OITE & ABOS Orthopedic Board Prep MCQs: Hip, Sports Medicine & Oncology | Part 148

Key Takeaway
This page presents Part 148 of a professional orthopedic board review quiz. Targeting surgeons and residents preparing for OITE/ABOS exams, it offers 100 high-yield, verified MCQs on Hip. Interactive study/exam modes with detailed explanations optimize your certification readiness.
About This Board Review Set
This is Part 148 of the comprehensive OITE and AAOS Orthopedic Surgery Board Review series authored by Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon.
This set has been strictly audited and contains 100 100% verified, high-yield multiple-choice questions (MCQs) modelled on the exact format of the Orthopaedic In-Training Examination (OITE) and the American Academy of Orthopaedic Surgeons (AAOS) board examinations.
How to Use the Interactive Quiz
Two distinct learning modes are available:
- Study Mode — After selecting an answer, you immediately see whether you are correct or incorrect, together with a full clinical explanation and literature references.
- Exam Mode — All feedback is hidden until you click Submit & See Results. A live timer tracks elapsed time. A percentage score and detailed breakdown are displayed upon submission.
Pro Tip: Use keyboard shortcuts A–E to select options, F to flag a question for review, and Enter to jump to the next unanswered question.
Topics Covered in Part 148
This module focuses heavily on: Hip.
Sample Questions from This Set
Sample Question 1: Which of the following abnormalities has been observed in a higher than expected frequency in patients with metal-on-metal hip bearings?...
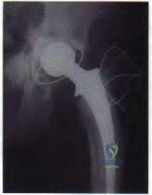
Sample Question 2: What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?...
Sample Question 3: Figures A and B are axial and coronal MRI images of a 21-year-old male athlete. He injured his left leg during a hurdling race approximately 1 week ago. What would be the next best step in the management of this injury? Review Topic...
Sample Question 4: Which of the following factors are considered prognostic of survival in patients with soft-tissue sarcomas?...
Sample Question 5: What is the most appropriate way to communicate instructions to a family when there is a language barrier?...
Why Active MCQ Practice Works
Evidence consistently demonstrates that active recall through spaced MCQ practice yields substantially greater long-term retention than passive reading alone (Roediger & Karpicke, 2006). All questions in this specific module have been algorithmically verified for clinical integrity and complete explanations.
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following abnormalities has been observed in a higher than expected frequency in patients with metal-on-metal hip bearings?
Explanation
REFERENCES: Dunstan E, Ladon D, Whittingham-Jones P, et al: Chromosomal aberrations in the peripheral blood of patients with metal-on-metal hip bearings. J Bone Joint Surg Am 2008;90:517-522. Ladon D, Doherty A, Newson R, et al: Changes in metal levels and chromosome aberrations in the peripheral blood of patients after metal-on-metal hip arthroplasty. J Arthroplasty 2004:19:78-83.
Visuri T, Pukkala E, Paavolainen P, et al: Cancer risk after metal on metal and polyethylene on metal total hip
arthroplasty. Clin Orthop Relat Res 1996:329:S280-S289. Question 61
A 73-year-old woman with a history of type II diabetes mellitus undergoes a total hip arthroplasty for osteoarthritis. She continues to have serosanguinous wound drainage from the midportion of the incision 12 days after surgery. What is the most appropriate treatment at this time?
Return to the operating room for debridement and irrigation with removal of all implants and immediate reimplantation
Return to the operating room for open debridement and irrigation, exchange of the polyethylene
insert, followed by appropriate antibiotics based on intraoperative culture results
Hip spica pressure dressing and a 2-week course of oral antibiotics
Hip aspiration for culture, followed by a 2-week course of appropriate IV antibiotics based on
culture results
Hip aspiration for culture, followed by a 6-week course of appropriate IV antibiotics based on culture results
DISCUSSION: This patient has an acute postoperative deep infection, with prolonged drainage at 12 days postoperatively. Even without other signs or symptoms of infection, the prolonged drainage this far out after surgery is concerning for an acute postoperative infection. The most appropriate treatment at this point is open debridement with retention of the implants. Modular parts, if present, are exchanged. Oral or IV antibiotics alone are generally inadequate to treat the infection, and this form of management alone would result in a missed opportunity to potentially cure the infection. Removal of all implants at this point is not required because early aggressive debridement within the first 2 weeks after surgery offers a reasonable outcome. After 4 to 6 weeks of symptoms, results of debridement are less favorable and removal of the implants is usually required.
REFERENCES: Crockarell JR, Hanssen AD, Osmon DR, et al: Treatment of infection with debridement and retention of the components following hip arthroplasty. J Bone Joint Surg Am 1998;80:1306-1313. Hanssen AD, Osmon DR: Assessment of patient selection criteria for treatment of the infected hip arthroplasty. Clin Orthop Relat Res 2000;381:91 -100.
Question 2
What are the optimal conditions for leaving the acetabular shell in place, replacing the acetabular liner, and grafting the osteolytic defect shown in Figure 39?
Explanation
REFERENCES: Ries MD: Complications in primary total hip arthroplasty: Avoidance and management. Wear. Instr Course Lect 2003;52:257-265.
Dumbleton JH, Manley MT, Edidin AA: A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002;17:649-661.
Pelicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000,
pp 175-180.
Question 3
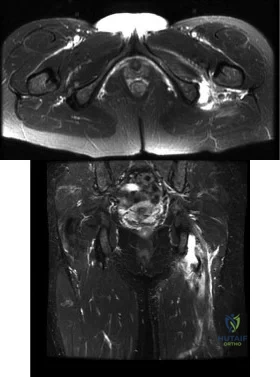
Figures A and B are axial and coronal MRI images of a 21-year-old male athlete. He injured his left leg during a hurdling race approximately 1 week ago. What would be the next best step in the management of this injury? Review Topic
Explanation
Athletes participating in sports that require sprinting, jumping, acceleration and deceleration are at increased risk of sustaining a proximal hamstring tendon avulsion. The greatest predictor of this injury is prior hamstring injury. Other risk factors include increasing age, high training demand, increased body mass index and tight hip flexor muscles. MRI is the gold standard imaging to identify these images. Open hamstring tendon repair is recommended in athletes when all of the hamstring tendons have avulsed off their origin or 2 tendons have avulsed and retracted more than 2 cm.
Cohen et al. wrote a JAAOS article on acute proximal hamstring rupture. They point out that testing the peroneal branch of the sciatic nerve function is important in the physical examination, as injury to this branch will cause weakness of the short head of the biceps femoris and may slow potential postoperative rehabilitation.
Lefevre et al. reviewed the return to sports after surgical repair of acute proximal hamstring ruptures. They performed a prospective observational study that included 34 patients. Patients returned to sports within a mean 5.7 ± 1.6 months, at the same level in 27 patients (79.4 %) and at a lower level in 7 patients (20.6 %). They conclude that surgical repair of acute proximal hamstring ruptures has the potential to significantly improve the functional prognosis of patients with these injuries.
Figures A and B shows a significant amount of swelling and hematoma around the hamstring tendon. The whole ischial tuberosity is denuded of tendon, which is consistent with a complete rupture. Illustration A shows a large posterior thigh ecchymosis commonly seen with this injury. The ecchymosis presents approximately 1 week following injury, which is know as latent ecchymosis. Illustration B shows a
schematic and intraoperative image of the open tendon repair of an acute injury.
Incorrect
Question 4
Which of the following factors are considered prognostic of survival in patients with soft-tissue sarcomas?
Explanation
REFERENCES: Cheng EY, Thompson RC Jr: New developments in the staging and imaging of soft-tissue sarcomas. Instr Course Lect 2000;49:443-451.
Fleming ID, et al: Manual for Staging of Cancer/American Joint Committee on Cancer, ed 5. Philadelphia, PA, Lippincott Raven, 1997, pp 149-156.
Question 5
What is the most appropriate way to communicate instructions to a family when there is a language barrier?
Explanation
Ideally, professional medical interpreters should be used in situations involving language difficulties. Printed instructions are helpful, but, if there is a language barrier, these instructions cannot substitute for conversing and answering questions. Asking the child to translate (no matter how fluent he or she may be) is suboptimal. Nonmedical staff may not be fluent enough to adequately translate medical terms.

RESPONSES FOR QUESTIONS 14 THROUGH 16
Aspiration, cultures, surgical irrigation and debridement, and intravenous (IV) nafcillin
Aspiration, cultures, surgical irrigation and debridement, and IV vancomycin
Aspiration, cultures, Lyme serology, and oral amoxicillin
Biopsy, culture, curettage, bone graft, and possible internal fixation
Physical therapy, ibuprofen, and an antinuclear antibody test
Select the most appropriate treatment above to address each clinical scenario below.
Question 6
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?
Explanation
REFERENCES: Rajasekaran S: The natural history of post-tubercular kyphosis in children: Radiological signs which predict late increase in deformity. J Bone Joint Surg Br
2001;83:954-962.
Rajasekaran S, Shanmagasundaram TK, Prabhakar R, Dheenadhayalan J, Shetty AP, Shetty DK: Tuberculous lesions of the lumbosacral region: A 15-year follow-up of patients treated by ambulant chemotherapy. Spine 1998;23:1163-1167.
Question 7
A 20-year-old collegiate pitcher sustains a medial collateral ligament (MCL) rupture of his throwing elbow for which surgical reconstruction is necessary. The goal of surgery is anatomic restoration of the MCL. Which statement best describes the kinematics of the native MCL?
Explanation
full extension and full flexion. True lateral radiographs reveal that the flexion-extension axis, or center of rotation, of the elbow lies in the center of the trochlea and capitellum. The origin of the anterior bundle of the MCL lies slightly posterior to the rotational center of the elbow. The anterior bundle is further divided into an anterior band and a posterior band. The eccentric origin of these anterior bundle components in relation to the rotational center through the trochlea creates a CAM effect during flexion and extension. The anterior band tightens during extension, and the posterior band tightens during flexion. This reciprocal tightening of the two functional components of the anterior bundle allows the ligament to remain taut throughout the full range of flexion. Cadaver dissection studies have identified the origin and insertion of both the medial and lateral stabilizing elbow ligaments. The anterior bundle of the MCL is isometric throughout the flexion/extension arc of motion, making Response C incorrect. The posterior bundle of the MCL elongates with elbow flexion, so Responses B and D are incorrect. The posterior bundle of the MCL also demonstrates the most change in
length from extension to flexion of all the elbow ligaments.
Question 8
Regarding the role of the orthopaedic surgeon in addressing domestic and family violence, all of the following statements are true EXCEPT:

Explanation
state. The AAOS Advisory statement gives information to assist in meeting the ethical and legal obligations on Domestic and Family Violence and Abuse.
Domestic and family violence affects over 10% of the US population (approximately 32 million Americans). Child abuse and neglect contributed to 1,400 fatalities in 2002 and there was 565,747 reports of suspected elder abuse.
Reporting of suspected child abuse is required in all states. The orthopaedic surgeon should hospitalize elderly victims who are in immediate danger and help develop a plan to insure their safety.
Question 9
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
REFERENCES: Rockwood CA Jr, Odor JM: Spontaneous atraumatic anterior subluxation of the sternoclavicular joint. J Bone Joint Surg Am 1989;71:1280-1288.
Rockwood CA, Matsen FA (eds): The Shoulder, ed 2. Philadelphia, PA, WB Saunders, 1998,
p 583.
Question 10
A 40-year-old man with a history of Legg-Calve-Perthes disease underwent a right hip resurfacing 3 years ago with no perioperative complications. Hip pain has developed gradually during the last 4 months. Radiographs show no evidence of fixation loosening or any adverse changes at the femoral neck. No periarticular osteolysis is evident. A large intra-articular and intrapelvic pseudotumor has developed. What predominant histological feature(s) is/are present in such a lesion?
Explanation
Controversy persists over what exactly is the best approach to managing patients with metal-on-metal (MOM) hip arthroplasties. All patients with painful MOM hip arthroplasties should be examined for fixation loosening, wear/osteolysis, and infection—no differently than patients without MOM hip arthroplasties. It is recommended to obtain serum trace element levels. If the levels are high, cross-sectional imaging should be obtained to determine whether any pseudotumor or tissue necrosis is present around the hip arthroplasty. Hip aspiration should be considered if concern for infection exists. Adverse tissue reaction has been identified to occur around MOM hip arthroplasties. The predominant histologic feature is tissue necrosis with infiltration of lymphocytes and plasma cells.
Question 11
A 46-year-old male is involved in a motor vehicle accident and suffers a proximal humerus fracture. Operative treatment is recommended, and plate fixation is performed through an extended anterolateral acromial approach. Which of the following structures is at increased risk of injury using this surgical exposure compared to the deltopectoral approach?

