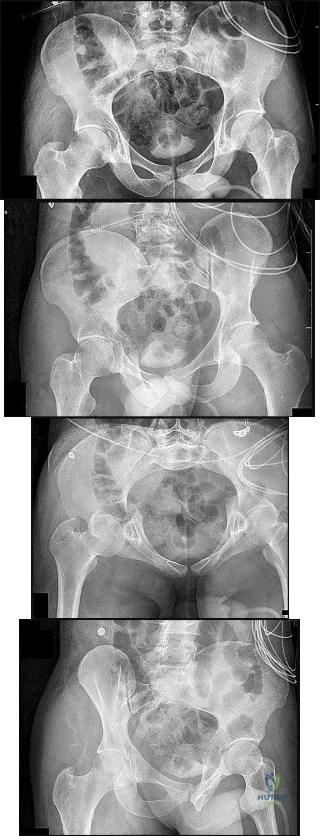
Question 90
Figures 15a through 15d
Explanation
Plain radiographic imaging of a patient with an acetabular injury begins with 5 standard views of the pelvis (anteroposterior [AP], iliac oblique, obturator oblique, inlet, and outlet views). These views will show fractures of the acetabulum and help to evaluate for pelvic fractures and hip joint integrity. The obturator oblique view is taken with the injured side rotated 45 degrees forward with the beam centered on the patient’s affected hip. This shows the anterior column and posterior wall and will reveal if any posterior subluxation of the hip is present. The iliac oblique view is taken with the injured side of the patient rolled 45 degrees forward with the beam centered on the affected hip. This shows the posterior column and the anterior wall. Inlet and outlet pelvic radiographs may depict pelvic injuries such as sacroiliac joint fracture or widening.
Judet and Letournel have a classification system for acetabular fractures. The system consists of 5 elementary fracture patterns: anterior wall, anterior column, posterior wall, and posterior column fractures of the acetabulum and a transverse pattern. There are also 5 associated fracture patterns: posterior column/posterior wall, transverse/posterior wall, T-type, anterior column with hemitransverse fracture of the posterior column, and both-column fractures.
Figure 12b shows a fracture of the posterior column on the Iliac oblique, and Figure 12c shows a fracture of the posterior wall in the obturator oblique.
In Question 13, the figures only reveal a fracture of the posterior wall, and this is best appreciated in Figure 13c, the obturator oblique view.
The T-type fracture is a transverse fracture with a secondary fracture line extending inferiorly. This causes the anterior and posterior columns to be separated. The iliac oblique view, Figure 14b, shows a fracture extending through the posterior column. In the obturator oblique view (Figure 14c), the yellow arrow shows a fracture extending through the anterior column, and the red arrow shows a fracture extending inferiorly through the ischium.
Fractures extending through the anterior and posterior columns are seen, which represent a transverse fracture, but there is no extension inferiorly, which eliminates T-type as a possible correct response. The anterior column fracture is best seen on the inlet view (Figure 15b), but it also can be seen in Figure 15d, the obturator oblique view. Figure 15c shows the fracture through the posterior column. For this patient, a small fracture of the posterior wall is visualized on the AP view (Figure 15a).
RECOMMENDED READINGS
Dickson KF, Dowling RM. Treatment of pelvic and acetabular fractures in elderly patients. Orthopaedic Knowledge Online Journal. Volume 11, Number 8 August 2013.
Tornetta P 3rd. Displaced acetabular fractures: indications for operative and nonoperative management. J Am Acad Orthop Surg. 2001 Jan-Feb;9(1):18-28. Review. PubMed PMID: 11174160. View Abstract at PubMed
Moed BR, Kregor PJ, Reilly MC, Stover MD, Vrahas MS. Current management of posterior wall fractures of the acetabulum. Instr Course Lect. 2015;64:139-59. Review. PubMed PMID: 25745901. View Abstract at PubMed
Question 91
Which of the following statements best describes labral tears in the hip? Review Topic
Explanation
Question 92
Type I collagen fibers in peripheral nerves are primarily responsible for which of the following?
Explanation
The COL1A1 gene produces a component of type I collagen, called the pro-alpha1(I) chain. This chain combines with another pro-alpha1(I) chain and also with a pro-alpha2(I) chain (produced by the COL1A2 gene) to make a molecule of type I procollagen. These triple-stranded, rope-like procollagen molecules must be processed by enzymes outside the cell. Once these molecules are processed, they arrange themselves into long, thin fibrils that cross-link to one another in the spaces around cells. The cross-links result in the formation of very strong mature type I collagen fibers.
Wong et al. provide a review of the basic science behind nerve healing and the recovery after nerve repair. They note the importance of minimizing additional surgical insult and careful handling of nerve tissue during repair to optimize outcomes.