Explanation
Gardner et al evaluated 23 patients who had acute displaced fractures of the proximal humerus treated with the anterolateral acromial approach and either a locking plate or an intramedullary nail. At one year post-op, there were no axillary nerve deficits, and they found that the approach allowed direct access to the lateral fracture planes for fracture reduction and plate placement or safe nail and interlocking screw placement.
Gardner et al, in another study, performed cadveric dissection using the extended anterolateral acromial approach and measured multiple parameters regarding the axillary nerve. The nerve was predictably found approximately 35 mm from the prominence of the greater tuberosity.
Morgan et al performed a cadaveric study to describe the anatomic insertion point of the deltoid onto the proximal humerus. They found that the deltoid insertion is long and broad, and that placement of 4.5-mm plate would result in detaching 13.5 mm of its insertional footprint. This would leave half of the insertion still attached to the humerus.
Illustration A identifies the location of the incision for the anterolateral acromial exposure , and Illustration B shows the position of the axillary nerve in relation to the approach.
Question 12
A 62-year-old man with a long history of ankylosing spondylitis has neck pain after lightly bumping his head on the wall. Examination reveals neck pain with any attempted motion; the neurologic examination is normal. Plain radiographs show extensive ankylosis of the cervical spine and kyphosis but no fracture. What is the next most appropriate step in management?
Explanation
REFERENCES: Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998,
pp 724-727.
McDowell GS, Cammisa FP, Eismont FJ: Hyperextension injuries of the cervical spine, in Levine AM, Eismont FJ, Garfin SR, Zigler JE (eds): Spine Trauma. Philadelphia, PA,
WB Saunders, 1998, pp 372-374.
Question 13
Lymphatic metastasis is a common feature of which of the following lesions?
Explanation
Question 14
- A 19-year-old man sustains a complete spinal cord injury at the C7 level as a result of diving into a lake. He has a blood pressure of 90/50 mm Hg, a pulse of 60/min, and respirations of 20/min. These values most likely signify
Explanation
Question 15
A 52-year-old woman who underwent cheilectomy 1 year ago for hallux rigidus now reports continued pain in the first metatarsophalangeal joint. She did not have any incision healing problems, and has not had any fevers, erythema, or drainage. Which of the following procedures will provide the best combination of pain relief and function?
Explanation
REFERENCES: Machacek F Jr, Easley ME, Gruber F, et al: Salvage of a failed Keller resection arthroplasty. J Bone Joint Surg Am 2004;86:1131-1138.
Myerson MS, Schon LC, McGuigan FX, et al: Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int
2000;21:297-306.
Question 16
A knock-out mouse for the Vitamin D receptor has which of the following phenotypes?
Explanation
REFERENCES: Glowacki J, Hurwitz S, Thornhill TS, et al: Osteoporosis and vitamin-D deficiency among postmenopausal women with osteoarthritis undergoing total hip arthroplasty. J Bone Joint Surg Am 2003;85:2371-2377.
Buckwalter JA, Einhorn TA, Simon SR (eds): Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, p 51.
Question 17
Among the ankle arthroscopy portals described below, which portal is at highest risk for serious complications?
Explanation
All of the portals listed pose risk for some structures. Because they have been shown to be the safest, the most common anterior portals are the anteromedial and the anterolateral. The safest posterior portal is the posterolateral portal. Because of the location of the posterior medial tendons and the neurovascular bundle, the posteromedial portal is at highest risk for serious complications.
RECOMMENDED READINGS
Golanó P, Vega J, Pérez-Carro L, Götzens V. Ankle anatomy for the arthroscopist. Part I: The portals. Foot Ankle Clin. 2006 Jun;11(2):253-73, v. Review. PubMed PMID: 16798511.View Abstract at PubMed
Ferkel RD, Hommen JP. Arthroscopy of the ankle and foot. In: Coughlin MJ, Mann RA, Saltzman CL, eds. Surgery of the Foot and Ankle. Vol 2. 8th ed. Philadelphia, PA: Mosby; 2007:1641-1726.
Figure 90 is an intraoperative image showing the medial approach to the elbow. The arm is proximal and to the right, and the forearm is distal and to the left. The blue arrow points to the medial epicondyle. A black arrow points to a piece of glass in a nervous structure. This injury most likely would affect which distal muscular structure?

Extensor digiti minimi
Flexor digitorum superficialis (FDS) to the index finger 77
Abductor pollicis brevis
First dorsal interossei
DISCUSSION
The intraoperative image shows a piece of glass splitting the ulnar nerve in the cubital tunnel. The extensor digiti minimi is innervated by the radial nerve. The FDS to the index finger and the abductor pollicis brevis are innervated by the median nerve. The first dorsal interossei is the last muscle innervated by the ulnar nerve.
RECOMMENDED READINGS
Miller MD. Review of Orthopaedics. 3rd ed. New York, NY: Saunders; 2000.
Anderson JE. Grant’s Atlas of Anatomy. 8th ed. Baltimore, MD: Williams & Wilkins; 1983.
Question 18
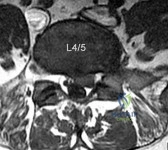
A 32-year-old male presents with left leg pain and weakness. An axial image from his MRI is shown in Figure A. Which of the following physical exam findings would be most consistent with this MRI finding. Review Topic
Explanation
radiculopathy.
While nerve root innervation shows some variability by patient, L5 is "characteristically" responsible for the sensation to the dorsal aspect of the foot, ankle dorsiflexion (tibialis anterior - along with L4), great toe extension (EHL), and hip abduction (gluteus medius).
Suri et al. reported on specific physical exam findings that significantly increased the likelihood of nerve root impingement at specific lumbar levels. They found: L2 was associated with decreased anterior thigh sensation. L3 was associated with a positive femoral stretch test. L4 was associated with a blunted patellar reflex, decreased medial ankle sensation or a positive crossed femoral stretch test. L5 was associated with was associated with decreased hip abductor strength.
Luri et al. reported 8-year follow up on the patients in the spine patient outcomes research trial who underwent surgical vs. conservative care for treatment of lumbar herniated disc. They found that patients who underwent surgical treatment had superior results that were maintained at 8 years compared to patients who underwent conservative management.
Figure A is an axial MRI at the L4/5 disc space that shows a left paracentral disc herniation compressing the descending L5 nerve root. Illustration A identifies the structures in the MRI image. Illustration B demonstrates the dermatome, reflex and motor function associated with the L4, L5 and S1 nerve root.
Incorrect Answers:
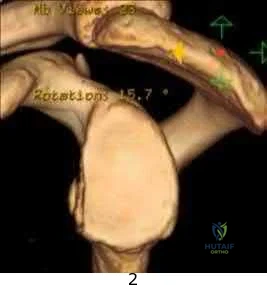
(SBQ13PE.102) An 26-year-old male presents to your office complaining of bilateral hip and low back pain. On physical examination, he has 10 degree bilateral hip flexion contractures. An AP pelvis radiograph is demonstrated in figure A. Which of the following findings is consistent with this patient's presentation? Review Topic

A positive flexion, adduction, internal rotation (FADDIR) test
A history of untreated slipped capital femoral epiphysis (SCFE)
A thrombophilia
Normal serum ESR and CRP
Positive Human Leukocyte Antigen B27 (HLA-B27)
The patient has large joint arthralgia and sacroiliac joint sclerosis on AP pelvis radiograph, which is consistent with ankylosing spondylitis. Patients with ankylosing spondylitis have positive Human Leukocyte Antigen B27 (HLA-B27).
Ankylosing spondylitis (AS) is a seronegative spondyloarthropathy that affects the axial skeleton as well as large joints including the hips and knees. The most common initial site of pain is the sacroiliac (SI) joint, and is demonstrated as sacroiliitis on pelvic radiograph. Hip involvement is common, and typically manifests as hip pain and flexion contracture. Serologic studies will be typically be negative for rheumatoid factor, but positive for HLA-B27 in 90% of patients.
Kubiak et. al. review orthopaedic management of AS. Common orthopaedic manifestations include SI joint pain, hip flexion contractures, and stiffness of the cervical and lumbar spine. They report that laboratory analysis of patients with active disease will typically demonstrate mild elevation of ESR, CRP, and WBC. Patients with chronic AS may demonstrate a normocytic anemia. If HLA-B27 is negative, a high clinical suspicion should still be maintained.
Gensler et al. review the different clinical conditions that compose of juvenile-onset spondyloarthritis. They report on the different spondyloarthritides includes ankylosing spondylitis, reactive arthritis, arthropathy associated with inflammatory bowel disease, and that associated with psoriasis. They emphasize that the appearance of sacroiliac joint and spinal disease in the form of ankylosing spondylitis usually takes 5–10 years after initial symptom presentation, and therefore, a definite diagnosis can take several years leading to a delay in diagnosis.
Figure A is an AP pelvis radiograph of a skeletally mature individual demonstrating sclerosis of the SI joint indicative of sacroiliitis. Illustration A shows a axial CT image of the patient in the stem. Sclerosis and bone erosion can be seen in the sacroiliac joint.
Incorrect Answers:
osteonecrosis Answer 3: A infarctions,
of
the
femoral
epiphysis.
thrombophilia may have
osseous manifestations such as bone
which
are
not
evident
on
this
image.
Question 19
Which of the following lumbar disk components has the highest tensile modulus to resist torsional, axial, and tensile loads? Review Topic
Explanation
Question 20
Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of
Explanation
REFERENCES: Pateder DB, Park HB, Chronopoulos E, et al: Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent: A case report. J Bone Joint Surg Am 2004;86:2290-2293.
Wang P Jr, Koval KJ, Lehman W, et al: Salter-Harris type III fracture-dislocation of the proximal humerus. J Pediatr Orthop B 1997;6:219-222.
Question 21
A 35-year-old runner has pain beneath the second metatarsophalangeal joint. He reports that he has significantly decreased his running distance since the onset of the pain. He denies any history of trauma or injury to the foot. A radiograph is shown in Figure 14. Initial management should consist of
Explanation
REFERENCES: Trepman E, Yeo SJ: Nonoperative treatment of metatarsophalangeal joint synovitis. Foot Ankle Int 1995;16:771-777.
Mizel MS, Michelson JD: Nonsurgical treatment of monarticular nontraumatic synovitis of the second metatarsophalangeal joint. Foot Ankle Int 1997;18:424-426.
Question 22
A 75-year-old female with a longstanding history of brachial plexus palsy 2 . A 63-year-old male with a 6 month history of shoulder pain and inability to abduct past 30 degrees