Pertici et al. noted that autologous nerve implantation to bridge a long nerve gap presents the greatest regenerative performance in spite of substantial drawbacks. They were able to show improved nerve guided regrowth with a type I collagen matrix conduit as compared to a conduit made of a mix of type I and type III collagen.
Illustration A shows a diagram of type I collagen, showing the rope-like characteristics behind the tensile strength.
Incorrect Answers:
Question 93
- An orthopaedic surgeon who is the developer of a knee arthroplasty system is discussing treatment options with a patient who has tricompartmental osteoarthritis. As a part of this discussion, the orthopaedic surgeon has an obligation to disclose
Explanation
III. Conflicts of Interest
B. Where there are financial interests involved in the ownership of a pharmacy, rehabilitation center, imaging equipment, surgery center, or health care facility where the orthopaedic surgeon’s financial interest is not immediately obvious, the orthopaedic surgeon must disclose that financial interest to the patient and to colleagues.
C. When an orthopaedic surgeon receives anything of value, including royalties, from a manufacturer, the orthopaedic surgeon must disclose this fact to the patient and to colleagues. It is unethical for an orthopaedic surgeon to receive compensation (excluding royalties) from a manufacturer for using a particular device or medication. Reimbursement for administrative costs in conducting or participating in a scientifically sound research trial is acceptable.
Question 94
What is the most common result if the acetabulum is rotated too far anteriorly during a periacetabular osteotomy?
Explanation
REFERENCES: Hussell JG, Rodriguez JA, Ganz R: Technical complications of the Bernese periacetabular osteotomy. Clin Orthop 1999;363:81-92.
Myers SR, Eijer H, Ganz R: Anterior femoroacetabular impingement after periacetabular osteotomy. Clin Orthop 1999;363:93-99.
Question 95
The patient decides to pursue surgical intervention. Which compartments should be released?
Explanation
>30 mm Hg at 1 minute post exercise, or >20 mm Hg at 5 minutes post-exercise. The anterior and lateral compartments are the only ones that meet strict diagnostic criteria for chronic exertional compartment syndrome. The superficial posterior compartment, although close to meeting criteria, is not responsible for the patient's symptoms and falls below current thresholds for diagnosis.
Question 96
Figure 29a shows the clinical photograph of a 26-year-old woman who has had the leg deformity since birth. She reports difficulty with walking and weight bearing and notes increased discomfort and swelling when the leg is dependent. She denies any history of trauma or family history of a similar disorder. Examination reveals a fixed equinovarus deformity of the foot but no evidence of a limb-length discrepancy. No other cutaneous findings or soft-tissue masses are noted. Sagittal and axial T1- and T2-weighted MRI scans are shown in Figures 29b and 29c. What is the most likely diagnosis?
Explanation
REFERENCES: Berquist TH (ed): MRI of the Musculoskeletal System, ed 3. Philadelphia, PA, Lippincott Raven, 1997, p 771.
Enzinger FM, Weiss SW: Soft Tissue Tumors, ed 3. St. Louis, MO, Mosby Year Book, 1995, p 688.
Question 97
The thumb metacarpophalangeal (MCP) joint should be flexed to what degree to properly assess ligamentous stability?
Explanation
REFERENCES: Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgery, 2002, pp 339-358.
Stener B: Displacement of the ruptured ulnar collateral ligament of the MP joint of the thumb: A clinical and anatomical study. J Bone Joint Surg Br 1962;44:869-879.
33 • American Academy of Orthopaedic Surgeons
Question 98
A 32-year-old man who works as a laborer has had left trapezius wasting and lateral scapular winging after injuring his shoulder when a cargo box fell onto his neck 8 months ago. He now reports posterior shoulder pain and fatigue, and he has difficulty shrugging his shoulder. Examination reveals marked scapular winging, impingement signs, and an asymmetrical appearance when the patient attempts a shoulder shrug. Primary scapular-trapezius winging is the result of damage to the
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;108:15-18.
Question 99
A patient undergoes cartilage implantation requiring amplification of donor cells. Which of the following statements best describes the transplants?
Explanation
REFERENCES: Brittberg M, Peterson L, Sjogren-Jansson E, et al: Articular cartilage engineering with autologous chondrocyte transplantation. J Bone Joint Surg Am
2003;85:109-115.
Caplan AI, Elyaderani M, Mochizuki Y, et al: Principles of cartilage repair and regeneration. Clin Orthop 1997;342:254-269.
Question 100
What is the second most common primary bone malignancy in children?
Explanation
REFERENCES: Menendez LR (ed): Orthopaedic Knowledge Update: Musculoskeletal Tumors. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 195.
Gibbs CP Jr, Weber K, Scarborough MT: Malignant bone tumors. Instr Course Lect 2002;51:413-428.