Explanation
A TSA involves replacement of the humeral head with a metal head and resurfacing of the glenoid to a cemented all-polyethylene surface. In order to achieve optimal results, patients must be selected carefully. Patients with an irreparable rotator cuff tear, non-functioning deltoid, inadequate glenoid bone stock and brachial plexopathy are poor candidates for TSA.
Edwards et al. conducted a multicenter randomized controlled trial to compare TSA versus hemiarthroplasty in patients with primary osteoarthritis of the shoulder. They found that TSA provided better scores for pain, mobility, and activity than hemiarthroplasty at 2 year follow-up. Boileau et al. followed 45 consecutive patients who underwent reverse TSA ( rTSA) for cuff tear arthropathy (CTA), post-traumatic arthritis, and failure of revision arthroplasty. After a mean follow-up of 40 months, they found that the reverse prosthesis improved function and was able to restore active elevation in patients with incongruent cuff-deficient shoulders. They also found that
the results were less predictable and complication and revision rates were higher in patients undergoing revision surgery as compared to those patients undergoing rTSA for CTA.
Illustrations A and B show the preoperative and postoperative x-rays of a patient with characteristic OA of the glenohumeral joint that was treated with TSA.
Incorrect Answers:

Figure A is a glenoid CT 3D reconstruction of a 26-year-old accountant who has recurrent shoulder instability. His first dislocation occurred after a fall while skiing. He has now sustained his third dislocation, which was reduced in the emergency department prior to being sent to your office. What is the most appropriate definitive treatment?
Immobilization in external rotation for 6 weeks Arthroscopic bony Bankart repair

Arthroscopic Remplissage procedure

Glenoid augmentation using coracoid transfer Glenoid augmentation using tricortical iliac crest graft
This patient has recurrent shoulder instability with a small bony defect of the anterior glenoid and no previous surgery. The most appropriate definitive management in this patient would be arthroscopic bony Bankart repair.
Older (>20 years old), recreational athletes with minor glenoid bone loss (<20 % of the glenoid surface area) may be treated with soft tissue stabilization procedures using suture anchors. Goals of this procedure include tightening and repairing the torn ligament and labrum to the glenoid.
Younger, contact sports athletes with large glenoid defect (>20%) may require bony augmentation type of procedures.
Lynch et al. review the clinical presentation, assessment and treatment algorithm for surgical management of bone loss associated with anterior shoulder instability. While defects larger than 25% of glenoid width should be managed with bony augmentation, they recommend soft-tissue stabilization in smaller defects.
Balg et al. analyzed 131 patients following Bankart procedure and identified following risk factors for failure: age <=20, competitive participation in contact sports, shoulder hyperlaxity, Hill-Sachs on AP radiograph, glenoid bone loss of contour on AP radiograph.
Using human cadaveric shoulders with various anterior glenoid defects sizes, The MOON Shoulder Group compared radiography, MRI and CT to determine the most reliable imaging modality for predicting bone loss. Three-dimensional CT, followed by regular CT were the most reliable and reproducible imaging modalities for predicting glenoid bone loss.
Figure A shows an en face sagittal 3D reconstruction of a glenoid with 10% surface area loss. Incorrect Answers:
A latissimus dorsi tendon transfer is a well established procedure for treatment of massive irreparable posterosuperior rotator cuff tears. All of the following factors have been shown to result in worse clinical outcomes after a transfer EXCEPT?

Nonsynergistic action of the transferred muscle Fatty atrophy of the supraspinatus and infraspinatus Deficiency of the subscapularis

Absence of the coracoacromial ligament Deltoid weakness
A latissimus dorsi tendon transfer can be utilized in patients with a massive, irreperable rotator cuff tear involving the supraspinatus and infraspinatus. It has been reported to relieve pain and improve function in a carefully selected patient population. Those patients with deficiency of the deltoid or subscapularis, nonsynergistic muscle action after transfer, or fatty infiltration of the posterosuperior cuff have worse clinical outcomes. Absence of the CA ligament may allow anterosuperior escape in RC deficient shoulders but has not been shown to lead to worse outcomes after a tendon transfer.
The paper by Warner, et. al demonstrated that poor tendon quality, stage 3/4 muscle fatty degeneration, and detachment of the deltoid insertion each had a statistically significant effect on the Constant score noting that salvage reconstruction of a previous cuff repair had more limited gains as compared to primary. The reference by Ianotti, et. al showed that synchronous in-phase contraction of the transferred latissimus dorsi is associated with a better clinical result while improved preoperative shoulder function and general strength also positively influence the clinical result.
An active 68-year-old woman undergoes an uncomplicated rotator cuff repair with a double-row construct using biocomposite knotless anchors. At her two month follow up, she is noted to have increased shoulder pain, weakness and limited motion. Imaging reveals failure of the rotator cuff repair. What is the most likely mechanism of failure?

Anchor fatigue and breakage Anchor pull out from bone

Suture rupture secondary to anchor eyelet abrasion Suture pull out from the repaired tissue

Infection
Rotator cuff repair (RCR) failure most commonly occurs from a failure of the repaired tissue to heal with suture anchor pull out from the repaired tissue.
The overall complication rate of arthroscopic RCR is roughly 10%. Failed RCR most commonly results from failure to heal (19-94%) secondary to poor rotator cuff tissue, insufficient vascularity or poor bone quality. Other causes of RCR failure include surgical complications (deltoid disruption, infection, foreign body reaction, stiffness, neurologic injury), diagnostic errors (missed lesions of the rotator interval, long head of biceps or subscapularis tear), and technical errors (excessive tension due to lack of proper tissue mobilization, anchor pull out secondary to improper anchor placement).
George et al evaluated the causes of failed RCR and results of revision RCR. While results of revision RCR are inferior to primary RCR, arthroscopic repair yields > 60% good or excellent results. Risk factors for poor results following revision RCR include poor tissue quality, detachment of the deltoid origin and multiple previous surgeries.
Diduch et al reviewed the design and composition of various anchors used in arthroscopic shoulder surgery. Current advancements in the field include highstrength polyethylene sutures, new biocompatible anchor materials (PEEK, biocomposite) and modified designs including knotless systems. With improved strength of the current anchors and repair constructs, the most common mode of arthroscopic RCR failure is now related to tissue failure occurring at the tissue-anchor interface.
Cole et al discussed the different primary rotator cuff repair constructs, including single row, double row, transosseous and transosseous equivalent. The authors concluded that construct selection depends on tear acuity, size and tissue quality. For acute tears < 12mm in anteroposterior length, singlerow configuration likely has sufficient strength to maintain the repair and promote healing. For more chronic tears, poor tissue quality, or tears > 1215 mm in the anteroposterior dimension, the authors recommend double-row or transosseous-equivalent repair to better restore the anatomic footprint and provide optimal mechanical stability to achieve healing. Illustration A is an algorithm from George et al detailing the decision-making process when considering revision RCR for a symptomatic failed RCR.
Incorrect Responses
Biocomposite anchors exhibit high load-to-failure and result in fatigue failure less commonly than metal anchors.
A 32-year-old cross-training athlete awakens with severe left neck and shoulder pain after a day of intense upper body training. Aside from a recent viral illness, he is otherwise healthy. His pain improves, but two weeks later he notes significant left shoulder weakness. Examination reveals weakness of shoulder abduction, forward elevation and external rotation with the arm at his side. Radiographs are normal. Electromyography demonstrates 2+ positive sharp waves and fibrillations. Sensory nerve conduction studies show reduced amplitudes. MRI of the brain, cervical spine and shoulder are shown in Figures A-D, respectively. Which of the following is true of his prognosis?
Decompression will result in improved muscle strength and function.

The patient can expect a gradual return of muscle strength without long term functional deficits. Immunomodulators may decrease the number and severity of his relapses. 4 . Arthroscopic repair will result in the best functional outcomes given the patient's high activity level.
Question 23
Figures 10a and 10b show the radiographs of a 47-year-old man who reports pain in both shoulders. He has a history of leukemia that was treated with chemotherapy and high-dose cortisone. What is the most reliable treatment option for pain relief in this patient? Review Topic

Explanation
Question 24
What is the most appropriate treatment?
Explanation
A common postsurgical problem after TKA is a sudden increase of pain that typically occurs about 2 to 3 weeks after surgery. ESR findings are not reliable during the acute postsurgical period. A CRP level exceeding 100 mg/L during the acute postsurgical period is a joint aspiration indication. If the patient does not have sepsis, there is no emergency. This pain is likely attributable to too much activity during physical therapy. Observation is recommended for this patient.
Question 25
Figure 83a shows an axillary radiograph and Figures 83b and 83c show axial MR arthrograms of a 20-year-old collegiate offensive lineman who has shoulder pain while pass-blocking. He sustained a shoulder injury 3 months earlier when he "jammed it." Prior to this injury, he denies any pain or instability in either shoulder. Despite undergoing rehabilitation with a physical therapist and trainer and abstaining from playing for 6 weeks, he is currently unable to play because of his symptoms. Examination reveals full active range of motion, a positive jerk test which reproduces his symptoms, and a grade 2 posterior translation of the humeral head with load and shift testing which also reproduces his symptoms. What is the best management option to allow him to return to his pre-injury function next season? Review Topic
Explanation
Question 26
Figures 1 through 4 show the radiographs and MRI obtained from a 40-year-old man who has a 6-week history of ring finger pain, redness, and swelling after puncturing the finger with a toothpick. Purulent drainage from the puncture wound site grew Eikenella corrodens . The patient was initially treated with oral antibiotics for 10 days and then intravenous (IV) antibiotics for 3 weeks. What is the best next step in treatment?

Explanation
This patient has a septic distal interphalangeal joint, which was treated with antibiotics alone. As a result, the patient developed osteomyelitis with bone destruction and abscess. The best way to treat this problem is to perform surgical débridement of bone and soft tissue, along with abscess drainage and an appropriate antibiotic regimen. Antibiotic treatment without surgery would not be successful in eliminating this particular infection. Bone scan with biopsy is not the correct option, because this problem is an infection and not a tumor, and MRI already has provided enough diagnostic information.
Question 27
A 37-year-old man who works in a factory has isolated, lateral unicompartmental pain about his knee with activities. Nonsurgical management has failed to provide relief. The radiograph shown in Figure 45 reveals a tibiofemoral angle of approximately 15 degrees which is clinically correctable to neutral. What is the best surgical option in this patient?
Explanation
REFERENCES: Mathews J, Cobb AG, Richardson S, et al: Distal femoral osteotomy for lateral compartment osteoarthritis of the knee. Orthopedics 1998;21:437-440.
Cameron HU, Botsford DJ, Park YS: Prognostic factors in the outcome of supracondylar femoral osteotomy for lateral compartment osteoarthritis of the knee. Can J Surg 1997;40:114-118.
Question 28
A 32-year-old man who sustained a tarsometatarsal (Lisfranc) injury 3 years ago now reports increasing pain in the left foot. Orthotics, nonsteroidal anti-inflammatory drugs, and injections have provided only temporary relief. Examination reveals swelling and tenderness over the tarsometatarsal joints. Radiographs show advanced arthrosis of the first and second tarsometatarsal joints. Management should now include
Explanation
REFERENCES: Sangeorzan BJ, Veith GR, Hansen ST Jr: Salvage of Lisfranc’s tarsometatarsal joints by arthrodesis. Foot Ankle 1990;10:193-200.
Komenda GA, Myerson MS, Biddinger KR: Results of arthrodesis of the tarsometatarsal joints after traumatic injury. J Bone Joint Surg Am 1996;78:1665-1676.
Question 29
A 30-year-old woman has had pain in her right leg for the past 6 months. A lytic lesion is noted in the anterior cortex of the midtibia, extending 5 cm in length without a soft-tissue mass. A radiograph and a biopsy specimen are shown in Figures 35a and 35b. What is the preferred treatment?
Explanation
REFERENCES: McCarthy EF, Frassica FJ: Pathology of Bone and Joint Disorders with Clinical and Radiographic Correlation. Philadelphia, PA, WB Saunders, 1998, p 263.
Moon NF, Mori H: Adamantinoma of the appendicular skeleton: Updated. Clin Orthop Relat Res 1986;204:215-237.
Question 30
He reports that he had no problems with the knee until 6 weeks ago when he noted the gradual onset of pain following a colonoscopy. Examination reveals a painful, swollen knee. Knee aspiration reveals a WBC count of 40,000/mm3. Management should consist of

Explanation
has been used successfully when the duration of symptoms is 3 weeks or less. Long-term suppressive antibiotics are most commonly used when the patient’s medical condition precludes further surgery. Delayed reimplantation has been shown to be superior to immediate reimplantation in multiple studies. Little data support the use of arthroscopic irrigation and debridement.
Question 31
A 28-year-old woman who is training for the New York Marathon reports pain in the posteromedial aspect of her right ankle. Examination reveals tenderness just posterior to the medial malleolus. Radiographs are normal. An MRI scan is shown in Figure 3. What is the most likely diagnosis?
Explanation
REFERENCES: Boden BP, Osbahr DC: High risk stress fractures: Evaluation and treatment. J Am Acad Orthop Surg 2000;8:344-353.
Lee JK, Yao L: Stress fractures: MR imaging. Radiology 1988;169:217-220.
Question 32
A 30-year-old patient has acetabular dysplasia and moderate secondary osteoarthrosis. Which of the following studies will best help predict the success of periacetabular osteotomy?
Explanation
REFERENCE: Murphy S, Deshmukh R: Periacetabular osteotomy: Preoperative radiographic predictors of outcome. Clin Orthop 2002;405:168-174.
Question 33
Autosomal dominant
Explanation
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following tumor suppressor genes is most likely involved:
Question 34
An active, right-handed 71-year-old woman fell on her left shoulder and sustained the injury shown in the radiographs in 52a and 52b and the CT scan in 52c. Management should consist of
Explanation

Question 35
A 42-year-old woman is brought to the emergency department following a motor vehicle accident. She has sustained multiple injuries, and she is intubated and pharmacologically paralyzed. Sagittal cervical CT scans through the right cervical facets, the left cervical facets, and the midline are shown in Figures 12a through 12c, respectively. Definitive management of her cervical injury should consist of Review Topic
Explanation
Question 36
Figures below represent the radiographs obtained from a 37-year-old man with severe right knee pain. He has a history of prior tibial osteotomy for adolescent tibia vara but notes residual bowing of his legs. On examination, he is 5'8" tall and weighs 322 pounds. He has a waddling gait with a bilateral varus thrust and 20° varus deformity of both legs. His right knee range of motion is 0° to 120° with a fixed varus deformity. What is the best next step?
Explanation
This patient has severe, uncorrectable varus deformity and pain from end-stage osteoarthritis secondary to prior adolescent tibia vara. Although he is young to consider arthroplasty, this option is likely to give him the most functional limb, compared with arthrodesis with a long antegrade nail. During arthroplasty surgery, his knee will likely require extensive medial release to achieve anatomic limb alignment. Standard components in total knee arthroplasty likely would result in lateral instability, so this option is
not the best answer. The best choice is total knee arthroplasty with a constrained device, which adds constraint to the knee to provide balance.
Question 37
What is the current 5-year survival rate for patients with classic nonmetastatic, high-grade osteosarcoma of the extremity?
Explanation
REFERENCES: Arndt CA, Crist WM: Common musculoskeletal tumors of childhood and adolescence. N Engl J Med 1999;341:342-352.
Glasser DB, Lane JM, Huvos AG, Marcove RC, Rosen G: Survival, prognosis, and therapeutic response in osteogenic sarcoma: The Memorial Hospital experience. Cancer 1992;69:698-708.
Question 38
Figures 1a and 1b are the MR images of a 69-year-old woman with bilateral leg pain that is worse with ambulation. She feels better when she is sitting down or leaning on a grocery cart. Which condition or structure is indicated by the arrows?
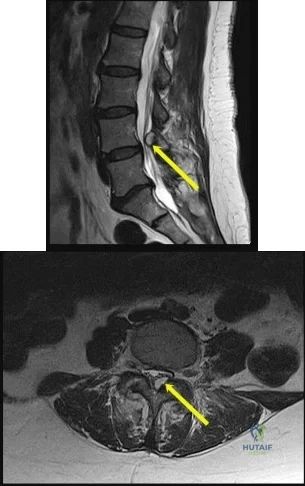
Explanation
This patient has neurogenic claudication as demonstrated by her “shopping cart” sign. Typically, spinal stenosis is attributable to bony spurs and/or a thick ligamentum flavum. However, for this patient, a large synovial cyst is the main contributing factor to stenosis. A cyst typically is filled with gelatinous material. If symptomatic, surgical excision is typically recommended because success with aspiration is unreliable. The need for fusion is debatable.
A disk herniation is not bright on T2. An arachnoid cyst is a sac filled with cerebrospinal fluid. Spinal arachnoid cysts are relatively uncommon, and typically are intradural, but they also can be extradural. Epidural lipomatosis is a condition caused by excessive accumulation of fat within the epidural space. It is not well circumscribed as seen with this lesion.
RECOMMENDED READINGS
Epstein NE, Baisden J. The diagnosis and management of synovial cysts: Efficacy of surgery versus cyst aspiration. Surg Neurol Int. 2012;3(Suppl 3):S157-66. doi: 10.4103/2152-7806.98576. Epub 2012 Jul 17. PubMed PMID: 22905322. View Abstract at PubMed
Xu R, McGirt MJ, Parker SL, Bydon M, Olivi A, Wolinsky JP, Witham TF, Gokaslan ZL, Bydon A. Factors associated with recurrent back pain and cyst recurrence after surgical resection of one hundred ninety-five spinal synovial cysts: analysis of one hundred sixty-seven consecutive cases. Spine (Phila Pa 1976). 2010 May 1;35(10):1044-53. PubMed PMID: 20173680. View Abstract at PubMed
Question 39
A 29-year-old woman is seen in the emergency department with a 24-hour history of severe back and leg pain precipitated by weight-lifting. The patient reports bilateral leg pain and is unable to urinate. She has dense anesthesia in the perineal region on examination. A MRI scan is shown in Figure 38. The patient is taken to surgery urgently. What is her prognosis for recovery? Review Topic

Explanation
Question 40
A 46-year-old man with a sacral chordoma is treated with sacrectomy.
Explanation
Complications frequently occur following treatment for spinal disorders. Postsurgical morbidity may range from minor complications such as urinary tract infection to death. Wound infections are among the most commonly encountered complications following any surgical intervention; however, their incidence after spine surgery has been reported to be in the range of only 1% to 6%. Meanwhile, risk for adjacent segment degeneration, particularly following a fusion procedure performed with an interbody device, has been documented as high as 30%. Pressure ulcers can occur when spinal injuries are treated with rigid orthoses, especially in individuals who are immobile. Risk for pressure sores and decubiti is further elevated in patients who are obtunded and cannot communicate regarding pain levels and their need to mobilize. Hardware failure may occur following any instrumented spine procedure, but risk for this complication is elevated in the event of pseudarthrosis or in settings in which no fusion is performed.
In the recent work of Lee and associates, hardware failure was the only complication encountered among patients who were treated with percutaneous stabilization without fusion for thoracolumbar burst fractures. Similarly, iatrogenic neurologic injury may transpire in the setting of any spinal intervention (its incidence is rare). For example, in a large cohort of
more than 10000 patients undergoing surgical treatment for spondylolisthesis, acute neurologic injury was reported in only 0.8% of cases. Postsurgical wound infection, although relatively rare in cases of elective spine surgery, is common following large tumor resection such as sacrectomy performed for treatment of chordomas.
RECOMMENDED READINGS
Eismont FJ, Norton RP, Hirsch BP. Surgical management of lumbar degenerative spondylolisthesis. J Am Acad Orthop Surg. 2014 Apr;22(4):203-13. doi: 10.5435/JAAOS-22-04-203. Review. PubMed PMID: 24668350. View Abstract at PubMed
Bransford RJ, Morgan RA. Thoracolumbar trauma. In: Schmidt AH, Teague DC, eds. Orthopaedic Knowledge Update: Trauma 4. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2010:373-385.
Lee JK, Jang JW, Kim TW, Kim TS, Kim SH, Moon SJ. Percutaneous short-segment pedicle screw placement without fusion in the treatment of thoracolumbar burst fractures: is it effective? comparative study with open short-segment pedicle screw fixation with posterolateral fusion. Acta Neurochir (Wien). 2013 Dec;155(12):2305-12; discussion 2312. doi: 10.1007/s00701-013-1859-x. Epub 2013 Sep 10. PubMed PMID: 24018981. View
Abstract at PubMed
Schoenfeld AJ, Carey PA, Cleveland AW 3rd, Bader JO, Bono CM. Patient factors, comorbidities, and surgical characteristics that increase mortality and complication risk after spinal arthrodesis: a prognostic study based on 5,887 patients. Spine J. 2013 Oct;13(10):1171-9. doi: 10.1016/j.spinee.2013.02.071. Epub 2013 Apr 9. PubMed PMID:
Question 41
Which of the following changes of calcium metabolism accompany the loss of bone during menopause?
Explanation
in intestinal absorption and an increase in urinary calcium loss. The reduction of
intestinal absorption is accompanied by reduced circulating concentrations of total, but
not free 1,25-dihydroxyvitamin D. However, estrogen may also directly regulate intestinal calcium resorption independent of vitamin D. Tubular resorption of calcium is higher in the presence of estrogen. Studies of the levels of PTH in the presence of estrogen are controversial.
REFERENCES: Oh KW, Rhee EJ, Lee WY, et al: The relationship between circulating osteoprotegerin levels and bone mineral metabolism in healthy women. Clin Endocrinol (Oxf) 2004;61:244-249.
Reid IR: Menopause, in Favus MJ (ed): Primer on Metabolic Bone Diseases and Disorders of Mineral Metabolism, ed 4. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 55-57.
Question 42
What factor is associated with a high risk of developing pseudotumors after metal-on-metal hip resurfacing?
Explanation
Question 43
What is the primary sign/symptom with unidirectional posterior instability of the shoulder? Review Topic
Explanation
Question 44
Figure 19 shows the radiograph of a 45-year-old woman who has a painful nonunion. Treatment should consist of
Explanation
REFERENCES: Haidukewych GJ, Israel TA, Berry DJ: Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg Am 2001;83:643-650.
Koval KJ, Zuckerman JD: Intertrochanteric fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 1635-1681.
Question 45
What is the recommended optimal timing of presurgical antibiotic administration to prevent infection in patients undergoing total joint replacement surgery?
Explanation
Question 46
The force generated by a muscle is most highly dependent on its
Explanation
Question 47
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child’s ability to walk in the future?
Explanation
REFERENCES: Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Tachdjian MO: The neuromuscular system: Cerebral palsy, in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 2, p 1621.
Question 48
The radiographic finding in Figure 58 is indicative of what type of acetabular fracture?

Explanation
(SBQ12TR.58) A 35-year-old male was involved in a high speed motorcycle accident. He has a closed head injury, bilateral pulmonary contusions and splenic rupture. His orthopaedic injuries are shown in Figure A. He has a blood pressure of 90/50 mm Hg and a heart rate of 115, despite aggressive resuscitation. An arterial blood gas reveals that his blood lactate is 3.5 and base deficit is -6 mmol/L. Following successful closed reduction of the right hip in the operating room with a percutaneous inserted Schantz pin, what is the next most appropriate treatment for his orthopaedic injuries? Review Topic

Bilateral open reduction and internal fixation
Open reduction internal fixation on the right, reamed intramedullary nailing on the left
Temporizing external fixation on the right, open reduction and internal fixation on the left
Bilateral reamed intramedullary nailing
Bilateral temporizing external fixation
This patient presents with features of hemodynamic instability and a high injury severity score. The next most appropriate treatment would be temporizing external fixation bilaterally. This patient meets the criteria for damage control orthopaedics.
Damage control orthopaedics is an approach that contains and stabilizes orthopaedic injuries so that the patient's overall physiology does not undergo further inflammatory insult. As a result, external fixation of femoral shaft fracture and pelvic stabilization is an effective treatment under this strategy. Other indications include vascular injury and severe open fracture.
Pallister et al. reviewed the effects of surgical fracture fixation on the systemic inflammatory response to major trauma. They show that early stabilization of major long bone fractures is beneficial in reducing the incidence of acute respiratory distress syndrome and multiple organ failure. However, early fracture surgery increases the post-traumatic inflammatory response, which carries a higher complication rate compared to temporary fixation.
Tisherman et al. created clinical guidelines for the endpoints of resuscitation. Level I data found that standard hemodynamic parameters do not adequately quantify the degree of physiologic derangement in trauma patients. The initial base deficit, lactate level, or gastric pH should be used to stratify patients with regard to the need for ongoing fluid resuscitation.
Pape et al. retrospectively reviewed the impact of early total care vs. damage control orthopaedics in the treatment of femoral shaft fractures in polytrauma patients. They found a significantly higher incidence of acute respiratory distress syndrome (ARDS) with intramedullary nailing (15.1%) compared to external fixation (9.1%) when DCO subgroups were compared.
Figure A is a pelvic AP radiograph showing a right hip fracture-dislocation with an ipsilateral femoral shaft fracture. On the left side there is a displaced pertrochanteric hip fracture.
Incorrect Answers:
Question 49
A 10-year-old girl sustained a Gartland type III supracondylar fracture after falling off a trampoline 1 hour ago. She has a well perfused hand but no palpable pulses. The remainder of her examination is otherwise normal. What is the next step in treatment? Review Topic
Explanation
If there is evidence of vascular compromise, the fracture should be reduced and pinned urgently and the limb reevaluated.
Question 50
A 9-year-old girl has had bilateral knee and leg pain for the past 2 years. The family has noted increasing deformity in both lower extremities. She is less than the fifth percentile for height. Examination reveals bilateral femoral bowing, mild medial-lateral laxity of the knees, and the deformities shown in the radiograph seen in Figure 3. What is the most likely diagnosis? Review Topic

Explanation
Question 51
A 14-year-old girl has had mild pain and nail deformity of the great toe for the past 4 months. A radiograph is shown in Figure 50. What is the most likely etiology of the lesion?
Explanation
REFERENCES: Lokiec F, Ezra E, Krasin E, Keret D, Wientraub S: A simple and efficient surgical technique for subungual exostosis. J Pediatr Orthop 2001;21:76-79.
Letts M, Davidson D, Nizalik E: Subungual exostosis: Diagnosis and treatment in children. J Trauma 1998;44:346-349.
Davis DA, Cohen PR: Subungual exostosis: Case report and review of the literature. Pediatr Dermatol 1996;13:212-218.
Question 52
A patient has a C6-7 herniated nucleus pulposus. What is the most likely distribution of symptoms? Review Topic
Explanation
(SBQ12SP.27) A 24-year-old male sustains the injury shown in Figure A. What was the most likely mechanism of injury? Review Topic

Hyperextension
Flexion-distraction
Flexion-compression
Rotational
Pure axial load
Figure A shows a quadrangular fracture pattern of C5. These injuries are observed with flexion-compression loads.
Quadrangular fractures of the cervical spine are considered flexion teardrop fractures. However, they present with a larger anterior lip fragment compared to the classic teardrop fracture pattern. The radiographic findings include a quadrangular-shaped fragment from the anterior one-third of the vertebral body with significant posterior vertebral subluxation, angular kyphosis, and an increased interspinous space with facet subluxation due to disruption of the posterior elements. These are unstable fractures, and almost always require anterior and posterior stabilization.
Moore et al. studied the reliability of Cervical Spine Injury Severity Score to measure stability after cervical spine trauma. The classification system is based on morphologic descriptions and, secondly, on stability based on a quantifiable value. They showed that the Cervical Spine Injury Severity Score had excellent reliability with intra-observer intraclass correlation coefficients (ICC) >0.97 and inter-observer ICC >0.88.
Vaccaro et al. published the subaxial cervical spine injury classification system (SLIC). This systems involves 3 main categories (injury morphology, disco-ligamentous complex, and neurologic status). The overall injury severity score is obtained by summing the scores from each category. They propose that SLIC < 4 can be treated non-operatively.
Allen et al. published a classification system of cervical spine injuries which breaks injuries of the subaxial spine into six phylogenic groups based on mechanism of injury. These include: 1) flexion-compression 2) vertical-compression 3) flexion-
distraction 4) extension-compression 5) extension-distraction 6) lateral flexion. Facet
dislocation
is
caused
by
flexion-distraction
force.
Figure A shows a lateral radiograph of the cervical spine demonstrating a typical flexion-compression fracture with anteriorly displaced quadrangular fragment. Illustration A shows a flexion-compression injury. Illustration B shows the mechanism of injury for a quadrangular fracture of the cervical spine. This unstable fracture pattern is characterized by anterior column failure in flexion/compression and posterior column failure in tension. Illustration C shows an illustration of the fracture morphology according to the Allen and Ferguson classification.
Incorrect Answer 1:
Hyperextension injuries
Flexion-distraction injuries usually result in facet dislocations.
Question 53
What is the most commonly reported complication following elbow arthroscopy?
Explanation
REFERENCES: Kelly EW, Morrey BF, O’Driscoll SW: Complications of elbow arthroscopy.
J Bone Joint Surg Am 2001;83:25-34.
Morrey BF: Elbow complication, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2001, pp 519-522.
Question 54
What is the primary benefit of using rhBMP-2 instead of autogenous bone graft inside an anterior spinal fusion cage?
Explanation
REFERENCE: Burkus JK, Gornet MF, Dickman CA, et al: Anterior lumbar interbody fusion using rhBMP-2 with tapered interbody cages. J Spinal Disord Tech 2002;15:337-349.
Question 55
Which of the following factors is responsible for causing the distal femur to pivot about a medial axis as the knee moves from full extension into early flexion?
Explanation
REFERENCES: Pellicci PM, Tria AJ Jr, Garvin KL (eds): Orthopaedic Knowledge Update:
Hip and Knee Reconstruction 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2000, pp 239-240.
Insall JN, Windsor RE, Scott WN, et al (eds): Surgery of the Knee, ed 2. New York, Churchill Livingstone, 1993, pp 1-13.
Question 56
Primary arthrodesis is associated with which outcome when compared to outcomes associated with open reduction and internal fixation (ORIF) without arthrodesis?
Explanation
There are longitudinal, oblique, and transverse ligaments at the TMT complex that are further defined by their location as dorsal, interosseous, or plantar. There are 3 ligaments between the medial cuneiform and the second MT base, the most important of which is the oblique interosseous ligament, which is also known as the Lisfranc ligament. Plantar and dorsal oblique ligaments contribute to stability to a lesser degree. The dorsal ligaments are weakest and may be the first to fail in a Lisfranc injury.
The second MT base should be aligned with the middle cuneiform at the medial borders, and the fourth MT base should be aligned with the cuboid at the medial borders on the oblique view. The dorsal and plantar aspects of the MTs
should align with the cuneiforms/cuboid on the lateral view. Any malalignment should raise the suspicion of a Lisfranc injury. Diastasis between the second MT and the first MT/medial cuneiform complex of more than 2 mm indicates injury, as does TMT joint subluxation of 2 mm more than seen on the uninjured contralateral side. Diastasis between the first and second MT up to 2.7 mm can be normal. Another radiographic sign of injury includes avulsion fracture of the second MT base or medial cuneiform. Additional imaging studies that may be helpful in identifying subtle injuries include weight-bearing radiographs and CT or MRI images.
Two prospective randomized studies compared primary fusion with ORIF Lisfranc injuries. The second study included fracture-dislocations, whereas the first looked at primarily ligamentous injuries. Results conflicted with an earlier study demonstrating improved results (less pain, better function) with primary fusion, while a more recent study showed no difference. Neither study showed worse results with primary fusion, and the rate of secondary surgery was more common in the ORIF group (salvage arthrodesis or hardware removal).
RECOMMENDED READINGS
Solan MC, Moorman CT 3rd, Miyamoto RG, Jasper LE, Belkoff SM. Ligamentous restraints of the second tarsometatarsal joint: a biomechanical evaluation. Foot Ankle Int. 2001 Aug;22(8):637-41. PubMed PMID: 11527024.View Abstract at PubMed
Watson TS, Shurnas PS, Denker J. Treatment of Lisfranc joint injury: current concepts. J Am Acad Orthop Surg. 2010 Dec;18(12):718-28. Review. PubMed PMID: 21119138.View Abstract at PubMed
Faciszewski T, Burks RT, Manaster BJ. Subtle injuries of the Lisfranc joint. J Bone Joint Surg Am. 1990 Dec;72(10):1519-22. PubMed PMID: 2254360.View Abstract at PubMed
Ly TV, Coetzee JC. Treatment of primarily ligamentous Lisfranc joint injuries: primary arthrodesis compared with open reduction and internal fixation. A prospective, randomized study. J Bone Joint Surg Am. 2006 Mar;88(3):514-20. PubMed PMID: 16510816.View Abstract at PubMed
Henning JA, Jones CB, Sietsema DL, Bohay DR, Anderson JG. Open reduction internal fixation versus primary arthrodesis for lisfranc injuries: a prospective randomized study. Foot Ankle Int. 2009 Oct;30(10):913-22. doi: 10.3113/FAI.2009.0913. PubMed PMID: 19796583. View
Abstract at PubMed
Question 57
Which of the following is included in safety checks on the World Health Organization Safe Surgery Guidelines Checklist?
Explanation
Preoperative checks are necessary for patient safety. On the WHO checklist, critical preoperative check points for the surgeon include: site marking, patient consent, allergies, blood loss, antibiotic prophylaxis, critical and non-routine steps, case duration, and whether preoperative imaging is readily visible.
The WHO Surgical Safety Checklist (see below) has 3 checkpoints: before induction of anesthesia, before skin incision, and before leaving the operating room.
Haynes et al. prospectively collected data on the outcomes of 3733 patients before, and 3955 patients after introduction of the Surgical Safety Checklist in 8 hospitals in 8 cities. They found an improvement in death rate (1.5% before, 0.8% after) and inpatient complication rate (11.0% before, 7.0% after). They concluded that implementation of the checklist led to reduction in death and complication rates.
Illustration A shows the WHO Surgical Safety Checklist. Incorrect Answers:
Question 58
Retrograde ejaculation is most commonly associated with what surgical approach?
Explanation
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Watkins RG (ed): Surgical Approaches to the Spine. New York, NY, Springer-Verlag, 1983,
p 107.
An HS, Riley LH III: An Atlas of Surgery of the Spine. New York, NY, Lippincott Raven, 1998, p 263.
Question 59
Figure 93 is the radiograph of 3½-year-old girl who was evaluated for a progressive increase in tibia vara and complains that her feet are turning in. What is the most appropriate course of action?

Explanation
Question 60
A 19-year-old college student reports a 1-week history of wrist pain following an intramural rugby match. A PA radiograph is shown in Figure 6. He denies any prior wrist injury. What is the best course of action?
Explanation
REFERENCES: Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Chan KW, McAdams TR: Central screw placement in percutaneous screw scaphoid fixation: A cadaveric comparison of proximal and distal techniques. J Hand Surg Am 2004;29:74-79.
Bedi A, Jebson PJ, Hayden RJ, et al: Internal fixation of acute non-displaced scaphoid waist fractures via a limited dorsal approach: An assessment or radiographic and functional outcomes. J Hand Surg Am 2007;32:326-333.
McCallister WV, Knight J, Kaliappan R, et al: Central placement of the screw in simulated fractures of the scaphoid waist: A biomechanical study. J Bone Joint Surg Am 2003;85:72-77.
Question 61
Figure 8 shows the radiograph of a 76-year-old man who has knee pain and swelling. History reveals that he underwent total knee arthroplasty 18 years ago. What is the most likely diagnosis?
Explanation
REFERENCES: Kilgus DJ, Moreland JR, Finerman GA, et al: Catastrophic wear of tibial polyethylene inserts. Clin Orthop Relat Res 1991;273:223-231.
Vince KG: Why knees fail. J Arthroplasty 2003;18:39-44.
Question 62
4 mg/kg for 48 hours
Explanation
Question 63
A 38-year-old woman with metastatic thyroid carcinoma has had increasing pain in the left hip for the past 3 months. An AP radiograph and coronal T 1 -weighted MRI scan are shown in Figures 28a and 28b. Management should consist of
Explanation
REFERENCES: Mirels H: Metastatic disease in long bones: A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop 1989;249:256-264.
Swanson KC, Pritchard DJ, Sim FH: Surgical treatment of metastatic disease of the femur. J Am Acad Orthop Surg 2000;8:56-65.
Clarke HD, Damron TA, Sim FH: Head and neck replacement endoprosthesis for pathologic proximal femoral lesions. Clin Orthop 1998;353:210-217.
Question 64
A 62-year-old man with a long history of right shoulder pain and weakness is scheduled to undergo hemiarthroplasty. Based on the radiographs shown in Figures 6a through 6c, what preoperative factor will most affect postoperative functional outcome?
Explanation
REFERENCES: Iannotti JP, Norris TR: Influence of preoperative factors on outcome of shoulder arthroplasty for glenohumeral osteoarthritis. J Bone Joint Surg Am 2003;85:251-258.
Hettrich CM, Weldon E III, Boorman RS, et al: Preoperative factors associated with improvements in shoulder function after humeral hemiarthroplasty. J Bone Joint Surg Am 2004;86:1446-1451.
Question 65
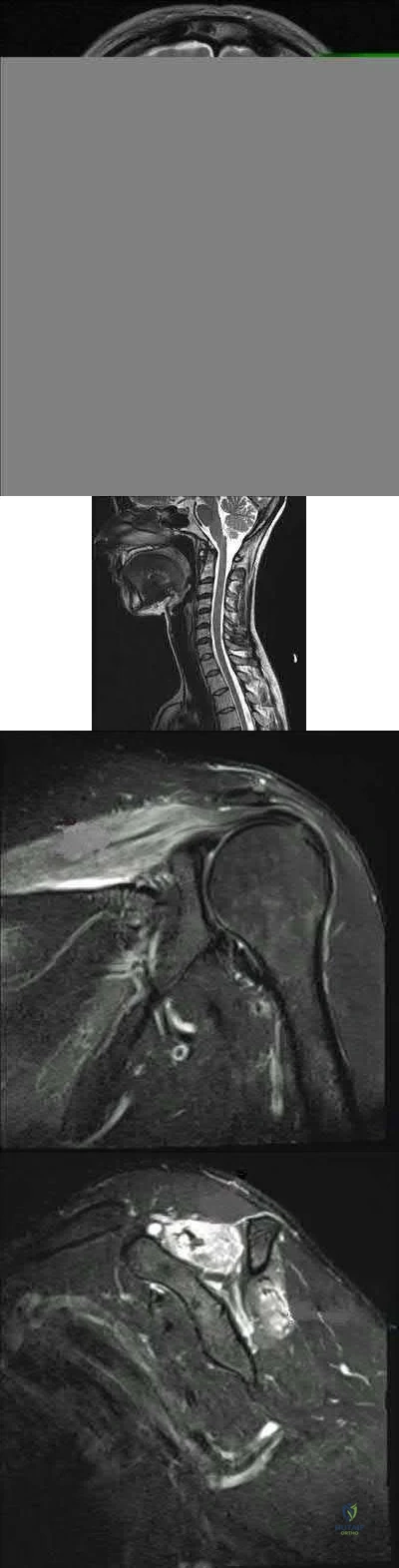
The images reveal T2-weighted MRI sequences with edema isolated to the infraspinatus. In the absence of a tear in the infraspinatus tendon, the edema is most likely due to compression of the suprascapular nerve in the spinoglenoid notch. As this pathology persists, progressive muscle atrophy and fatty infiltration can result. Compression of the suprascapular nerve in the suprascapular notch would have resulted in edema and weakness in both the supra- and infraspinatus muscles. Compression is commonly caused by cysts from the joint secondary to labral tears. A rotator cuff tear of the infraspinatus is not identified on these images, and there is no history of trauma provided. There is no evidence of an anteroinferior labral tear, nor would this be expected to result in external rotation weakness or MRI abnormality of the infraspinatus. Quadrilateral space syndrome results in compression of the axillary nerve, which supplies the teres minor. Correcr answer : C
Explanation
Figure 1 is the radiograph of a 12-year-old baseball player who has posterolateral elbow pain with throwing. The area of interest is designated by the black arrow. His range of motion and strength are full. No previous treatment has been provided. What is the most appropriate initial treatment?
Elbow arthroscopy with debridement
Immobilization and rest for 6 weeks
Corticosteroid injection
Open osteochondral autograft transfer
Osteochondritis dissecans of the capitellum is a painful condition that affects immature athletes who undergo repetitive compression of the radiocapitellar joint. Management is based primarily on the integrity of the articular cartilage surface and the stability of the lesion. Nonsurgical treatment is typically selected for patients
with early-grade, stable lesions, and it involves activity modification with cessation of sports participation. The duration of activity modification is dictated by symptoms, with 3 to 6 weeks of rest followed by return to sport in 3 to 6 months commonly used as a guideline. Strengthening and stretching exercises are commonly incorporated after the pain has subsided. Surgical intervention or corticosteroid injection would not be first-line treatment.
Figures 1 and 2 are the radiographs of a 69-year-old man with a history of treated prostate cancer and hemodialysis-dependent end- stage renal disease who presents to the emergency department with progressively worsening right shoulder pain and stiffness. Laboratory tests reveal a white blood cell count of 17,000, erythrocyte sedimentation rate, 75, and CRP, 10.1. He has a draining sinus located along the anterior shoulder. What is the best next step?
Question 66
A lower chance of failure when using an extensor mechanism allograft to address a chronic disruption of an extensor tendon is associated with
Explanation
Disruption of the extensor mechanism is a rare but devastating complication of knee arthroplasty. Primary repair is associated with a high rate of failure. The results associated with using an extensor mechanism allograft are still variable overall, but the literature on the subject supports tensioning of the allograft in full extension. In studies conducted by Burnett and associates and Nazarian and Booth, the patellar remnant is excised. The use of a fresh-frozen nonirradiated allograft is recommended, and patellar resurfacing of the insensate patella is unnecessary and potentially weakens the allograft.
CLINICAL SITUATION FOR QUESTIONS 133 THROUGH 135
A middle-age man who had an anterior cruciate ligament (ACL) reconstruction with a carbon fiber ligament as a teenager also had a debridement, synovectomy, and a medial unicompartmental arthroplasty. Fourteen years later, he has a painful knee (mainly laterally and anteriorly) that swells with activity. His range of motion is 0 to 120 degrees.
Question 67
An active 47-year-old woman with rheumatoid arthritis reports forefoot pain and deformity and has difficulty with shoe wear. Examination reveals hallux valgus and claw toes. A radiograph is shown in Figure 10. What is the most appropriate surgical treatment?
Explanation
REFERENCES: Coughlin MJ: Arthritides, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, p 572.
Abdo RV, Iorio LJ: Rheumatoid arthritis of the foot and ankle. J Am Acad Orthop Surg 1994;2:326-332.
Question 68
A 7-year-old child is unresponsive, tachycardic, and has a systolic blood pressure of 50 mm Hg after being struck by a car. The patient is intubated and venous access is obtained. The secondary survey reveals an unstable pelvis. Despite adequate resuscitation, the patient continues to be hemodynamically unstable. What is the best course of action?
Explanation
REFERENCES: Torode I, Zieg D: Pelvic fractures in children. J Pediatr Orthop 1985;5:76-84.
Eichelberger MR, Randolph JG: Pediatric trauma-initial resuscitation, in Moore EE, Eisman B, Van Way CE (eds): Critical Decisions in Trauma. St Louis, MO, CV Mosby, 1984, p 344.
Ganz R, Krushell RJ, Jacob RP, Kuffer J: The antishock pelvic clamp. Clin Orthop 1991;267:71-78.
Question 69
Which of the following structures is predominantly composed of Type 1 collagen? Review Topic
Explanation
Type 1 collagen accounts for more than 90% of the total collagen content in the body. Type 1 collagen is found in bone, ligament, tendon, meniscus, annulus of intervertebral discs, skin, healed cartilage, scar tissue, and nerves.
Duthon et al present a review of the ACL and its histologic and mechanical properties. The ACL has a mean length of 32 mm and a width of 7-12 mm. They state that the ACL has a microstructure of collagen bundles of multiple types (mostly type I) and a matrix made of a network of proteins, glycoproteins, elastic systems, and glycosaminoglycans with multiple functional interactions.
Incorrect
1: Epithelial
2: L4 disc
Basement
Membrane is made up of Type
nucleus pulposus is composed of mostly Type
4 collagen.
2 collagen
4: Medial femoral condyle articular cartilage is comprised mostly of Type 2 collagen. 5: Dupuytren's contracture tissue is mostly Type 3 collagen.
Question 70
A 58-year-old man underwent distal radius ORIF with a volar locking plate yesterday. Preoperatively, he reported some mild sensory disturbances in the volar thumb and index finger, but had 2-point discrimination of 6mm in each finger. Now, he complains of worsening hand pain and sensory disturbances in his volar thumb and index finger. Two-point discrimination is now >10mm in these fingers. Radiographs show a well-fixed fracture in good alignment. What is the most appropriate treatment at this time?

Explanation
Mack et al reported on ten cases of acute carpal tunnel syndrome (ACTS) and six cases of nerve contusion in patients with acute median neuropathy associated with blunt wrist trauma. The patients with ACTS initially had normal sensation and subsequently developed objective sensory loss (2-point discrimination greater than 15 mm) in the median nerve distribution associated with severe wrist pain. In contrast, patients with nerve contusion injuries had immediate sensory loss and symptoms were nonprogressive. Four of five patients with ACTS who underwent carpal tunnel release within 40 hours of the onset of numbness had normal 2-point discrimination within 96 hours. Neuropathy, secondary to nerve contusion without coexisting ACTS, may be treated initially by observation.
Ford et al reported of five cases of ACTS. Four with delayed treatment had poor outcomes while the one patient with early CTR had full recovery. All patients with ACTS had increasing and severe pain in the wrist with parasthesia and impaired sensation in the median distribuation. These symptoms initially weren’t present after wrist trauma, but developed rapidly in the next few hours.
Question 71
A 42-year-old female undergoes a subtalar bone block distraction arthrodesis as sequelae of a nonoperatively treated calcaneus fracture ten years prior. This procedure addresses which of the following issues?

Explanation
Question 72
Figure 1 is the ultrasound of a 23-year-old patient who has had a volar radial 1.5-cm tender and painful wrist mass for 6 months. The additional workup prior to surgery should consist of

Explanation
The ultrasound shows a homogeneous anechoic mass consistent with a ganglion cyst. As a benign lesion, no further workup or biopsy is required prior to a marginal surgical excision other than age-appropriate laboratory studies. An MRI study with contrast would provide no diagnostic benefit.
Question 73
-Four months after injury, the tibia is showing evidence of slow healing on radiographs. What is the optimal treatment for this potential nonunion?
Explanation
This patient is unstable and is not a good candidate for Early Total Care (ETC) and therefore should be managed by the tenets of Damage Control Orthopaedics (DCO). Débridement and external fixation is preferable for this patient. Intramedullary nails would be a component of ETC. Calcaneal traction is not considered ideal because it does not allow the patient to travel as easily. The S.P.R.I.N.T. study concluded that while reamed nails may offer benefit in closed fractures, there was no difference between reamed or unreamed nails in the treatment of open fractures of the tibia. Uniplanar external fixation and tibial plating are not considered the best options for open tibia fractures. Additional findings of the S.P.R.I.N.T. study conclude that delaying surgical intervention for at least 6 months after injury may reduce the need for reoperation.
Question 74
A polytrauma patient sustains a right bicondylar tibial plateau fracture and a right humeral shaft fracture both treated with open reduction, internal fixation. He also underwent statically locked intramedullary nailing of a left femoral shaft fracture. What is the appropriate weightbearing status?

Explanation
Question 75
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. What is the next diagnostic step?
Explanation
Question 76
What is the most important preoperative factor predicting conversion to total hip arthroplasty after arthroscopic surgery of the hip?
Explanation
The authors cited in the references examined large databases to determine the risk factors for conversion to total hip arthroplasty after arthroscopic surgery of the hip. In the study by Kester and associates, obesity had an odds ratio (OR) of 5.6 for conversion to hip arthroplasty, whereas age over 60 years had an OR of
Question 77
Radiographs of a pediatric patient reveal a suspected osteosarcoma of the distal femur. Additional staging studies should consist of
Explanation
REFERENCE: O’Reilly R, Link M, Fletcher B, et al: NCCN pediatric osteosarcoma practice guidelines: The National Comprehensive Cancer Network. Oncology (Huntingt) 1996;10:1799-1806, 1812.
Question 78
A professional baseball player has had intermittent, mild shoulder pain for the past 2 years. Nonsurgical management has consisted of anti-inflammatory drugs. Examination reveals atrophy of the infraspinatus muscle but not the supraspinatus. There is weakness in external rotation with the arm at his side but not at 90 degrees of abduction. He has no weakness or pain with resisted abduction. Electromyography confirms an isolated lesion of the suprascapular nerve branch to the infraspinatus. He is otherwise neurologically intact. An MRI scan of the shoulder shows no cysts but confirms atrophy of the infraspinatus muscle. What is the next most appropriate step in management?
Explanation
REFERENCES: Cummins CA, Bowen M, Anderson K, et al: Suprascapular nerve entrapment at the spinoglenoid notch in a professional baseball pitcher. Am J Sports Med 1999;27:810-812.
Cummins CA, Messer TM, Nuber GW: Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-424.
Ferretti A, De Carli A, Fontana M: Injury of the suprascapular nerve at the spinoglenoid notch: The natural history of infraspinatus atrophy in volleyball players. Am J Sports Med 1998;26:759-763.
Question 79
Which of the following 50-year-old patients with an irreparable rotator cuff tendon is the best candidate for an isolated latissimus dorsi muscle transfer? Review Topic
Explanation
Question 80
Which of the following is considered a major characteristic of hyaluronate?
Explanation
REFERENCES: Callaghan JJ, Dennis DA, Paprosky WA, Rosenberg AG (eds): Orthopedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 69-78.
Felson DT: Osteoarthritis. Rheum Dis Clin North Am 1990;16:499-512.
Hurd ER: Extraarticular manifestations of rheumatoid arthritis. Semin Arthritis Rheum 1979;8:151-176.
Question 81
A 74-year-old patient is seen for follow-up 6 weeks after undergoing a total shoulder arthroplasty for glenohumeral osteoarthritis. The patient missed the 2-week follow-up appointment and is currently wearing a sling. The incision is well healed with no signs of breakdown. Examination reveals that passive range of motion is forward elevation of 90 degrees, external rotation at the side 0 degrees, and internal rotation up the back is to the level of the greater trochanter. A radiograph shows no signs of fracture or dislocation. What is the next most appropriate management for this patient? Review Topic
Explanation
Question 82
A 65-year-old woman who works as a florist has had pain in her right elbow for the past 6 months after lifting a flowerpot. MRI scans are shown in Figures 55a and 55b. The area of increased signal intensity seen in Figure 55b most likely represents which of the following findings?
Explanation
REFERENCES: Morrey BF: Tendon injuries about the elbow, in Morrey BF (ed): The Elbow and Its Disorders, ed 2. Philadelphia, PA, WB Saunders, 1993, pp 492-504.
Morrey B: Distal biceps tendon rupture, in Master Techniques in Orthopedic Surgery:
The Elbow, ed 2. Philadelphia, PA, Lippincott Williams and Wilkins, 2002, pp 173-192.
Question 83
A 6-year-old sustains the injury shown in Figures A and B. The nerve most commonly affected by this fracture pattern innervates which of the following motor groups?

Explanation
The most common neurapraxia after pediatric extension-type supracondylar fractures involve the AIN. It supplies the FPL (thumb IP flexion), the pronator quadratus, and the FDP of the index/long fingers. Subsequently, patients are often unable to make an “a-ok” sign. Most of these neuropraxias resolve without complication. The ulnar nerve is most commonly implicated with flexion-type supracondylar fractures.
Abzug et al. review management of supracondylar fractures. They note that the AIN
is most commonly injured nerve in extension type supracondylar fractures. They note that nerve injuries often resolve within 6-12 weeks.
Babal et al. completed a meta-analysis to determine the risk of neurapraxia associated with pediatric supracondylar fractures. The rate of traumatic neurapraxia was 11.4% amongst 5000 patients. The AIN was affected 34.1% of the time. AIN neurapraxia was most common in extension type injuries.
Figures A and B show an AP and lateral radiographs of a displaced pediatric supracondylar fracture
Incorrect Answers
Question 84
A 13-year-old girl has had pain in her ankle and difficulty with sporting activities for the past 6 months. Nonsteroidal anti-inflammatory drugs and use of a short leg cast have provided minimal relief. A radiograph and MRI scan are shown in Figures 43a and 43b. What is the next most appropriate step in treatment?
Explanation
REFERENCES: McCormack TJ, Olney B, Asher M: Talocalcaneal coalition resection: A 10-year follow-up. J Pediatr Orthop 1997;17:13-15.
Thometz J: Tarsal coalition. Foot Ankle Clin 2000;5:103-118.
Question 85
Figures 15a through 15c show the radiographs of a 23-year-old football player who was injured when another player fell on his flexed and planted foot. He reports severe pain in the midfoot with a feeling of numbness on the dorsum of the foot, and he is unable to bear weight on the limb. Examination reveals mild swelling. Management should consist of
Explanation
REFERENCES: Baxter DE: The Foot and Ankle in Sport, ed 1. St Louis, MO, Mosby, 1995,
pp 107-123.
Curtis MJ, Myerson M, Szura B: Tarsometatarsal joint injuries in the athlete. Am J Sports Med 1993;21:497-502.
Kuo RS, Tejwani NC, DiGiovanni CW, et al: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am 2000;82:1609-1618.
Thompson MC, Mormino MA: Injury to the tarsometatarsal joint complex. J Am Acad Orthop Surg 2003;11:260-267.
Question 86
A previously healthy 29-year-old man reports a 2-day history of severe atraumatic lower back pain. He denies any bowel or bladder difficulties and no constitutional signs. Examination is consistent with mechanical back pain. No focal neurologic deficits or pathologic reflexes are noted. What is the most appropriate management? Review Topic
Explanation
Question 87
Figure 7 shows the CT scan of a 22-year-old professional baseball pitcher who has had elbow pain for the past 6 months despite rest from throwing. Management should consist of
Explanation
REFERENCES: Ahmad CS, ElAttrache NS: Valgus extension overload syndrome and stress injury of the olecranon. Clin Sports Med 2004;23:665-676.
Garrick JG (ed): Orthopaedic Knowledge Update: Sports Medicine 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 101-111.
Question 88
A 55-year-old woman with a 15-year history of systemic lupus erythematosus has had left shoulder pain for the past 3 months. She reports that the pain has grown progressively worse over the past few months, and her shoulder function is severely limited. She is presently being treated with azathioprine and has used corticosteroids in the past. AP and axillary radiographs are shown in Figures 19a and 19b, and MRI scans are shown in Figures 19c and 19d. Which of the following forms of management will yield the most predictable pain relief and return of shoulder function?
Explanation
REFERENCES: Hattrup SJ, Cofield RH: Osteonecrosis of the humeral head: Results of replacement. J Shoulder Elbow Surg 2000;9:177-182.
L’Insalata JC, Pagnani MJ, Warren RF, et al: Humeral head osteonecrosis: Clinical course and radiographic predictors of outcome. J Shoulder Elbow Surg 1996;5:355-361.
Cruess RL: Steroid-induced avascular necrosis of the head of the humerus: Natural history and management. J Bone Joint Surg Br 1976;58:313-317.
Question 89
A 24-year-old runner who underwent an allograft reconstruction of the anterior cruciate ligament (ACL) 3 years ago now reports anterior knee pain. Examination reveals no swelling or effusion, and the patient has full motion. A Lachman test and a pivot-shift test are negative. Palpation reveals tenderness on the patellar tendon and at the inferior pole of the patella. AP and lateral radiographs are shown in Figures 41a and 41b. Management should consist of
Explanation
REFERENCES: Fahey M, Indelicato PA: Bone tunnel enlargement after anterior cruciate ligament replacement. Am J Sports Med 1994;22:410-414.
Victoroff BN, Paulos L, Beck C, Goodfellow DB: Subcutaneous pretibial cyst formation associated with anterior cruciate ligament allografts: A report of four cases and literature review. Arthroscopy 1995;11:486-494.
Question 90
03 Figure 33 shows the radiograph of a 48-year-old man who sustained a fracturedislocation of his dominant arm and a significant head injury in a fall from a roof. Eight days after injury he is medically cleared for surgery. Treatment should consist of

Explanation
proximal humerus, with what appears to be a head-splitting component. Answer 1
(rotator cuff repair) is certainly not indicated yet – maybe as a secondary procedure
once the bone is healed, or as a subsequent procedure while dealing with the fracture.
Similar to question #109, there is no need to resurface the glenoid unless we have
evidence of significant degenerative changes, which we don’t. ORIF of head-splitting
fractures hasn’t had any promising results, and AVN is always an issue here. Both
articles referenced discuss the outcomes of acute hemiarthroplasty in the
treatment of 3- and 4-part proximal humerus fractures versus late replacement for
failed non-operative treatment, and the benefits of early management in regards
to difficulty of procedure, post-operative pain, and functional ROM/strength outcomes. Arthrodesis is a viable option, but not with the good results of hemiarthroplasty as evidenced here.
Goldman RT, Koval KJ, Cumom F, Gallagher MA, Zuckerman JD: Functional outcome after humeral head replacement for acute three- and four-part proximal humeral fractures. J Shoulder Elbow Surg 1995;4:81-86.
Norris TR, Green A, McGuigan FX: Late prosthetic shoulder arthroplasty for displaced proximal humerus fracture. J Shoulder Elbow Surg 1995;4:271-280.
back to this question next question
Question 91
Which of the following best describes athletic pubalgia?
Explanation
REFERENCES: Meyers WC, Foley DP, Garrett WE, Lohnes JH, Mandlebaum BR: Management of severe lower abdominal or inguinal pain in high-performance athletes: PAIN (Performing Athletes with Abdominal or Inguinal Neuromuscular Pain Study Group). Am J Sports Med 2000;28:2-8.
Albers SL, Spritzer CE, Garrett WE Jr, Meyers WC: MR findings in athletes with pubalgia. Skeletal Radiol 2001;30:270-277.
Question 92
Which of the following statements best describes the process of articular cartilage degeneration in osteoarthritis?
Explanation
REFERENCE: Buckwalter JA, Mankin HJ, Grodzinsky AJ: Articular cartilage and osteoarthritis. Instr Course Lect 2005;54:465-480.
Question 93
A 28-year-old woman has left shoulder pain and a tender soft-tissue mass. Based on the MRI scan and biopsy specimens shown in Figures 74a through 74c, what is the most likely diagnosis?
Explanation
REFERENCES: Damron TA, Sim FH: Soft-tissue tumors about the knee. J Am Acad Orthop Surg 1997;5:141-152.
Weiss SW, Goldblum JR, Enzinger FM: Enzinger and Weiss’s Soft Tissue Tumors, ed 4. Philadelphia, PA, Elsevier, 2001, pp 1146-1167.
Question 94
What mechanism contributes to strength gains during conditioning of the preadolescent athlete?
Explanation
REFERENCES: Grana WA: Strength training, in Stanitski CL, DeLee JC, Drez D Jr (eds): Pediatric and Adolescent Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 520-526.
Micheli LJ: Strength training, in Sullivan JA, Grana WA (eds): The Pediatric Athlete. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 17-20.
Question 95
A 25-year-old male professional lacrosse player collides with another player, with injury resulting from a knee impacting the athlete’s thigh. He has immediate pain in the mid-thigh area and is unable to return to the game because of difficulty with running. Examination reveals developing swelling in the anterior mid-thigh area. The thigh compartments are soft, and he is able to extend his knee against gravity. Knee flexion at 90° gives him discomfort in the thigh but no knee pain. The knee and hip examinations are otherwise unremarkable. Plain films of the femur are negative. What is the best next step?
Explanation
A. only type 1 collagen.
B. only type 2 collagen.
C. type 1 and type 2 collagen.
D. neither type 1 or type 2 collagen.
The MRI scan shows a full-thickness cartilage defect. When treated with a marrow stimulation technique, such as a microfracture, the reparative tissue is fibrocartilage. Unlike hyaline cartilage, which is composed of only type 2 collagen, fibrocartilage is composed of both type 1 and type 2 collagen.
15- Figures 1 and 2 are the radiographs of a 58-year-old retired laborer who has had many years of right shoulder pain. He initially experienced relief with anti-inflammatory medication over the past year, but this no longer provides him pain relief. He has pain with overhead activities and is dissatisfied with his shoulder function. Examination indicates active and passive forward elevation to 130°, full strength with external rotation, and a negative belly press test. MRI demonstrates an intact rotator cuff. What is the best next step in treatment?
A. Anatomic total shoulder arthroplasty (TSA)
B. Hemiarthroplasty
C. Reverse shoulder arthroplasty
D. Arthroscopy with debridement and biceps tenodesis
The patient has glenohumeral osteoarthritis based on the radiograph. His examination demonstrates limited motion and no significant rotator cuff pathology – full strength with external rotation, negative belly press, and no pseudoparalysis. Of all the answer choices, an anatomic TSA would be the most appropriate treatment option. Hemiarthroplasty does not address glenoid pathology and provides inferior pain relief and function, compared with TSA. A reverse shoulder arthroplasty is utilized for patients with degenerative shoulder changes in conjunction with irreparable rotator cuff pathology. Shoulder arthroscopy with debridement and biceps tenodesis is not appropriate for those with severe degenerative changes of the shoulder.
16- According to the MRI scan shown in Figure 1, which pathologic finding is expected to be encountered during arthroscopy?
A. Figure 2
B. Figure 3
C. Figure 4
D. Figure 5
The sagittal MRI scan is a clear example of a double posterior cruciate ligament (PCL) sign. This sign has a high specificity for a displaced bucket handle tear of the medial meniscus as seen in Figure 4. The other arthroscopic
images show a flap tear of the medial meniscus (Figure 2), anterior cruciate ligament tear (Figure 3), and a full thickness articular cartilage defect (Figure 5). Other less likely causes of a double PCL sign include intermeniscal ligament, meniscofemoral ligaments, loose bodies, osteophytes, and fracture fragments. Correct answer : C 13
17- Figures 1 and 2 are the radiographs of a 21-year-old football player who underwent anterior cruciate ligament (ACL) reconstruction with patellar tendon autograft 1 year ago. He reports mild stiffness in his knee. Upon examination, he has a negative Lachman test, trace effusion, and range of motion from 0 to 85° of knee flexion. Which factor is most contributory to his examination findings?
A. Incorrect graft choice
B. Improper tunnel position
C. Tibial graft-tunnel mismatch
D. Femoral fixation at 80° flexion
Technical failure is the most common reason for ACL reconstruction failure. Tunnel position is the most frequent cause of technical failure. Malpositioning of the tunnel affects the length of the graft, causing either decreased range of motion or increased graft laxity. This patient has anterior and vertical placement of his femoral tunnel, which has been shown to cause stiffness in knee flexion. Although graft choice is an important factor when planning ACL reconstruction, overall outcomes with autograft tissues are fairly similar. Fixation of the graft at the femoral or tibial end is not as important as tunnel position. Fixing the graft in flexion can cause extension loss when isometry is not achieved, but this condition is not touched upon in this scenario.
Question 96
What is the most frequent complication of percutaneous repair of an acute Achilles tendon rupture?
Explanation
REFERENCES: Aracil J, Pina A, Lozano JA, et al: Percutaneous suture of Achilles tendon ruptures. Foot Ankle 1992;13:350-351.
Sutherland A, Maffulli N: A modified technique of percutaneous repair of the ruptured Achilles tendon. Oper Orthop Traumatol 1998;10:50-58.
Assal M, Jung M, Stern R, et al: Limited open repair of Achilles tendon ruptures: A technique with a new instrument and findings of a prospective multicenter study. J Bone Joint Surg Am
2002;84:161-170.
Question 97
A polytrauma patient sustains a right bicondylar tibial plateau fracture and a right humeral shaft fracture both treated with open reduction and internal fixation. He also underwent statically locked intramedullary nailing of a left femoral shaft fracture. What is the appropriate weightbearing status?
Explanation
Tingstad et al found favorable results of immediate weightbearing on humeral shaft fractures treated with plating and full weightbearing did not have any effect on the union or malunion rates.
Brumback et al evaluated the feasibility, safety and efficacy of immediate
weightbearing after treatment of femoral shaft fractures with statically locked IM nail. All the patients went on to union and no loss of fixation occurred.
OrthoCash 2020
Question 98
A 34-year-old man underwent open reduction and internal fixation of a closed both bones forearm fracture 11 months ago. The radiographs shown in Figures 32a and 32b reveal a 3-mm gap and loose screws. What is the best treatment option?
Explanation
REFERENCES: Ring D, Allende C, Jafarnia K, et al: Ununited diaphyseal forearm fractures with segmental defects: Plate fixation and autogenous cancellous bone-grafting. J Bone Joint Surg Am 2004;86:2440-2445.
Question 99
Figures 29a and 29b show the radiograph and CT scan of a 48-year-old man who has diffuse spinal pain. What is the most likely diagnosis?
Explanation
REFERENCES: McCullough JA, Transfeldt EE: Macnab’s Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 190-194.
Frymoyer JW, Wiesel SW (eds): The Adult and Pediatric Spine, ed 3. Philadelphia, PA, Lippincott, Williams and Wilkins, 2003, pp 141-151.
Question 100
A year-old woman with a history of osteoporosis is involved in a high-speed motor vehicle accident, resulting in left hip pain and deformity. The initial radiograph from the trauma bay is shown in Postreduction CT is shown in 2 through What is the most appropriate definitive surgical treatment?
Explanation
The radiograph shows a posterior wall acetabular fracture-dislocation. Post reduction CT indicates a large comminuted posterior wall fracture with marginal impaction of the articular surface. A comminuted femoral head fracture also is seen extending to the superior weight-bearing surface. Given the marginal
impaction of the acetabulum and the considerable comminution of the femoral head (which is likely unreconstructible), this injury would have a high risk of causing posttraumatic arthritis if treated with ORIF of the fractures alone. Considering this fact and the patient’s age, ORIF of the posterior wall and acute total hip arthroplasty would likely have the best functional result and the lowest risk of reoperation. Hemiarthroplasty is inappropriate for this injury considering the acetabular fracture. Skeletal traction currently plays a limited role in the definitive treatment of acetabular fractures.
